Back to Journals » OncoTargets and Therapy » Volume 13
Programmed Cell Death Protein-1 (PD-1)-Targeted Immunotherapy for Advanced Hepatocellular Carcinoma in Real World
Received 16 October 2019
Accepted for publication 16 December 2019
Published 8 January 2020 Volume 2020:13 Pages 143—149
DOI https://doi.org/10.2147/OTT.S234868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Hanzhi Cui, 1,* Guanghai Dai, 2,* Jingzhi Guan 1
1Department of Oncology, The Eighth Medical Center, Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Department of Oncology, The General Hospital of People’s Liberation Army, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanghai Dai
Department of Oncology, The General Hospital of People’s Liberation Army, No. 28 Fuxing Road, Haidian District, Beijing 100853, People’s Republic of China
Tel +86 66937291
Email [email protected]
Background: Hepatocellular carcinoma (HCC) is one of the most common malignant solid tumors. Its incidence is increasing worldwide due to the dissemination of hepatitis B infection, HCV infection and nonalcoholic steatohepatitis-related HCC. For patients with advanced HCC, the available treatments are extremely limited and the prognosis is very poor. Therefore, it is urgent to discover new innovative approaches. Programmed cell death protein-1-targeted immunotherapy has shown promising results in multicenter clinical trials.
Aim: To evaluate the effectiveness and safety of anti-PD-1 agent in patients with advanced primary hepatocellular carcinoma.
Methods: A retrospective analysis of 55 patients with advanced primary hepatocellular carcinoma who had been administered anti-PD-1 agent. Tumor response was assessed according to the modified Response Evaluation Criteria in Solid Tumors and any adverse events were recorded.
Results: The median overall survival (OS) was 15 months. The median progression-free survival (PFS) was 10 months. No patient had complete response (CR) and 12 (22%) participants achieved partial response (PR), resulting in an overall response rate (ORR) of 22%. Thirty-seven (67%) patients showed stable disease (SD) and 6 (11%) subjects had progressive disease (PD) at first radiological evaluation. The disease control rate (DCR) was 89%. The total side effect rate was 61.8% and most were relieved after treatment.
Conclusion: Programmed cell death protein‐1‐targeted immunotherapy is a safe and effective treatment for advanced primary hepatocellular carcinoma.
Keywords: hepatocellular carcinoma, programmed cell death protein-1-targeted immunotherapy, immune checkpoint inhibitor, adverse events
Introduction
Hepatocellular carcinoma (HCC) is one of the most common malignant solid tumors, which is also mainly counted for the death of patients with liver cirrhosis. It is the fifth most common cancer1 and is the third leading cause of cancer-related death worldwide. On a global scale, liver cancer accounts for more than 850,000 new cancer cases annually, and approximately 90% of these are HCC.2 Its incidence is increasing worldwide due to the dissemination of hepatitis B infection in Africa and Middle East3 and increased incidence of HCV infection and nonalcoholic steatohepatitis-related HCC in Europe, and North America.4 About 80% of victims are distributed in Asian countries. Among them, over 50% of the patients are distributed in China. Most of them are diagnosed at advanced stages with poor prognosis and only to receive palliative treatments or best supportive care. The curative treatments can be applied to only 30% of patients. Despite those curative efforts, the survival benefits are still limited, and the majority of patients ultimately experience a recurrence or disease progression. Therefore, there is an urgent need to develop an effective treatment for the patients with HCC. For the last decade, a multi-tyrosine kinase inhibitor, sorafenib, was the only effective drug available for HCC.5 After the development of sorafenib,6,7 4 agents have demonstrated improved outcome data: lenvatinib8 in the first-line and regorafenib,9 cabozantinib,10 and ramucirumab11 after first-line disease progression. However, their efficacy is limited and lack predictive factors of response.
Immunotherapy has shown promising survival outcome in patients with HCC. Immune checkpoint inhibitor (ICI) demonstrated encouraging efficacy in certain cancer types, particularly in melanoma and lung cancer.12 Programmed cell death protein-1 (PD-1), programmed death-ligand 1 (PD-L1), and cytotoxic T lymphocyte-associated protein-4 (CTLA-4) are the main targets of ICIs.13 Following by the approval of ipilimumab for malignant melanoma in 2011, a number of ICIs, including three anti-PD-1 antibodies (nivolumab, pembrolizumab, and cemiplimab) and three anti-PD-L1 antibodies (atezolizumab, durvalumab, and avelumab), have been approved by the Food and Drug Administration (FDA) for different types of cancers.14 In the present clinical trials, Nivolumab and pembrolizumab have shown promising efficacy and safety results in non-comparative, open-label Phase II studies of advanced HCC.15,16 Based on these studies, the United States Food and Drug Administration (FDA) already granted accelerated conditional approval to both agents for sorafenib-experienced patients with HCC. Both nivolumab and pembrolizumab are currently being investigated in ongoing Phase III trials.
