Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Progressive Resistance Training Combined with Neuromuscular Electrical Stimulation for Sarcopenic Dysphagia in Elderly Inpatients: A Retrospective Cohort Study in China
Authors Ma J, Zhang H, Shu S, Qiu F, Chen H, Jiao X, Ma C, Ding X
Received 12 January 2026
Accepted for publication 19 May 2026
Published 9 June 2026 Volume 2026:19 595697
DOI https://doi.org/10.2147/JMDH.S595697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Jiangchen Ma,1,* Hongzhu Zhang,1,* Song Shu,2,* Fanghui Qiu,3 Haiyan Chen,2 Xiaofei Jiao,4 Cui Ma,5 Xiaowei Ding2
1Department of Geriatrics, Affiliated Hangzhou First People’s Hospital Chengbei Campus, School of Medicine, Westlake University (Hangzhou Geriatric Hospital), Hangzhou, Zhejiang, 310000, People’s Republic of China; 2Department of Rehabilitation Medicine, Affiliated Hangzhou First People’s Hospital Chengbei Campus, School of Medicine, Westlake University (Hangzhou Geriatric Hospital), Hangzhou, Zhejiang, 310000, People’s Republic of China; 3Department of Rehabilitation Medicine, Hangzhou First People’s Hospital Chengbei Campus (Hangzhou Geriatric Hospital), Hangzhou, Zhejiang, People’s Republic of China; 4Department of Radiology, Affiliated Hangzhou First People’s Hospital Chengbei Campus, School of Medicine, Westlake University (Hangzhou Geriatric Hospital), Hangzhou, Zhejiang, 310000, People’s Republic of China; 5Department of Endocrinology, The First People’s Hospital of Yuhang District, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaowei Ding, Department of Rehabilitation Medicine, Affiliated Hangzhou First People’s Hospital Chengbei Campus, School of Medicine, Westlake University (Hangzhou Geriatric Hospital), 50 Jingshen Street, Gongshu District, Hangzhou, 310000, Zhejiang, People’s Republic of China, Tel +86-13758120616, Email [email protected]
Background: Sarcopenic dysphagia, defined as swallowing dysfunction attributable to generalized skeletal muscle loss involving swallowing-related musculature, poses a growing challenge in geriatric rehabilitation. While conventional swallowing therapy (CST) and neuromuscular electrical stimulation (NMES) have demonstrated individual efficacy, combined therapeutic approaches incorporating progressive resistance training (PRT) may yield superior outcomes, yet evidence specific to sarcopenic dysphagia remains limited.
Objective: To evaluate the efficacy of PRT combined with NMES for improving swallowing function and nutritional status in elderly inpatients with sarcopenic dysphagia.
Methods: This retrospective cohort study in Hangzhou, China analyzed 96 elderly inpatients (mean age: 81.9 years) with sarcopenic dysphagia treated from January 2022 to December 2024 (6-week follow-up). Patients received one of three treatment protocols: CST alone (n=36), CST combined with NMES (CST+NMES; n=33), or CST combined with NMES and PRT (CST+NMES+PRT; n=27). Primary outcomes included the Standardized Swallowing Assessment (SSA), Videofluoroscopic Dysphagia Scale (VDS), and oral transit time (OTT). Secondary outcomes included the Functional Oral Intake Scale (FOIS), Penetration-Aspiration Scale (PAS), and nutritional parameters.
Results: All groups demonstrated significant within-group improvements (P < 0.001). Between-group differences significantly favored CST+NMES+PRT. SSA improvement was greatest in CST+NMES+PRT (− 8.40 ± 2.85 points) versus CST+NMES (− 5.70 ± 2.42) and CST alone (− 3.20 ± 1.95) (F = 8.21, P < 0.001). VDS pharyngeal scores demonstrated significant between-group differences (P < 0.001). FOIS improvement was significantly greater in CST+NMES+PRT (median change: 3 [IQR: 2– 3]; H = 28.45, P < 0.001). Prealbumin showed significant between-group differences (P = 0.013); serum albumin did not reach significance.
Conclusion: The combination of PRT with NMES and conventional swallowing therapy was associated with greater improvements in swallowing function compared with less intensive protocols in elderly inpatients with sarcopenic dysphagia. The retrospective design limits causal inference; randomized controlled trials are needed to confirm these findings.
Keywords: sarcopenic dysphagia, progressive resistance training, neuromuscular electrical stimulation, swallowing disorders, elderly, rehabilitation
Introduction
Sarcopenic dysphagia is a distinct clinical entity characterized by swallowing dysfunction attributable to generalized skeletal muscle loss and specific deterioration of swallowing-related musculature. This condition was first conceptualized by Wakabayashi in 20141 and has subsequently been formalized through a position paper by four professional organizations in Japan, which established diagnostic criteria requiring the presence of both whole-body sarcopenia and swallowing muscle involvement.2 Recent systematic reviews and meta-analyses have demonstrated a robust association between sarcopenia and dysphagia, with pooled adjusted odds ratios of 4.06 (95% CI: 2.27–7.29),3 establishing sarcopenia as an independent risk factor for swallowing dysfunction in elderly populations.
Despite growing recognition of sarcopenic dysphagia as a distinct clinical entity, several diagnostic and conceptual challenges merit acknowledgment. The diagnosis requires the simultaneous presence of whole-body sarcopenia and swallowing muscle involvement; however, dysphagia in elderly inpatients is frequently multifactorial. Subclinical neurological impairment, frailty, deconditioning, polypharmacy, and structural oropharyngeal changes may coexist and contribute to swallowing dysfunction, making exclusive attribution to sarcopenia clinically challenging.2,4 Although the diagnostic criteria explicitly exclude neurogenic dysphagia, undetected subclinical neurological contributions cannot be fully eliminated without comprehensive neurological assessment. Furthermore, much of the existing evidence on dysphagia rehabilitation derives predominantly from neurogenic or post-stroke populations, and its extrapolation to sarcopenic dysphagia requires careful qualification. This diagnostic ambiguity underscores the need for studies specifically targeting well-characterized sarcopenic dysphagia populations.
The epidemiological burden of sarcopenic dysphagia is substantial and increasing with global population aging. A recent large-scale retrospective cohort study of 3134 hospitalized geriatric patients identified multiple independent risk factors, including advanced age, decreased self-care ability, low body mass index, frailty, and poor oral health.4 The prevalence of sarcopenic dysphagia in patients requiring dysphagia rehabilitation has been reported at approximately 32% using the validated 5-step diagnostic algorithm, which employs a tongue pressure cutoff of <20 kPa.5 Notably, dysphagia prevalence is markedly higher in sarcopenic individuals (78.5%) compared with non-sarcopenic counterparts (42.6%),6 underscoring the clinical imperative for targeted therapeutic interventions.
