Back to Journals » Clinical Ophthalmology » Volume 20
Prospective Randomized Study of Visual Outcomes with Mini-Monovision Between the Light-Adjustable Lens and Clareon Monofocal Toric Intraocular Lens
Authors Blehm C ![]() , Balest Z, Hall B
, Balest Z, Hall B ![]()
Received 8 April 2026
Accepted for publication 23 June 2026
Published 9 July 2026 Volume 2026:20 610426
DOI https://doi.org/10.2147/OPTH.S610426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Clayton Blehm,1 Zach Balest,1 Brad Hall2
1North Georgia Eye Associates, Gainesville, GA, USA; 2Sengi, Penniac, NB, Canada
Correspondence: Clayton Blehm, North Georgia Eye Associates, Gainesville, GA, USA, Tel +1 770 532 4444, Email [email protected]
Purpose: To compare binocular visual outcomes between the Light-Adjustable Lens (LAL) and the Clareon monofocal toric intraocular lens when both are targeting mini-monovision.
Methods: This was a prospective, randomized, double-arm, multi-surgeon study. Subjects were evaluated at 1 and 3 months postoperatively. Data collected included monocular and binocular uncorrected and distance corrected visual acuities at distance (UDVA, CDVA), intermediate (66 cm; UIVA, DCIVA), and near (40 cm; UNVA, DCNVA), higher order aberrations (HOA), administration of the Patient-Reported Spectacle Independence Questionnaire (PRSIQ), manifest refraction, monocular and binocular defocus curve, and the postoperative number of visits and days to release of care.
Results: Seventy patients in the Clareon group and 68 in the LAL group completed the study. At three months, Clareon was non-inferior to LAL for all binocular corrected and uncorrected visual acuities except UNVA. Spectacle independence for distance, intermediate, and near were 91% (64/70), 87% (61/70), and 33% (23/70) (Clareon) vs 93% (63/68), 94% (64/68), and 43% (29/68) (LAL). Routine care release took 31.7 ± 13.0 days (Clareon) vs 53.9 ± 17.5 days (LAL) (p < 0.001). Both groups had high refractive accuracy at 3 months, however, outcomes with Clareon remained stable from 1 to 3 months, while LAL improved with UV treatment.
Conclusion: Results of this study suggest similarly good refractive and visual outcomes for both Clareon monofocal/toric and LAL when both are targeting same mini-monovision.
Keywords: mini-monovision, LAL, Clareon, monofocal
Introduction
Cataract surgery patients are increasingly expecting spectacle independence at far, intermediate, and near following intraocular lens (IOL) implantation. Monofocal IOLs are the most popular type of implant, offering good visual outcomes at far distances. The Clareon monofocal IOL (Alcon Vision, LLC) is composed of a hydrophobic acrylic material containing phenylethyl acrylate blended with some hydroxyethyl methacrylate (HEMA) and a UV absorber with or without a blue-light filtering chromophore. We previously reported on the visual and refractive outcomes with the Clareon monofocal IOL.1 The results of that study suggested good distance vision, functional intermediate vision, and stable refraction for patients.1 Other studies have reported similar outcomes.2–4 However, as with any monofocal implant, spectacles may still be needed to see clearly at near distances. Diffractive multifocal and extended depth of focus IOLs offer greater spectacle independence at intermediate and near compared to a monofocal, although with the risk of unwanted visual disturbances.5–8 In addition, enhanced monofocals may offer improved intermediate vision, compared to their parent monofocal IOLs, but with similar distance vision and photic phenomena.9
Another option for patients is the use of mini-monovision, where the dominant eye is targeted for emmetropia and the contralateral eye for slight myopia.10 This allows the dominant eye to see clearly at far distances and the non-dominant eye to provide excellent intermediate and functional near vision. Mini-monovision can be achieved using monofocal, multifocal, or EDOF IOLs—although monofocal implants may have cost savings and fewer visual disturbances compared to multifocal and EDOF lenses.11–13
The light-adjustable lens (LAL; RxSight, Inc.) is a relatively new tool for surgeons to achieve the refractive target following IOL implantation. It is currently the only US Food and Drug Administration (FDA) approved IOL capable of postoperative IOL sphere and cylinder power adjustment and is indicated for the correction of astigmatism following cataract surgery and lens implantation. The LAL contains a special light-sensitive material that responds to ultraviolet (UV) light from the Light Delivery Device (LDD; RxSight, Inc). Through a series of treatments, this allows relatively non-invasive adjustments to lens refractive power. When the target refraction is achieved, the polymers of the material can be “locked-in” with 2 additional UV lock-in treatments to prevent future refractive changes.14 However, compared to a fixed power monofocal IOL, the LAL requires more postoperative visits (3–5 total UV treatments) and significant costs.15 Studies of the LAL have reported good visual and refractive outcomes for patients, including those with prior corneal refractive surgery.16–18 The ability to adjust the lens refractive power allows the LAL to be applied for different anisometropia strategies, including blended vision.19 Currently, there is limited data on the use of the LAL for mini-monovision. Comparative outcomes between the LAL and monofocal intraocular lenses with similar refractive target approach remain largely unreported. The purpose of this study was to compare visual outcomes between the LAL and the Clareon monofocal/toric IOL when both are targeting mini-monovision.
Methods
Design
This was a randomized, prospective, double-arm, multi-surgeon, single-site study of visual outcomes with mini-monovision between a monofocal toric IOL and an adjustable IOL. There was no masking as the LAL group received UV treatment and the Clareon group did not. An independent institutional review board approved the study (Salus IRB, approval #CB-23-02). The study was conducted in a private practice, therefore an independent review board was used. The study was registered on clinicaltrials.gov (NCT06122103), and followed the tenets of the Declaration of Helsinki, and International Harmonization (ICH) guidelines, and Good Clinical Practice (GCP). All study participants gave written informed consent before participation.
Participants
Inclusion criteria were adult patients undergoing age-related cataract surgery with expected corrected distance visual outcomes of 20/25 or better with regular corneal astigmatism of 0.75 D to 2.50 D (corresponding to on label treatment with LAL) and dilated pupil diameter of 7 mm or greater. Exclusion criteria were moderate-severe corneal pathology, irregular astigmatism, preexisting macular disease, and other retinal degenerative diseases that is expected to cause future vision loss, glaucoma, severe dry eye disease, history of uveitis, ocular herpes simplex viral infection, nystagmus, strabismus, zonular laxity or dehiscence, pseudoexfoliation, history of corneal refractive and intraocular surgery, and patients taking systemic medication that may increase sensitivity to UV light or that may cause toxicity to the retina.
Eligible subjects were randomized to receive mini-monovision with either the Clareon monofocal/toric IOL (Clareon Group) or with the light-adjustable lens (LAL Group). Randomization was performed using block randomization which was determined prior to recruitment and applied sequentially to enrolled participants.
Surgery
Preoperative biometry measurements were obtained using the Argos (Movu, a Santec Company) and the Atlas 9000 (Carl Zeiss Meditec). Total corneal power was determined using the Argos, which incorporates both anterior and posterior corneal astigmatism. Using the Argos and Barrett Universal II and Barrett Toric formulas, the dominant eye was targeted for emmetropia and the non-dominant for −1.00 D in the Clareon group, while the LAL group followed the manufacturer’s recommendation of a +0.25 D target in both eyes. The lens constant used was 119.1 for both the LAL and Clareon IOLs. Intraoperative aberrometry (the ORA System® with Verifeye+ TechnologyTM, Alcon Vision LLC) was used to confirm preoperative planning and toric power and final alignment for the Clareon IOL. All patients underwent femtosecond laser assisted cataract surgery with the Ally Robotic Cataract Laser System (Lensar). The non-dominant eye was completed first followed by the dominant eye one week apart. Clareon monofocal toric and non-toric IOLs (Alcon Vision, LLC) and the light-adjustable lens (RxSight) were implanted in each respective group. The refractive lens power of the implanted LAL IOLs was adjusted at postoperative visits, approximately 1–3, which began approximately 17–28 days after 2nd eye surgery and continued approximately weekly until the target refraction was achieved. At these visits, a manifest refraction was performed, then eyes were dilated and the LDD treatments were assigned to target emmetropia in the dominant eyes and −1.0 D in the non-dominant eyes. When the target refraction was achieved, there were 2 subsequent postoperative UV lock-in treatments to finalize the final refractive power of the LAL IOLs, which were approximately 1 week apart. In this study, we use the term “mini-monovision” to describe a refractive strategy that targets emmetropia in the dominant eye and slight myopia in the non-dominant eye. A final target of −1.00 D was chosen to give a reasonable range of vision for both arms without compromising stereoscopic vision.
Intraocular Lenses
The Clareon monofocal IOL incorporates a hydrophobic acrylic material, made up of hydroxyethyl methacrylate (HEMA), phenylethyl acrylate, and a UV absorber. It is a single piece fixed power monofocal IOL. The overall length is 13 mm, with a 6 mm biconvex aspheric optic. The LAL is a 3-piece silicone IOL. The optic is composed of a photoreactive, UV-absorbing silicone material with a biconvex design and a 6.0 mm optic diameter. The haptics are manufactured from blue-core polymethylmethacrylate (PMMA) monofilament.
Procedures
All subjects in both groups attended visits at postoperative months 1 and 3 (following the second eye surgery). However, subjects in the LAL group attended 3–5 postoperative visits depending on the number of UV treatments needed to adjust the desired refractive power. Monocular and binocular uncorrected and distance corrected visual acuities at distance (UDVA and CDVA), intermediate (66 cm; UIVA and DCIVA), and near (40 cm; UNVA and DCNVA) were assessed using standard Early Treatment Diabetic Retinopathy (ETDRS) charts (Precision Vision). Chart background luminance was maintained approximately at 85 cd/m2. The iTrace system (Tracey Technologies) was used to assess higher order aberrations (HOA). The aperture size for HOA measurement was determined automatically by the iTrace at the time of acquisition. The Cassini topographer (i-Optics) was used to measure pupil sizes under photopic and mesopic conditions. Subjects were administered the Patient-Reported Spectacle Independence Questionnaire (PRSIQ). Data were also collected for manifest refraction, monocular distance corrected defocus curve, and binocular target corrected defocus curve.