In this study, to evaluate the effectiveness and safety of anti-PD-1 targeted therapy in advanced HCC, we retrospectively analyzed the data of advanced HCC patients treated with nivolumab or pembrolizumab in our hospital.
Materials and Methods
Study Design and Participants
This was a retrospective study of advanced HCC patients treated with anti-PD-1 agent in Chinese People’s Liberation Army General Hospital (Beijing, China). Patients with histologically or radiologically confirmed advanced HCC who received PD-1-targeted immunotherapy with nivolumab or pembrolizumab were eligible. We confirmed the written informed consent from patients and patient data confidentiality. The retrospective analysis was approved by Chinese PLA General Hospital Ethics Committees. The recommendations of the Declaration of Helsinki for biomedical research involving human subjects were also followed. Fifty-six patients were recruited in this study.
Dosing of Nivolumab and Pembrolizumab
Nivolumab was administered at 1–3 mg/kg body weight or at a fixed dose of 240 mg every 2 weeks intravenously. Pembrolizumab was given at 2 mg/kg body weight or at a fixed dose of 200 mg every 3 weeks intravenously. AK105, a kind of home-made anti-PD-1 agents in clinical trials, was given at a fixed dose of 200 mg every 3 weeks intravenously. Dose delays were made based on toxicity.
Assessments
Patients had to have measurable disease. Tumor response was assessed according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST).17 Hyperprogression was defined as a progressive disease (RECIST version 1.118) on the first radiological evaluation during immunotherapy with a delta tumor growth rate of >50%, corresponding to an absolute increase in tumor growth rate exceeding 50% per month.19
Statistical Analysis
The primary endpoint was included overall survival (OS), progression-free survival (PFS), the secondary endpoints was included disease control rate (DCR), defined as the percentage of patients achieving a best overall response of either a complete response (CR), partial response (PR), or stable disease (SD) (maintained for at least 8 weeks), objective response rate (ORR), duration of response and toxicity of anti-PD-1 agents.
The Kaplan–Meier method was used to estimate the rates of PFS and OS. PFS was measured from the start date of treatment to the date of documented disease progression or death from any cause, whichever occurred first. The DCR and ORR were estimated by the percentage of patients achieving these criteria. These statistical analyses were performed using SPSS statistical software (version 13.0). A P value <0.05 was considered to be statistically significant.
