Back to Journals » Patient Preference and Adherence » Volume 14
Proposal for a Framework to Enable Elicitation of Preferences for Clients in Need of Long-Term Care
Authors van Leersum CM ![]() , van Steenkiste B, Moser A, Wolf JRLM, van der Weijden T
, van Steenkiste B, Moser A, Wolf JRLM, van der Weijden T ![]()
Received 9 April 2020
Accepted for publication 7 July 2020
Published 25 August 2020 Volume 2020:14 Pages 1553—1566
DOI https://doi.org/10.2147/PPA.S257501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Catharina M van Leersum,1 Ben van Steenkiste,1 Albine Moser,1,2 Judith RLM Wolf,3 Trudy van der Weijden1
1Department of Family Medicine, CAPHRI School for Public Health and Primary Care, Maastricht University Medical Center, Maastricht, the Netherlands; 2Research Center for Autonomy and Participation of Persons with a Chronic Illness, Zuyd University of Applied Sciences, Heerlen, the Netherlands; 3Impuls-Netherlands Center for Social Care Research, Radboud Institute for Health Sciences, Radboud University Medical Center, Nijmegen, the Netherlands
Correspondence: Catharina M van Leersum
Department of Family Medicine, CAPHRI School for Public Health and Primary Care, Maastricht University Medical Center, Peter Debyeplein 1 (Room 3.022), Maastricht 6229 HA, the Netherlands
Tel +31 43 388 2295
Email [email protected]
Purpose: Collaborative deliberation comprises personal engagement, recognition of alternative actions, comparative learning, preference elicitation, and preference integration. Collaborative deliberation may be improved by assisting preference elicitation during shared decision-making. This study proposes a framework for preference elicitation to facilitate collaborative deliberation in long-term care consultations.
Methods: First, a literature overview was conducted comprising current models for the elicitation of preferences in health and social care settings. The models were reviewed and compared. Second, qualitative research was applied to explore those issues that matter most to clients in long-term care. Data were collected from clients in long-term care, comprising 16 interviews, 3 focus groups, 79 client records, and 200 online client reports. The qualitative analysis followed a deductive approach. The results of the literature overview and qualitative research were combined.
Results: Based on the literature overview, five overarching domains of preferences were described: “Health”, “Daily life”, “Family and friends”, ”Living conditions”, and “Finances”. The credibility of these domains was confirmed by qualitative data analysis. During interviews, clients addressed issues that matter in their lives, including a “click” with their care professional, safety, contact with loved ones, and assistance with daily structure and activities. These data were used to determine the content of the domains.
Conclusion: A framework for preference elicitation in long-term care is proposed. This framework could be useful for clients and professionals in preference elicitation during collaborative deliberation.
Keywords: preference elicitation, long-term care, patient preferences, collaborative deliberation, decision support
Introduction
Collaborative deliberation is a process whereby care professionals and clients build a relationship that requires interest on the part of the professional, and the sharing of views on the priorities, preferences, needs and wants of the client.1 It has been suggested as the ideal model for shared decision-making (SDM).1 SDM is an approach whereby professionals provide information and deliberate with those clients who are faced with a preference-sensitive decision.2 In SDM professionals partner with clients to acknowledge there is a decision to be made, improve the sharing of preferences, and discuss the courses of action for an individual.2,3 This approach is important in order to understand the client’s situation, and together to decide on the most suitable course of action. One possible process, the three-talk SDM model, starts with the “team talk”, followed by the “option talk”, and ends with the “decision talk”, where preference-based decisions about treatment are made.4
Collaborative deliberation has the potential to assist with all steps in SDM, and it is the key to the decision talk; clients are invited to share the issues that matter to them and formulate preferences for decision values and decision-making.5 The term preferences is in spoken language used as an umbrella term to refer to someone’s perspectives.6 In this study, client preferences encompass all aspects of health and healthcare and the decision values.3,6 Preferences include aspects of client health itself, and should ideally be expanded with aspects beyond health important to the quality of life.5 Furthermore, the preferences include the positive and negative aspects described by client and professional considering the courses of action.3 Individual preferences differ due to the differing contexts and multiple aspects that play a role in constructing preferences.7–9 Each individual will consider different aspects and also weigh them differently.10–12
Construction and elicitation of preferences as part of a conversation between professionals and clients is at the core of collaborative deliberation. Supporting clients to engage in the process of decision-making is essential to maximize the preferred outcome and to gain insight into someone’s preferences.13,14 Preferences need to be understood and integrated into decision-making to improve client-centered care outcome and quality of life.15 However, engaging clients in collaborative deliberation is not standard practice in health and social care settings.16 Both professionals and clients have suggested that more assistance with engaging in discussion and with preference elicitation might be helpful.17 Preference elicitation and the understanding of someone’s preferences should become central in the decision-making process in order to provide care tailored to an individual’s needs and wishes.2,18
Tools could help in strengthening the preference elicitation part of the decision-making process.19,20 Many approaches are currently used, an example is the Outcome Prioritization Tool (OPT). The OPT is a tool to support patient-centred decision-making in curative treatment decisions by facilitating talk on prioritized preferences for specific outcomes, as part of the consultation process in general practice for example.21 Using OPT in preference-sensitive decision-making leads to enhanced engagement of clients, and a deepening of the relationship resulting in better insight into a client’s views on care.21 A similar conversation-supporting model specifically developed for clients in need of long-term care could be beneficial to assist with preference elicitation during the search for preferred care. Long-term care is regarded as care provided for at least six months for reasons of ageing, disability, chronic illness, or any situation that limits the ability to self-care and manage activities, eg, washing, grocery shopping, or work.22 Care can be provided in any setting, including home care, care facilities, or nursing homes.23 Decisions concerning the long term usually have an impact on someone’s life, as the outcome is uncertain and the outcome might be care and support.24
A model to assist with collaborative deliberation and communication on preferences could support professionals in encouraging and engaging their clients in making decisions about long-term care. This could enhance collective understanding by the reflection on preferences. It might diminish bias and create an agreement on a strategy suitable both for the client and the situation.25 Some established techniques for developing models originated from health technology assessment (HTA).26 Discrete choice experiments could support preference elicitation, but these methods may be cognitively too complex for clients in need of long-term care.26 The number of validated models aimed at discussing the preferences of clients is limited.27–29 There are few models specifically made for clients in long-term care settings.
There is a need for a model specifically designed for clients in need of long-term care. Different from models made for single-disease decision-making, decisions regarding long-term care are more complex, because they are made for a longer period with different care moments and multiple preference-sensitive decisions. In the long-term care settings, it seems important to change the focus from a one-time decision towards multiple decisions. Aspects beyond care need to be considered to assist clients and caregivers with the difficulties they experience in the decision-making.17 Therefore, the aim of this study was to propose a framework specifically designed to support preference elicitation for clients and professionals in long-term care. The following two research questions were addressed: “Which models are available to support preference elicitation in health and social care?”, and “What are the preferences of clients in need of long-term care?” In order to answer the first research question, a literature overview was performed to examine different models of preference elicitation and identify overarching domains. Qualitative data were collected to explore the preferences of clients in long-term care and complement the framework with the aspects that matter most in long-term care, to answer the second research question. The combination of a literature overview with qualitative data is useful to propose a framework to assist preference elicitation specific for individual clients in need of long-term care. This study is part of a larger project on assistance with the decision-making process of clients in four long-term care sectors in the Netherlands: the nursing and care of elderly, mental healthcare, care of people with disabilities, and social care.