Outcome Measures
The key outcome measures included binocular and monocular CDVA, UDVA, DCIVA, UIVA, refractive outcomes, and efficiency data (number of days and postoperative visits until routine release of care). Exploratory outcome measures included binocular DCNVA, UNVA, monocular and binocular defocus curves, patient-reported outcomes on the PRSIQ, and HOAs.
Statistical Analysis
All statistical analyses were performed using the software R (version 4.4.2, The R Foundation for Statistical Computing, Vienna, Austria). Visual outcomes were compared using the 2-sample t-test. If the upper boundary of the 95th confidence interval was not greater than 0.1 logMAR, non-inferiority was claimed for the Clareon Group compared to the LAL Group. A margin of 0.10 logMAR represents 5 letters of visual acuity and has been used in previous FDA clinical trials.20 To control the family-wise Type I error rate, non-inferiority of the 3-month postoperative binocular endpoints were evaluated using a sequential testing method on outcomes in the following order: CDVA, UDVA, DCIVA, UIVA, DCNVA, and UNVA. Testing began on the first outcome in the sequence and stopped when an endpoint could not be confirmed as non-inferior. All other statistical comparisons, as detailed below, were exploratory and should be interpreted with appropriate caution.
Exploratory comparisons for defocus curves were achieved using a mixed model for repeated measures, which adjusted for any bias from multiple measures with the same subject for the different levels of defocus. From the defocus curves, areas under the curve (AUC) below 0.30 logMAR were calculated using the trapezoidal numerical integration method, normalizing the 0.5 D defocus steps.21 The total defocus range for AUC was +1.00 D to −2.50 D, including +0.50 D to −0.50 D for far and −0.50 D to −2.00 D for intermediate, and −2.00 D to −2.50 D for near. Responses on the PRSIQ were compared using the Chi-squared statistic. Higher order aberrations were compared using an analysis of variance. Post-hoc exploratory inferential statistics included comparisons for monocular visual outcomes and postoperative HOAs at 3 months postoperatively. These exploratory comparisons were performed using linear mixed effects models, which adjusted for any bias from multiple measures with the same subject. In all cases, a p-value ≤0.05 was considered significant. We estimated that the study would require a sample of 69 subjects in each group (138 total), assuming a difference in mean visual acuity between groups of 0.05 logMAR, a pooled standard deviation of 0.1 logMAR, a power of 90%, and an alpha of 0.05.