Results
General Data
This study included 46 male and 9 female patients with a median age of 56 years old (range from 40 to 83 years old). All patients were diagnosed with HCC by pathology or radiology. The clinical-pathological features of the patients, including age, gender, ECOG performance status, liver cirrhosis, extrahepatic metastasis, vascular invasion, Child-Pugh grade, serum Alpha-fetoprotein (AFP) level, hepatitis B surface antigen (HBsAg) status, the name of anti-PD-1 agents and previous treatment are summarized in Table 1.
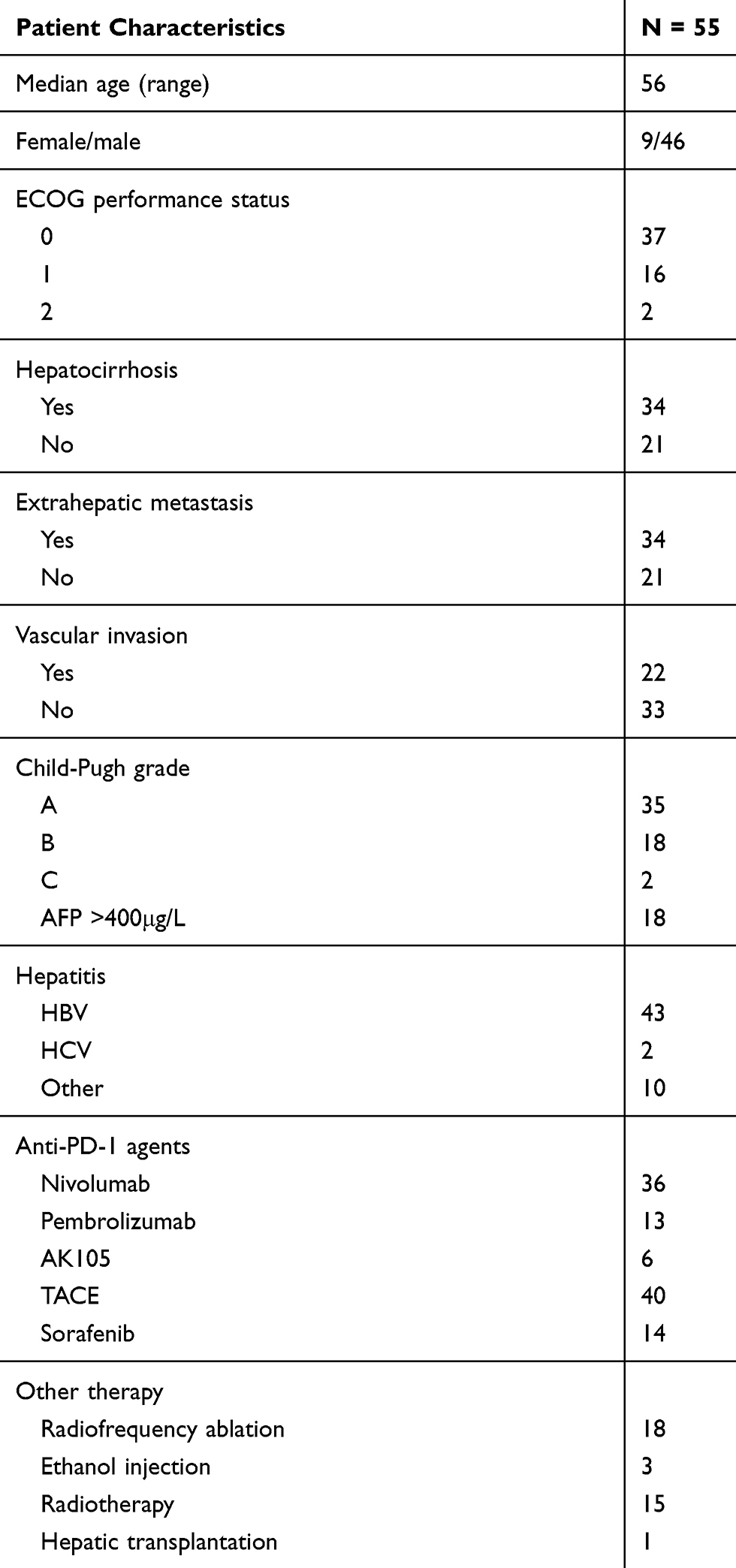 |
Table 1 Clinicopathologic Features in 55 Patients with HCC |
Twenty patients (36.3%) had Child‐Pugh stage B/C. At data cut-off, 2 (6%) and 9 (29%) patients were still on treatment with anti-PD-1 agents. Immunotherapy was discontinued mainly due to radiological or clinical disease progression and adverse events.
Clinical Survival
Thirty‐six subjects were treated with nivolumab,13 patients with pembrolizumab and 6 with AK105, a kind of home-made anti-PD-1 agent. As of 1st April 2016, the median follow-up period was 13 months (3–34 months) and the one-year survival rate was 29.9%. The date of data cut‐off was August 31, 2019. There were 30 (55%) surviving cases and still under follow-up, with a median overall survival (OS) of 15 months (95% CI: 8.4–21.6, Figure 1A). The median progression-free survival (PFS) was 10 months (95% CI: 6.0–14.0, Figure 1B). Median OS for patients with partial response or stable disease was 19 months (95% CI: 8.6–29.4) and was significantly longer compared to that of patients with progressive disease, which was 2 (95% CI,0.4–3.6; P = 0.000) months (Figure 2A). Median PFS for patients with partial response or stable disease was 11 months (95% CI,7.2–14.8) and was significantly longer compared to that of patients with progressive disease, which was 1 (95% CI,6.0–14.0; P = 0.000) month (Figure 2B). Patients with Child-Pugh A or B had significantly better survival than those with Child-Pugh C. Median OS for patients with Child-Pugh A, Child-Pugh B, and Child-Pugh C were 19 months, 10 months and 3 months, respectively (P = 0.01) (Figure 3A). Median PFS for patients with Child-Pugh A, Child-Pugh B, Child-Pugh C were 11 months, 7 months and 2 months, respectively (P = 0.026) (Figure 3B). ECOG performance status and Child-Pugh grade were influence factors of OS and PFS by univariate analysis (Table 3).
