Back to Journals » Drug Design, Development and Therapy » Volume 19
Prospective Dose-Finding of Esketamine for Suppressing Cervical Dilation Response in Ambulatory Hysteroscopy Under Monitored Anesthesia Care
Authors Yan L ![]() , Wang X, Wei J, Zhang M, Yang B
, Wang X, Wei J, Zhang M, Yang B ![]()
Received 31 July 2025
Accepted for publication 2 December 2025
Published 7 December 2025 Volume 2025:19 Pages 10835—10845
DOI https://doi.org/10.2147/DDDT.S557340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Anastasios Lymperopoulos
Lijuan Yan,1,* Xiao Wang,2,* Jianfei Wei,3 Meiqin Zhang,4,5 Bin Yang1
1Department of Anesthesiology, The First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, People’s Republic of China; 2Department of Ultrasound, The First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, People’s Republic of China; 3Department of Anesthesiology, The First Hospital of Zhangzhou China Merchants Economic and Technological Development Zone, Zhangzhou, People’s Republic of China; 4Department of Medical Affairs, The First Affiliated Hospital of Xiamen University, Xiamen, People’s Republic of China; 5Xiamen Daytime Medical Management Quality Control Center, Xiamen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Yang, Email [email protected] Meiqin Zhang, Email [email protected]
Background: Cervical dilation during ambulatory hysteroscopy often triggers somatic responses that challenge patient comfort and procedure smoothness. While esketamine’s unique analgesic profile could address this, its effective dose within a dexmedetomidine-remifentanil monitored anesthesia care (MAC) protocol is undefined.
Methods: In this prospective, double-blind, dose-finding study, 30 women received a standardized MAC protocol (dexmedetomidine 0.6 μg∙kg− 1 loading dose followed by 0.4 μg∙kg− 1∙h− 1, with remifentanil 5 μg∙kg− 1∙h− 1). Esketamine was administered via Dixon’s up-and-down sequential design (initial dose 0.3 mg∙kg− 1; increments/decrements 0.02 mg∙kg− 1) before cervical dilation. Positive response is defined as the absence of purposeful movement. The median effective dose (ED50) and 95% effective dose (ED95) were calculated using probit regression.
Results: 30 patients completed the study. The ED50 of esketamine was 0.36 mg∙kg− 1 (95% CI 0.35– 0.37) and the ED95 was 0.39 mg∙kg− 1 (95% CI 0.37– 0.42). Hemodynamic stability was maintained (mean arterial pressure change ≤ 15% from baseline) with no respiratory depression. Adverse events were self-limiting dizziness (66.7%) and nausea (6.7%). Recovery was swift, with a time to meet post-anesthesia care unit (PACU) discharge criteria of 17.93± 3.30 min, and patient satisfaction was high (median score 9/10, IQR 8– 10).
Conclusion: Under dexmedetomidine-remifentanil MAC, esketamine 0.39 mg∙kg− 1 (ED95) effectively suppresses the cervical dilation response, promotes hemodynamic and respiratory stability, and facilitates a rapid, enhanced recovery after surgery (ERAS)-compliant recovery. This dose-finding study provides a practical and effective anesthetic combination for clinical implementation in ambulatory hysteroscopy.
Clinical Trial Registration: ClinicalTrials.gov (identifier: NCT07034963). Principal Investigator: Lijuan Yan.
Plain Language Summary: This study determined the optimal dose of esketamine by testing different doses in thirty patients, finding that 0.39 mg∙kg− 1 effectively prevented patient movement and discomfort during cervical dilation in ambulatory hysteroscopy. Patients showed minimal movement during cervical dilation, while blood pressure and heart rate remained stable. Notably, no episodes of respiratory depression occurred. The most common side effect was temporary, mild dizziness, which resolved quickly without treatment. Importantly, patients recovered within about 20 minutes. This allowed for same-day discharge and was associated with high satisfaction with their care. This study provides anesthesiologists with robust, evidence-based guidance for using esketamine to enhance patient comfort and streamline recovery in ambulatory settings.
Keywords: cervical dilation response, effective dose, esketamine, hysteroscopy, monitored anesthesia care
Introduction
Hysteroscopic procedures have evolved into first-line interventions for intrauterine pathologies, owing to technological advancements enabling minimally invasive diagnosis and treatment.1 These procedures are frequently performed under monitored anesthesia care (MAC) in ambulatory surgery settings, which benefits patients by reducing hospital stays and clinical costs.2,3 However, it is important to note that cervical dilation, a critical step in hysteroscopic procedures, activates sacral parasympathetic pathways (S2–S4),4 provoking considerable visceral nociception and discomfort.2,5 This necessitates the optimization of patient-centered analgesic strategies of MAC while maintaining hemodynamic stability and respiratory safety.
