Back to Journals » Journal of Pain Research » Volume 19
Progressive Early Mobilization and Its Impact on Pain and Function After Lumbar Vertebral Compression Fracture: A Retrospective Study Based on the Oswestry Disability Index
Authors Liu X, Huang Y, Zhang Y
Received 26 December 2025
Accepted for publication 10 March 2026
Published 25 March 2026 Volume 2026:19 579740
DOI https://doi.org/10.2147/JPR.S579740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Xingxing Liu, Yuejiao Huang, Yuye Zhang
Department of Orthopedics, The Second Affiliated Hospital of Soochow University, Suzhou, 215004, People’s Republic of China
Correspondence: Yuye Zhang, Department of Orthopedics, The Second Affiliated Hospital of Soochow University, No. 28 Rehabilitation Lane, High Tech Zone, Suzhou City, Jiangsu, 215004, People’s Republic of China, Email [email protected]
Background: The optimal timing and content of postoperative rehabilitation for elderly patients with osteoporotic vertebral compression fractures (OVCF) remain controversial. This study evaluated whether the addition of a progressive early mobilization protocol to routine care could enhance pain relief, functional recovery, and safety.
Methods: This single-center retrospective study included 120 OVCF patients (≥ 60 years) treated surgically from February 2023 to February 2025. Patients were allocated by admission order to routine rehabilitation (control, n=60) or routine care plus progressive early mobilization (observation, n=60). All patients received interventions from the same team over 12 weeks. The progressive protocol included preoperative prone training; turning from 6 hours postoperatively; lower-limb exercises from postoperative days 1– 3; lumbar training from weeks 2– 3; standing and gait training from week 5; and abdominal bracing at week 12. Clinical data were analyzed using t-tests and χ2-tests with SPSS 26.0.
Results: The observation group demonstrated significantly shorter length of hospital stay (15.60 ± 2.21 vs. 18.10 ± 2.75 days, P < 0.001), time to first ambulation (14.59 ± 3.66 vs. 17.38 ± 4.20 d, P < 0.001), time to callus formation (23.88 ± 3.25 vs. 27.25 ± 4.10 d, P < 0.001), and time to fracture union (54.85 ± 7.29 vs. 59.68 ± 8.75 d, P < 0.001) compared to controls. The overall treatment efficacy was significantly higher in the observation group (96.67% vs. 91.67%, P = 0.041). Both groups showed significant improvements in VAS and ODI scores from baseline (P < 0.05), with significantly lower scores in the observation group at both 8 and 12 weeks postoperatively (P < 0.05). The complication rate was significantly lower in the observation group (3.33% vs. 13.33%, P = 0.047).
Conclusion: The addition of a structured progressive early mobilization program to routine postoperative care may improve pain relief, functional recovery, and safety in elderly patients undergoing surgery for OVCF. These findings suggest that early staged mobilization could be beneficial in this population.
Keywords: progressive early mobilization, pain, function, lumbar vertebral compression fracture, retrospective study
Osteoporotic vertebral compression fracture (OVCF) is a leading cause of pain, disability, and loss of independence in older adults, with its incidence rising as the global population ages.1–3 Lumbar involvement is particularly common and often results in prolonged bed rest, leading to deconditioning, sarcopenia, and complications such as pressure ulcers, infections, and delayed union, all of which exacerbate functional decline and increase healthcare utilization.4–7 While percutaneous vertebral augmentation and instrumented fixation can effectively stabilize fractures and provide acute pain relief in selected patients,8–10 postoperative rehabilitation remains essential for consolidating analgesic benefits, restoring function, and minimizing complications. However, the optimal timing and content of rehabilitation for OVCF remain controversial, particularly in frail patients with multiple comorbidities who face a high risk of iatrogenic harm from prolonged immobility.11–13
Early mobilization is a cornerstone of enhanced recovery protocols in musculoskeletal and spine care, associated with shorter hospital stays, earlier ambulation, improved patient-reported outcomes, and fewer adverse events.14,15 A progressive, structured rehabilitation program typically includes preoperative education and positioning, early postoperative turning, staged lower-limb activation, trunk stabilization, lumbar extensor strengthening, and graded standing-to-gait practice. Such an approach facilitates safe axial loading, enhances neuromuscular control, promotes callus formation, and may help prevent OVCF-specific deficits and secondary injuries.16–18 However, high-quality evidence specifically targeting elderly OVCF populations remains limited, and rehabilitation protocols continue to vary widely across institutions.
In this study, researchers conducted a single-center, retrospective cohort study of elderly patients with osteoporotic vertebral compression fractures undergoing surgery. Patients received either routine postoperative care or routine care plus a 12-week, progressive early mobilization program delivered by an experienced multidisciplinary team. Despite increasing recognition of early mobilization in spine surgery,19 high-quality, procedure-specific evidence for staged rehabilitation protocols in elderly OVCF patients remains scarce. In particular, it is unclear whether a progressive, criteria-based program can safely enhance fracture healing, reduce complications, and improve functional recovery beyond standard care in this vulnerable population. We hypothesized that the progressive program would improve pain control and functional recovery. We also expected fewer complications and fewer cases of delayed union. In addition, we anticipated better care efficiency, including shorter time to first ambulation, earlier callus formation and fracture union, and reduced length of stay.
