Back to Journals » Medical Devices: Evidence and Research » Volume 19
Prospective Multicenter Evaluation of Patient Satisfaction and Radiologist Image Interpretation Using the Envision™ Mammography Platform
Authors Parghi CR, Niklewski PJ, Cooper A, Waqas M
Received 5 September 2025
Accepted for publication 11 February 2026
Published 21 March 2026 Volume 2026:19 560551
DOI https://doi.org/10.2147/MDER.S560551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mohamad Bashir
Chirag R Parghi,1,2,* Paul J Niklewski,3,* Alexis Cooper,3,* Muhammad Waqas3,*
1Department of Radiology, HCA Houston Healthcare Kingwood, Spring, TX, USA; 2Solis Mammography, Addison, TX, USA; 3Global Clinical Affairs, Hologic Inc., Marlborough, MA, USA
*These authors contributed equally to this work
Correspondence: Alexis Cooper, Global Clinical Affairs, Hologic Inc., 250 Campus Dr, Marlborough, MA, 01752, USA, Email [email protected]
Purpose: Improving image quality without increasing patient discomfort remains a challenge in mammography. This study evaluated the ability of the Envision™ platform in a prospective, multicenter observational case-collection study (NCT05199701), focusing on patient comfort and radiologist-assessed image quality.
Patients and Methods: Across nine US breast-imaging sites, 929 women aged ≥ 35 years undergoing a clinically indicated screening or diagnostic mammogram, or a mammogram in the context of a recommended biopsy, were enrolled. All subjects received a standard four-view bilateral exam (RCC, RMLO, LCC, LMLO) on the Envision platform. Radiologists rated image quality (positioning, contrast, sharpness, tissue visibility, noise, artifacts, and overall clinical image quality) using a three-category scale (requires reimaging, acceptable, excellent). Patient comfort and device preference were assessed via questionnaire. Analyses were descriptive.
Results: Most subjects (79%) preferred the investigational mammogram over prior mammograms, and 70% reported greater compression comfort. Discomfort scores were low: 34% reported no discomfort (0/10) and 52.5% reported minimal discomfort (1– 2/10). Radiologists rated the majority of images acceptable or excellent, with excellent ratings of 41.9– 48.5% for contrast, 41.8– 42.0% for sharpness, 50.2– 50.5% for tissue visibility, and 33.4– 34.5% for artifacts. Repeat-imaging recommendations were infrequent (0– 6.6% across views), and overall clinical image quality was acceptable or excellent in 94.1– 100% of images.
Conclusion: The Envision platform produced consistently high levels of clinically acceptable image quality while maintaining or improving patient comfort compared to prior mammography experiences. These findings support its feasibility for routine clinical use.
Keywords: mammography, screening, imaging, image quality, comfort
Introduction
Breast cancer remains the most commonly diagnosed cancer among women worldwide and the second-leading cause of cancer-related mortality, with recent 2022 GLOBOCAN estimates reporting 2.3 million new cases annually.1 Early detection through screening mammography reduces disease-specific mortality, particularly in women aged 40 and older.2 Current appropriate-use criteria recommend mammography for routine screening, diagnostic evaluation of symptoms, and assessment of imaging findings that warrant further characterization.
Despite its established benefits, conventional mammography can be limited by patient discomfort due to breast compression and by variability in image quality, both of which may influence screening compliance, diagnostic accuracy, and the need for repeat imaging.3 As technology evolves, newer mammography systems aim to improve diagnostic accuracy and improve patient comfort, as both parameters will affect the ultimate adoption. Moreover, innovations in image acquisition geometry and image quality, such as three-dimensional (3D) imaging, have been introduced to improve diagnostic outcomes.4
The Envision™ mammography platform incorporates several design features intended to improve both patient experience and image acquisition, including adjustable positioning geometry and enhanced in-plane sharpness technologies. Whether these design changes translate into more favorable patient-reported outcomes and radiologist-assessed image quality in routine clinical settings requires empirical evaluation.5
This prospective multicenter observational case-collection study was conducted to assess patient comfort and radiologist scoring of image quality across standard bilateral mammographic views using the Envision platform. The purpose of this preliminary analysis is to describe early clinical performance across participating sites and characterize both patient- and image-level outcomes.
