Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Promoting Community Pharmacy Practice for Chronic Obstructive Pulmonary Disease (COPD) Management: A Systematic Review and Logic Model
Authors Hu Y, Yao D ![]() , Ung COL
, Ung COL ![]() , Hu H
, Hu H ![]()
Received 24 March 2020
Accepted for publication 3 July 2020
Published 3 August 2020 Volume 2020:15 Pages 1863—1875
DOI https://doi.org/10.2147/COPD.S254477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Yuqi Hu, Dongning Yao, Carolina Oi Lam Ung, Hao Hu
State Key Laboratory of Quality Research in Chinese Medicine, Institute of Chinese Medical Sciences, University of Macau, Macau, People’s Republic of China
Correspondence: Carolina Oi Lam Ung; Hao Hu
State Key Laboratory of Quality Research in Chinese Medicine, Institute of Chinese Medical Sciences, University of Macau, N22-2057, Taipa, Macau. People’s Republic of China
Tel +853 88228538
Email [email protected]; [email protected]
Purpose: This study aimed 1) to identify and analyse the professional services provided by community pharmacists for chronic obstructive pulmonary disease (COPD) management; and 2) to develop a logic model for community pharmacy practice for COPD management.
Methods: A systematic review with a logic model was applied. English-language databases (PubMed, Web of Science, Embase, and Scopus) and a Chinese database (CNKI) were searched for articles published between January 2009 and June 2019. Studies concerning pharmacists and COPD were identified to screen for studies that focused on professional services provided at a community pharmacy level. Evidence on economic, clinical, and humanistic outcomes of interventions was summarized.
Results: Twenty-five articles were included in this study. Four categories of COPD-related interventions by community pharmacists were identified: 1) primary prevention; 2) early detection; 3) therapy management; and 4) long-term health management. The most common outputs examined were improvement in inhaler technique, medication adherence, and rate of smoking cessation. The clinical (improved quality of life, reduced frequency and severity of symptoms and exacerbation), humanistic (patient satisfaction), and economic (overall healthcare costs) outcomes were tested for some interventions through clinical studies. Contextual factors concerning pharmacists, healthcare providers, patients, facilities, clinic context, and socio-economic aspects were also identified.
Conclusion: Studies in the literature have proposed and examined different components of professional services provided by community pharmacists for COPD management. However, relationships among outcomes, comprehensive professional services of community pharmacists, and contextual factors have not been systematically tested. More well-designed, rigorous studies with more sensitive and specific outcomes measures need to be conducted to assess the effect of community pharmacy practice for COPD management.
Keywords: community pharmacy, community pharmacist, chronic obstructive pulmonary disease, COPD, systematic review, logic model
Introduction
Chronic obstructive pulmonary disease (COPD) has been a major challenge in the field of public health worldwide because of its high morbidity and mortality rates. In 2012, more than 3 million people worldwide died of this disease and its complications, and it is expected to be the third leading cause of death by 2030.1 COPD cannot be cured, as a chronic progressive disease, but it can be controlled at a relatively stable stage after effective treatment.2 However, most patients with COPD cannot control the progress of the disease effectively. One of the key reasons for this is that patients face many medication-related problems, including low medication adherence rates,3,4 inability to use inhaler devices correctly,5 and failure to take medication properly.6 The medication-related issues that COPD patients face and the consistent care that they need to manage their chronic conditions highlight the importance of the professional role of pharmacists.7
The responsibility of the pharmacist is no longer simple drug-adjustment work, but has been expanded to become patient-centric diversified health management.8,9 The situation is particularly prominent in COPD, in which the roles of pharmacist had been expanded to encompass prevention, screening potential patients, disease counselling, comprehensive disease management, and education.10–12 Studies have demonstrated that COPD patients benefit from multifactorial intervention by clinical pharmacists, including improvement of their COPD knowledge, medication adherence, and quality of life; and decreases in the hospitalization rate and exacerbations.13,14 However, a thorough understanding of the role of community pharmacists in COPD management is comparatively scarce.
Being positioned as the first point of contact with the healthcare service and medical experts, community pharmacists are uniquely placed to help manage each stage of COPD.15–18 However, the components of professional services provided by community pharmacists for COPD patients, health-related outcomes from community pharmacist interventions, and the impact of contextual factors vary in the existing literature.19 There is a need to comprehensively review and summarize community pharmacists’ contribution to COPD management into a theoretical structure to guide the planning and implementation of community pharmacist’s’ professional services for COPD patients in community settings.
Thus, the aim of this research was to identify and analyse the professional services provided by community pharmacists for patients with COPD, the outcomes of such services, and contextual factors affecting the practice, using a systematic literature review guided by the logic modelling approach. It is expected that the findings could help to guide the future development and implementation of professional services of community pharmacists in COPD management.
Methods
Search Strategy
This systematic review was performed according to the PRISMA guidelines for searching the literature. The literature search was conducted in June 2019. Articles published from January 2009 to June 2019 were included.
Four English-language databases (PubMed, Web of Science, Embase, and Scopus) and one Chinese database (CNKI) were searched for peer-reviewed research published between January 2009 and June 2019. The three primary search terms were “pharmacy or pharmacist”, “COPD”, and “professional service”. As shown in Table 1, the operational definition used for these three primary terms referred to “pharmacy or pharmacist” as the location or provider of COPD management intervention, “COPD” as COPD-related vocabularies, and “professional service” as the intervention provided associated with COPD management. MeSH terms and keywords were used to develop a comprehensive search strategy and to ensure the validity of the strategy. Terms within “pharmacy or pharmacist”, “COPD”, and “professional service” were combined with OR, and the following results from each concept were combined with AND. In addition, reference lists and citations of the included studies in this review were examined in an attempt to identify additional papers relevant for inclusion. For the Chinese literature, the search strategy was translated into Chinese and employed in a similar manner.
 |
Table 1 Search Term Identifiers |
Inclusion and Exclusion Criteria
For study selection, the following inclusion criteria were used: 1) community pharmacists should be the main intervention providers; 2) the main target disease is COPD; 3) it must include specific services or interventions provided by community pharmacists; and 4) it should be original research, but with no limits on research methods. Exclusion criteria included: 1) the main location for implementation was a hospital; 2) research was specific to a certain drug; and 3) review articles.
Study Selection Procedure
Figure 1 presents the whole study selection procedure. First, we acquired 9971 articles from the English literature and 263 from the Chinese literature. Second, we excluded the duplicated literature and obtained 6391 independent records. Third, we screened the remaining records by applying the inclusion criteria mentioned in the previous subsection, and obtained 32 records that potentially met the requirements. Fourth, we excluded 10 of the records after full-text reading. Fifth, we included another 3 papers from the references of the selected articles.