MAC has emerged as the preferred anesthetic strategy for high-volume, fast-paced ambulatory hysteroscopic surgery, particularly valued for its rapid recovery profile.6,7 Despite the expansion of options for managing MAC due to pharmacological innovations and the advent of nerve blocks, available options each present limitation. Intravenous lidocaine has been demonstrated to attenuate cervical dilation response but has a short context-sensitive half-time and potential toxicity.5,8,9 Magnesium sulfate has analgesic and opioid-sparing effects but may delay recovery.10,11 Cervical blocks are effective but require expertise ill-suited to fast-paced workflows.12 While propofol and remimazolam provide sedation, they impair sleep architecture and lack specific visceral analgesic properties.13,14 Propofol also causes injection pain and increases the risks of oxygen desaturation.15
In contrast, dexmedetomidine preserves respiratory drive and synergizes with remifentanil’s ultrashort half-life (3 minutes), allowing precise titration against nociceptive stimuli.3,16 This combination achieves targeted analgesia without the cognitive or respiratory trade-offs associated with GABAergic sedation. Although dexmedetomidine-remifentanil significantly reduces the incidence of respiratory depression with propofol-remifentanil (14.3% vs 44.1%),17 Remifentanil-induced hyperalgesia (RIH) remains a concern after long-time or high-dose infusion.18,19
Esketamine, the derivative of ketamine, has emerged as a promising analgesic adjuvant in hysteroscopy. It acts via N‑methyl‑D‑aspartate (NMDA) receptor antagonism, producing dose-dependent sedation and analgesia.20,21 Importantly, esketamine has minimal effects on respiratory function and can counteract opioid-induced respiratory depression by enhancing ventilatory CO2 chemosensitivity22—a valuable property in contemporary opioid-sparing ambulatory anesthesia, fundamentally eliminating hypoventilation risks.23–25 However, its potential neuropsychiatric effects, such as dizziness and emergence agitation, require consideration, although these are typically dose-dependent and self-limiting.20,21 Esketamine and dexmedetomidine act synergistically to reduce opioid requirements via complementary α2-adrenergic and NMDA-receptor mechanisms.26 This strategic shift necessitates precision-balanced multimodal approaches that synergistically combine mechanistically distinct agents to address the dual imperatives of nociceptive blockade and ventilatory preservation.27 Therefore, dexmedetomidine-esketamine-remifentanil triad represents a promising alternative to propofol-based regimens,28 while esketamine’s anti-hyperalgesic properties may mitigate remifentanil-induced RIH risk.19
To date, no previous study has quantified esketamine’s dose-response relationship under dexmedetomidine-remifentanil based MAC during hysteroscopic surgery. Therefore, this study aimed to determine the median effective dose (ED50) and 95% effective dose (ED95) of esketamine for suppressing the somatic response to cervical dilation, defined as any purposeful movement, during ambulatory hysteroscopic surgery.
Methods
Study Design and Subjects
This prospective, double-blind, single-center dose-finding study was designed following the principles of the Declaration of Helsinki and the Standard Protocol Items: Recommendations for Interventional Trials guidelines.29 It was conducted from June to July 2025 at the Department of Anesthesiology of the First Affiliated Hospital of Xiamen University, China. This study was approved by the Ethics Committee of the First Affiliated Hospital of Xiamen University (Approval No. 101; 2025) and subsequently registered at the ClinicalTrials.gov (identifier: NCT07034963). According to the study flow chart (Figure 1), patients scheduled to undergo ambulatory hysteroscopic surgery under MAC were enrolled in this study. Before the procedure, all participants were furnished with a comprehensive explanation of the study’s procedures and potential risks, after which they were required to sign an informed consent form.
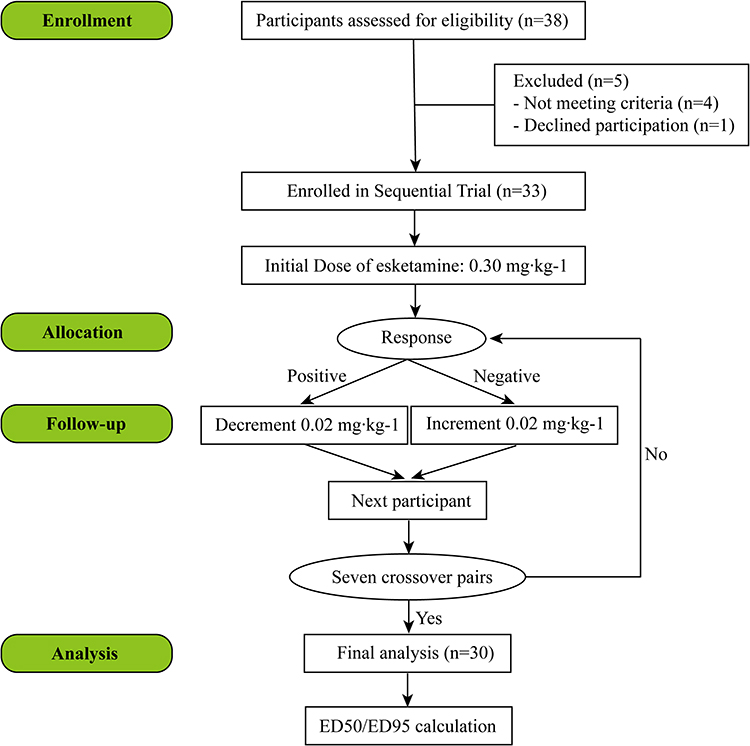 |
Figure 1 Flow chart of the study. Abbreviations: ED50, the median effective dose; ED95, 95% effective dose. |
Inclusion, Exclusion, and Termination Criteria
Inclusion Criteria
This study enrolled women aged 18–55 years with American Society of Anesthesiologists (ASA) physical status I–II, who were scheduled for elective ambulatory hysteroscopy under monitored anesthesia care. Additional standard inclusion and exclusion criteria about comorbidities, pharmacological contraindications, and airway risks were consistent with our previously published protocol.30
Exclusion and Withdrawal Criteria
Patients were excluded or withdrawn based on the predefined criteria detailed in our previously published protocol,30 which comprehensively addresses pharmacological contraindications, significant cardiopulmonary/hepatic comorbidities, neurological/psychiatric conditions, and perioperative risks. For the present hysteroscopy-specific cohort, the key exclusion factors were a body mass index (BMI) >28 kg∙m−2 and an anticipated difficult airway.
Study Protocol
Perioperative Management and Monitoring
All participants underwent standardized preoperative fasting (≥8 hours for solids, ≥2 hours for clear fluids) before anesthesia induction. Upon arrival in the operating room, patients were positioned in the lithotomy position and monitored using continuous electrocardiography (ECG), non-invasive mean arterial pressure (MAP) measurements at 3-minute intervals, SpO2, and nasal cannula-based capnography (Microstream™, Medtronic) for respiratory rate (RR) and end-tidal carbon dioxide (EtCO2) tracking. Supplemental oxygen was delivered via Venturi mask at 5 L∙min−1 throughout the procedure to maintain SpO2 ≥95%.
Comprehensive physiological monitoring was conducted at six predefined intervals: pre-anesthesia baseline, 60 seconds following esketamine (Jiangsu Hengrui Medicine Co., Ltd., Lianyungang, Jiangsu, China) administration, during vaginal disinfection, cervical dilation, intrauterine manipulation, and in the post-anesthetic care unit (PACU). Hemodynamic and respiratory parameters—including ECG, MAP, SpO2, and EtCO2—were continuously recorded via a validated anesthesia information management system with automated data extraction.
