Back to Journals » Open Access Emergency Medicine » Volume 14
Program of Uncontrolled Donation After Circulatory Death as Potential Solution to the Shortage of Organs: A Canadian Single-Center Retrospective Cohort Study
Authors D'Aragon F ![]() , Lachance O, Lafleur V, Ortega-Deballon I, Masse MH, Trepanier G
, Lachance O, Lafleur V, Ortega-Deballon I, Masse MH, Trepanier G ![]() , Lamarche D, Battista MC
, Lamarche D, Battista MC
Received 29 March 2022
Accepted for publication 3 June 2022
Published 5 August 2022 Volume 2022:14 Pages 413—420
DOI https://doi.org/10.2147/OAEM.S361930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Frederick D’Aragon,1,2 Olivier Lachance,1 Vincent Lafleur,1 Ivan Ortega-Deballon,3,4 Marie-Helene Masse,5 Gabrielle Trepanier,6 Daphnee Lamarche,1 Marie-Claude Battista5
1Department of Anesthesiology, Faculty of Medicine and Health Sciences Université de Sherbrooke, Sherbrooke, Quebec, Canada; 2Centre de recherche du Centre hospitalier universitaire de Sherbrooke, Sherbrooke, Quebec, Canada; 3Nursing Department, Faculty of Medicine and Health Sciences, Universidad de Alcalá, Madrid, Spain; 4Helicopter & Nursing Care Unit, Emergency Medical Service SUMMA 112, Madrid, Spain; 5Department of Medicine, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, Quebec, Canada; 6Department of Family Medicine and Emergency, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, Quebec, Canada
Correspondence: Frederick D’Aragon, 3001 12e Avenue N, Sherbrooke, PQ, J1H 5N4, Canada, Tel +1 819 821-8000 ext. 70103, Email Frederick.D’[email protected]
Purpose: Worldwide, the number of patients waiting for organ transplantation exceeds the number of organs available. Program for uncontrolled donation after circulatory death (uDCD) implemented in Europe has resulted in a 10– 15% expansion of the donor pool. We aimed to describe the number of patients eligible for an uDCD program in a regional tertiary care center.
Methods: We conducted a retrospective cohort study in a Canadian tertiary academic center located in a rural area including all adults who received cardiopulmonary resuscitation in 2016 and died in the emergency department (ED) or during their hospitalization. The primary outcome was the number of patients eligible for uDCD defined as aged between 18 and 60 years old whose collapse was witnessed and where the time between cardiac arrest to cardiopulmonary resuscitation and ED arrival was, respectively, less than 30 and 120 minutes. As a secondary outcome, we determined the number of patients eligible for controlled donation after circulatory death.
Results: Of the 130 patients included, 84 did not return to spontaneous circulation. We identified 15 potential uDCD candidates, with a mean age of 46.6 (95% Confidence Interval [CI] 41.3 to 52) years. Twelve had an out-of-hospital cardiac arrest with a mean time between collapse and arrival to the ED of 43.2 (29.8 to 56.6) minutes. Among the 46 patients who died after a return of spontaneous circulation, 10 (21.7%) were eligible for organ donation after circulatory death.
Conclusion: Implementing an uDCD program in a tertiary hospital covering a rural area could increase the number of donors.
Keywords: tissue and organ procurement, out-of-hospital cardiac arrest, donor selection, death, uncontrolled donation after circulatory death
Background
Organ transplantation saves lives and improves the quality of life.1 Although transplantation has become the definitive treatment for patients suffering from end-stage organ failure, demand still exceeds the supply.2 Of the 4351 Canadians waiting for a transplant in 2018, 223 died, and 420 were removed from the waitlist due to worsened health conditions.3 As the demand for organs increases, supply constantly falls short highlighting the need to increase organ procurement especially when patients are dying during these prolonged wait times. In 2019, Canada ranked 17th for the deceased organ donation rate with 20.6 donors per million population.2
In Canada, 71% of the organs transplanted are obtained from neurologically deceased donors.4 However, due to considerable ameliorations to prevent neurological incidents (eg, seat belt, helmet), and improve neurocritical care and decompressive craniotomy, the pool of neurologically deceased donors has greatly decreased.5 Moreover, anoxic brain injury has surpassed traumatic brain injury as the leading cause of death of donors, consequently, decreasing the quality of organs to be recovered.5,6 Accordingly, Canadians are now facing a shortage of eligible organs for transplantation.