Materials and Methods
Envision Platform
The Envision platform (Figure 1) is a mammography platform that generates conventional two-dimensional (2D) FFDM images, synthesized 2D images (a 2D mammography image from a 3D data set created from the stack of tomosynthesis reconstructed slices to a single synthesized 2D image), and tomosynthesis three-dimensional (3D) mammography image sets of the breast in the two conventional views (Craniocaudal and Mediolateral oblique) for screening and diagnostic purposes.
 |
Figure 1 The Hologic Envision™ mammography platform used in the multicenter case-collection study. The system incorporates adjustable positioning geometry and enhanced sharpness technology designed to support patient comfort and image quality during routine bilateral mammographic imaging. |
The Envision platform was designed to offer improved image quality while incorporating features to improve patient comfort, such as Tilt Positioning. Tilt was performed at a maximum angle on a subset of the patients. In the Envision platform’s design, patient comfort design elements must not come at the expense of image quality. Radiologists are critical in evaluating whether these devices can maintain or improve diagnostic accuracy, particularly in routine breast cancer screening. This study evaluates early feedback from radiologists who reviewed the images acquired using the Envision platform.
Study Design
This was a prospective, multicenter case collection study (NCT05199701) designed to evaluate the safety, efficacy, and clinical utility of the Envision mammography platform. The Envision platform incorporates innovative features such as Focusing Technology, Tilt Positioning, reduced scan time and 15-language audio prompts. The study aimed to assess key parameters, including patient satisfaction and radiologist interpretation of image quality.
The study was conducted at 9 clinical sites across the United States. Enrollment commenced in December 2021 and involved subjects undergoing routine screening or diagnostic mammograms. This is a preliminary analysis of 929 subjects aged 35 and older. Imaging was performed using the Envision platform in a standard four-view bilateral protocol (right craniocaudal (RCC), left craniocaudal (LCC), right mediolateral oblique (RMLO), and left mediolateral oblique (LMLO)).
Ethics Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. Prior to initiation, the study protocol and informed consent documents were reviewed and approved by the appropriate Institutional Review Boards/Ethics Committees at each participating site (WCG IRB ID #:20214242). All participants provided written informed consent prior to study procedures.
Study Population
The study population consisted of women aged 35 years and older who were recommended for screening or diagnostic mammograms. Key inclusion criteria included:
- Female subjects of any race or ethnicity.
- Subjects who were clinically indicated for screening or diagnostic mammograms or breast biopsies.
The exclusion criteria were as follows:
- Pregnant subjects or those who believed they might be pregnant.
- Subjects with breast implants, cardiac pacemakers, nipple piercings, or intravenous (IV) ports in the mammography field of view.
Study Population and Data Collection
Demographic, clinical, and imaging-related data were collected in electronic case report forms (eCRFs) using a secure, 21 CFR Part 11–compliant electronic data capture (EDC) system (Zelta). Collected variables included age, height, weight, body habitus, race and ethnicity, breast symptoms, personal and family history of breast cancer, and the clinical indication for the mammogram (screening, diagnostic evaluation, or recommended biopsy). Procedural variables included view (RCC, RMLO, LCC, LMLO), imaging mode, and date of exam.
Imaging Protocol
Each subject underwent a four-view bilateral mammogram using the Envision platform. Tilt positioning was used for a subcohort of patients at the maximum angle with the flat paddle. The standard imaging protocol included craniocaudal (CC) and mediolateral oblique (MLO) views for both breasts. Based on clinical requirements, the technologist selected the appropriate imaging mode for each subject, including full-field digital mammography (FFDM) or 3D tomosynthesis. All imaging was performed using the “Auto Filter” mode with automatic exposure control (AEC) to ensure optimal image quality and minimize radiation dose.