Methods
Participants and Eligibility
This study is a retrospective, non-randomized cohort study. The study protocol was approved by the ethics committee of The Second Affiliated Hospital of Soochow University (Approval number: JD-HG-2025-149), and the requirement for informed consent was waived due to the retrospective nature of the study. From February 2023 to February 2025, we retrospectively reviewed medical records of 120 eligible OVCF patients who underwent surgical treatment in the Department of Orthopedics at our hospital. Patients were divided into two groups based on the perioperative rehabilitation regimen they actually received: a control group receiving standard rehabilitation (n = 60) and an intervention group receiving standard rehabilitation plus a progressive rehabilitation program (n = 60). Baseline data extracted from medical records included sex, age, body mass index (BMI), and fracture level. All patients underwent percutaneous vertebral augmentation procedures, including either percutaneous kyphoplasty (PKP) or percutaneous vertebroplasty (PVP), as determined by the attending surgeon based on fracture morphology and bone quality. All procedures were single-level surgeries involving one vertebral body. The surgical approach was minimally invasive in all cases, with no open fixations performed. Although bone mineral density (BMD) data were not uniformly available in all medical records due to the retrospective design, all patients had been diagnosed with osteoporotic fractures based on clinical presentation and imaging. Information on preoperative use of anti-osteoporosis medications (eg, bisphosphonates, denosumab, or teriparatide) and nutritional status (eg, serum albumin levels) was also extracted when available to assess potential confounding; however, these data were incomplete and therefore not included in the final adjusted analysis.
Inclusion criteria were: (1) age ≥ 60 years; (2) OVCF confirmed by preoperative imaging within one week prior to surgery, defined as either the presence of fresh bone marrow edema on T2-weighted MRI or evidence of cortical discontinuity or an acute fracture line on CT; (3) surgical treatment was indicated and completed uneventfully; (4) complete medical records and follow-up data were available.
Exclusion criteria were as follows: (1) severe major organ dysfunction, including cardiac function of New York Heart Association (NYHA) class III or IV, Child–Pugh class C liver disease, or estimated glomerular filtration rate (eGFR) < 30 mL/min/1.73 m2 or requiring dialysis; (2) coagulopathy; (3) immune dysfunction; (4) hematologic disease; (5) active infectious disease; (6) malignancy; (7) cognitive impairment or psychiatric disorders; (8) incomplete medical records or loss to follow-up.
Rehabilitation Interventions
To minimize operator-related variability, all patients received rehabilitation care from the same multidisciplinary team, which comprised attending physicians with at least five years of clinical experience and nurses with more than three years of experience. The intervention period lasted 12 weeks.
To ensure intervention fidelity and monitor patient adherence, each patient in the observation group was provided with a structured rehabilitation logbook. Patients or their caregivers were instructed to record the daily completion of each prescribed exercise (eg, sessions, duration, and any discomfort experienced). These logbooks were reviewed twice weekly by the attending physician or bedside nurse during hospitalization, and during each follow-up visit after discharge. In addition, nurses documented observed patient participation in turning and limb exercises on daily nursing records. Any deviation from the prescribed protocol was discussed with the patient and corrected promptly. This combined approach of self-report and staff observation ensured consistent delivery of the intervention across patients.
Rehabilitation protocols were extracted from medical records as follows:
Control group:
(1) Preoperative: condition monitoring, health education, psychological support;
(2) Postoperative: vital signs monitoring, basic nursing care, dietary guidance, and complication prevention;
(3) Positioning and turning: starting on postoperative day 1, patients were turned every 24 hours with head-of-bed elevation ≤30°, using log-rolling technique; the time to first ambulation was determined by the physician’s assessment and documented in the medical records.
Observation group: Routine rehabilitation plus a progressive rehabilitation program that had consisted of:
(1) Preoperative instruction: prone-position training for 0.5 h per session, 2–3 sessions daily.
(2) Postoperative turning: initiated at 6 hours postoperatively; thereafter patients were turned every 2 hours to prevent pressure injury, with careful lumbar protection to avoid secondary injury.
(3) Lower-limb training: ankle dorsiflexion/plantarflexion and rotation had been started on postoperative day (POD) 0–1; straight-leg raise was initiated on POD 1 (unilateral raise to approximately 20°, hold 30s, then lowered slowly; alternating both limbs; 20 min per session, 3 sessions/day); cycling-type flexion–extension was started on POD 3 (both limbs), 5 min per session, 3–5 sessions/day.
(4) Positioning/bracing of the trunk: abdominal bracing exercises had been initiated at postoperative week (POW) 12, 15 min per session, 3–5 sessions/day.
(5) Lumbar extensor and paraspinal training: exercises were begun at POW 2 with support on elbows, feet, and head; at POW 3, patients progressed to exercises supported on feet and head.
(6) Standing and gait training: considering the fragility of osteoporotic bone and the need to ensure adequate early fracture healing before axial loading, standing and gait training was intentionally initiated at POW 5. This delayed timing was designed to allow sufficient time for initial callus formation and to minimize the risk of vertebral re-collapse or implant failure in this elderly osteoporotic population. Training was initiated at POW 5; standing and walking were adjusted and practiced, 10 min per session, 8–10 sessions/day.
