Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Programmed Cell Death Ligand 1 (PD-L1) and Major Histocompatibility Complex Class I (MHC Class I) Expression Patterns and Their Pathologic Associations in Triple-Negative Breast Cancer
Authors Kaewkedsri P, Intarawichian P ![]() , Jessadapattarakul S, Kunprom W, Koonmee S, Thanee M, Somintara O, Wongbuddha A, Chadbunchachai P, Nawapun S, Aphivatanasiri C
, Jessadapattarakul S, Kunprom W, Koonmee S, Thanee M, Somintara O, Wongbuddha A, Chadbunchachai P, Nawapun S, Aphivatanasiri C ![]()
Received 24 November 2024
Accepted for publication 24 January 2025
Published 6 February 2025 Volume 2025:17 Pages 123—143
DOI https://doi.org/10.2147/BCTT.S506833
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Ponkrit Kaewkedsri,1 Piyapharom Intarawichian,1 Sirawich Jessadapattarakul,1 Waritta Kunprom,1 Supinda Koonmee,1 Malinee Thanee,1 Ongart Somintara,2 Anongporn Wongbuddha,2 Payia Chadbunchachai,3 Supajit Nawapun,3 Chaiwat Aphivatanasiri1
1Department of Pathology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 3Department of Radiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Chaiwat Aphivatanasiri, Department of Pathology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand, Email [email protected]
Purpose: This study aims to investigate the clinicopathological characteristics of triple-negative breast cancer (TNBC) in relation to programmed cell death ligand 1 (PD-L1) and major histocompatibility complex class I (MHC class I) expression, with a focus on their prognostic significance.
Patients and Methods: A retrospective analysis was conducted on formalin-fixed paraffin-embedded (FFPE) tissue samples from 148 TNBC patients diagnosed between 2008 and 2021. Immunohistochemical analysis evaluated PD-L1 and MHC class I expression. PD-L1 was assessed using Combine Positive Scores (CPS), with the threshold set at CPS ≥ 1 and CPS ≥ 10. MHC class I expression was categorized into low and high levels. Associations between these markers, clinicopathological features, overall survival (OS), and disease-free survival (DFS) were analyzed. PD-L1 expression was also compared between older FFPE blocks (2008– 2018) versus newer blocks (2019– 2021).
Results: PD-L1 expression was observed in 29.1% of cases with a Combined Positive Score (CPS) ≥ 1 and 8.8% of CPS ≥ 10 cases. MHC class I expression was evenly split between low and high levels. Older FFPE blocks (2008– 2018) showed lower PD-L1 expression than newer blocks (2019– 2021). There was no significant association between PD-L1 expression and overall survival (OS) or disease-free survival (DFS). However, high MHC class I expression was strongly associated with improved OS (HR = 0.469, 95% CI: 0.282– 0.780, p=0.004). Patients with negative PD-L1 and high MHC class I expression had the most favorable prognosis, with significant OS for CPS ≥ 1 (HR = 0.447, 95% CI: 0.236– 0.846, p=0.013) and CPS ≥ 10 (HR = 0.516, 95% CI: 0.307– 0.869, p=0.013).
Conclusion: These findings support the potential of PD-L1 and MHC class I expression as prognostic markers for TNBC, offering insights to guide treatment decisions and improve patient outcomes.
Keywords: triple-negative breast cancer, TNBC, programmed cell death ligand 1, PD-L1, major histocompatibility complex class I, MHC class I, immunohistochemistry, prognosis
Introduction
Triple-negative breast cancer (TNBC) comprises 10–20% of invasive breast cancers.1 It lacks estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) expression, presenting challenges in prognosis and treatment. This subtype is associated with higher tumor grade, high mitotic index, and advanced stage at diagnosis.1,2 TNBC’s pronounced immunogenic nature is evidenced by high levels of tumor-infiltrating lymphocytes (TILs), which correlate with patient outcomes and responsiveness to chemotherapy.3,4 High levels of TILs in TNBC patients are linked to improved survival, particularly in response to anthracycline chemotherapy, while low levels of TILs are associated with poorer prognostic factors.5,6
Programmed cell death ligand 1 (PD-L1), an immune checkpoint protein, is found in about 20% of TNBC cases and facilitates immune evasion.7 PD-L1 binds to the PD-1 receptor on T cells, suppressing their activity and helping tumor cells evade immune detection. This mechanism is central to immune escape in cancer. Elevated PD-L1 levels correlate with decreased anti-tumor immune responses due to suppression of T-cell activity and cytokine production, which has varied implications for TNBC patient survival.7–9
Contrasting evidence from studies suggests that while PD-L1 can indicate an unfavorable prognosis, its association with high TILs may improve disease-free survival (DFS) and overall survival (OS) in TNBC patients.10–13 This dual nature suggests that PD-L1’s role in TNBC could depend on the broader immune context, including the extent of immune cell infiltration and other tumor microenvironment factors. Additionally, PD-L1 expression has been identified as a predictive biomarker for response to immunotherapy, underscoring its potential clinical utility in guiding treatment strategies for TNBC.14,15
Major histocompatibility complex class I (MHC class I) molecules are critical for eliciting an immune response against cancer cells. Their interaction with CD8+ T cells is vital for immune surveillance and activating the immune system’s killing mechanisms.16 However, downregulation of MHC class I, noted in various cancers,17–19 including TNBC, impairs immune responses and has emerged as a prognostic biomarker.20–22
While studies in other cancers, such as head and neck squamous cell carcinoma and non-small cell lung carcinoma, have demonstrated that higher PD-L1 expression is associated with loss of MHC class I expression and poorer clinical outcomes,23,24 the exact relationship between PD-L1 and MHC class I in TNBC remains underexplored and needs further elucidation. As such, our study aims to investigate the co-expression of PD-L1 and MHC class I in TNBC, which could provide valuable insights into the tumor immune landscape of TNBC patients and influence future treatment pathways that restore immune function and improve outcomes.
Materials and Methods
Patients and Tissue Samples
Cases were selected from a cohort of 1,979 Thai breast cancer patients who underwent various surgical procedures at the Srinagarind Hospital Department of Pathology in Khon Kaen Province from 2008 to 2021. Formalin-fixed paraffin-embedded (FFPE) tissue specimens from 148 TNBC patients were available from among 233 individuals diagnosed with this condition.
