Back to Journals » Drug Design, Development and Therapy » Volume 20
Prophylactic Efficacy of Cipepofol Against Postoperative Nausea and Vomiting in Moderate to High-Risk Patients of Apfel Score: A Multicenter, Randomized, and Parallel-Group Comparative Trial
Authors Deng J, He J ![]() , Li P, Liu T, Chen Y, Jiang Y, Fu Q, Jiang X, Li L, Li J, Li J, Xia B, Xu L, Zhang Q, Zhong Q
, Li P, Liu T, Chen Y, Jiang Y, Fu Q, Jiang X, Li L, Li J, Li J, Xia B, Xu L, Zhang Q, Zhong Q ![]() , Luo X, Liu S, Yang M
, Luo X, Liu S, Yang M
Received 19 May 2025
Accepted for publication 5 March 2026
Published 16 March 2026 Volume 2026:20 541456
DOI https://doi.org/10.2147/DDDT.S541456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Leonidas D. Panos
Jia Deng,1,* Jing He,2,* Peiyu Li,3 Ting Liu,4 Yufeng Chen,5 Yi Jiang,6 Qiang Fu,7 Xian Jiang,8 Linji Li,9 Jun Li,10 Jun Li,11 Bingchun Xia,12 Liu Xu,13 Qiang Zhang,14 Qing Zhong,15 Xiaoxiu Luo,16 Shaoxing Liu,17 Mengchang Yang1
1Department of Anesthesiology, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, Sichuan, People’s Republic of China; 2Department of Anesthesiology, People’s Hospital of Deyang, Chengdu, Sichuan, People’s Republic of China; 3Department of Anesthesiology, Sichuan Provincial Orthopedic Hospital, Chengdu, Sichuan, People’s Republic of China; 4Department of Anesthesiology, Qionglai Medical Center Hospital, Qionglai, Sichuan, People’s Republic of China; 5Department of Anesthesiology, People’s Hospital of Changzhi, Changzhi, Shanxi, People’s Republic of China; 6Department of Anesthesiology, Chongzhou Traditional Chinese Medicine Hospital, Chongzhou, Sichuan, People’s Republic of China; 7Department of Anesthesiology, the Third People’s Hospital of Chengdu, Chengdu, Sichuan, People’s Republic of China; 8Department of Anesthesiology, Luzhou People’s Hospital, Luzhou, Chengdu, Sichuan, People’s Republic of China; 9Department of Anesthesiology, Nanchong Central Hospital, Nanchong, Sichuan, People’s Republic of China; 10Department of Anesthesiology, Dazhou Central Hospital, Dazhou, Sichuan, People’s Republic of China; 11Department of Anesthesiology, Mianyang Central Hospital, Mianyang, Sichuan, People’s Republic of China; 12Department of Anesthesiology, Dazhu County People’s Hospital, Dazhou, Sichuan, People’s Republic of China; 13Department of Anesthesiology, Wenjiang District People’s Hospital, Wenjiang, Sichuan, People’s Republic of China; 14Department of Anesthesiology, the First People’s Hospital of Longquanyi District, Chengdu, Sichuan, People’s Republic of China; 15Department of Anesthesiology, Jianyang People’s Hospital, Chengdu, Sichuan, People’s Republic of China; 16Department of Intensive Care Center, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, Sichuan, People’s Republic of China; 17Department of Anesthesiology, The Second People’s Hospital of Chengdu City, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mengchang Yang, Department of Anesthesiology, Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, 32# W. Sec 2, 1st Ring Road, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Objective: This investigation systematically evaluated the antiemetic efficacy and safety of cipepofol for prophylaxis of postoperative nausea and vomiting (PONV) in surgical candidates with moderate to high Apfel risk.
Methods: A prospective, multicenter, randomized, parallel-group comparative trial was conducted at 18 clinical centers (N=594). Participants aged 18– 60 years (ASA physical status I–III) with 2– 4 Apfel risk factors undergoing elective noncardiac surgery were randomized into three anesthesia maintenance cohorts after cipepofol induction: cipepofol monotherapy (0.8 mg/kg/h), sevoflurane (1.5– 2.0%), and combination therapy (cipepofol 0.4 mg/kg/h plus sevoflurane 1.0%). The primary endpoint was the incidence of PONV at 24 h postoperatively. Secondary endpoints included the incidence of PONV at 48 h postoperatively and intraoperative hemodynamic stability.
Results: Cipepofol monotherapy yielded a significantly lower 24-h PONV incidence (32.97% [95% CI, 27.1– 39.2]) than sevoflurane (65.75% [59.4– 71.6]; p< 0.001). This difference persisted at 48 h (cipepofol: 35.68% [29.5– 42.3]; sevoflurane: 69.06% [62.8– 74.8]). A significantly lower proportion of patients required rescue antiemetic therapy in the cipepofol group than in the sevoflurane group within 48 h postoperatively (7.03% vs 16.02%, p=0.007). In addition, cipepofol was associated with a lower incidence of intraoperative hypotension than sevoflurane (9.73% vs 19.34%, p=0.009).
Conclusion: Compared with sevoflurane alone, cipepofol significantly reduced PONV incidence at 24 and 48 h after surgery, with more stable intraoperative hemodynamics.
