Back to Journals » Local and Regional Anesthesia » Volume 17
Prolonged Duration of Peripheral Nerve Blockade in a Pediatric Patient with Charcot Marie Tooth Disease: A Case Report
Authors Barnett NR ![]() , Bunnell AM, Dow MA
, Bunnell AM, Dow MA
Received 16 December 2023
Accepted for publication 11 April 2024
Published 20 April 2024 Volume 2024:17 Pages 49—53
DOI https://doi.org/10.2147/LRA.S455285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Natalie R Barnett,1 Amanda M Bunnell,1 Matthew A Dow2
1Department of Anesthesiology and Perioperative Medicine, Medical University of South Carolina, Charleston, SC, USA; 2Department of Orthopaedics and Physical Medicine, Medical University of South Carolina, Charleston, SC, USA
Correspondence: Natalie R Barnett, Associate Professor in Anesthesiology, Department of Anesthesiology and Perioperative Medicine, Medical University of South Carolina, 10 McClennan Banks Dr, Suite 2190, MSC 940, Charleston, SC, 29425, USA, Tel +1-843-792-5454, Email [email protected]
Abstract: Charcot Marie Tooth disease is a common cause of pediatric peripheral neuropathy, which can lead to distal muscle wasting and weakness necessitating orthopedic procedures. We present an eleven-year-old male with Charcot Marie Tooth disease who received peripheral nerve blocks for ankle surgery, with a total dose of 1.75 mg/kg of bupivacaine 0.25%. Upon follow-up, it was identified that the sensory blockade did not resolve until thirty-six hours, postoperatively. There were no noted long-term sequalae on surgical follow-up. If a patient with Charcot Marie Tooth receives a peripheral nerve block, the patient should receive close short- and long-term follow-up to monitor for block complication or disease exacerbation.
Keywords: regional anesthesia, local anesthesia, peripheral neuropathy
Introduction
As a common cause of chronic peripheral neuropathy in childhood, Charcot Marie Tooth disease (CMTD) is an autosomal dominant disorder that typically presents as distal muscle weakness and wasting of the lower extremities. Upper extremities are usually affected later in the course of the disease.1 Patients with CMTD will likely require multiple orthopedic procedures for musculoskeletal pathology over the course of a lifetime.2 As with most pre-existing neurologic disorders, there has been hesitation to promote widespread use of regional anesthesia in patients with CMTD due to concern for disease exacerbation or direct nerve injury.2,3 In the adult literature, there have been case reports and case series of CMTD patients that received a peripheral nerve block (PNB) as part of their perioperative analgesic strategy with minimal complications or long-term sequelae.3–8 However, there is less corresponding literature exploring the utility of and/or safety of PNB in pediatric patients with CMTD. Typically, pediatric patients are included with adult patients as part of a case series.4 This is a case report of a pediatric patient with CMTD who received popliteal and adductor canal blocks for ankle surgery and experienced a prolonged sensory block without experiencing long-term sequelae or disease exacerbations.
Written Health Insurance Portability and Accountability Act authorization was obtained from the patient’s parent (legal guardian) for the reporting and publication of this case report and associated images. Local Institutional Review Board approval was not required for the publication of this case report. This article was prepared utilizing the case report guidelines (CARE) to adhere to the applicable Enhancing the Quality and Transparency of Health Research (EQUATOR) guidelines.
Case Description
An 11-year-old, 42.9 kg male with CMTD presented for surgical correction of a right foot deformity (arthrotomy, tendon lengthening, osteotomy) under general anesthesia with PNB for postoperative pain management. He did not have prior experience with PNB. For the presented procedure, a post-induction single-shot right-sided ultrasound-guided adductor canal block and popliteal nerve block were performed utilizing an in-plane approach (21-gauge, 90 mm, StimuQuik Echo Insulated Peripheral Nerve Block Needle, Teleflex®, Reading PA, USA) with injected bupivacaine 0.25% 10 mL and 20 mL, respectively (total dose 1.75 mg/kg). During ultrasound examination for the PNB placement, the popliteal nerve was noted to be larger than expected for his age as well as odd in appearance, with distinct, numerous fascicular bundles (Figure 1). There were no noted technical difficulties, as well as no immediate complications noted during the PNB placement. Though no formal measurement of the onset of nerve blockade was obtained, there was minimal response to surgical stimulation at the start of the procedure approximately 30 minutes post-block placement. This would correspond to an expected onset of nerve blockade.