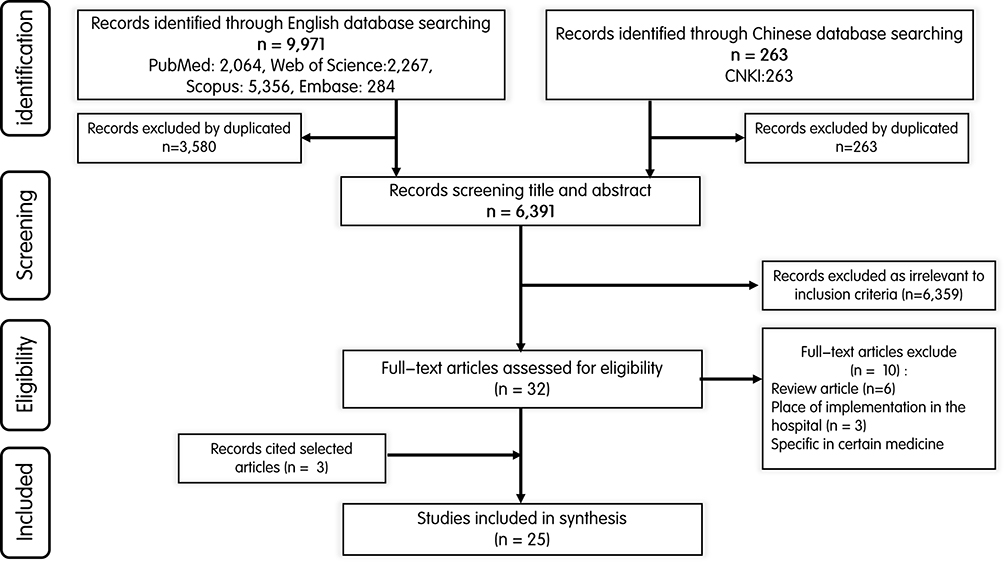 |
Figure 1 Study selection procedure. |
This screening process was completed by two authors (YH and DY) independently. When there was a conflict between the two authors’ opinions, the selected literature was further discussed, and another researcher (COLU) participated in the ruling to jointly determine the final included literature. In the end, no Chinese literature met the selection criteria, and 25 English literature articles were used for the final analysis.
Data Extraction and Analysis
Data were extracted using four extraction tables (Tables 2–6), where the basic information on the article, intervention from pharmacists, outputs, outcomes, and contextual factors were compiled and extracted.
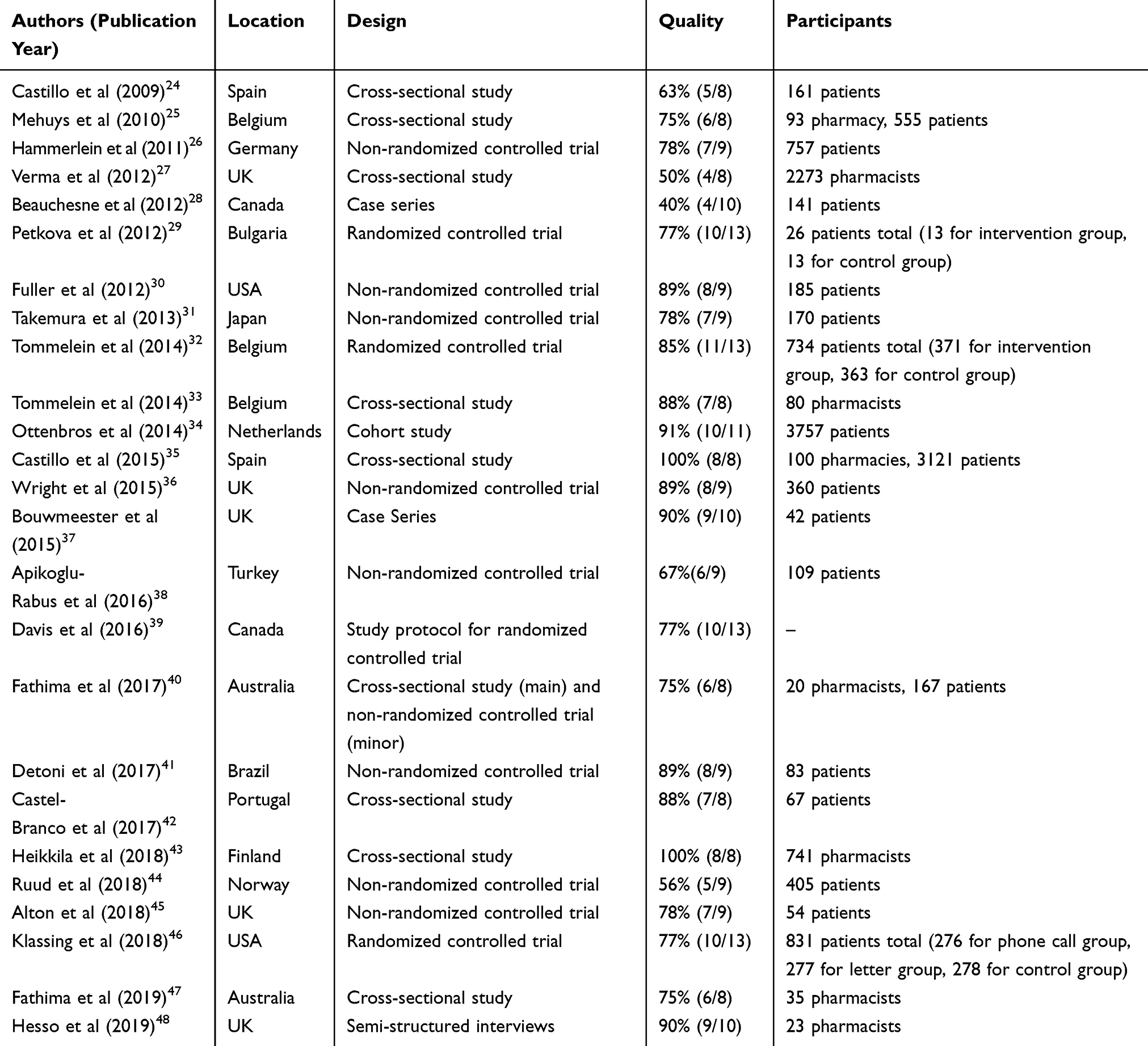 |
Table 2 Summary of Basic Information of Selected Articles |
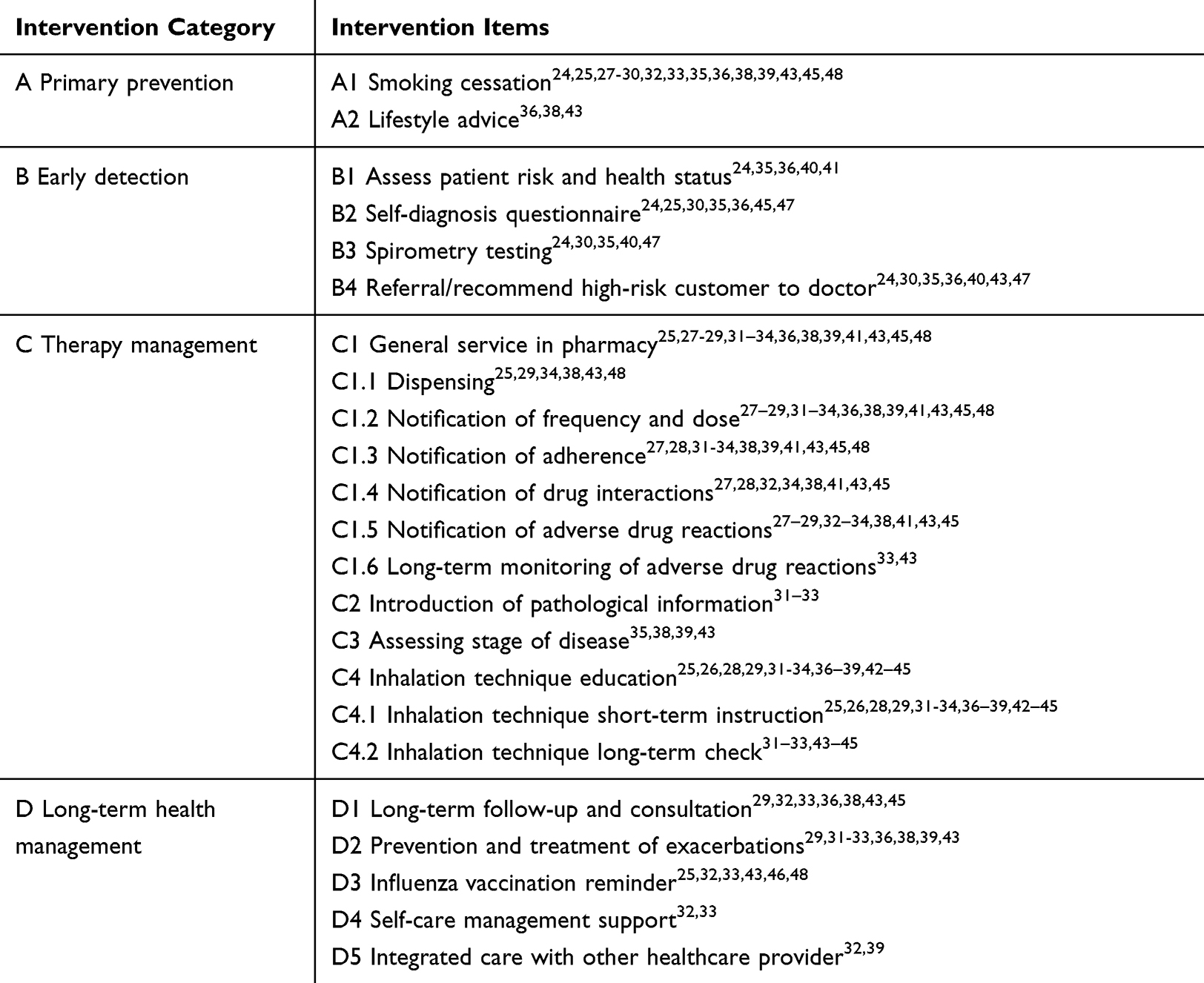 |
Table 3 Interventions Conducted by Pharmacists |
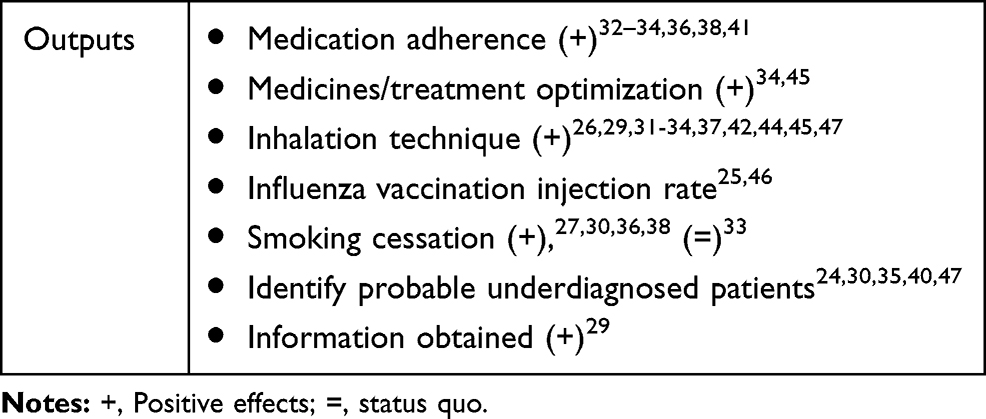 |
Table 4 Outputs of Pharmacist Intervention |
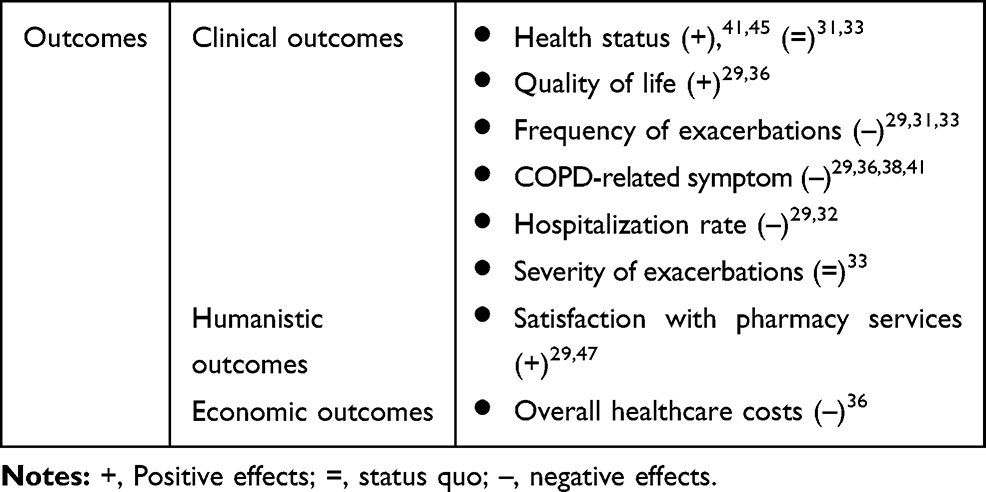 |
Table 5 Outcomes of Pharmacist Intervention |
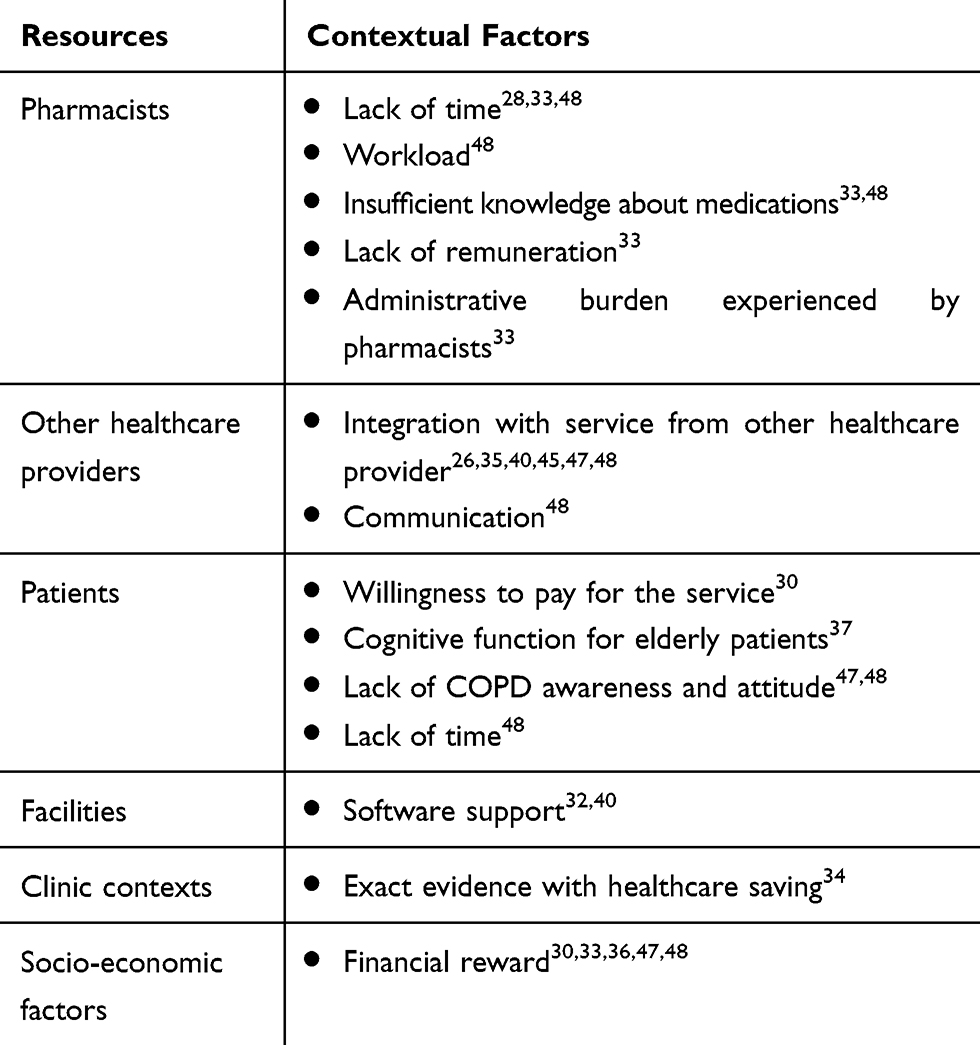 |
Table 6 Contextual Factors for Pharmacist Intervention |
For professional services, we integrated the models of the International Pharmaceutical Federation (FIP)10 and van der Molen,18 which specified the definition of services for COPD provided by community pharmacists. The services were classified into four categories according to the previous research: 1) primary prevention: pharmacists are ideally placed to provide information on disease awareness and risk prevention campaigns; 2) early detection: pharmacists play an important role in the early identification of patients with COPD; 3) therapy management: pharmacists can assist patients on drug-related issues during treatment; and 4) long-term health management: pharmacists play a role in monitoring adherence and ongoing inhaler technique in patients with COPD.18 For output and outcome, the Economic, Clinical, and Humanistic Outcomes (ECHO) model was used to summarize the economic, clinical, and humanistic outputs and outcomes.19 All of the outputs and outcomes about COPD have been confirmed in previous research.21,22
Study Appraisal
Considering the diversity of the study types included in this review, the Critical Appraisal Tools developed by the Joanna Briggs Institute (JBI) were applied as an evaluation tool to critically assess the methodological quality and risk of bias.23 The JBI tools, which evaluate the risk of bias from different aspects, include checklists of 6–13 questions, depending on the type of research methodology. There are four options for the assessment answers to each items on the JBI checklists: “Yes”, “No”, “Unclear”, and “Not applicable”. For the purpose of this study, we considered the option “Unclear” as equivalent to the option “No”, while the option “Not applicable” was considered equivalent to the option “Yes”. For the convenience of normalizing the calculation of the overall score for each study, either “Unclear” or “No” in the response would score 0 points for that specific item, while “Not applicable” or “Yes” would score 1 point.