Keywords: cipepofol, Postoperative nausea and vomiting, PONV, total intravenous anesthesia, inhalational anesthetics, apfel risk stratification
Introduction
Postoperative nausea and vomiting (PONV) is defined as nausea and/or vomiting that occur within the first 24–48 h after surgery. However, symptoms may persist for 3–5 days in 5–10% of patients. As one of the most common perioperative complications, PONV affects approximately 30% of the general surgical population.1 This risk increases to 70–80% in high-risk groups, such as patients with a history of motion sickness or those who use postoperative opioids.2 PONV is distressing for patients and can significantly affect patient satisfaction,3,4 leading to complications such as fluid and electrolyte imbalance, wound dehiscence, incisional hernia, aspiration, and aspiration pneumonia. Additionally, each episode of vomiting may delay discharge from the recovery room by about 20 min.5
Current clinical guidelines recommend that patients at moderate risk receive two or more antiemetic agents, whereas a multimodal prophylactic approach is generally advised for individuals at high risk.6 However, in clinical practice, the implementation of multimodal prophylactic strategies remains suboptimal, and adherence to these guidelines among healthcare providers is limited,7 which hinders their widespread application.
Volatile inhalation agents such as sevoflurane are among the cornerstones of general anesthesia in clinical practice. Sevoflurane is preferred for its hemodynamic stability, smooth induction, and rapid recovery. However, studies have shown that patients under sevoflurane anesthesia experience significantly higher rates of PONV than those receiving propofol-based total intravenous anesthesia (TIVA), particularly in the early postoperative period.8–11 Propofol-based TIVA offers distinct advantages, including rapid onset and rapid postoperative recovery, and it consistently maintains anesthesia while exerting a strong antiemetic effect that reduces PONV.12–15 Nevertheless, propofol is associated with adverse effects such as injection pain, cardiopulmonary depression, and rare but serious complications.16
Cipepofol (Haisco Pharmaceutical Group Co., Ltd., Liaoning Province, China), an innovative intravenous anesthetic, is a structural derivative of propofol modified by the addition of a cyclopropyl group. This modification enhances its selectivity for GABAA receptors compared to propofol.14 Emerging16 studies have shown that cipepofol is noninferior to propofol for PONV prevention after selected surgical procedures.17,18 However, no randomized comparative trials have directly compared the incidence of PONV between cipepofol and volatile inhalation agents during maintenance of anesthesia.
Therefore, this study aims to compare and evaluate the efficacy and safety of cipepofol, sevoflurane, and their combination in preventing PONV among patients at moderate to high risk (as defined by the Apfel score) undergoing elective tracheal intubation surgery.
Materials and Methods
Participants and Study Design
This multicenter, randomized, and parallel-group comparative trial compared cipepofol, sevoflurane, and their combination for preventing PONV in adults at moderate-to-high PONV risk (Apfel score ≥2) undergoing elective surgery under general anesthesia with endotracheal intubation. The study was approved by the Ethics Committee of Sichuan Provincial People’s Hospital (Ethics Approval No. [Research] 2023–23-1). It was registered at ClinicalTrials.gov (NCT05837156) and conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was obtained from all participants prior to their participation. All patients underwent a preoperative visit the day before surgery, which included a detailed clinical history, physical examination, and any required investigations. This trial was conducted at 18 centers in China from January 2023 to April 2025.
Patients were eligible if they met all of the following inclusion criteria: (1) at least 2 of the 4 risk factors for PONV (history of PONV or motion sickness, non-smoker, female, and use of opioid analgesics);1 (2) elective surgery with an estimated anesthesia duration of ≥1and ≤3 h (non-emergency, non-cardiothoracic, and non-neurosurgical procedures) with priority given to laparoscopic surgery, gastrointestinal surgery, gynecological surgery, tympanoplasty, and tonsillectomy, among others; anesthesia duration was defined as the time from the start of anesthetic induction to cessation of anesthetic maintenance drugs; (3) male or female patients aged≥18 years, with a body mass index (BMI) of 18–28 kg/m2, and an American Society of Anesthesiologists Physical Status (ASA-PS) score of I to III.
Patients were excluded if they had any of the following conditions: (1) vestibular nerve disorder, dizziness, nausea, or vomiting within 24 h before the surgery, or if they had undergone routine antiemetic treatment within 24 h before the surgery; (2) need for postoperative ventilation support or placement of a nasogastric tube for a period of time after surgery; (3) any other factors deemed by the investigator to make them unsuitable for participation in the study. Enrolled patients were assessed for baseline PONV risk using the simplified Apfel scale. The scale assigns 0–4 points, corresponding to approximate PONV risks of 10%, 20%, 40%, 60%, and 80%. Patients in this study had 2–4 risk factors, corresponding to an expected incidence of PONV of 40% to 80%.
Randomization and Masking
Participants were randomly allocated in a 1:1:1 ratio to one of three groups for anesthetic maintenance: cipepofol (Group C), sevoflurane (Group S), or their combination (Group CS), following cipepofol induction. All patients remained blinded throughout the study. Assessment of nausea and vomiting severity, investigation of intraoperative awareness, evaluation of postoperative delirium, and satisfaction assessments of subjects and anesthesiologists were conducted by independent evaluators in a blinded manner.
Study Procedures and Drug Administration
All eligible subjects were permitted to receive pre-treatment, excluding sedative-hypnotics, analgesics with PONV-inducing effects, and antiemetics, prior to surgery. An intravenous bolus of sufentanil at 0.3 μg/kg was administered 2 min (±30 s) before anesthesia induction and completed within 30s (±5 s). Subjects in all three groups received cipepofol for anesthesia induction following this protocol: an initial loading dose of ≤0.4 mg/kg, based on body weight, administered over 30s (±5 s). Supplemental doses of ≤0.2 mg/kg could be administered over 10s (±2 s) at approximately 1-min intervals, depending on subject response.