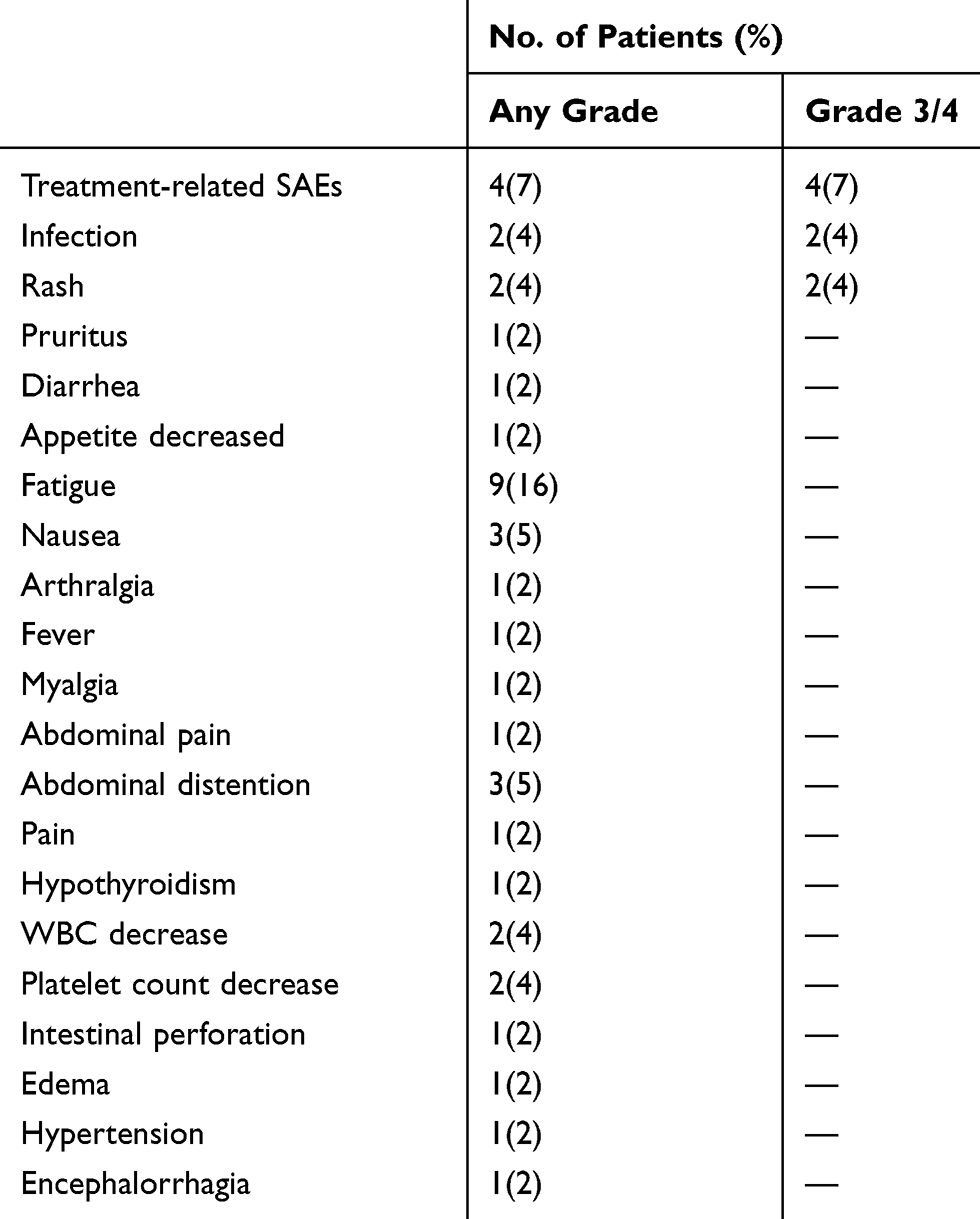 |
Table 2 Toxicity in 55 Patients with HCC |
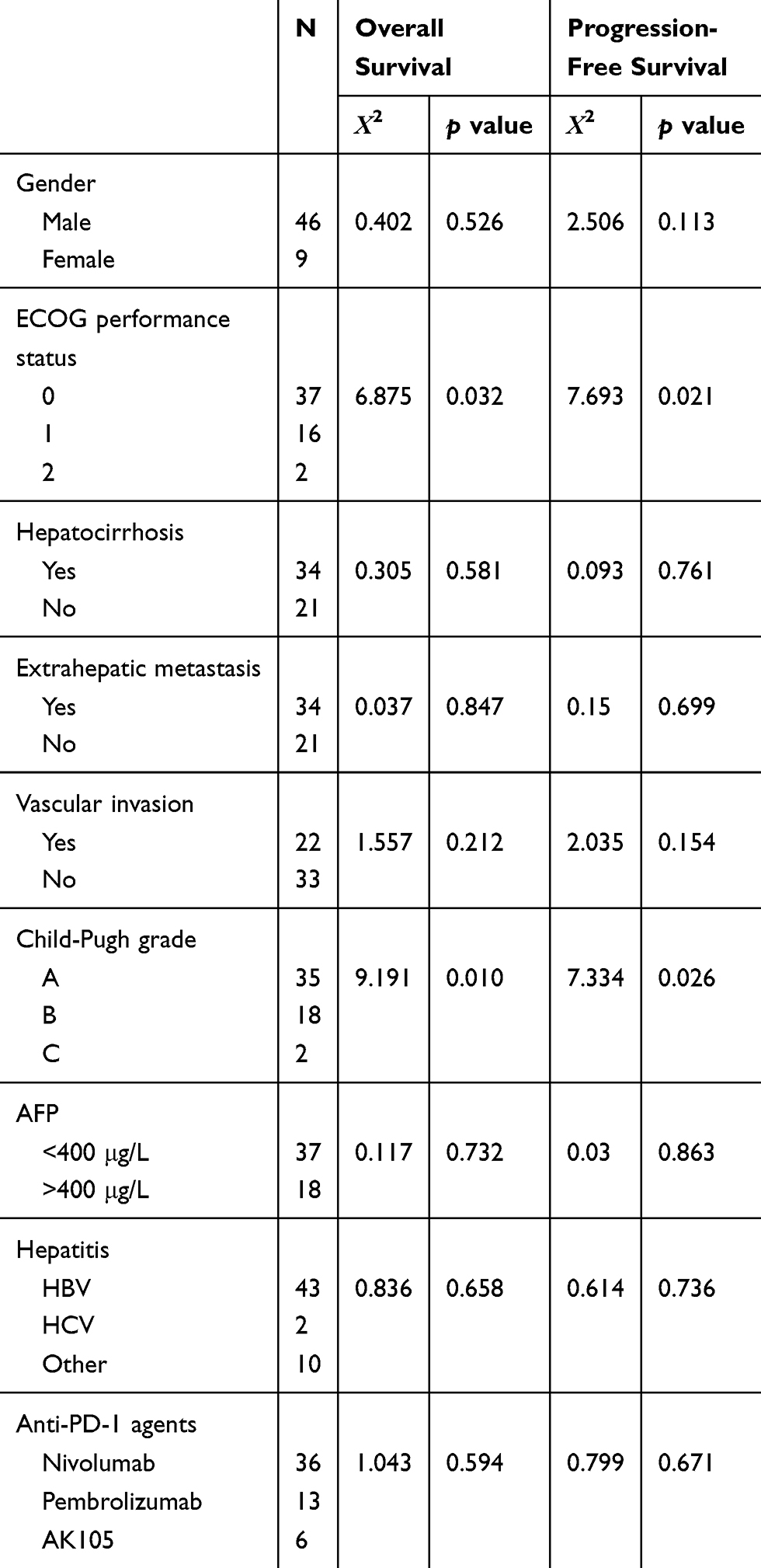 |
Table 3 Univariate Analysis for Overall Survival and Progression-Free Survival |
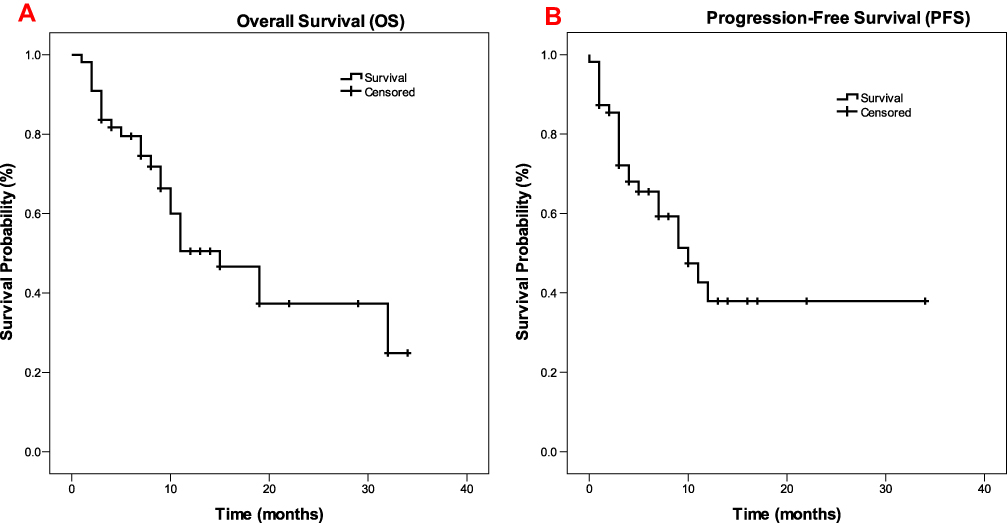 |
Figure 1 Kaplan–Meier curve showing OS and PFS for the whole cohort of patients treated with programmed cell death protein‐1 (PD‐1)‐targeted immunotherapy. (A) OS rates in patients with HCC receiving anti-PD-1 agents. (B) PFS rates in patients with HCC receiving anti-PD-1 agents. |
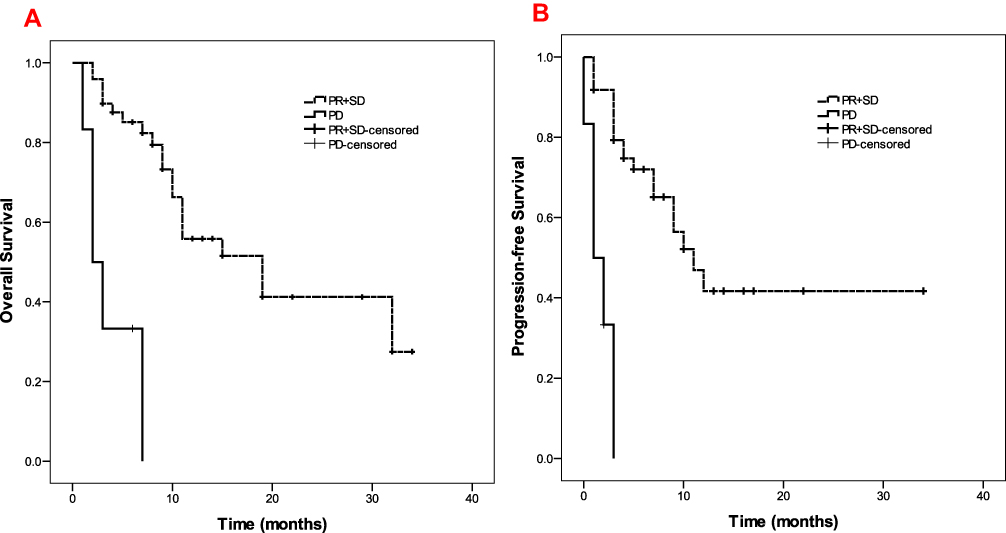 |