Two authors (YH and DY) evaluated each article independently, based on the JBI tool. If there was a conflict in the evaluation result between the two authors’ opinions, an independent third researcher (COLU) participated in the evaluation process and made the final decision. The quality of all studies was classified as good quality, fair quality, or poor quality based on the degree to which they satisfied the checklists. Research was considered good quality if the study met all items on the checklist; a study was considered fair quality if it satisfied 70% or more of total items; and a study was considered poor quality if the it satisfied less than 70% of all the items on the corresponding checklists.
Results
Included Studies
As shown in Table 2, 25 studies published in English met the criteria and were included in the systematic review. With regard to the method of the article, 13 (52%) of the literature results were observational studies, including 9 cross-sectional studies, 2 case series, 1 cohort study, and 1 interview research; 10 (40%) of them were experimental studies, including 7 non-randomized controlled trials, 3 randomized controlled trials (RCTs), 1 study protocol for an RCT and 1 study that used cross-sectional research and an RCT in a mixed method. Fifteen countries were involved in the studies, with the most common study locations including the UK (n=5), Belgium (n=3), Australia (n=2), Canada (n=2), Spain (n=2), and the USA (n=2). The included studies involved both patient and pharmacist as participants, in which patients alone were involved in 17 of the included studies (68%), pharmacists alone were involved in 6 studies (24%), and both patients and pharmacists were involved in 2 studies (8%).
Study Quality
Among the 25 included studies, 2 cross-sectional studies26,34 were deemed to have good quality, having full compliance to the corresponding checklist; 18 studies were considered as having fair quality, as most of them were found to have non-compliance to at least 2 items on the corresponding checklists. Major methodological flaws were noted in 5 studies (comprising 2 cross-sectional studies, 2 non-randomized control studies, and 1 case series), which were evaluated as having poor quality (see Supplementary material 1). Despite the variations in the study quality, considering the purpose of this study, which was to provide a broad overview of the current understanding about community pharmacists’ role in COPD management (including the contextual factors, types of interventions, and possible output and outcomes) but not to evaluate the effectiveness of the interventions, all of the studies were included for further analysis.
Professional Services
Primary Prevention
Primary prevention was suggested as a role for community pharmacist practice. Regarding the responsibility of pharmacists, on the one hand, the pharmacist should provide health education for potentially high-risk patients and encourage people, especially those who show airway obstruction and a history of lung disease, to cease smoking.24,35,36 On the other hand, for patients already diagnosed with COPD, the pharmacist needs to ask them whether they smoke, inform them about the risks of smoking, and encourage them to quit .25,27-30,32,33,38,39,43,45,48 Other high-risk factors, such as diet and nutrition,36,43 weight control,36,43 drinking,36 and other lifestyle changes that reduce the incidence and progression of diseases, have also been mentioned.
Early Detection