The pathophysiology of sarcopenic dysphagia involves age-related changes in swallowing musculature, including reduced tongue pressure generation, decreased pharyngeal propulsive forces, and compromised suprahyoid muscle function.7,8 Videofluoroscopic studies reveal that only 16% of healthy older adults demonstrate normal swallowing, with 55% showing laryngeal penetration and approximately 15% exhibiting aspiration.9 The relationship between sarcopenia and dysphagia is bidirectional: swallowing dysfunction leads to inadequate nutritional intake, which further exacerbates muscle wasting, creating a vicious cycle that accelerates functional decline.6,10
Current evidence supports multimodal approaches to sarcopenic dysphagia management. Conventional swallowing therapy (CST) encompasses compensatory strategies, dietary modifications, and oral motor exercises, as recommended in clinical practice guidelines.11,12 Progressive resistance training (PRT) targeting swallowing-related muscles has emerged as a promising intervention based on substantial meta-analytic evidence. Systematic reviews of tongue strengthening exercises demonstrate significant improvements in tongue pressure, with the greatest benefits observed in adults aged ≥65 years.13 Chin tuck against resistance (CTAR) has demonstrated superiority over traditional Shaker exercises, with significant improvements in aspiration severity and oral intake measures.14 Expiratory muscle strength training (EMST) has shown efficacy for enhancing suprahyoid muscle activity and reducing aspiration risk in randomized controlled trials.15,16
Neuromuscular electrical stimulation (NMES) represents an adjunctive modality with growing evidence for efficacy. A comprehensive meta-analysis of 46 randomized controlled trials (n = 3,346) demonstrated that NMES combined with conventional therapy significantly improved PAS, FOIS, and SSA scores, while achieving a 63% reduction in swallowing-related complications.17 Optimal stimulation parameters identified through systematic review include frequency of 60–80 Hz, pulse width of 700 μs, and treatment duration of ≤4 weeks with simultaneous voluntary swallowing.18 Recent network meta-analyses have demonstrated that combined NMES approaches achieved markedly superior outcomes, substantially outperforming single modalities.19
Despite compelling theoretical rationale and emerging evidence for combined therapeutic approaches, trials specifically examining PRT combined with NMES for confirmed sarcopenic dysphagia—as opposed to neurogenic or mixed-etiology dysphagia—remain absent from the literature. A pilot randomized controlled trial examining combined electrical stimulation and resistance exercise (Ampcare ESP) demonstrated large effect sizes (Cohen’s d = 0.72–0.82), with FOIS improvements from 2.90 to 4.34 (estimated difference: 1.44 units).20 A recent case report documented successful outcomes using combined NMES and resistance training specifically for sarcopenic dysphagia.21 The present study aimed to evaluate the effectiveness of PRT combined with NMES and conventional therapy compared with less intensive protocols in elderly inpatients with sarcopenic dysphagia.
Methods
Study Design and Ethical Approval
This retrospective cohort study was conducted at Affiliated Hangzhou First People’s Hospital Chengbei Campus, School of Medicine, Westlake University. Medical records of patients treated between January 2022 and December 2024 were reviewed. Although this is a retrospective study, treatment protocols were standardized through institutional clinical protocols established prior to the study period; the PRT and NMES parameters documented in medical records reflect structured departmental protocols applied consistently throughout the study period, rather than individually tailored prescriptions. The study was approved by the Institutional Ethics Committee (Approval No. GL002-202,501-005), which granted a waiver of informed consent for retrospective data analysis. As this was a retrospective study, ethical approval was obtained prior to data extraction and analysis, in accordance with institutional protocols for retrospective research. The study was conducted in compliance with the Declaration of Helsinki and reported according to STROBE guidelines for observational studies. To minimize potential biases, data extraction was performed independently by two investigators (JM and HZ), with discrepancies resolved by consensus or adjudication by a third investigator (XD), using pre-specified standardized data extraction forms.
Participants
Patients were eligible for inclusion if they met the following criteria: (1) age ≥65 years; (2) diagnosis of sarcopenia according to the Asian Working Group for Sarcopenia (AWGS) 2019 criteria,22 defined as low muscle strength (handgrip strength <28 kg for men or <18 kg for women), low physical performance (gait speed <1.0 m/s), and/or low muscle mass (appendicular skeletal muscle mass index <7.0 kg/m2 for men or <5.4 kg/m2 for women by dual-energy X-ray absorptiometry); (3) presence of dysphagia confirmed by clinical assessment using the Standardized Swallowing Assessment and videofluoroscopic swallowing study (VFSS); (4) tongue pressure <20 kPa, consistent with the 5-step sarcopenic dysphagia diagnostic algorithm;5 and (5) completion of at least 6 weeks of treatment with available outcome data.
Exclusion criteria included: (1) dysphagia attributable to neurological conditions (eg., stroke, Parkinson’s disease, motor neuron disease); (2) structural abnormalities of the oropharynx or esophagus; (3) severe cognitive impairment precluding participation in therapy; (4) concurrent treatment with medications known to affect swallowing function; and (5) incomplete medical records.
Patient allocation to treatment groups was not randomized but was based on clinical decision-making at the time of admission by the treating physician, reflecting real-world rehabilitation practice patterns. Of 142 patients initially screened, 96 met all inclusion criteria: 40 were excluded due to neurological etiology of dysphagia, and 6 had incomplete follow-up data. The CST group comprised 36 patients, CST+NMES comprised 33 patients, and CST+NMES+PRT comprised 27 patients. This study was not pre-registered, and sample size was determined by patient availability during the study period rather than a priori power calculation, representing a key limitation of the retrospective design.
Treatment Protocols
Conventional Swallowing Therapy (CST)
All patients received CST as the foundation of treatment, consistent with current clinical practice guidelines.11,12 The protocol comprised: (1) compensatory strategies, including postural adjustments (chin tuck, head rotation) and swallowing maneuvers (supraglottic swallow, effortful swallow); (2) dietary modifications based on International Dysphagia Diet Standardisation Initiative (IDDSI) guidelines; (3) oral motor exercises targeting labial, lingual, and mandibular function; and (4) thermal-tactile stimulation. Sessions were conducted for 30 minutes, twice daily, 6 days per week, for 6 weeks.