The patients were divided into two groups: 105 cases from 2008 to 2018, constituting the primary dataset, and 43 cases from 2019 to 2021. This was done to compare the proportions of PD-L1 and MHC class I expression in FFPE blocks of different ages.
TNBC status was confirmed through immunohistochemistry testing negative for estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2). Additionally, all cases were validated as HER2-negative by dual in-situ hybridization (DISH) assays. Clinical data were collected, including age at diagnosis, T stage, N stage, histologic subtype, histologic grade, neoadjuvant therapy, presence of in-situ component, Ki-67 proliferation index, recurrence, and follow-up information.
This study was performed in accordance with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Khon Kaen University (HE651278). All data were fully anonymized, and the IRB waived the requirement for informed consent due to minimal risk.
Tumor-Infiltrating Lymphocytes (TILs) Assessment
TILs were assessed on whole hematoxylin and eosin (H&E) tumor slides by pathologists blinded to all clinical and pathological information. The number of TILs was determined according to the International TILs Working Group (ITWG) guidelines.25 Scoring was performed to calculate TIL density, represented as a percentage of the stromal area, to the nearest 5%. Rather than focusing on hotspots, which might lead to a biased view of TIL density, scores were determined by averaging across the entire slide.
The assessment was limited to TILs located within the confines of the invasive tumor border. Following ITWG guidelines, inflammatory cells such as neutrophils and granulocytes were excluded, while all mononuclear cells, including lymphocytes and plasma cells, were included as TILs. TILs found within nests, epithelial cells, necrosis, and fibrosis were also excluded from the assessment. The cut-off of 50% for dividing high and low TILs was based on a previous study showing the 50% cut-off score is a potent predictor of overall survival (OS) and disease-free survival (DFS).26
Tissue Microarray (TMA) and Immunohistochemistry (IHC)
FFPE tissue samples were prepared at the Srinagarind Hospital Department of Pathology. Histological slides were reviewed, and pathologists selected tumor areas for analysis. Each case was represented by duplicated 3 mm cores, ensuring heterogeneous tissue representation.
The TMA blocks were sectioned into 4 µm thick slices, deparaffinized, and rehydrated. IHC was performed using a Ventana Benchmark XT automated stainer (Ventana Medical Systems, Tucson, AZ, USA). The antibodies used were PD-L1 (clone 22C3, dilution 1:33, Agilent, California, USA) and MHC class I (clone EMR8-5, dilution 1:200, Abcam, Cambridge, UK). Normal tonsil tissue served as a positive control for all antibodies.
PD-L1 expression was calculated using the Combined Positive Score (CPS), which is a percentage that represents the proportion of PD-L1-positive cells compared to other tumor cells. The CPS was calculated by dividing the number of cells expressing PD-L1 (including tumor cells, lymphocytes, and macrophages) by the total number of viable tumor cells and multiplying the result by 100. The result was considered positive when the Combined Positive Score (CPS) was ≥1 and compared to a threshold of ≥10.
MHC class I expression was evaluated using a semi-quantitative histochemical staining method (H-score), calculated by combining the staining intensity and the proportion of stained cells at each intensity level. The staining intensity was graded as follows: 0 for no staining, 1 for weak staining, 2 for moderate staining, and 3 for strong staining. The proportion of stained cells ranged from 0% to 100%. The final H-score for each core was obtained by summing the products of the intensities and their corresponding proportions, resulting in a score range of 1 to 300. The cut-off value for distinguishing between high and low MHC class I expression was determined using the median H-score of 187.5.
Independent reviews of all IHC slides were conducted using images digitally captured on a digital slide scanner (Hamamatsu NanoZoomer S360, Japan) at a maximum magnification of ×400 by pathologists blinded to the clinicopathological data. A combination of PD-L1 and MHC class I expression status yielded four groups: Group 1 (PD-L1 Negative / MHC class I Low), Group 2 (PD-L1 Negative / MHC class I High), Group 3 (PD-L1 Positive / MHC class I Low), and Group 4 (PD-L1 Positive / MHC class I High). These four groups were analyzed for clinical significance.
Statistical Analysis
All statistical analyses were conducted using SPSS Statistical Software (version 28.0, IBM Corp., Armonk, NY, USA). The Chi-square or Fisher’s exact test assessed the association between PD-L1 and MHC class I expression and clinicopathological characteristics. Survival analyses were performed using Kaplan-Meier curves, and differences between curves were evaluated with Log rank tests. The mean follow-up time was calculated using the reverse Kaplan-Meier method. Univariate and multivariate analyses were performed using Cox regression, reporting hazard ratios (HR), and 95% confidence intervals (CI). Variables statistically significant in univariate analyses or a p-value <0.10 were included in the multivariate model. While not statistically significant, PD-L1 and MHC class I were included due to their clinical relevance. Statistical significance was defined as p-value <0.05, with all reported p-values being two-sided.
Results
Immunohistochemistry Analysis of PD-L1 and MHC Class I Expression in TNBC Samples
The comparison of PD-L1 and MHC class I expression in 148 cases, as shown in Table 1, revealed a significant difference in PD-L1 expression across different ages of FFPE blocks. Specifically, a lower presence of PD-L1 was observed in blocks older than five years (2008–2018 group) compared to blocks aged five years or less (2019–2021 group) (p=0.003 for CPS≥1 and p<0.001 for CPS≥10). Similarly, MHC class I expression differed significantly by age group (p=0.046).