After successful induction, rocuronium bromide 0.6 mg/kg was administered as a bolus over 15±2 s, followed by endotracheal intubation after the onset of neuromuscular blockade. Maintenance anesthesia was initiated within 60s after intubation. Subjects were randomized in a 1:1:1 ratio to three maintenance groups (C/S/CS) with balanced PONV risk factors: C) Cipepofol maintenance: Continuous infusion starting at 0.8 mg/kg/h, adjustable between 0.4–2.4 mg/kg/h based on response. S) Sevoflurane maintenance: Initial inspired concentration of 1.5–2.0%, adjusted as needed. CS) Combined maintenance: Sevoflurane (initial 0.5%) plus low-dose cipepofol (initial 0.4 mg/kg/h), with cipepofol adjustable between 0.2–1.2 mg/kg/h.
A flowchart of the surgical procedure is provided below (Figure 1). Intraoperative remifentanil was administered at a rate of 0.1–0.5 μg/kg/min. All subjects received sufentanil at a dose of 0.1 μg/kg, 5±1 min before the conclusion of surgery. Postoperative use of the patient-controlled analgesia (PCA) pump was unrestricted. If needed, the PCA pump was configured with sufentanil at a concentration of 0.001 mg/mL. During anesthesia induction, injection pain and the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) score were recorded. The MOAA/S score was used to assess sedation, ranging from 5 (responsive to auditory stimuli) to 0 (deeply sedated/unresponsive/comatose). Vital signs, adverse events (AEs), and bispectral index were monitored during the intraoperative period.
 |
Figure 1 Flowchart of the surgical procedure. Group C, cipepofol maintenance. Group S, sevoflurane maintenance. Group CS, low-dose cipepofol + sevoflurane maintenance. |
Use of sedative-hypnotic drugs, analgesics (including opioids and tramadol), and antiemetic drugs (including but not limited to phenothiazines, butyrophenones, benzamide derivatives, corticosteroids, anticholinergics, antihistamines, and 5-HT3 antagonists), other than those specified in the protocol, was prohibited during preoperative preparation and throughout the surgery. Antiemetic drugs for the prevention of vomiting were prohibited during the first 24 h after surgery to assess the effect of the three treatment groups on PONV incidence. The severity of PONV was assessed using a 10-point Visual Analog Scale (VAS), where 0 indicated “no nausea at all” and 10 indicated “the worst imaginable nausea”. Patients rated the intensity of nausea by pointing to the corresponding number on a printed scale. Moderate-to-severe nausea was defined as VAS≥5, as this level of discomfort typically necessitates rescue intervention.19–21 If patients experienced moderate-to-severe nausea (VAS≥5) or ≥2 vomiting episodes, they immediately received dolasetron maleate (12.5 mg) intravenously as rescue medication. If vomiting recurred (≥ 3 episodes), additional antiemetic agents were permitted. Atropine was permitted to treat sinus bradycardia. Intraoperative AEs, including hypotension, hypertension, bradycardia, tachycardia, or hypoxemia, were managed with available medications at the clinician’s discretion.
Outcomes and Definitions
The primary efficacy endpoint was the incidence of PONV within 24 h after surgery (PONV24), defined as the occurrence of any nausea, retching, or vomiting. PONV incidence (%) was calculated as (number of patients experiencing nausea and/or vomiting / total number of patients in the group) × 100%. Secondary efficacy endpoints included the incidence of nausea and vomiting within 48 h after surgery (PONV48) and the number of patients requiring rescue antiemetic therapy, defined as subjects reporting moderate to severe nausea and vomiting [VAS score of 5–10]. These outcomes were recorded at 24 and 48 h after surgery.
Safety evaluations included the incidence of hypotension (defined as a >30% decrease in systolic blood pressure [SBP] or diastolic blood pressure [DBP] from baseline, SBP <80 mmHg, or DBP <40 mmHg), bradycardia (heart rate <50 beats/min), and hypoxemia (peripheral oxygen saturation [SpO2] <90%). Intraoperative monitoring was continuous, and the lowest values were recorded to determine the incidence of hypotension, bradycardia, and hypoxemia. Postoperative follow-up was conducted by evaluators in the ward.
Statistical Analysis
Analyses were performed using SAS version 9.4 with a block size of 3. All tests were two-sided with a significance level of p≤0.05. Continuous variables are reported as mean ± standard deviation (SD), and categorical variables are presented as frequencies and percentages.
For continuous data, including baseline characteristics and hemodynamic parameters, one way analysis of variance (ANOVA) was used for intergroup comparisons. Normality of continuous data was assessed using the Shapiro–Wilk test, and homogeneity of variances was evaluated using Levene’s test to verify the assumptions of ANOVA. All continuous variables met the assumptions of normality and homogeneity of variances. Since no statistically significant differences were observed among the three groups for any continuous variable, no post-hoc tests for ANOVA were required.