Results
Safety
Participant flow diagram is shown in Figure 1. The preoperative and patient demographics are summarized in Table 1. There were no significant differences between groups. There were 6 adverse events in the Clareon group and 14 in the LAL group. For the Clareon group, these were YAG laser capsulotomy (4) and dry eye (2). The LAL events included YAG laser capsulotomy (4), dry eye (7), Herpes simplex virus keratitis (2), and endophthalmitis (1). Standard graphs for IOL studies are shown in Figure 2 for postoperative month 3 (binocular outcomes), in Figures 3 and 4 for postoperative month 3 (monocular outcomes) for the dominant and non-dominant eyes, respectively, and in Figures 5 and 6 for postoperative month 1 (monocular outcomes) for the dominant and non-dominant eyes.
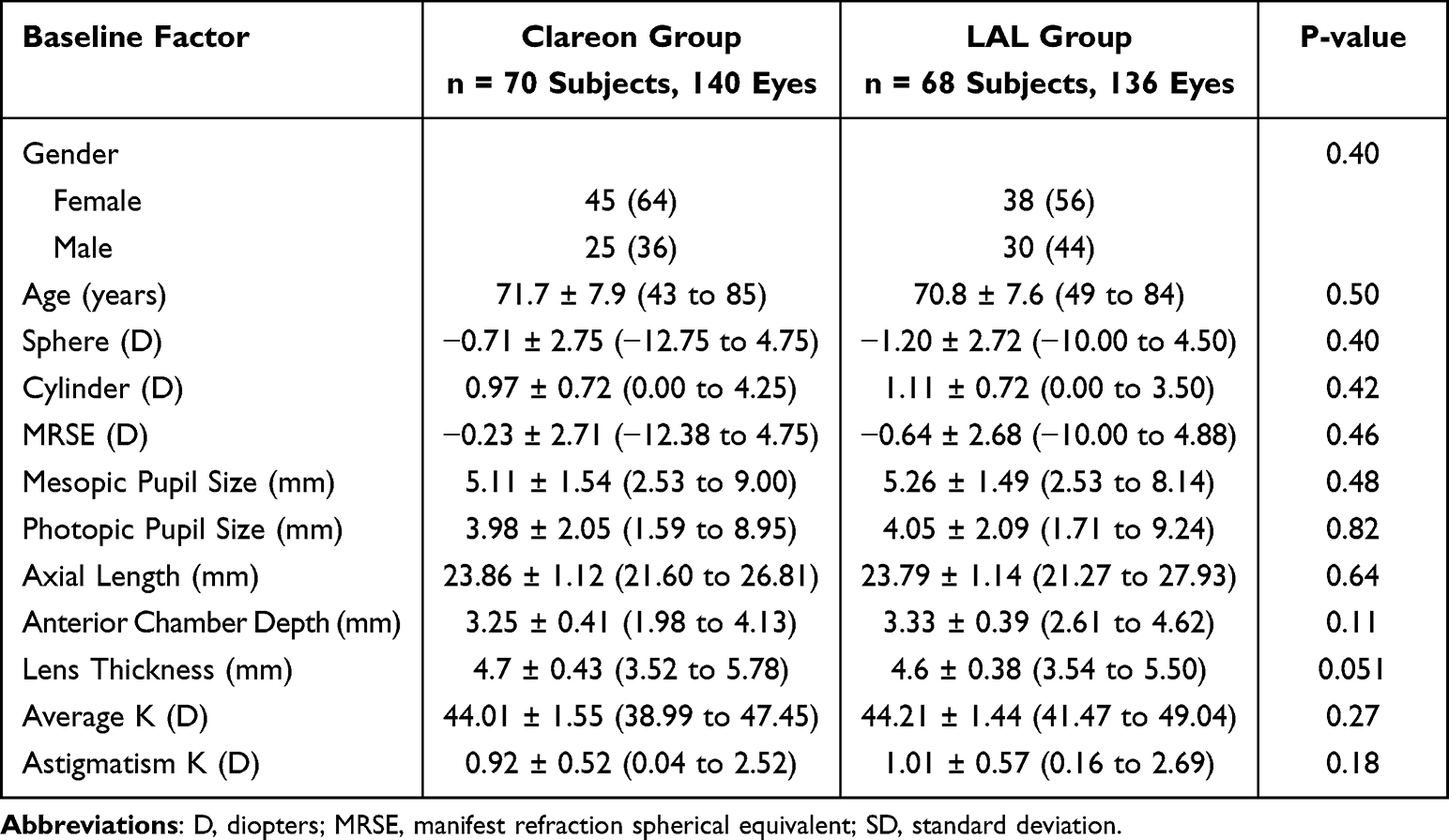 |
Table 1 Preoperative and Demographic Data |
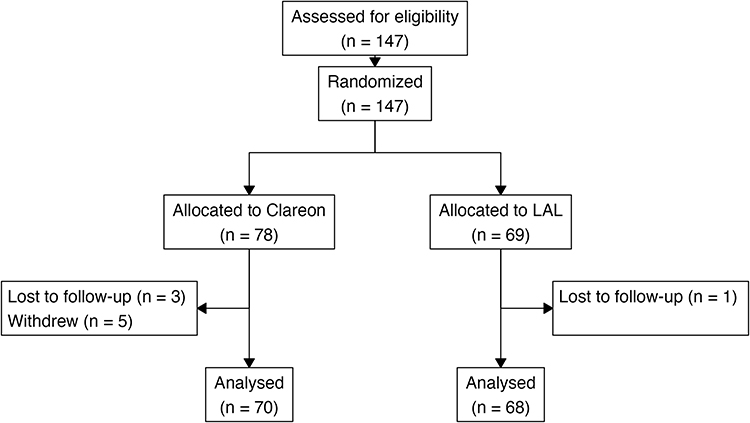 |
Figure 1 Flow diagram of participant progress through the study. |
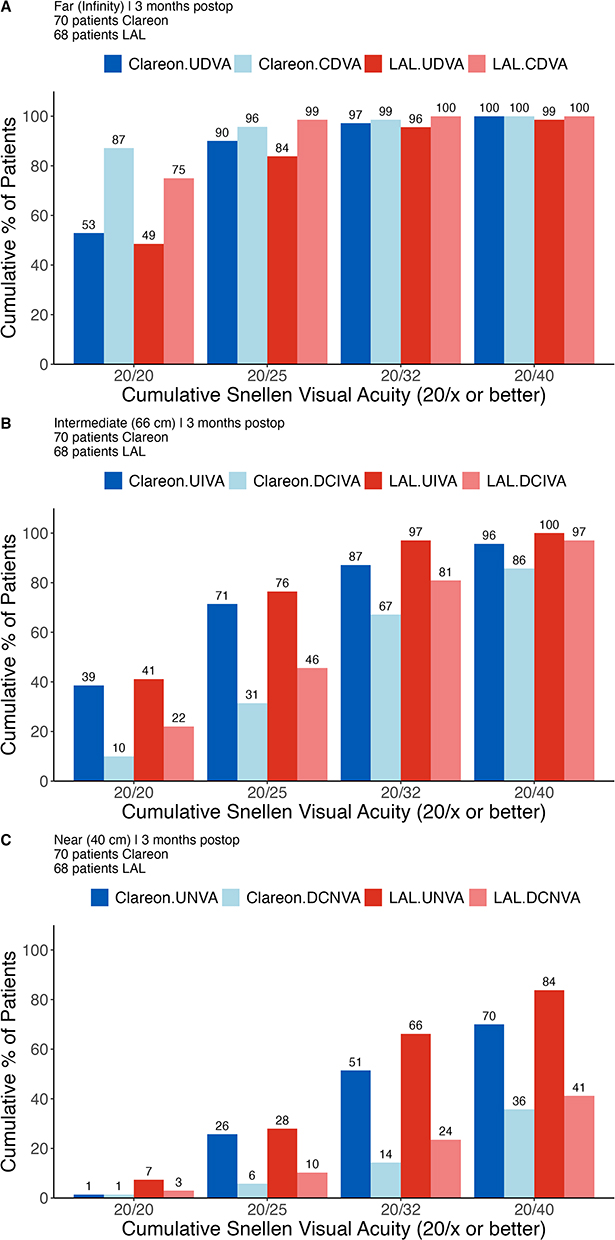 |
Figure 2 Cumulative percentage of patients achieving binocular uncorrected and distance corrected visual acuities, (A) far, (B) intermediate, (C) near. |
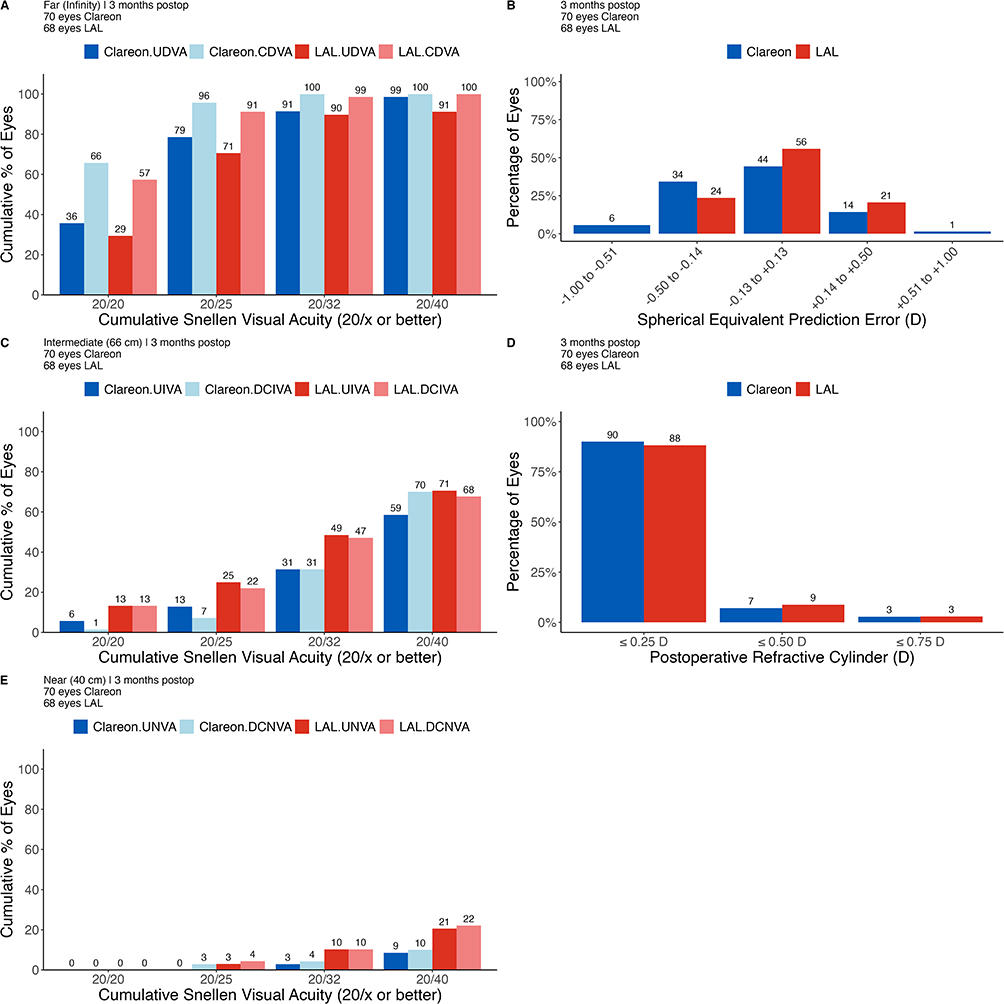 |
Figure 3 Standard efficacy plots for intraocular lenses at postoperative month 3 for the dominant eyes. (A) Cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at far, (B) postoperative spherical equivalent prediction error distribution, (C) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at intermediate, (D) postoperative refractive cylinder distribution, and (E) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at near. |
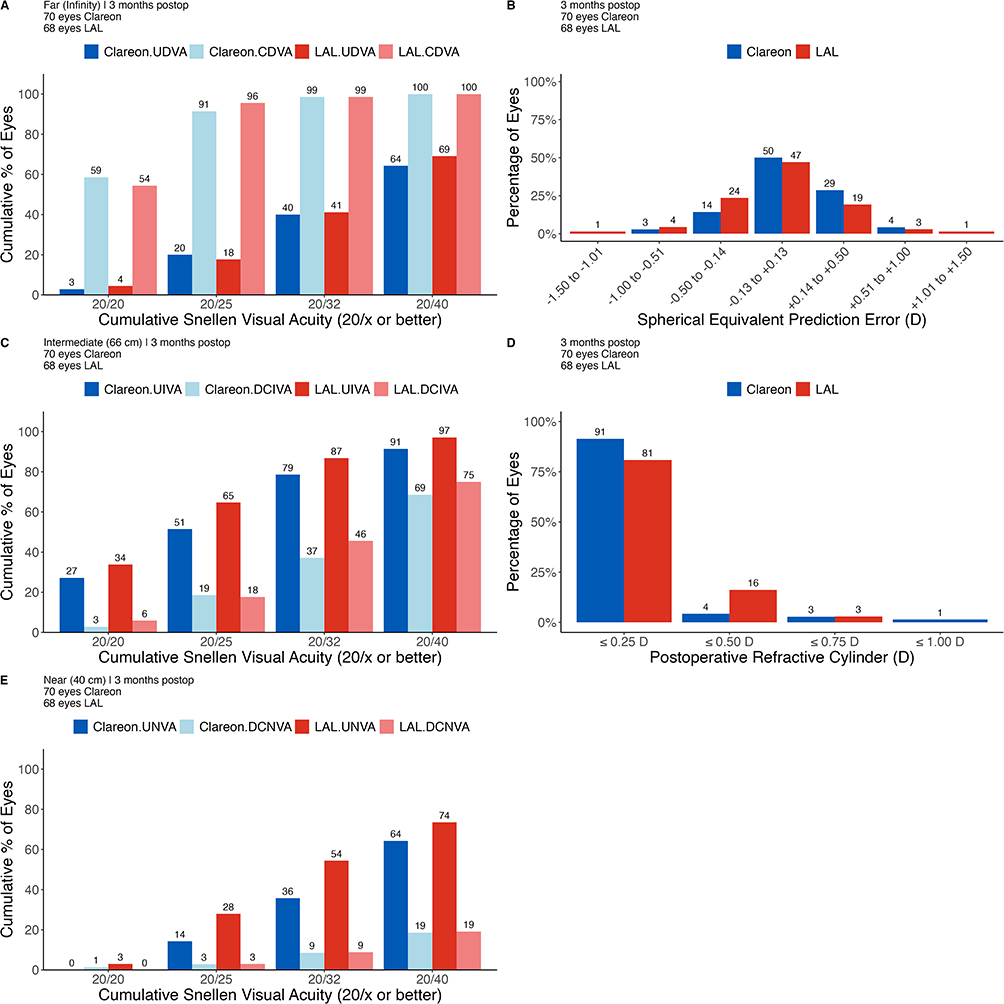 |
Figure 4 Standard efficacy plots for intraocular lenses at postoperative month 3 for the non-dominant eyes. (A) Cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at far, (B) postoperative spherical equivalent prediction error distribution, (C) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at intermediate, (D) postoperative refractive cylinder distribution, and (E) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at near. |