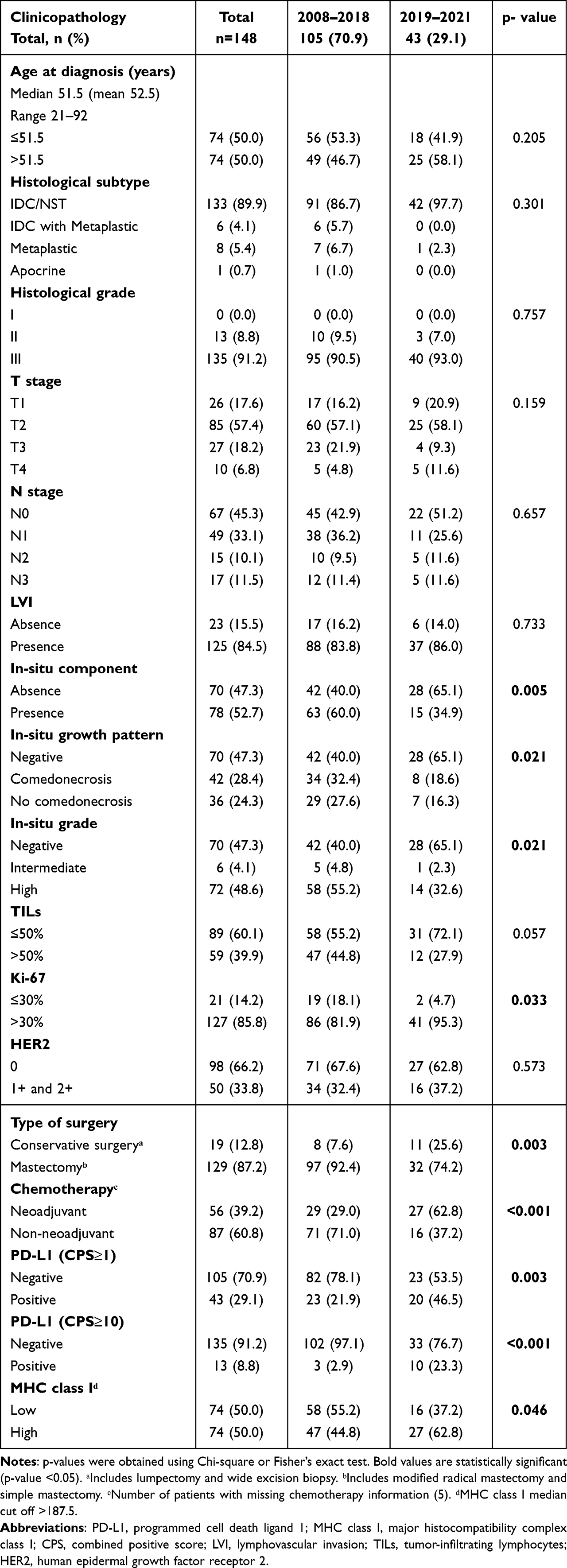 |
Table 1 Comparison of Clinicopathological Characteristics Between FFPE Age Groups |
The analysis of PD-L1 expression with CPS≥1 showed negative expression in 105 (70.9%) cases and positive expression in 43 (29.1%) cases. For CPS≥10, 135 (91.2%) cases were negative for PD-L1, while 13 (8.8%) cases were positive. The correlation between PD-L1 expression and the clinical characteristics of patients is summarized in Table 2.
 |
Table 2 Clinicopathological Characteristics of Triple-Negative Breast Cancer Patients and PD-L1 Expression |
No significant correlation was found between PD-L1 expression and most clinicopathological characteristics. However, PD-L1 expression for CPS≥1 and CPS≥10 was significantly associated with age (p=0.046 and 0.042, respectively), T stage (p=0.047 and 0.006, respectively), and lymphovascular invasion (LVI) (p=0.002 and 0.032, respectively).
In contrast, TILs and MHC class I were associated only with CPS≥1 (p=0.001 and <0.001, respectively). The in-situ component and in-situ grade were significantly associated only with CPS≥10 (p=0.025 and 0.042, respectively).
Low expression of MHC class I was observed in 74 (50.0%) cases, while high expression was found in the remaining 74 (50.0%) cases. Among clinicopathological characteristics (Table 3), significant associations were found between MHC class I expression and lymphovascular invasion (LVI) (p<0.001) as well as TILs (p=0.029).
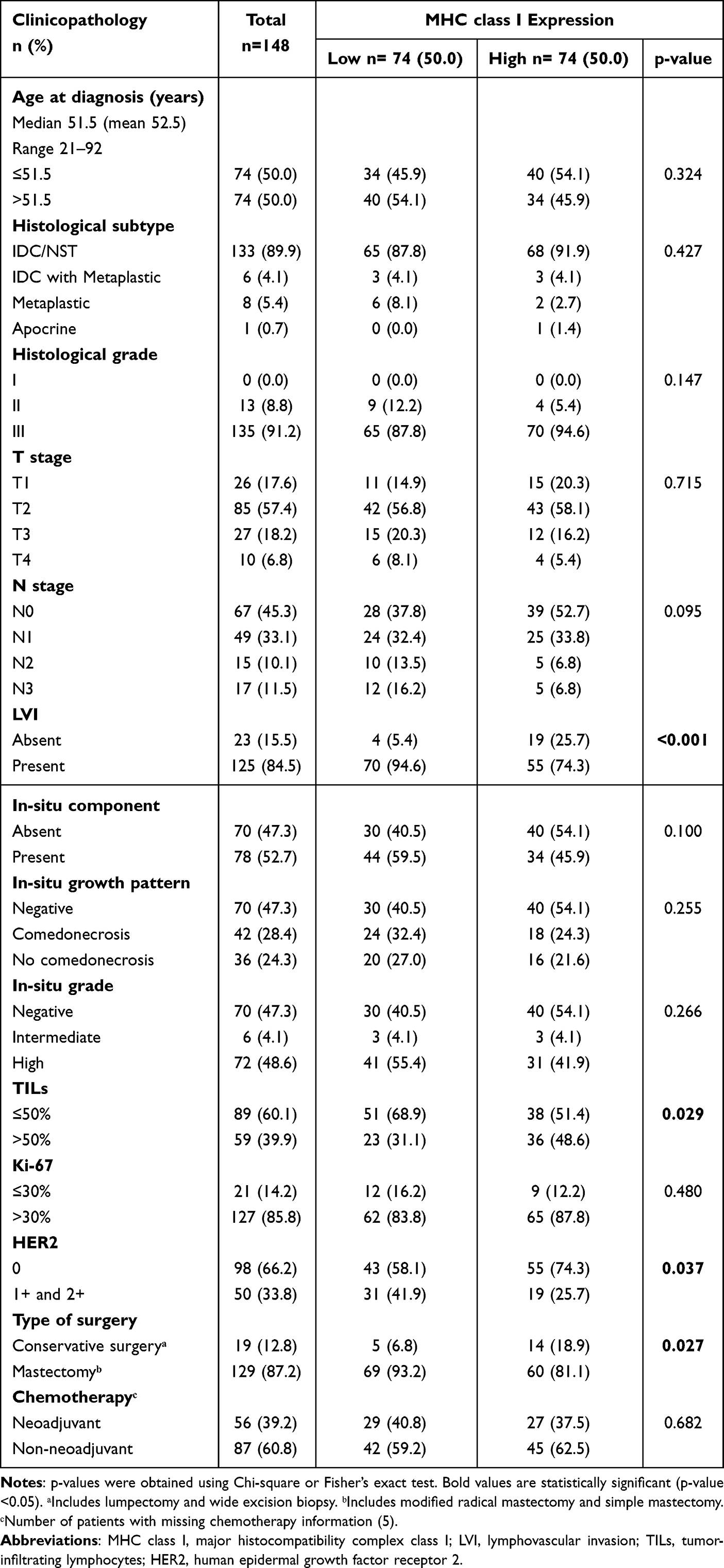 |
Table 3 Clinicopathological Characteristics of Triple-Negative Breast Cancer Patients and MHC Class I Expression |
Relationship Between PD-L1 Expression and MHC Class I Expression
Table 4 shows that among TNBC patients with PD-L1 CPS ≥1, 62 cases (41.9%) showed PD-L1 negativity with low MHC class I expression. PD-L1 negativity with high MHC class I expression was observed in 43 cases (29.1%). PD-L1 positivity with low MHC class I expression was seen in 12 cases (8.1%), while PD-L1 positivity with high MHC class I expression was found in 31 cases (20.9%).