Dose Determination and Administration
The study employed Dixon’s up-and-down sequential design31 with an initial esketamine dose of 0.3 mg∙kg−1. The dosage administered to the latter patient was modified following the feedback provided by the researcher to the former patient. Dose adjustments followed a 0.02 mg∙kg−1 increment/decrement protocol based on purposeful movement during cervical dilation: purposeful movement triggered dose escalation, while absence of purposeful movement prompted dose reduction.
An independent nurse anesthetist prepared all esketamine solutions using weight-based calculations, diluting the designated dose with 0.9% saline to a fixed 20 mL volume in identical opaque syringes. To maintain blinding, syringes were labelled with a unique identifier and dispensed to the attending anesthesiologist who remained unaware of dose assignments and study protocol.
Anesthetic Protocol
All patients received a standardized anesthetic regimen sequentially. Dexmedetomidine (Sichuan Medco Huakang Pharmaceutical Co., Ltd., Jining, Shandong, China) (4 μg∙mL−1) infusion initiated with 0.6 μg∙kg−1 loading dose over 10 minutes, followed by 0.4 μg∙kg−1∙h−1 maintenance. Remifentanil (Jiangsu Enhua Pharmaceutical Co., Ltd., Xuzhou, Jiangsu, China) (50 μg∙mL−1) continuous infusion at 5 μg∙kg−1∙h−1. Esketamine bolus is administered intravenously over 60 seconds following the completion of the infusion of the loaded dose of dexmedetomidine. Procedural commencement required achieving Ramsay Sedation Scale (RSS)32 ≥5 within 1 minute post-esketamine administration. Surgical procedures were performed by the same board-certified gynecologist using standardized 9 mm rigid hysteroscopes, with cervical dilation performed via Hegar dilators under direct visualization. After the operation, 100 mg of flurbiprofen axetil was intravenously injected as an adjuvant drug for multimodal analgesia, and 4 mg of ondansetron was intravenously injected for preventive antiemesis. All patients were transferred to the day surgery ward only after recovery through the PACU.
A predefined rescue analgesia protocol was implemented for positive cervical dilation responses (defined as purposeful movement): intravenous remifentanil 0.5 μg∙kg−1 boluses were administered immediately, with subsequent doses permitted at 2-minute intervals. Anesthetic failure was declared if >3 rescue doses were required within 10 minutes, triggering protocol escalation with propofol 100 mg IV followed by supraglottic airway insertion and transition to controlled mechanical ventilation.
Airway compromise management adhered to a tiered algorithm. Initial interventions for respiratory depression (SpO2 <90% for >30 seconds or EtCO2 >55 mmHg) included chin lift and jaw thrust maneuvers, progressing to facemask ventilation with 100% oxygen if unresolved. Persistent hypoventilation unresponsive to manual maneuvers within 60 seconds mandated immediate supraglottic airway insertion and positive-pressure ventilation.
Hemodynamic instability triggered protocolized interventions: bradycardia (HR <45 bpm) was treated with atropine 0.5 mg IV, while hypotension (MAP <80% baseline) received phenylephrine 50 μg IV boluses. All adverse events, pharmacological interventions, rescue interventions, and protocol deviations were timestamped and quantified by blinded research personnel using validated case report forms. Onset duration, severity grading, and causal relationship assessment of adverse events were classified and reported.
Outcomes
The primary efficacy outcome was purposeful movement during cervical dilation. Negative response is defined as any purposeful movement, indicating unsuccessful response suppression. This included limb withdrawal, head elevation, or vocalization. Minor reflexes, such as finger flexion/extension or facial grimacing, were explicitly excluded. A positive response was the absence of such movement, indicating successful response suppression.
Secondary outcomes encompass postoperative pain, adverse events, and recovery-related clinical parameters. The intensity of pain experienced post-surgery was measured using a 10-cm Numeric Rating Scale (NRS), with 0 representing no pain and 10 representing severe pain at 2 h, 6 h, and 24 h post-surgery. Supplemental analgesic requirements (the dosage of oral acetaminophen) were also documented.
Adverse events were systematically categorized and monitored, including the following: (i) Cardiovascular: Hypotension (MAP <65 mmHg for >2 minutes), hypertension (MAP >110% baseline), sinus bradycardia (HR <45 bpm) or sinus tachycardia (HR >100 bpm). (ii) Neurological: dizziness was assessed by the attending anesthesiologist through directly asking “Do you feel dizzy?” Psychotomimetic reactions were actively monitored by the attending anesthesiologist. (iii) Gastrointestinal: Postoperative nausea and vomiting (PONV). (iv) Respiratory: Hypoxemia (peripheral oxygen saturation <90% for >15 seconds) or apnea (EtCO2 >55 mmHg).
Recovery-related clinical parameters, including awakening time, PACU time, discharge time, and the patient’s satisfaction score. The awakening time was defined as the period from the cessation of anesthetic drug infusion to the time when the patient regains consciousness. The PACU time was defined as the time from patient admission to the PACU until the fulfillment of the criteria for PACU discharge. PACU discharge criteria were assessed using the modified Aldrete score, with a predefined score of ≥9. The discharge time was defined as the interval between patient admission to the operating room and the fulfillment of the criteria for hospital discharge. Patient’s satisfaction score was graded using a 10-tier scale (0 = very unsatisfied; 10 = very satisfied).
Statistical Analysis
All analyses were performed using IBM SPSS Statistics (v20.0) and R statistical environment (v4.4.3; R Foundation) with RStudio interface (v2024.12.1+563). The sample size was guided by the target of obtaining 6–8 independent crossover pairs, which typically requires 20–30 evaluable participants based on previous dose-finding studies using this methodology. To account for potential non-evaluable responses that could break the sequential chain, 33 patients were ultimately enrolled to ensure statistical adequacy. The study was terminated after 30 patients because the dose-response relationship had stabilized with 7 obtained crossover pairs, which followed the sequential allocation principles of Dixon’s up-and-down method and were deemed sufficient for reliable probit analysis. There were no protocol deviations, withdrawals, or missing data for the primary endpoint; thus, no data imputation was necessary.