For categorical variables, including the primary endpoint (incidence of PONV at 24 h) and key secondary endpoints (incidence of PONV at 48 h, rescue antiemetic use at 24/48 h, and intraoperative safety events), comparisons among the three treatment groups were performed using Pearson’s chi-square test or Fisher’s exact test (for low-frequency outcomes). When the overall chi-square test was significant, post-hoc pairwise comparisons were conducted with a Bonferroni correction, setting the adjusted significance threshold at α=0.017 (0.05/3 comparisons) to control the family-wise error rate. Subgroup analyses based on Apfel risk scores (2, 3, or 4 factors) were also performed using chi-square tests within each score category. The Cochran-Mantel-Haenszel test, which accounts for center effects, was employed for the primary response analysis (PONV at 24 h). Changes in PONV incidence from 24 h to 48 h within each group were assessed using McNemar’s test.
Due to the restricted inclusion criteria (age 18–60 years, BMI 18–28 kg/m2), no extreme outliers were present in the continuous variables. All primary and secondary outcomes were binary variables, which are not affected by outliers. No outlier handling was required.
Sample Size Calculation
Based on preliminary trial results, the anticipated incidence of PONV was approximately 40% in Group C, 60% in Group S, and 50% in Group CS. Using PASS 15 with α=0.05, β=0.1, and a 20% dropout rate, a total of 594 subjects are planned for enrollment.
Results
Baseline Characteristics
A total of 610 patients were assessed for eligibility, of whom 594 met the inclusion criteria. Of these, 13 patients withdrew their consent, and 32 violated the study protocol during surgery, resulting in a final sample of 549 patients for analysis (Figure 2). The three groups were well-balanced at baseline with respect to sex, age, weight, height, BMI, Apfel risk score, underlying diseases, ASA classification, and surgical type (all P>0.05) (Table 1).
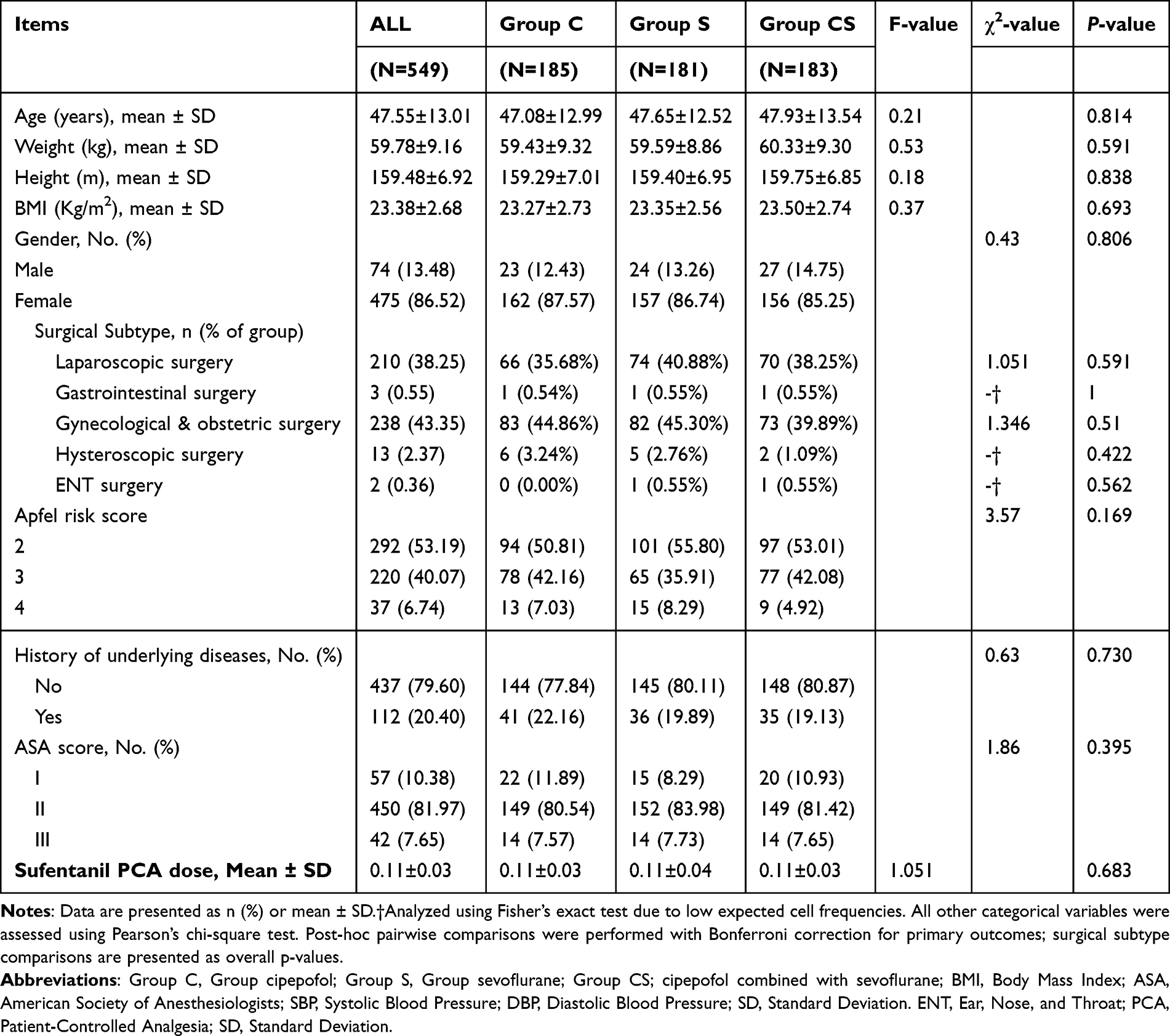 |
Table 1 Demographic and Baseline Characteristics of Enrolled Patients |
 |
Figure 2 Enrollment flow diagram of the study design. |
Efficacy Outcomes
The incidence of PONV showed significant intergroup differences at both 24 h (χ2=37.02, p<0.001) and 48 h (χ2=33.44, p<0.001) (Table 2 and Figure 3). Group S had the highest PONV rates at 24 h (65.75%) and 48 h (69.06%), which were significantly higher than in Group C (32.97% at 24 h, 35.68% at 48 h; p<0.001) and Group CS (42.62% at 24 h, 44.81% at 48 h; p<0.001). No statistically significant difference was observed between Group C and Group CS at either time point (p=0.056 at 24 h; p=0.074 at 48 h). For patients with an Apfel score of 2–3 (indicating 2–3 PONV risk factors), significant differences were observed among the three treatment groups.
