Back to Archived Journals » Transplant Research and Risk Management » Volume 14
Prophylaxis of Cytomegalovirus Infection in Solid Organ Transplantation, Retrospective Evaluation
Authors Albekairy AM, Shawaqfeh MS ![]() , Alharbi SH, Almuqbil F, Alghamdi MA, Albekairy NA, Muflih SM
, Alharbi SH, Almuqbil F, Alghamdi MA, Albekairy NA, Muflih SM ![]() , Alkatheri A
, Alkatheri A
Received 16 March 2022
Accepted for publication 12 May 2022
Published 7 June 2022 Volume 2022:14 Pages 35—45
DOI https://doi.org/10.2147/TRRM.S366213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qing Yi
Abdulkareem M Albekairy,1– 3 Mohammad S Shawaqfeh,1,2 Shroug H Alharbi,3,4 Faisal Almuqbil,1,2 Mesfer A Alghamdi,3,5 Nataleen A Albekairy,6 Suhaib M Muflih,7 Abdulmalik Alkatheri1– 3
1Department of Pharmacy Practice, College of Pharmacy, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Pharmaceutical Care Department, King Saud Medical City, Riyadh, Saudi Arabia; 4King Faisal Specialist Hospital and Research center, Jeddah, Saudi Arabia; 5Clinical Pharmacy Department, King Saud Medical City, Riyadh, Saudi Arabia; 6College of Medicine, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 7Department of Clinical Pharmacy, College of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Abdulkareem M Albekairy, Department of Pharmacy Practice, College of Pharmacy, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia, Tel +966 11-4295001, Email [email protected]; [email protected]
Introduction: Cytomegalovirus infection is one of the opportunistic infections that occur within the first year of solid organ transplantation (SOT). Antiviral prophylaxis like valganciclovir is recommended for organ transplant recipients if the donors are seropositive. The study aims to assess the association between compliance with CMV prevention guidelines and the incidence of CMV infection post kidney and liver transplantation.
Methods: A single-center, cross-sectional chart review study was conducted at a tertiary care facility. The study included patients with liver and/or kidney transplantation and received valganciclovir for CMV prevention. The primary endpoint is to determine the incidence of CMV post SOT. The secondary endpoint is to assess the association between compliance with the CMV prevention guidelines and the incidence of CMV infection. Descriptive statistics were used to report the incidence of CMV and logistic regression for risk factor comparisons. The study was approved by the Institutional Review Board.
Results: A total of 493 patients had a mean age of 48.6 ± 15.3 years were included. For the primary endpoint, there were a total of 257 patients with CMV occurrence (52.1%). For the secondary endpoint, there was no statistically significant association between CMV incidence and starting CMV prophylaxis agent post-transplantation within 10 days post-transplant (p < 0.75) and duration of CMV prophylactic medications (p < 0.47). In this study, the cases of CMV disease that occurred within 3– 6 months following completion of antiviral prophylaxis were in 28% of the patients. Other factors associated with increased risk of CMV infection were evaluated.
Conclusion: We found about 28% of CMV infection cases occurred within 3– 6 months following completion of antiviral prophylaxis. This was attributed to non-adherence to prophylaxis guidelines. The study has shown that there is a need for improvement in clinical practice. Future studies should address the optimal duration of the CMV prophylaxis.
Keywords: Cytomegalovirus, prophylaxis, solid-organ transplantation
Introduction
Solid Organ Transplantation (SOT) is a life-saving procedure for many patients with end-stage organ diseases.1 Many complications can happen after SOT ranging from less serious to very sophisticated complications. The use of immunosuppressive therapy after SOT can cause infectious and non-infectious complications. Infectious complications after SOT mainly include bacterial, fungal infections, and viral infections (Cytomegalovirus, hepatitis B, and hepatitis C). However, non-infectious complications after SOT may include cardiovascular disorders, such as diabetes mellitus, dyslipidemia, and hypertension. Immunological complications such as acute rejection, chronic rejection, post-transplant lymphoproliferative disease, and renal impairment can be considered non-infectious complications.2–6 Cytomegalovirus is known to be the most common opportunistic infection that may occur within the first year of solid organ transplantation. The pre-transplant CMV serology status is the most prevalent measure that can evaluate the occurrence of CMV. The accounted seroprevalence rate of CMV in the USA is 50% compared to 30–97% outside the USA. The major risk factor to develop CMV is allograft rejection, specifically when the affected patients are treated with lymphocyte-depleting agents. Also, the use of high doses of maintenance immunosuppressive therapy may increase the risk of developing CMV after SOT.7–9 According to the American Society of Transplantation, CMV infection is defined as the presence of CMV replication in tissue, blood, or other bodily fluids regardless of symptomatology.10,11 While the definition of CMV disease is CMV infection that is accompanied by clinical signs and symptoms. CMV disease is categorized into CMV syndrome and end-organ CMV disease (eg, gastrointestinal disease, pneumonitis, hepatitis, nephritis, myocarditis, pancreatitis, encephalitis, retinitis, others).10,11
The American Society of Transplantation established a risk category for CMV prevention after SOT based on their serology of donors and recipients. Two approaches had been established to prevent CMV after SOT including antiviral prophylaxis and preemptive therapy.12–14
According to AST, the recommendations for CMV prevention, particularly after kidney and liver transplantation, for CMV D−/R− SOT recipient antiviral prophylaxis are not recommended. However, antiviral prophylaxis is recommended for CMV D−/R+, for 3 months for both kidney and liver SOT recipients. Also, for CMV D+/R− antiviral prophylaxis is recommended, and the duration of antiviral prophylaxis is 3 to 6 months for liver SOT recipients. However, the duration of antiviral prophylaxis must be at least 6 months in kidney transplantation recipients. The antiviral drug regimens approved for the prevention of CMV are Valganciclovir (900 mg PO once daily) and Ganciclovir (5mg/kg/day intravenous). Valganciclovir is the preferred first choice as prophylaxis for CMV.15–18 To detect CMV after SOT, the best-recommended strategy is the use of molecular assays (CMV QNAT), which provide rapid diagnosis of CMV, aid in the initiation of antiviral therapy, and help to monitor treatment responses.19 The preferred antiviral drugs approved for the treatment of CMV are Ganciclovir (5 mg/kg twice daily intravenous) and Valganciclovir (900 mg PO twice daily). Other second-line choices for the treatment of CMV resistance are Foscarnet and Cidofovir which are highly nephrotoxic. Ganciclovir is the preferred choice for the initial treatment of life-threatening CMV.20–22 The duration of antiviral drugs should be continued until achieving the clearance of clinical symptoms, virological clearance, and at least two weeks of antiviral treatment have been given.15,22,23 Many studies had been conducted to evaluate the adherence to the recommendation in the guidelines that were compared to clinical practice in many centers from a prospective point of view of the prophylaxis and treatment doses of CMV. In our study, the primary endpoint is used to determine the incidence of CMV post SOT. The secondary endpoint is to assess the association between compliance with the CMV prevention guidelines and the incidence of CMV infection.