Patient Satisfaction
After their exam, subjects were asked to complete a feedback questionnaire assessing their experience with the investigational Envision platform. This feedback included ratings of breast compression comfort, ease of positioning, and overall experience compared to prior mammograms. Specific questions included:
- Discomfort Level: Rated on a 0–10 scale.
- Preference: Subjects were asked whether they preferred the investigational mammogram to previous experiences.
- Positioning Comfort: Subjects were asked whether the breast positioning was more comfortable with the investigational Envision platform compared to previous experiences, including in the subset that used the Tilt Positioning feature.
Radiologist Feedback
Radiologists reviewed the image cases, evaluating them for image quality using the following criteria:
- Positioning and Tissue Coverage: Ensuring the images captured sufficient tissue, particularly near the chest wall.
- Image Contrast: The ability to distinguish between different types of tissue (eg, fatty vs dense tissue) and abnormalities such as masses or microcalcifications.
- Sharpness: The clarity of anatomical structures, especially small details such as microcalcifications.
- Artifacts and Noise: The presence of image distortions or graininess that could interfere with diagnostic interpretation.
Radiologists rated each image as excellent (would consider sending to the American College of Radiology (ACR)), acceptable (may not be perfect yet does not inhibit interpretation), or requires reimaging for these categories. The primary endpoint was determination of the percentage of images rated as clinically acceptable or better for diagnostic purposes.
Radiologist Variability Analysis
In this case-collection design, each participating site had a single breast-imaging radiologist who reviewed all investigational images for that site. Images were not independently interpreted by multiple readers; therefore, formal inter-reader reliability metrics (eg, Cohen’s kappa or ICC) could not be calculated. To characterize variability in image-quality assessment within the constraints of the design, radiologist ratings at the level of site, view, and image-quality parameter (RCC, RMLO, LCC, LMLO; positioning/tissue coverage, contrast, sharpness, tissue visibility, noise, artifacts, and overall clinical image quality) were summarized. For each site/view/parameter combination, the percentage of images rated as requires reimaging, acceptable, or excellent was calculated. Between-site variability using the distribution (minimum, maximum, median, and interquartile range) of the proportion of images rated excellent, and the combined proportion rated acceptable or excellent for each parameter was described.
Data Collection and Analysis
All analyses were descriptive. Continuous variables (eg, age) were summarized using means, standard deviations, and ranges. Categorical variables—patient comfort responses and radiologist image-quality ratings—were summarized using counts and percentages. Site-level variability in radiologist ratings was summarized using the distribution (minimum, maximum, mean, and median) of the proportion of images rated excellent and acceptable or excellent for each parameter and view. Statistical analyses were performed using R (version 4.4.1). Data were managed and exported using the study’s EDC system.
Results
This multicenter, prospective study (NCT05199701) enrolled 929 female subjects (≥35 years) undergoing a mammogram across 9 US clinical sites. The mean age was 56.62 years (SD ± 10.58), ranging from 35 to 88 years. The mean height was 64.85 inches (SD ± 7.79), ranging from 46.0 to 73.0 inches, and the mean weight was 170.67 pounds (SD ± 37.73), ranging from 77.6 to 310.0 pounds. The racial distribution of the population was predominantly White (83.9%), with smaller proportions of Black (8.6%), Asian (0.5%), Native American (0.3%), Pacific Islander (0.1%), and 6.6% of the population being of unknown race. Regarding body habitus, the majority of subjects were classified as endomorphic (44.6%), with 27.6% classified as mesomorphic and 27.7% as ectomorphic. Only 0.2% were unspecified.
Most subjects (86.5%) were undergoing routine screening mammograms, while 10.8% were recommended for a biopsy, and 2.7% were undergoing diagnostic evaluations. Most of the subjects (96.8%) did not present breast cancer symptoms. Specific symptoms included palpable masses in 1.4% of subjects, nipple discharge in 0.1%, and discomfort in 0.3%. Notably, no subjects showed changes in nipple texture or shape.
A small percentage (6.7%) of subjects had a history of breast cancer, while nearly half (46.0%) had a family history of breast cancer.
All the results described above are summarized in Table 1.