 |
Table 4 Associations Between Clinicopathological Characteristics and PD-L1 (CPS≥1) With MHC Class I Expression Pattern |
In TNBC patients with a PD-L1 CPS cut-off ≥10, 70 cases (47.3%) were PD-L1 negative with low MHC class I expression, and 65 cases (43.9%) were PD-L1 negative with high MHC class I expression. PD-L1 positivity with low MHC class I expression was observed in 4 cases (2.7%), while PD-L1 positivity with high MHC class I expression was detected in 9 cases (6.1%). Representative images illustrating the relationship between MHC class I and PD-L1 expression are presented in Figure 1.
 |
Figure 1 Expression Patterns of PD-L1 and MHC class I in triple-negative breast cancer Samples (x200). (A–C) Invasive ductal carcinoma, no special type (IDC/NST) (A), showing no expression of PD-L1 (B) and very low MHC class I expression (C). (D–F) IDC/NST (D) with no PD-L1 expression (E) and high MHC class I expression (F). (G–I) Metaplastic squamous cell carcinoma (G) with PD-L1 positivity (H) and low MHC class I expression (I). (J–L) IDC/NST (J) with positive PD-L1 (K) and high MHC class I expression (L). |
We found significant associations between PD-L1 CPS ≥1 and MHC class I expression with age (p=0.004), LVI (p<0.001), and TILs (p=0.001), as shown in Table 4. Similarly, PD-L1 CPS ≥10 and MHC class I expression were significantly associated with T stage (p=0.020), LVI (p<0.001), in-situ component (p=0.036), in-situ grade (p=0.030), and HER2 (p=0.022), as shown in Table 5.
 |
Table 5 Associations Between Clinicopathological Characteristics and PD-L1 (CPS≥10) With MHC Class I Expression Pattern |
Survival Analysis and Prognosis Significance
In the survival analysis, data were available on 143 patients, with a median follow-up of 38.30 months (ranging from 0.20 to 180.33 months). By the conclusion of the study in March 2024, 40 patients experienced recurrence, and 65 patients died.
Kaplan-Meier analysis assessed the prognostic value of PD-L1 and MHC class I expression. Using different cut-offs for PD-L1 (CPS≥1 and CPS≥10), no significant differences were observed in overall survival (OS) or disease-free survival (DFS) (Figures 2A and 2B). There were also no statistically significant differences in DFS for MHC class I expression (p=0.291). However, a statistically significant association with favorable prognosis was observed in patients with high MHC class I expression (p=0.003), with a mean OS of 119.34 months compared to patients with low MHC class I expression (Figure 2C).
 |
Figure 2 Kaplan-Meier curves for survival analyses in TNBC patients. Disease-free survival (DFS) and overall survival (OS) according to:PD-L1 combined positive score (CPS) at a threshold of 1 (A), PD-L1 combined positive score (CPS) at a threshold of 10 (B), MHC class I (C), the association of PD-L1 (CPS≥1) with MHC class I (D), and the association of PD-L1 (CPS≥10) with MHC class I (E). |
When combining PD-L1 and MHC class I expression, survival outcomes were analyzed based on the PD-L1 CPS cut-offs of ≥1 and ≥10 with MHC class I status. The Kaplan-Meier survival curves for PD-L1 CPS ≥1 with MHC class I status showed no significant difference in DFS (p=0.479) but a significant difference in OS (p=0.027) (Figure 2D). Similarly, PD-L1 CPS ≥10 was associated with a significant difference in OS (p=0.017) but not DFS (p=0.085) (Figure 2E).
To identify prognostic factors, we investigated the association between clinical parameters, DFS, and OS through univariate and multivariate analyses using Cox regression, as shown in Table 6. Age, T stage, and chemotherapy were significant factors in the univariate analysis of DFS; however, only age and chemotherapy remained significant in the multivariate analysis.
 |
Table 6 Univariate and Multivariate Regression Analyses in TNBC Patients |
In the Cox regression analysis for OS, age, T stage, N stage, LVI, TILs, chemotherapy, and MHC class I were all significant factors. Interestingly, PD-L1 (CPS≥1) negativity with high MHC class I expression (HR=0.447, 95% CI 0.236–0.846, p=0.013) and PD-L1 (CPS≥10) negativity with high MHC class I expression (HR=0.516, 95% CI 0.307–0.869, p=0.013) were significantly associated with a favorable prognosis in OS compared to PD-L1 negativity with low MHC class I expression, PD-L1 positivity with low MHC class I expression, and PD-L1 positivity with high MHC class I expression in the univariate analysis. However, these subgroup differences did not remain significant in the multivariate analysis.
