Back to Journals » Advances in Medical Education and Practice » Volume 17
Promoting the Dissemination of 3D Printing Technology in Reconstructing Critical-Sized Defects of Long Bone and Vertebral Body Through a “Six-in-One” Targeted Teaching Method
Authors Liu B, Wang B ![]() , Wang Z, Li Y, Tian Y
, Wang Z, Li Y, Tian Y
Received 14 October 2025
Accepted for publication 24 January 2026
Published 13 March 2026 Volume 2026:17 566011
DOI https://doi.org/10.2147/AMEP.S566011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Bingchuan Liu,* Ben Wang,* Zhengguang Wang, Yang Li, Yun Tian
Department of Orthopaedics, Peking University Third Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang Li, Email [email protected] Yun Tian, Email [email protected]
Introduction: Three-dimensional (3D) printing technology has revolutionized the treatment of bone defects. However, medical education has lagged in integrating 3D printing into clinical training, limiting its widespread adoption. This study aimed to promote the dissemination of 3D printing technology through a novel, targeted teaching method.
Methods: First, we implemented a bibliometrics aiming to identify core research forces and potential breakthrough directions. Then, from January 2022 to January 2025, a prospective cohort of 278 trainees (102 residents and 176 fellows) at a single center participated in a structured six-stage educational program encompassing: (1) foundational 3D printing knowledge, (2) video-assisted learning, (3) hands-on practice with 3D printed anatomical models, (4) virtual reality (VR)-based surgical simulation, (5) multidisciplinary treatment (MDT) discussions, and (6) supervised surgical operations. Teaching effectiveness was evaluated using pre- and post-training theoretical exams, operational assessments, and comprehensive self-evaluation questionnaires.
Results: Through the bibliometrics, 3D printing technology has been maintaining a high level of research hotspot, but the targeted education is still vacant. For the teaching study, both resident and fellowship doctors demonstrated statistically significant improvements in theoretical knowledge scores, rising from 14.3 to 32.7 in residents and from 19.1 to 33.3 in fellows (P < 0.001). Residents exhibited a greater magnitude of improvement compared to fellows. Operational metrics showed significant reductions in completion time and intraoperative blood loss (P < 0.001), alongside a marked increase in the proportion of “excellent” or “good” procedural quality ratings. Comprehensive ability assessment revealed significant gains across all evaluated domains (P < 0.001), except for self-study ability, which remained stable The total self-evaluation scores improved from 19.5 to 30.1 for residents and from 20.9 to 33.6 for fellows.
Conclusion: This targeted, multimodal teaching method significantly enhances theoretical understanding, operative proficiency, and clinical competence in the use of 3D printing technology for bone defect repair.
Keywords: medical education, targeted teaching method, 3D printing technology, resident doctor, fellowship doctor
Introduction
During the past ten years, 3D printing technology has been widely acknowledged and implemented to repair bone defects in clinical practice.1,2 It can achieve anatomical shape matching and stable stress conduction, compensating for the shortcomings of traditional bone defect repair methods. However, medical education focusing on the use of 3D printing technology to repair bone defects lags behind. On the one hand, the slow pace of textbook updates makes it difficult for medical students to learn sufficient relevant knowledge in the classroom. On the other hand, in regions with uneven distribution of medical technology and resources, resident physicians also find it difficult to encounter 3D printing technology in clinical practice.
In recent years, the field of medical education has undergone continuous reform and innovation, particularly in teaching methods. Simulation-based learning (SBL), flipped classrooms (FC), problem-based learning (PBL), team-based learning (TBL), case-based learning (CBL), bridge-in, objective, pre-assessment, participatory learning, post-assessment, and summary (BOPPPS) all have effectiveness in improving learning quality and efficiency for medical students.3,4 However, there are currently no specific teaching methods for promoting the clinical application of 3D printing technology, which cannot meet the actual demand for the rapid clinical promotion and popularisation of 3D printing technology.
The application of 3D-printed models enhances the quality of teaching in orthopedic clinical settings. Rodrigues et al created the 3D models of nonunion fractures and found these models could represent the different manifestations that characterize this disease incur a low cost, and could be used for teaching such subjects as anatomy and surgery.5 More researchers have explored the integration of 3D printing technology with other teaching models. Wang et al integrated 3D printing and case-based learning in orthopedic residency education for geriatric hip fracture management. They indicated that this teaching method could enhance training effectiveness and learner satisfaction in geriatric hip fracture education, supporting its adoption in standardized orthopedic residency programs.6 Ali et al combined the BOPPPS (bridge-in, objective, preassessment, participatory learning, post assessment, summary) teaching model and 3D printing technology to address the spatial and practical challenges of orthopedic training. Through a comparative study, they found that integrating the BOPPPS teaching model with 3D printing technology enhanced theoretical knowledge, clinical skills, self-perceived competence, and student satisfaction in orthopedic education.7 Virtual reality (VR) technology also plays a significant role in improving the quality of orthopedic education. Coxe et al included twenty-three studies across six subspecialty areas to synthesize contemporary data assessing the efficacy of VR simulation in orthopedic surgical training. They demonstrated that trainees performed better in the VR simulation groups when compared to control education modalities, and participants readily embraced VR.8 Some researchers have also combined 3D printing technology with virtual reality technology for orthopedic education. Akgun et al assessed the effectiveness and safety of VR simulations for education of posterior spinal instrumentation, which was proved to be a promising solution for surgical education, particularly for junior residents, for improving the understanding of spinal instrumentation.9 Wang et al evaluated the pedagogical value of integrating 3D-printed model with mixed reality technology in clinical orthopaedic surgery education. They concluded that this integrated method could boosted student performance, learning efficiency, and overall teaching quality, demonstrating strong potential for wider application.10 However, current researches lack specific innovations in teaching methodologies for the disease of bone defect. The “six-in-one” targeted teaching method we propose represents a significant innovation and reform direction.