The ED50 and ED95 of esketamine were estimated via probit regression analysis using the generalized linear model (GLM) framework with a probit link function. The generation of dose-response curves was achieved through the implementation of maximum likelihood estimation, complemented by the bootstrap resampling (1000 iterations) to derive robust 95% confidence intervals (CI). Sequential dose-response patterns were visualized using GraphPad Prism (v9.0.0), incorporating nonlinear regression modeling for curve fitting. Throughout the study, statistical significance was defined by a two-tailed alpha level of 0.05.
Results
Baseline Characteristics
30 enrolled patients completed the trial. Baseline characteristics are summarized in Table 1. No significant differences existed across sequential dose cohorts.
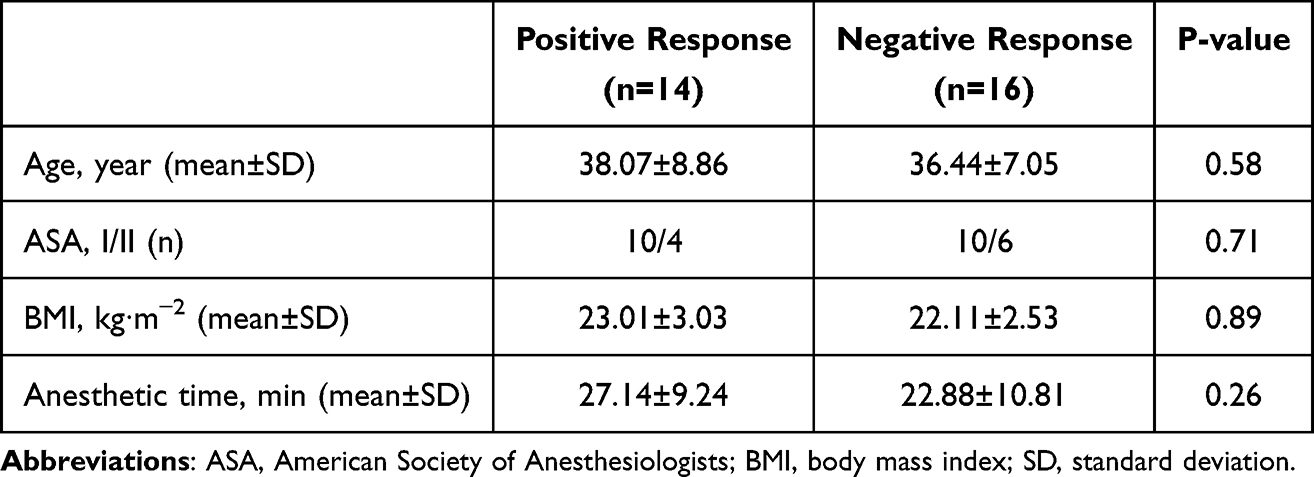 |
Table 1 Patients’ Baseline Characteristics |
Sequential Trial Dose-Response
Figure 2 depicts the dose-response sequence using Dixon’s up-and-down method. Starting from 0.30 mg∙kg−1, seven crossover pairs were achieved after 30 patients (dose range: 0.30–0.40 mg∙kg−1). Negative response rates decreased with esketamine dose escalation (Table 2).
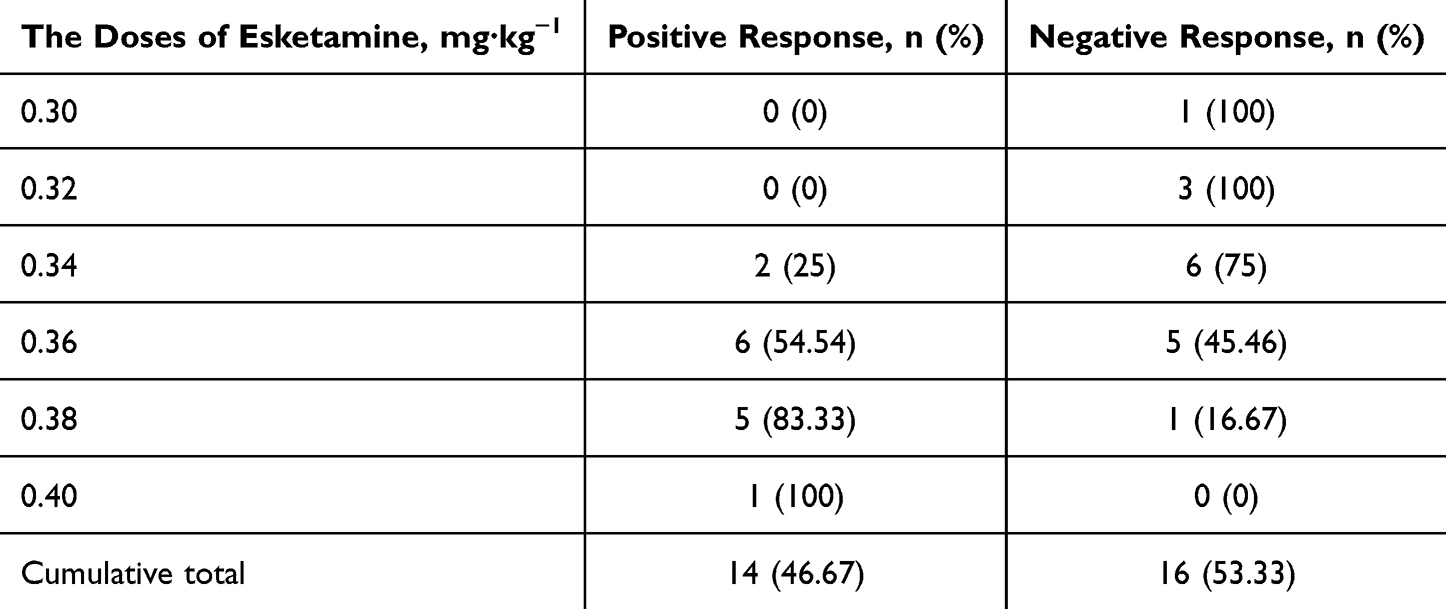 |
Table 2 Positive/Negative Response Among Different Doses |
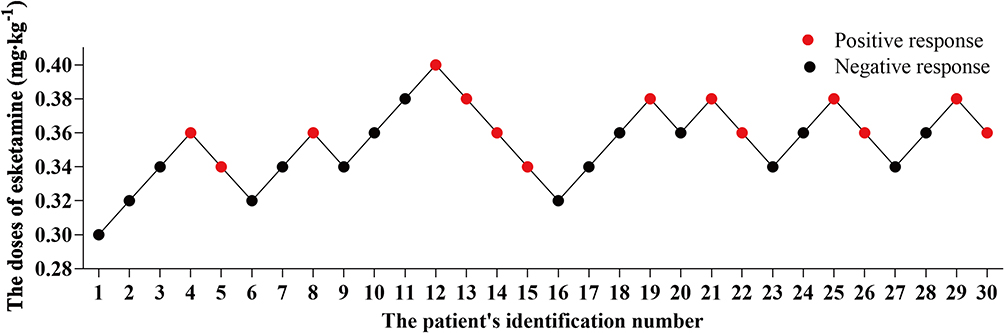 |
Figure 2 Dose-response using Dixon’s up-and-down method. |
Dose-Response Curve and ED50/ED95 Calculation
Probit analysis demonstrated an ED50 of 0.36 mg∙kg−1 and an ED95 of 0.39 mg∙kg−1 for somatic response suppression (Figure 3). The model showed adequate fit by the Hosmer-Lemeshow test (χ2=0.07, p=0.97).