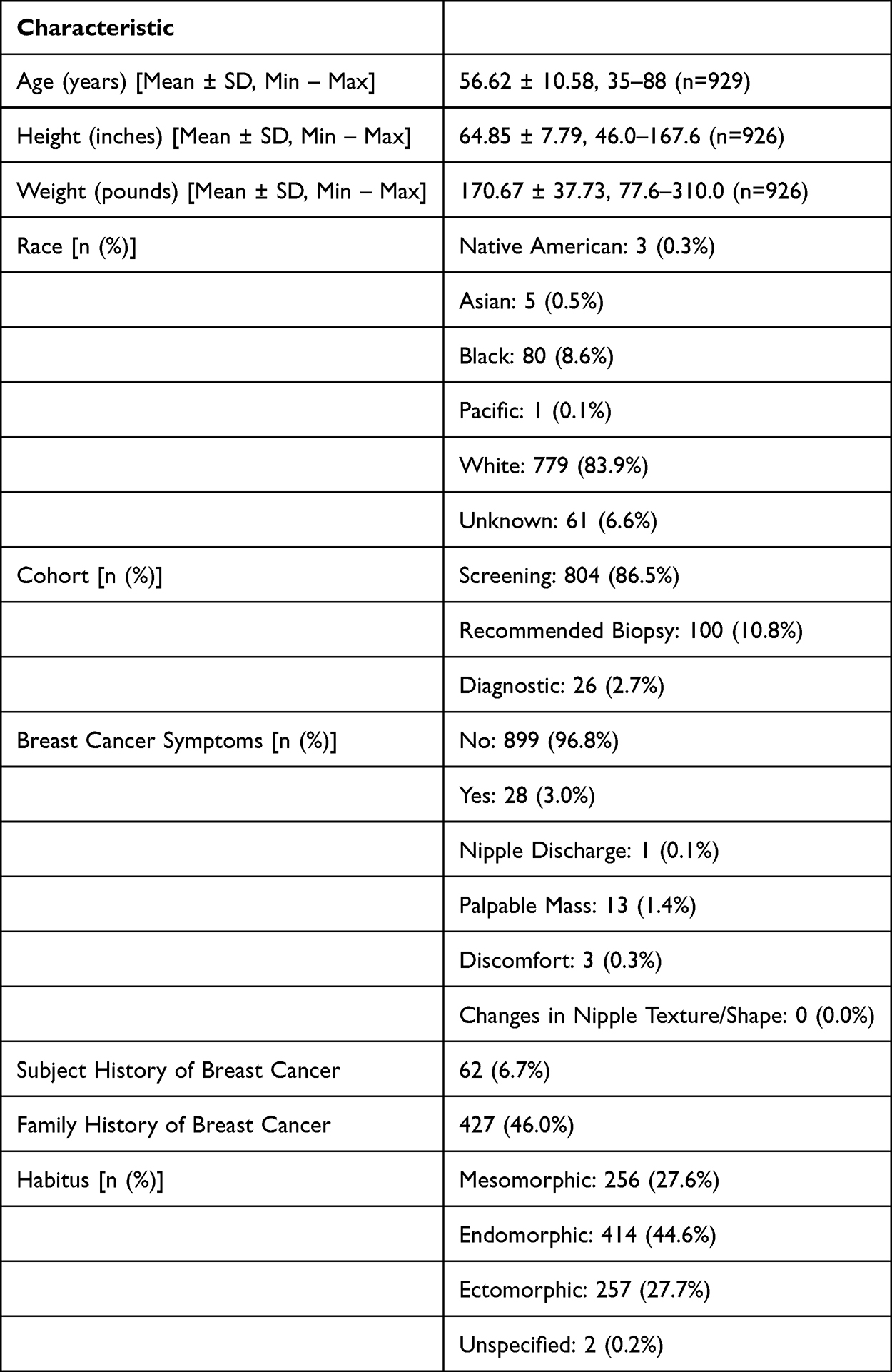 |
Table 1 Demographics |
Patient Feedback
Patient feedback on comfort during the investigational mammogram, compared to their prior experiences, is presented in Figure 2 and Table 2. Overall, the majority of subjects reported low levels of discomfort during their investigational mammogram. As shown in Figure 2, 316 (34.0%) of subjects reported no discomfort (rating of 0), and 488 (52.5%) reported minimal discomfort (ratings of 1–2). Moderate discomfort (ratings of 3–4) was reported by 91 subjects (9.8%). Less than 29 (5.5%) of subjects rated their discomfort at a level of 5 or higher. Overall 804 subjects (86.5%) experienced no or minimal discomfort during the investigational mammogram.