Organ donation after circulatory death (DCD) seeks to recover organs after the cessation of respiratory and circulatory functions.7 Controlled DCD (cDCD) occurs in the intensive care unit following planned withdrawal of life-sustaining therapy. Uncontrolled donation after circulatory death (uDCD) refers to organ retrieval after an unexpected cardiac arrest with unsuccessful resuscitation and is initiated most frequently after an out-of-hospital cardiac arrest.
As the world leader in organ donations, Spain created its first uncontrolled donation after circulatory death program in 19868 and has reported a 12.1% increase in donors.9 Other European countries have also successfully implemented uncontrolled donation programs and reported a 10–15% increase within the organ pool.10,11 As cardiac disease represents the second most common cause of death with 53,134 deaths annually in Canada,12 these patients represent a substantial reservoir of potential donors. However, currently, in Canada, uDCD is not commonly practiced for legal reasons (eg, presumed consent), and variability within the policies of transplant programs.13 No prior study has investigated yet the potential pool of donors associated with an uDCD program in a Canadian location. Moreover, most studies outside of Canada focused on urban centers with a high-density population.
The primary objective of this study was to assess the number of potential donors eligible for a program of uDCD in a rural tertiary care center. Secondary objectives were to compare in versus out-of-hospital cardiac arrest with regard to eligible donors to a program of uDCD and to determine among a population of patients with cardiac arrest the number of donors after cDCD.
Methods
Study Design, Period and Setting
This descriptive observational retrospective single-center cohort study took place between January 1st and December 31st, 2016. The study was conducted at the Centre Intégré Universitaire de Santé et de Services Sociaux de l’Estrie – Centre hospitalier universitaire de Sherbrooke (CIUSSS de l’Estrie-CHUS) located in the Province of Québec in Canada. This tertiary academic center is an organ-procurement center, a level I regional trauma center and a referral center for interventional cardiology. This center covers a population of 500,000 individuals over a rural area of13000km2. In 2016, our center had 14 neurologically deceased organ donors. The Research Ethics Board of the CIUSSS de l’Estrie-CHUS approved this study (#2016-1416).
Study Population
All consecutive medical charts were reviewed for eligibility by two physicians. We included all patients who had health-care providers perform cardiopulmonary resuscitation, and who subsequently died in the emergency department or during their hospitalization. We excluded patients under 18 years old due to unique technical considerations related to organ donation and organ perfusion by ECMO in this population. Patients were excluded if at least one eligibility criteria for a uDCD program was missing.
Definition of the Potential Organ Donors
Based on validated international criteria, patients were considered as potential candidates for a uDCD program if 1) they were between 18 and 60 years of age, 2) they experienced a witnessed cardiac arrest, 3) their time between cardiac arrest and paramedic arrival was less than 30 minutes, and 4) their time between cardiac arrest and hospital arrival was less than 120 minutes.14–16
Patients were deemed potential donors after controlled circulatory death if they 1) had experienced a return to spontaneous circulation, 2) were intubated and on mechanical ventilation, 3) were aged between 18 and 70 years old, 4) had a neurological examination inconsistent with neurological death, and 5) withdrawal of life-sustaining therapy was anticipated as reported in hospital records.17,18
Patients’ eligibility for either program was abrogated if they presented signs of intravenous drug abuse, neoplasia or an active reported infection.
Data Collection
Age, sex, organ-donor registration number, and premorbid conditions (ie, infectious disease, drug abuse, and chronic comorbidities) were collected from hospital records. For each episode of cardiopulmonary resuscitation, etiology, time and date of the arrest, time of cardiopulmonary resuscitation (CPR) initiation and its duration, initial rhythm, and the presence of witnesses were collected. For out-of-hospital cardiac arrest, we recorded the emergency medical service time of notification and time of arrival to the hospital. Time to CPR was defined by the time of collapse reported by a witness and the initiation of CPR recorded on the emergency medical records. For potential cDCD, we collected the legal time, date and cause of death. In this study, time of death was defined as the time reported on the death certificate. If a withdrawal of life support occurred, data relevant to the organ donation process (eg, notification to the organ procurement organization, approach for organ donation) were obtained. A case report form and a corresponding instruction manual were designed and tested prior to launching the study. All investigators collected data from enrolled patients. The first ten charts were collected in parallel to assess inter-rater reliability. Data collection was only launched after a kappa of at least 0.70 for the items related to our primary outcome was reached.