Postoperative Clinical Endpoints
Endpoints included: (1) length of stay, defined as days from admission for surgery to discharge; (2) time to first ambulation, defined as time from surgery to the first safe out-of-bed activity under staff supervision; (3) time to callus formation: defined as the time from the day of surgery to the first CT showing continuous trabecular bridging at the fracture ends.; and (4) time to fracture union: assessed using the Vertebral Fracture Healing Score System. Union is defined as a blurred fracture line on CT with continuous trabecular bridging across the fracture area, and no progressive loss of vertebral height (<2 mm) on two consecutive imaging assessments at least 4 weeks apart.
Efficacy Assessment
Pain was assessed using the Janne Scott visual pain ruler, a 10-cm scale where 0 cm represents no pain and 10 cm represents the worst imaginable pain. On this scale, the 2.5 cm mark indicates mild pain, 5 cm indicates moderate pain, and 7.5 cm indicates severe pain. All patients received standardized instructions on the use of the scale prior to treatment. Pain scores were recorded before and after the intervention. The percentage of pain relief was calculated using the formula: [(pre-treatment score − post-treatment score)/pre-treatment score] × 100%. Categories: cure, 100%; marked improvement, ≥50%; improvement, ≥20% and <50%; no effect, <20%.
Pain and Function Assessment
Pain and function were assessed at postoperative weeks 8 and 12. Pain intensity was measured using a visual analogue scale (VAS) ranging from 0 to 10, where 0 indicates no pain, 1–3 mild pain, 4–6 moderate to severe pain, and 7–10 severe pain. Lower scores reflect better pain control. Functional status was evaluated using the Oswestry Disability Index (ODI), which comprises ten domains (including personal care, walking, sitting, standing, and social life), each scored on a six-point scale. Higher scores indicate greater pain-related disability. The total ODI score was calculated using the following formula: (sum of item scores/(5 × number of items answered)) × 100%. Missing ODI data were handled using multiple imputation prior to statistical analysis.
Complications
All complications that occurred during the rehabilitation period and postoperative follow-up were retrospectively identified and recorded. These included surgical-site infection, pressure injury, iatrogenic radiculopathy, and delayed union. The overall incidence of complications was calculated to evaluate the safety profile and risk reduction associated with the different rehabilitation strategies.
Statistical Analysis
Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) and compared between the two groups using independent-samples t-tests after confirming normal distribution. Categorical variables were presented as frequencies and percentages and compared using the chi-square (χ2) test or Fisher’s exact test, as appropriate. A two-sided P value < 0.05 was considered statistically significant for all analyses.
Results
Baseline Characteristics
A total of 120 patients were enrolled, with 60 assigned to the control group and 60 to the observation group. Baseline characteristics, including sex, age, body mass index (BMI), disease duration, surgical technique, and fracture level distribution, were well balanced between the two groups, with no statistically significant differences observed (all P > 0.05) (Table 1).
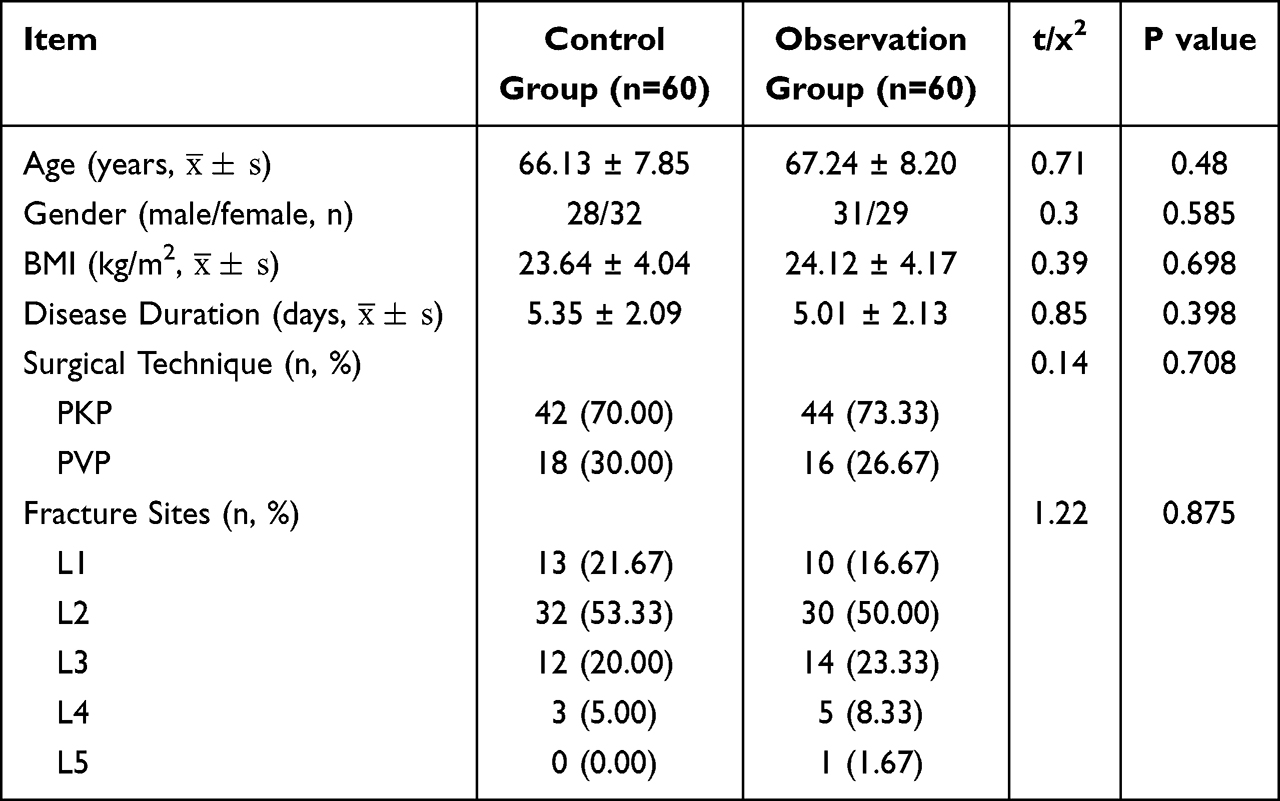 |
Table 1 Comparison of Baseline Characteristics Between the Two Groups |
Postoperative Clinical Outcomes
Compared with the control group, the observation group had significantly shorter hospital stay (15.6 ± 2.2 vs. 18.1 ± 2.8 days, t = 6.033, P < 0.001; Figure 1A), time to ambulation (14.6 ± 3.7 vs. 17.4 ± 4.2 days, t = 3.847, P < 0.001; Figure 1B), callus formation (23.9 ± 3.3 vs. 27.3 ± 4.1 days, t = 5.259, P < 0.001; Figure 1C), and fracture union (54.9 ± 7.3 vs. 59.7 ± 8.8 days, t = 4.237, P < 0.001; Figure 1D) The reductions in time to callus formation and time to union were particularly pronounced, indicating a positive effect of the progressive rehabilitation program on fracture healing.
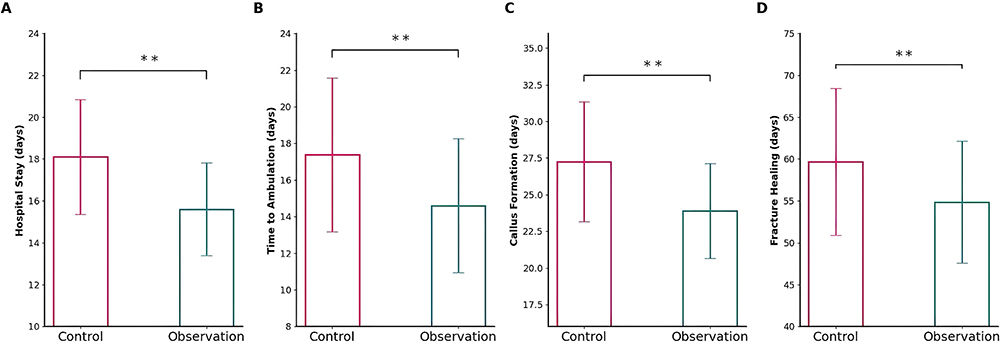 |
Figure 1 Comparison of postoperative clinical data between the two groups. (A) Hospital stay (days): comparison of length of hospitalization between control group and observation group; (B) Time to first ambulation (days): comparison of days from surgery to first safe out-of-bed activity between the two groups; (C) Time to callus formation (days): comparison of days from surgery to first CT evidence of continuous trabecular bridging at fracture ends; (D) Time to fracture union (days): comparison of days from surgery to radiographic union defined by blurred fracture line with continuous trabecular bridging and no progressive vertebral height loss. Data are presented as mean ± SD. **P < 0.001 vs. control group. |
Effect of Rehabilitation on Treatment Efficiency
As shown in Figure 2, the observation group demonstrated a significantly higher overall treatment efficacy compared to the control group (58/60, 96.67% vs. 55/60, 91.67%; χ2 = 4.160, P = 0.041). Specifically, the observation group had a higher proportion of patients achieving marked improvement (38/60, 63.33% vs. 29/60, 48.33%) and a lower proportion with no effect (2/60, 3.33% vs. 5/60, 8.33%) compared to controls. These findings indicate superior rehabilitation outcomes associated with the progressive mobilization protocol.