Methods
A single-center, retrospective chart review study was conducted at a tertiary care facility. The study included all patients ≥18 years with liver, kidney, or combined kidney/liver transplantation who were admitted over the past five years (2016–2020) and received Valganciclovir for CMV prevention. Other organ transplant patients and pediatrics were excluded. The data collection includes demographic information like age, gender, transplantation type, type of transplantation, and transplanted organ. The clinical variables like donor and recipient CMV status were also included. The induction therapy, as well as acute cellular rejection, was collected. CMV prophylaxis detailed information was also recorded.
Descriptive statistics were used to report the incidence of CMV and all continuous variables. Logistic regression to evaluate the risk factor associations with CMV incidence.
The univariate analysis evaluated all variables associated with increased incidence of CMV infection (ie, age, gender, type of organ, type of transplant, type of induction therapy, the timing of receiving CMV prophylaxis, and patient risk of CMV). After completing univariate logistic regression, the statistically significantly associated variables, as well as variables with p-value <0.25, were included in the multiple logistic regression model.
A simple logistic regression model was then used to identify the factors associated with the development of CMV among transplant patients. The adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were established. The statistical significance was set as α=0.05. All statistical analyses were performed using Statistical Package for Social Sciences version 24.0 (SPSS 24.0).
Ethical Approval
The study was approved by King Abdullah International Medical Research Center’s Institutional Review Board, Riyadh, Saudi Arabia (Approval number: KAIMRC RC20/284/R). The study is a retrospective evaluation of included patient medical records, and the patient's consent was exempted as there will be no intervention and the data collection and management were approved by the IRB. Patient confidentiality and privacy were maintained according to ethical standards and research conduct principles and the guidelines outlined in the Declaration of Helsinki were followed. According to the Saudi Ministry of Health, living organ donation is limited strictly to first-degree relatives and this issue is highly regulated. The authors confirm that all organs were donated voluntarily with written informed consent and that this was conducted in accordance with the Declaration of Istanbul.
Results
Table 1 summarizes all the demographics of the study sample population. The study included 493 patients, 293 (59.4%) were male. The average mean age was 48.6 ± 15.3 (Range: 18–87). There 359 (72.8%) were kidney transplanted organ types. Out of 493 patients, 345 (70%) were living donors, and 146 (30%) were deceased donors. There were 482 (97.8%) positive donor CMV IgG, and 453 (91.9%) were positive recipient CMV IgG. These patients were categorized according to the recipient CMV risk. CMV risk is high when there is a serological mismatch between the donor and the recipient (the recipient is CMV seronegative and the donor is seropositive), (CMV D+/R-). If the recipient is CMV seropositive and the donor is either seropositive or seronegative (CMV D+/R+ CMV D-/R+), it is considered a moderate risk for the development of CMV infection. If both recipient and donor are CMV seronegative (CMV D-/R-), it is considered low risk for the development of CMV infection.