The convenience of contact between pharmacists and patients and the professionalism of pharmacists8,18,30 provide pharmacists with the advantage of being able to identify potential COPD patients in high-risk groups and to allow them to receive effective treatment as early as possible to control the further development of the disease. Pharmacists could observe the patient’s health status, whether the patient showed symptoms of airway obstruction,24 had a history of lung disease over the age of 40,35 purchased drugs for COPD but had not been diagnosed,36 and had a history of smoking over the age of 35.40,47 For those at high risk of COPD, patients were provided with self-filled questionnaires for self-diagnosis and self-evaluation. Questionnaires provided for patients included the GOLD screening questionnaire,24,30,35 St. George’s Respiratory Questionnaire (SGRQ),25 COPD Assessment Test (CAT),36,45 and Initial Screening Questionnaire (ISQ),40,47 four different kinds of questionnaire but all used to assess the risk of COPD and the extent of disease progression. For patients whose questionnaire scores reach a certain level, it is recommended that they undergo lung function tests (LFTs) to further evaluate the risk of COPD disease. Patients with higher risks are referred to a physician for further treatment, according to the test results.24,30,35,40,47 For all this, there may be some uncertainty in the questionnaire and LFTs, so it is necessary, according to the judgement of the pharmacist, to recommend seeking further medical treatment, even if the patients who are tested are at low risk.48
Therapy Management
The management of patients’ therapy by pharmacists can be divided into two levels. On the first level, pharmacists provided non-specific pharmacy services,25,27-29,31–34,36,38,39,41,43,45,48 such as dispensing;25,29,34,38,43,48 counselling on medicine administration dose and frequency,27–29,31–34,37–39,41,43,45,48 adherence,27,28,31-34,38,39,41,43,45,48 drug interactions,27,28,32,34,38,41,43,45 and adverse drug reactions,27–29,32–34,38,41,43,45 as well as long-term monitoring of adverse drug reactions.33,43 On the second level, owing to the particular characteristics of the medication and management of COPD, there were other pharmacy practices that community pharmacists could provide specifically for COPD patients, such as the introduction of pathological information31–33 and assessing the stage of disease.35,38,39,43 At the same time, as the current mainstay of treatment for COPD, inhaled medication therapy needed more education from pharmacists, leading to improved inhalation techniques.12,49 To achieve the goal of optimizing the inhalation technique, pharmacists’ education for patients needs to include both short-term instruction, in which pharmacists teach patients how to correctly use the inhalation device until the patients demonstrate understanding and proper handling techniques;25,26,28,29,31-34,36–39,42–45 and long-term using monitor levels, in which patients are required to demonstrate using the device while the pharmacist evaluates them and then, if necessary, corrects their use in the subsequent process.31–33,43–45
Long-Term Health Management
Based on the basic short-term treatment, pharmacists will further monitor the patients as long-term health management. The main intervention measures were worsening risk monitoring29,31-33,36,38,39,43 and long-term patient follow-up and counselling services,29,32,33,36,38,43,45 which aimed to check the compliance of patients with medication and the progress of COPD, and to provide professional guidance to patients at any time when they needed it.