 |
Table 2 Subject Comfort with the Investigational Device Compared to Prior Mammogram |
 |
Figure 2 Distribution of subject-reported discomfort during the investigational mammogram. Discomfort was rated on a 0–10 scale, where 0 indicates no discomfort and 10 indicates the highest level of discomfort imaginable. Most subjects reported low discomfort, with 34.0% rating 0, 21.5% rating 1, and 31.0% rating 2. Moderate discomfort (scores 3–4) was reported by 9.8% of subjects, and high discomfort (scores ≥5) by 3.1% of subjects. |
When comparing the investigational mammogram to their previous experiences, the majority of subjects found the investigational mammogram to be equally or more comfortable. As shown in Table 2, 37.4% of subjects rated the investigational mammogram as equally comfortable as their previous mammograms, while 33.4% found it slightly more comfortable, and 17.8% reported it to be much more comfortable. Only 10.8% of subjects found the investigational mammogram to be less comfortable than their previous experience.
Overall, 79% of subjects preferred the investigational mammogram over their prior mammograms, while only 16% preferred the prior mammogram. When tilt was used (79 patients), 86% of patients reported they were equally or more comfortable having their mammogram with the Envision platform than their prior mammogram experience. These results show that most subjects preferred the investigational mammogram, particularly in terms of overall comfort and breast compression, where 70% of women report that compression is equally or more comfortable on the Envision platform compared to their prior mammogram. Some reported areas for potential improvement were in positioning and communication with the technologist. However, this is potentially confounded due to early system utilization under strict-use protocol.
Radiologist Feedback
Radiologists evaluated various aspects of image quality generated by the investigational Envision platform across four standard views: RCC, RMLO, LCC, and LMLO. These assessments provide a comprehensive overview of how the investigational Envision platform performed in critical areas such as positioning, contrast, sharpness, tissue visibility, noise, artifacts, and overall clinical image quality, presented in Table 3. Across all views, ratings were dominated by the acceptable and excellent categories for all parameters. For example, contrast was rated excellent in 41.9–48.5% of images depending on view, with all remaining images rated acceptable. Sharpness demonstrated a similar pattern, with 41.8–42.0% excellent ratings and the remainder acceptable. Tissue visibility was excellent in 50.2–50.5% of images, and noise was acceptable or excellent in all images. Artifacts were rated excellent in 33.4–34.8% of images, with <0.3% requiring reimaging. Overall clinical image quality was acceptable or excellent in 94.1–100% of cases across views. Positioning/tissue coverage showed expected view-specific differences, with craniocaudal views more frequently rated excellent than mediolateral oblique views, consistent with known variations in patient anatomy and positioning complexity.
 |
Table 3 Radiologist Assessment |
Radiologist Variability Across Sites
Radiologist variability was assessed descriptively at the level of site, view, and image-quality parameter. Across all seven sites and four views, the proportion of images rated acceptable or excellent for clinical image quality, contrast, sharpness, tissue visibility, noise, and artifacts was uniformly high, with means of 98–100% and median values of 100% for all parameters. Even for positioning and tissue coverage, where greater variability is expected due to anatomic and technical factors, the mean proportion of images rated acceptable or excellent remained high at 95.1% (median 100%; range 60–100%).