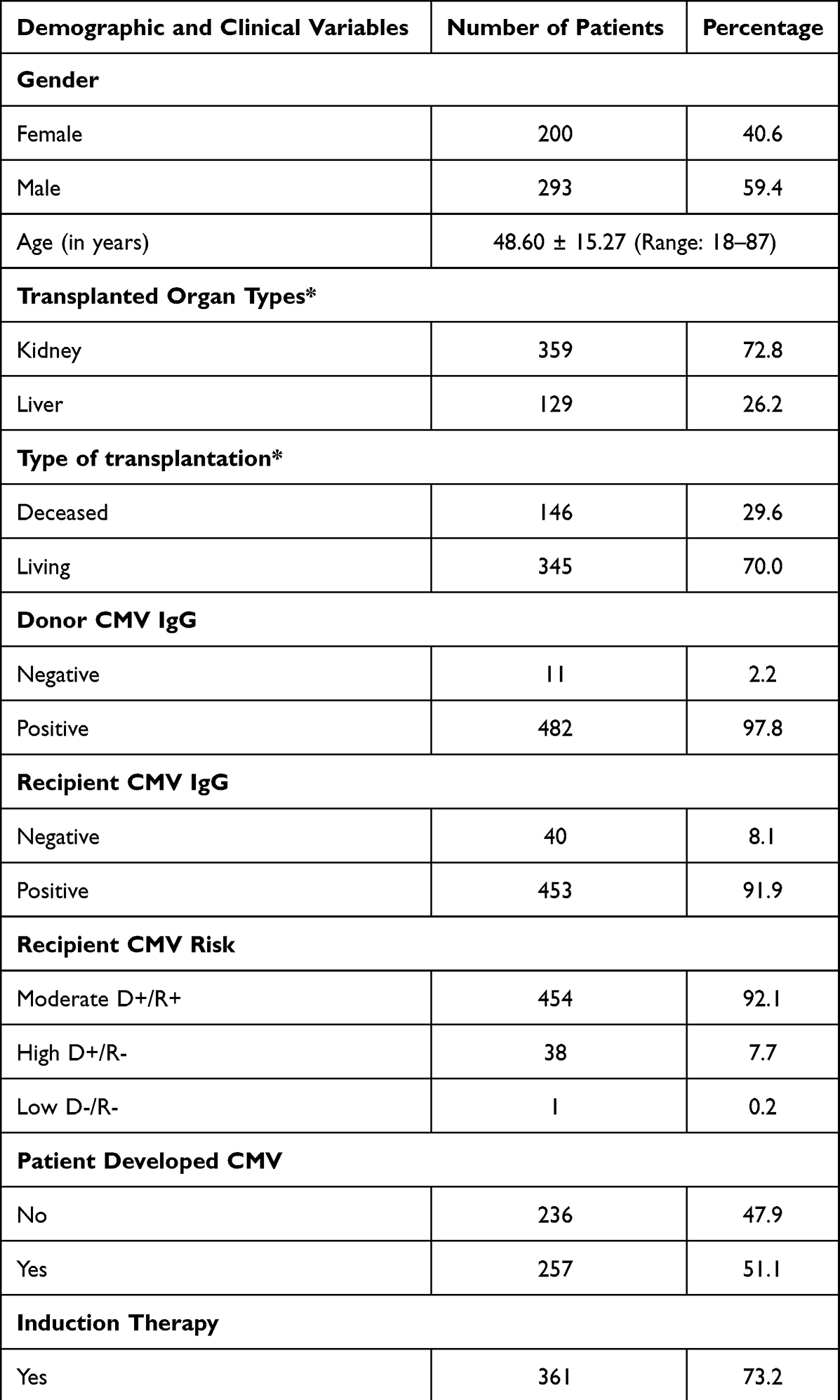 |
Table 1 Distribution of Demographic and Clinical Variables Among Patients (N = 493) |
The majority, 453 (92.1%), was moderate recipient CMV risk, and only 39 (7.9%) was high recipient CMV risk. There was a total of 257 (52.1%) patients who developed CMV infection. Out of 257 CMV patients, there were 235 (91.4%) had CMV infection and only 22 (8.6%) had CMV disease, there were 361 (73.2%) patients who received induction treatment before transplantation. There were 190 (52.6%) patients who received the interleukin-2 antagonist Basiliximab (BMX) as induction therapy and 171 (47.4%) patients who received Antithymocyte Globulin (ATG). Only 35 patients (7.1%) developed acute cellular rejection, while most of the patients 458 (92.9%) did not. The distribution of these CMV infections were distributed over time as follows: (0–3 months; 20.2%, 3–6 months; 27.6%, 6–12 months; 38.1%, 12–24 months; 9.7%, 24–36 months; 4.3%).
Table 2 There were 363 patients (73.6%) who started CMV prophylaxis that is based on oral valganciclovir 450 mg. Surprisingly, there were 130 patients (26.4%) who did not receive any prophylaxis. Out of those who received prophylaxis there were 332 patients (67.3%) who started prophylactic medications within 10 days according to guideline recommendations. The rest started with prophylaxis but rather later than 10 days (n = 31, 6.3%). These patients who received late start prophylaxis were 19 patients within 11 to 29 days from transplantation and 12 within 30 to 60 days.
 |
Table 2 Cytomegalovirus Prophylaxis Among Patients with Solid Organ Transplantation |
Table 3 shows the CMV treatment variables for solid organ transplantation. There was a total of 257 patients (52.1%) who developed CMV disease (n = 22, 6.8%) and CMV infection (n = 235, 91.4%). There were only 47 patients (18.3%) who were eligible for CMV treatment according to the treatment guidelines. These patients’ severity ranges from asymptomatic (n = 25, 9.7%), to mild-moderate (n = 17, 6.6%), to Severe/Life-threatening (n = 5, 1.9%). Furthermore, only 29 patients (11.3%) were initiated the CMV treatment; however, 6 patients’ dosages (2.3%) were not adjusted appropriately according to renal dosing guidelines. The median PCR CMV DNAemia count was 44 (IU/mL), IQR: (19.0–322.50). Table 3 summarizes all treatment-related results.
 |
Table 3 Cytomegalovirus Treatment Among Solid Organ Transplantation (N = 257) |
The total incidence of CMV infection and disease among various risk factors was obvious in the high recipient CMV risk group 66.7% in comparison to the moderate CMV recipient risk group 50.9%. The living donor transplant CMV incidence was 54.5% vs 45.9% in the deceased transplantation group. The incidence of CMV was notably higher in patients who developed rejection (97.7%) compared to only 10% incidence of CMV in patients who did not develop any acute cellular rejection episode. In addition, we observed higher chances of developing CMV disease or infection in around 65% of the recipients who still received mycophenolate mofetil and prednisone when they stopped antiviral prophylactic treatment.