At the same time, pharmacists helped COPD patients to enhance their self-management of the disease,32,33 assisted in establishing a lifestyle in which patients could manage themselves, and actively cooperated with other medical service providers, such as physicians32,45 and nurses;39 all in all, they provided patients with long-term and comprehensive supervision services. In addition, pharmacists would recommend that patients with COPD, especially those over 65 years of age,25 received an influenza vaccine during the flu-prone season to reduce the risk of acute exacerbation of COPD.25,32,33,43,46,48
Outputs
Among all of the outputs, the most popular output referred to in the studies was the patients’ technique in using inhalation devices, and all studies showed positive intervention effects (n=11).26,29,31-34,37,42,44,45,47 This was followed by medication compliance; all studies involving compliance showed that patient compliance improved after intervention by a pharmacist.32–34,36,38,41 Of the studies involving interventions for patients to quit smoking, most (n=4) showed a positive effect;27,30,36,38 however, Tommelein et al reported there was no help available for the intervention. The literature also supported pharmacists’ ability to assist in identifying high-risk patients with COPD from the population after professional training.24,30,35,40,47 Two studies on influenza vaccination for COPD patients showed that after being given a reminder and explanation of professional knowledge by pharmacists, the proportion of influenza vaccinations in patients increased.25,46 In another study, the pharmacist’s counselling service had a positive effect on patients’ access to relevant COPD information.29
Outcomes
The impact of outputs on patients can be further summarized as final outcomes, involving patients in clinical (n=6), humanistic (n=1), and economic (n=1) aspects. In terms of the clinical outcomes of pharmacist intervention, the related symptoms of patients with COPD29,36,38,41 the frequency of acute onset,29,31,33 and the hospitalization rate of patients29,32 decreased, but the severity of the onset period did not change significantly.33 Detoni et al and Alton and Farndon, in their reports of patients’ health status, proved that intervention by the pharmacist can improve the overall health of patients, through two sets of experimental methods,41,45 but Takemura et al and Tommelein et al did not recognize the positive effect on the patient’s health status.31,33 Two other studies showed positive effects of pharmacist services on patients’ quality of life, but one of the studies showed no significant positive effects, possibly because of the short intervention time.29,36
In terms of patients’ humanistic outcomes, two related studies revealed that patients’ satisfaction with pharmacy services was improved by pharmacists’ services.29,47 As for economic outcomes, Wright et al indicated that community pharmacists provided patients with 6-month counselling, lifestyle advice, smoking cessation advice, and referral to physicians, which led to a significant cost reduction in treating COPD in health costs, due to pharmacist intervention.36
Contextual Factors
In the selected literature, the contextual factors affecting the pharmacist’s provision of pharmacy services can be summarized for three stakeholders involved in medical services, namely pharmacists, patients, and other medical service providers, as well as three economic factors, namely the facilities, clinic context, and socio-economic factors.
For pharmacists, the most commonly mentioned related contextual factor was that the existing workload of the pharmacist meant that the pharmacist lacked service time28,33,48 and had a work overload problem.48 Studies have also shown that pharmacists were concerned about inadequate service competence, and a lack of knowledge in this area could lead to confusion when serving patients, which is not conducive to pharmacists’ providing long-term services.33,48 Some studies have pointed out that pharmacists considered that the control of COPD requires the assistance of many healthcare providers,26,35,40,45,47,48 such as physicians26,40 and nurses,45 in addition to pharmacists; communication between different healthcare providers35 and interdisciplinary collaboration47 also need to receive attention. Contextual factors for patients included that patients may not have enough time to receive services from pharmacists,48 the willingness to pay for pharmacy services, which needs further research,30 possible cognitive function decline in older patients,37 and patients’ attitude and lack of COPD awareness.47,48
At the external environmental level, pharmacists need more economic funding support to provide the impetus to implement interventions;30,33,36,47,48 in particular, financial support from the government would demonstrate its positive role in this process.36,47 If researchers could prove that the cost of pharmaceutical care in COPD reduced health insurance spending, further promotion of this service would be supported by medical insurance departments.34 In addition, if the pharmaceutical service required the intervention of the medical insurance department, the software-related support required for the service and the connection with the medical insurance payment system would also need to be established simultaneously.32,40
Discussion
This research identified 25 studies from the literature published in the past decade and employed a logic model to display the current research landscape on the professional services provided by community pharmacists in COPD management. As depicted in the model shown in Figure 2, the influence of external contextual factors on the intervention’s ability to produce outputs and outcomes, the interrelationships among interventional components, and the pathways through which interventions produced certain outputs and outcomes (clinical, humanistic, and economic) were clearly illustrated. Unlike most of the previous research, which mainly focused on reporting the pharmacist’s interventions and the expected output and/or outcome, this study provided a broader perspective on the relationships among the contextual factors, interventions, outputs, and outcomes, which can be used to inform the development, implementation, and evaluation of community pharmacist services in COPD management.