Neuromuscular Electrical Stimulation (NMES)
Patients in the CST+NMES and CST+NMES+PRT groups received additional NMES therapy using a VitalStim device (Chattanooga Group, USA). Surface electrodes were placed following optimal placement protocols: horizontal placement above the hyoid bone and at the thyroid notch over the thyrohyoid muscle.23 Stimulation parameters were selected based on systematic review recommendations:18 biphasic rectangular pulses at 80 Hz frequency and 700 μs pulse width, with intensity titrated to achieve visible muscle contraction without discomfort (range: 0–15 mA). NMES was administered for 20 minutes per session, once daily, 6 days per week, with patients performing voluntary swallowing during stimulation to maximize therapeutic effect.
Progressive Resistance Training (PRT)
Patients in the CST+NMES+PRT group received additional PRT targeting swallowing-related muscles. The protocol was designed according to established dosing principles24 and included: (1) tongue strengthening exercises using the Iowa Oral Performance Instrument (IOPI), with resistance set at 60% of maximum isometric pressure and progressively increased to 80%, based on meta-analytic evidence demonstrating optimal gains with this intensity range;13 (2) chin tuck against resistance (CTAR) using an inflatable ball, with 3 sets of 10 repetitions, following protocols demonstrated to be superior to Shaker exercises with better elderly compliance;14 and (3) expiratory muscle strength training (EMST) using a threshold device set at 75% of maximum expiratory pressure, with 5 sets of 5 breaths (25 breaths/day).15 PRT sessions lasted 15–20 minutes, once daily, 6 days per week. Intensity progression followed recommended guidelines of 60% 1RM for untrained patients, advancing to 80% 1RM.24
Outcome Measures
All outcome assessments were performed by trained nurses with a minimum of two years of clinical experience in dysphagia management, using standardized protocols. Different nurses assessed different outcome measures, and assessors were not blinded to treatment group allocation, which is acknowledged as a potential source of detection bias. Primary outcomes included: (1) Standardized Swallowing Assessment (SSA), a validated bedside clinical assessment tool scoring from 18 (normal) to 46 (severe dysfunction), with demonstrated sensitivity of 97% and specificity of 90% for dysphagia detection;25 (2) Videofluoroscopic Dysphagia Scale (VDS), with separate scores for oral (0–40) and pharyngeal (0–60) phases, demonstrating excellent inter-rater reliability (ICC = 0.953) and intra-rater reliability (ICC = 0.958) when using standardized protocols;26 VDS scores were interpreted according to published classification thresholds: oral Phase 0–17 (normal), 18–29 (mild dysfunction), 30–40 (moderate-severe dysfunction); pharyngeal phase 0–17 (normal), 18–29 (mild dysfunction), 30–60 (moderate-severe dysfunction); and (3) oral transit time (OTT) measured in seconds during VFSS (normal reference value: ≤1.0 second).26
Secondary outcomes included: (1) Functional Oral Intake Scale (FOIS), a validated 7-level ordinal scale (1 = nothing by mouth; 7 = total oral diet without restrictions), with established inter-rater reliability of κ = 0.86–0.91 and 85% perfect agreement;27,28 (2) Penetration-Aspiration Scale (PAS), an 8-point ordinal scale developed by Rosenbek et al,29,30 where score 1 indicates no airway invasion and score 8 indicates silent aspiration; and (3) nutritional parameters including serum albumin, prealbumin, and Mini Nutritional Assessment (MNA) scores. The full 18-item MNA was administered, assessing anthropometric measurements, general health status, dietary intake, and subjective self-assessment; total scores range from 0 to 30, with ≥24 indicating normal nutritional status, 17–23.5 indicating risk of malnutrition, and <17 indicating malnutrition.31
Statistical Analysis
Continuous variables were assessed for normality using Shapiro–Wilk tests and expressed as mean ± standard deviation. Ordinal variables (FOIS and PAS) were analyzed using non-parametric methods and reported as median with interquartile range, as recommended given the non-interval nature of these scales.32 Baseline characteristics were compared using one-way analysis of variance (ANOVA) for continuous variables and Kruskal–Wallis tests for ordinal variables.
Between-group differences in treatment outcomes were analyzed using one-way ANOVA for continuous variables, with Bonferroni correction for post-hoc pairwise comparisons. Kruskal–Wallis tests with Dunn’s post-hoc procedure were used for ordinal variables. Within-group changes from baseline to 6 weeks were assessed using paired t-tests for continuous variables and Wilcoxon signed-rank tests for ordinal variables.
Effect sizes were calculated using eta-squared (η2) for ANOVA, with conventional thresholds of 0.01 (small), 0.06 (medium), and 0.14 (large). Statistical significance was set at P < 0.05. All analyses were performed using R version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
A total of 142 patients were initially screened, of whom 96 met all inclusion criteria and were included in the analysis (Figure 1). Forty patients were excluded due to neurological etiology of dysphagia, and 6 patients had incomplete follow-up data. The CST group comprised 36 patients, the CST+NMES group comprised 33 patients, and the CST+NMES+PRT group comprised 27 patients.
 |
Figure 1 Study flow diagram showing patient screening, enrollment, and allocation to treatment groups. |
Baseline demographic and clinical characteristics are summarized in Table 1. The three groups were comparable with respect to age (overall mean: 81.9 ± 5.9 years), sex distribution (44% male), body mass index (20.6 ± 2.9 kg/m2), and sarcopenia-related parameters. All patients met AWGS 2019 criteria for sarcopenia.22 No significant between-group differences were observed for any baseline swallowing assessments or nutritional parameters (all P > 0.05).