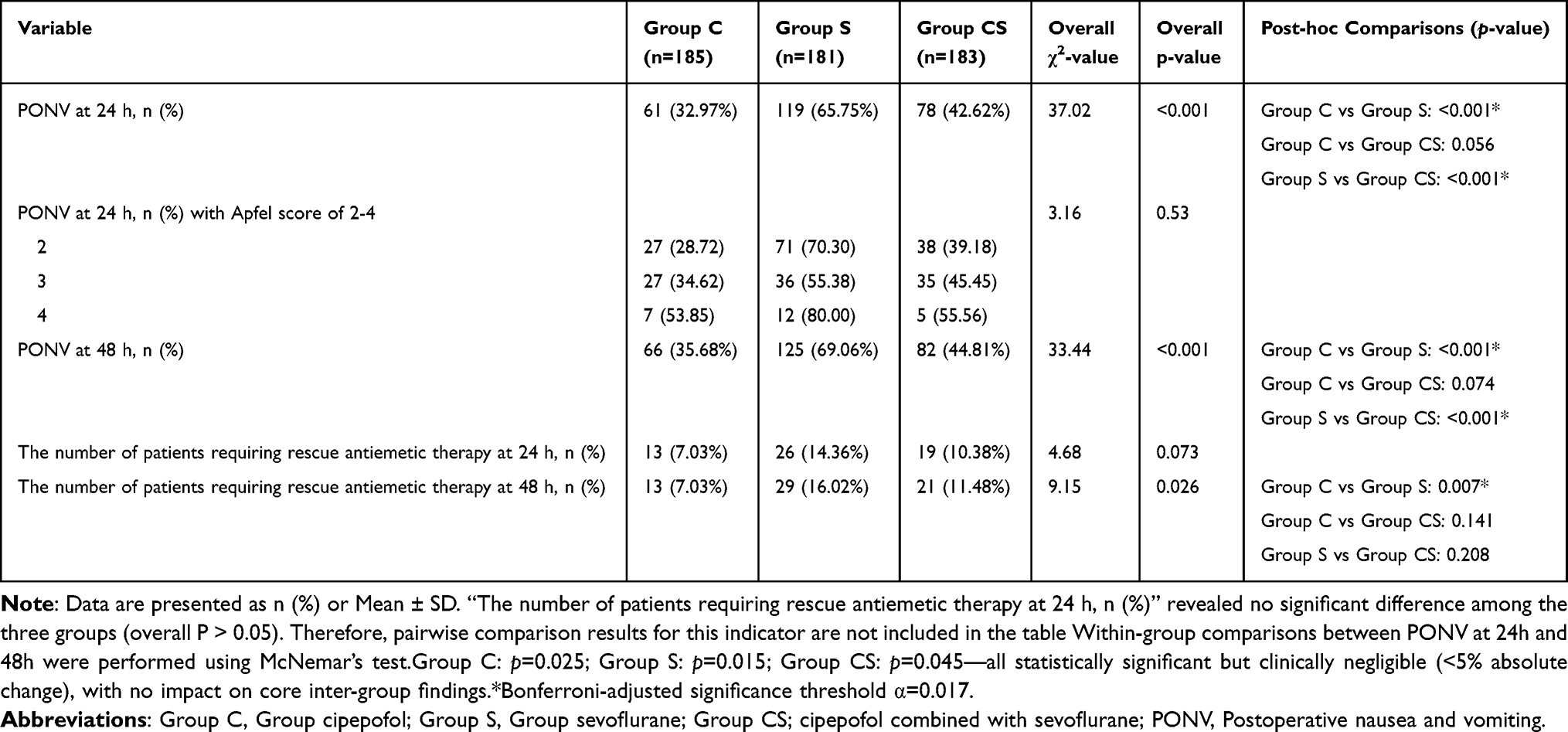 |
Table 2 Comparative Postoperative Outcomes with Bonferroni-Adjusted Comparisons |
 |
Figure 3 Incidence of PONV and the percentage of patients requiring rescue antiemetic therapy within 24 h post-operation in Groups C, S, and CS. *Group C vs. S, p<0.017 (adjusted α=0.017).Group C, cipepofol maintenance (0.8 mg/kg/h). Group S, sevoflurane maintenance. Group CS, low-dose cipepofol (0.4 mg/kg/h) + sevoflurane maintenance. PONV, postoperative nausea and vomiting. |
For rescue antiemetic therapy within 48 h, Group C (7.03%, 13/185) required significantly fewer interventions than Group S (16.02%, 29/181; p=0.007), whereas Group CS (11.48%, 21/183) showed intermediate values without statistical significance. The number of patients requiring rescue antiemetic therapy within 24 h did not differ significantly among the three groups (p=0.073).