 |
Figure 2 Economic, Clinical, and Humanistic Outcomes (ECHO) model of patient outcomes of pharmacists’ intervention on COPD management. |
Community pharmacists remain some of the most accessible healthcare professionals to address patient needs with appropriate support in many countries around the world.8,18 Their interventions in COPD extend beyond patient-focused management (therapy management and long-term health management) towards population-oriented services (primary prevention and early detection), reflecting pharmacists’ increasingly important role in public health. These findings concur with the guidance developed by the FIP on how pharmacists contribute towards overcoming COPD and other non-communicable diseases in the community.10 The primary effect of pharmaceutical services was to optimize the drug treatment for patients: to ensure that patients can use drugs safely and effectively,maximize the effects of drugs in use and minimize adverse drug reactions.41 Long-term follow-up for patients by pharmacists and monitoring of the risk of exacerbations were also expected to improve patient medication behaviours, thereby improving medication compliance and, finally, greatly reducing the further development of COPD.50
Moreover, based on the current study, there was a general agreement on the practicality and feasibility of community pharmacists’ interventions in improving early detection and diagnosis,24,30,35,40,47 supporting smoking cessation,27,30,36,38 ensuring that patients acquire the skills to use inhalator devices appropriately,26,29,31-34,37,42,44,45,47 and promoting influenza vaccination to population groups at risk of COPD or exacerbations.25,46 However, areas such as collaborating with doctors and other healthcare providers to provide integrative care were under-researched. Optimizing health-related outcomes for COPD patients requires coordinated care from a multidisciplinary healthcare team including pharmacists, doctors, nutritionists, and physiotherapists, as well as patients and caregivers.10 Existing studies on collaborative COPD care models focused mainly on clinical pharmacists.6,51 Considering the importance of continuity of care in improving COPD patient outcomes (including a reduction in all-cause mortality52), a collaborative care model with guided practice protocols should be developed to integrate community pharmacists into the ongoing therapeutic support for COPD patients and to promote the understanding of and respect for pharmacists’ potential to contribute, and most importantly, to guide good practice among pharmacists.5,53-55
To expand and consolidate the role of community pharmacists in managing COPD, it is important to demonstrate the added value of pharmacists’ interventions on the overall disease management and the clinical outcome of the patients. As shown in Figure 2, previous research analysed in this study may be divided into two groups: simple intervention, with the impact often measured in terms of output (the grey dotted lines); and multi-intervention study design, to evaluate the impact on patient outcomes (the coloured solid lines). Traditionally, the practice of community pharmacists focused on outputs, which were mainly process or practice focused.56 While outputs remain important performance indicators of pharmacists’ intervention, professional services provided by pharmacists should strive to demonstrate their true values, ie the translation from process output into patient outcomes. For instance, direct measurement may be sufficient to demonstrate the effect of pharmacist-led smoking cessation programmes in increasing smoking cessation rates compared with usual care.57 However, more robust studies are needed to demonstrate that the intervention provided by pharmacists could result in positive outcomes on COPD prevention and progression.45 Furthermore, it usually took multiple interventions that worked collectively to contribute to a common set of patient outcomes.29,31-33,36,38,41,45,47 For instance, Wright et al demonstrated that the support service provided by community pharmacists for COPD patients may include, in addition to smoking cessation support, simultaneous therapy management and long-term care, to enhance medication adherence and increase quitting rates, which can eventually help to improve patients’ quality of life, reduce COPD symptoms, and cut costs.36
The patient outcomes of pharmacists’ intervention on COPD management were classified using the ECHO model, as shown in Figure 2. The ECHO model advocated a balanced and multidimensional assessment of the value of pharmacists’ interventions.20 Not surprisingly, the majority of previous research aimed to understand the impact of pharmacists’ contribution to COPD management in terms of clinical indicators and outcomes, which were typically more familiar and accepted measures for healthcare providers when evaluating patients’ health status. However, the other two constructs of the ECHO model, humanistic and economic outcomes, were tested less frequently, although they have become increasingly critical indicators in evaluation of healthcare in the context of patient-centred care and limited healthcare resources, respectively.
Humanistic outcome is often measured in terms of patient satisfaction with pharmaceutical services.58,59 Patient satisfaction also served as an important determinant of the viability and sustainability of healthcare services, effective use of healthcare resources, likelihood of continuously using healthcare services, adherence to treatment, and resulting in better health outcomes.60,61 However, reports about humanistic outcomes associated with pharmacists’ intervention in COPD management remained scarce. The value of pharmacists’ intervention should also be measured in economic terms, whether they be direct, indirect, or intangible costs. On the other hand, economic evaluation of clinical pharmacy services has been promoted since the late 1990s62,63 and positive economic benefits as a result of pharmacists’ interventions and services have been reported.64 Among the great challenges to improving the quality of healthcare despite limited healthcare resources, economic outcomes are an increasingly substantive focus among healthcare policy-makers, consumers, and payers during their decision-making process with regard to identifying the most cost-effective healthcare interventions and developing reasonable remuneration mechanisms for the professional services provided.65–67 To be able to achieve a sustainable development of pharmacists’ interventions in COPD management, there needs to be a reasonable remuneration system for which economic indicators about the pharmacists’ intervention, such as reductions in direct costs, unscheduled hospital days, or total treatment costs, would be highly relevant.68
A range of contextual factors that may affect community pharmacists’ intervention in COPD management were also summarized in this study. This reconfirmed the multifactorial nature of the readiness to make changes and improvements in pharmacy practice. However, few studies have been conducted to test the effect of the contextual factors, despite their being important predictors of pharmacists’ performance. In particular, the shift of the pharmacists’ focus from patient/disease management to population/disease prevention requires an additional set of knowledge, skills, attitudes, and behaviour. Formal training of the pharmacy workforce to provide appropriate services in COPD management has been shown to be insufficient.10 The change towards patient-centred care has also made apparent the need for competence building to enable the transformation of pharmacist services.69 However, a lack of knowledge regarding COPD management was repeatedly discussed in the literature reviewed in this study as one of the major challenges faced by community pharmacists. Pharmacy education on direct patient care and public health should be reinforced and monitored for its effect on improving pharmacists’ practice in COPD management.70 Likewise, other modifiable contextual factors should be considered collectively to formulate a strategy that would help to improve pharmacists’ skills and eventually benefit patient outcomes.
This study has some limitations. First, this research is based only on a systematic review of published empirical studies. A future study could collect information from other sources, including key stakeholders’ opinions, to enrich or modify the model, especially the contextual factors such as funding (reimbursement for COPD drugs and pharmacy services). Second, this model indicates the causal chains among the components, but has not obtained confirmative results about those chains. Future research is needed to test this by conducting quantitative research, for example through meta-analysis or newly designed experimental studies.
Conclusion
Studies in the literature have proposed and examined different components of professional services provided by community pharmacists for COPD management. However, he relationships among outcomes, comprehensive professional services of community pharmacists, and contextual factors have not been systematically tested. More well-designed, rigorous studies with more sensitive and specific outcome measures need to be conducted to assess the effect of community pharmacy practice for COPD management.
Data Sharing Statement
All the data for this systematic review have been included in the manuscript and Supplementary Material 1.
Ethics Approval and Informed Consent
The study was reviewed and approved by the Ethics Committee of China Pharmaceutical University (ndrplc201901). Informed consent is not applicable for this systematic review study.
Acknowledgments
We acknowledge the comments from colleagues at the University of Macau and China Pharmaceutical University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. World Health Organization (WHO). Burden of COPD [online]. 2019. Available from: http://www.who.int/respiratory/copd/burden/en/.
2. Vogelmeier C, Criner G, Martinez F, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–582. doi:10.1164/rccm.201701-0218PP
3. National Council on Patient Information and Education. Enhancing prescription medicine adherence: a national action plan [online]. 2007. Available from: http://www.talkaboutrx.org/documents/enhancing_prescription_medicine_adherence.pdf.
4. Rogliani P, Ora J, Puxeddu E, et al. Adherence to COPD treatment: myth and reality. Resp Med. 2017;129:117–123. doi:10.1016/j.rmed.2017.06.007
5. Crompton G, Barnes P, Broeders M, et al. The need to improve inhalation technique in Europe: a report from the aerosol drug management improvement team. Resp Med. 2006;100(9):1479–1494. doi:10.1016/j.rmed.2006.01.008
6. Gentene AJ, Guido MR, Woolf B, et al. Multidisciplinary team utilizing pharmacists in multimodal, bundled care reduce chronic obstructive pulmonary disease hospital readmission rates. J Pharm Pract. 2019:089719001988944. doi:10.1177/0897190019889440
7. Bluml BM. White paper on expanding the role of pharmacists in chronic obstructive pulmonary disease: American Pharmacists Association Foundation. J Am Pharm Assoc. 2011;51(2):203–211. doi:10.1331/JAPhA.2011.11513
8. Zhong H, Ni X, Cui M, et al. Evaluation of pharmacist care for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Clin Pharm. 2014;36(6):1230–1240. doi:10.1007/s11096-014-0024-9
9. Hepler C, Strand L. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47:533–543.
10. International Pharmaceutical Federation (FIP). Beating non-communicable diseases in the community: the contribution of pharmacists [online]. 2019. Available from: https://www.fip.org/files/content/publications/2019/beating-ncds-in-the-community-the-contribution-of-pharmacists.pdf.