Methods
A mixed-method approach with an explanatory design was applied.30 The design was chosen to complement the literature overview with qualitative data. Various models were retrieved from the literature then reviewed and compared with one another. Subsequently, a set of five overarching domains of preferences were determined and defined. Data from qualitative research among clients in long-term care were used to gain in-depth insight into what mattered most to these clients as voiced by clients themselves. An open interview guide was used without the five overarching domains. With the data analysis, the issues that mattered most to clients in long-term care were deductively analyzed and clustered in the five overarching domains.
Literature Overview
To answer the first research question a literature overview was made. First, a literature search was conducted using the All Field terms (Figure 1) “preference(s) elicitation and construction”, “value(s) elicitation and construction” and “decision aid(s)”. The term decision aid was added, because decision aids should include preference elicitation exercises to facilitate individuals in understanding of preferences important during decision-making.31,32 The search was performed in April 2017 in the databases PubMed, Web of Science, PsycINFO, and BioMed Central. To update this literature, a second search was performed in August 2019. The inclusion criteria were studies describing a method, model or framework for preference construction and elicitation, in setting of health and social care in the Netherlands. There were no restrictions on publication date, type of research, peer review or study design. Records not in English or Dutch were excluded. In total 2691 records were retrieved (Figure 1), of which 41 duplicates were removed. After screening the titles and abstracts of the remaining 2651 records, 2610 records were removed as extensive inclusion of preference elicitation was missing. The remaining 41 records were screened for actual use in health and social care. Twenty-two records remained for full-text reading and analysis (Supplementary file 1). All records describing models for preference elicitation for a single-disease were excluded.
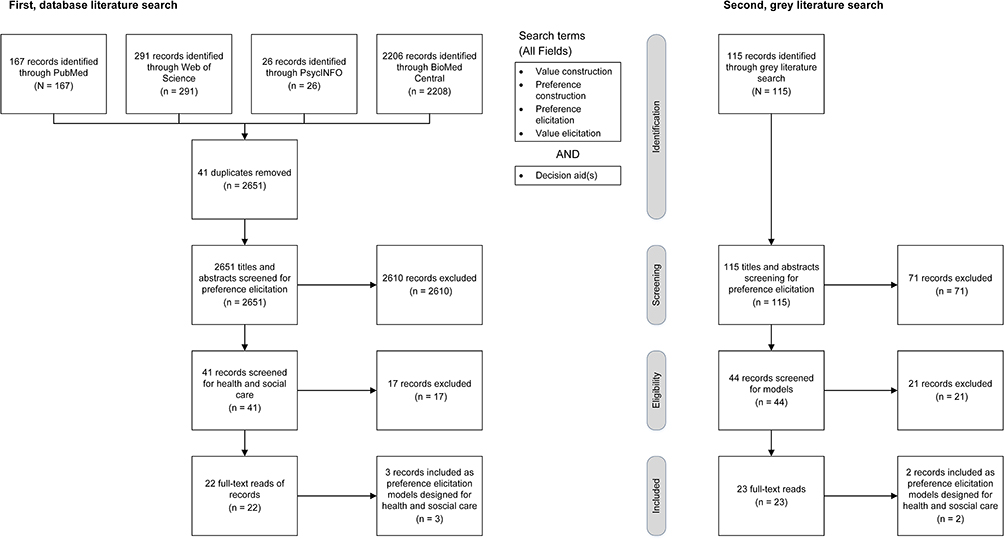 |
Figure 1 Literature search for records on preference elicitation and decision aids. Databases PubMed, Web of Science, PsycINFO, and BioMed Central were used. The search delivered 2651 records after duplicate removal, 2610 records were excluded due to lack of preference elicitation, and 17 records were excluded due to lack of use in healthcare. We included 22 records for full-text reading and further analysis. Three records were specifically on preference elicitation models for health and social care. The grey literature search delivered 115 records, 71 records were excluded based on screening for preference elicitation, and 21 records were excluded based on screening for models on preference elicitation. Twenty-three records were included for further analysis. Two records were specifically on preference elicitation models for health and social care. |
Second, a grey literature search was performed using the same search terms (Figure 1), including conference papers, reports and publications of governmental and non-governmental organizations, research institutes, Dutch care organizations, and Dutch insurance companies. An additional Google Web search was used to retrieve books, non-scientific research reports, information folders, and newsletters. Records not in English or Dutch were excluded. All records identified focused on preference construction and elicitation, and health and social care settings. There were no restrictions on publication date. A total of 115 titles and abstracts or summaries were screened for the reporting of preference elicitation, which led to the exclusion of 71 records. The remaining 44 records were screened for a model designed or used in health and social care settings to support preference elicitation. In all the included records, the authors stated that the model was applicable to health and social care settings. Ultimately, 23 records were included for full-text reading and analysis (Supplementary file 1).
Methods for Analysis
Three researchers performed the search. One reviewer took the first step and screened all records and together with the others, the final steps were performed. The literature search resulted in 45 records of which for full-text reading. Five of these records, three from the database search and two from the grey search, reported on a model for preference elicitation used in Dutch health and social care settings. The five records were analyzed using a qualitative inductive approach.33 An overview of the five models and all the domains within these models was created (Supplementary file 2). The definition and proposed content of each domain within the existing models was described, and all domains were compared with one another. Codes were created based on the definitions of the domains in the models. The comparison made it possible to analyze and group the domains.33 After the grouping process, all content was categorized and summarized into five overarching domains (Table 1). The overarching domains contain most of the domains of the five models. Only the domain quality of life was not included, because this was incorporated in all the five overarching domains.