Figure 2 Kaplan–Meier curves showing OS and PFS for patients treated with PD-1-targeted immunotherapy according to radiological tumor response (partial response (PR)/stable disease (SD) vs progressive disease (PD)). (A) OS rates in patients with or without disease progression. (B) PFS rates in patients with or without disease progression. |
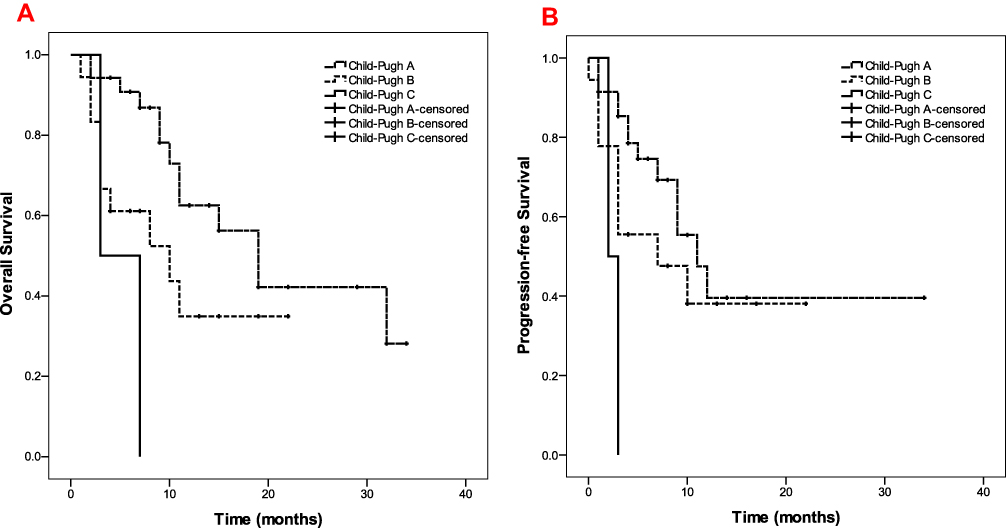 |
Figure 3 Kaplan–Meier curves showing OS and PFS for patients with different Child-Pugh Grade. (A) OS rates in patients with Child-Pugh A, B, C, respectively. (B) PFS rates in patients with Child-Pugh A, B, C, respectively. |
Efficacy
No patient had complete response (CR) and 12 (22%) participants achieved partial response (PR), resulting in an overall response rate (ORR) of 22%. Thirty-seven (67%) patients showed stable disease (SD) and 6 (11%) subjects had progressive disease (PD) at first radiological evaluation. The disease control rate (DCR) was 89%. Among all the patients, only one patient (2%) administered pembrolizumab was evaluable for hyperprogression. Among the six patients evaluated PD, two of them were given following treatment, one was administered lenvatinib, one was given TACE, the other four patients died of disease progression, including one hyperprogression case.