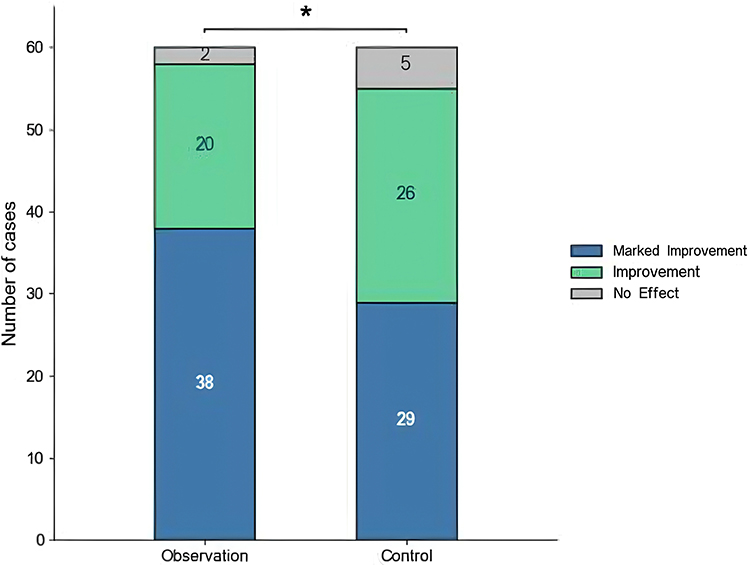 |
Figure 2 Comparison of effective rates after rehabilitation between the two groups. Bar chart showing the proportion of patients in each category (marked improvement, improvement, no effect) and the total effective rate in control group and observation group. The observation group demonstrated a significantly higher overall response rate compared with the control group (P = 0.041). *P < 0.05 vs. control group. |
Effects of Postoperative Rehabilitation on Pain and Function
Before treatment, no significant differences were observed between groups in VAS pain scores or ODI disability scores (P > 0.05). Postoperatively, both groups demonstrated significant improvements in pain and function relative to baseline (P < 0.05). At week 8, the observation group exhibited significantly lower VAS scores (2.27 ± 0.40 vs. 2.84 ± 0.36, P < 0.05) and ODI scores (22.98 ± 2.35 vs. 26.26 ± 2.25, P < 0.05) compared to controls. These differences remained significant at week 12, with the observation group showing superior VAS (0.84 ± 0.52 vs. 1.20 ± 0.47, P < 0.05) and ODI scores (19.16 ± 1.26 vs. 21.40 ± 2.01, P < 0.05). These results suggest that the progressive mobilization protocol confers enhanced pain relief and functional recovery (Figure 3).
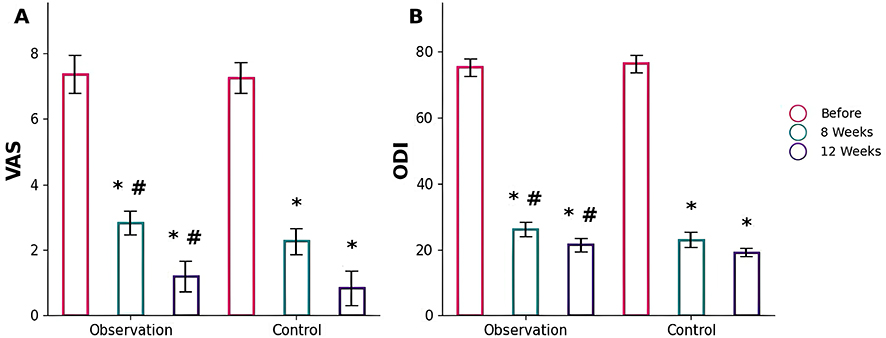 |
Figure 3 Comparison of before and after treatment VAS scores and ODI indices between the two groups. (A) VAS scores at baseline, 8 weeks, and 12 weeks postoperatively; (B) ODI scores at baseline, 8 weeks, and 12 weeks postoperatively. *P < 0.05 vs. before treatment within the same group; #P < 0.05 vs. control group at the same time point. |
Complications
The complication rate was 3.33% in the observation group (2/60: 1 surgical-site infection, 1 pressure injury) and 13.33% in the control group (8/60: 2 surgical-site infections, 3 pressure injuries, 1 iatrogenic radiculopathy, 2 delayed unions). The difference between groups was statistically significant by chi-square test (Figure 4).
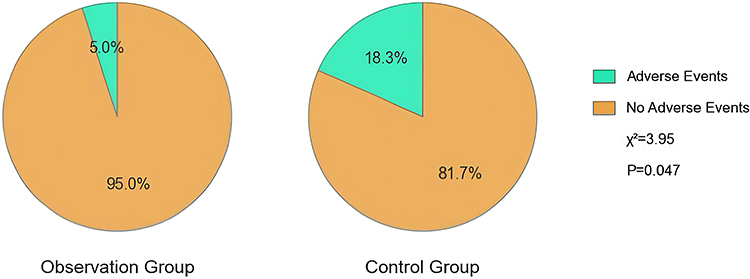 |
Figure 4 Impact of two rehabilitation methods on complications. Pie charts showing the proportion of patients with and without postoperative complications in the control group and observation group. The observation group had a significantly lower overall complication rate compared with the control group (χ2 = 3.95, P = 0.047). |
Discussion
In this parallel-group study including 60 patients per arm, baseline characteristics (sex, age, BMI, disease duration, and fracture location) were comparable between the two groups, minimizing confounding from imbalance in prognostic factors. Against this balanced background, the progressive, structured rehabilitation program yielded consistently superior perioperative and post-discharge outcomes compared with conventional rehabilitation. Specifically, the observation group demonstrated significantly shorter length of stay, earlier first ambulation, and accelerated callus formation and radiographic union; higher overall clinical effectiveness; greater reductions in pain and disability at 8 and 12 weeks; and a lower incidence of postoperative complications. Collectively, these findings support the hypothesis that a staged, criteria-based rehabilitation pathway confers meaningful clinical benefit after fracture surgery.