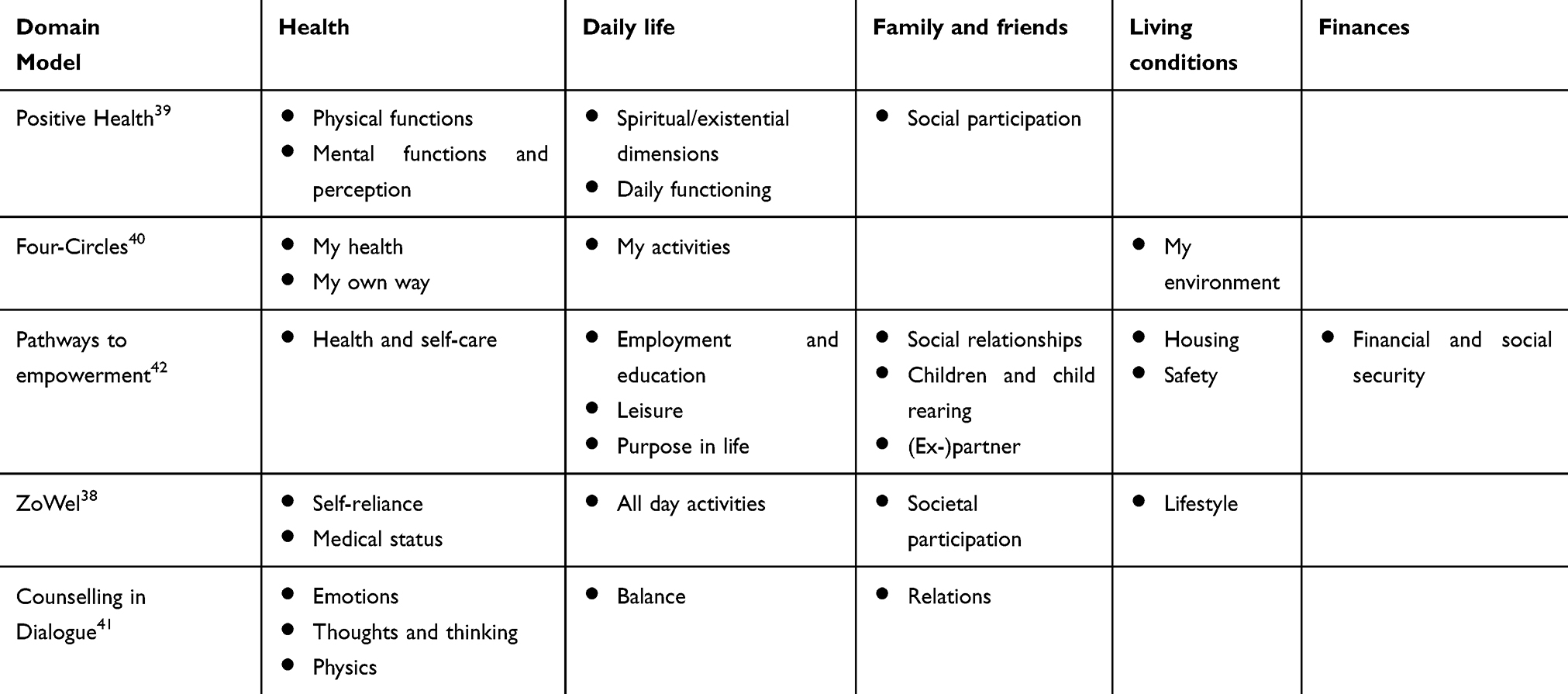 |
Table 1 The Five Models for the Elicitation of Preferences (First Column) Obtained from the Literature Overview and the Five Overarching Domains (First Row) Based on the Content of the Domains of the Models (Content of This Table) |
Qualitative Study
Qualitative research was performed to explore the decision-making process for long-term care, to answer the second research question. The matters that clients regard as important in long-term care and the sources clients use to acquire information about care were determined.10
Participants
Twelve long-term care organizations participated in this study. These organizations were divided over four care sectors in the Netherlands, ie, nursing and care of elderly, mental health care, care of people with disabilities, and social care. Two organizations were operational in the nursing and care of the elderly sector, four in the care of people with disabilities sector, one in the mental health care sector and two in the social care sector; three organizations provided care in all sectors. The participant group comprised equal numbers of males and females, and were aged between 20 and 93 years-old. Forty percent had never received an education or had a low educational level. The clients all used care from one of the long-term care organizations, and lived in a specialized care facility, or independently with homecare.
Ethical approval for this study was obtained from the Zuyderland Zuyd Ethics Committee (dossier-number 2015–1791). The participants were informed they could withdraw from the study at any time and gave written informed consent. Data were anonymized and data confidentiality was maintained. All files were anonymized by the care organizations in preparation for analysis.
Data Collection
The qualitative data were collected between September 2015 and July 2017. The data consisted of 16 interviews with clients, 3 focus groups (6 clients, 7 informal caregivers, and 11 care professionals), 79 client records,8 and 200 short online client reports from www.zorgkaartnederland.nl.
Four experienced researchers conducted in-depth semi-structured interviews and focus groups. Field notes were taken during the interviews and focus group meetings, and audiotapes were transcribed verbatim. The interviews and focus group meetings consisted of open-ended questions (Box 1). Seven clients from the client panels of care organizations reviewed the topic guide. They regarded the language as too difficult, and said questions addressing emotional issues were missing from the decision-making process. The researchers used the feedback to adjust the language and the emotional issues were addressed in the first and third questions of the topic guide. The interviews took place at the client’s home to ensure an environment that was comfortable. The interviews lasted between 30 and 60 minutes, the focus group meetings lasted approximately 90 minutes.
Box 1. Topic guide for the interviews and focus group discussions
- The current situation and phase of decision-making of the participant.
- The events, contacts, and issues crucial for the decision a client was making.
- The client’s need for support during the decision-making process.
- The fit of the actual choice with the client’s preferences.
The information sources the client used and the relevance of these sources.
The client records were selected from the databases of the included care organizations. The records comprised notes from care organizations, care logs, life or activity plans, and sometimes notes on consultations or arguments about decisions. The content of the records was comparable between the organizations and was a valid and rich source of information about elicitation of preferences. The same four researchers that conducted the interviews reviewed the client records.
The data sets were complemented with 200 short online client reports. Clients had written reports on their satisfaction with healthcare on the national patient portal of the Dutch federation of patient organizations (https://www.zorgkaartnederland.nl/), an online platform where clients of all sectors in health and social care share experiences about the care they have received by scoring qualitative indicators and sharing narratives. The presumption is that the experiences reported by these clients cover those issues that matter to them. These client reports were extracted from the database in July 2017. To represent the four care sectors in the Netherlands, 50 client reports were randomly selected from each sector.
Analysis
The qualitative data analysis followed a deductive approach33 to explore and determine all the preferences specifically for long-term care. In the preparation phase of the deductive approach choices for analysis were made.33 The notes and documented files in the client records and the written client reports were combined with the transcripts of the interviews and focus groups. All issues that matter most mentioned in any type of data were equal in the analysis. During the organizing phase,33 a structured analysis matrice was developed comprising the proposed overarching domains. The overarching domains were chosen to complement the literature overview with the qualitative data and define the content of the domains within the proposed framework.
Two researchers independently coded the transcript files of six interviews and one focus group, and the text files of six client records and twenty online client reports. The data coding of the researchers was compared and discussed. This comparison showed that all codes fitted within the five overarching domains. No other overarching domains were identified. Within each of the five overarching domains, the researchers identified the specific issues that matter most for clients in their search for appropriate tailor-made long-term care. One researcher coded all other data by the use of the list with the issues that matter most.
In the resulting phase,33 the findings were evaluated by the members of the research team during weekly meetings. Four client representatives reviewed the proposed framework. They discussed the content of the framework and the overarching domains. The researchers adjusted the framework on the basis of these discussions. The proposed framework was also discussed during an invitational conference with participants, clients, professionals, care organizations, and all others who had an interest in the project. Data saturation was reached when no new aspects that matter most emerged during data collection. It was reached after the 12 interviews and the 3 focus groups. Data management was performed using the NVivo version 11 software package.