Discussion
Most invasive breast cancers are positive for estrogen, progesterone, and HER-2 receptors, which is also true of normal breast cells. In contrast, triple-negative breast cancer (TNBC) is negative for these receptors. Thus, it does not respond to therapies targeting these receptors. This makes TNBC, which tends to be an aggressive cancer, more challenging to treat. Worldwide, TNBC accounts for approximately 10% to 20% of all breast cancer cases.1
The unique features of TNBC speak to the necessity of exploring the role of different biomarkers to improve prognosis and guide treatment decisions. This study sought to do that by identifying how diverse patient and clinicopathological characteristics are related to overall survival and recurrence. This included examining the interaction of PD-L1, MHC Class I, and TIL biomarkers.
More specifically, our study analyzed 148 Thai women diagnosed with TNBC over a 14-year span from 2008 to 2021. This Thai cohort’s demographic and clinical traits closely resembled prior observations. For example, Leeha et al reported 52.3 as the mean age of diagnosis (range 25–92 years) among Thai TNBC patients,27 which is almost identical to the mean age of 52.5 years found in the present study.
Interestingly, there are cultural differences in the mean age of diagnosis. The Thai mean age of 52 surpasses the median age of Moroccan women (46 years), closely matches the median age of Hispanic TNBC patients (50 years), and is significantly lower than the median age of TNBC among African women (64 years).28,29 Cultural variations in age distribution may be due to lifestyle and environmental factors as well as possible genetic predispositions unique to each population, which could impact disease onset and progression. Exploring the role of those factors in cultural differences of TNBC is beyond the scope of the present study but certainly worthy of future study.
In our study of Thai women diagnosed with TNBC, the most prevalent histological subtype was invasive ductal carcinoma, no special type (IDC/NST) (89.9%), followed by Metaplastic (5.4%), IDC with Metaplastic (4.1%), and Apocrine (0.7%). These results align with the histological subtypes identified in a study of Dutch women conducted by Balkenhol et al.30 This variation in histological subtypes highlights the need for tailored therapeutic approaches and personalized treatment strategies.
In our study, 13 cases (8.8%) were histological grade II, and 135 cases (91.2%) were grade III, with no grade I cases. This aligns with earlier findings that most TNBCs are high-grade IDCs.31 This underscores the importance of histological grade in identifying patients with TNBC who may benefit from systemic chemotherapy.
Within our study, 21 cases (14.2%) had low Ki-67 expression levels, while 127 cases (85.8%) had high expression levels, indicating a high proliferative tumor phenotype. Zhu X et al32 found that 74.2% of TNBC cases with high Ki-67 (cut-off of 30%) are significantly associated with a poorer prognosis (OS and DFS) and may benefit from adjuvant chemotherapy.
Additionally, 125 cases (84.5%) in our study showed the presence of lymphovascular invasion (LVI), while 23 cases (15.5%) did not. This observation is consistent with the findings of Agarwal et al,33 who emphasize a higher incidence of LVI in TNBC patients than in non-TNBC patients. LVI is a prognostic factor for relapse and death in TNBC, which has important implications for therapeutic treatment options.
TILs demonstrate potential as a valuable prognostic marker in TNBC, considering their correlation with improved outcomes, enhanced pathologic complete response, and overall better prognosis.26,34–36 In the present study, 89 cases (60.1%) exhibited low TILs, while 59 cases (39.9%) had high TILs, indicating varied immune cell infiltration.
However, there was no significant association between TILs and overall survival (OS) or disease-free survival (DFS) in TNBC patients. Tumor heterogeneity, immune checkpoint expression, the complex composition of TILs, and their dynamic interaction with the tumor microenvironment are potential contributing factors to this lack of association. Further research is necessary to fully understand the underlying mechanisms behind the prognostic significance of TILs in TNBC.
The reported prevalence of PD-L1 expression in TNBC has ranged from 13.7% to 75% across several studies.7,37–39 A previous study assessed CPS using thresholds of 1 and 10 for PD-L1 evaluation in Phase III clinical trials of TNBC involving pembrolizumab, utilizing the clone 22C3, found a prevalence of 53.9% for CPS≥1 cut-off and 27.2% for ≥10 cut-off.40 In our study, PD-L1 expression was 29.1% for CPS≥1 cut-off and 8.8% for CPS≥10 cut-off. The prevalence in CPS≥1 cut-off is similar to the approximately 19% reported in the studies by Mittendorf et al and Ali et al7,38 However, Mittendorf et al used the clone 5H1, where PD-L1 positivity was defined as tumor cell surface membrane staining in >5% of cells.7 In contrast, Ali et al employed the clone E1L3N, scoring PD-L1 expression in tumor and immune cell separately on a four-point scale: 0 (≤1% positive cells), 1 (1%–5%), 2 (5%–10%), and 3 (≥10%).38 It is important to note that using different PD-L1 antibody clones and cut-off points across studies may contribute to variations in reported findings.
When we compared PD-L1 expression between two time periods, we found a lower presence of PD-L1 expression in FFPE blocks older than 5 years (2008–2018) than in those 5 years old or newer (2019–2021). This finding is consistent with a previous study that reported reduced PD-L1 expression in FFPE blocks older than 3 years in a non-small-cell lung cancer study.41
PD-L1 expression in TNBC is linked to unfavorable prognosis, emphasizing the need for advanced therapeutic approaches.37,42–44 Importantly, none of the patients in our cohort received anti-PD-L1 therapy during the 2008–2018 study period, ensuring that this treatment did not affect survival outcomes. This is particularly relevant given the increased use of anti-PD-L1 treatments for TNBC in recent years, which have shown encouraging results. Surprisingly, our study found no significant correlation between PD-L1 expression and disease-free survival or overall survival in TNBC patients. This illustrates the complexities of PD-L1’s role in TNBC and suggests that other factors may influence survival outcomes in these patients.
MHC class I in TNBC plays a crucial role in both immune evasion and clinical outcomes. Several studies have reported low expression of MHC class I in TNBC, with percentages ranging from 12.8% to 59.37%.21,39,45,46 In our study, the frequency of low MHC class I expression was approximately 50.0%. This variation may be due to different cut-off points for defining high and low expression. The standardization of cut-off points would improve the ability to compare findings across studies, including meta-analyses.
While previous studies have associated enhanced MHC class I expression with better DFS,20–22 our findings pointed to a significant correlation with OS but not DFS. The lack of DFS correlation in our study highlights the complexity and heterogeneity of TNBC. Further research is needed to understand the nuances of MHC class I expression and its impact on survival outcomes.