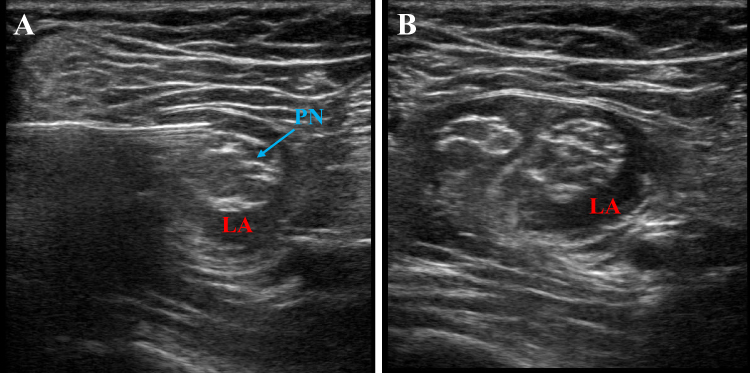 |
Figure 1 Ultrasound-guided popliteal nerve block. (A) Proximal popliteal nerve with “onion-bulb” appearance, with needle placement and local anesthetic deposition. (B) Distal spread of local anesthetic, post-bifurcation of popliteal nerve. Abbreviations: LA: local anesthetic. PN: popliteal nerve. |
The patient tolerated the procedure well, appeared comfortable in the post-anesthesia care unit, and no immediate perioperative complications were noted. Intraoperatively, he received a total of fentanyl 100 mcg and hydromorphone 0.2 mg intravenously, mostly for presumed tourniquet pain. Postoperatively, he received acetaminophen and ibuprofen per os scheduled around the clock. There was hydromorphone intravenous and oxycodone per os available as needed. He received zero doses of hydromorphone and only two doses of oxycodone during his overnight hospital stay. On physical examination prior to discharge, he was able to move all toes but still had numbness in the exposed digits. The operative extremity was in a large post-operative surgical splint, and only his toes were exposed.
As standard at our institution, the patient was followed until block resolution was noted by patient and/or family. Per report of the patient’s parent on follow-up telephone calls, the sensory block did not resolve until approximately 36-hours post-placement as indicated by residual numbness and sensory changes, presumed to be in both the sciatic and femoral nerve distribution based upon description by his parent. At 2-week, 4-week, 6-week, 3-month, 4-month, 1-year, and 2-year follow-up appointments with the surgical team, there was no documented complication, disease exacerbation or prolonged neuropathy per the electronic medical record clinic notes. Patient and family were extremely satisfied with the overall perioperative experience.
Discussion
Charcot Marie Tooth disease (CMTD) is a hereditary peripheral neuropathy primarily affecting distal musculature and is characterized by distal muscle weakness, muscle wasting and sensory deficits.4,9 Gait disturbance and changes to balance develop from resultant foot deformities.10 Consequently, patients commonly require extensive orthopedic procedures for correction of musculoskeletal pathology, such as soft tissue dissection, bony realignment, tendon transfers, osteotomies, and fusions.4 Historical perioperative concerns for patients with CMTD presenting for surgical procedures and general anesthesia include cardiac arrhythmias and conduction abnormalities, malignant hyperthermia, respiratory insufficiency due to respiratory muscle dysfunction, and an unpredictable response to non-depolarizing neuromuscular blockade due to nerve demyelination.1,8 Due to the extensive nature of surgical orthopedic correction, there is commonly a high degree of postoperative pain which often requires high doses of narcotic medication.4 Unfortunately, there has been hesitation to utilize regional anesthesia in patients with pre-existing neurologic conditions despite the known effective analgesia for extensive orthopedic surgical procedures.2 The common belief is that patients with pre-existing peripheral neuropathy are at an increased risk for complications following PNB given already compromised peripheral nerves.11,12