The total incidence of CMV infection and disease among kidney transplant patients was higher than liver transplant patients (64.6% vs 17.8%), respectively. Similarly, the total CMV incidence was higher with Antithymocyte Globulin (ATG) induction (70.7%) than that with Basiliximab induction therapy (46.3%), as shown in Table 4.
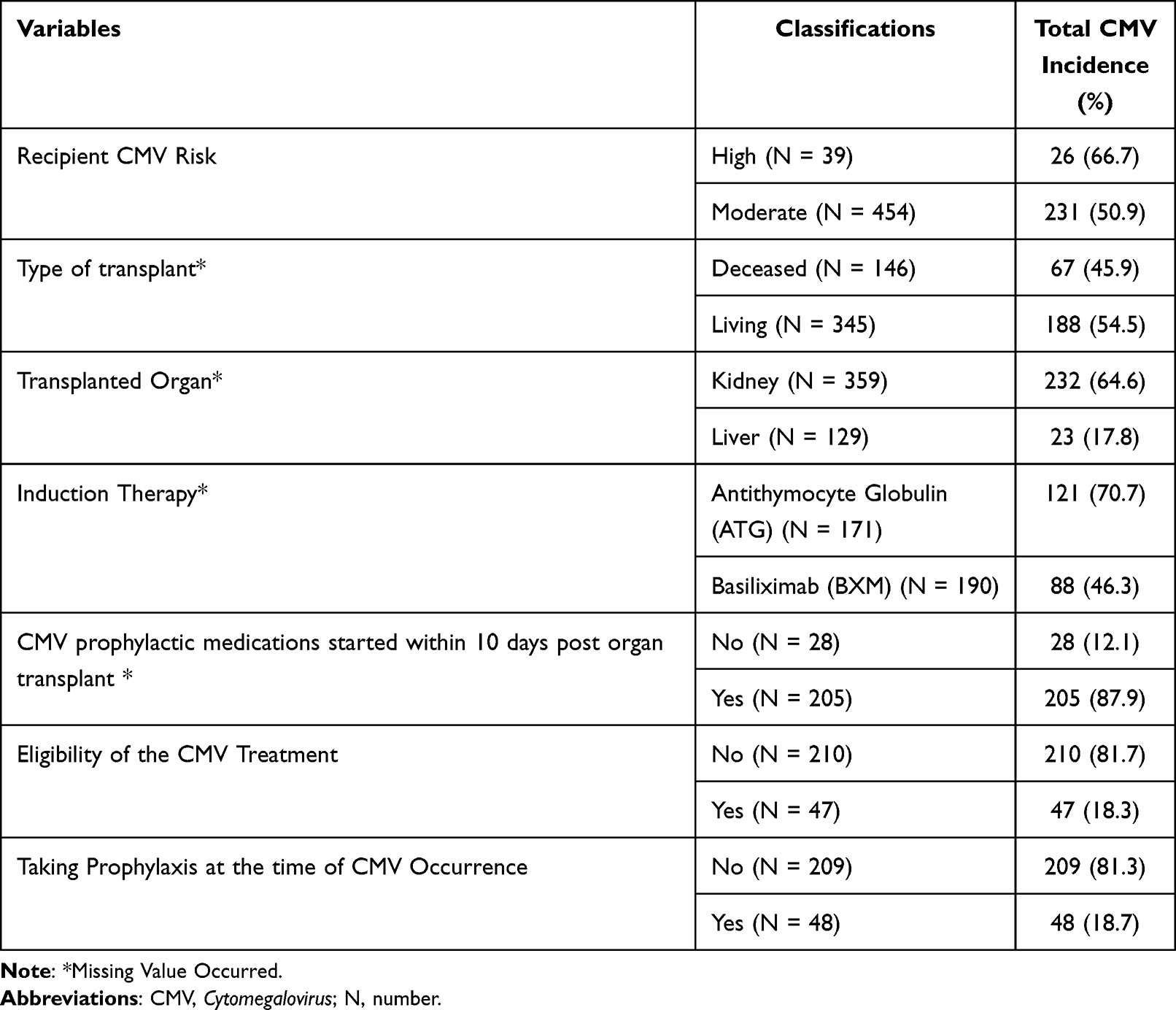 |
Table 4 Total Incidence of Cytomegalovirus Among Different Risk Factors |
A simple univariate regression model was then used to identify the factors associated with the development of CMV among transplant patients (ie, age, gender, type of organ, type of transplant, type of induction therapy, the timing of receiving CMV prophylaxis, and patient risk of CMV). The univariate analysis found that participants 30 years of age or younger had a higher risk of developing CMV than those over 60. The findings revealed no statistically significant difference in the likelihood of contracting CMV based on gender. Patients who had a kidney transplant or a living donor solid organ were similarly more likely to develop CMV than those who received a liver transplant or a deceased donor solid organ. Furthermore, the chances of contracting CMV after induction therapy with basiliximab (BXM) were substantially lower than after Antithymocyte Globulin (ATG). Furthermore, patients identified as high-risk for CMV were more likely (p = 0.069) to get CMV than those classed as moderate risk. After completing univariate logistic regression, statistically significant variables as well as variables with p-value <0.25 were included in the multiple logistic regression model. According to the findings, patients who received a liver transplant, BXM as induction therapy, were significantly less likely to acquire CMV. Furthermore, the multiple regression model revealed that having induction therapy within the first week was more protective against CMV than not receiving a prophylactic or receiving it weeks to months after the transplant operation. The study revealed that age was a risk factor for CMV development; however, the relationship was not significant (p = 0.12).