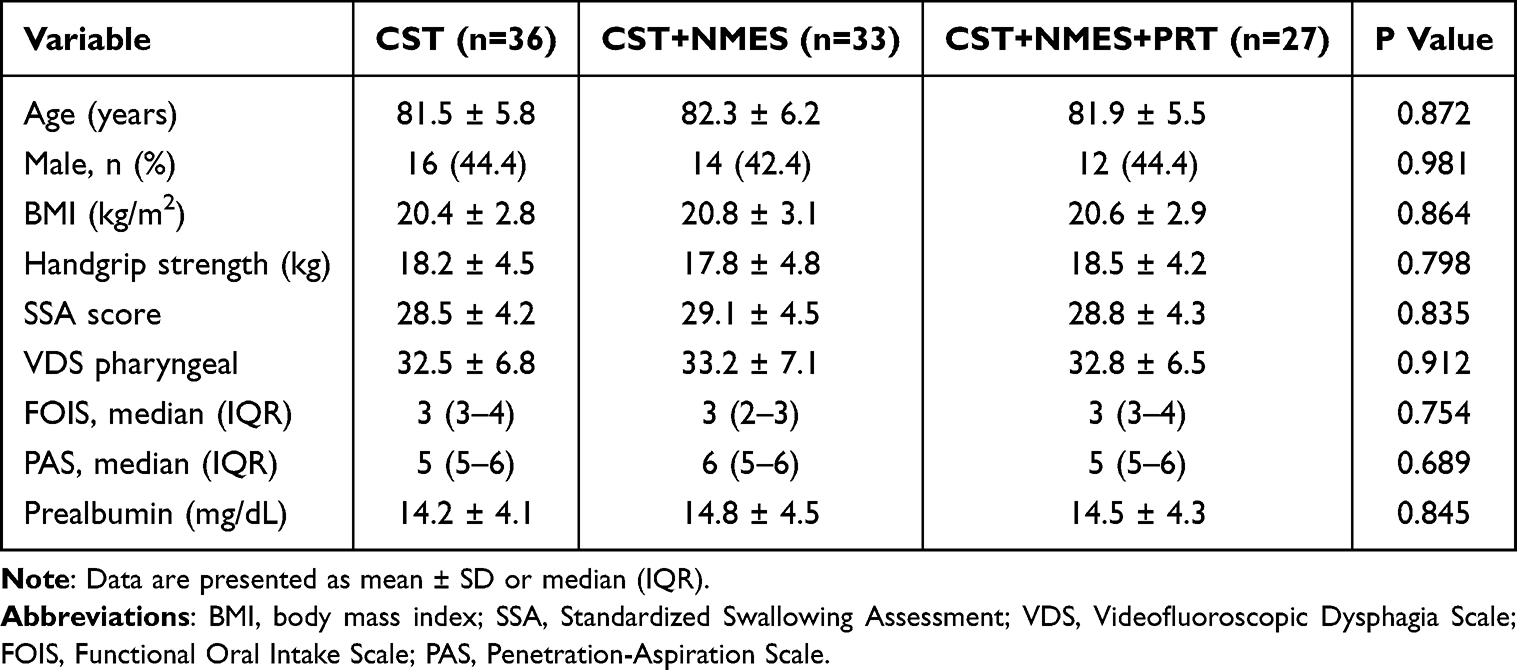 |
Table 1 Baseline Demographic and Clinical Characteristics |
Treatment Adherence
Treatment adherence was generally high across all groups and comparable to rates reported in previous multimodal therapy trials.20 In the CST group, 34 of 36 patients (94.4%) completed all scheduled sessions. In the CST+NMES group, 31 of 33 patients (93.9%) achieved full adherence. The CST+NMES+PRT group demonstrated slightly lower adherence, with 24 of 27 patients (88.9%) completing all sessions, consistent with previous observations that CTAR-based protocols demonstrate better tolerability than traditional Shaker exercises but may still present challenges for some elderly patients.14 No serious adverse events were reported, consistent with safety recommendations for geriatric exercise interventions.12
Swallowing Function Outcomes
All three groups demonstrated statistically significant improvements in swallowing function from baseline to 6 weeks (Table 2). Between-group comparisons revealed significant differences in the magnitude of improvement favoring the CST+NMES+PRT group.
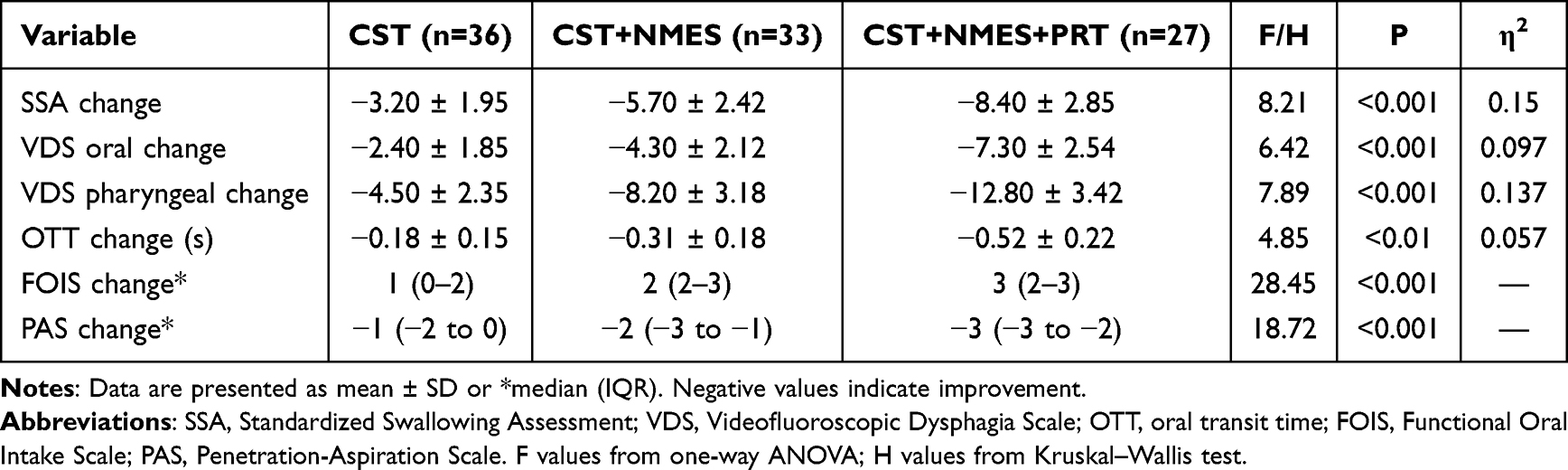 |
Table 2 Swallowing Function Outcomes After 6 Weeks of Treatment |
For the primary outcome of SSA score change, the CST+NMES+PRT group demonstrated the greatest improvement (mean change: −8.40 ± 2.85 points), followed by CST+NMES (−5.70 ± 2.42 points) and CST alone (−3.20 ± 1.95 points). One-way ANOVA confirmed significant between-group differences (F = 8.21, P < 0.001), with a large effect size (η2 = 0.150). Post-hoc comparisons with Bonferroni correction revealed significant differences between all pairwise group comparisons (all P < 0.01).
VDS pharyngeal phase scores demonstrated a similar pattern, with the CST+NMES+PRT group showing the greatest reduction (improvement) in scores (−12.80 ± 3.42). The between-group effect size was large (η2 = 0.137, P < 0.001). VDS oral phase scores also differed significantly between groups (η2 = 0.097, P < 0.001). OTT reductions were observed in all groups, with a medium effect size for between-group differences (η2 = 0.057, P < 0.01).