Patients with CMTD have underlying peripheral neuropathy and, therefore, a perceived increased susceptibility to nerve injury due to the “double-crush phenomenon” either from direct local anesthetic toxicity to a demyelinated nerve or direct nerve trauma from the block needle.2,4,6 However, there have been case reports and case series describing successful single-shot PNB in adult patients with CMTD without complication or disease exacerbation. In the case series by Dhir et al,6 three patients with CMTD underwent surgical procedures of the upper extremity following an axillary brachial plexus block. The authors conclude that with ultrasound guidance, patients with CMTD may undergo PNB more effectively and safely.6 Single case reports have also reported successful brachial plexus blocks with complication or disease exacerbation.5,8 Of note, Bui et al reported an unexpected block duration of 30 hours.5 Additionally, Barbary et al report a successful sciatic nerve block for extreme postoperative pain following ankle realignment surgery.3 There was no reported immediate complication or at 6-month follow-up.3 Finally, a recent 53-patient cohort study found no increased risk of nerve injury or documented neurological complications secondary to regional anesthesia in adult patients with CMTD.7
When considering peripheral nerve block catheters, An et al4 did not identify any catheter-related complications, long-term sequelae or disease exacerbations in a prospective case series of twenty patients, including some pediatric patients (ages 13–18) with CMTD who received ultrasound-guided popliteal nerve block catheters with a single-injection saphenous nerve block for foot and ankle surgery. The authors report low postoperative numerical pain scores as well as high patient satisfaction.4 Schmitt et al10 previously reported similar findings effective analgesia without catheter-associated complications or disease exacerbations in an adult case-series of CMTD patients who received nerve-stimulator guided popliteal nerve catheters for foot and ankle surgery.
This reported patient reported excellent postoperative analgesia with single-shot PNB for a complex ankle surgery. Anatomically, the ultrasound examination of the popliteal nerve in our patient was consistent with previously described “onion-bulb” appearance (Figure 1). This “onion-bulb” is attributed to a cycle of demyelination and remyelination with subsequent nerve enlargement.8 Though formal measurements were not taken during ultrasound examination, the nerve appeared to be enlarged which is also consistent with previous descriptions of nerve appearance in CMTD patients.8 There were no noted perioperative complications, pertaining to surgery or anesthesia, including with PNB placement. However, there was a prolonged sensory block, approximately 36-hours, as reported by the patient’s parent. This finding of unreliable block duration has also been reported in the adult literature.5,9 Bupivacaine 0.25% was administered for PNB with a total dose 1.75 mg/kg, well below toxic dosing, and without any block additives. Bupivacaine is considered to have a slow onset with long duration, typically reported between 4 and 12 hours.13