The most notable advantages were the shortened times to callus formation and fracture union. Mechanistically, early but controlled loading and range-of-motion exercises can optimize the local mechanical milieu, enhance regional perfusion, and stimulate osteogenesis through mechanotransductive pathways, thereby accelerating reparative bone biology. Concurrently, mitigating disuse-related bone loss and muscle atrophy preserves the biomechanical context necessary for effective callus maturation, aligning with prior evidence that early mobilization and functional weight-bearing can hasten bone healing without compromising fixation stability when appropriately indicated.20–22 The accelerated fracture healing observed in our observation group aligns with previous findings that enhanced bone healing may contribute to better clinical outcomes, as a recent meta-analysis reported that fracture non-union is associated with residual back pain after OVCF treatment.23
The reductions in length of stay and time to first ambulation further underscore the clinical utility of standardized early mobilization embedded within a multidisciplinary framework (eg, multimodal analgesia, respiratory training, progressive strengthening and balance exercises, gait retraining, and environmental safety education). Such pathways have been associated with fewer bedrest-related complications and more efficient recovery of basic activities, translating into both clinical and health-economic gains.24–26 These improvements are consistent with previous studies in related populations. Phruetthiphat et al27 reported that elderly patients with hip fractures and concurrent OVCF had significantly longer hospital stays compared to those with isolated hip fractures, highlighting the need for targeted rehabilitation to reduce hospitalization. Additionally, Emre et al28 demonstrated that vertebroplasty under local anesthesia enabled early ambulation with effective pain control in high-risk elderly patients, supporting the feasibility of early mobilization in this population. Furthermore, Yang et al23 identified fracture non-union as a key risk factor for residual back pain after OVCF treatment, suggesting that the accelerated fracture healing achieved in our observation group may contribute to better long-term pain outcomes.
The observed superiority in pain (VAS) and function (ODI) at 8 and 12 weeks likely reflects a synergy between optimized pain control, via multimodal strategies that facilitate participation and phased, goal-directed neuromuscular and proprioceptive retraining that improves motor control and reduces compensatory movement patterns.29,30 The VAS and ODI improvements in our observation group align with previous meta-analyses. Than et al31 reported that exercise after vertebral augmentation significantly reduced VAS and ODI compared to controls, with baseline scores similar to our cohort.
From a clinical implementation perspective, this rehabilitation protocol can be adapted for routine practice even in resource-limited settings. Core components such as preoperative education and bedside exercises do not require specialized equipment and can be delivered by nursing staff or through low-cost digital platforms.32 Evidence from non-Western healthcare settings supports the feasibility of structured rehabilitation.33 Regarding patient selection, older adults and those with comorbidities may derive particular benefit due to the gradual progression and safety focus. Pennicooke et al7 reported that patients over 70 years undergoing lumbar fusion had higher rates of discharge to inpatient rehabilitation, highlighting the need for tailored programs in this population. However, patients with cognitive impairment or severe cardiovascular instability may require modified protocols with closer supervision. Future research should develop stratified rehabilitation pathways based on frailty and comorbidity burden to optimize resource allocation and clinical benefit.24,33
Safety outcomes also favored the progressive rehabilitation approach. The overall complication rate was significantly lower in the observation group, with fewer infections and pressure injuries, and no excess in iatrogenic nerve root injury or delayed union. Early mobilization improves ventilation, hemodynamics, and pressure distribution while engaging patients in nutrition and self-care, which collectively reduces common postoperative complications. Moreover, protocolized, criteria-based progression may decrease the risk of overloading the repair while avoiding the harms of prolonged immobilization, thereby balancing stability and function.32
Clinically, these results support adopting a progressive, structured, and monitored rehabilitation pathway as a standard adjunct to surgical care for fracture patients. Such implementation may enhance rates of timely union, expedite recovery of function, reduce pain burden, shorten hospitalization, and improve overall perioperative safety, benefits that are likely to translate into improved patient-reported outcomes and system-level efficiency. From a policy perspective, integrating these pathways with discharge planning and community or tele-rehabilitation may further sustain gains and improve adherence.34
Several limitations should be acknowledged. First, the retrospective single-center design may introduce inherent biases, despite balanced baseline characteristics. Second, adherence data after discharge relied on patient self-reporting, which is subject to recall bias. Third, potential confounders affecting bone healing, including baseline bone mineral density, preoperative anti-osteoporosis medication use, and nutritional status, were not systematically collected or adjusted for, which may have introduced residual confounding. Fourth, surgical procedures were not uniform across all patients, although all were performed by the same experienced team. Fifth, the timing of standing and gait training was protocol-driven for safety in this elderly population but may limit generalizability. Finally, the 12-week follow-up period is insufficient to evaluate long-term outcomes such as re-fracture rates or quality of life. Prospective multicenter studies with longer follow-up and comprehensive confounder adjustment are warranted.
In summary, within a cohort balanced at baseline, progressive rehabilitation after fracture surgery produced earlier union, faster mobilization, superior pain and functional recovery at medium-term follow-up, and fewer complications compared with conventional care. These results reinforce the role of structured, criteria-based rehabilitation as a high-value component of perioperative fracture management and justify broader implementation alongside confirmatory multicenter trials.