11. Hallit S, Zeidan RK, Saade S, et al. Knowledge, attitude and practice of lebanese community pharmacists toward chronic obstructive pulmonary disease. J Epidemiol Glob Health. 2020;10(1):86–95. doi:10.2991/jegh.k.191215.004
12. Saini B. Role of community pharmacists in asthma – Australian research highlighting pathways for future primary care models. Aust Med J. 2011;4(4):190. doi:10.4066/AMJ.2011.790
13. Suhaj A, Manu MK, Unnikrishnan MK, Vijayanarayana K, Mallikarjuna RC. Effectiveness of clinical pharmacist intervention on health-related quality of life in chronic obstructive pulmonary disorder patients - a randomized controlled study. J Clin Pharm Ther. 2016;41:78–83. doi:10.1111/jcpt.12353
14. Jarab AS, Alqudah SG, Khdour M, Shamssain M, Mukattash TL. Impact of pharmaceutical care on health outcomes in patients with COPD. Int J Clin Pharm. 2012;34(1):53–62. doi:10.1007/s11096-011-9585-z
15. Eussen SR, Elst MEVD, Klungel OH, et al. A pharmaceutical care program to improve adherence to statin therapy: a randomized controlled trial. Ann Pharmacother. 2010;44(12):1905–1913. doi:10.1345/aph.1P281
16. Saini B, Krass I, Armour C. Development, implementation, and evaluation of a community pharmacy-based asthma care model. Ann Pharmacother. 2004;38:1954–1960. doi:10.1345/aph.1E045
17. Santschi V, Chiolero A, Burnand B, Colosimo AL, Paradis G. Impact of pharmacist care in the management of cardiovascular disease risk factors: a systematic review and meta-analysis of randomized trials. Arch Intern Med. 2011;171(16):1441–1453. doi:10.1001/archinternmed.2011.399
18. van der Molen T, van Boven JF, Maguire T, Goyal P, Altman P. Optimizing identification and management of COPD patients–reviewing the role of the community pharmacist. Brit J Clin Pharmaco. 2017;83(1):192–201. doi:10.1111/bcp.13087
19. Barefield KL, DeBellis HF. A review of health-related outcomes from community pharmacist interventions in patients with chronic obstructive pulmonary disease. J Am Col Clin Pharm. 2019;2(4):433–443. doi:10.1002/jac5.1151
20. Kozma C, Reeder C, Schulz R. Economic, clinical, and humanistic outcomes: a planning model for pharmacoeconomic research. Clin Ther. 1993;15(6):1121–1132.
21. Gourley GA, Portner TS, Gourley DR, et al. Part 3. Humanistic outcomes in the hypertension and COPD arms of a multicenter outcomes study. J Am Pharm Assoc. 1998;38(5):586–597.
22. Solomon DK, Portner TS, Bass GE, et al. Part 2. Clinical and economic outcomes in the hypertension and COPD arms of a multicenter outcomes study. J Am Pharm Assoc. 1998;38(5):574–585.
23. Moola S, Munn Z, Tufanaru C, et al. Joanna Briggs Institute Reviewer’s manual. The Joanna Briggs Institute. Chapter 7: systematic reviews of etiology and risk. [online] 2017. Available from: https://reviewersmanual.joannabriggs.org/.
24. Castillo D, Guayta R, Giner J, et al. COPD case finding by spirometry in high-risk customers of urban community pharmacies: a pilot study. Resp Med. 2009;103(6):839–845. doi:10.1016/j.rmed.2008.12.022
25. Mehuys E, Boussery K, Adriaens E, et al. COPD management in primary care: an observational, community pharmacy-based study. Ann Pharmacother. 2010;44(2):257–266. doi:10.1345/aph.1M481
26. Hammerlein A, Muller U, Schulz M. Pharmacist-led intervention study to improve inhalation technique in asthma and COPD patients. J Eval Clin Prac T. 2011;17(1):61–70. doi:10.1111/j.1365-2753.2010.01369
27. Verma A, Harrison A, Torun P, Vestbo J, Edwards R, Thornton J. Are pharmacists reducing COPD’S impact through smoking cessation and assessing inhaled steroid use? Resp Med. 2012;106(2):230–234. doi:10.1016/j.rmed.2011.08.011
28. Beauchesne M-F, Bercier D, Julien-Baker F, Lalonde L, Boileau R, Blais L. Community pharmacy–based medication assessment program for asthma and chronic obstructive pulmonary disease. Can Pharm J. 2012;145(2):70. doi:10.3821/145.2.cpj70
29. Petkova V, Andreevska K, Gueurguiev S, et al. Community pharmacy-based program for patients with asthma and chronic obstructive pulmonary disease. Biotechnol Biotec Eq. 2012;26(6):3437–3442. doi:10.5504/BBEQ.2012.0099
30. Fuller L, Conrad WF, Heaton PC, Panos R, Eschenbacher W, Frede SM. Pharmacist-managed chronic obstructive pulmonary disease screening in a community setting. J Am Pharm Assoc. 2012;52(5):
31. Takemura M, Mitsui K, Matsumoto IM, et al. Effect of a network system for providing proper inhalation technique by community pharmacists on clinical outcomes in COPD patients. Int J Chronic Obstr. 2013;8:239. doi:10.2147/COPD.S44022
32. Tommelein E, Mehuys E, Van Hees T, et al. Effectiveness of pharmaceutical care for patients with chronic obstructive pulmonary disease (PHARMACOP): a randomized controlled trial. Brit J Clin Pharmaco. 2014;77(5):756–766. doi:10.1111/bcp.12242
33. Tommelein E, Tollenaere K, Mehuys E, Boussery K. Pharmaceutical care for patients with COPD in Belgium and views on protocol implementation. Int J Clin Pharm-Net. 2014;36(4):697–701. doi:10.1007/s11096-014-9956-3
34. Ottenbros S, Teichert M, de Groot R, et al. Pharmacist-led intervention study to improve drug therapy in asthma and COPD patients. Int J Clin Pharm-Net. 2014;36(2):336–344. doi:10.1007/s11096-013-9887-4
35. Castillo D, Burgos F, Guayta R, et al. Airflow obstruction case finding in community-pharmacies: a novel strategy to reduce COPD underdiagnosis. Respir Med. 2015;109(4):475–482. doi:10.1016/j.rmed.2015.02.009
36. Wright D, Twigg M, Barton G, Thornley T, Kerr C. An evaluation of a multi-site community pharmacy-based chronic obstructive pulmonary disease support service. Inte J Pharm Pract. 2015;23(1):36–43. doi:10.1111/ijpp.12165
37. Bouwmeester C, Kraft J, Bungay KM. Optimizing inhaler use by pharmacist-provided education to community-dwelling elderly. Resp Med. 2015;109(10):1363–1368. doi:10.1016/j.rmed.2015.07.013
38. Apikoglu-Rabus S, Yesilyaprak G, Izzettin FV. Drug-related problems and pharmacist interventions in a cohort of patients with asthma and chronic obstructive pulmonary disease. Resp Med. 2016;120:109–115. doi:10.1016/j.rmed.2016.10.006
39. Davis E, Marra C, Gamble JM, et al. Effectiveness of a pharmacist-driven intervention in COPD (EPIC): study protocol for a randomized controlled trial. Trials. 2016:17. doi:10.1186/s13063-016-1623-7