In our institution, 3D printing technology has been effectively applied in the repair of long bone and vertebral defects.11,12 In the process of clinical practice, we have established a targeted teaching method specifically for using 3D printing technology to repair bone defects. This targeted method included basic knowledge learning of 3D printing technology, video-assisted learning, 3D printed samples operation, VR-based surgery simulation, multi-disciplinary treatment (MDT), and actual surgical operation. This targeted teaching method specifically designed for 3D printing technology is reported for the first time in the literature.
With regard to the study design, we first analyzed the hot topics in medical education research based on bibliometrics and knowledge graph visualization. By constructing keyword clusters, and high-impact citation networks, we aimed to identify core research forces and potential breakthrough directions. Then, we summarized and compared the prospective teaching outcomes of resident physicians and fellowship physicians using the targeted teaching method. The study findings can provide valuable references for the clinical promotion teaching of other innovative technologies, such as robotic-assisted surgery, new-type biodegradable implants, and wearable devices.
Materials and Methods
Bibliometrics Analysis
We utilized the Web of Science database as the data source, the time span of literature search ranged from 2009 to 2025. The search query was constructed as: TS= ((3D printing OR three-dimensional printing OR additive manufacturing) AND (combined teaching OR targeted teaching OR hybrid teaching OR blended learning OR PBL OR CBL OR EBL OR Sandwich teaching OR case-based learning OR problem-based learning)). The inclusion criteria of literature included: (1) original research; (2) review (3) meta-analyses (4) case report (5) brief communications. The exclusion criteria of literature included: (1) non-peer reviewed materials (eg, preprints, conference abstracts, book chapters); (2) retracted publications; (3) non-English publications to ensure consistency in data processing. Extracted bibliometric parameters included: article title, publication year, citation frequency, source journal, publication type, keywords, and reference lists.
The extracted data were imported into CiteSpace (version 6.3. R1 Advanced Edition), Microsoft Excel, RStudio (version 4.4.2). CiteSpace, a pivotal analytical tool, employs visualized bibliometric methods to reveal latent insights within scientific literature. It generates scientific knowledge maps to intuitively illustrate the structure and distribution of scientific knowledge. We used the graphs of “map of keywords occurrence” “the clustering of keywords” “time dynamic evolution of keywords” “the top 15 keywords with the strongest citation bursts” to reflect the trends and hotspots related to our study.
Trainee Enrollment
This prospective study was initiated in January 2022 and was completed by January 2025. The anticipative included trainee was 166 according to the sample power calculation via statistical analysis. Actually, during the three years, we taught 278 trainees to use 3D printing technology to repair bone defects via the targeted teaching method. The trainees were divided into two groups, including 102 resident doctors and 176 fellowship doctors. The average age of the trainees in resident-doctor and fellowship-doctor groups was 26.8 and 42.8 years old, respectively. This study has been ethically approved by the Medical Science Research Ethics Committee of Peking University Third Hospital (No. M2018174).
“Six-in-One” Targeted Teaching Method
The “six-in-one” targeted teaching method specifically established for teaching 3D printing technology included the following six stages:
- Stage 1, basic knowledge learning of 3D printing technology. Trainees need to grasp the development history, operation technique, current clinical application status, and future directions via reading related books and literature. This stage of teaching combines offline classroom teaching with online network teaching, twice a month, each session lasting 90 minutes.
- Stage 2, video-assisted learning. We recorded some videos about the production process of 3D printed samples and the clinical application process of 3D printed samples for trainee learning. The instructor provides detailed explanations of the video content, twice a month, each session lasting 45 minutes.
- Stage 3, 3D printed samples operation (Figure 1). The 3D printed samples included guide plate, bone molds, and anatomical-shaped prostheses. Trainees can use these samples to perform in-vitro osteotomy, prosthesis implanting, and internal fixation. Twice a month, each session lasting 45 minutes.