Multivariate logistic regression that includes age, gender, type of organ, type of transplant, and induction therapy was not significant. However, the duration of prophylaxis and patient CMV risk were significant (p-values were 0.032 and 0.001), respectively. The results are shown in Table 5.
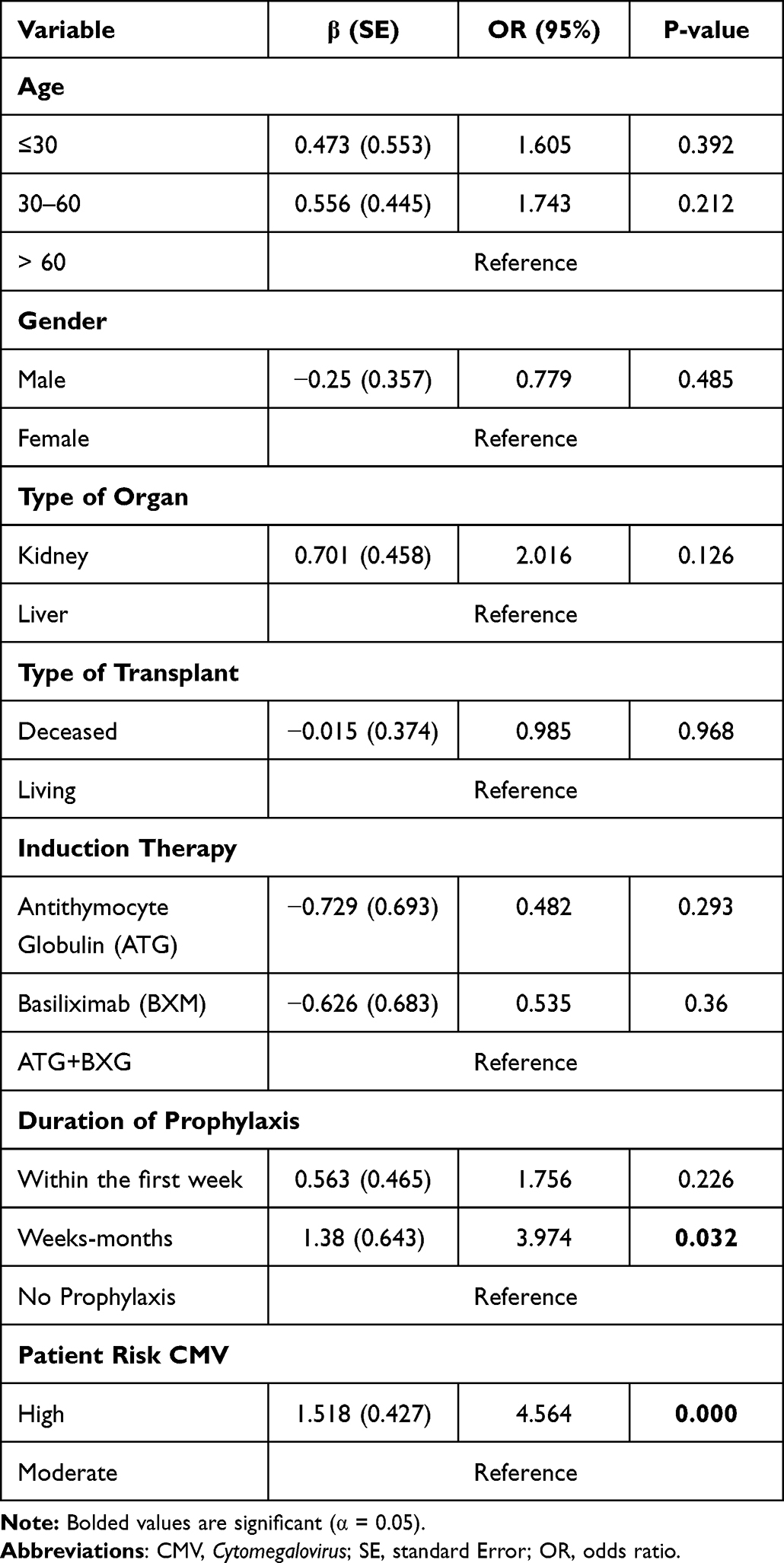 |
Table 5 The Logistic Regression of Sociodemographic and Health-Related Factors Associated with the Cytomegalovirus Infection in Organ Transplant (N = 493) |
Discussion
Cytomegalovirus infection is the biggest complication after solid transplantation that may affect the clinical outcomes. In the absence of prophylactic treatment, CMV disease affects up to 60% of transplant recipients.24,25 In our analysis, we found that 52.1% of the patients (n = 257) developed either CMV infection (91.4%) or CMV diseases (8.6%) post kidney or liver transplant.
Despite antiviral prophylaxis extending to 6 months following kidney transplantation, CMV disease commonly occurs in SOT recipients with CMV D+/R- for 3–6 months following completion of antiviral prophylaxis.16,26,27 In this study, most cases of CMV disease or infection occurred after 6 months post-transplant. The distribution of these CMV infections were distributed over time as follows: (0–3 months; 20.2%, 3–6 months; 27.6%, 6–12 months; 38.1%, 12–24 months; 9.7%, 24–36 months; 4.3%).