Toxicity
Toxicity data are shown in Table 2. The major treatment-related AEs (AEs using CTCAE-4 criteria) observed included fatigue, nausea, abdominal distention, with a total side effect rate of 61.8% (in 34 of 55 patients). The treatment-related AEs in most patients were relieved after symptomatic treatment. Treatment-related serious AEs occurred in 4 patients (7%) including immunoassociated pneumonia in two patients, encephalorrhagia in one patient and disease hyperprogression in one patient.
Among of them, one died of rupture and hemorrhage of liver cancer. In addition, a patient died of bleeding during hepatectomy operation.
Discussion
In this retrospective research, we demonstrate that PD-1-targeted immunotherapy showed promising efficacy and mild toxicity in a real-world cohort of patients with advanced stage HCC. There was no CR case in this research. Overall survival of patients with PR or SD was significantly longer than that of subjects with PD (19 vs 2 months). For most patients, the side effects were manageable. Only four cases suffered serious AEs.
To the best of our knowledge, one of the earliest immunotherapy trials that established promising activity was a Phase 2 study of the anti-CTLA-4 monoclonal antibody tremelimumab in patients with advanced HCC and HCV-related cirrhosis who developed disease progression while receiving sorafenib.4 Two phase II clinical trials proved the efficacy of nivolumab and pembrolizumab in patients with intermediate‐advanced stage HCC. One is the CheckMate 040 study, an open-label, noncomparative, phase I/II trial, tested nivolumab in 262 patients with HCC and Child‐Pugh class A.15 Overall response rate was 23% in sorafenib-naive and 19% in sorafenib-pretreated patients. A median overall survival was 28.6 months in sorafenib-naive and around 15 months in sorafenib-experienced patients. Based on these promising results, nivolumab, a fully human immunoglobulin G4 monoclonal antibody to PD-1, was conditionally approved as second-line treatment of patients with advanced and metastatic HCC. Another is the KEYNOTE-224 trial,16 a nonrandomised, open-label phase II study investigating pembrolizumab in sorafenib-pretreated patients (n = 104) with Child‐Pugh stage A. Again, it showed encouraging results with an overall response rate of 17%, a median PFS of 4.9 months, and a median OS of 12.9 months, which making pembrolizumab receive FDA approval in the United States. In our study, most patients received combination therapy, such as anti-PD-1 agents with TACE, target therapy, radiofrequency ablation and radiotherapy. Therefore, the median OS and PFS were 15 months and 10 months, respectively, significantly better than the two trials above. As we know, TACE and some anti-angiogenic agents, such as sorafenib and regorafenib could intensify tumor hypoxia, which promotes an immunosuppressive tumor microenvironment,20,21 increasing tumoral PD-L1 expression in experimental models in HCC.22,23 Therefore, immunotherapy maybe has a synergistic effect when combined with anti-angiogenic agents or TACE. A Phase 1/2 trial currently is recruiting patients for a comparative study of durvalumab plus tremelimumab in combination with TACE, radiofrequency ablation, or cryoablation (ClinicalTrials.gov identifier NCT02821754). Similarly, a phase ⅠB trial of lenvatinib with pembrolizumab currently is underway (ClinicalTrials.gov identifier NCT03006926).4
The CheckMate-040 and the KEYNOTE‐224 study only included Child‐Pugh A patients. However, in our study, nearly 40% of patients were Child‐Pugh B or C. There was no significant increase in the number of patients with any grade and high-grade adverse events, suggesting that immunotherapy is safe enough even in patients with advanced liver function impairment. As we know, monoclonal antibodies are not metabolized by the liver, which could make immune checkpoint inhibitors adaptable to patients with advanced liver cirrhosis.24 Moreover, it was shown that Child-Pugh grade was an influential factor of OS and PFS by univariate analysis in our study. The OS and PFS in patients with Child-Pugh A or B were better than those with Child-Pugh C significantly.
In conclusion, the advent of immunotherapy using ICIs has a great impact on many malignant tumors, including HCC. Anti-PD-1 agents are safe, effective and provide another treatment option for advanced HCC patients. However, there is no clear biomarker to predict the efficacy and sensitivity. It is generally known that HCC can be diagnosed by radiology, which means difficult to get pathological specimen. Therefore, it is necessary to find blood examination indicators and biomarkers to select patients who are most likely to benefit from immunotherapy. In addition, the combination of immunotherapy and other therapy (e.g. target therapy, TACE) may have the potential to further improve the outcome, which needs to be verified by clinical research. Further studies need to be performed to benefit advanced HCC patients.