- Stage 4, VR-based surgery simulation (Figure 2). Through medical-engineering interaction platform, trainees are able to simulate the process of prosthesis implanting and design appropriate fixation modes for diverse 3D printed prostheses. In the detailed operation procedure, three-dimensional CT scans of the skeleton were imported into Materialise Mimics Innovation Suite 21.0 software in DICOM data format for three-dimensional reconstruction. The bone segmentation module was used to identify normal bone and bone defect areas. Osteotomy guide design was performed using Materialise 3-matic 17.0, combined with 3D-printed prostheses and screw models to match the internal fixation pattern. After prosthesis implantation and internal fixation, we used the HyperMesh 14.0 software (Altair, Michigan, USA) and FEBio 3.7 software to finish the finite element analysis, in order to evaluate the feasibility and rationality for the established plan for bone defect repair. Twice a month, each session lasting 90 minutes.
- Stage 5, multi-disciplinary treatment (MDT). Common causes of bone defects include tumors, infections, non-union, and deformities. We have established specialized MDT teams to address bone defects caused by different factors. Trainees lead each case-based MDT, deepening their understanding of the disease through condition analysis, differential diagnosis, and treatment plan formulation. Once a month, each session lasting 90 minutes.
- Stage 6, actual surgical operation. Under the guidance of experienced specialists, trainees personally performed the 3D-printed prosthesis implantation and internal fixation to complete bone defect reconstruction. The patients were informed the whole study and the details of the surgical procedure and the personnel involved.
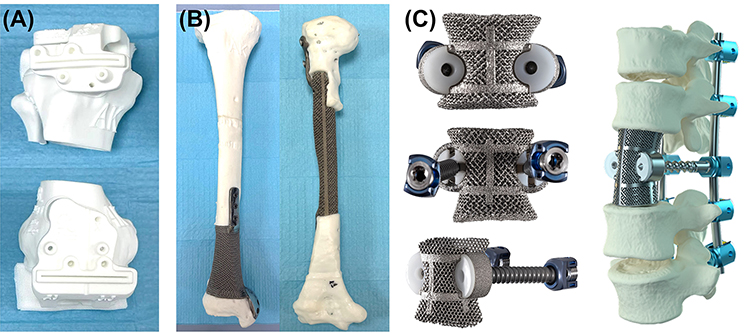 |
Figure 1 Teaching tools: (A) 3D printed osteotomy guide plate; (B) 3D printed resin molds and 3D printed titanium alloy prostheses for tibia and humerus; (C) 3D printed resin molds and 3D printed titanium alloy prostheses for spine. |
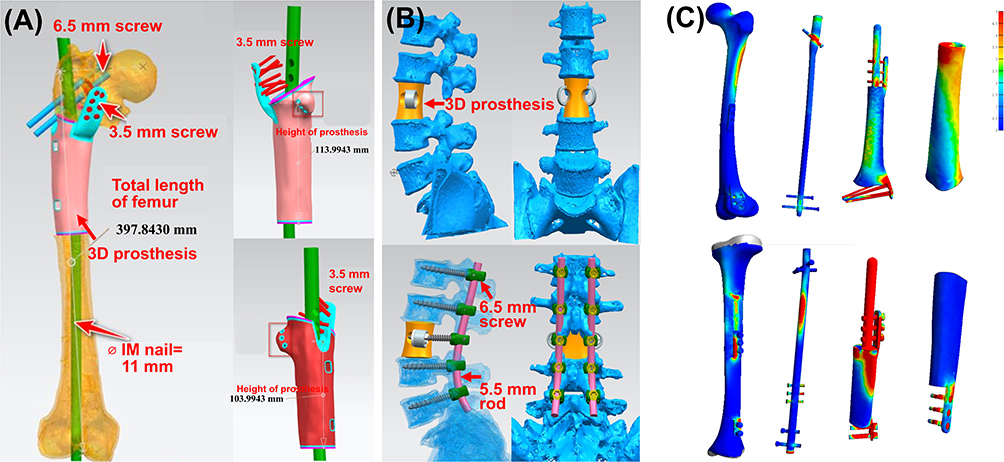 |
Figure 2 Simulation of surgical modeling and operation: (A) the implantation and internal fixation for using 3D printed prosthesis to repair a femoral defect; (B) the implantation and internal fixation for using 3D printed prosthesis to repair a lumbar defect; (C) finite element analysis. |
Assessment of Teaching Effect
We assessed the teaching effect by comparing the performance of the trainees from the same group before and after teaching. Assessment content include:
Theoretical Knowledge Assessment
Conducted in the form of a written examination. There are 25 multiple-choice questions, each worth 2 points, for a total of 50 points. The content covers basic concepts of 3D printing technology and diseases, case analysis, clinical diagnosis, disease classification, treatment decisions, etc.
Operation Assessment
We assessed the operation ability for osteotomy, 3D-printed prosthesis implantation, and internal fixation. The assessment indicators included completion time, completion quality, and blood loss volume. The completion quality was classified into three grades: excellent, good, and poor. The operative metrics were collected during live surgery. The amount of bleeding and the duration of the surgery were recorded by the anesthesiologist. The quality of the surgical operation was evaluated by the chief surgeon within the surgical team.