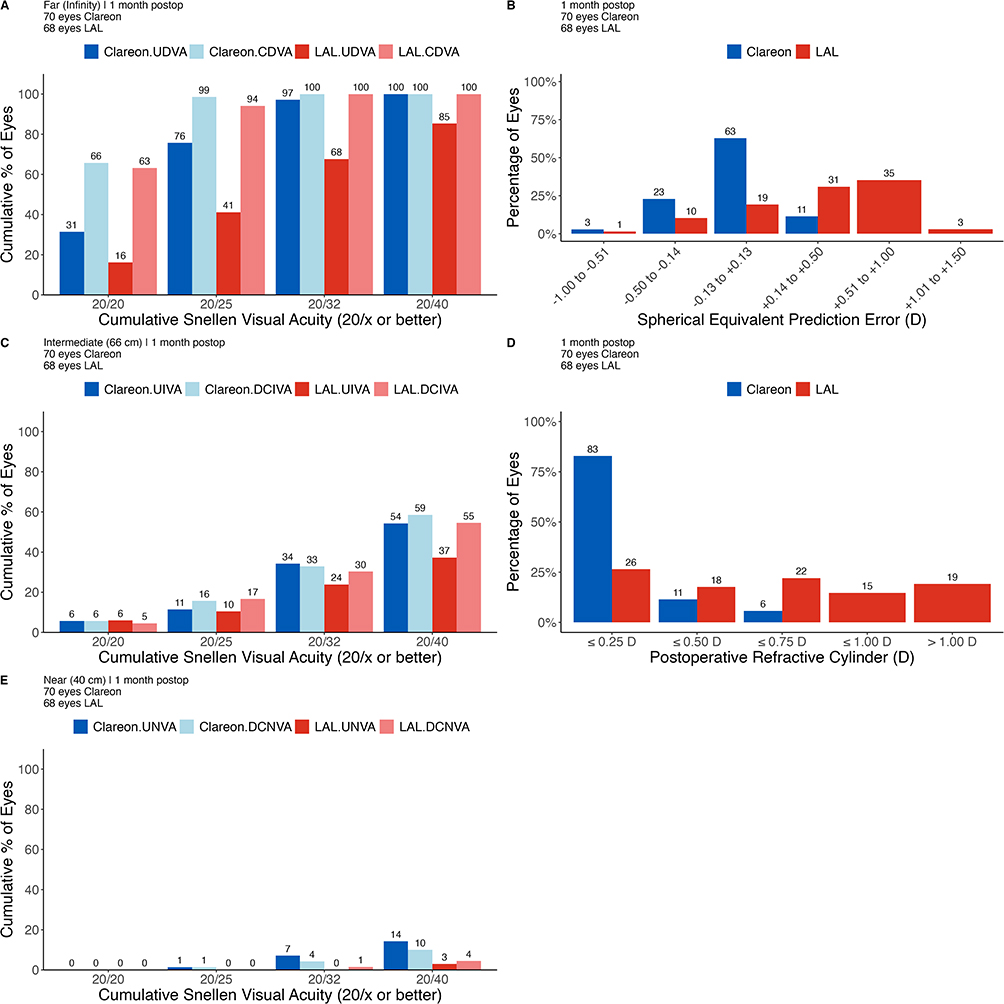 |
Figure 5 Standard efficacy plots for intraocular lenses at postoperative month 1 for the dominant eyes. (A) Cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at far, (B) postoperative spherical equivalent prediction error distribution, (C) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at intermediate, (D) postoperative refractive cylinder distribution, and (E) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at near. |
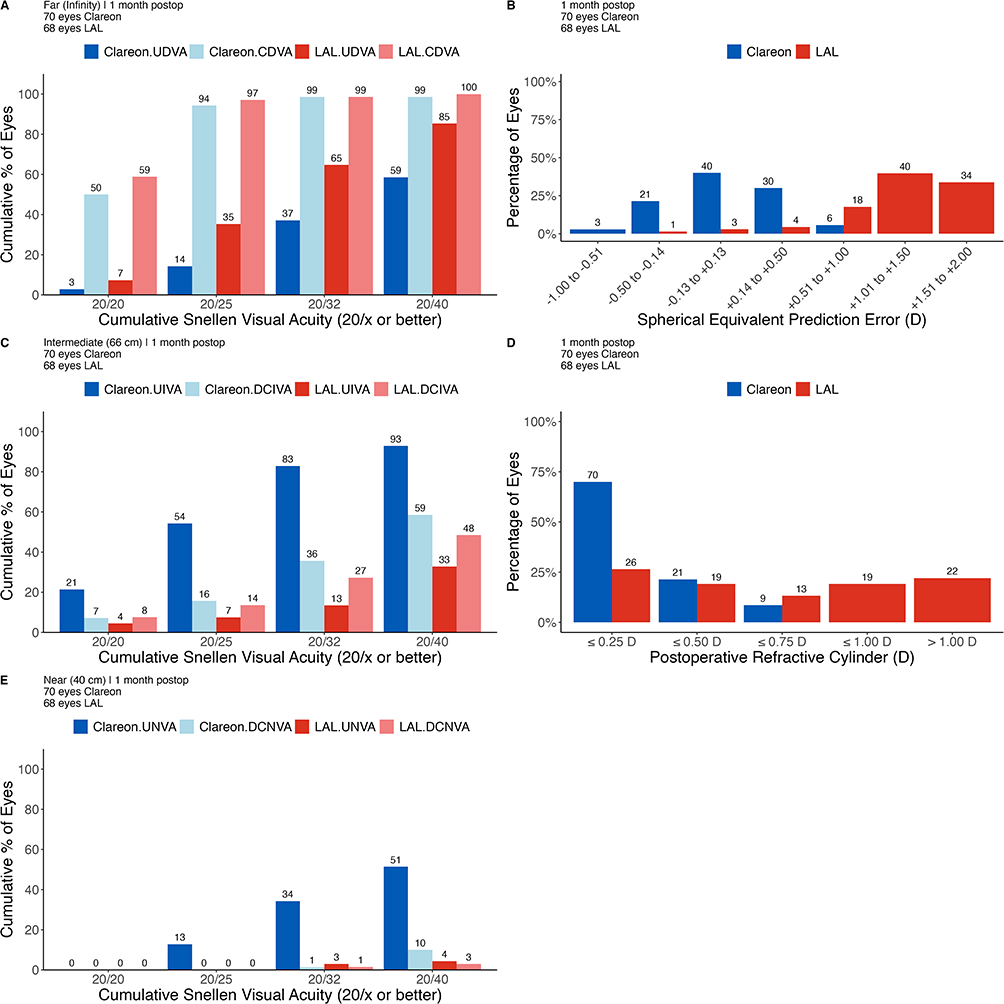 |
Figure 6 Standard efficacy plots for intraocular lenses at postoperative month 1 for the non-dominant eyes. (A) Cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at far, (B) postoperative spherical equivalent prediction error distribution, (C) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at intermediate, (D) postoperative refractive cylinder distribution, and (E) cumulative percentage of eyes achieving monocular uncorrected and distance corrected visual acuity at near. |
Visual Outcomes
Table 2 summarizes the 1 and 3 month postoperative binocular visual acuities in both groups. Postoperative month 3 binocular visual acuities in the Clareon group were confirmed non-inferior to the LAL group for all primary and secondary endpoints. However, the exploratory endpoint of UNVA could not be confirmed as non-inferior. In addition, binocular UNVA (p < 0.01) and DCIVA (p < 0.01) were significantly lower in the LAL group compared to the Clareon group with 3.5 - and 3 - letter difference, respectively. Inferential statistics at 1 month between groups are not a fair comparison as the LAL group would not have completed the UV treatments or lock-in at this time. Therefore, these calculations were not performed, nor were the differences between 1 and 3 months within groups compared. However, the data does appear to show binocular intermediate and near visual acuities improved in the LAL group between postoperative months 1 and 3 and were stable in the Clareon group. Monocular visual outcomes are summarized in Table 3.
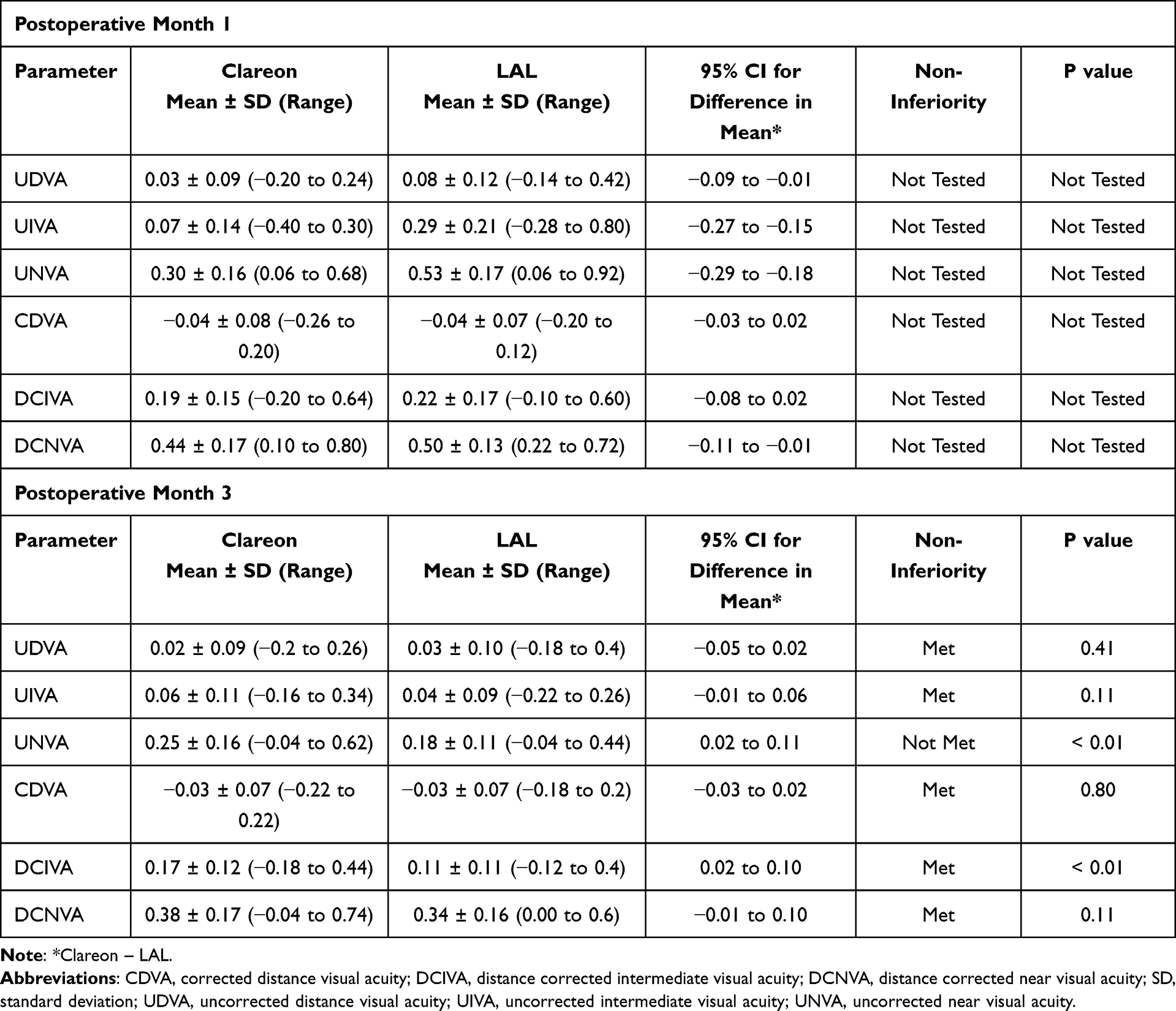 |
Table 2 Postoperative Binocular Visual Acuities |