Trustworthiness
To establish credibility,34 differing data collection methods were used (method triangulation), ie, a literature search, in-depth interviews, focus groups, client records, and online client reports. Two researchers performed the literature search and analyzed its results, and four researchers collected and analyzed the qualitative data. The data collection process was discussed at regular meetings. The data were read and analyzed in several steps to compare and discuss contrasting findings (investigator triangulation). As part of a member check, the proposed framework was first discussed with four client representatives. During the qualitative data analysis, they were asked to review the framework and provide feedback. They discussed the content and proposed names for the overarching domains covering the content in a meaningful way. The adjustments proposed by the client representatives were used to improve the proposed framework. The findings were then discussed during an invitational conference where the proposed framework was presented. Some participants, clients, professionals, employees of care organizations and others who had an interest in this research attended the conference.
Results and Findings
In this section, those models of preference construction and elicitation that were identified based on the literature are presented first (research question 1). The comparison of these models is presented and overarching domains are defined. Then the findings of the qualitative research define those issues that matter most for long-term care settings (research question 2). Lastly, the structure of a proposed framework for preference elicitation in long-term care, based on the literature overview and the qualitative research is given.
Five Models of Preference Elicitation
Most records in the literature overview consider those preference elicitation and decision aids aimed at ensuring a preference-guided decision to be single-disease-oriented.12,17,35 All records agree on the importance of preference elicitation and the discussion of preferences in consultations in order to strengthen SDM.31,36,37 However, most of these records do not derive on a model that is specifically designed for preference elicitation. The records include models designed to evaluate the goals, preferences, capabilities, values, or wishes in health and in life. From the 45 records obtained for the literature overview, five models were selected based on the use in health and social care and fitting the research aim, these were Positive Health, Four Circles, Pathway to Empowerment, ZoWel, Counselling in Dialogue.38–42
Although the underlying theories and concepts of the included models are based on international models, the models selected for further analysis were all Dutch. The choice to use the Dutch representation of the models was a practical one in order to propose a framework for Dutch clients. The five selected models are oriented to health and social care as a whole, and quality of life and the exploration of preferences; they can be used to explore the person behind the client with a health or social care need. All models aim to help the professionals and clients to identify and use the strengths of the client, and to support clients in their process of recovery. They can be used to gain insight into those preferences and desires that ultimately give meaning to someone’s life.
Huber’s model of Positive Health (in Dutch Positieve Gezondheid) is based on a new definition of health: “Health as the ability to adapt and to self-manage in the face of social, physical and emotional challenges.43” This model has potential as an instrument in decision-making in the hospital and other healthcare settings.39 Positive Health visualizes someone’s state of health by means of six domains: physical functions, mental functions and perception, spiritual/existential dimensions, quality of life, social participation, and daily functioning.39 Information on the content and definition of these domains is given in Supplementary file 2.
The Four Circles (in Dutch Vier bollen) model is based on the framework to assist goal setting of the “International Classification of Functioning Disability and Health” (ICF).40 The Four Circles model aims to assist the dialogue between client and professional in visualizing the desirable situation from the client’s perspective, starting from their perspective of personal capabilities. The client is supported in personal goal setting within four domains, ie, my health, my activities, my own way, and my environment,40,44(Supplementary file 2).Pathways to Empowerment (in Dutch Krachtwerk) is based on The Strengths model used in the United States45 This working methodology is based on the Social Quality Theory which discerns four constitutional factors that influence the quality of the daily lives of people, knowledge about determinants of social exclusion and inclusion, and the experiences of vulnerable, marginalized citizens, and involved professionals. Its purpose is to improve the social participation and self-direction of people who have difficulty holding their own in society.42 The working methodology has been applied in various target populations in differing health and social care sectors. The ten life domains of Pathways to Empowerment are those that clients consider as most important for a good life, ie, housing, employment and education, social relationships, children and child rearing, health and self-care, finances and social security, leisure, (ex-)partner, purpose in life, and safety,42 (Supplementary file 2). The ZoWel model is based on the difficulties clients experience during the search for care31 The intent of the model is to maximize personalized care and support by discussing domains that are influential on future care, and writing a personalized care plan based on those things that matter in the client’s life.38,46 The model contains five domains, ie, self-reliance, medical status, daily life activities, societal participation, and lifestyle (Supplementary file 2).
The model of Counselling in Dialogue (in Dutch Dialoogmodel) is based on cognitive, emotional, behavior, and social elements, and experiences in dialogues on retrospection, diagnostic findings, and treatment plan and policy agreements.41 The model focuses on mental health care and a client’s well-being from the point of view of treatment options, but it could also be used in other healthcare sectors to find more in-depth information about the client. This is done by visualizing the client’s context and their preferences.41,47 The five Counselling in Dialogue domains are relations, emotions, thoughts and thinking, physics, and balance41(Supplementary file 2).
Five Overarching Domains
The overview of the models showed that although each model has a different number of domains with different labels, the content of these domains is quite similar. In Four Circles, for example, the activities someone does or wants to do are discussed as “my activities” and in Pathway to Empowerment as “leisure” or in ZoWel as “all day activities”. The five overarching domains “Health”, “Daily life”, “Family and friend”, “Living conditions”, and “Finances” were determined by analyzing these five models. These domains were determined to cover elicitation on preferences in health and social care.
“Health” is defined as client’s care needs and their preferences on how to receive care. This domain helps clients identify to what extent they are self-reliant in providing their care, and in what areas they need assistance; it also includes preferences for care professionals. “Daily life” is defined as client’s preferences for all kinds of activities ranging from work to sport, and culture to religion. “Family and friends” is defined as the importance of relatives and all kind of social contacts. “Living conditions” is defined as client’s preferences regarding housing and environment as well as social interaction in their living environment. The last domain “Finances” is defined as financial resources and considers the role money or debts plays in life, and the preferences for assistance with finances or administration. The “Quality of Life” domain from the Positive Health model is the only domain that is not categorized within one single overarching domain. Other models do not have this domain as such, but quality of life is the central focus of preference elicitation in all models. The overarching five domains were the starting point to design a framework for preference elicitation in long-term care. To determine the content of each overarching domain specifically for long-term care, the qualitative data were used to explore all issues that matter to clients in need of long-term care.
Preference Elicitation in Long-Term Care: The Issues That Matter Most
Participants
The participants in the 16 interviews and three focus groups were 57% male and 43% female, between 20 and 93 years old. One third of them lived alone and the others lived with a partner or parents. Forty percent had never received education or had a low educational level. The interviews included seven clients in the nursing and care of the elderly sector, four clients in the care of people with disabilities sector, one client in the mental health care sector, and one client in the social care sector. Three clients received help from more than one care sector. Three interviews were held with the client alone, eight interviews with the client’s relatives, and five interviews with both the client and relative. One focus group was conducted with eight clients, one with six caregivers, and one with six relatives.
The 79 client records included 46% male and 54% female, and 47% lived in a specialized care facility and 53% lived independently. There were 23 clients in the nursing and care of the elderly sector, 20 clients in the care of people with disabilities sector, 10 clients in the mental health care sector, and 26 clients in the social care sector.
The 200 short online client reports were anonymized before sending to the researchers. Fifty reports were from clients in the nursing and care of the elderly sector, 50 from the care of people with disabilities sector, 50 from the mental health care sector, and 50 from the social care sector.