Funding
The study was supported by NSFC (National Nature Science Foundation of China), No. 31671298 (Guang-hai Dai).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1. doi:10.4103/jcar.JCar_9_16
2. Llovet JM, Zucman-Rossi J, Pikarsky E, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2016;2:16018. doi:10.1038/nrdp.2016.18
3. Waller LP, Deshpande V, Pyrsopoulos N. Hepatocellular carcinoma: A comprehensive review. World J Hepatol. 2015;7:2648–2663. doi:10.4254/wjh.v7.i26.2648
4. El Dika I, Khalil DN, Abou‐Alfa GK. Immune checkpoint inhibitors for hepatocellular carcinoma. Cancer. 2019;1–8.
5. Pinter M, Peck‐Radosavljevic M. Review article: systemic treatment of hepatocellular carcinoma. Aliment Pharmacol Ther. 2018;48:
6. Llovet JM, Ricci S, Mazzaferro V, et al.; SHARP Investigators Study Group. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 359;2008:378–390. doi:10.1056/NEJMoa0708857
7. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25–34. doi:10.1016/S1470-2045(08)70285-7
8. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391:1163–1173. doi:10.1016/S0140-6736(18)30207-1
9. Bruix J, Qin S, Merle P, et al.; RESORCE Investigators. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 389;2017:56–66. doi:10.1016/S0140-6736(16)32453-9
10. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379:54–63. doi:10.1056/NEJMoa1717002
11. Zhu AX, Kang YK, Yen CJ, et al. REACH-2 study in Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20:282–296. doi:10.1016/S1470-2045(18)30937-9
12. Smyth MJ, Ngiow SF, Ribas A, Teng MW. Combination cancer immunotherapies tailored to the tumor microenvironment. Nat RevClin Oncol. 2016;13:143–158.
13. Elsegood CL, Tirnitz-Parker JE, Olynyk JK, Yeoh GC. Immune checkpoint inhibition: prospects for prevention and therapy of hepatocellular carcinoma. Clin Transl Immunol. 2017;6:e161. doi:10.1038/cti.2017.47
14. Okusaka T, Ikeda M. Immunotherapy for hepatocellular carcinoma: current status and future perspectives. ESMO Open. 2018;3:e000455. doi:10.1136/esmoopen-2018-000455
15. El‐Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non‐comparative, phase 1/2 dose escalation and expansion trial. Lancet. 2017;389:2492–2502. doi:10.1016/S0140-6736(17)31046-2
16. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE‐224): a non‐randomised, open‐label phase 2 trial. Lancet Oncol. 2018;19:940–952. doi:10.1016/S1470-2045(18)30351-6
17. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30:52–60. doi:10.1055/s-0030-1247132
18. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumors: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–247. doi:10.1016/j.ejca.2008.10.026
19. Ferrara R, Mezquita L, Texier M, et al. Hyperprogressive disease in patients with advanced non‐small cell lung cancer treated with PD‐1/PD‐L1 inhibitors or with single‐agent chemotherapy. JAMA Oncol. 2018;4:1543–1552. doi:10.1001/jamaoncol.2018.3676
20. Jain RK. Antiangiogenesis strategies revisited: from starving tumors to alleviating hypoxia. Cancer Cell. 2014;26:605–622. doi:10.1016/j.ccell.2014.10.006
21. Pinter M, Jain RK. Targeting the renin‐angiotensin system to improve cancer treatment: implications for immunotherapy. Sci Transl Med. 2017;9:eaan5616. doi:10.1126/scitranslmed.aan5616
22. Chen Y, Huang Y, Reiberger T, et al. Differential effects of sorafenib on liver versus tumor fibrosis mediated by stromal‐derived factor 1 alpha/C‐X‐C receptor type 4 axis and myeloid differentiation antigen‐positive myeloid cell infiltration in mice. Hepatology. 2014;59:1435–1447. doi:10.1002/hep.26790
23. Chen Y, Ramjiawan RR, Reiberger T, et al. CXCR4 inhibition in tumor microenvironment facilitates anti‐programmed death receptor‐1 immunotherapy in sorafenib‐treated hepatocellular carcinoma in mice. Hepatology. 2015;61:1591–1602. doi:10.1002/hep.27665
24. Hato T, Goyal L, Greten TF, Duda DG, Zhu AX. Immune checkpoint blockade in hepatocellular carcinoma: current progress and future directions. Hepatology. 2014;60:1776–1782. doi:10.1002/hep.v60.5
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.