When the excellent category was examined independently, greater dispersion was observed, reflecting differences in how individual radiologists used the upper end of the three-point scale rather than differences in perceived adequacy. Median excellent ratings across site–view combinations were 80% for overall clinical image quality (range 14–100%), 83% for contrast (16–100%), 94% for sharpness (1–100%), and 95% for tissue visibility (3–100%). Artifacts and noise demonstrated similar patterns, with median excellent ratings of 80% (3–97%) and 89% (1–100%), respectively. Positioning and tissue coverage showed the lowest excellent proportions (median 23%; range 3–86%), consistent with radiologists more frequently reserving the “excellent” designation for other image-quality attributes.
Taken together, these findings indicate that although radiologists varied in their use of the “excellent” rating, particularly for positioning, the proportion of images judged to be at least clinically acceptable was consistently high across sites and views, demonstrating minimal practical variability in interpretive performance.
Positioning and Coverage
Most images across all views were rated as either acceptable or excellent, with RMLO and LMLO showing a slightly higher proportion of acceptable ratings compared to RCC and LCC. Specifically, 83.2% of RMLO images were rated as acceptable, compared to 66.2% of RCC images. However, the proportion of images rated as excellent was higher for the RCC (32.7%) and LCC (32.6%) views compared to RMLO (10.3%) and LMLO (11.1%). This suggests that while positioning was overall satisfactory or excellent, there may be an opportunity to obtain excellent coverage for oblique views.
Image Contrast
Contrast in mammography is essential for distinguishing between normal and abnormal tissues, particularly for identifying microcalcifications and masses. Approximately one-half of the images (48.4–48.5%) across the RCC, RMLO, and LMLO views were rated as excellent for contrast, whereas LCC images had slightly fewer excellent ratings (41.9%). The majority of images were deemed acceptable for contrast, with no images being rated as requiring reimaging, indicative of delivery of acceptable image contrast from the Envision platform.
Sharpness (In-Plane Resolution)
Sharpness is another critical factor in mammography, as it impacts the visibility of fine details, such as small masses or calcifications. Around 50% of the images across all views were rated as excellent for sharpness, with the other half rated as acceptable. These numbers are consistent across views, indicating that the investigational Envision platform delivers good in-plane resolution, which is crucial for diagnostic purposes.
Tissue Visibility at the Skin Line
Proper visibility of tissues near the skin line is important for ensuring that abnormalities near the breast surface are not missed. Approximately half of the images were rated as excellent for tissue visibility near the skin line, with the remainder rated as acceptable. This suggests that the investigational Envision platform performs well in this regard, capturing clear images of the tissue near the breast surface across all views.
Noise (Graininess)
Image noise, or graininess, can obscure fine details and affect the clarity of mammograms. Approximately 35% were rated excellent, while approximately 65% of the images across all views were rated as acceptable No images were deemed to require reimaging, indicating that the device produces images with minimal noise. This positively indicates the system’s ability to generate clear, diagnostically useful images across different views.
Artifacts
Artifacts are any undesired image components that could interfere with the interpretation of the mammogram. Only a very small percentage of images (0.2–0.3%) had unacceptable levels of artifacts, with the majority rated as acceptable (approximately 65%) or excellent (approximately 35%). A very low fraction of images (<0.5%) were rated as requiring reimaging. These results show that the investigational Envision platform effectively minimizes artifacts, further supporting the reliability of the images produced.
Clinical Image Quality
Finally, radiologists provided an overall assessment of clinical image quality. The LCC view had a slightly higher proportion of acceptable ratings (83.0%) compared to the other views, which had around 50% of images rated as acceptable. Conversely, the proportion of excellent ratings for views excluding LCC (around 48%), where the LCC view was lower (11.1%). This suggests that while LCC images are generally acceptable, there are opportunities to enhance the image quality for this view compared to the other angles.
Discussion
The preliminary findings from this analysis highlight several strengths of the Envision platform, particularly in patient comfort and diagnostic imaging despite the challenges in improving both image quality and comfort. These results are promising for both clinicians and patients, given the ongoing need to balance patient experience with the diagnostic accuracy of mammographic technologies.