Comprehensive Ability Assessment
Trainees were asked to complete the questionnaire survey about their self-evaluation and satisfaction at the end of the teaching course. The questionnaire was modified and adopted by Zhao et al13 and Oderinu et al.14 The questionnaire with ten self-evaluation items involving clinical thinking ability, learning initiative, self-study ability, basic knowledge mastery, anatomical knowledge mastery, confidence in learning, ability to analyze and solve problems, comprehension of the knowledge, help to clinical thinking. Students graded the aspects based on a 5-point Likert scale, where each item was scored from 1 to 5 points, respectively.
Statistical Analysis
SPSS 22.0 software was used to complete the statistical analysis. The measurement data were expressed as  + SD. Data were assessed by independent sample t-test. The categorical data were analyzed by the chi-square test. P <0.05 was considered statistically significant.
+ SD. Data were assessed by independent sample t-test. The categorical data were analyzed by the chi-square test. P <0.05 was considered statistically significant.
Results
The keyword co-occurrence network (Figure 3A) identified high-frequency and high-centrality keywords, including 3D printing, additive manufacturing, medical education, education, augmented reality, and so on. Cluster analysis grouped keywords into 10 thematic clusters (Figure 3B), such as #0 3D printing, #1 additive manufacturing, #2 engineering education, #3 information technology, #4 three-dimensional displays, #5 3D imaging techniques. Timeline visualization (Figure 3C) showed thematic clusters shifts: 3d printing and additive manufacturing dominated from 2015 to 2025 with the longest time span; #6 surgical simulation, #7 primate brain, #8 multispecies architecture, and #9 design education gradually emerged during the past five years. Burst detection (Figure 3D) highlighted emerging keywords like “surgery”, “models”, “technology” and “virtual reality” “maching learning” (2009–2025), signaling current and future research directions.
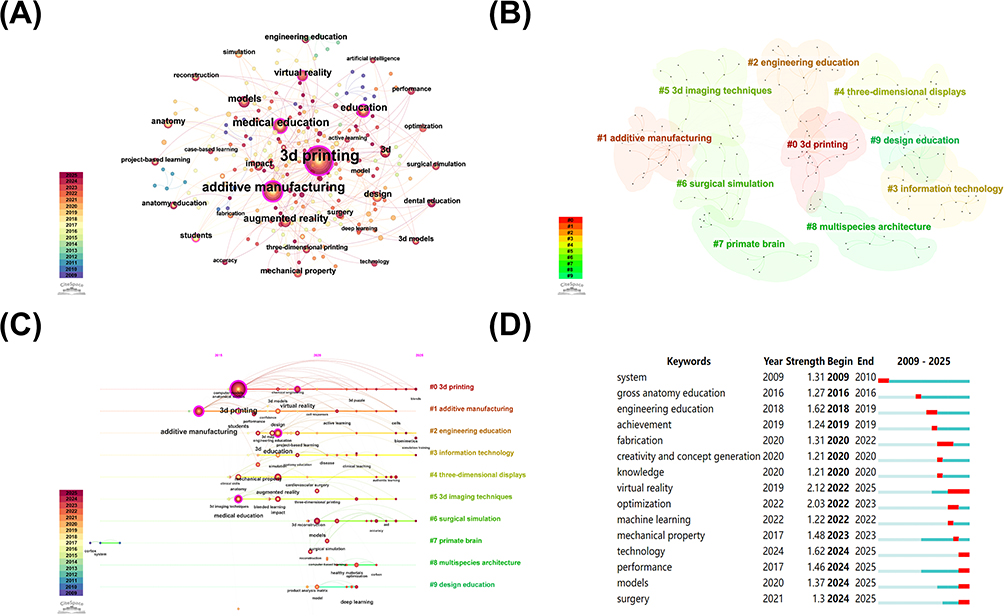 |
Figure 3 Visualization graphs of bibliometrics analysis: (A) map of keywords occurrence; (B) the clustering of keywords; (C) time dynamic evolution of keywords; (D) top 15 keywords with the strongest citation bursts. |
In the aspect of theoretical knowledge assessment, the scores of doctors from both groups significantly improved (P < 0.001), from mean 14.3 to 32.7 in resident-doctor group and from mean 19.1 to 33.3 in fellowship-doctor group (Tables 1 and 2). The initial mean score of resident doctors was lower than those fellowship doctors, and resident doctors achieved a higher increase.