When a PNB has a longer than expected duration of action, there is concern for nerve injury or in this patient’s case, disease exacerbation. There are three general mechanisms of nerve injury attributed to regional anesthesia and include traumatic injury (whether mechanical or injection related), toxic injury (chemical), and ischemic injury (Table 1).11,12,14 The resultant injury can lead to either axonal loss (axonotmesis or neurotmesis) or neuropraxia, with neuropraxic injuries having a better prognosis due to preservation of the axon.11,12 If a patient develops signs and symptoms consistent with nerve injury following PNB, the patient should have a complete physical exam with differentiation between motor and sensory deficits and presence or absence of pain (Table 1).11,14,15 With mild deficits, reassurance and observation is often sufficient given that the majority of neurological injury following PNB will resolve within 4–6 weeks.11,14,15 However, with more severe deficits, it is recommended to obtain further workup including electrophysiologic studies such as nerve conduction studies and electromyography along with nerve imaging studies.11,14,15 Ideally, the studies should first be obtained within a few days of injury and then again 2–3 weeks later.11,14,15
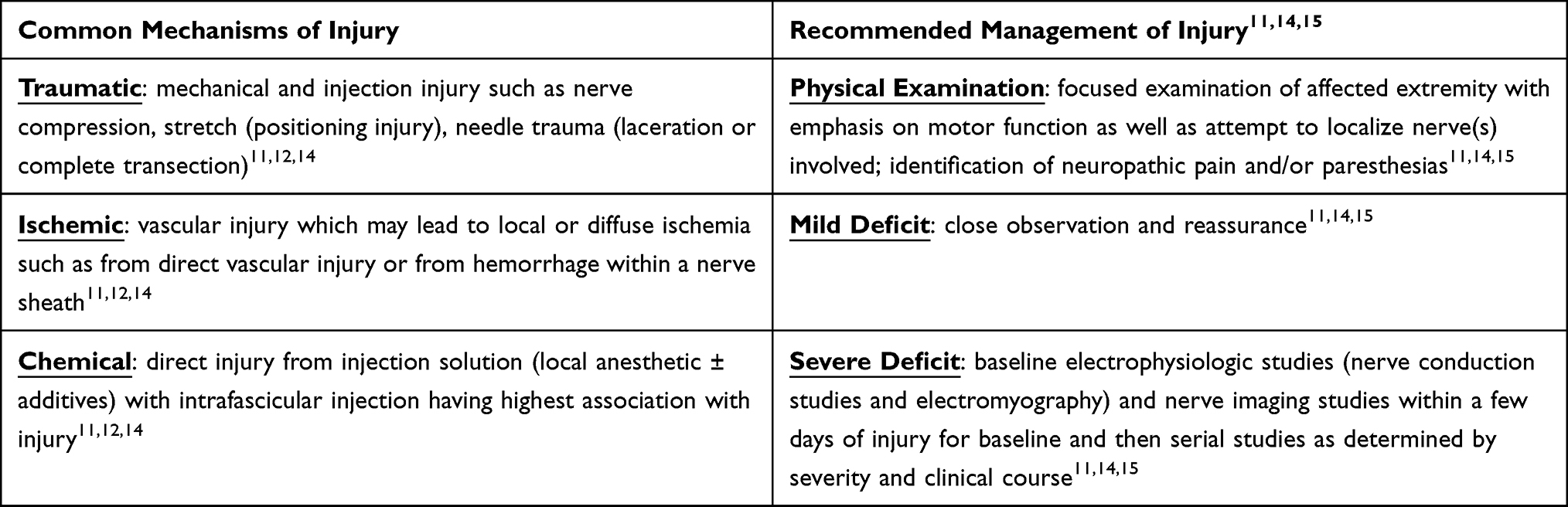 |
Table 1 Nerve Injury Following Peripheral Nerve Block |
In the presented case, there were no noted difficulties or immediate complications during PNB placement, and the needle was visualized utilizing ultrasound guidance without observed direct nerve or vascular injury. The surgical procedure was uneventful, tourniquet time was within accepted limits, and there were no obvious patient positioning problems that could have contributed to nerve injury. The postoperative splint was not too tight, potentially causing nerve entrapment and/or vascular occlusion. Because the motor block resolved within the expected time frame and the patient was not describing new neuropathic pain or paresthesias, the decision was made to reassure the family and continue to observe. Electrophysiologic studies and/or nerve imaging was not obtained prior to patient discharge. The sensory block completely resolved after approximately 36-hours. The patient did not have any identified long-term complications, paresthesias, or disease exacerbations over the course of 2 years during follow-up surgical appointments. Therefore, his course seems to parallel that of other case reports in the literature that have described an unreliable block duration.
In conclusion, patients with a suspected postoperative nerve injury following a PNB should receive a physical examination with clear identification and description of deficits. Most injuries are typically mild and nearly all will resolve within 4–6 weeks. For more severe deficits, obtaining electrophysiologic studies and nerve imaging as a baseline is recommended, with serial follow-up studies as warranted based on clinical course.11,14,15 When considering pediatric patients with CMTD, further research is required to definitively delineate the overall safety of and risks/benefits associated with PNB.
Abbreviations
CARE, Case Report Guidelines; CMTD, Charcot Marie Tooth Disease; EQUATOR, Enhancing the Quality and Transparency of Health Research; PNB, Peripheral Nerve Block.