40. Fathima M, Saini B, Foster JM, Armour CL. Community pharmacy-based case finding for COPD in urban and rural settings is feasible and effective. Int J Chronic Obstr. 2017;12:2753–2761. doi:10.2147/copd.S145073
41. Detoni KB, Oliveira IV, Nascimento MM, Caux TR, Alves MR, Ramalho-de-Oliveira D. Impact of a medication therapy management service on the clinical status of patients with chronic obstructive pulmonary disease. Int J Clin Pharm. 2017;39(1):95–103. doi:10.1007/s11096-016-0402-6
42. Castel-Branco MM, Fontes A, Figueiredo IV. Identification of inhaler technique errors with a routine procedure in Portuguese community pharmacy. Pharm Pract. 2017;15(4):1072. doi:10.18549/PharmPract.2017.04.1072
43. Heikkila JM, Parkkamaki S, Salimaki J, Westermarck S, Pohjanoksa-Mantyla M. Community pharmacists’ knowledge of COPD, and practices and perceptions of medication counseling of COPD patients. Int J Chronic Obstr. 2018;13:2065–2074. doi:10.2147/copd.S159726
44. Ruud KW, Ronningen SW, Faksvag PK, Ariansen H, Hovland R. Evaluation of a structured pharmacist-led inhalation technique assessment service for patients with asthma and COPD in Norwegian pharmacies. Patient Educ Couns. 2018;101(10):1828–1837. doi:10.1016/j.pec.2018.05.018
45. Alton S, Farndon L. The impact of community pharmacy-led medicines management support for people with COPD. Brit J Commun Nurs. 2018;23(6):266–271. doi:10.12968/bjcn.2018.23.6.266
46. Klassing HM, Ruisinger JF, Prohaska ES, Melton BL. Evaluation of pharmacist-initiated interventions on vaccination rates in patients with asthma or COPD. J Commun Health Nurs. 2018;43(2):297–303. doi:10.1007/s10900-017-0421-9
47. Fathima M, Saini B, Foster JM, Armour CL. A mixed methods analysis of community pharmacists’ perspectives on delivering COPD screening service to guide future implementation. Res Social Adm Pharm. 2019;15(6):662–672. doi:10.1016/j.sapharm.2018.08.007
48. Hesso I, Kayyali R, Nabhani-Gebara S. Supporting respiratory patients in primary care: a qualitative insight from independent community pharmacists in London. BMC Health Serv Res. 2019;19:5. doi:10.1186/s12913-018-3814-2
49. Casset A, Meunier-Spitz M, Rebotier P, et al. Asthma management and inhalation techniques among community pharmacists in 2009: a comparison with the 1999 survey. J Asthma. 2014;51(9):964–973. doi:10.3109/02770903.2014.936446
50. Bischoff EW, Hamd DH, Sedeno M, et al. Effects of written action plan adherence on COPD exacerbation recovery. Thorax. 2011;66(1):26–31. doi:10.1136/thx.2009.127621
51. Hunt V, Anderson D, Lowrie R, et al. A non-randomised controlled pilot study of clinical pharmacist collaborative intervention for community dwelling patients with COPD. Npj Prim Care Resp M. 2018;28(1):1–10.
52. Cho KH, Kim YS, Nam CM, et al. The association between continuity of care and all-cause mortality in patients with newly diagnosed obstructive pulmonary disease: a population-based retrospective cohort study, 2005–2012. PLoS One. 2015;10(11). doi:10.1371/journal.pone.0141465
53. Tan EC, Stewart K, Elliott RA, George J. Pharmacist services provided in general practice clinics: a systematic review and meta-analysis. RSAP. 2014;10:608–622. doi:10.1016/j.sapharm.2013.08.006
54. Jorgenson D, Laubscher T, Lyons B, Palmer R. Integrating pharmacists into primary care teams: barriers and facilitators. Int J Pharm Pract. 2014;22:292–299. doi:10.1111/ijpp.12080
55. Traynor K. Pharmacist fits on high-intensity transitional care team. Am J Health Syst Pharm. 2014;71(13):1066–1068. doi:10.2146/news140047
56. Moltó-Puigmartí C, Vonk R, van Ommeren G, Hegger I. A logic model for pharmaceutical care. J Health Serv Res Policy. 2018;23(3):
57. El Hajj MS, Kheir N, Al Mulla AM, Shami R, Fanous N, Mahfoud ZR. Effectiveness of a pharmacist-delivered smoking cessation program in the State of Qatar: a randomized controlled trial. BMC Public Health. 2017;17(1):215. doi:10.1186/s12889-017-4103-4
58. Schommer JC, Kucukarslan SN. Measuring patient satisfaction with pharmaceutical services. Am J Health Syst Ph. 1997;54(23):2721–2732.
59. Naik P, Saini B, Armour C. Measurement of patient satisfaction with community pharmacy services: a review. Pharm World Sci. 2009;31:525–537. doi:10.1007/s11096-009-9311-2
60. Gupta KS, Rokade V. Importance of quality in health care sector: a review. J Health Manag. 2016;18(1):84–94. doi:10.1177/0972063415625527
61. Schuessler TJ, Ruisinger JF, Hare SE, Prohaska ES, Melton BL. Patient satisfaction with pharmacist-led chronic disease state management programs. J Pharm Pract. 2016;29(5):484–489. doi:10.1177/0897190014568672
62. Schumock GT, Meek PD, Ploetz PA, Vermeulen LC. Economic evaluations of clinical pharmacy services(1988–1995). Pharmacotherapy. 1996;16:1188–1208.
63. Perez A, Doloresco F, Hoffman JM, et al. Economic evaluations of clinical pharmacy services 2001–2005. Pharmacotherapy. 2009;29(1):128. doi:10.1592/phco.29.1.128
64. Murray ME, Barner JC, Pope ND, Comfort MD. Impact and feasibility of implementing a systematic approach for medication therapy management in the community pharmacy setting: a pilot study. J Pharm Pract. 2019;32(6):664–670. doi:10.1177/0897190018779847
65. Chisholm-Burns MA, Graff Zivin JS, Lee JK, et al. Economic effects of pharmacists on health outcomes in the United States: a systematic review, Am J Health Syst Pharm. 2010;67(19):1624–1634. doi:10.2146/ajhp100077
66. Benrimoj SI, Langford JH, Berry G, et al. Economic impact of increased clinical intervention rates in community pharmacy. Pharmacoeconomics. 2000;18(5):459–468. doi:10.2165/00019053-200018050-00005
67. Félix J, Ferreira D, Afonso-Silva M, et al. Social and economic value of Portuguese community pharmacies in health care. BMC Health Serv Res. 2017;17(1):606. doi:10.1186/s12913-017-2525-4
68. Bourbeau J, Granados D, Roze S, et al. Cost-effectiveness of the COPD patient management European trial home-based disease management program. Int J Chronic Obstr. 2019;14:645. doi:10.2147/COPD.S173057
69. Stewart DW, Brown SD, Clavier CW, Wyatt J. Active-learning processes used in US pharmacy education. Am J Pharm Educ. 2011;75:68. doi:10.5688/ajpe75468
70. Doucette WR, Nevins JC, Gaither C, et al. Organizational factors influencing pharmacy practice change. Res Soc Admin Pharm. 2012;8(4):274–284. doi:10.1016/j.sapharm.2011.07.002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.