Patient Comfort and Satisfaction
One of the most notable outcomes of the study is the high level of patient satisfaction, with 79% of subjects preferring the mammogram with the Envision platform compared to prior mammograms. Patient comfort is a critical metric in breast imaging, as pain during mammography compression is a known barrier to screening compliance.3,6 The Envision platform, specifically designed to reduce discomfort associated with breast compression, was preferred by patients compared to their prior mammography experience. Moreover, 37.8% of subjects found breast compression to be more comfortable with the investigational device compared to prior mammography experiences, a key factor that likely contributed to the higher overall patient satisfaction.
Patient comfort is particularly significant in the context of population-based screening programs, where compliance to regular mammograms is vital for early detection of breast cancer. If the Envision platform continues to provide patient comfort, it could have a long-term impact on improving compliance with screening guidelines, especially among women who have previously avoided mammograms due to discomfort.
Radiologist Image Quality Feedback
The feedback from radiologists regarding image quality was generally positive. The majority of images were rated as either acceptable or excellent across multiple parameters, including positioning, contrast, sharpness, tissue visibility, and noise reduction. These parameters constitute key aspects of mammographic image quality that directly impact a radiologist’s ability to detect early-stage breast cancer.
However, the differences in the quality ratings for specific views, particularly RMLO and LMLO, suggest technical challenges are associated with these oblique angles. RMLO and LMLO views had lower percentages of images rated as excellent for positioning and coverage compared to RCC and LCC. This is likely due to the inherent difficulties in capturing optimal images for oblique angles.7,8
Radiologist Variability
This preliminary case-collection study was designed with a single radiologist at each site interpreting the investigational images within routine clinical workflow. We assessed variability descriptively across sites and views. The proportion of images rated acceptable or excellent was uniformly high (typically ≥98% for all parameters including ≥95% for positioning), indicating that images were generally judged to be of at least clinically adequate quality. At the same time, the proportion rated excellent alone varied more widely between sites and views, particularly for positioning/tissue coverage, suggesting differences in how individual radiologists use the upper end of the 3-point scale rather than fundamental differences in perceived adequacy. This pattern should be considered when interpreting the image-quality results. The high overall rates of acceptable or excellent ratings are robust, but fine-grained differences in the use of the “excellent” category may reflect reader preference and local practice.
Contrast and Sharpness
The findings related to image contrast and sharpness are encouraging, as these metrics are important for detecting microcalcifications and soft tissue masses, which are early indicators of breast cancer. The Envision platform performed well, with approximately 40–50% of images rated as excellent for contrast, particularly in the RCC and RMLO views, and no images being rated as requiring reimaging in terms of contrast or sharpness. This suggests that the Envision platform is capable of generating high-quality diagnostic images. Interestingly, the LCC view had a lower proportion of images rated as excellent for contrast and clinical quality. The reason for this difference is unclear in the data.
Tissue Visibility and Noise Reduction
Visibility of breast tissue near the skin line is another critical factor in mammography, as lesions in this region may be difficult to detect if not imaged clearly. The Envision platform’s performance in this area was robust, with approximately 50% of images rated as excellent in terms of skin line visibility. This demonstrates that the Envision platform can provide comprehensive breast tissue visualization, which is essential for detecting superficial lesions.
Radiologists also reported low levels of noise (graininess) in the images, with nearly half rated as acceptable and around 34% rated as excellent. Low noise levels are crucial for maintaining image clarity and ensuring that fine details, such as microcalcifications, are not obscured. The Envision platform’s ability to minimize noise while maintaining high contrast and sharpness contributes to its overall diagnostic performance.
Clinical Implications
The study results have demonstrated the potential of the Envision platform to improve the patient experience during breast cancer screening without compromising image quality. Moreover, the Envision platform’s ability to minimize artifacts and noise while maintaining high levels of contrast and sharpness is particularly important in modern mammography, where early detection of subtle lesions is critical for improving patient outcomes. These results are promising for both clinicians and patients, offering new options and advancements which have the potential to improve screening compliance and early cancer detection in screening.
Limitations
There are some limitations to this study that should be considered when interpreting the results. First, one-third of the images lacked a radiologist’s evaluation, which may have introduced bias into the reported percentages for each image quality parameter. Reassessing the data with a reduced denominator for only the evaluated cases could offer clearer insights into performance.