Safety Profile
Hemodynamic indicators were recorded during the intraoperative period. The incidence of hypotension differed significantly across groups (p=0.031), with Group C showing a markedly lower rate (9.73%) than Group S (19.34%, p=0.009). No statistically significant differences were observed in bradycardia among the groups (Group C: 14.59%, Group S: 15.47%, Group CS: 10.38%; p=0.314) (Table 3 and Figure 4). Hypoxemia was rare, occurring in only two cases (one each in Groups S and CS). These findings suggest enhanced hemodynamic stability with cipepofol relative to sevoflurane.
 |
Table 3 Comparative Intraoperative Safety Profile Within Three Groups |
 |
Figure 4 Incidence of intraoperative TRAEs in Groups C, S, and CS. Abbreviations: Group C, cipepofol maintenance. Group S, sevoflurane maintenance. Group CS, low-dose cipepofol + sevoflurane maintenance. TRAEs, treatment-related adverse events. Note: *Group C vs. S, hypotension, p<0.017 (adjusted α=0.017). |
Discussion
Our study provides direct evidence that cipepofol-based anesthesia maintenance (monotherapy or combined with sevoflurane) significantly reduces the incidence of PONV within 24 h after surgery in moderate- to high-risk patients compared with sevoflurane, while also providing superior intraoperative hemodynamic stability. This finding is consistent with evidence indicating that volatile anesthetics such as sevoflurane are independent risk factors for PONV.8–11 The same trend persisted within 48 h postoperatively. The nearly twofold difference in PONV incidence between the cipepofol and sevoflurane groups highlights a clinically important effect. Critical to interpretation is the robust baseline balance across the three study groups: as shown in Table 1, all key baseline indicators were evenly distributed. This balance minimizes the influence of preexisting or intraoperative confounders, supporting the conclusion that the observed differences in PONV incidence and intraoperative hemodynamic stability reflect the anesthetic maintenance regimens rather than baseline differences.
According to the Apfel score, patients with 2–4 risk factors for PONV have an incidence of 40%-80%5 Notably, these rates are markedly higher than those observed in our cipepofol groups (monotherapy: 32.97%; combination: 42.62%). This finding suggests that cipepofol exerts a substantial suppressive effect on PONV, consistent with prior reports of propofol-based TIVA.22–25
In subgroup analyses by Apfel risk score (2–4 factors), the incidence of PONV24 was significantly lower in Group C than in Group S among patients with 2 or 3 risk factors (both p<0.05), indicating a more favorable antiemetic effect of cipepofol in this population. Among patients with 4 risk factors, no statistically significant difference in PONV24 incidence was observed between Group C and Group S, although a trend toward lower incidence in Group C was noted; this may reflect the limited sample size of this high-risk subgroup.
As a novel intravenous anesthetic, cipepofol incorporates a cyclopropyl moiety into the structure of propofol, enhancing hypnotic potency by roughly 4-5-fold compared with propofol26 while mitigating common propofol-associated drawbacks such as injection site pain and pronounced respiratory and cardiovascular effects.27 Mechanistically, the suppressive effect of cipepofol on PONV is plausible. As a structural derivative of propofol, cipepofol is postulated to share similar mechanisms of action—potentially involving modulation of the chemoreceptor trigger zone and inhibition of 5-HT and dopamine receptors.28 This stands in contrast to sevoflurane: existing evidence links sevoflurane to dopaminergic activation in the hippocampus, a mechanism associated with a higher incidence of PONV.29 Therefore, the present findings align with the expected pharmacological profiles of these two classes of anesthetics, which helps explain why the PONV24 and PONV48 rates were lower in the cipepofol group than in the sevoflurane group. Nonetheless, there is an apparent discrepancy with the study by Bansal et al,30 which reported that sevoflurane does not increase the risk of PONV during laparoscopic surgery This discrepancy may stem from differences in patient selection: Bansal et al excluded individuals with a history of nausea, vomiting, or motion sickness, whereas our study specifically enrolled patients at moderate to high risk for PONV.
Notably, although the requirement for rescue antiemetic therapy within the first 24 h did not differ significantly among the three groups (p=0.073), Group C had a significantly lower proportion of patients requiring rescue therapy than Group S at 48 h (7.03% vs 16.02%, p=0.007), suggesting a sustained antiemetic effect of cipepofol against delayed PONV.
In addition, our study showed that cipepofol is associated with an approximately 50% lower risk of hypotension compared with sevoflurane, indicating that cipepofol may provide more stable intraoperative hemodynamics. Previous research has demonstrated that a high incidence of hypotension may be attributed to a high incidence of PONV,31–33 which is consistent with our results. Furthermore, our study showed that, compared with the maintenance dose of 0.4 mg/kg/h in the combined group, the cipepofol group with a maintenance dose of 0.8 mg/kg/h had a lower incidence of PONV. The absolute difference in PONV incidence was approximately 10% at both 24 and 48 h, although these differences did not reach statistical significance (24h: 32.97% vs. 42.62%, p=0.056; 48 h: 35.68% vs 44.81%, p=0.074). The trend suggests a potential dose-dependent relationship for the antiemetic effect of cipepofol. Given the advantages of sevoflurane, such as its myocardial protective effects,34,35 the combination of low-dose cipepofol with sevoflurane may represent a practical balanced technique, particularly in settings where pure TIVA is not feasible or when the benefits of an inhaled agent are desired.