Statistical Analysis
We performed descriptive analyses and reported continuous data as means (95% confidence interval [CI]) or medians (interquartile range [IQR]) as appropriate and dichotomous data as proportions. We used Fisher's exact test (for fewer than 5 counts) or Chi-square test to compare dichotomous variables and Student’s T-test or Mann–Whitney test for continuous variables. We determined the normality of the distribution with a Shapiro–Wilk test. We considered a two-sided p-value of less than 5% as statistically significant. We conducted all analyses using SPSS (version 24.0). Patients were not included in the analysis when data required to determine their eligibility for organ donation after circulatory death were missing.
Results
Patients and Cardiac Arrest Characteristics
From January 1st to December 31st, 2016, 1111 patients died at the CIUSSS de l’Estrie-CHUS, and 178 fulfilled the study eligibility criteria. We excluded 48 patients due to incomplete medical records and thus included 130 patients in our analyses (Figure 1). The mean (95% CI) age was 68.1 (65.5 to 70.6) years old, 82 (63.1%) were males and 58 (44.6%) were diagnosed with coronary artery disease (Table 1).
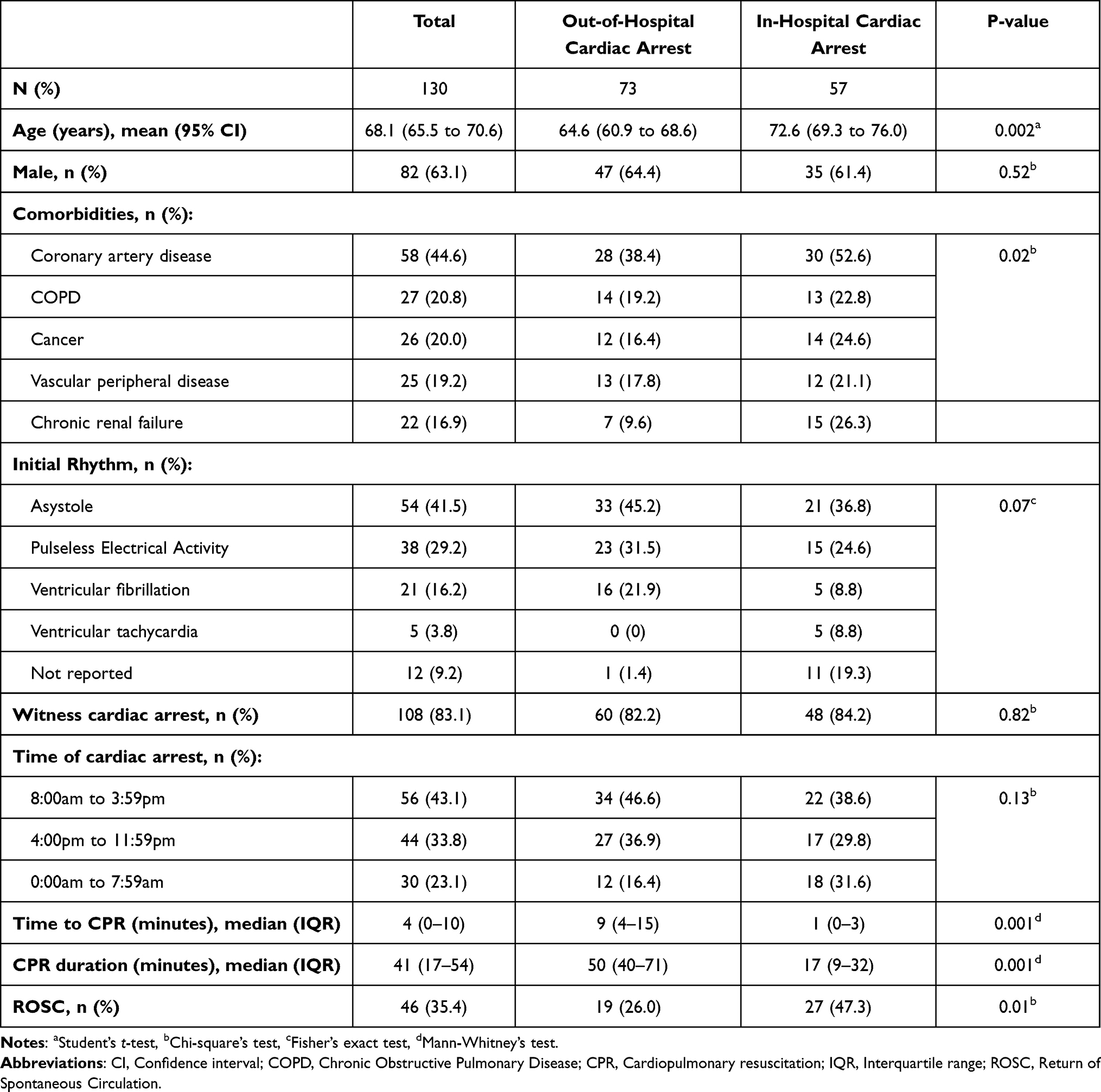 |