For FOIS, the CST+NMES+PRT group demonstrated the greatest improvement (median change: 3 [IQR: 2–3]), compared with CST+NMES (median change: 2 [IQR: 2–3]) and CST alone (median change: 1 [IQR: 0–2]). Kruskal–Wallis testing confirmed significant between-group differences (H = 28.45, P < 0.001). PAS scores improved significantly across all groups, with the CST+NMES+PRT group showing the greatest reduction (H = 18.72, P < 0.001). The magnitude of improvements across treatment groups is illustrated in Figure 2, which demonstrates the progressive increase in treatment effect from CST alone to CST+NMES to CST+NMES+PRT for all swallowing outcomes.
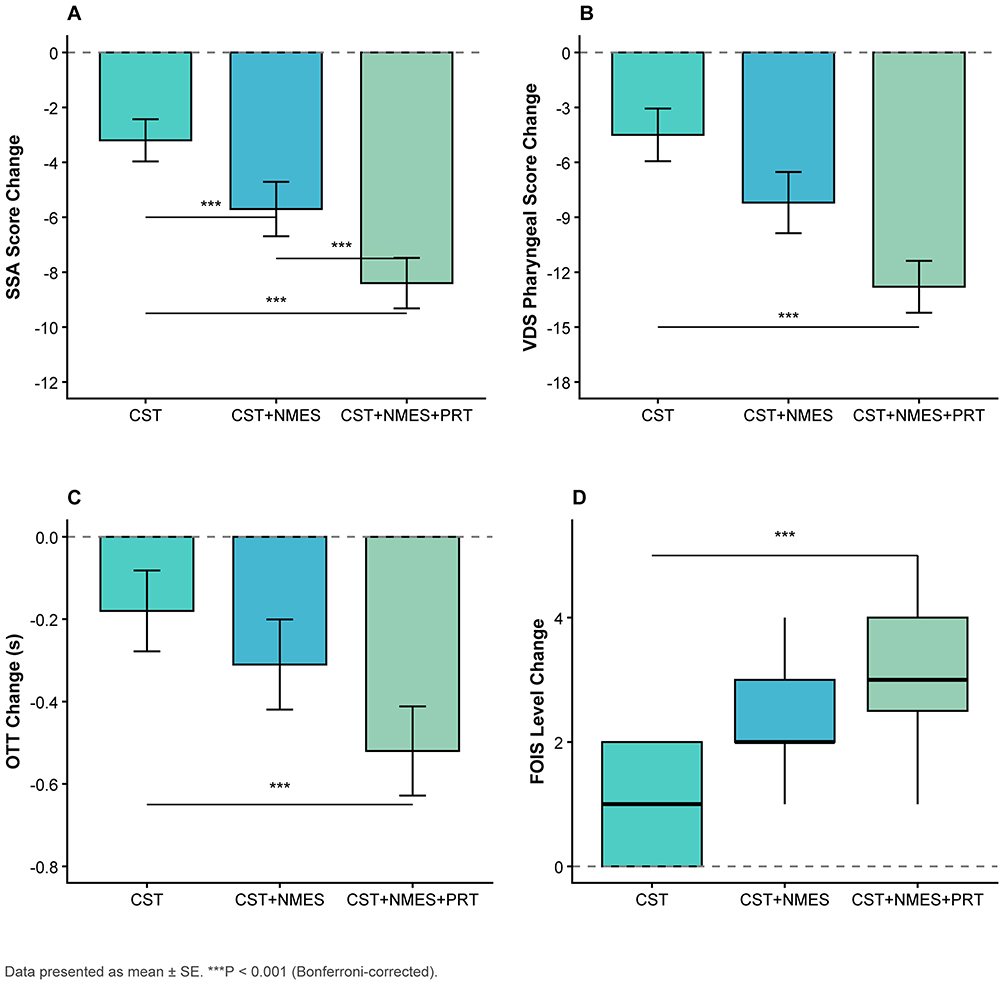 |
Figure 2 Swallowing function outcomes after 6 weeks of treatment. (A) SSA score change; (B) VDS pharyngeal score change; (C) OTT change; (D) FOIS level change. Data are presented as mean ± SE for continuous variables and box plots for ordinal variables. ***P < 0.001. |
Nutritional Outcomes
Nutritional parameters demonstrated variable responses to treatment (Table 3). Prealbumin levels increased significantly in all groups, with the greatest increase observed in the CST+NMES+PRT group (mean change: +4.77 ± 2.85 mg/dL). Between-group differences were statistically significant (F = 4.52, P = 0.013), with a medium effect size (η2 = 0.055).
 |
Table 3 Nutritional Outcomes After 6 Weeks of Treatment |
MNA scores improved across all groups, with a small but statistically significant between-group difference (F = 2.18, P = 0.042, η2 = 0.025). In contrast, serum albumin levels, while showing a trend toward improvement, did not demonstrate significant between-group differences (F = 1.42, P = 0.246). The nutritional response patterns across treatment groups are presented in Figure 3, highlighting the differential effects on prealbumin compared with albumin.
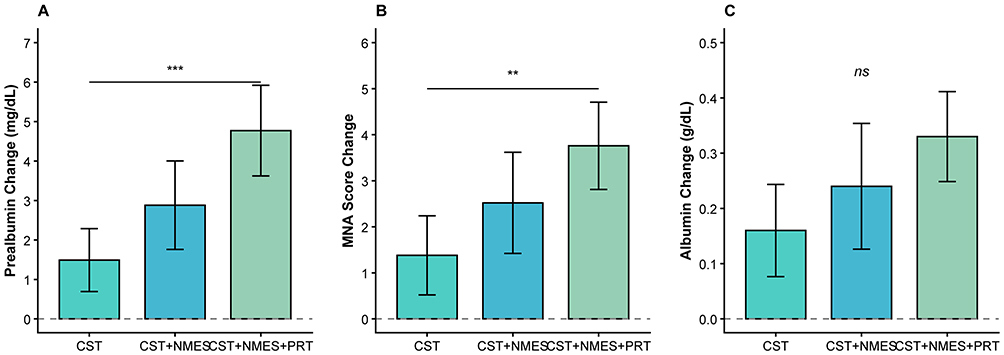 |
Figure 3 Nutritional outcomes after 6 weeks of treatment. (A) Prealbumin change; (B) MNA score change; (C) Albumin change. Data are presented as mean ± SE. **P < 0.01, ***P < 0.001. Abbreviation: ns, not significant. |
Discussion
This retrospective cohort study examined the efficacy of progressive resistance training combined with neuromuscular electrical stimulation and conventional therapy for sarcopenic dysphagia in elderly inpatients. Our findings suggest that the addition of PRT to NMES and conventional swallowing therapy may provide incremental benefits for swallowing function, with large effect sizes observed for SSA (η2 = 0.150) and VDS pharyngeal scores (η2 = 0.137). These results align with and extend previous literature on multimodal dysphagia rehabilitation19,20 and provide preliminary evidence supporting targeted resistance training for the sarcopenic component of swallowing dysfunction.