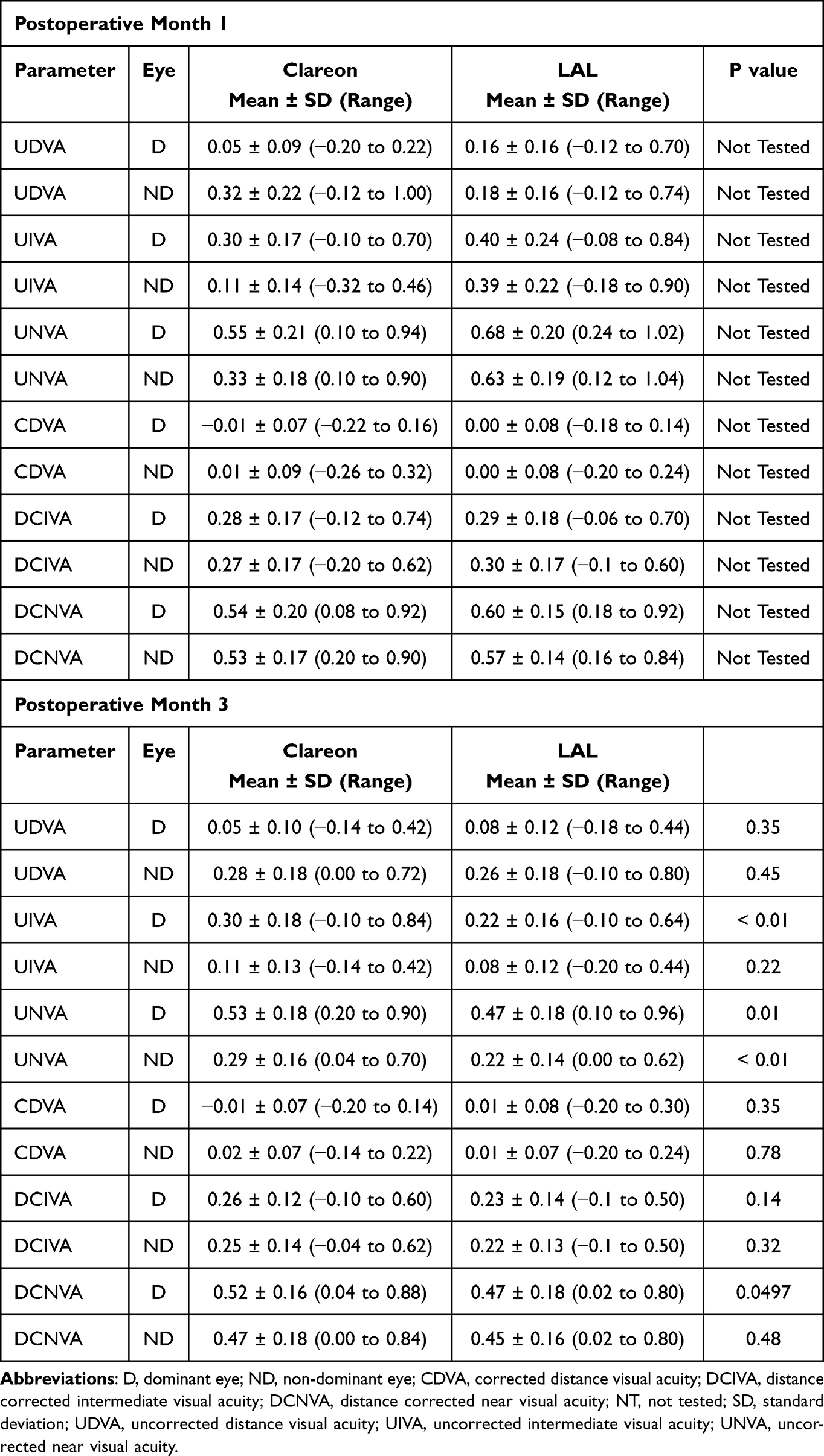 |
Table 3 Postoperative Monocular Visual Acuities |
Defocus Curves
Binocular target corrected defocus curves at 3 months postoperatively are summarized in Figure 7. Areas under the curve (AUCs) were similar between groups at far, intermediate, and total AUC. There was no significant difference between the groups for the binocular defocus curve when averaged across defocus levels (p = 0.34). However, there were significant group-by-defocus interactions, specifically at +0.50 D (p < 0.01) and +0.25 D (p < 0.01). Monocular defocus curves at 3 months postoperatively for the dominant eye in the Clareon group and the dominant and non-dominant eyes in the LAL group are also summarized in Figure 7. Note that a Clareon ND defocus curve was not collected as part of the study design. There was no significant overall difference between the groups for the monocular defocus curve averaged across defocus levels (p = 0.26). However, there were significant group-by-defocus interactions, specifically at +0.50 D (p < 0.01), +0.25 D (p = 0.01), and 0.00 D (p = 0.04) for Clareon dominant eyes and LAL dominant eyes, and at −1.50 D (p = 0.01), −2.00 D (p < 0.01), and −2.50 D (p = 0.01) for Clareon dominant eyes and LAL non-dominant eyes. In the dominant eyes, AUCs were similar between groups at far, intermediate, and total AUC between groups. However, the non-dominant eyes in the LAL group had a smaller area of functional visual acuity (indicated by the lower AUC) compared to the dominant eyes in both groups.
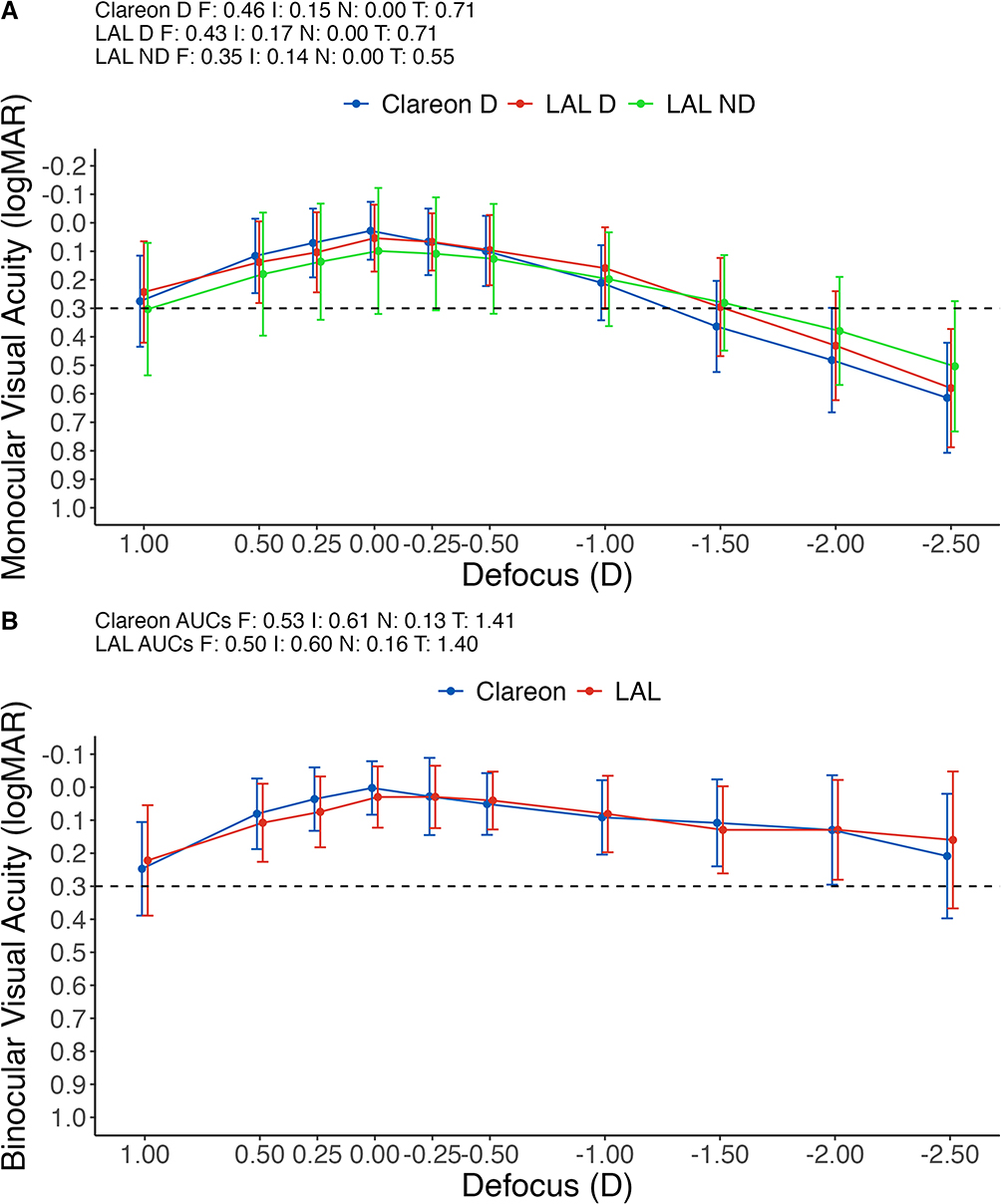 |
Figure 7 (A) Monocular and (B) Binocular defocus curve including areas under the curve for (F) far, (I) intermediate, (N) near, and (T) total, at 3 months postoperatively. Error bars represent the standard deviation. |
Refractive Error and Higher-Order Aberrations
Postoperative refractive outcomes are summarized in Table 4. Generally, refractive outcomes in the Clareon group were stable between postoperative month 1 and 3, while outcomes were significantly improved in the LAL group at postoperative month 3 compared to 1. Postoperative HOAs are summarized in Table 5. At 3 months postoperatively, total ocular HOA in the non-dominant eyes were significantly higher (p < 0.01) in the LAL group (0.449) compared to the Clareon group (0.306).