Table 1 Baseline Characteristics |
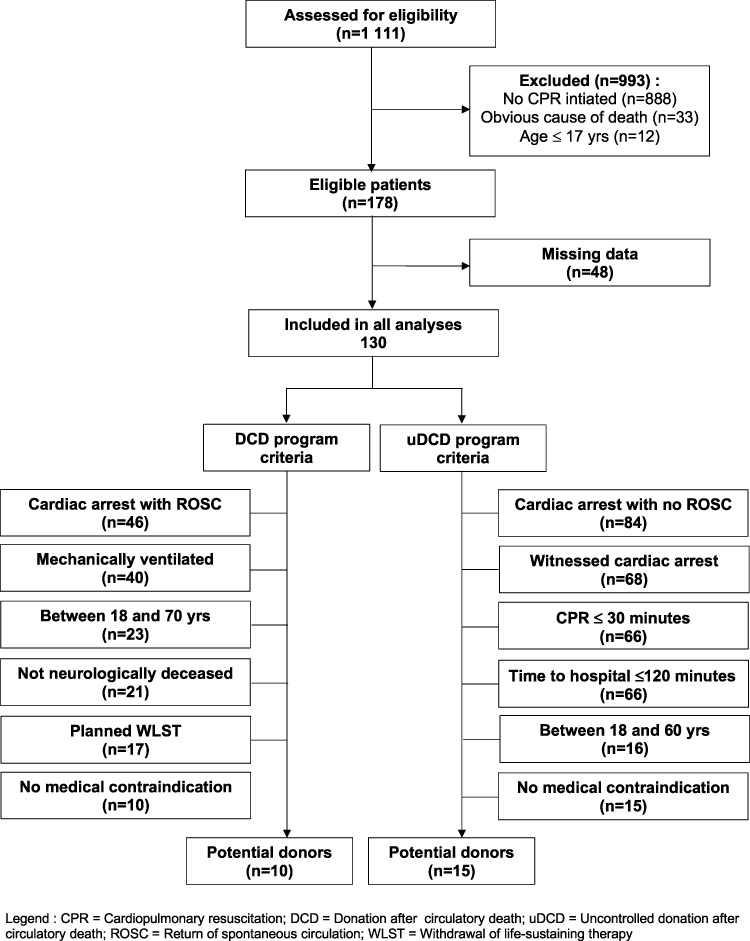 |
Figure 1 Patient flow diagram. Abbreviations: CPR, Cardiopulmonary resuscitation; DCD, Donation after circulatory death; uDCD, Uncontrolled donation after circulatory death; ROSC, Return of spontaneous circulation; WLST, Withdrawal of life-sustaining therapy. |
Of the 130 included patients, 84 (64.6%) did not return to spontaneous circulation and the remaining 46 (35.4%) patients with a return to spontaneous circulation.
Among the 73 patients who experienced out-of-hospital cardiac arrests, 60 (82.2%) of these had a witness. The median (IQR) time from collapse to CPR was 4 (0 to 10) minutes and the mean (95% CI) time from CPR initiation to arrival at the hospital was 40 (31.3 to 48.3) minutes. Fifty-six (76.7%) patients died at the emergency department. Compared to patients who suffered in-hospital cardiac arrest, patients who had out-of-hospital cardiac arrest were younger and had less chronic renal failure incidence (Table 1). Return to spontaneous circulation was less frequent in patients with out-of-hospital cardiac arrest (out-of-hospital cardiac arrest: 19/73; 26% vs in-hospital cardiac arrest 27/57; 47.3%, p = 0.012).