In our study, we found that PD-L1 positivity, defined using the 22C3 clone with a Combined Positive Score (CPS) ≥1, was associated with low MHC class I expression (clone EMR8-5, H-score with a median cut-off) in 12 cases (8.1%). When a more stringent CPS ≥10 was applied, PD-L1 positivity with low MHC class I expression was observed in 4 cases (2.7%).
In comparison to previous studies, one study by Lee ji Shin et al reported that among 166 TNBC cases, 69.2% were classified as PD-L1-positive based on a ≥1% PD-L1 expression threshold in tumor-associated immune cells. Notably, Lee ji Shin et al also observed a significant loss of MHC class I expression; however, specific details regarding the PD-L1 antibody clone and MHC class I cut-off values were not provided.47 Another study by Dusenbery AC et al documented MHC class I loss in 46% (11 out of 24) of PD-L1-positive TNBC cases. Dusenbery AC et al utilized the MHC class I clone EMR8-5, with expression categorized as “intact”, “subclonal loss”, or “diffuse loss” according to the extent of membranous staining. Cases with subclonal or diffuse loss were classified as MHC class I negative. PD-L1 positivity in the same study was determined using the SP142 clone, with cases considered positive if PD-L1-positive immune cells occupied ≥1% of the area.39
Our study adds to the growing body of evidence that PD-L1 positivity and MHC class I loss can coexist in TNBC, though variations in methodologies, such as PD-L1 clones and scoring systems, make cross-study comparisons challenging. These differences underscore the need for standardized assays in future studies to better define the relationship between PD-L1 and MHC class I expression in TNBC.
This research aimed to analyze TNBC to identify prognostic factors by examining the expression of tumor PD-L1 and MHC class I. Previous studies highlight the intricate relationship between MHC class I and PD-L1 in different cancers, indicating varied prognostic implications. Positive MHC class I expression with negative or rare PD-L1 expression is linked to a favorable clinical course in intrahepatic cholangiocarcinoma. In contrast, in adenocarcinoma of the lung, cases with both positive MHC class I and PD-L1 expression have exhibited significantly shorter overall survival, while in PD-L1-positive and MHC class I-negative cases, no significant prognostic impact was observed. In head and neck squamous cell carcinoma (HNSCC), MHC class I loss with positive PD-L1 is associated with significantly poorer survival than MHC class I-positive cases.23,48,49
In our study, PD-L1 negativity with high MHC class I expression significantly improved OS, possibly by contributing to reduced immune evasion or by promoting a stronger immune response. In either case, patients with this combination may be more likely to benefit from immunotherapy or other treatment approaches. The interplay of PD-L1 negativity and high MHC class I expression in triple-negative breast cancer warrants further investigation to validate and refine the prognostic value of these biomarkers.
Our study’s limitations necessitate careful interpretation of the findings. The extended storage period of the formalin-fixed paraffin-embedded (FFPE) tissue blocks raises concerns about decreased protein antigenicity. Over time, protein degradation could result in suboptimal immunohistochemical staining intensity, potentially leading to false-negative results, especially for PD-L1. Additionally, using tissue microarrays (TMAs) as representatives for entire tumors may not provide a comprehensive depiction of intratumoral heterogeneity, which is critical in triple-negative breast cancer prognosis. Each of these potential limitations should be further explored to ensure the integrity of the methodology used to investigate TNBC and other forms of cancer.
Conclusions
In the present study, we analyzed 148 patients with TNBC, revealing significant age-related differences and associations with clinicopathological characteristics. Older FFPE blocks showed lower PD-L1 expression. PD-L1 and MHC class I expression were linked to age, T stage, LVI, and TILs. High MHC class I expression was associated with better overall survival, while PD-L1 expression alone had no significant impact on survival outcomes. PD-L1 negativity, in combination with high MHC class I expression, was associated with favorable overall survival. This study emphasizes the evolving characteristics of triple-negative breast cancer and highlights the potential of several prognostic factors for future investigation.
Abbreviations
PD-L1, Programmed Cell Death Ligand 1; MHC Class I, Major Histocompatibility Complex Class I;
TNBC, Triple-Negative Breast Cancer; CPS, Combined Positive Score; OS, Overall Survival; DFS, Disease-Free Survival; FFPE, Formalin-Fixed Paraffin-Embedded; ER, Estrogen Receptor; PR, Progesterone Receptor; HER2, Human Epidermal Growth Factor Receptor 2; TILs, Tumor-Infiltrating Lymphocytes; TMA, Tissue Microarray; IHC, Immunohistochemistry; H&E, Hematoxylin and Eosin; ITWG, International TILs Working Group.
Data Sharing Statement
The raw data supporting the conclusion of this article will be made available by the authors without undue reservation.
Ethics Approval and Consent to Participate
The study protocol was approved by the Khon Kaen University Ethics Committee for Human Research (HE651278). All data were fully anonymized, and the IRB waived the requirement for informed consent due to minimal risk.
Acknowledgments
We want to express our gratitude to Srinagarind Hospital for providing the specimens and follow-up data. We also thank Suwit Balthaisong for constructing the tissue microarray slides used in this work. Piyanan Suparattanagool in the Khon Kaen University, Faculty of Medicine’s Clinical Epidemiology Unit provided valuable guidance in the biostatistical analysis of our data. Thanks also to Dylan Southard at the KKU Publication Clinic for helping edit this manuscript. Finally, we respectfully acknowledge the women diagnosed with TNBC in this study. We sincerely hope that this and future research will eventually identify the causes and, more importantly, life-saving treatments for breast cancer.