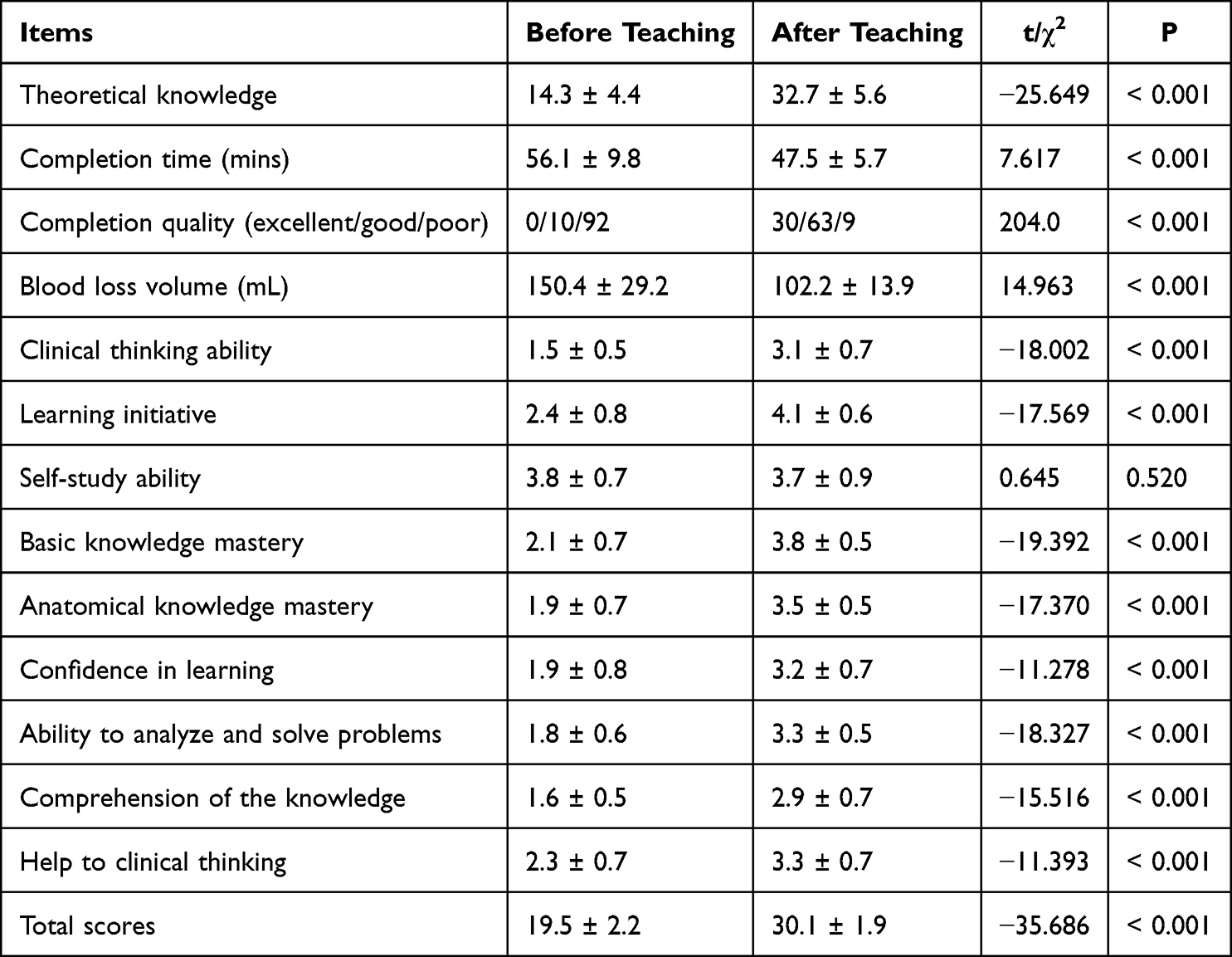 |
Table 1 Evaluation of the Teaching Effectiveness of Resident Doctors |
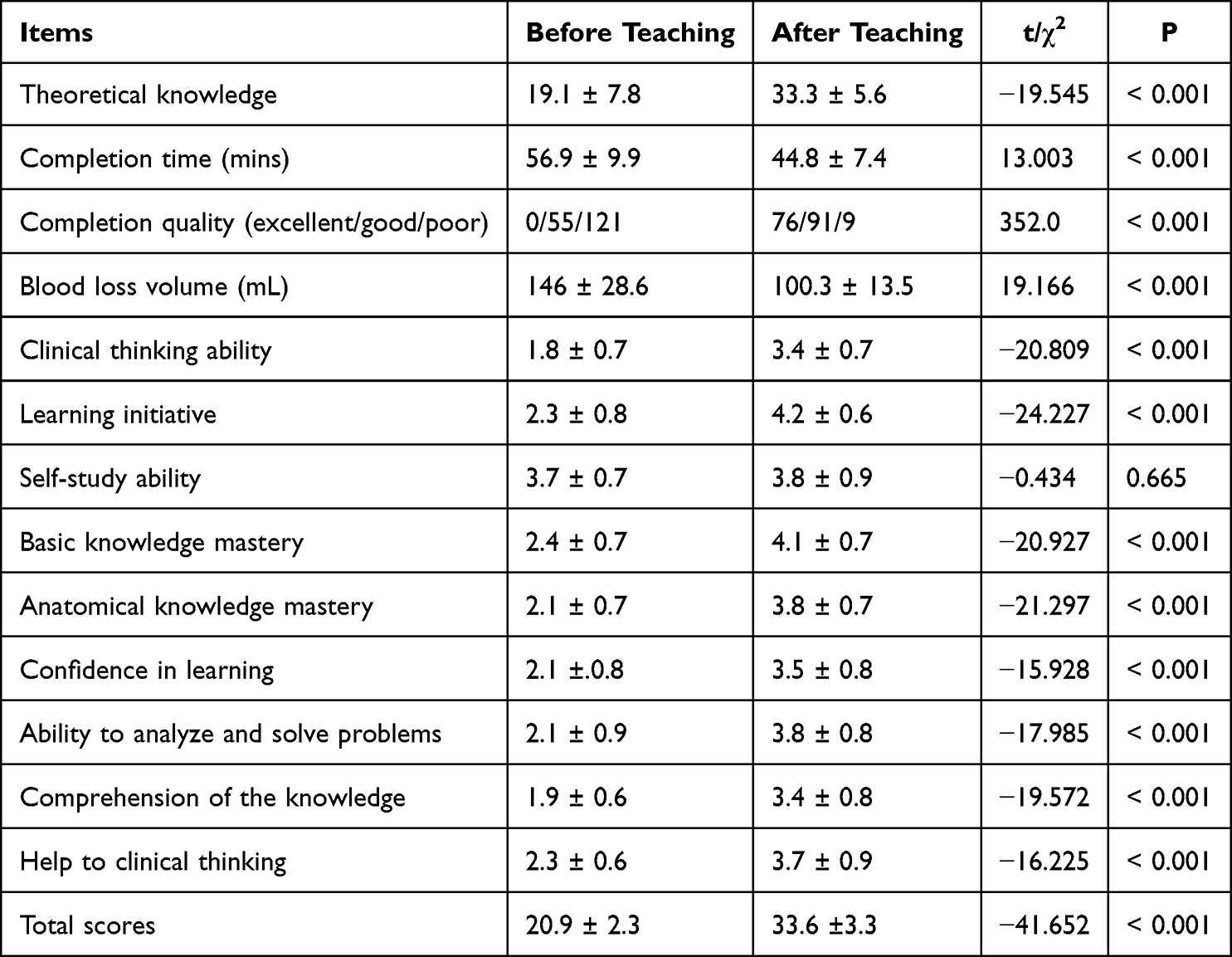 |
Table 2 Evaluation of the Teaching Effectiveness of Fellowship Doctors |
In the aspect of operation assessment, the completion time and blood loss volume of doctors from both groups significantly decreased (P < 0.001) (Tables 1 and 2). Besides, the completion quality also significantly improved (P < 0.001). After targeted teaching, the total excellent and good rate of operation of resident and fellowship doctors were 91.2% and 91.9%, respectively.
In the aspect of comprehensive ability assessment, the scores of clinical thinking ability, learning initiative, basic knowledge mastery, anatomical knowledge mastery, confidence in learning, ability to analyze and solve problems, comprehension of the knowledge, and help to clinical thinking for doctors from both groups significantly improved (P < 0.001) (Tables 1 and 2). The score of self-study ability both remained relatively stable (P > 0.05). For the total score of the 9 items of comprehensive ability assessment, doctor from both groups achieved significant improvement (P < 0.001), from mean 19.5 to 30.1 in resident-doctor group and from mean 20.9 to 33.6 in fellowship-doctor group.
Discussion
According to the results of bibliometric analysis, 3D printing technology has maintained a high level of research hotspot over the past decade. But researchers have commonly used 3D printing technology as an auxiliary tool in medical education without conducting targeted education on 3D printing technology itself. To our knowledge, this is the first educational study specially on the application and promotion of 3D printing technology in the treatment of bone defects.
In this study, towards resident and fellowship doctors, we conducted a structured, six-stage curriculum combining education, digital media, simulation-based learning, MDT engagement, and hands-on surgical experience. This highly-targeted teaching method conforms with the concept of precision medicine teaching. In 2023, Triola MM and Burk-Rafel J put forward the framework of precision medicine teaching,15 they emphasized that the necessity to develop targeted new skills needed by learners. Furthermore, Drake et al demonstrated that the