In contrast, the Colombian Cohort study reported that in 86% (n = 264) of the cases, CMV disease occurred during the first 6 months after the transplantation.4 Also, a similar study reported that the cumulative incidence of CMV disease after the withdrawal of anti-CMV prophylaxis was 2%, 25%, 27%, 27%, and 29% at 1, 3, 6, 12, and 24 months, respectively.28
There has been controversy regarding optimal valganciclovir dosing in kidney transplant recipients across the literature. Low (or “mini”) dosing of valganciclovir has been reported, with a maximum dose of 450 mg daily in this population.17,29 In our study, we found n = 48 (18.7%) only of cases developed CMV infection, while the patients on CMV prophylaxis (450 mg low dose valganciclovir daily) like what was shown in previous studies, valganciclovir 450 mg daily can prevent the incidence of CMV with good outcomes.30–33
A study published in 2015 found that low-dose and high-dose valganciclovir regimens were similar in preventing CMV disease in high-risk RTR, with a reduced incidence of leukopenia with the low-dose regimen and no difference in resistant CMV. A low dose of valganciclovir may offer significant cost savings.31 Also, a systematic review and meta-analysis describing outcomes in kidney transplant recipients receiving high-dose (900 mg daily) or low-dose (450 mg daily) valganciclovir was published. The study found that low-dose valganciclovir at 450 mg daily was effective for CMV prophylaxis, had no impact on patient or graft survival, and may reduce the risk of leukopenia.30
The mortality rate of CMV reaches 90% if left untreated. CMV can be diagnosed early if risk factors are identified.34 Studying demographic features, risk factors, and outcome data related to CMV infection in recipients despite valganciclovir prophylaxis was an important part of our study. Traditional risk factors for CMV infection include D+/R- status, allograft rejection, severe lymphopenia, and intense immunosuppression. HLA mismatches, other concurrent infections (such as those with herpes virus 6 or 7), and genetic polymorphisms.35–37 From our results, we found a significant difference between the rate of CMV infection and recipient CMV risk and duration of prophylaxis (p-value <0.05).
It is noteworthy that Babazadeh et al's research showed a higher incidence of CMV infection in patients over 40. Among those 41–60 years old, the incidence of CMV disease was 4 times higher than among those under 20 of age (P = 0.001).38 The result of our study showed no significant difference between the rate of CMV infection and the age groups (p-value >0.05).
Taking aggressive measures to minimize immunosuppression can also be beneficial to reduce the incidence of CMV disease, including the use of prednisone-free regimens. In one program for kidney and pancreas transplant recipients, the incidence of CMV disease was drastically reduced by prescribing a steroid-free immunosuppressive regimen.39–41
Based on a retrospective analysis, they found that transplant recipients who were receiving mycophenolate mofetil and prednisone at the time when they discontinued antiviral prophylaxis were more likely to develop CMV disease.39 Like our analysis we observed higher chances of developing CMV disease or infection around (65%) with recipients still receiving mycophenolate mofetil and prednisone when they stopped antiviral treatment. It must be noted that the main disadvantage of this approach is the possibility of causing allograft rejection when immunosuppression levels are reduced to levels that are less than the necessary levels.
There were several limitations to this study. First, this was a retrospective study, which may impose a risk of much missing information. Second, our study was a single-center study, which may limit the generalizability of our findings due to the relatively small sample size. Despite this, the study had several strengths. A representative population of seropositive kidney and liver transplant recipients was included in this study. To confirm the result observed in our study, a prospective multicenter study with a standardized methodology in multi-SOT may be required.
In summary, the findings revealed no statistically significant difference in the likelihood of contracting CMV based on gender, suggesting that CMV has a similar effect on adaptive immunity in both genders. Patients who had a kidney transplant or a living donor solid organ were similarly more likely to develop CMV than those who received a liver transplant or a deceased donor solid organ. This could be related to the fact that active or latent infections in organs donated by living donors are more likely to evolve or reactivate than in organs donated by deceased donors, making them less usable for donation in the absence of careful monitoring and preventive or prophylactic interventions. Furthermore, the chances of contracting CMV after induction therapy with Basiliximab (BXM) were substantially lower than after Antithymocyte Globulin (ATG) (ATG). This is due, in part, to the immunosuppressant medications that patients must take after a kidney transplant. While immunosuppressive medicines minimize the likelihood of the given organ being rejected, they also reduce the immune system’s ability to fight infections. Further, ATG has been used in approximately 50% of kidney transplants compared to 4% of liver transplants, resulting in significant immune system depletion and modification, which possibly explains the higher risk of opportunistic infections in kidney transplants. Furthermore, patients identified as high-risk for CMV were more likely to get CMV than those classed as moderate risk, indicating a lack of ability to generate an effective immune response against CMV. In conclusion, CMV infection remains one of the most important causes of morbidity among kidney and liver recipients who are CMV seropositive despite preexisting CMV immunity. After cessation of antiviral prophylaxis, clinicians should consider CMV disease as a diagnosis for SOT patients presenting with compatible signs and symptoms. The use of CMV prophylaxis without following the guidelines increases the risk of developing CMV infection and/or disease. Therefore, adherence to CMV prophylaxis guidelines may decrease the incidence of CMV infection or disease in this cohort of transplant patients.