Our study is the first to compare cipepofol and sevoflurane in relation to PONV, contributing meaningfully to research on PONV management. However, several limitations exist. First, we did not analyze PONV incidence within 2 and 6 h after surgery. Second, the study included multiple surgical types with differing PONV risks. While this enhances generalizability, it may introduce confounding; the balanced distribution of procedures across groups reduces this risk. Finally, hemodynamic evaluation was limited to the intraoperative period and does not reflect postoperative stability. Future studies focusing on high-risk surgeries and including extended hemodynamic monitoring could provide more targeted insights.
Conclusion
This trial demonstrates that, in moderate- to high-risk patients, cipepofol monotherapy significantly reduces the incidence of PONV at 24 and 48 h and improves intraoperative hemodynamic stability compared with sevoflurane. Combination therapy showed intermediate effects. Cipepofol is an effective alternative for PONV prophylaxis; implementation should be guided by individual patient and surgical factors.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
This study was sponsored by Haisco Pharmaceutical Group Co., Ltd. and Special Research Fund (Grant No. 2020ZX02). The authors thank the patients who participated in this trial, as well as their families, and the investigators, study coordinators, study teams, and nurses.
Author Contributions
All authors made significant contributions to this work, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Medical and Health Research and Development Fund Project - Clinical and Basic Research Special Project (Project No. S182), sponsored by Beijing Kangmeng Charity Foundation.
Disclosure
The authors declare no competing interests in this work.
References
1. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2020;131(2):411–12. doi:10.1213/ANE.0000000000004833
2. Apfel CC, Läärä E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91(3):693–700. doi:10.1097/00000542-199909000-00022
3. Myles PS, Williams DL, Hendrata M, Anderson H, Weeks AM. Patient satisfaction after anaesthesia and surgery: results of a prospective survey of 10,811 patients. Br J Anaesth. 2000;84(1):6–10. doi:10.1093/OXFORDJOURNALS.BJA.A013383
4. Eberhart LHJ, Mauch M, Morin AM, Wulf H, Geldner G. Impact of a multimodal anti-emetic prophylaxis on patient satisfaction in high-risk patients for postoperative nausea and vomiting. Anaesthesia. 2002;57(10):1022–1027. doi:10.1046/J.1365-2044.2002.02822.X
5. Gan TJ, Diemunsch P, Habib AS, et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2014;118(1):85–113. doi:10.1213/ANE.0000000000000002
6. Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) society recommendations: 2018. World J Surg. 2019;43(3):1. doi:10.1007/s00268-018-4844-y
7. Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2017;35(28):3240–3261. doi:10.1200/JCO.2017.74.4789
8. Zhao Y, Qin F, Liu Y, Dai Y, Cen X. The safety of propofol versus sevoflurane for general anesthesia in children: a meta-analysis of randomized controlled trials. Front Surg. 2022;9:924647. doi:10.3389/fsurg.2022.924647
9. Shin JM, Park JS, Park BS, Lee YJ. The comparison of recovery characteristics following anesthesia with propofol, sevoflurane or isoflurane in adults undergoing outpatient surgery. Korean J Anesthesiol. 2004;46(2):213. doi:10.4097/KJAE.2004.46.2.213
10. Singh SK, Kumar A, Mahajan R, Katyal S, Mann S. Comparison of recovery profile for propofol and sevoflurane anesthesia in cases of open cholecystectomy. Anesth Essays Res. 2013;7(3):386–389. doi:10.4103/0259-1162.123259
11. Ahn H, Chae YJ, Kang S, Yi IK. Postoperative nausea and vomiting and recovery of heart rate variability following general anesthesia with propofol or sevoflurane: a randomized, double-blind preliminary study. Front Med. 2025;12:1575865. doi:10.3389/FMED.2025.1575865/BIBTEX
12. Yoo YC, Bai SJ, Lee KY, Shin S, Choi EK, Lee JW. Total intravenous anesthesia with propofol reduces postoperative nausea and vomiting in patients undergoing robot-assisted laparoscopic radical prostatectomy: a prospective randomized trial. Yonsei Med J. 2012;53(6):1197–1202. doi:10.3349/YMJ.2012.53.6.1197
13. Tramèr M, Moore A, McQuay H. Meta-analytic comparison of prophylactic antiemetic efficacy for postoperative nausea and vomiting: propofol anaesthesia vs omitting nitrous oxide vs total i.v. anaesthesia with propofol. Br J Anaesth. 1997;78(3):256–259. doi:10.1093/bja/78.3.256
14. Habib AS, Gan TJ. Evidence-based management of postoperative nausea and vomiting: a review. Can J Anesth. 2004;51(4):326–341. doi:10.1007/BF03018236
15. Visser K, Hassink EA, Bonsel GJ, Jeroen MRN, Cor JK. Randomized controlled trial of total intravenous anesthesia with propofol versus inhalation anesthesia with isoflurane-nitrous oxide postoperative nausea and vomiting and economic analysis. Anesthesiology. 2001;95(3):616–626. doi:10.1097/00000542-200109000-00012
16. Uchinami Y, Takikawa S, Takashima F, et al. Incidence of postoperative nausea and vomiting is not increased by combination of low concentration sevoflurane and propofol compared with propofol alone in patients undergoing laparoscopic gynecological surgery. JA Clin Rep. 2019;5(1). doi:10.1186/S40981-019-0292-4
17. Zhihao L, Lei L, Jianjun Y. Efficacy and safety of cipepofol in elderly patients undergoing thoracoscopic combined anesthesia. J Clin Anesthesiol. 2023;39(12):1276–1281.