Funding
No funding was received for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Greenberg RS, Parker SD. Anesthetic management for the child with Charcot-Marie-Tooth Disease. Anesth Analg. 1992;74(2):305–307. doi:10.1213/00000539-199202000-00026
2. McSwain JR, Doty JW, Wilson SH. Regional anesthesia in patients with pre-existing neurologic disease. Curr Opin Anaesthesiol. 2014;27(5):538–543. doi:10.1097/ACO.0000000000000107
3. Barbary JB, Remerand F, Brilhault J, Laffon M, Fusciardi J. Ultrasound-guided nerve blocks in the Charcot-Marie-Tooth disease and Friedreich’s ataxia. Br J Anaesth. 2012;108(6):1042–1043. doi:10.1093/bja/aes160
4. An T, Schwartz E, Kissen M, Pollock G, Pfeffer G. Safety and efficacy of postoperative indwelling popliteal nerve catheters for outpatient Charcot-Marie-Tooth Surgery. Foot Ankle Int. 2022;43(4):504–508. doi:10.1177/10711007211060038
5. Bui AH, Marco AP. Peripheral nerve blockade in a patient with Charcot-Marie-Tooth Disease. Can J Anaesth. 2008;55(10):718–719. doi:10.1007/BF03017751
6. Dhir S, Balasubramanian S, Ross D. Ultrasound-guided peripheral regional blockade in patients with Charcot-Marie-Tooth Disease: a review of three cases. Can J Anaesth. 2008;55(8):515–520. doi:10.1007/BF03016671
7. McClain RL, Rubin DI, Bais KS, Navarro AM, Robards CB, Porter SB. [Regional anesthesia in patients with Charcot-Marie-Tooth disease: a historical cohort study of 53 patients]. Anesthesie regionale chez les patients atteints de la maladie de Charcot-Marie-Tooth: une etude de cohorte historique de 53 patients. Can J Anaesth. 2022;69(7):880–884. French. doi:10.1007/s12630-022-02258-5
8. Shiraishi T, Masumoto K, Nakamura M, Hidano G. Enlarged brachial plexus nerve found during ultrasound-guided peripheral nerve block diagnosed as Charcot-Marie-Tooth Disease: a case report. Local Reg Anesth. 2020;13:141–146. doi:10.2147/LRA.S270189
9. Jacob AK, Kopp SL, Hebl JR. Regional anesthesia in the patient with preexisting neurologic disease. In: Hadzic A, editor. Hadzic’s Textbook of Regional Anesthesia and Acute Pain Management, 2e. McGraw-Hill Education; 2017.
10. Schmitt HJ, Huberth S, Huber H, Munster T. Catheter-based distal sciatic nerve block in patients with Charcot-Marie-Tooth Disease. BMC Anesthesiol. 2014;14(1):8. doi:10.1186/1471-2253-14-8
11. Sorenson EJ. Neurological injuries associated with regional anesthesia. Reg Anesth Pain Med. 2008;33(5):442–448. doi:10.1016/j.rapm.2005.08.011
12. Barrington MJ, Brull R, Reina MA, Hadzic A. Complications and prevention of neurologic injury with peripheral nerve blocks. In: Hadzic A, editor. Hadzic’s Textbook of Regional Anesthesia and Acute Pain Management, 2e. McGraw-Hill Education; 2017.
13. Barash PG. Clinical Anesthesia, 8e: EBook Without Multimedia. Wolters Kluwer; 2017.
14. Weyker PD, Webb CA, Pham TM. Workup and management of persistent neuralgia following nerve block. Case Rep Anesthesiol. 2016;2016:9863492. doi:10.1155/2016/9863492
15. Watson JC. Assessment of neurologic complications of regional anesthesia. In: Hadzic A, editor. Hadzic’s Textbook of Regional Anesthesia and Acute Pain Management, 2e. McGraw-Hill Education; 2017.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Utility of Ultrasound-Guided Erector Spinae Plane Blocks for Postoperative Pain Management Following Thoracolumbar Spinal Fusion Surgery
Zelenty WD, Li TY, Okano I, Hughes AP, Sama AA, Soffin EM
Journal of Pain Research 2023, 16:2835-2845
Published Date: 16 August 2023
Incidence of Hemidiaphragmatic Paresis After Low Volume of Anterior Suprascapular Nerve Block for Arthroscopic Shoulder Surgery: A Randomized, Double-Blind Controlled Trial
Tunprasit C, Areeruk P, Chawachart C, Nitithamakul W, Saeaeh L, Termpornlert S, Arnuntasupakul V
Journal of Pain Research 2026, 19:568402
Published Date: 23 January 2026