Funding
This research was supported by a Postgraduate Study Support Grant from the Faculty of Medicine, Khon Kaen University, and the Invitation Research Fund from the Faculty of Medicine, Khon Kaen University, Thailand (No. IN66001).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Kumar P, Aggarwal R. An overview of triple-negative breast cancer. Arch Gynecol Obstet. 2016;293(2):247–269. doi:10.1007/s00404-015-3859-y
2. Won KA, Spruck C. Triple‑negative breast cancer therapy: current and future perspectives (Review). Int j Oncol. 2020;57(6):1245–1261. doi:10.3892/ijo.2020.5135
3. Bianchini G, De Angelis C, Licata L, Gianni L. Treatment landscape of triple-negative breast cancer - expanded options, evolving needs. Nat Rev Clin Oncol. 2022;19(2):91–113. doi:10.1038/s41571-021-00565-2
4. Stanton SE, Adams S, Disis ML. Variation in the incidence and magnitude of tumor-infiltrating lymphocytes in breast cancer subtypes: a systematic review. JAMA Oncol. 2016;2(10):1354–1360. doi:10.1001/jamaoncol.2016.1061
5. Denkert C, von Minckwitz G, Darb-Esfahani S, et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018;19(1):40–50. doi:10.1016/S1470-2045(17)30904-X
6. Loi S, Drubay D, Adams S, et al. Tumor-infiltrating lymphocytes and prognosis: a pooled individual patient analysis of early-stage triple-negative breast cancers. J clin oncol. 2019;37(7):559–+. doi:10.1200/JCO.18.01010
7. Mittendorf EA, Philips AV, Meric-Bernstam F, et al. PD-L1 expression in triple-negative breast cancer. Cancer Immunol Res. 2014;2(4):361–370. doi:10.1158/2326-6066.CIR-13-0127
8. Gatalica Z, Snyder C, Maney T, et al. Programmed cell death 1 (PD-1) and its ligand (PD-L1) in common cancers and their correlation with molecular cancer type. Cancer Epidemiol Biomarkers Prev. 2014;23(12):2965–2970. doi:10.1158/1055-9965.EPI-14-0654
9. Qin T, Duo ZY, Qin G, et al. High PD-L1 expression was associated with poor prognosis in 870 Chinese patients with breast cancer. Oncotarget. 2015;6(32):33972–33981.
10. Bae SB, Cho HD, Oh MH, et al. Expression of programmed death receptor ligand 1 with high tumor-infiltrating lymphocytes is associated with better prognosis in breast cancer. J Breast Cancer. 2016;19(3):242–251. doi:10.4048/jbc.2016.19.3.242
11. Mori H, Kubo M, Yamaguchi R, et al. The combination of PD-L1 expression and decreased tumor-infiltrating lymphocytes is associated with a poor prognosis in triple-negative breast cancer. Oncotarget. 2017;8(9):15584–15592. doi:10.18632/oncotarget.14698
12. Tomioka N, Azuma M, Ikarashi M, et al. The therapeutic candidate for immune checkpoint inhibitors elucidated by the status of tumor-infiltrating lymphocytes (TILs) and programmed death ligand 1 (PD-L1) expression in triple negative breast cancer (TNBC). Breast Cancer. 2018;25(1):34–42. doi:10.1007/s12282-017-0781-0
13. Wang X, Liu Y. PD-L1 expression in tumor infiltrated lymphocytes predicts survival in triple-negative breast cancer. Pathol Res Pract. 2020;216(3):152802. doi:10.1016/j.prp.2019.152802
14. Michaels E, Chen N, Nanda R. The role of immunotherapy in Triple-Negative Breast Cancer (TNBC). Clinical Breast Cancer. 2024;24:263–270. doi:10.1016/j.clbc.2024.03.001
15. Davis AA, Patel VG. The role of PD-L1 expression as a predictive biomarker: an analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J Immunother Cancer. 2019;7:278. doi:10.1186/s40425-019-0768-9
16. Wu X, Li T, Jiang R, Yang X, Guo H, Yang R. Targeting MHC-I molecules for cancer: function, mechanism, and therapeutic prospects. mol Cancer. 2023;22(1):194. doi:10.1186/s12943-023-01899-4
17. Friedman LA, Bullock TN, Sloan EA, Ring KL, Mills AM. MHC class I loss in endometrial carcinoma: a potential resistance mechanism to immune checkpoint inhibition. Mod Pathol. 2021;34(3):627–636. doi:10.1038/s41379-020-00682-w
18. Schrörs B, Lübcke S, Lennerz V, et al. HLA class I loss in metachronous metastases prevents continuous T cell recognition of mutated neoantigens in a human melanoma model. Oncotarget. 2017;8(17):28312–28327. doi:10.18632/oncotarget.16048
19. Erdogdu IH. MHC Class 1 and PDL-1 status of primary tumor and lymph node metastatic tumor tissue in gastric cancers. Gastroenterol Res Pract. 2019;2019:1–7. doi:10.1155/2019/4785098
20. Pedersen MH, Hood BL, Beck HC, Conrads TP, Ditzel HJ, Leth-Larsen R. Downregulation of antigen presentation-associated pathway proteins is linked to poor outcome in triple-negative breast cancer patient tumors. Oncoimmunology. 2017;6(5):e1305531. doi:10.1080/2162402X.2017.1305531
21. Han SH, Kim M, Chung YR, Woo JW, Choi HY, Park SY. Expression of HLA class I is associated with immune cell infiltration and patient outcome in breast cancer. Sci Rep. 2022;12(1):20367. doi:10.1038/s41598-022-24890-3
22. Qiao W, Jia Z, Guo W, Liu Q, Guo X, Deng M. Prognostic and clinical significance of human leukocyte antigen class I expression in breast cancer: a meta-analysis. Mol Diagn Ther. 2023;27(5):573–582. doi:10.1007/s40291-023-00664-z
23. Yoo SH, Keam B, Ock CY, et al. Prognostic value of the association between MHC class I downregulation and PD-L1 upregulation in head and neck squamous cell carcinoma patients. Sci Rep. 2019;9:7680. doi:10.1038/s41598-019-44206-2
24. Perea F, Sánchez-Palencia A, Gómez-Morales M, et al. HLA class I loss and PD-L1 expression in lung cancer: impact on T-cell infiltration and immune escape. Oncotarget. 2018;9(3):4120–4133. doi:10.18632/oncotarget.23469
25. Salgado R, Denkert C, Demaria S, et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann Oncol. 2015;26(2):259–271. doi:10.1093/annonc/mdu450