A central conceptual challenge in interpreting these findings, and in the sarcopenic dysphagia field more broadly, deserves explicit discussion. The diagnosis of sarcopenic dysphagia requires ruling out neurological etiologies; however, in clinical practice, dysphagia in elderly inpatients is frequently multifactorial. Subclinical neurological impairment, frailty, deconditioning, medication effects, and structural oropharyngeal changes may coexist, rendering strict etiological attribution challenging even with the validated 5-step diagnostic algorithm.5 Although patients with established neurological diagnoses were systematically excluded (40 patients excluded on this basis), the presence of undetected subclinical neurological contributions cannot be fully eliminated without comprehensive neurological evaluation. Consequently, the observed treatment benefits may partly reflect general rehabilitation effects common to all dysphagia interventions, rather than effects specific to sarcopenic pathophysiology. This interpretation is further complicated by the fact that much of the evidence cited in the present discussion derives from neurogenic or post-stroke populations,13,14,17 and its applicability to sarcopenic dysphagia requires careful qualification. Readers should therefore interpret our findings as preliminary evidence for this population, pending confirmation from trials with rigorous diagnostic and neurological exclusion protocols.
The observed treatment effects are consistent with the theoretical rationale underlying PRT for sarcopenic dysphagia. Swallowing requires coordinated activity of over 30 muscles,7 many of which are susceptible to age-related sarcopenia. Meta-analytic evidence indicates that tongue strengthening exercises yield significant improvements in tongue pressure, with the greatest benefits observed in adults aged ≥65 years (MD = 8.01 kPa; 95% CI: 4.39–11.64).13 By combining tongue strengthening with CTAR and EMST, our protocol addressed multiple components of the swallowing musculature, potentially explaining the larger effect sizes observed compared with NMES or conventional therapy alone.
The large effect sizes observed for primary swallowing outcomes in our study (η2 = 0.137–0.150) are comparable to those reported in meta-analyses of combined therapeutic approaches. The 2025 network meta-analysis demonstrated that NMES combined with effortful swallowing and traditional therapy achieved SUCRA values of 73.9–95.3%, substantially outperforming single modalities (7.7–36.2%).19 Our findings suggest that the addition of structured PRT may provide similar or greater benefits for the specific population of patients with sarcopenic dysphagia, though this hypothesis requires confirmation in randomized trials.
The improvement in FOIS scores is particularly relevant from a clinical perspective. The median 3-point improvement observed in the CST+NMES+PRT group represents a substantial functional gain, potentially allowing patients to transition from tube feeding to modified oral diets. This magnitude of improvement is consistent with the estimated FOIS improvement of 1.44 units reported in a pilot RCT of combined NMES and resistance exercise.20 Such improvements have important implications for quality of life, as nutritional status has been shown to mediate approximately 30% of the relationship between dysphagia severity and quality of life outcomes.33
These effect magnitudes are broadly consistent with prior reports. The improvement observed in the CST+NMES group for SSA scores is consistent with the mean difference of −6.39 reported in a comprehensive meta-analysis of NMES combined with conventional therapy (46 RCTs, n = 3,346).17 Regarding nutritional outcomes, the absence of significant between-group differences for albumin likely reflects its longer plasma half-life (15–20 days) and sensitivity to acute-phase responses rather than short-term nutritional intake,31 rendering it a less sensitive marker of nutritional recovery over a 6-week period compared with prealbumin (half-life: 2–3 days).
Our findings are broadly consistent with previous research examining resistance-based and electrical stimulation interventions for dysphagia. A systematic review and meta-analysis of tongue strengthening exercises (12 RCTs, n = 388) demonstrated significant improvements in anterior tongue strength (MD = 5.34 kPa) and posterior tongue strength (MD = 8.12 kPa).13 Similarly, meta-analytic evidence for CTAR (9 RCTs, n = 548) has demonstrated superiority over traditional Shaker exercises, with significant improvements in PAS scores (MD = −1.43) and oral intake measures (SMD = −1.82).14
The added benefit of NMES observed in this study aligns with comprehensive meta-analytic evidence. A systematic review of 46 RCTs (n = 3,346) found that NMES combined with conventional therapy significantly improved multiple outcomes, including a 63% reduction in swallowing-related complications (OR = 0.37; 95% CI: 0.24–0.57).17 Importantly, recent evidence suggests that NMES alone may not be superior to conventional therapy, but the combination achieves significantly better outcomes (SMD = 0.91; 95% CI: 0.68–1.14),23 consistent with our findings.
The specific application of combined PRT and NMES for sarcopenic dysphagia represents an emerging area of research. The 2024 case report by Eimoto et al documented successful outcomes using combined NMES and resistance training specifically for confirmed sarcopenic dysphagia,21 representing the first such report in the literature. The present study extends this preliminary evidence by examining outcomes in a larger cohort with standardized treatment protocols and validated outcome measures.
Several alternative explanations for the observed findings warrant consideration. First, the dose-response relationship between treatment intensity and outcomes may partly reflect non-specific effects of increased therapeutic contact time: the CST+NMES+PRT group received approximately 45–50 minutes of therapy per day, compared with 30 minutes for CST alone, and this differential exposure could independently contribute to better outcomes irrespective of the specific PRT mechanism. Second, unmeasured differences in patient motivation, family engagement, or therapist attention across groups may have confounded the observed effects. Third, because group allocation was based on clinical judgment, patients selected for more intensive treatment may have had greater functional reserve at baseline, introducing selection bias despite the statistically comparable baseline characteristics. These alternative explanations cannot be excluded given the retrospective, non-randomized design, and should be addressed in future prospective trials.
Limitations
Several limitations warrant consideration when interpreting these findings. First, the retrospective design precludes causal inference and introduces potential confounding. Treatment allocation was based on clinical judgment rather than randomization, raising the possibility that patients selected for more intensive treatment may have differed systematically from those receiving standard care. Although baseline characteristics were statistically comparable across groups, unmeasured confounders such as pre-existing frailty severity, motivation, or family support could have influenced outcomes.
Second, several sources of bias merit acknowledgment. Selection bias may have occurred if patients with greater functional reserve were preferentially assigned to the PRT group. Detection bias is also possible, as outcome assessors were not blinded to treatment allocation. While the SSA has demonstrated excellent psychometric properties (sensitivity 97%, specificity 90%),25 its subjective components may be susceptible to assessor expectations. The absence of blinded assessment represents a significant limitation that should be addressed in future prospective studies.