Potential Contribution to Organ Donation
Of the 84 patients without a return to spontaneous circulation, 15 (17.9%) met the donor eligibility criteria for the uDCD program (Figure 1). Their mean (95% CI) age was 46.6 (41.3 to 52) years old, 11 (11/15; 68.8%) were male and three (3/15; 20%) were known for coronary artery disease. Among these 15 potential donors, 12 had an out-of-hospital cardiac arrest and the median (IQR) time between patient’s collapse and CPR was 14.0 (2.3 to 16.0) minutes, the mean (95% CI) time between collapse and arrival at the emergency department was 43.2 (29.8 to 56.6) minutes and most cardiac arrest occurred between 8:00 am and 3:59 pm. For out-of-hospital cardiac arrest patients, the time and duration of CPR were comparable between patients and potential candidates for the uDCD program (Supplementary Table 1).
Among the 46 patients with a return to spontaneous circulation, 10 were considered potential donors for cDCD (Figure 1). They were all identified and referred to the organ procurement organization, but none became donors (family declined to consent to organ donation [n = 4], patient not medically suitable by the organ procurement organization [n = 3], not reported [n = 3]).
Discussion
Our study was performed in a cohort of patients who died following a cardiac arrest in a tertiary hospital center in Canada. This study aimed to determine the number of patients who would have been eligible donors through uncontrolled donation after circulatory death (uDCD) program if this program was implemented in Canada. We considered eligible, patients who had experienced cardiac arrest, with a time to CPR under 30 minutes, an absence of neoplasia, drug abuse and concomitant active infection. Out of 1111 cumulative deaths, 130 had resuscitative measures and were included in this study. Fifteen would have been eligible donors to a uDCD program. Since there is presently no official program for uDCD in Canada, our results can be used to estimate the expansion of the pool of potential donors to ultimately help reduce the transplant waiting list.
With regard to out-of-hospital cardiac arrests, the median time from arrest to the initiation of CPR was very short and comparable to other Canadian locations.19 A delay in the initiation of CPR longer than 30 minutes is an independent factor associated with poor graft function in the recipient.10,20 Hence, most uDCD protocols recommend the initiation of CPR within 15 to 30 minutes after cardiac arrest.14,21,22 Even though our center covers rural areas, our mean time from CPR initiation to arrival at the hospital was 40.6 minutes. This result is comparable to delays seen in urban centers with an extracorporeal cardiopulmonary resuscitation (ECPR) program.23 Equally important, the majority of cardiac arrest events occurred during the day. Therefore, our data show that the time reported from cardiac arrest to hospital and the timing of cardiac arrest could facilitate the implementation of a uDCD program in a region similar to ours.
Several European countries have implemented a program of uDCD in urban areas (eg, Madrid, Paris) which was associated with a 10% to 20% increase in deceased donors.21 However, in the United States of America, previous experience with an uDCD program has reported conflicting results. Indeed, after one year, the uDCD program in New York City had no patients who proceed to organ recovery after an out-of-hospital cardiac arrest due to breaches in the protocol, and confusion in determining the clinical eligibility.24 In contrast, a recent Canadian multidisciplinary group published results of a project assessing the feasibility of a lung uDCD program.25 Among the 44 eligible potential donors, five had lungs recovered and transplanted and none of the recipients developed primary graft dysfunction at 72 hours. Therefore, this first Canadian experience conducted in the emergency department demonstrates the feasibility of successfully implementing such a program.
Besides this single centre pilot project, no permanent program currently exists in Canada. This could be attributed to the ethical debate between saving the life of the patient versus preserving the organs for transplantation.26 This paradigm is fueled by the fact that ECPR and extracorporeal interval support until organ retrieval (EISOR) in uDCD programs used ECMO system.27 Recognizing this conflict, a multidisciplinary group of experts and researchers was assembled by the Canadian Blood Service in 2015 to elucidate this issue. They concluded that ECMO should be used with the primary intention of saving lives but if resuscitation failed, then organ donation after controlled circulatory should be considered.28
Our study report data from a single university hospital center in Canada. Whether these results can be generalized to other hospital is unknown and need to be further investigated. The potential number of donors eligible for uDCD reported in this study represents the most optimistic scenario. Indeed, we did not take into consideration potential limitations such as missed identification of potential donor, organ donation consent rate, an exclusion for judicial reasons, and logistical obstacles, which could increase the risk of selection bias. The retrospective data collection limited our ability to collect comprehensive data on all patients. For example, at least one variable from the eligibility criteria for uncontrolled donation after circulatory death program was missing in 48 patients. Moreover, the time to CPR was based on the time recorded by a witness on the emergency medical service which could be potentially incorrect. The modest sample size of this study influences the power of these analyses and could have led to spurious findings. These limitations will be addressed in a larger prospective multicentre observational study.