Health
In the domain “Health”, an issue that matters most to clients is preferred care, such as the capacities and self-reliance of a client, or the necessity of assistance in someone’s life. This assistance includes the different care options a client would prefer to receive in order to be able to participate in society. The importance of having a “click” with a care professional, to feel respected and the ability to build a trustworthy relationship was another aspect often mentioned by the participants. Other preferences for care were considered important, such as the gender and continuity of care professionals. Table 2 shows all “Health” aspects that matter most to clients in long-term care. These aspects include the preference for professionals, availability of care and staff, personalized treatment, and discussing the care plan and changes.
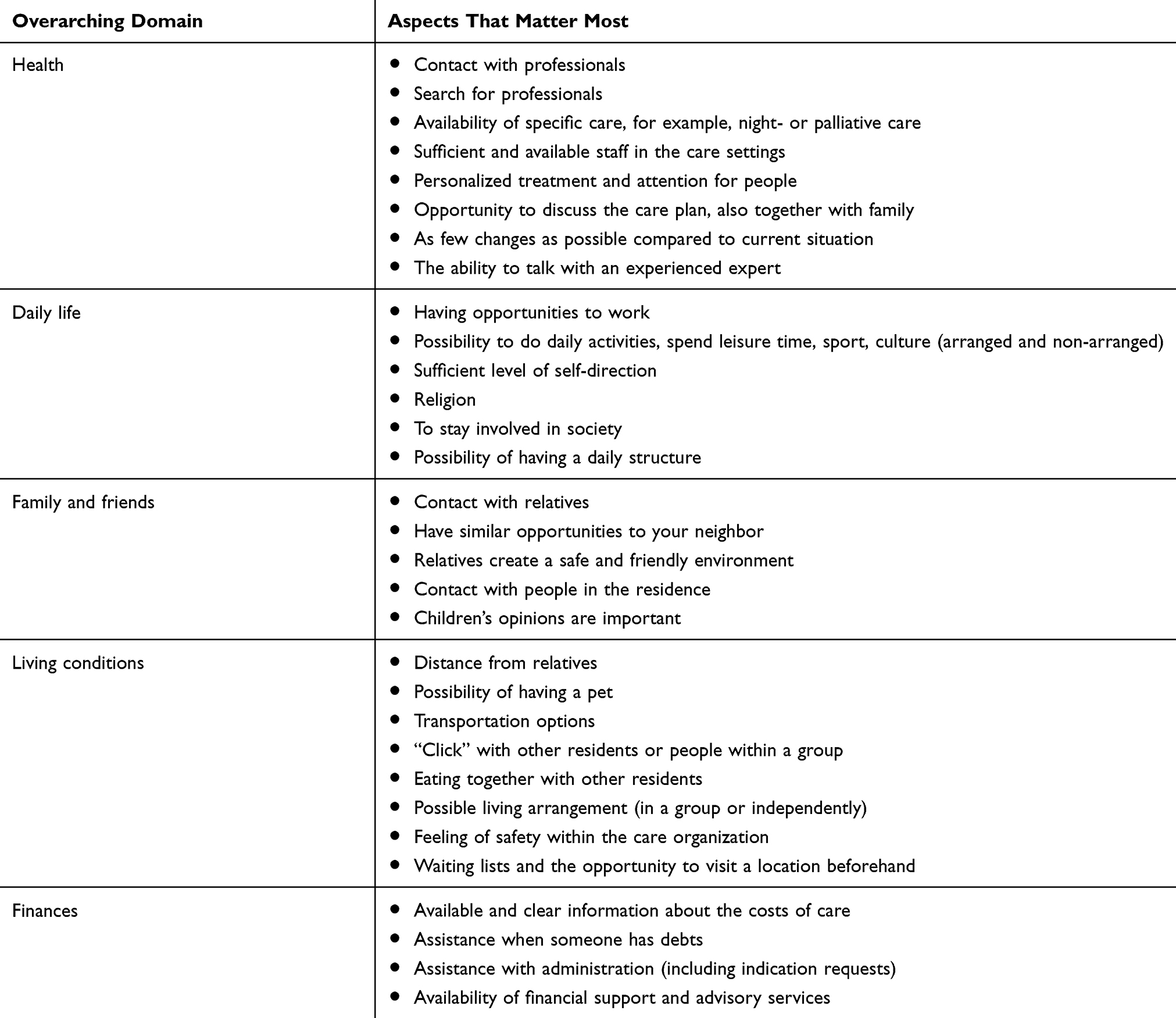 |
Table 2 The Five Overarching Domains Obtained from the Models in the Literature and the Corresponding Aspects That Matter Most Based on All Different Qualitative Data Sources |
Caregiver 2 (focus group): “I will call it physical support and mental support, which should give him the ability to take part in the society despite of his disabilities.”
Client 6 (focus group):
If I had to make the decision for myself, being able to arrange to receive palliative care would be something that appeals to me. Supposing my health were to deteriorate, or if I became incurably ill and there was no option for palliative care, I would have to move again.
Client 3 (interview):
This is very important. For example, say a care professional is assigned to you but you don’t ‘click’ with this person, it should be possible to switch to another care professional. If that wasn’t possible, I would want a transfer to another organization. For me this is very important, you need to feel supported when you tell your story. Without the ’click’, this will not work and you will not be helped.
Daily Life
All kinds of activities fitted into the domain “Daily life”. These activities range from work to all kinds of leisure time, sport, culture, and religion. For example, the parents of a child with several disabilities knew that their child liked working on a care farm, and they were searching for a location where this was possible. The aspects included in “Daily life” were daily structure, possibilities to work and do activities, religion, and involvement in society (Table 2).
Relative 1 (interview):
She has work/daytime activities at a care farm where she very much likes to go. We can tell because she jumps out of the car as soon as we arrive at the farm, and she is just very happy. She needs assistance to work, but she just likes to do it, for example she plants the beets all by herself and things like that.
Relative 5 (interview):
At that location, they have a care farm and apparently most people with disabilities like to go there. I immediately told them that it would not be an option for our son. This is not because I did not like it, but we have already experienced that our son does not like it. If they want to try, it is fine by us, but I do not think that it is somewhere he would like to go.
Family and Friends
The domain “Family and friends” includes meaningful social contacts in all aspects of life, often the clients want to stay close to family members, friends, neighbors or significant others in their network. Social contact and loved ones close-by create a safe environment. One of the most important aspects is the actual contact moments and time spent together with loved ones. Although most people do not want to be lonely, some just want to have people around to have a chat with them, whereas others are dependent on loved ones to do activities. To sum up, the aspects that matter most in the domain “Family and friends” include contact with relatives and friends, a friendly environment with loved ones, and children (Table 2).
Client 9 (interview): “Because I know a lot of people from my previous apartment building, I want to live in the same building as they have moved to.”
Relative 2 (interview):
It may also be possible that someone just visits him for company, listening to music or actually to do something like going to watch football, or going to a concert of his favorite music. Things like that.
“Living Conditions”
The domain “Living conditions” covers aspects of the living environment, housing, and lifestyle. When someone had to move to a long-term care facility, they often mentioned their preference to stay close to the neighborhood and to live in similar housing. The possibility of having a pet was also frequently mentioned. What also mattered to clients were characteristics of facilities, the location, room size, and safety within a residence. They expressed a desire to try living somewhere before the final decision was made. Overall the preferences were location, having a pet, transportation, “click” within a group and living arrangements, eating together with others, safety, and waiting lists (Table 2). In “Living conditions”, however, participant preferences varied a lot. Where one person preferred a large building with many facilities, others preferred a small but safe residence.