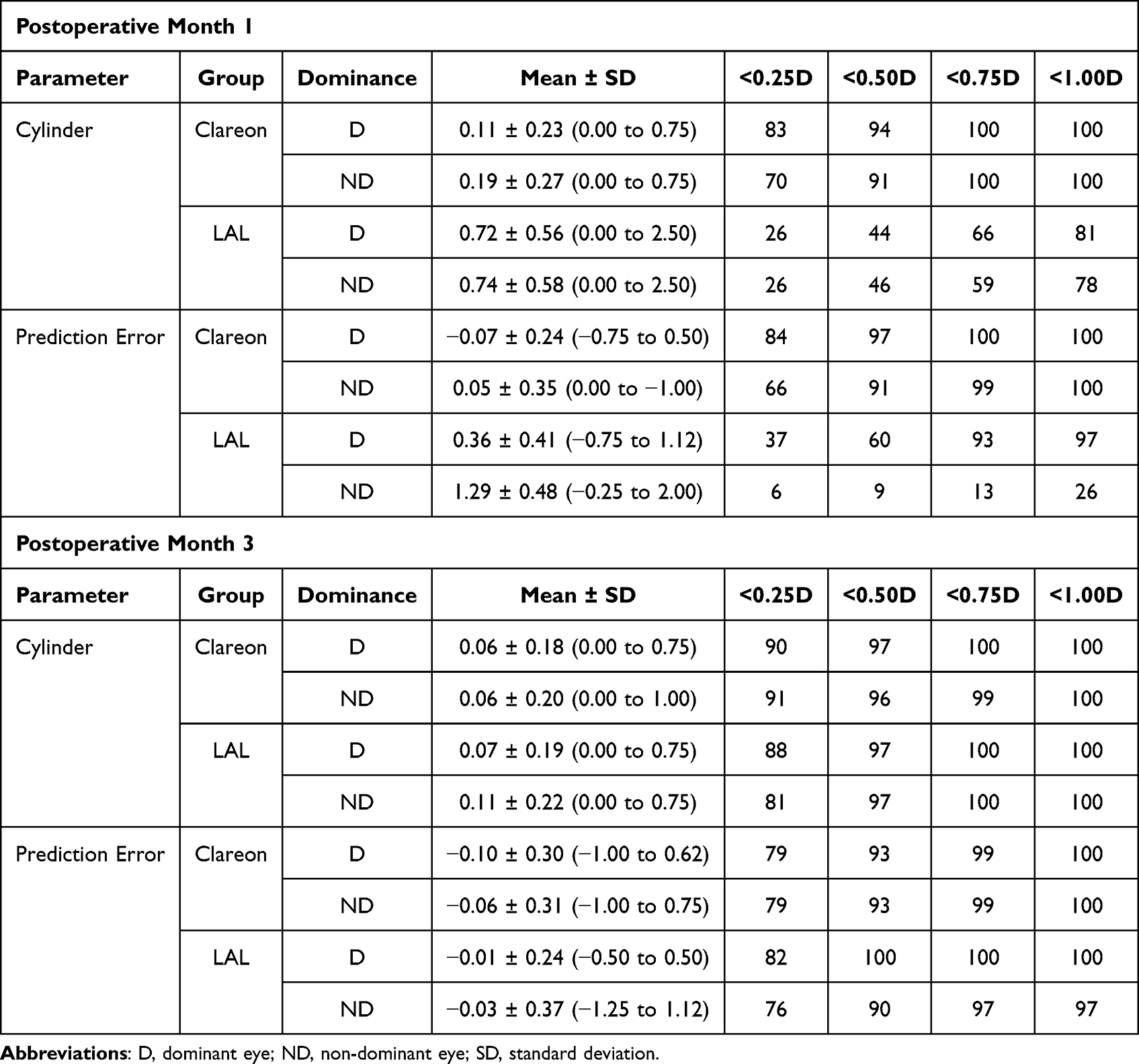 |
Table 4 Postoperative Refractive Outcomes |
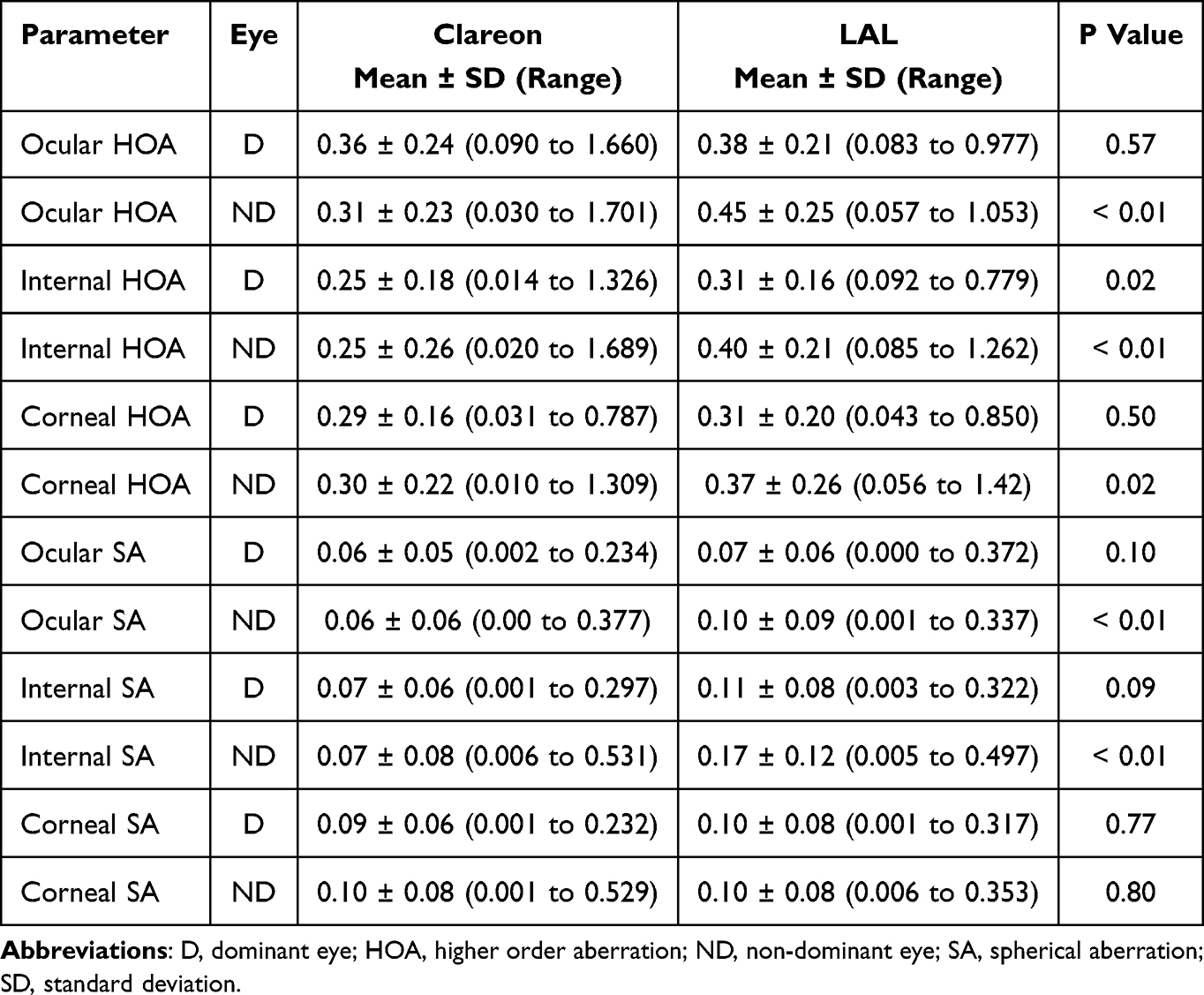 |
Table 5 Postoperative Month 3 Higher Order Aberrations |
Patient-Reported Outcomes and Number of Visits
Postoperative 1 and 3 month responses on the PRSIQ questionnaire are summarized in Tables 6 and 7, respectively. At 3 months postoperatively, spectacle independence (PRSIQ question 1) was reported for distance, intermediate, and near as 91% (64/70), 87% (61/70), and 33% (23/70) in the Clareon group, respectively, and 93% (63/68), 94% (64/68), and 43% (29/68) in the LAL group, respectively. These differences were not significant between groups for distance (p > 0.99), intermediate (p = 0.27), or near (p = 0.31). The percentage of subjects responding “None of the time” when asked about overall spectacle use in the last 7 days was 50% (34/68) in the LAL group compared to 39% (27/70) for the Clareon group. The mean number of postoperative days until routine release of care was 31.7 ± 13.0 (range 16 to 86) in the Clareon group and 53.9 ± 17.5 (range 35 to 112) in the LAL group (p < 0.001). The mean number of postoperative visits until routine release of care was 1.1 ± 0.3 (range 1 to 2) in the Clareon group and 4.2 ± 1.2 (range 3 to 10) in the LAL group (p < 0.01). However, this difference is expected due to the UV treatments required in the LAL group.