26. Fuchs TL, Pearson A, Pickett J, et al. Why pathologists and oncologists should know about tumour-infiltrating lymphocytes (TILs) in triple-negative breast cancer: an Australian experience of 139 cases. Pathology. 2020;52(5):515–521. doi:10.1016/j.pathol.2020.04.004
27. Leeha M, Kanokwiroon K, Laohawiriyakamol S, Thongsuksai P. Immunohistochemistry-based molecular subtyping of triple-negative breast cancer and its prognostic significance. Pathol Oncol Res. 2023;29:1611162. doi:10.3389/pore.2023.1611162
28. Lara-Medina F, Pérez-Sánchez V, Saavedra-Pérez D, et al. Triple-negative breast cancer in Hispanic patients. Cancer. 2011;117(16):3658–3669. doi:10.1002/cncr.25961
29. Siddharth S, Sharma D. Racial disparity and triple-negative breast cancer in African-American Women: a multifaceted affair between obesity, biology, and socioeconomic determinants. Cancers. 2018;10(12):514. doi:10.3390/cancers10120514
30. Balkenhol MCA, Vreuls W, Wauters CAP, Mol SJJ, Van Der Laak JAWM, Bult P. Histological subtypes in triple negative breast cancer are associated with specific information on survival. Ann Diagn Pathol. 2020;46:151490. doi:10.1016/j.anndiagpath.2020.151490
31. Geyer FC, Pareja F, Weigelt B, et al. The spectrum of triple-negative breast disease. Am J Pathol. 2017;187(10):2139–2151. doi:10.1016/j.ajpath.2017.03.016
32. Zhu X, Chen L, Huang B, et al. The prognostic and predictive potential of Ki-67 in triple-negative breast cancer. Sci Rep. 2020;10(1):225. doi:10.1038/s41598-019-57094-3
33. Agarwal G, Nanda G, Lal P, et al. Outcomes of Triple-Negative Breast Cancers (TNBC) compared with Non-TNBC: does the survival vary for all stages? World J Surg. 2016;40(6):1362–1372. doi:10.1007/s00268-016-3422-4
34. Loi S, Michiels S, Salgado R, et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: results from the FinHER trial. Ann Oncol. 2014;25(8):1544–1550. doi:10.1093/annonc/mdu112
35. Abuhadra N, Sun R, Yam C, et al. Predictive roles of baseline stromal tumor-infiltrating lymphocytes and Ki-67 in pathologic complete response in an early-stage triple-negative breast cancer prospective trial. Cancers. 2023;15(13):3275. doi:10.3390/cancers15133275
36. Sun GY, Zhang J, Wang BZ, et al. The prognostic value of tumour-infiltrating lymphocytes, programmed cell death protein-1 and programmed cell death ligand-1 in Stage I–III triple-negative breast cancer. Br J Cancer. 2023;128(11):2044–2053. doi:10.1038/s41416-023-02218-w
37. Guo L, Li W, Zhu X, et al. PD-L1 expression and CD274 gene alteration in triple-negative breast cancer: implication for prognostic biomarker. SpringerPlus. 2016;5(1):805. doi:10.1186/s40064-016-2513-x
38. Ali HR, Glont SE, Blows FM, et al. PD-L1 protein expression in breast cancer is rare, enriched in basal-like tumours and associated with infiltrating lymphocytes. Ann Oncol. 2015;26(7):1488–1493. doi:10.1093/annonc/mdv192
39. Dusenbery AC, Maniaci JL, Hillerson ND, Dill EA, Bullock TN, Mills AM. MHC class I loss in triple-negative breast cancer: a potential Barrier to PD-1/PD-L1 checkpoint inhibitors. Am J Surg Pathol. 2021;45(5):701. doi:10.1097/PAS.0000000000001653
40. Sigurjonsdottir G, De Marchi T, Ehinger A, et al. Comparison of SP142 and 22C3 PD-L1 assays in a population-based cohort of triple-negative breast cancer patients in the context of their clinically established scoring algorithms. Breast Cancer Res. 2023;25(1):123. doi:10.1186/s13058-023-01724-2
41. Kim SY, Kim TE, Park CK, et al. Comprehensive Comparison of 22C3 and SP263 PD-L1 expression in non-small-cell lung cancer using routine clinical and conditioned archives. Cancers. 2022;14(13):3138. doi:10.3390/cancers14133138
42. Polónia A, Pinto R, Cameselle-Teijeiro JF, Schmitt FC, Paredes J. Prognostic value of stromal tumour infiltrating lymphocytes and programmed cell death-ligand 1 expression in breast cancer. J Clin Pathol. 2017;70(10):860–867. doi:10.1136/jclinpath-2016-203990
43. Choi SH, Chang JS, Koo JS, et al. Differential prognostic impact of strong PD-L1 expression and 18F-FDG uptake in triple-negative breast cancer. Am J Clin Oncol. 2018;41(11):1049. doi:10.1097/COC.0000000000000426
44. Lotfinejad P, Asghari Jafarabadi M, Abdoli Shadbad M, et al. Prognostic role and clinical significance of Tumor-Infiltrating Lymphocyte (TIL) and Programmed Death Ligand 1 (PD-L1) Expression in Triple-Negative Breast Cancer (TNBC): a systematic review and meta-analysis study. Diagnostics. 2020;10(9):704. doi:10.3390/diagnostics10090704
45. Lee HJ, Song IH, Park IA, et al. Differential expression of major histocompatibility complex class I in subtypes of breast cancer is associated with estrogen receptor and interferon signaling. Oncotarget. 2016;7(21):30119–30132. doi:10.18632/oncotarget.8798
46. Park HS, Cho U, Im SY, et al. Loss of Human leukocyte antigen class i expression is associated with poor prognosis in patients with advanced breast cancer. J Pathol Transl Med. 2019;53(2):75–85. doi:10.4132/jptm.2018.10.11
47. Ji Shin L, Nah Ihm K. Park min ho. abstract PD9-02: MHC class I and PD-L1 expression in triple-negative breast cancer subtypes: impact on T-cell infiltration and clinical outcome. Cancer Res. 2023;83(5_Supplement):PD9–02. doi:10.1158/1538-7445.SABCS22-PD9-02
48. Sabbatino F, Villani V, Yearley JH, et al. PD-L1 and HLA Class I antigen expression and clinical course of the disease in intrahepatic cholangiocarcinoma. Clin Cancer Res. 2016;22(2):470–478. doi:10.1158/1078-0432.CCR-15-0715
49. Kim H, Chung JH. PD-L1 testing in non-small cell lung cancer: past, present, and future. J Pathol Transl Med. 2019;53(4):199–206. doi:10.4132/jptm.2019.04.24
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.