Client 14 (interview): “The most important to me were my personal preferences, indeed close to my home town and the animals. I wanted to keep my pet dog.”
Relative 1 (interview):
One of the most important aspects of the decision-making process was the location, as close to our current neighborhood as possible. We think that it will be most convenient for our daughter. […] If we live within walking distance from her, we could get there quickly. For example last week we had to take her to the dentist.
Relative 4 (focus group): “I found out that there was a small-scale residence. They will have more attention for the residents there, and that is something my mother prefers.”
Finances
Many participants agreed that financial issues such as having sufficient financial resources or being in debt played a role in the decision-making process. Participants prefer to have information about care costs, and assistance with debts when needed. Knowledge about receiving a refund or paying for the desired care services also belongs in the domain “Finances”. Furthermore, clients asked for assistance with their administration and budget (Table 2).
Client 7 (focus group):
They leave it to you to find out about it on your own. And then you discover that you won’t get a subsidy, and you will have to pay it all yourself. Then you are given a list of caregivers and wished the best of luck …
Client 1 (interview): “Yes, that care organization is now involved in assisting with the decision-making process, and even more with support in financial matters.”
Discussion
This study aimed to propose a framework for preference elicitation to facilitate collaborative deliberation on long-term care. Clients facing choices in long-term care and professionals responsible for coaching these clients in finding their way in long-term care are in need of assistance in preference elicitation during consultations. A communicative tool, such as OPT,21 will improve collaborative deliberation because it helps with preference-sensitive decision-making, enhances engagement of clients, and deepens the relationship with care professionals. A practical framework for client in long-term care to assist with preference elicitation would be beneficial. In this study, the proposed framework is based on a literature overview and qualitative data.
The first results (research question 1) are based on a literature overview of models designed to assist with preference elicitation in health and social care settings. Five models that focus on preference construction and elicitation were identified: Positive Health, Four Circles, Pathways to Empowerment, ZoWel, Counselling in Dialogue.38–42 These five models underlie the domains of the content of a framework for preference elicitation in long-term care: “Health”, “Daily life”, “Family and friends”, “Living conditions”, and “Finances”. The domains were obtained from the literature overview.
As well as the five models used in this study, there are a variety of models that focus mainly on preference elicitation in the areas of treatment, healthcare quality, and outcome of care.17,21,48-51 These models may assist preference elicitation regarding the development of a generalized care plan49 by prioritizing health outcomes,21 or by supporting decision-making in a new situation for clients with dementia.50,51 The literature overview shows that most models do not have an underlying framework of domains for preference elicitation in health and social care settings. Many of these models focus more on a specific population or on a specific underlying problem, and less on long-term care, or specifically on the preferences of individual clients. Other models have a focus on gaining insight into someone’s preference structure or scores for raking of preferences and courses of action.13,52 This might be done through bipolar scales,53 rank-dependent aggregation,54 or pairwise comparisons.55 These preference elicitation models were not taken into this study, because the aim was to identify overarching domains of preference elicitation within the existing models.
The second section of the results is based on the qualitative data to answer research question 2. The content of the five overarching domains was determined. Clients addressed issues that matter in their life, such as a “click” with their care professional, the safety of their living environment, residences close to loved ones, and assistance with daily structure and activities. These aspects were considered as the things that matter most in the lives of clients in long-term care and were taken as the content of the overarching domains of the proposed framework.
In comparison with issues included in most available models, long-term care preferences depend more on the personal, environmental, social, and cultural.21,56 This was confirmed in this study. The participants considered issues of care, as well as issues beyond care, to be things that matter in their lives. For example, “Daily life” deals with preferences for specific activities, but also preferences for the specific care that is needed to be enabled to undertake these activities. Clients mainly talked about the preferences beyond care, and when talking about these preferences, clients described them by using “everyday” indicators, including location, cleanliness, friendliness of the staff, comfortable furniture in the rooms, the feeling of being at home, and religious affiliation.57,58 These everyday indicators are important for clients in long-term care, due to their enduring impact on their daily lives. This shows the importance of including aspects that go beyond care in the framework. Including all these preferences will help engaging clients in a collaborative deliberative manner to decide on the preferred course of action based on their preferences.13
An important preference expressed by clients, which although part of care also goes beyond care, is trust in their care professionals and their situation. Clients want to build a relationship, especially with the person providing support during the decision-making process.59 Collaborative deliberation is beneficial in building a relationship and gaining mutual trust, especially by encouraging clients to talk and deliberate about preferences.1,31 However, preference elicitation on the spot during a consultation may delay the decision-making process due to emotional and unstable or imprecise responses.31,52 This study confirms the challenge of dealing with emotional responses in long-term care, as well as instability of preferences due to urgent care needs. These challenges may inhibit the discussion of aspects that matter most to the client. The translation of issues that matter into a practical framework for clients and their care professionals may overcome the barrier of delay in the decision-making process, and use of this framework in practice could improve collaborative deliberation, especially preference elicitation for long-term care.
Strengths and Weaknesses
Not performing an extensive systematic review could be regarded as a weakness of this study. However, an extensive overview of existing models for preference elicitation was obtained by the inclusion of the so-called grey literature. This seemed beneficial for this study since some models included in the proposed framework were found in these particular records. Although all records included in the proposed framework of this study were Dutch, the underlying theories and concepts of the included models in these records are based on international models. A large number of records consider preference elicitation in single-disease-oriented decision-making. Thus, a large number of records were excluded in this study because they focused on curative decision-making. A long-term care decision is usually a multi-faceted and complex decision, because the clients make decisions for care that has an impact on their quality of life on a daily basis.
A strength of this study is the combination of a literature overview and qualitative data to determine the content of the overarching domains specific to clients in need of long-term care. The overarching domains – proposed by analyzing the content of the five models from the literature overview – were confirmed by the qualitative data. Furthermore, the qualitative data consisting of interviews, focus groups, client records, and online client reports, were rich and represented the clients in need of long-term care. The presumption was that the experiences and the concerns the clients described are the aspects that matter most. A weakness is the missing personal information about the clients who wrote the online reports, because these were posted anonymously. Although specific information about the population was unavailable, it was known in which care sector the client received support. Furthermore, in addition to the interviews, focus groups, and client records, using the 200 online client reports gave more details about those issues that matter.
The proposed framework may improve collaborative deliberation by assisting the preference elicitation part of SDM, coping with preference-sensitive decisions, and building a trusting relationship.60 The framework may give clients and professionals a practical instrument to use in decision-making about long-term care since preferences occur during the whole process of decision-making.3 Further research is needed to explore recommendations for design and the feasibility of the use of such a framework in decision-making and its effects. It is recommended that the views of stakeholders on the development and use of the framework should be explored.4 Developing a framework that is acceptable to all stakeholders is something of a balancing act.4,61 Involving all stakeholders might overcome barriers to implementation by exploring the different views on the application and the use of the framework in practice.48 Strategies for implementation and the environment for implementation need to be explored in more depth in order to determine who the stakeholders are, and the current practices in which the framework could be used. It is necessary to include all stakeholders in follow-up research to develop this framework into a tool to engage clients in collaborative deliberation, and enhance the understanding and incorporation of preferences during the decision-making process.