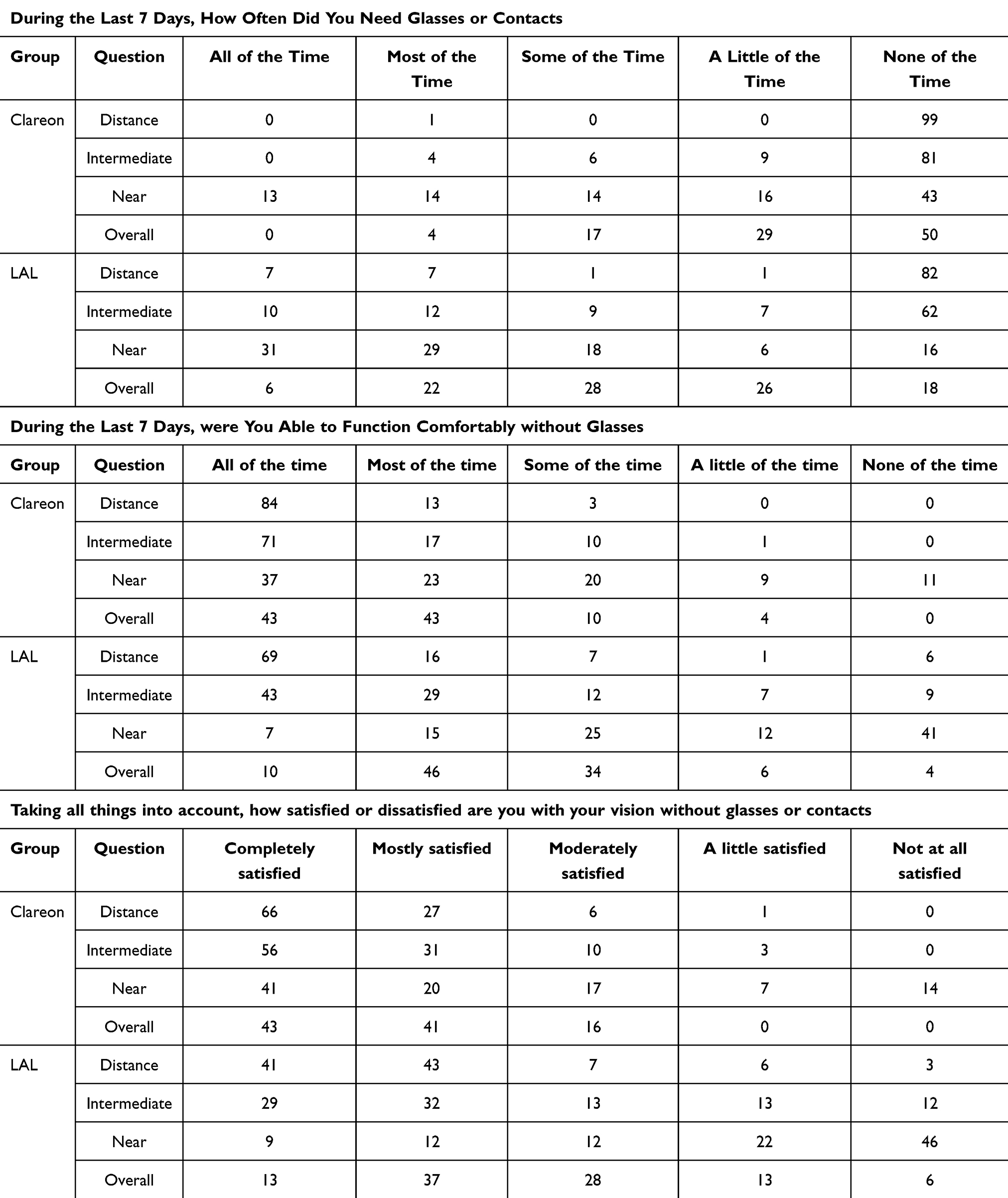 |
Table 6 Patient Reported Outcomes on the Patient-Reported Spectacle Independence Questionnaire (Percentages of Subjects) at 1 Months Postoperatively |
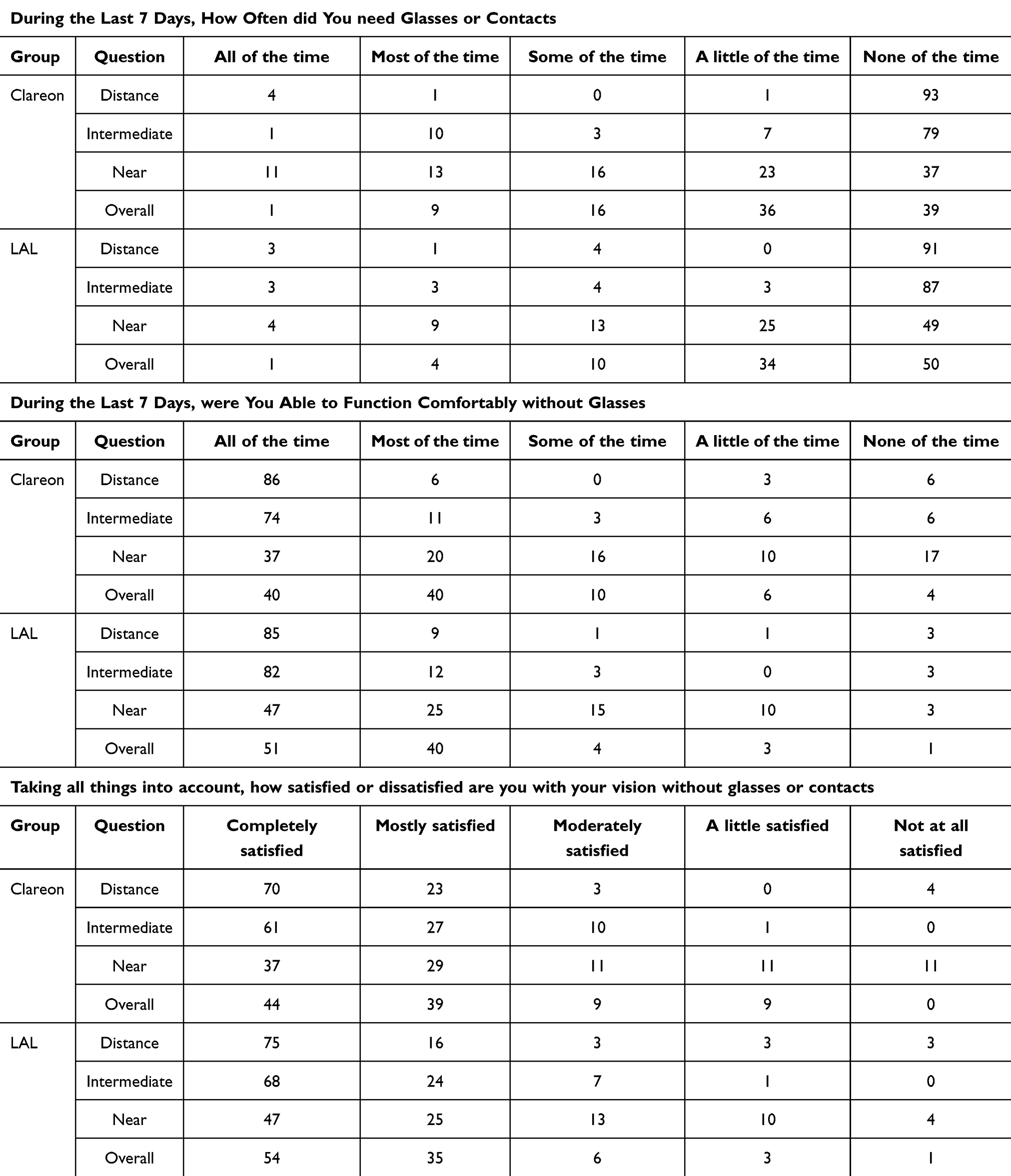 |
Table 7 Patient Reported Outcomes on the Patient-Reported Spectacle Independence Questionnaire (Percentages of Subjects) at 3 Months Postoperatively |
Discussion
Cataract surgery patients have a variety of options to choose from to reduce spectacle dependence. Mini-monovision can be a safe and effective choice to some extent, but outcomes may also be limited by refractive accuracy. The LAL can be adjusted after implantation to fine-tune the postoperative refraction. However, the increased out of pocket expenses and number of office visits to adjust the optics (compared to a monofocal IOL) are additional burdens on patients and clinical practices. In addition, patients receiving LAL treatment must also receive dilation drops at each visit and wear UV blocking eyewear until the final lock-in is completed, which would not be required for a standard monofocal implant. The question we wanted to answer in this study was whether the adjustability of the LAL will lead to superior postoperative outcomes compared to a standard monofocal IOL. We therefore compared postoperative visual acuities, spectacle independence, defocus curves between the LAL and the Clareon monofocal/toric IOL when both were targeted for mini-monovision. To the best of our knowledge, this is the first report of mini-monovision with the LAL compared to a fixed power monofocal/toric IOL.
Mean binocular uncorrected visual acuities for the LAL group were worse for intermediate and near at 1 month postoperatively compared to 3 months. This makes sense given that this was before any UV treatments and the mean MRSE at 1 month postoperatively for the LAL group was slightly hyperopic in both the dominant and non-dominant eyes. We note that this is in line with the manufacturer recommended starting refractive targets of +0.25 D. Other studies have reported similar outcomes for MRSE prior to UV treatments.16,18,22 In addition, there were approximately means of 0.72 D and 0.74 D of residual astigmatism in both the dominant and non-dominant eyes in the LAL group, respectively. The LAL is a spherical IOL that acquires astigmatism correction through UV treatment, which is not performed until at least 3–4 weeks after implantation. It is therefore critical that preoperative consultations set appropriate expectations with patients, especially those with high preoperative corneal astigmatism.
At 3 months postoperatively, mean UDVA and UIVA were similar between the LAL and Clareon groups, although there was a significant difference for UNVA (mean difference of 0.07 logMAR, 3.5 letters in favor of the LAL group). The clinical relevance of this difference is uncertain. Likewise for mean monocular UDVA, UIVA, and UNVA at 3 months postoperatively, there were no differences between groups greater than 0.10 logMAR. We suspect the differences in visual outcomes between the Clareon and LAL groups are due to slight differences in depth of focus, which is likely caused by the higher HOAs in the LAL group.23 Further studies would be beneficial to explore this relationship between HOA and depth of focus, specifically related to LAL. The binocular uncorrected outcomes for UDVA, UIVA, and UNVA for both the LAL and Clareon groups are similar to other reports of mini-monovision using standard monofocal IOLs.24–26 Disparities between our results and those from other reports may be due to differences on refractive targets in the dominant and non-dominant eyes between studies.27 Overall, the results of our study suggest good distance vision and functional intermediate vision with the Clareon monofocal IOL and the LAL when both target mini-monovision (−1.00 D).
The uncorrected visual acuities in both the Clareon and LAL groups translated into high patient-reported spectacle independence at distance and intermediate, but comparatively lower independence at near. Christenbury and Hall28 previously reported high spectacle independence with the Clareon monofocal at distance and intermediate. We are not aware of any reports of spectacle independence at distance, intermediate, and near for the LAL. Spectacle independence was not significantly different between the Clareon and LAL groups, although a higher percentage of subjects reported using spectacles “None of the time” overall in the LAL group (50%) compared to the Clareon group (39%). This difference can be interpreted as a trend, and not necessarily evidence of a clinically meaningful difference. The patient reported outcomes in both the Clareon and LAL groups were similar to the patient reported outcomes in other studies of mini-monovision for distance and intermediate vision, but appear lower for near vision.10,27 Differences between other published reports and our study may be due to differences in the questionnaires used to assess spectacle independence.
There were a greater number of adverse events in the LAL group compared to the Clareon group. Both groups had the same number of YAG laser capsulotomies. However, the LAL group had 2 reports of ocular HSV compared to 0 in the Clareon group. We note that patients with a history of ocular HSV are contraindicated for LAL and LDD treatment as the UV light may cause reactivation. Dry eye symptoms were also higher in the LAL group (7) compared to the Clareon group (2). One possible explanation is that the increased number of visits may have created more opportunities for patients to report adverse events.
The LAL is a premium cost IOL. However, patients may wonder if they will achieve better outcomes that justify the increased costs. In our study of mini-monovision, the mean binocular uncorrected visual acuities at 3 months postoperatively of the standard monofocal (Clareon) were non-inferior to that of the LAL, using a margin of 0.10 logMAR for clinical significance. In addition, the binocular defocus curves and AUCs were similar. We note that our results should be interpreted with caution as the total defocus range was +1.00 D to −2.50 D, compared to the suggested range of +1.00 D to −4.00 D.21 From a clinical practice perspective, there are also additional burdens of technician time and the administration of LDD therapy by a qualified provider across multiple patient visits. With the results of our study and the costs (both in time and money) associated with each treatment in mind, surgeons and patients can decide if the results are worth the costs. We would also note that intraoperative aberrometry was used in our study, which has been reported to improve refractive predictability;29,30 however, its use may confound interpretation of the relative cost-effectiveness of one IOL compared to the other.