Second, the study population consisted primarily of subjects undergoing routine screening mammograms, which may limit the generalizability of the results to populations with more complex diagnostic needs, such as women with known breast cancer or those undergoing follow-up evaluations. Additionally, the use of the investigational Envision platform under early-use conditions (for example, maximum tilt angle) and within a controlled study protocol may not fully reflect real-world usage patterns and outcomes.
Previous mammograms were not defined, controlled, or evaluated. Therefore, this study is unable to more precisely state or compare alternative cohorts to the Envision platform.
Finally, while patient feedback was generally positive, the study did not assess long-term outcomes related to diagnostic accuracy, patient compliance, or patient retention in breast cancer screening programs, all of which are critical measures of success in mammography systems.
Future refinements aimed at addressing the limitations identified in this study could further elevate the clinical utility of the Envision platform, making it an essential tool for breast cancer screening and diagnosis.
Conclusion
In this multicenter case-collection study, the Envision™ platform achieved consistently high acceptable-or-excellent ratings across all image-quality parameters, with expected view-specific variation in excellent scores for RMLO, LMLO, and LCC projections. Patient-reported comfort was favorable, with most subjects experiencing low discomfort and preferring the investigational exam. Because discomfort can influence screening behavior, improved comfort may help reduce barriers to participation. Both patients and radiologists provided favorable feedback overall, reflecting the high comfort ratings reported by subjects and the consistently adequate image quality assessments provided by radiologists.
Data Sharing Statement
Individual deidentified participant data will not be made publicly available. The study sponsor does not plan to share individual-level datasets beyond the summary results required for posting on ClinicalTrials.gov. Summary-level results from this preliminary case-collection study are available in the present manuscript and will be posted on ClinicalTrials.gov in accordance with applicable requirements. No additional study documents (eg, study protocol, statistical analysis plan, or analytic code) will be made available. Requests for clarification about the study findings may be directed to the corresponding author; however, no additional data will be shared.
Acknowledgments
Sami Elmoufti, Hologic Inc. Santina Wendling, Hologic Inc. April Sawko, Hologic Inc. Abuzar Shaukat, Hologic Inc. Claudia Perez-Ortega, Hologic Inc.
Funding
This study was funded by Hologic Inc.
Disclosure
Alexis Cooper and Muhammad Waqas are employees of Hologic Inc. Paul J Niklewski consults for and reports personal fees from Hologic Inc. The authors report no other conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–12. doi:10.3322/caac.21834
2. Duffy SW, Tabar L, Yen AM, et al. Mammography screening reduces rates of advanced and fatal breast cancers: results in 549,091 women. Cancer. 2020;126(13):2971–2979. doi:10.1002/cncr.32859
3. Whelehan P, Evans A, Wells M, Macgillivray S. The effect of mammography pain on repeat participation in breast cancer screening: a systematic review. Breast. 2013;22(4):389–394. doi:10.1016/j.breast.2013.03.003
4. Mercer CE, Hogg P, Szczepura K, Denton ERE. Practitioner compression force variation in mammography: a 6-year study. Radiography. 2013;19(3):200–206. doi:10.1016/j.radi.2013.06.001
5. Mercer CE, Szczepura K, Kelly J, et al. A 6-year study of mammographic compression force: practitioner variability within and between screening sites. Radiography. 2015;21(1):68–73. doi:10.1016/j.radi.2014.07.004
6. Rama S, Michael P, Shalom David S, Irit HH, Nathan C. Does Mammography Hurt? J Pain Symptom Manage. 2003;25(1):53–63. doi:10.1016/S0885-3924(02)00598-5
7. Yagil Y, Shalmon A, Rundstein A, et al. Challenges in contrast-enhanced spectral mammography interpretation: artefacts lexicon. Clin Radiol. 2016;71(5):450–457. doi:10.1016/j.crad.2016.01.012
8. Gardezi S, Elazab A, Lei B, et al. Breast cancer detection and diagnosis using mammographic data: systematic review. J Med Internet Res. 2019;21(7):e14464. doi:10.2196/14464
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.