18. Zhang H, Zhang M, Hao L, et al. Comparison of the effects of ciprofol and propofol on postoperative nausea and vomiting in patients undergoing outpatient hysteroscopy. Drug Des Devel Ther. 2024;18:5701–5707. doi:10.2147/DDDT.S489223
19. Comparison of predictive models in postoperative nausea and vomiting in patients undergoing breast cancer surgery | supportive Care in Cancer. Available from: https://link.springer.com/article/10.1007/s00520-024-08781-z.
20. Krishnan D, Asokan A, Muthalu A, Suganya S, Sujatha C. A comparative study on the efficacy of intravenous palonosetron versus a combination of ondansetron and dexamethasone as prophylaxis for prevention of postoperative nausea and vomiting after laparoscopic surgeries. Cureus. 2024;16;(10)doi:10.7759/cureus.72214
21. Tahir S, Mir AA, Hameed A. Comparison of palonosetron with granisetron for prevention of postoperative nausea and vomiting in patients undergoing laparoscopic abdominal surgery. Anesth Essays Res. 2018;12(3):636–643. doi:10.4103/aer.AER_84_18
22. Chen HP, Hsu YH, Hua KC, Lin CC, Lo YF, Yu HP. Comparison of sevoflurane versus propofol under auditory evoked potential monitoring in female patients undergoing breast surgery. Biomed J. 2013;36(3):125–131. doi:10.4103/2319-4170.113228
23. Kim EG, Park HJ, Kang H, Choi J, Lee HJ. Antiemetic effect of propofol administered at the end of surgery in laparoscopic assisted vaginal hysterectomy. Korean J Anesthesiol. 2014;66(3):210–215. doi:10.4097/KJAE.2014.66.3.210
24. Price ML, Walmsley A, Swaine C, Ponte J. Comparison of a total intravenous anaesthetic technique using a propofol infusion, with an inhalational technique using enflurane for day case surgery. Anaesthesia. 1988;43(84–87). doi:10.1111/J.1365-2044.1988.TB09081.X
25. Lebenbom-Mansour MH, Pandit SK, Kothary SP, Randel GI, Levy L. Desflurane versus propofol anesthesia: a comparative analysis in outpatients. Anesth Analg. 1993;76(5):936–941. doi:10.1213/00000539-199305000-00004
26. Liao J, Li M, Huang C, et al. Pharmacodynamics and pharmacokinetics of HSK3486, a novel 2,6-disubstituted phenol derivative as a general anesthetic. Front Pharmacol. 2022:13. doi:10.3389/FPHAR.2022.830791/PDF.
27. Zhao MJ, Hu HF, Li XL, Li XM, Wang DC, Kuang MJ. The safety and efficacy between remimazolam and propofol in intravenous anesthesia of endoscopy operation: a systematic review and meta-analysis. Int J Surg Lond Engl. 2023;109(11):3566–3577. doi:10.1097/JS9.0000000000000638
28. Habib AS, Gan TJ. Pharmacotherapy of postoperative nausea and vomiting. Expert Opin Pharmacother. 2003;4(4):457–473. doi:10.1517/14656566.4.4.457
29. Hayase T, Tachibana S, Yamakage M. Effect of sevoflurane anesthesia on the comprehensive mRNA expression profile of the mouse hippocampus. Med Gas Res. 2016;6(2):70–76. doi:10.4103/2045-9912.184715
30. Bansal T, Singhal S, Kundu K. Prospective randomized double-blind study to evaluate propofol and combination of propofol and sevoflurane as maintenance agents in reducing postoperative nausea and vomiting in female patients undergoing laparoscopic surgery. Med Gas Res. 2022;12(4):137–140. doi:10.4103/2045-9912.337994
31. Maleczek M, Laxar D, Geroldinger A, Kimberger O. Intraoperative hypotension is associated with postoperative nausea and vomiting in the PACU: a retrospective database analysis. J Clin Med. 2023;12(5). doi:10.3390/JCM12052009
32. Goss S, Jedlicka J, Strinitz E, et al. Association between intraoperative hypotension and postoperative nausea and vomiting: a retrospective cohort study. Curr Med Res Opin. 2024;40(8):1439–1448. doi:10.1080/03007995.2024.2373885
33. Nakatani H, Naito Y, Ida M, et al. Association between intraoperative hypotension and postoperative nausea and vomiting: a retrospective analysis of 247 thyroidectomy cases. Braz J Anesthesiol Elsevier. 2023;73(5):635–640. doi:10.1016/J.BJANE.2021.02.029
34. Guarracino F, Landoni G, Tritapepe L, et al. Myocardial damage prevented by volatile anesthetics: a multicenter randomized controlled study. J Cardiothorac Vasc Anesth. 2006;20(4):477–483. doi:10.1053/j.jvca.2006.05.012
35. De Hert SG, der Linden PJ V, Cromheecke S, et al. Cardioprotective properties of sevoflurane in patients undergoing coronary surgery with cardiopulmonary bypass are related to the modalities of its administration. Anesthesiology. 2004;101(2):299–310. doi:10.1097/00000542-200408000-00009
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.