Conclusion
This study proposes a framework to assist clients in need of long-term care during preference construction and elicitation in the decision-making process and search for preferred care. Based on a literature overview, five overarching domains were defined to explore client preferences, namely “Health”, “Daily life”, “Family and friends”, “Living conditions”, and “Finances”. Combined with qualitative data, the proposed content of the framework is specifically designed for clients in their search for tailor-made long-term care. This qualitative data strongly supported the five overarching domains. Further study is needed to validate the content and feasibility of the proposed framework. This practical framework is designed for preference construction and elicitation in long-term care practice, to support collaborative deliberation in consultations between clients and care professionals.
Abbreviations
HTA, Health Technology Assessment; ICF, International Classification of Functioning Disability and Health; OPT, Outcome Prioritization Tool; SDM, Shared Decision-Making.
Data Sharing Statement
All relevant data are in the manuscript and its supporting information files. The dataset that supports the findings and conclusion of this study is available from the corresponding author on reasonable request. The data are not publicly available due to privacy and/or ethical restrictions.
Ethics Approval and Informed Consent
Ethical approval for this study was obtained from the Zuyderland Zuyd Ethics Committee (dossier-number 2015-1791). The participants were informed they could withdraw from the study at any time and gave written informed consent. Data were anonymized and data confidentiality was maintained. All files were anonymized by the care organizations in preparation for analysis.
Acknowledgments
The authors wish to thank all participants for their contribution to this research. The authors thank Renee de Vet (RdV), Tessa van Loenen (TvL), Marjan Faber (MF), and Miriam Harmsen (MH), employees of Radboud University Medical Center, IQ Healthcare, Impuls, Nijmegen, The Netherlands, for their contribution to the data collection. The authors also thank Silvia Bours as a research assistant of University Maastricht for her contribution during the data analysis.
Author Contributions
All authors made substantial contribution to conception and design, acquisition of data, or analysis and interpretation of data. All took part in drafting the article or revising it critically for important intellectual content. All gave final approval of the version to be published, and all agree to be accountable for all aspects of the work.
Disclosure
Trudy van der Weijden reports grants from Dutch Institute of Health Services Research, during the conduct of the study. The authors report no other potential conflicts of interest for this work.
References
1. Elwyn G, Lloyd A, May C, et al. Collaborative deliberation: a model for patient care. Patient Educ Couns. 2014;97(2):158–164. doi:10.1016/j.pec.2014.07.027
2. Elwyn G, Cochran N, Pignone M. Shared decision making – the importance of diagnosing preferences. JAMA Intern Med. 2017;177(9):1239–1240. doi:10.1001/jamainternmed.2017.1923
3. Llewellyn-Thomas HA, Crump RT. Decision support for patients: values clarification and preference elicitation. Med Care Res Rev. 2013;70(1 Suppl):50S–79S. doi:10.1177/1077558712461182
4. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
5. Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891. doi:10.1136/bmj.j4891
6. Utens CMA, Dirksen CD, van der Weijden T, Joore MA. How to integrate research evidence on patient preferences in pharmaceutical coverage decisions and clinical practice guidelines: a qualitative study among Dutch stakeholders. Health Policy (New York). 2016;120(1):120–128. doi:10.1016/j.healthpol.2015.10.005
7. Dai XC, Brendl CM, Ariely D. Wanting, liking, and preference construction. Emotion. 2010;10(3):324–334. doi:10.1037/a0017987
8. van Leersum CM, Moser A, van Steenkiste B, Wolf J, van der Weijden T. Getting to grips with the process of decision-making in long-term care. Descriptive cases illustrate the chaotic reality of the construction of preferences. PLoS One. 2019;14(5):e0217338. doi:10.1371/journal.pone.0217338
9. Warren C, McGraw AP, Van Boven L. Values and preferences: defining preference construction. Wiley Interdiscip Rev Cogn Sci. 2011;2(2):193–205. doi:10.1002/wcs.98
10. Borcherding K, Schmeer S, Weber M. Biases in multiattribute weight elicitation. In: Contributions to Decision Making - I. 1995:3–28.
11. Feldman-Stewart D, Brundage MD, Van Manen L, Svenson O. Patient-focussed decision-making in early-stage prostate cancer: insights from a cognitively based decision aid. Health Expect. 2004;7(2):126–141.
12. Jayadevappa R, Chhatre S, Gallo JJ, et al. Treatment preference and patient centered prostate cancer care: design and rationale. Contemp Clin Trials. 2015;45(Pt B):296–301. doi:10.1016/j.cct.2015.09.024
13. Crump T, Llewellyn-Thomas HA. Assessing Medicare beneficiaries’ strength-of-preference scores for health care options: how engaging does the elicitation technique need to be? Health Expect. 2011;14(Suppl 1):33–45. doi:10.1111/j.1369-7625.2010.00632.x
14. Lichtenstein S, Slovic P. The Construction of Preferences: An Overview.
15. Murray MA, Wilson K, Kryworuchko J, Stacey D, O’Connor A. Nurses’ perceptions of factors influencing patient decision support for place of care at the end of life. Am J Hosp Palliat Care. 2009;26(4):254–263. doi:10.1177/1049909108331316
16. Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70(4):351–379. doi:10.1177/1077558712465774
17. Kaiser K, Beaumont JL, Webster K, et al. Development and validation of the functional assessment of cancer therapy-antiangiogenesis subscale. Cancer Med. 2015;4(5):690–698. doi:10.1002/cam4.385
18. Turnpenny A, Beadle-Brown J. Use of quality information in decision-making about health and social care services – a systematic review. Health Soc Care Comm. 2015;23(4):349–361. doi:10.1111/hsc.12133
19. O’Connor AM, Fiset V, DeGrasse C, et al. Decision aids for patients considering options affecting cancer outcomes: evidence of efficacy and policy implications. J Natl Cancer Inst Monogr. 1999;1999(25):67–80. doi:10.1093/oxfordjournals.jncimonographs.a024212
20. Fagerlin A, Pignone M, Abhyankar P, et al. Clarifying values: an updated review. BMC Med Inform Decis Mak. 2013;13(Suppl 2):S8. doi:10.1186/1472-6947-13-S2-S8
21. van Summeren JJ, Schuling J, Haaijer-Ruskamp FM, Denig P. Outcome prioritisation tool for medication review in older patients with multimorbidity: a pilot study in general practice. Br J Gen Pract. 2017;67(660):e501–e506. (). doi:10.3399/bjgp17X690485
22. McCall N. Long term care: definition, demand, cost, and finance. In: McCall N, editor. Who Will Pay for Long Term Care?: Insights from the Partnership Programs. University of Michigan: Health Administration Press; 2001:3–31.
23. Kane RA. Long-term care and a good quality of life: bringing them closer together. Gerontologist. 2001;41(3):293–304. doi:10.1093/geront/41.3.293
24. Carter G, van der Steen JT, Galway K, Brazil K. General practitioners’ perceptions of the barriers and solutions to good-quality palliative care in dementia. Dementia. 2015;2.