Conclusion
This study highlights that uncontrolled donation after circulatory death program held the potential to increase the reservoir of available organs for transplantation in regional centers. If such a program was to be introduced, the majority of donors would have come from out-of-hospital cardiac arrest thus highlighting the crucial contribution of the emergency department to expand donor pool. The findings of this study support the investigation of the implementation of a uDCD program in Canada on a larger scale.
Abbreviations
CIUSSS de l’Estrie-CHUS, Centre Intégré Universitaire de Santé et de Services Sociaux de l’Estrie – Centre hospitalier universitaire de Sherbrooke; CPR, Cardiopulmonary Resuscitation; DCD, Donation after Circulatory Death; cDCD, controlled Donation after Circulatory Death; uDCD, uncontrolled Donation after Circulatory Death; ECMO, Extra-corporeal membrane oxygenator; ECPR, Extracorporeal Cardiopulmonary Resuscitation; EISOR, Extracorporeal Interval Support until Organ Retrieval; SD, Standard Deviation; IQR, Interquartile range.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study complies with the Declaration of Helsinki. The Research Ethics Board of the CIUSSS de l’Estrie-CHUS approved this study (#2016-1416). Waiver of research consent from individual participants was obtained from REB given the retrospective design and minimal risk related to the study (ie, data collection).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by the Fonds de Recherche du Québec-Santé.
Disclosure
The authors declare no conflicts of interest and have no competing interests.
References
1. World Health Organization. Human organ transplantation [Internet]; 2004. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA57/A57_R18-en.pdf.
2. Donation and Transplantation Institute. International registry in organ donation and transplantation [Internet]; 2020. Available from: https://www.irodat.org/.
3. Canadian Institute of Health Information. Canadian organ replacement register: CORR annual statistics. [Internet]; 2018 Available from: https://www.cihi.ca/en/organ-replacement-in-canada-corr-annual-statistics-2018.
4. Kramer AH, Zygun DA, Doig CJ, Zuege DJ. Incidence of neurologic death among patients with brain injury: a cohort study in a Canadian health region. CMAJ. 2013;185(18):E838–E845. doi:10.1503/cmaj.130271
5. Kramer AH, Baht R, Doig CJ. Time trends in organ donation after neurologic determination of death: a cohort study. CMAJ Open. 2017;5(1):E19–E27. doi:10.9778/cmajo.20160093
6. D’Aragon F, Lamontagne F, Cook D, et al. Variability in deceased donor care in Canada: a report of the Canada-DONATE cohort study. Can J Anaesth. 2020;67(8):992–1004. doi:10.1007/s12630-020-01692-7
7. Thuong M, Ruiz A, Evrard P, et al. New classification of donation after circulatory death donors definitions and terminology. Transpl Int. 2016;29(7):749–759. doi:10.1111/tri.12776
8. Sánchez-Fructuoso AI, Prats D, Torrente J, et al. Renal transplantation from non-heart beating donors: a promising alternative to enlarge the donor pool. J Am Soc Nephrol. 2000;11(2):350–358. doi:10.1681/ASN.V112350
9. Organizacion Nacional de Trasplantes (ONT). Actividad de Donacion Y Trasplante [Internet]; 2019. Available from: http://www.ont.es/infesp/Memorias/ACTIVIDAD%20DE%20DONACI%C3%93N%20Y%20TRASPLANTE%20ESPA%C3%91A%202019.pdf.
10. Smith M, Dominguez-Gil B, Greer DM, Manara AR, Souter MJ. Organ donation after circulatory death: current status and future potential. Intensive Care Med. 2019;45(3):310–321. doi:10.1007/s00134-019-05533-0
11. Choudhury RA, Prins K, Moore HB, Yoeli D, Kam A, Nydam TL. Uncontrolled deceased cardiac donation: an unutilized source for organ transplantation in the United States. Clin Transplant. 2019;33(3):e13474. doi:10.1111/ctr.13474
12. Statistics Canada. Leading causes of death, total population, by age group [Internet]; 2020. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401.