Third, the relatively small sample size, particularly in the CST+NMES+PRT group (n = 27), limits statistical power for detecting smaller effects and restricts generalizability. The sample size was determined by patient availability during the study period rather than a priori power analysis. Additionally, the single-center design may limit external validity.
Fourth, the 6-week follow-up period does not permit assessment of long-term outcomes or treatment durability. Evidence suggests that exercise-based dysphagia therapies require sustained intervention periods, with recommendations of 8–12 weeks for progressive resistance training.24 Whether the observed improvements are maintained after cessation of treatment remains unknown.
Finally, caution is warranted regarding the potential for adverse effects in elderly populations. Expert consensus recommends that extreme exercise can cause trauma and fatigue in elderly patients, and cognitive and physical limitations may affect compliance.12 The slightly lower adherence rate observed in the CST+NMES+PRT group (88.9% vs. 93.9–94.4%) may reflect these concerns.
Clinical Implications
Despite these limitations, our findings have potential clinical implications when considered alongside existing evidence. Current clinical practice guidelines recommend tongue and pharyngeal strengthening exercises for dysphagia rehabilitation,11,12 and the 2024 VA/DoD clinical practice guidelines specifically recommend CTAR and respiratory muscle strength training.34 Our findings suggest that these recommendations may extend to the specific population of patients with sarcopenic dysphagia, though confirmation through randomized trials is needed.
The PRT protocol employed in this study is feasible for implementation in inpatient rehabilitation settings and utilizes commercially available equipment. However, clinicians should consider patient factors including cognitive status, physical tolerance, and motivation when selecting treatment intensity. The multidisciplinary approach combining physical therapy, speech-language pathology, and nutritional intervention appears essential for optimal outcomes, consistent with position statements emphasizing that sarcopenic dysphagia requires both dysphagia rehabilitation and nutritional support.2,10
Future Directions
Randomized controlled trials with adequate sample sizes are needed to confirm these preliminary findings and establish causal relationships. Such trials should incorporate: (1) blinded outcome assessment to minimize detection bias; (2) longer follow-up periods (≥12 weeks) to assess treatment durability; (3) evaluation of patient-reported outcomes and quality of life measures; and (4) economic analyses to inform resource allocation. Research examining optimal dosing parameters for PRT in sarcopenic dysphagia, including intensity progression and treatment duration, would further inform clinical practice.
Conclusions
In this retrospective cohort study of elderly inpatients with sarcopenic dysphagia, the combination of progressive resistance training with neuromuscular electrical stimulation and conventional swallowing therapy was associated with greater improvements in swallowing function compared with less intensive treatment protocols. Effect sizes were large for primary swallowing outcomes and small to medium for nutritional parameters. These findings are consistent with emerging evidence supporting multimodal rehabilitation approaches for dysphagia and provide preliminary support for targeting the sarcopenic component of swallowing dysfunction. However, the retrospective design and associated limitations preclude definitive conclusions regarding causality. These findings provide a rationale for prospective randomized trials to evaluate the efficacy of combined PRT and NMES for sarcopenic dysphagia. Future trials should incorporate blinded outcome assessment, longer follow-up periods (≥12 weeks), patient-reported outcome measures, and comprehensive neurological exclusion protocols to confirm and extend these preliminary findings.
Abbreviations
AWGS, Asian Working Group for Sarcopenia; CTAR, chin tuck against resistance; CST, conventional swallowing therapy; EMST, expiratory muscle strength training; FOIS, Functional Oral Intake Scale; IDDSI, International Dysphagia Diet Standardisation Initiative; IOPI, Iowa Oral Performance Instrument; MNA, Mini Nutritional Assessment; NMES, neuromuscular electrical stimulation; OTT, oral transit time; PAS, Penetration-Aspiration Scale; PRT, progressive resistance training; RCT, randomized controlled trial; SSA, Standardized Swallowing Assessment; STROBE, Strengthening the Reporting of Observational studies in Epidemiology; VDS, Videofluoroscopic Dysphagia Scale; VFSS, videofluoroscopic swallowing study.
Data Sharing Statement
The data supporting this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Ethics Committee of Affiliated Hangzhou First People’s Hospital Chengbei Campus, School of Medicine, Westlake University (Approval No. GL002-202501-005), which granted a waiver of informed consent for retrospective data analysis. As this was a retrospective study, ethical approval was obtained prior to data extraction and analysis, in accordance with institutional protocols for retrospective research. Patient data confidentiality was maintained throughout the study; all data were de-identified prior to analysis, and no personally identifiable information was retained in the analytical dataset. The study was conducted in compliance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Research Project of Zhejiang Provincial Science and Technology Plan for Traditional Chinese Medicine (Grant No. 2024ZL753), the Research Project of Zhejiang Provincial Medical and Health Science and Technology Plan (Grant No. 2024KY1406), and the Hangzhou Health Science and Technology Program Project (Grant No. B20262643).
Disclosure
The authors declare no conflicts of interest.
References
1. Wakabayashi H. Presbyphagia and sarcopenic dysphagia: association between aging, sarcopenia, and deglutition disorders. J Frailty Aging. 2014;3(2):97–13. doi:10.14283/jfa.2014.8
2. Fujishima I, Fujiu-Kurachi M, Arai H, et al. Sarcopenia and dysphagia: position paper by four professional organizations. Geriatr Gerontol Int. 2019;19(2):91–97. doi:10.1111/ggi.13591
3. Zhao WT, Yang M, Wu HM, et al. Systematic review and meta-analysis of the association between sarcopenia and dysphagia. J Nutr Health Aging. 2018;22(8):1003–1009. doi:10.1007/s12603-018-1055-z
4. He P, Li Y, Ding F, et al. Prevalence and risk factors of sarcopenic dysphagia in elderly hospitalized patients: a retrospective cohort study based on data from a comprehensive geriatric assessment system. BMC Geriatr. 2025;25:525. doi:10.1186/s12877-025-06162-7
5. Wakabayashi H, Kishima M, Itoda M, et al. Diagnosis and treatment of sarcopenic dysphagia: a scoping review. Dysphagia. 2021;36(3):523–531. doi:10.1007/s00455-021-10266-8
6. Chen KC, Jeng Y, Wu WT, et al. Sarcopenic dysphagia: a narrative review from diagnosis to intervention. Nutrients. 2021;13(11):4043. doi:10.3390/nu13114043
7. Clavé P, Shaker R. Dysphagia: current reality and scope of the problem. Nat Rev Gastroenterol Hepatol. 2015;12(5):259–270. doi:10.1038/nrgastro.2015.49
8. Sporns PB, Muhle P, Hanning U, et al. Atrophy of swallowing muscles is associated with severity of dysphagia and age in patients with acute stroke. J Am Med Dir Assoc. 2017;18(7):
9. Wang XW, Hu HJ, Wang CY, et al. Presbyphagia: dysphagia in the elderly. World J Clin Cases. 2023;11(11):2363–2373. doi:10.12998/wjcc.v11.i11.2363
10. Azzolino D, Damanti S, Cesari M. Sarcopenic dysphagia, malnutrition, and oral frailty in elderly: a comprehensive review. Nutrients. 2022;14(5):982. doi:10.3390/nu14050982
11. Korean Dysphagia Society. Clinical practice guidelines for oropharyngeal dysphagia. Ann Rehabil Med. 2023;47(4):183–241. doi:10.5535/arm.23069.