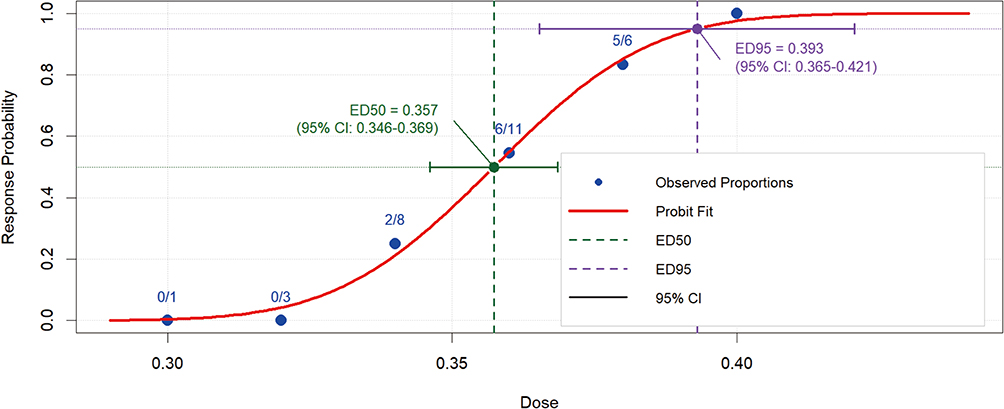 |
Figure 3 Dose-response curve. Abbreviations: ED, the effective dose; ED50, the median effective dose; ED95, 95% effective dose; CI, confidence intervals. |
Adverse Events
Hemodynamics remained stable with a mean MAP fluctuation ≤15% from baseline. No respiratory depression or cardiovascular events occurred, with all patients maintaining SpO2 ≥94% and EtCO2 ≤48 mmHg. The adverse events that were observed included nausea (2/30, 6.67%) and dizziness (20/30, 66.67%), both of which were self-limiting and resolved without intervention within one hour.
Recovery Quality After Anesthesia and Dose-Related Analysis
Recovery profiles aligned with enhanced recovery after surgery (ERAS) principles: time to meet PACU discharge criteria was about 20 min. Median patient satisfaction score was 9/10 (IQR: 8–10) on a 10-point scale (Table 3). The postoperative pain scores (2h/6h/24h) were all 0, so no one required rescue analgesics.
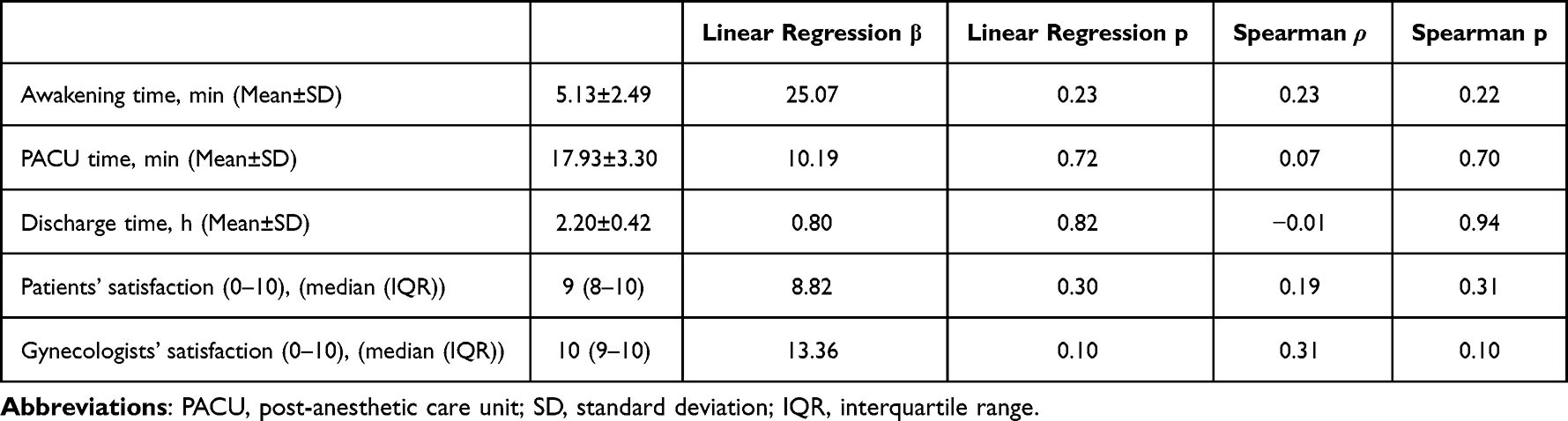 |
Table 3 Recovery Quality After Anesthesia and Dose-Related Analysis |
Based on the analysis of the current dataset, changes in esketamine dose showed no statistically significant effects on any of the measured recovery outcomes (Table 3).