The measured pupil sizes in our study appear larger than those observed in other clinical trials. This is likely due to inter-device variability in measured pupil diameter. A study by Fernández et al31 compared the mesopic and photopic pupil diameters obtained with two commonly used diagnostic devices in eyes with multifocal IOLs. The authors observed significant differences, highlighting that pupil size measurements should be interpreted based on illumination, device, and testing distance.
The primary limitation of this study was the relatively short follow up period. Using a 3 month follow up limits, conclusions to be drawn about the long term effectiveness of visual performance, refractive outcomes, and spectacle independence between the Clareon monofocal IOL and the LAL. In particular, the long term stability of the LAL is unknown. Therefore, longer follow up may be needed to assess whether outcomes are maintained. In addition, there was no masking of patients—or examiners—since the LAL group received UV treatment and the Clareon group did not. This may have influenced the subjective patient-reported outcomes, such as spectacle independence and satisfaction. Visual outcomes may have also been affected as unmasked examiners could unintentionally bias testing through differences in encouragement or refraction. Finally, as the LAL and LDD are relatively new technologies, we cannot exclude the influence of a learning-curve effect on outcomes. Different clinicians may have preferred adjustment timings, magnitudes, or techniques, which may limit the generalizability of our findings.
Conclusions
The results of this study suggest similarly good refractive and visual outcomes for both Clareon monofocal/toric and LAL IOLs when both are targeting same mini-monovision. The Clareon group was able to achieve stable refractive and good visual outcomes sooner after surgery. The LAL group had greater depth of field.
Data Sharing Statement
Data are not available for sharing.
Acknowledgment
This paper was presented at the 2025 American Society of Cataract and Refractive Surgery (ASCRS) Annual Meeting as a conference paper.
Funding
This study was supported with an investigator-initiated study grant (89850521) from Alcon Vision, LLC, Fort Worth, TX, USA.
Disclosure
BH reports independent contractor fees from Topcon Healthcare Inc. The authors have no other financial or proprietary interest in any material or method mentioned in this work.
References
1. Blehm C, Hall B. Evaluation of visual outcomes and 3-month refractive stability of a new hydrophobic acrylic intraocular lens. Clin Ophthalmol. 2023;17:1859–19. doi:10.2147/OPTH.S415400
2. Werner L, Thatthamla I, Ong M, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45:1490–1497. doi:10.1016/j.jcrs.2019.05.017
3. Nuijts R, Bhatt U, Nanavaty MA, Roberts TV, Peterson R, Teus MA. Three-year multinational clinical study on an aspheric hydrophobic acrylic intraocular lens. J Cataract Refract Surg. 2023;49:672–678. doi:10.1097/j.jcrs.0000000000001173
4. Micheletti JM, Duncan NB, Hall B. Head-to-head comparison of intermediate vision of two monofocal intraocular lenses. Clin Ophthalmol. 2023;17:3983–3990. doi:10.2147/OPTH.S444696
5. Schallhorn JM. Multifocal and extended depth of focus intraocular lenses: a comparison of data from the United States food and drug administration premarket approval trials. J Refract Surg. 2021;37:98–104. doi:10.3928/1081597X-20201111-02
6. Hovanesian JA, Jones M, Allen Q. The PanOptix trifocal IOL vs the ReSTOR 2.5 active focus and ReSTOR 3.0-add multifocal lenses: a study of patient satisfaction, visual disturbances, and uncorrected visual performance. Clin Ophthalmol. 2021;15:983–990. doi:10.2147/OPTH.S285628
7. Cao K, Friedman DS, Jin S, et al. Multifocal versus monofocal intraocular lenses for age-related cataract patients: a system review and meta-analysis based on randomized controlled trials. Surv Ophthalmol. 2019;64:647–658. doi:10.1016/j.survophthal.2019.02.012
8. Pedrotti E, Carones F, Talli P, et al. Comparative analysis of objective and subjective outcomes of two different intraocular lenses: trifocal and extended range of vision. BMJ Open Ophthalmol. 2020;5:e000497. doi:10.1136/bmjophth-2020-000497
9. Auffarth GU, Gerl M, Tsai L, et al. Clinical evaluation of a new monofocal IOL with enhanced intermediate function in patients with cataract. J Cataract Refract Surg. 2021;47:184–191. doi:10.1097/j.jcrs.0000000000000399
10. Goldberg DG, Goldberg MH, Shah R, Meagher JN, Ailani H. Pseudophakic mini-monovision: high patient satisfaction, reduced spectacle dependence, and low cost. BMC Ophthalmol. 2018;18:293. doi:10.1186/s12886-018-0963-3
11. Newsom TH, Potvin R. Evaluation of quality of vision and visual outcomes with bilateral implantation of a non-diffractive extended vision intraocular lens with a target of slight myopia in the non-dominant eye. Clin Ophthalmol. 2022;16:183–190. doi:10.2147/OPTH.S350850
12. Beltraminelli T, Rizzato A, Toniolo K, Galli A, Menghini M. Comparison of visual performances of enhanced monofocal versus standard monofocal IOLs in a mini-monovision approach. BMC Ophthalmol. 2023;23:170. doi:10.1186/s12886-023-02920-6
13. Labiris G, Toli A, Perente A, Ntonti P, Kozobolis VP. A systematic review of pseudophakic monovision for presbyopia correction. Int J Ophthalmol. 2017;10:992–1000. doi:10.18240/ijo.2017.06.24
14. Ford J, Werner L, Mamalis N. Adjustable intraocular lens power technology. J Cataract Refract Surg. 2014;40:1205–1223. doi:10.1016/j.jcrs.2014.05.005
15. Nishihara TW, Hu JQ, Buchholz RD, Murphy JD, Afshari NA. Cost-effectiveness analysis of light adjustable lens compared to monofocal intraocular lens in cataract surgery. J Refract Surg. 2023;39:777–782. doi:10.3928/1081597X-20231016-01
16. Jones M, Terveen DC, Berdahl JP, Thompson V, Kramer BA, Ferguson TJ. Clinical outcomes of the light-adjustable lens in eyes with a history of prior corneal refractive surgery. J Cataract Refract Surg. 2024;50:936–941. doi:10.1097/j.jcrs.0000000000001481
17. Kozhaya K, Wang L, Weikert MP, Koch DD. Early outcomes of second-generation light-adjustable lenses in eyes with and without corneal refractive surgery. J Cataract Refract Surg. 2023;49:1180–1182. doi:10.1097/j.jcrs.0000000000001282
18. Wong JR, Folden DV, Wandling GR, et al. Visual outcomes of a second-generation, enhanced UV protected light adjustable lens in cataract patients with previous LASIK and/or PRK. Clin Ophthalmol. 2023;17:3379–338719. doi:10.2147/OPTH.S432457
19. Jun JH, Lieu A, Afshari NA. Light adjustable intraocular lenses in cataract surgery: considerations. Curr Opin Ophthalmol. 2024;35:44–49. doi:10.1097/ICU.0000000000001015
20. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022;48:1297–1304. doi:10.1097/j.jcrs.0000000000000978
21. Fernandez J, Ribeiro FJ, Rodriguez-Vallejo M, et al. Standard for collecting and reporting outcomes of IOL-based refractive surgery: update for enhanced monofocal, EDOF, and multifocal IOLs. J Cataract Refract Surg. 2022;48:1235–1241. doi:10.1097/j.jcrs.0000000000001013
22. Moshirfar M, Wagner WD, Linn SH, et al. Astigmatic correction with implantation of a light adjustable vs monofocal lens: a single site analysis of a randomized controlled trial. Int J Ophthalmol. 2019;12:1101–1107. doi:10.18240/ijo.2019.07.08
23. Fernandez J, Rodriguez-Vallejo M, Burguera N, Rocha-de-Lossada C, Pinero DP. Spherical aberration for expanding depth of focus. J Cataract Refract Surg. 2021;47:1587–159523. doi:10.1097/j.jcrs.0000000000000713
24. Abdelrazek Hafez T, Helaly HA. Spectacle independence and patient satisfaction with pseudophakic mini-monovision using aberration-free intraocular lens. Clin Ophthalmol. 2019;13:2111–2117. doi:10.2147/OPTH.S215229
25. Beiko GHH. Comparison of visual results with accommodating intraocular lenses versus mini-monovision with a monofocal intraocular lens. J Cataract Refract Surg. 2013;39:48–55. doi:10.1016/j.jcrs.2012.08.059
26. Dell SJ, Hannan SJ, Venter JA, et al. Comparative analysis of clinical and patient-reported outcomes of a new enhanced monofocal IOL and a conventional monofocal IOL. Clin Ophthalmol. 2024;18:1157–1169. doi:10.2147/OPTH.S456332
27. Wrobel-Dudzinska D, Moura-Coelho N, Palma-Carvajal F, Zebdeh A, Manero F, Guell JL. Ten-year outcomes of pseudophakic mini-monovision correction of hyperopic presbyopia. J Cataract Refract Surg. 2023;49:367–372. doi:10.1097/j.jcrs.0000000000001116
28. Christenbury J, Hall B. Visual outcomes and patient satisfaction with a hydrophobic acrylic monofocal IOL delivered using a manual system. Clin Ophthalmol. 2024;18:3485–3491. doi:10.2147/OPTH.S491589
29. Cionni RJ, Dimalanta R, Breen M, Hamilton C. A large retrospective database analysis comparing outcomes of intraoperative aberrometry with conventional preoperative planning. J Cataract Refract Surg. 2018;44:1230–1235. doi:10.1016/j.jcrs.2018.07.016
30. Cionni RJ, Breen M, Hamilton C, Williams R. Retrospective analysis of an intraoperative aberrometry database: a study investigating absolute prediction in eyes implanted with low cylinder power toric intraocular lenses. Clin Ophthalmol. 2019;13:1485–1492. doi:10.2147/OPTH.S191887
31. Fernández J, Burguera N, Rocha-de-Lossada C, Rodríguez-Calvo-de-Mora M, Rodríguez-Vallejo M. Agreement between two devices for measuring pupil diameter in patients implanted with multifocal intraocular lenses. Vision. 2023;7:40. doi:10.3390/vision7020040
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Head-to-Head Comparison of Intermediate Vision of Two Monofocal Intraocular Lenses
Micheletti JM, Duncan NB, Hall B
Clinical Ophthalmology 2023, 17:3983-3990
Published Date: 21 December 2023