Conclusion
CMV infection cases occurred following the completion of antiviral prophylaxis, especially in high CMV risk patients where the donors are seropositive. The study revealed that non-adherence to prophylaxis guidelines in terms of the time of administration is a major factor. Other risk factors were associated with an increased risk of CMV infections and disease but were not significant. The study has shown there is a need for improvement in clinical practice. Future studies should address the optimal timing and duration of the CMV prophylaxis.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Jenssen T, Hartmann A. Post-transplant diabetes mellitus in patients with solid organ transplants. Nat Rev Endocrinol. 2019;15(3):172–188. doi:10.1038/s41574-018-0137-7
2. Black CK, Termanini KM, Aguirre O, Hawksworth JS, Sosin M. Solid-organ transplantation in the 21st century. Ann Transl Med. 2018;6(20):409. doi:10.21037/atm.2018.09.68
3. Helantera I, Lautenschlager I, Koskinen P. The risk of cytomegalovirus recurrence after kidney transplantation. Transpl Int. 2011;24(12):1170–1178. doi:10.1111/j.1432-2277.2011.01321.x
4. Arthurs SK, Eid AJ, Pedersen RA, et al. Delayed-onset primary cytomegalovirus disease and the risk of allograft failure and mortality after kidney transplantation. Clin Infect Dis. 2008;46(6):840–846. doi:10.1086/528718
5. Kliem V, Fricke L, Wollbrink T, Burg M, Radermacher J, Rohde F. Improvement in long-term renal graft survival due to CMV prophylaxis with oral ganciclovir: results of a randomized clinical trial. Am J Transplant. 2008;8(5):975–983. doi:10.1111/j.1600-6143.2007.02133.x
6. Witzke O, Hauser IA, Bartels M, Wolf G, Wolters H, Nitschke M. Valganciclovir prophylaxis versus preemptive therapy in cytomegalovirus-positive renal allograft recipients: 1-year results of a randomized clinical trial. Transplantation. 2012;93(1):61–68. doi:10.1097/TP.0b013e318238dab3
7. Bate SL, Dollard SC, Cannon MJ. Cytomegalovirus seroprevalence in the United States: the national health and nutrition examination surveys, 1988–2004. Clin Infect Dis. 2010;50(11):
8. Cannon MJ, Schmid DS, Hyde TB. Review of cytomegalovirus seroprevalence and demographic characteristics associated with infection. Rev Med Virol. 2010;20(4):
9. Meesing A, Abraham RS, Razonable RR. Clinical correlation of cytomegalovirus infection with CMV-specific CD8+ T-cell immune competence score and lymphocyte subsets in solid organ transplant recipients. Transplantation. 2019;103(4):832–838. doi:10.1097/TP.0000000000002396
10. Ljungman P, Boeckh M, Hirsch HH, et al. Definitions of cytomegalovirus infection and disease in transplant patients for use in clinical trials. Clin Infect Dis. 2017;64(1):87–91. doi:10.1093/cid/ciw668
11. Humar A, Michaels M. American society of transplantation recommendations for screening, monitoring, and reporting of infectious complications in immunosuppression trials in recipients of organ transplantation. Am J Transplant. 2006;6(2):262–274. doi:10.1111/j.1600-6143.2005.01207.x
12. Khoury JA, Storch GA, Bohl DL, et al. Prophylactic versus preemptive oral valganciclovir for the management of cytomegalovirus infection in adults renal transplant recipients. Am J Transplant. 2006;6(9):2134–2143. doi:10.1111/j.1600-6143.2006.01413.x
13. Reischig T, Jindra P, Hes O, Svecova M, Klaboch J, Treska V. Valacyclovir prophylaxis versus preemptive valganciclovir therapy to prevent cytomegalovirus disease after renal transplantation. Am J Transplant. 2008;8(1):69–77. doi:10.1111/j.1600-6143.2007.02031.x
14. Singh N, Winston DJ, Razonable RR, et al. Preemptive therapy versus prophylaxis for prevention of cytomegalovirus disease in high-risk donor seropositive/recipient seronegative liver transplant recipients: an NIH-sponsored, randomized, controlled, multicenter trial. ID Week. 2018;5(Suppl 1):S766. doi: 10.1093/ofid/ofy229.2195
15. Razonable RR, Humar A. Cytomegalovirus in solid organ transplant recipients-guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019;33(9):e13512. doi:10.1111/ctr.13512
16. Humar A, Lebranchu Y, Vincenti F, et al. The efficacy and safety of 200 days valganciclovir cytomegalovirus prophylaxis in high-risk kidney transplant recipients. Am J Transplant. 2010;10(5):1228–1237. doi:10.1111/j.1600-6143.2010.03074.x
17. Kalil AC, Mindru C, Florescu DF. Effectiveness of valganciclovir 900 mg versus 450 mg for cytomegalovirus prophylaxis in transplantation: direct and indirect treatment comparison meta-analysis. Clin Infect Dis. 2011;52(3):313–321. doi:10.1093/cid/ciq143
18. Levitsky J, Singh N, Wagener MM, Stosor V, Abecassis M, Ison MG. A survey of CMV prevention strategies after liver transplantation. Am J Transplant. 2008;8(1):158–161. doi:10.1111/j.1600-6143.2007.02026.x
19. Razonable RR, Hayden RT. Clinical utility of viral load in management of cytomegalovirus infection after solid organ transplantation. Clin Microbiol Rev. 2013;26(4):
20. Asberg A, Humar A, Rollag H, et al. Oral valganciclovir is noninferior to intravenous ganciclovir for the treatment of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant. 2007;7(9):2106–2113. doi:10.1111/j.1600-6143.2007.01910.x
21. Humar A, Kumar D, Boivin G, Caliendo AM. Cytomegalovirus (CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease. J Infect Dis. 2002;186(6):829–833. doi:10.1086/342601
22. Sia IG, Wilson JA, Groettum CM, Espy MJ, Smith TF, Paya CV. Cytomegalovirus (CMV) DNA load predicts relapsing CMV infection after solid organ transplantation. J Infect Dis. 2000;181(2):717–720. doi:10.1086/315242
23. Asberg A, Humar A, Jardine AG, et al. Long-term outcomes of CMV disease treatment with valganciclovir versus IV ganciclovir in a solid organ transplant recipients. Am J Transplant. 2009;9(5):1205–1213. doi:10.1111/j.1600-6143.2009.02617.x
24. Hodson EM, Barclay PG, Craig JC, et al. Antiviral medications for preventing cytomegalovirus disease in solid organ transplant recipients. Cochrane Database Syst Rev. 2005;19(4):CD003774.