25. Hansen H. Managing to beat death: the narrative construction process. J Organ Change Manag. 2011;24(4):442–463. doi:10.1108/09534811111144610
26. Janus SI, Weernink MG, van Til JA, Raisch DW, van Manen JG. A systematic review to identify the use of preference elicitation methods in health care decision making. Value Health. 2014;17(7):A515–A516. doi:10.1016/j.jval.2014.08.1596
27. Constand MK, MacDermid JC, Dal Bello-Haas V, Law M. Scoping review of patient-centered care approaches in healthcare. BMC Health Serv Res. 2014;14(1):271. doi:10.1186/1472-6963-14-271
28. Vermunt N, Elwyn G, Westert G, Harmsen M, Olde Rikkert M, Meinders M. Goal setting is insufficiently recognised as an essential part of shared decision-making in the complex care of older patients: a framework analysis. BMC Fam Pract. 2019;20(1):76. doi:10.1186/s12875-019-0966-z
29. van Bon J. IT Service Management Best Practices. Vol. 4. ‘s-Hertogenbosch: Van Haren Publishing; 2007.
30. Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research.
31. de Vries M, Fagerlin A, Witteman HO, Scherer LD. Combining deliberation and intuition in patient decision support. Patient Educ Couns. 2013;91(2):154–160. doi:10.1016/j.pec.2012.11.016
32. Hordern A, Georgiou A, Whetton S, Prgomet M. Consumer e-health: an overview of research evidence and implications for future policy. Health Inf Manag. 2011;40(2):6–14. doi:10.1177/183335831104000202
33. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
34. Lincoln YS, Guba EG. Naturalistic Inquiry. Newsbury Park: CA: SAGE Publications; 1985.
35. Gray J, Lie ML, Murtagh MJ, Ford GA, McMeekin P, Thomson RG. Health state descriptions to elicit stroke values: do they reflect patient experience of stroke? BMC Health Serv Res. 2014;14(1):573. doi:10.1186/s12913-014-0573-6
36. Cabri J, Pollard M, Pena A, et al. Impact of a decision aid and preference assessment on urolithiasis patient decision making. J Urology. 2018;199(4):. doi:10.1016/j.juro.2018.02.2356
37. Henselmans I, Van Laarhoven HW, Van der Vloodt J, De Haes HC, Smets EM. Shared decision making about palliative chemotherapy: a qualitative observation of talk about patients’ preferences. Palliat Med. 2017;31(7):625–633. doi:10.1177/0269216316676010
38. CZ. ZoWel Model. CZnl Alles Voor Betere Zorg. 2013;1.
39. Huber M, van Vliet M, Giezenberg M, et al. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: a mixed methods study. BMJ Open. 2016;6(1):e010091. doi:10.1136/bmjopen-2015-010091
40. Lenzen SA, Daniels R, van Bokhoven MA, van der Weijden T, Beurskens A. Development of a conversation approach for practice nurses aimed at making shared decisions on goals and action plans with primary care patients. BMC Health Serv Res. 2018;18(1):891. doi:10.1186/s12913-018-3734-1
41. Westermann GM, Verheij F, Winkens B, Verhulst FC, Van Oort FV. Structured shared decision-making using dialogue and visualization: a randomized controlled trial. Patient Educ Couns. 2013;90(1):74–81. doi:10.1016/j.pec.2012.09.014
42. Wolf JRLM. Kracthwerk: Methodisch Werken Aan Participatie En Zelfregie.
43. Huber M, Knottnerus JA, Green L, et al. How should we define health? BMJ. 2011;343(jul26 2):d4163. doi:10.1136/bmj.d4163
44. Lenzen SA, Daniels R, van Bokhoven MA, van der Weijden T, Beurskens A. Setting goals in chronic care: shared decision making as self-management support by the family physician. Eur J Gen Pract. 2015;21(2):138–144. doi:10.3109/13814788.2014.973844
45. Rapp CA, Goscha RJ. The Strengths Model. A Recovery-Oriented Approach to Mental Health Services.
46. CZ. Evaluatierapportage ZoWel Model. CZnl Alles Voor Betere Zorg. 2016.
47. Maurer J, Westermann G. Beter Communiceren in De Hulpverlening: Het Dialoogmodel Als Leidraad. Houten: Bohn Stafleu van Loghum; 2007.
48. Virues-Ortega J, Pritchard K, Grant RL, et al. Clinical decision making and preference assessment for individuals with intellectual and developmental disabilities. Ajidd-Am J Intellect. 2014;119(2):151–170.
49. Vlek H. Plan van eigen generiek Individueel ZorgPlan. Vilans. 2014;1:2546.
50. Span M, Smits C, Groen-van de Ven L, et al. Towards an interactive web tool that supports shared decision-making in dementia: identifying user requirements. Int J Adv Life Sci. 2014;6:
51. Span M, Smits C, Jukema J, et al. An interactive web tool for facilitating shared decision-making in dementia-care networks: a field study. Front Aging Neurosci. 2015;7.
52. Mousseau V, Pirlot M. Preference elicitation and learning. Euro J Decis Process. 2015;3(1–2):1–3. doi:10.1007/s40070-015-0044-2
53. Rolland A, Ah-Pine J, Mayag B. Elicitation of 2-additive bi-capacity parameters. Euro J Decis Process. 2015;3(1–2):5–28. doi:10.1007/s40070-015-0043-3
54. Benabbou N, Gonzales C, Perny P, Viappiani P. Minimax regret approaches for preference elicitation with rank-dependent aggregators. Euro J Decis Process. 2015;3(1–2):29–64. doi:10.1007/s40070-015-0040-6
55. Labreuche C, Mayag B, Duqueroie B. Extension of the MACBETH approach to elicit an ordered weighted average operator. Euro J Decis Process. 2015;3(1–2):65–105. doi:10.1007/s40070-015-0041-5
56. Lehnert T, Heuchert M, Hussain K, König H. Stated Preferences for Long-Term Care: A Literature Overview. Ageing & Society Cambridge University Press; 2018.
57. Castle NG. Searching for and selecting a nursing facility. Med Care Res Rev. 2003;60(2):223–247. doi:10.1177/1077558703060002005
58. Davies S, Nolan M. ‘Making the best of things’: relatives’ experiences of decisions about care-home entry. Ageing Soc. 2003;23:429–450. doi:10.1017/S0144686X03001259
59. Baxter K, Glendinning C. Making choices about support services: disabled adults’ and older people’s use of information. Health Soc Care Community. 2011;19(3):272–279. doi:10.1111/j.1365-2524.2010.00979.x
60. Witt J, Elwyn G, Wood F, Brain K. Decision making and coping in healthcare: the Coping in Deliberation (CODE) framework. Patient Educ Couns. 2012;88(2):256–261. doi:10.1016/j.pec.2012.03.002
61. Li LC, Adam PM, Townsend AF, et al. Usability testing of ANSWER: a web-based methotrexate decision aid for patients with rheumatoid arthritis. BMC Med Inform Decis Mak. 2013;13(1):131. doi:10.1186/1472-6947-13-131
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.