12. Bahat G, Catikkas NM, Ozcan F, et al. Best practice recommendations for geriatric dysphagia management with 5 Ws and 1H. Ann Geriatr Med Res. 2022;26(2):94–124. doi:10.4235/agmr.22.0035
13. Lin CJ, Lee YS, Hsu CF, et al. Effects of tongue strengthening exercises on tongue muscle strength: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2022;12:10438. doi:10.1038/s41598-022-14335-2
14. Liu J, Wang Q, Tian J, et al. Effects of chin tuck against resistance exercise on post-stroke dysphagia rehabilitation: a systematic review and meta-analysis. Front Neurol. 2023;13:1109140. doi:10.3389/fneur.2022.1109140
15. Park JS, Oh DH, Chang MY, Kim KM. Effects of expiratory muscle strength training on oropharyngeal dysphagia in subacute stroke patients: a randomised controlled trial. J Oral Rehabil. 2016;43(5):364–372. doi:10.1111/joor.12382
16. Wang Z, Wang Z, Fang Q, et al. Effect of expiratory muscle strength training on swallowing and cough functions in patients with neurological diseases: a meta-analysis. Am J Phys Med Rehabil. 2019;98(12):1060–1066. doi:10.1097/PHM.0000000000001242
17. Wang Y, Xu L, Wang L, et al. Effects of transcutaneous neuromuscular electrical stimulation on post-stroke dysphagia: a systematic review and meta-analysis. Front Neurol. 2023;14:1163045. doi:10.3389/fneur.2023.1163045
18. Díaz-Pérez I, Leirós-Rodríguez R. Effectiveness of different application parameters of neuromuscular electrical stimulation for the treatment of dysphagia after a stroke: a systematic review. J Clin Med. 2020;9(8):2618. doi:10.3390/jcm9082618
19. Wang S, Shi Z, Wu T, et al. Comparative efficacy of combined and single neuromuscular electrical stimulation and traditional swallowing training for neurogenic dysphagia: a network meta-analysis. Front Neurol. 2025;16:1700317. doi:10.3389/fneur.2025.1700317
20. Sproson L, Pownall S, Enderby P, Freeman J. Combined electrical stimulation and exercise for swallow rehabilitation post-stroke: a pilot randomized control trial. Int J Lang Commun Disord. 2018;53(2):405–417. doi:10.1111/1460-6984.12359
21. Eimoto K, Nagai K, Nakao Y, et al. Swallowing rehabilitation with neuromuscular electrical stimulation for sarcopenic dysphagia: a case report. Cureus. 2024;16(4):e59256. doi:10.7759/cureus.59256
22. Chen LK, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21(3):300–307.e2. doi:10.1016/j.jamda.2019.12.012
23. Doan TN, Ho WC, Wang LH, et al. Therapeutic effect and optimal electrode placement of transcutaneous neuromuscular electrical stimulation in patients with post-stroke dysphagia. Life. 2022;12(6):875. doi:10.3390/life12060875
24. Krekeler BN, Rowe LM, Connor NP. Dose in exercise-based dysphagia therapies: a scoping review. Dysphagia. 2021;36(1):1–32. doi:10.1007/s00455-020-10104-3
25. Perry L. Screening swallowing function of patients with acute stroke. Part one: identification, implementation and initial evaluation of a screening tool for use by nurses. J Clin Nurs. 2001;10(4):463–473. doi:10.1046/j.1365-2702.2001.00501.x
26. Min I, Woo H, Kim JY, et al. Inter-rater and intra-rater reliability of the videofluoroscopic dysphagia scale with the standardized protocol. Dysphagia. 2024;39(1):43–51. doi:10.1007/s00455-023-10590-1
27. Crary MA, Carnaby Mann GD, Groher ME. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch Phys Med Rehabil. 2005;86(8):1516–1520. doi:10.1016/j.apmr.2004.11.049
28. Milewska M, Jamroz B, Panczyk M, et al. Validation of the polish version of the functional oral intake scale against flexible endoscopic evaluation of swallowing and the international dysphagia diet standardization initiative functional diet scale. Front Nutr. 2025;12:1524335. doi:10.3389/fnut.2025.1524335
29. Rosenbek JC, Robbins JA, Roecker EB, et al. A penetration-aspiration scale. Dysphagia. 1996;11(2):93–98. doi:10.1007/BF00417897
30. Kitila M, Borders JC, Krisciunas GP, et al. Confidence, accuracy, and reliability of penetration-aspiration scale ratings on flexible endoscopic evaluations of swallowing by speech pathologists. Dysphagia. 2024;39(3):504–513. doi:10.1007/s00455-023-10635-5
31. Nakadate A, Otaka Y, Kondo K, et al. Nutritional assessment in adult patients with dysphagia: a scoping review. Nutrients. 2021;13(3):778. doi:10.3390/nu13030778
32. Steele CM, Grace-Martin K. Reflections on clinical and statistical use of the penetration-aspiration scale. Dysphagia. 2017;32(5):601–616. doi:10.1007/s00455-017-9809-z
33. Zeng H, Zeng X, Xiong N, et al. How stroke-related dysphagia relates to quality of life: the mediating role of nutritional status and psychological disorders. Front Nutr. 2024;11:1339694. doi:10.3389/fnut.2024.1339694
34. Eapen BC, Tran J, Ballard-Hernandez J, et al. Stroke rehabilitation: synopsis of the 2024 U.S. department of veterans affairs and U.S. department of defense clinical practice guidelines. Ann Intern Med. 2025;178(2):249–268. doi:10.7326/ANNALS-24-02205
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.