Discussion
The ED50 of 0.36 mg∙kg−1 (95% CI: 0.35–0.37) and ED95 of 0.39 mg∙kg−1 (95% CI: 0.37–0.42) provide an evidence-based solution to a recognized practice gap: the lack of a precise dosing guideline for esketamine within opioid-sparing MAC regimens. This directly enables anesthesiologists to optimize analgesia while systematically minimizing opioid-related risks, thereby advancing ERAS protocols in ambulatory settings.
The Synergistic Mechanism of the Three Drugs
The observed dose-efficacy relationship stems from a triple synergistic mechanism between esketamine, dexmedetomidine, and remifentanil. Esketamine’s NMDA receptor antagonism converges with dexmedetomidine’s α2-adrenergic modulation to enhance descending inhibitory pathways.26 Concurrently, the ultra-short half-life of remifentanil allows for precise titration against dynamic nociceptive stimuli.3 At an ED95 of 0.39 mg∙kg−1, esketamine achieves a threshold sufficient to block somatic responses during cervical dilation without inducing excessive sedation or psychotomimetic reactions. This equilibrium is further exemplified by the respiratory safety measure of the anesthesia protocol, which has led to a complete elimination of incidents of hypoxemia.
Hemodynamic stability was maintained (mean MAP fluctuation ≤15% from baseline), and respiratory safety was confirmed (SpO2 ≥94%, EtCO2 ≤48 mmHg). The observed hemodynamic stability likely results from esketamine’s sympathomimetic properties33 effectively counteracting the cardiovascular depression inherent to the dexmedetomidine-remifentanil base regimen. This balancing effect underscores the rationale for the triple-drug combination. However, the absence of continuously archived waveform data precludes finer analysis of peak physiologic responses. Future studies would benefit from incorporating high-resolution data capture to delineate more subtle pharmacodynamic profiles.
The Value of the Daytime Surgery Centers During Clinical Practice
From a clinical perspective, these doses offer pragmatic solutions to the challenges prevalent in China’s rapidly expanding ambulatory surgery infrastructure. The high patients’ satisfaction score (median score 9/10, IQR 8–10) likely reflects the combination of effective intraoperative analgesia, a comfortable recovery without recall of pain, well-controlled postoperative pain (as measured by NRS at 2 h, 6 h, and 24 h), and the rapid return to clear-headed function. Such characteristics align with ERAS protocols, prompting same-day discharge for uncomplicated hysteroscopic surgery. The protocol’s efficacy in reducing opioid requirements has the potential to mitigate symptoms of nausea (2/30, 6.67%), which, in the context of outpatient care, is a critical consideration given the limitations of antiemetic resources.
The rapid recovery time (time to meet PACU discharge criteria was 17.93±3.30 min) supports high-volume surgical workflows, with the potential to increase daily procedure capacity by 5–8 cases per operating room in day-surgery centers that perform large-volume surgeries.
The protocol’s alignment with ERAS and opioid-sparing goals is further evidenced by its exceptional respiratory safety profile. In this trial, no patients required airway escalation beyond basic maneuvers, eliminating the need for resource-intensive advanced airway management. It is possible that the esketamine-based MAC may offer advantages over propofol-based regimens in preserving airway integrity.33 This key advantage is crucial for maintaining workflow efficiency and safety in resource-limited ambulatory settings.
Collectively, minimal opioid use, avoidance of advanced airways, rapid recovery, and high patient satisfaction attributes establish the ED95-based regimen as a practical and scalable model for ambulatory hysteroscopy. This is particularly impactful in resource-constrained settings, such as primary hospitals or high-volume day-surgery centers.
Limitations and Future
This study has several limitations inherent to its design as a dose-finding trial. As with many studies employing Dixon’s sequential methodology, the single-center design and relatively small sample size may affect the generalizability of our results across diverse patient populations (eg, ASA III–IV, BMI >28 kg∙m−2), varying surgical stimuli, or different levels of operator experience. While this approach efficiently provided initial ED50/ED95 estimates, we explicitly recommend the ED95 of 0.39 mg∙kg−1 as the clinically applicable dose to ensure high efficacy in broader populations. Future multi-center studies with larger sample sizes are warranted to validate this dosing regimen in higher-risk patients and more complex hysteroscopic procedures.
The high incidence of transient dizziness (66.7%), while self-limiting and not observed to prolong PACU stay or diminish patient satisfaction in this cohort, warrants vigilant clinical monitoring to mitigate potential fall risks during early ambulation and ensure safe discharge readiness. Future comparative studies should incorporate patient-reported outcome measures to better quantify the impact of dizziness on perioperative experience.
A binary somatic response was selected as the primary endpoint for this dose-finding study because it provides an objective, reproducible, and clinically decisive measure of analgesic efficacy during the intense, transient stimulus of cervical dilation. Its unambiguous nature ensures reliable assessment across patients, directly influences surgical conditions, and is not confounded by the sedative effects of the anesthetic regimen. While the objective somatic response is a robust and clinically critical endpoint for dose-finding, reliance on it as a binary endpoint may underestimate subjective pain experiences, particularly in chronic pain or opioid tolerance populations. Notably, the reliable assessment of subjective pain is confounded by the level of sedation, as sedative medications alter mental status and compromise the validity of patient-reported outcomes. Therefore, it is necessary to incorporate validated pain scales to refine dosing further and perform multicenter validation of these doses in diverse populations, including those with obesity or chronic pain.
The future optimization of ambulatory hysteroscopy extends beyond pharmacological refinement to encompass both technological innovation and information management. The long-term goal remains the development of AI-driven pain monitoring systems34 for real-time esketamine titration. Concurrently, mitigating the risk of patient anxiety fueled by unreliable online content35 through curated education is equally critical. Addressing these dual challenges of objective assessment and subjective perception will be key to delivering a truly personalized anesthesia strategy.