13. Bernat JL, Bleck TP, Blosser SA, et al. Circulatory death determination in uncontrolled organ donors: a panel viewpoint. Ann Emerg Med. 2014;63(4):384–390. doi:10.1016/j.annemergmed.2013.05.018
14. Ortega-Deballon I, Hornby L, Shemie SD. Protocols for uncontrolled donation after circulatory death: a systematic review of international guidelines, practices and transplant outcomes. Crit Care. 2015;24(19):268. doi:10.1186/s13054-015-0985-7
15. Grunau B, Hornby L, Singal RK, et al. Extracorporeal cardiopulmonary resuscitation for refractory out-of-hospital cardiac arrest: the state of the evidence and framework for application. Can J Cardiol. 2018;34(2):146–155. doi:10.1016/j.cjca.2017.08.015
16. Ortega-Deballon I, Hornby L, Shemie SD, Bhanji F, Guadagno E. Extracorporeal resuscitation for refractory out-of-hospital cardiac arrest in adults: a systematic review of international practices and outcomes. Resuscitation. 2016;101:12–20. doi:10.1016/j.resuscitation.2016.01.018
17. Lewis J, Peltier J, Nelson H, et al. Development of the University of Wisconsin donation after cardiac death evaluation tool. Prog Transplant. 2003;13(4):265–273. doi:10.1177/152692480301300405
18. Domínguez-Gil B, Delmonico FL, Shaheen FAM, et al. The critical pathway for deceased donation: reportable uniformity in the approach to deceased donation. Transpl Int. 2011;24(4):373–378. doi:10.1111/j.1432-2277.2011.01243.x
19. Grunau B, Scheuermeyer FX, Stub D, et al. Potential candidates for a structured Canadian ECPR program for out-of-hospital cardiac arrest. CJEM. 2016;18(6):453–460. doi:10.1017/cem.2016.8
20. Peris A, Fulceri GE, Lazzeri C, et al. Delayed graft function and perfusion parameters of kidneys from uncontrolled donors after circulatory death. Perfusion. 2021;36(3):299–304. doi:10.1177/0267659120938928
21. Coll E, Miñambres E, Sánchez-Fructuoso A, Fondevila C, Campo-Cañaveral de la Cruz JL, Domínguez-Gil B. Uncontrolled donation after circulatory death: a unique opportunity. Transplantation. 2020;104(8):1542–1552. doi:10.1097/TP.0000000000003139
22. Af Geijerstam P, Forsberg S, Claesson A, et al. Potential organ donors after out-of-hospital cardiac arrest during a ten-year period in Stockholm, Sweden. Resuscitation. 2019;137:215–220. doi:10.1016/j.resuscitation.2019.01.001
23. Bednarczyk JM, White CW, Ducas RA, et al. Resuscitative extracorporeal membrane oxygenation for in hospital cardiac arrest: a Canadian observational experience. Resuscitation. 2014;85(12):1713–1719. doi:10.1016/j.resuscitation.2014.09.026
24. Wall SP, Kaufman BJ, Williams N, et al. Lesson from the new york city out-of-hospital uncontrolled donation after circulatory determination of death program. Ann Emerg Med. 2016;67(4):
25. Healey A, Watanabe Y, Mills C, et al. Initial lung transplantation experience with uncontrolled donation after cardiac death in North America. Am J Transplant. 2020;20(6):1574–1581. doi:10.1111/ajt.15795
26. Ortega-Deballon I, Uncontrolled R-AD. DCD: when should we stop trying to save the patient and focus on saving the organs? Hastings Cent Rep. 2018;48(Suppl 4):S33–S35. doi:10.1002/hast.950
27. Conrad SA, Broman LM, Taccone FS, et al. The extracorporeal life support organization Maastricht treaty for nomenclature in extracorporeal life support. a position paper of the extracorporeal life support organization. Am J Respir Crit Care Med. 2018;198(4):447–451. doi:10.1164/rccm.201710-2130CP
28. Brooks SC, Shemie SD, Torrance S, et al. Barriers and opportunities related to extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest in Canada: a report from the first meeting of the Canadian ECPR research working group. CJEM. 2018;20(4):507–517. doi:10.1017/cem.2017.429
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.