implementation of precision education strategy could fill residents’ experiential gaps and complement strengths with targeted educational interventions.16 The findings of this study further provided robust evidence to support the implementation of targeted teaching method in medical education, particularly in high-tech and interdisciplinary domains such as 3D printing.
In terms of theoretical knowledge acquisition, both resident and fellowship doctors exhibited statistically significant improvements (P < 0.001). Although the fellowship group began with a higher baseline score, resident doctors achieved a greater magnitude of improvement, indicating that the targeted teaching method is especially effective for early-career learners in theoretical knowledge education. This is consistent with previous studies showing that early immersion in clinical simulation and technical content accelerates knowledge acquisition in junior learners.17,18 Medical education has been drastically changing for both resident and fellowship doctors.19 These two types of doctors have different knowledge foundations and training needs, requiring us to tailor our teaching methods precisely. We adopt a combination of online and offline methods when teaching theoretical knowledge, offering flexibility and reinforcement through repetition and accessibility to both levels of doctors.
Operational assessment results further confirmed the effectiveness of the targeted teaching method. There was a significant reduction in both completion time and intraoperative blood loss (P < 0.001), indicating improved procedural efficiency and safety. Furthermore, the total “excellent and good” operation quality rate exceeded 91% in both groups after training, which strongly supports the model’s capacity to enhance technical proficiency. Prior research has shown that simulation-based training, particularly with patient-specific 3D printed models, enhances surgical precision and reduces intraoperative complications.20,21 As recommended by Quek et al,22 educators must recognize that there is no “one-size-fits-all” approach, and a flexible multimodal strategy is necessary to meet diverse learning needs. We combined the digital simulation with actual operation for two-level educational purposes, achieving a unified goal to improve their operational skills.