Conclusion
This prospective dose-finding study establishes the ED50 and ED95 of intravenous esketamine (0.36 and 0.39 mg∙kg−1, respectively) for suppressing somatic responses to cervical dilation under a dexmedetomidine-remifentanil MAC regimen. The ED95 dose provided effective nociceptive blockade while maintaining hemodynamic and respiratory stability, facilitating rapid recovery and high patient satisfaction aligned with ERAS. The principal trade-off was a high, yet self-limiting, incidence of dizziness, underscoring the need for proactive patient counselling. Although these data provide a validated dosing framework for esketamine in ambulatory hysteroscopy, external validation across broader patient cohorts and different clinical settings remains warranted.
Generative AI Statement
The authors declare that no generative artificial intelligence (Gen AI) tools (such as ChatGPT) were used for content generation or the conceptual development of this manuscript.
Data Sharing Statement
The de-identified data that support the findings of this study are available from Principal Investigator Lijuan Yan upon reasonable request. Please contact via Email at [email protected].
Ethics Statement
This study has been approved by the Ethics Committee of the First Affiliated Hospital of Xiamen University (Approval No. 101; 2025) on June 5, 2025.
Acknowledgments
We would like to express our sincere gratitude to Dr Yayun Xu from the Department of Obstetrics and Gynecology for her invaluable support during the execution of this research study. We thank BioRender.com (https://BioRender.com) for providing the graphical elements used in the Graphical Abstract.
Author Contributions
Lijuan Yan and Xiao Wang are co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by Fujian Research and Training Grants for Young and Middle-aged Leaders in Healthcare (Bin Yang), and Scientific Research Special Grant Fund Project of Wu Jieping Medical Foundation (grant number: 320.6750.2024-05-50).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Guan Y, Pan H, Cong X, et al. Effect of esketamine on haemodynamic fluctuations in patients undergoing hysteroscopic surgery: a prospective, double-blind randomized clinical trial. Br J Clin Pharmacol. 2024;90(11):2754–2762. doi:10.1111/bcp.16165
2. Harrison R, Kuteesa W, Kapila A, et al. Pain-free day surgery? Evaluating pain and pain assessment during hysteroscopy. Br J Anaesth. 2020;125(6):e468–e470. doi:10.1016/j.bja.2020.08.015
3. Ryu JH, Kim JH, Park KS, Do SH. Remifentanil-propofol versus fentanyl-propofol for monitored anesthesia care during hysteroscopy. J Clin Anesth. 2008;20(5):328–332. doi:10.1016/j.jclinane.2007.12.015
4. Lee J, Lee S, Lee H, Kim HC, Park C, Kim JY. The effect of preoperative intravenous lidocaine on postoperative pain following hysteroscopy: a randomized controlled trial. Medicine. 2020;99(42):e22751. doi:10.1097/MD.0000000000022751
5. Xu L, Wang C, Dai S, et al. Intravenous lidocaine attenuates response to cervical dilation for hysteroscopy: a randomised controlled trial. Br J Anaesth. 2021;127(5):e166–e168. doi:10.1016/j.bja.2021.07.020
6. Cooper NAM, Ireland N. Analgesia and anaesthesia for hysteroscopy. In: Diagnostic and Operative Hysteroscopy; 2020:72–82. doi:10.1017/9781316276020.006
7. Centini G, Troia L, Lazzeri L, Petraglia F, Luisi S. Modern operative hysteroscopy. Minerva Ginecol. 2016;68(2):126–132.
8. Neal JM, Barrington MJ, Fettiplace MR, et al. The third American Society of regional anesthesia and pain medicine practice advisory on local anesthetic systemic toxicity: executive summary 2017. Reg Anesth Pain Med. 2018;43(2):113–123. doi:10.1097/AAP.0000000000000720
9. Beaussier M, Delbos A, Maurice-Szamburski A, Ecoffey C, Mercadal L. Perioperative use of intravenous lidocaine. Drugs. 2018;78(12):1229–1246. doi:10.1007/s40265-018-0955-x
10. Gao PF, Lin JY, Wang S, et al. Antinociceptive effects of magnesium sulfate for monitored anesthesia care during hysteroscopy: a randomized controlled study. BMC Anesthesiol. 2020;20(1):240. doi:10.1186/s12871-020-01158-9
11. Altan A, Turgut N, Yildiz F, Turkmen A, Ustun H. Effects of magnesium sulphate and clonidine on propofol consumption, haemodynamics and postoperative recovery. Br J Anaesth. 2005;94(4):438–441. doi:10.1093/bja/aei070
12. Cingiloglu P, Mooney S, McNamara H, et al. Pain experience with outpatient hysteroscopy: a prospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2024;300:302–308. doi:10.1016/j.ejogrb.2024.07.047
13. Zhang X, Li S, Liu J. Remimazolam-remifentanil causes less postoperative nausea and vomiting than remimazolam-alfentanil during hysteroscopy: a single-centre randomized controlled trial. BMC Anesthesiol. 2023;23(1):199. doi:10.1186/s12871-023-02164-3
14. Schuttler J, Eisenried A, Lerch M, Fechner J, Jeleazcov C, Ihmsen H. Pharmacokinetics and pharmacodynamics of remimazolam (CNS 7056) after continuous infusion in healthy male volunteers: part I. Pharmacokinetics Clin Pharmacodynamics Anesthesiol. 2020;132(4):636–651. doi:10.1097/ALN.0000000000003103
15. Shen Y, Yin L, Hu B, Xia Y, Zhang L. Preoperative anxiety’s impact on the median effective dose of esketamine for alleviating propofol injection pain in patients undergoing painless abortion: a randomized, double-blind, controlled trial. Drug Des Devel Ther. 2024;18:5863–5872. doi:10.2147/DDDT.S482019
16. Bingol Tanriverdi T, Koceroglu I, Devrim S, Gura Celik M. Comparison of sedation with dexmedetomidine vs propofol during hysteroscopic surgery: single-centre randomized controlled trial. J Clin Pharm Ther. 2019;44(2):312–317. doi:10.1111/jcpt.12793