Confidentiality of Patient Data
In accordance with the waiver of informed consent granted by the Ethics Committee of The Second Affiliated Hospital of Soochow University (Approval No. JD-HG-2025-149), all patient data were anonymized and strictly confidential. Personal identifiers were removed prior to data collection and analysis, and access to medical records was limited to authorized members of the research team. The study was conducted in compliance with applicable data protection regulations and the ethical principles of the Declaration of Helsinki.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Human Ethics and Consent to Participate
All experimental protocols were approved by the Ethics Committee of The Second Affiliated Hospital of Soochow University (Approval number: JD-HG-2025-149), and the requirement for informed consent was waived due to the retrospective nature of the study. All methods were carried out in accordance with Declaration of Helsinki.
Funding
The work was not funded by any funding.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Park JS, Park YS. Survival analysis and risk factors of new vertebral fracture after vertebroplasty for osteoporotic vertebral compression fracture. Spine J. 2021;21(8):1355–10. doi:10.1016/j.spinee.2021.04.022
2. Jeon I, Kim SW, Yu D. Paraspinal muscle fatty degeneration as a predictor of progressive vertebral collapse in osteoporotic vertebral compression fractures. Spine J. 2022;22(2):313–320. doi:10.1016/j.spinee.2021.07.020
3. Prost S, Pesenti S, Fuentes S, Tropiano P, Blondel B. Treatment of osteoporotic vertebral fractures. Orthop Traumatol Surg Res. 2021;107(1S):102779. doi:10.1016/j.otsr.2020.102779
4. Gentile L, Benazzo F, De Rosa F, et al. A systematic review: characteristics, complications and treatment of spondylodiscitis. Eur Rev Med Pharmacol Sci. 2019;23(2 Suppl):117–128. doi:10.26355/eurrev_201904_17481
5. Zhu L, Cai T, Shan Y, Zhang W, Zhang L, Feng X. Comparison of clinical outcomes and complications between percutaneous endoscopic and minimally invasive transforaminal lumbar interbody fusion for degenerative lumbar disease: a systematic review and meta-analysis. Pain Physician. 2021;24(6):441–452.
6. Abel F, Tan ET, Chazen JL, Lebl DR, Sneag DB. MRI after lumbar spine decompression and fusion surgery: technical considerations, expected findings, and complications. Radiology. 2023;308(1):e222732. doi:10.1148/radiol.222732
7. Pennicooke B, Santacatterina M, Lee J, Elowitz E, Kallus N. The effect of patient age on discharge destination and complications after lumbar spinal fusion. J Clin Neurosci. 2021;91:319–326. doi:10.1016/j.jocn.2021.07.006
8. Espahbodinea S, Ku JC, Costa Alves Junior A, et al. Percutaneous vertebral augmentation-pearls and pitfalls. J Spine Surg. 2023;9(1):13–16. doi:10.21037/jss-22-106
9. Lin YH, Lin J, Xu JY, et al. What Risk factors are associated with recurrent osteoporotic vertebral compression fractures after percutaneous vertebral augmentation? A meta-analysis. Clin Orthop Relat Res. 2025;483(8):1528–1539. doi:10.1097/CORR.0000000000003430
10. Dong C, Zhu Y, Zhou J, Dong L. Therapeutic efficacy of third-generation percutaneous vertebral augmentation system (PVAS) in osteoporotic vertebral compression fractures (OVCFS): a systematic review and Meta-analysis. Biomed Res Int. 2022;2022:9637831. doi:10.1155/2022/9637831
11. Xu Y, Li D, Zhang Q, Tong L. Efficacy of lumbar and abdominal muscle rehabilitation training on degree of osteoporosis, pain and anxiety in elderly patients with osteoporotic vertebral compression fracture after PKP and compliance analysis. Front Med Lausanne. 2024;11:1364497. doi:10.3389/fmed.2024.1364497
12. Luo Y, Jiang T, Guo H, Lv F, Hu Y, Zhang L. Osteoporotic vertebral compression fracture accompanied with thoracolumbar fascial injury: risk factors and the association with residual pain after percutaneous vertebroplasty. BMC Musculoskelet Disord. 2022;23(1):343. doi:10.1186/s12891-022-05308-7
13. Teixeira Taborda A, C DMB, Sánchez Tarifa P. Rehabilitation and orthopedic management of osteoporotic vertebral compression fractures. Manejo rehabilitador y ortopédico de las fracturas por compresión vertebral osteoporótica. Rev Esp Cir Ortop Traumatol. 2024;68(6):624–628. doi:10.1016/j.recot.2024.10.003
14. Huang J, Li P, Wang H, Lv C, Han J, Lu X. Exploring elderly patients’ experiences and concerns about early mobilization implemented in postoperative care following lumbar spinal surgery: a qualitative study. BMC Nurs. 2023;22(1):355. doi:10.1186/s12912-023-01510-7
15. Alexander M, Lou Garey M, Yates E, Vogt M. Postoperative mobilization protocol in lumbar laminectomy patients. Orthop Nurs. 2023;42(3):151–155. doi:10.1097/NOR.0000000000000941