The comprehensive ability assessment revealed significant improvement across a range of critical competencies, including clinical thinking, learning initiative, anatomical and basic knowledge mastery, confidence, and problem-solving ability (P < 0.001). Interestingly, self-study ability did not show significant change (P > 0.05), likely because the structured format provided consistent external guidance, thus limiting opportunities for independent exploration. As required by Accreditation Council for Graduate Medical Education,23 the self-study is a useful way to assess program strengths and weaknesses in the context of current environmental and institutional factors, and helps develop an effective framework for improvements geared at achieving program aims and taking the program to the next level. Nevertheless, the overall scores increased from 19.5 to 30.1 in the resident group and from 20.9 to 33.6 in the fellowship group, further affirming the educational value of this targeted method. These findings echo the importance of multimodal training strategies in enhancing both technical and cognitive domains of surgical education.24,25
Our teaching model stands out by integrating core knowledge, video learning, hands-on 3D model manipulation, VR-based simulation, MDT discussion, and supervised surgical practice—forming a coherent, progressive framework. This aligns with principles of competency-based medical education (CBME), which emphasizes measurable skill development and integration of learning modalities.26,27 Kj et al28 used a similar teaching method with simulation based learning on knowledge and skills among medical students undergoing, they demonstrated that this targeted teaching method could improve both immediate clinical performance and long-term skill retention significantly.
As 3D printing becomes an integral tool in orthopedic and reconstructive surgery, it is imperative that medical education systems adapt accordingly. The strength of this targeted teaching method lies in its holistic design. Educationally, the results support broader implementation of targeted curricula for surgical trainees, especially in emerging technological domains. Traditional lecture-based models may fall short in conveying the complexity of interdisciplinary, patient-specific innovations. In contrast, the targeted teaching method presented here supports not only knowledge acquisition but also the development of practical and cognitive skills essential for safe, effective clinical application. Besides, our “six-in-one” teaching method, developed specifically for bone defect disease, has rarely been reported in previous research and remains unparalleled in the field of orthopedic education, demonstrating significant innovation and pioneering value.
Despite these strengths, the study still has some limitations that should be acknowledged. First, as a single-center study, the size of enrolled doctors was relatively small, which may limit the generalizability of the findings to broader populations. Second, the absence of a control group prevents direct comparison with traditional teaching methods, making it difficult to fully evaluate the specific effectiveness of the targeted teaching approach. Future multicenter studies with larger participant cohorts and randomized controlled designs would help address these limitations and provide more robust evidence.
Conclusion
In summary, the targeted teaching method markedly improved trainee performance across theoretical, surgical, and innovative domains. It offers a scalable and adaptable educational model to support the wider dissemination of 3D printing applications in orthopedic surgery. As such technologies become increasingly embedded in clinical workflows, equipping trainees with the necessary competencies through structured and immersive training is essential for future surgical innovation.
Acknowledgments
Bingchuan Liu and Ben Wang are co-first authors for this study. We thank Niu Xiaoyan for her help in collecting data.
Funding
This study was funded by Peking University Health Science Center Medical Education Research (2025YB16) and Funding Project Beijing Municipal Science & Technology Commission (No. Z181100001718195).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kelly C, Adams SB Jr. 3D printing materials and technologies for orthopaedic applications. J Orthop Trauma. 2024;38(4S):S9–9. doi:10.1097/BOT.0000000000002765
2. Wong RMY, Wong PY, Liu C, et al. 3D printing in orthopaedic surgery: a scoping review of randomized controlled trials. Bone Joint Res. 2021;10(12):807–819. doi:10.1302/2046-3758.1012.BJR-2021-0288.R2
3. Ma X, Zeng D, Wang J, Xu K, Li L. Effectiveness of bridge-in, objective, pre-assessment, participatory learning, post-assessment, and summary teaching strategy in Chinese medical education: a systematic review and meta-analysis. Front Med Lausanne. 2022;9:975229. doi:10.3389/fmed.2022.975229
4. Zhang SL, Ren SJ, Zhu DM, et al. Which novel teaching strategy is most recommended in medical education? A systematic review and network meta-analysis. BMC Med Educ. 2024;24(1):1342. doi:10.1186/s12909-024-06291-4