25. Sagedal S, Hartmann A, Rollag H. The impact of early cytomegalovirus infection and disease in renal transplant recipients. Clin Microbiol Infect. 2005;11:518–530. doi:10.1111/j.1469-0691.2005.01190.x
26. Azevedo LS, Pierrotti LC, Abdala E, et al. Cytomegalovirus infection in transplant recipients. Clinics. 2015;70(7):515–523. doi:10.6061/clinics/2015(07)09
27. Razonable RR. Cytomegalovirus infection after liver transplantation: current concepts and challenges. World J Gastroenterol. 2008;14(31):4849–4860. doi:10.3748/wjg.14.4849
28. Díaz J, Henao J, Rodelo J, García A, Arbeláez M, Jaimes F. Incidence and risk factors for cytomegalovirus disease in a Colombian cohort of kidney transplant recipients. Transplant Proc. 2014;46(1):160–166. doi:10.1016/j.transproceed.2013.07.070
29. Stevens DR, Sawinski D, Blumberg E, Galanakis N, Bloom RD, Trofe-Clark J. Increased risk of breakthrough infection among cytomegalovirus donors- positive/recipient negative kidney transplant recipients receiving lower-dose valganciclovir prophylaxis. Transpl Infect Dis. 2015;17(2):163–173. doi:10.1111/tid.12349
30. Xin W, Hui Y, Xiaodong Z, Xiangli C, Shihui W, Lihong L. Effectiveness of valganciclovir 900mg versus 450mg for cytomegalovirus prophylaxis in renal transplantation: a systematic review and meta-analysis. J Pharm Pharm Sci. 2017;20:168–183. doi:10.18433/J3805B
31. Gabardi S, Asipenko N, Fleming J, et al. Evaluation of low- versus high-dose valganciclovir for prevention of cytomegalovirus disease in high-risk renal transplant recipients. Transplantation. 2015;99(7):1499–1505. doi:10.1097/TP.0000000000000570
32. Heldenbrand S, Li C, Cross RP, et al. Multicenter evaluation of efficacy and safety of low-dose versus high-dose valganciclovir for prevention of CMV disease in donor and recipient positive (D+/R+) renal transplant recipients. Transpl Infect Dis. 2016;18(6):904–912. doi:10.1111/tid.12609
33. Gabardi S, Cross R, DePiero K, et al. Prevention of cytomegalovirus with valganciclovir 450 mg daily vs. 900 mg daily in intermediate-risk renal transplant recipients (D-/R+); a multicenter safety and efficacy evaluation. Am J Transplant. 2013;13:210.
34. Kute VB, Vanikar AV, Shah PR, et al. Post-renal transplant cytomegalovirus infection: a study of risk factors. Transplant Proc. 2012;44(3):706–709. doi:10.1016/j.transproceed.2011.12.025
35. Rayes N, Seehofer D, Lullius SG, et al. Monitoring of human cytomegalovirus, HHV-6, and HHV-7 infection in kidney transplant recipients by molecular methods to predict HCMV disease after transplantation: a prospective study. Ann Transplant. 2005;10(2):23–28.
36. Hoffmann TW, Halimi JM, Büchler M, et al. Association between a polymorphism in the human programmed death-1 (PD-1) gene and cytomegalovirus infection after kidney transplantation. J Med Genet. 2009;47(1):54–58. doi:10.1136/jmg.2009.068841
37. Adu D, Cockwell P, Ives NJ, Shaw J, Wheatley K. Interleukin-2 receptor monoclonal antibodies in renal transplantation: a meta-analysis of randomized trials. BMJ. 2003;326(7393):789. doi:10.1136/bmj.326.7393.789
38. Babazadeh A, Javanian M, Oliaei F, et al. Incidence and risk factors for cytomegalovirus in kidney transplant patients in Babol, northern Iran. Caspian J Intern Med. 2017;8(1):23–29.
39. Axelrod D, Leventhal JR, Gallon LG, Parker MA, Kaufman DB. Reduction of CMV disease with steroid-free immunosuppression in simultaneous pancreas-kidney transplant recipients. Am J Transplant. 2005;5(6):1423–1429. doi:10.1111/j.1600-6143.2005.00855.x
40. Matas AJ, Kandaswamy R, Humar A, et al. Long- term immunosuppression, without maintenance prednisone, after kidney transplantation. Ann Surg. 2004;240(3):510–517. doi:10.1097/01.sla.0000137140.79206.d0
41. Cantarovich D, Giral-Classe M, Hourmant M, et al. Low incidence of kidney rejection after simultaneous kidney-pancreas transplantation after antithymocyte globulin induction and in the absence of corticosteroids: results of a prospective pilot study in 28 consecutive cases. Transplantation. 2000;69:1505–1509. doi:10.1097/00007890-200004150-00051
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.