17. Park S, Choi SL, Nahm FS, Ryu JH, Do SH. Dexmedetomidine-remifentanil vs propofol-remifentanil for monitored anesthesia care during hysteroscopy: randomized, single-blind, controlled trial. Medicine. 2020;99(43):e22712. doi:10.1097/MD.0000000000022712
18. Zhao HY, Liu LY, Cai J, Cui YJ, Xing GG. Electroacupuncture treatment alleviates the remifentanil-induced hyperalgesia by regulating the activities of the ventral posterior lateral nucleus of the thalamus neurons in rats. Neural Plast. 2018;2018:6109723. doi:10.1155/2018/6109723
19. Wang J, Feng Y, Qi Z, et al. The role and mechanism of esketamine in preventing and treating remifentanil-induced hyperalgesia based on the NMDA receptor-CaMKII pathway. Open Life Sci. 2024;19(1):20220816. doi:10.1515/biol-2022-0816
20. Weng M, Wang D, Zhong J, Qian M, Zhang K, Jin Y. Comparison between esketamine and alfentanil for hysteroscopy: a prospective, double-blind, randomized controlled trial. Drug Des Devel Ther. 2024;18:3629–3641. doi:10.2147/DDDT.S472651
21. Wan JX, Zeng SS, Wu ZQ, et al. Effect of different doses of esketamine on the median effective concentration of propofol for inhibiting body movement during hysteroscopy. Sci Rep. 2024;14(1):25153. doi:10.1038/s41598-024-75902-3
22. Jonkman K, van Rijnsoever E, Olofsen E, et al. Esketamine counters opioid-induced respiratory depression. Br J Anaesth. 2018;120(5):1117–1127. doi:10.1016/j.bja.2018.02.021
23. Zbarsky SJD, Hanna IA, Ryu JD, et al. Multi-institutional retrospective study on opioid prescribing patterns of oral and maxillofacial surgeons. J Am Dent Assoc. 2025;156(2):124–132e121. doi:10.1016/j.adaj.2024.11.009
24. Pappu A, Singh M. Best perioperative practices in the management of obstructive sleep apnea patients undergoing ambulatory surgery. Curr Opin Anaesthesiol. 2024;37(6):644–650. doi:10.1097/ACO.0000000000001441
25. Martin LD, Franz AM, Rampersad SE, et al. Outcomes for 41 260 pediatric surgical patients with opioid-free anesthesia: one center’s experience. Paediatr Anaesth. 2023;33(9):699–709. doi:10.1111/pan.14705
26. Huang Z, Liu N, Hu S, Ju X, Xu S, Wang S. Effect of dexmedetomidine and two different doses of esketamine combined infusion on the quality of recovery in patients undergoing modified radical mastectomy for breast cancer - a randomised controlled study. Drug Des Devel Ther. 2023;17:2613–2621. doi:10.2147/DDDT.S422896
27. Coppens M, Steenhout A, De Baerdemaeker L. Adjuvants for balanced anesthesia in ambulatory surgery. Best Pract Res Clin Anaesthesiol. 2023;37(3):409–420. doi:10.1016/j.bpa.2022.12.003
28. Chen H, Zhi J, Wang L, et al. Subanesthetic dose of esketamine improves the sedative and analgesic effects of dexmedetomidine and remifentanil in liposuction anesthesia: a prospective, double-blinded, randomized controlled trial. Drug Des Devel Ther. 2024;18:3645–3658. doi:10.2147/DDDT.S470891
29. Chan AW, Tetzlaff JM, Gotzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346(e7586). doi:10.1136/bmj.e7586
30. Wang X, Yan L, Cai J, Wei J, Zhang Z, Yang B. Esketamine versus fentanyl as adjuncts to hepatic hilar nerve block for ambulatory percutaneous liver tumor ablation focusing on respiratory safety: protocol for a randomized controlled trial. Front Pharmacol. 2025;16:1644029. doi:10.3389/fphar.2025.1644029
31. Pace NL, Stylianou MP. Advances in and limitations of up-and-down methodology: a precis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
32. Sheng Z, Liu X, Lin K, Liu J, Mao J, Qian X. Determining the effective dose of esketamine combined with propofol for painless hysteroscopy: a prospective dose-finding study. Front Pharmacol. 2024;15:1419732. doi:10.3389/fphar.2024.1419732
33. Si J, Li X, Wang Y, Feng N, Cui M. Effects of adding low-dose esketamine to sufentanil and propofol sedation during cervical conization: a single-centre, randomized controlled trial. BMC Anesthesiol. 2024;24(1):15. doi:10.1186/s12871-023-02389-2
34. Salama V, Godinich B, Geng Y, et al. Artificial intelligence and machine learning in cancer pain: a systematic review. J Pain Symptom Manage. 2024;68(6):e462–e490. doi:10.1016/j.jpainsymman.2024.07.025
35. Libretti A, Vitale SG, Saponara S, et al. Hysteroscopy in the new media: quality and reliability analysis of hysteroscopy procedures on youtube. Arch Gynecol Obstet. 2023;308(5):1515–1524. doi:10.1007/s00404-023-07172-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effective Doses of Nalbuphine Combined with Propofol in Painless Hysteroscopy
Zhong W, Chen C, Tang W
International Journal of General Medicine 2022, 15:5609-5614
Published Date: 11 June 2022
RETRACTED ARTICLE: Effective Doses of Oliceridine Combined with Propofol for Painless Hysteroscopy: A Prospective Dose-Finding Study
Gao L, Tan A, Wang Z, Wei L, Wang X
International Journal of General Medicine 2025, 18:2651-2657
Published Date: 21 May 2025
Comparison of the Effective Dose 90 (ED90) and Clinical Outcomes of Fentanyl Versus Esketamine for Analgesia in Hysteroscopy: A Two-Part, Randomized, Double-Blind Trial
Du J, Li C, Huang M, Qin X
Drug Design, Development and Therapy 2026, 20:574516
Published Date: 13 January 2026
Effect of Different Doses of Esketamine on the Propofol Effect-Site Concentration Required to Suppress Cervical Dilation-Associated Movement During Hysteroscopy: A Prospective, Randomised, Controlled, Parallel-Group Dose-Response Trial
Shen Y, Yin L, Xu S, Hu B, Zhang L
Drug Design, Development and Therapy 2026, 20:602098
Published Date: 4 May 2026