5. Rodrigues KEM, Lucas KDA, Cordeiro ALL, Silva RPM, Santos FGA, De carvalho YK. 3D models of nonunion fractures in long bones as education tools. Braz J Vet Med. 2021;43:e114820. doi:10.29374/2527-2179.bjvm114820
6. Wang H, Yang T, Hua W, Zhang W, Lu L. Integrated 3D printing and case-based learning in orthopedic residency education for geriatric Hip fracture management. Front Surg. 2025;12:1659207. doi:10.3389/fsurg.2025.1659207
7. Ali KA, Zhang J, Xia Z, et al. Enhancing orthopedic education in China with the BOPPPS teaching model and 3D printing technology: a comparative study. 3D Print Med. 2025. doi:10.1186/s41205-025-00308-4
8. Coxe FR, Stauffer TP, Ast MP. Virtual reality simulation in orthopedic surgery education improves immediate procedural skill and knowledge acquisition, but evidence on cost-effectiveness and skill retention remains lacking. Curr Rev Musculoskelet Med. 2025;18(10):363–378. doi:10.1007/s12178-025-09973-8
9. Akgun MY, Baran O, Ogretmen E, et al. Use of 3- dimensional modeling and virtual reality in the education of posterior spinal instrumentation. Turk Neurosurg. 2024;34(6):958–965. doi:10.5137/1019-5149.JTN.46204-24.1
10. Wang H, Xu A, Hua W, Ye Z, Lu L. Application of a hybrid virtual-physical teaching model integrating mixed reality and 3D printing in clinical joint orthopedic education. Front Surg. 2025;12:1638619. doi:10.3389/fsurg.2025.1638619
11. Zhou H, Liu S, Li Z, et al. 3D-printed vertebral body for anterior spinal reconstruction in patients with thoracolumbar spinal tumors. J Neurosurg Spine. 2022;37(2):274–282. doi:10.3171/2022.1.SPINE21900
12. Hou G, Liu B, Tian Y, et al. An innovative strategy to treat large metaphyseal segmental femoral bone defect using customized design and 3D printed micro-porous prosthesis: a prospective clinical study. J Mater Sci Mater Med. 2020;31(8):66. doi:10.1007/s10856-020-06406-5
13. Zhao W, He L, Deng W, Zhu J, Su A, Zhang Y. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ. 2020;20(1):381. doi:10.1186/s12909-020-02306-y
14. Oderinu OH, Adegbulugbe IC, Orenuga OO, Butali A. Comparison of students’ perception of problem-based learning and traditional teaching method in a Nigerian dental school. Eur J Dent Educ. 2020;24(2):207–212. doi:10.1111/eje.12486
15. Triola MM, Burk-Rafel J. Precision medical education. Acad Med. 2023;98(7):775–781. doi:10.1097/ACM.0000000000005227
16. Drake CB, Rhee DW, Panigrahy N, et al. Toward precision medical education: characterizing individual residents’ clinical experiences throughout training. J Hosp Med. 2025;20(1):17–25. doi:10.1002/jhm.13471
17. Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA. 2011;306(9):978–988. doi:10.1001/jama.2011.1234
18. Haskins IN, Tan WH, Zaman J, et al. Current status of resident simulation training curricula: pearls and pitfalls. Surg Endosc. 2024;38(9):4788–4797. doi:10.1007/s00464-024-11093-2
19. Sofka CM. Developments and innovations in resident and fellowship education: review article. HSS J. 2014;10(3):225–229. doi:10.1007/s11420-014-9396-6
20. Thiruchandran G, Dean O, Alim D, Crawford A, Salim O. Three-dimensional printing in orthopaedic surgery: a review of current and future applications. J Orthop. 2024;59:22–26. doi:10.1016/j.jor.2024.07.013
21. Tack P, Victor J, Gemmel P, Annemans L. 3D-printing techniques in a medical setting: a systematic literature review. Biomed Eng Online. 2016;15(1):115. doi:10.1186/s12938-016-0236-4
22. Quek FF, Meldrum S, Hislop J. A systematic scoping review of the current applications of digital technology in undergraduate surgical education. Cureus. 2025;17(1):e77278. doi:10.7759/cureus.77278
23. Maniar KP, Arva N, Blanco LZ Jr, et al. Accreditation council for graduate medical education self-study for pathology: one institution’s experience and lessons learned. Arch Pathol Lab Med. 2019;143(10):1271–1277. doi:10.5858/arpa.2018-0467-RA
24. Davidson EL, Penniston KL, Farhat WA. Advancements in surgical education: exploring animal and simulation models in fetal and neonatal surgery training. Front Pediatr. 2024;12:1402596. doi:10.3389/fped.2024.1402596
25. Barsom EZ, Graafland M, Schijven MP. Systematic review on the effectiveness of augmented reality applications in medical training. Surg Endosc. 2016;30(10):4174–4183. doi:10.1007/s00464-016-4800-6
26. Alharbi NS. Evaluating competency-based medical education: a systematized review of current practices. BMC Med Educ. 2024;24(1):612. doi:10.1186/s12909-024-05609-6
27. Schumacher DJ, Gielissen K, Kinnear B. Competency-based medical education: connecting training outcomes to patient care. Curr Probl Pediatr Adolesc Health Care. 2024;54(10):101675. doi:10.1016/j.cppeds.2024.101675
28. Kj DP, R K, Dgsr KM, Reddy YN, A SR. Impact of simulation based learning on knowledge and skills among medical students undergoing competency based medical education. Cureus. 2025;17(7):e88749. doi:10.7759/cureus.88749
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.