16. Greenwood J, McGregor A, Jones F, Hurley M. Evaluating rehabilitation following lumbar fusion surgery (REFS): study protocol for a randomised controlled trial. Trials. 2015;16:251. doi:10.1186/s13063-015-0751-9
17. Jain K, Rishi P, Aggarwal A. Evidence based physiotherapy intervention on lumbar instability: a systematic review. Musculoskel Care. 2025;23(2):e70132. doi:10.1002/msc.70132
18. Bogaert L, Thys T, Depreitere B, et al. Rehabilitation to improve outcomes of lumbar fusion surgery: a systematic review with meta-analysis. Eur Spine J. 2022;31(6):1525–1545. doi:10.1007/s00586-022-07158-2
19. van de Wijgert IH, de Groot JC, Rood A, et al. Scoping review of early pain-related outcome domains and measurement instruments after degenerative lumbar spine surgery. Reg Anesth Pain Med. 2023;48(3):134–140. doi:10.1136/rapm-2022-103929
20. Jankaew A, Chen JC, Chamnongkich S, Lin CF. Therapeutic exercises and modalities in athletes with acute hamstring injuries: a systematic review and meta-analysis. Sports Health. 2023;15(4):497–511. doi:10.1177/19417381221118085
21. Lewis SR, Pritchard MW, Parker R, et al. Rehabilitation for ankle fractures in adults. Cochrane Database Syst Rev. 2024;9(9):CD005595. doi:10.1002/14651858.CD005595.pub4
22. Labanca L, Rocchi JE, Giannini S, et al. Early superimposed NMES training is effective to improve strength and function following ACL reconstruction with hamstring graft regardless of tendon regeneration. J Sports Sci Med. 2022;21(1):91–103. doi:10.52082/jssm.2022.91
23. Yang XG, Dong YQ, Liu X, et al. Incidence and prognostic factors of residual back pain in patients treated for osteoporotic vertebral compression fractures: a systematic review and meta-analysis. Eur Spine J. 2024;33(12):4521–4537. doi:10.1007/s00586-024-08426-z
24. Manni T, Ferri N, Vanti C, et al. Rehabilitation after lumbar spine surgery in adults: a systematic review with meta-analysis. Arch Physiother. 2023;13(1):21. doi:10.1186/s40945-023-00175-4
25. van Middelkoop M, Rubinstein SM, Kuijpers T, et al. A systematic review on the effectiveness of physical and rehabilitation interventions for chronic non-specific low back pain. Eur Spine J. 2011;20(1):19–39. doi:10.1007/s00586-010-1518-3
26. Greenwood J, Hurley M, McGregor A, McCourt O, Jones F. A qualitative evaluation of participants experiences of living with back pain, lumbar fusion surgery, and post-operative rehabilitation. Pilot Feasibility Stud. 2022;8(1):91. doi:10.1186/s40814-022-01050-y
27. Phruetthiphat OA, Kanokwongnuwat W, Satravaha Y, Pinijprapa P, Chaichankul C, Gajaseni P. Functional outcomes following Hip fracture with concurrent vertebral fracture within a fracture liaison service. Sci Rep. 2025;15(1):25417. doi:10.1038/s41598-025-11387-y
28. Emre TY, Gökcen HB, Atbaşı Z, Kavadar G, Enercan M, Ozturk C. ASA III osteoporotic fracture in 62 patients treated with vertebroplasty under local anesthesia. Eur J Orthop Surg Traumatol. 2016;26(1):47–52. doi:10.1007/s00590-015-1700-8
29. Rushton A, Wright C, Goodwin P, Calvert M, Freemantle N. Physiotherapy rehabilitation post first lumbar discectomy: a systematic review and meta-analysis of randomized controlled trials. Spine. 2011;36(14):E961–E972. doi:10.1097/BRS.0b013e3181f0e8f8
30. Shen SC, Chen HC, Tsou HK, et al. Percutaneous endoscopic lumbar discectomy for L5-S1 disc herniation based on image analysis and clinical findings: a retrospective review of 345 cases. Medicine. 2023;102(5):e32832. doi:10.1097/MD.0000000000032832
31. Than CA, Adra M, Curtis TJ, et al. The effect of exercise post vertebral augmentation in osteoporotic patients: a systematic review and meta-analysis. J Orthop Res. 2023;41(12):2703–2712. doi:10.1002/jor.25631
32. Guo YJ, Hu XY, Li JY, Yang L. Effects of a WeChat-based individualized post-discharge rehabilitation program on patients with lumbar fusion surgery. J Back Musculoskelet Rehabil. 2022;35(3):545–557. doi:10.3233/BMR-200280
33. Jain S, Khanna K, Shetty GM, et al. Changes in standing and walking time after multimodal physical rehabilitation in low grade degenerative lumbar spondylolisthesis: a non-randomised pilot study. Physiother Theory Pract. 2023;39(4):727–737. doi:10.1080/09593985.2022.2025965
34. Badr M, Elkhawaga H, Fawaz K, Kasem M, Fayez E. Effects of multimodal physical therapy on pain, disability, H-reflex, and diffusion tensor imaging parameters in patients with lumbosacral radiculopathy due to lumbar disc herniation: a preliminary trial. Cureus. 2024;16(6):e63501. doi:10.7759/cureus.63501
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.