Back to Journals » Journal of Inflammation Research » Volume 18
Prognostic Values of the Systemic Immune Inflammation Index and Ferritin Level Combined with Pathological Indicators for the Patients with Colon Cancer After Radical Resection
Authors Wu Y, Wang W, Ye B, Zhu L
Received 22 June 2025
Accepted for publication 30 September 2025
Published 21 October 2025 Volume 2025:18 Pages 14503—14513
DOI https://doi.org/10.2147/JIR.S548834
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Junhao Wang
Yanmin Wu,1,* Wenyuan Wang,1,* Bing Ye,1,* Lixia Zhu2
1Digestive Disease Treatment Center, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China; 2Department of Gastrointestinal Surgery, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi Medical Center, Nanjing Medical University, Wuxi People’s Hospital, Wuxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lixia Zhu, Department of Gastrointestinal Surgery, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi Medical Center, Nanjing Medical University, Wuxi People’s Hospital, Wuxi, People’s Republic of China, Email [email protected]
Background: The systemic immune-inflammation index (SII) has become a new inflammatory biomarker in recent years. However, ferritin, as a readily measurable marker, is elevated in cancer patients. Therefore, in this study, we determined the predictive value of SII combined with ferritin (FS) and the pathological features associated with the prognosis of patients with colon cancer after radical resection.
Methods: Univariate and multivariate Cox regression analyses were performed to analyze the independent factors affecting the prognosis of patients with colon cancer. Kaplan-Meier survival curves and receiver operating characteristic (ROC) curves were plotted to evaluate the predictive efficacy of the SII, F, and FS for the overall survival of patients with colon cancer after radical resection. A nomogram prediction model was constructed, and the consistency index (C-index) and calibration curve were used to evaluate the performance of the nomogram.
Results: The five-year overall survival rates of patients in the training set and validation set were 56.8% and 57.3%, respectively. The results of multivariate Cox regression analysis revealed that the FS grade (grade 2 vs grade 1: hazard ratio (HR) = 6.375, 95% CI = 2.725– 14.911; grade 3 vs grade 1: HR = 21.623, 95% CI = 9.897– 47.240); vascular cancer thrombus (HR = 1.706, 95% CI = 1.082– 2.689); nerve infiltration (HR = 1.634, 95% CI = 1.070– 2.495), etc. were independent influencing factors for overall survival after surgery (all P < 0.05). Kaplan-Meier survival curve analysis showed that the SII, ferritin level, and FS were independent influencing factors for overall survival after radical resection in patients with colon cancer (all P < 0.05).
Conclusion: Preoperative FS grading is an effective and practical method to predict the overall survival of patients with colon cancer after radical resection. Moreover, its combination with pathological indicators can achieve a better prediction effect.
Keywords: systemic immune-inflammation index, SII, ferritin, colon cancer, predictive model
Introduction
Colon cancer is the third most common type of malignant tumor, and along with lung cancer, prostate cancer, and breast cancer, it is considered to be the main cause of threats to human life and health.1 The recommended screening methods for defective DNA repair mechanisms include initial immunohistochemistry (IHC) testing and/or microsatellite instability (MSI) testing. However, simplifying the biological and technical heterogeneity of MSI testing into available data is somewhat challenging. Sola Adeleke et al2 reported a case of a patient with Lynch syndrome and metastatic colorectal carcinoma (mCRC) who had a false-negative result from the IHC test. The study suggested that immunohistochemical testing for mismatch repair mechanisms may yield different results for the same germline mutation, which might be due to somatic mutations. However, the incidence of colon cancer continues to increase, and the five-year survival rate is very low.2,3 From an epidemiological perspective, the authors should note that new favorable subsets of cancers of unknown primary (CUP) have recently emerged, including a colon-like CUP subtype. This newly recognized clinical entity is managed similarly to colon cancer and contributes to the observed rise in colon cancer incidence.4 A study5 reported that the survival rate of patients with colon cancer is not high, and the five-year survival rates of patients with stages II, III, and IV disease are 82%, 66%, and 10%, respectively, with an overall five-year survival rate <50%.6 These results indicate that colon cancer is an extremely serious malignant tumor threatening human life. Radical resection is the main clinical treatment for colon cancer. However, a study revealed that after five years of follow-up, 16% of patients with colon cancer experienced recurrence after surgery, including 11% of stage II patients and 29% of stage III patients.7 Another study revealed that the median recurrence times for patients with colon cancer after surgery were 14.0 months and 21.5 months, respectively.8 Even though older patients are more prone to severe postoperative complications, there is no consensus that age affects survival outcomes. The prognosis of older patients may be confounded by differences in stage at presentation, tumor site, preexisting comorbidities, and type of treatment received.
The systemic immune-inflammation index (SII) is a new inflammatory index calculated based on the counts of neutrophils, platelets, and lymphocytes in the peripheral blood. This index can reflect different inflammatory and immune pathways in the body and is widely used to predict the prognosis of patients with malignant tumors.9,10 Chen et al11 reported that the SII can be used to predict the survival of patients with colon cancer and serve as an independent predictor of disease-free survival. Previous studies have confirmed that ferritin is involved in the development of colon cancer and may be involved in the proliferation and metastasis of colon tumor cells.12,13 Demir et al14 found that ferritin is closely related to the prognosis of colon cancer patients, and high ferritin levels are negatively correlated with survival. Additionally, the TNM staging system for colon cancer is the most commonly used predictor of survival and recurrence. However, prognostic heterogeneity exists among patients with the same TNM stage.15 Biological markers (such as SII and ferritin) can supplement the deficiencies of TNM staging from the perspectives of inflammation, metabolism, and immunity, thereby providing more comprehensive prognostic information and improving the accuracy of risk stratification. Only a few studies have investigated the application of the joint appeal index to predict the survival rate after colon cancer surgery. SII reflects the overall inflammatory state. A high SII indicates a pro-tumor inflammatory response, which inhibits anti-tumor immunity and promotes metastasis. Ferritin is involved in iron metabolism and acute-phase response proteins. Heterometaporphyrin is associated with tumor progression, oxidative stress, and immunosuppressive tumor microenvironment (TME). The combination of these two may be beneficial for predicting the postoperative prognosis of patients with colon cancer. But the SII combined with ferritin and pathological indicators can improve the prognostic efficacy of postoperative colon cancer is not clear. Therefore, this study aims to explore the prognostic value of the systemic immune inflammation index (SII) combined with ferritin and pathological indicators for patients after radical resection of colon cancer, and to construct a nomogram model to complement the shortcomings of the traditional TNM staging in evaluating the biological behavior of tumors and host factors. This model, by integrating inflammatory status, iron metabolism abnormalities and pathological features, can more accurately identify patient groups with high recurrence risk, providing important guidance for clinical decision-making. At the same time, this model can serve as a dynamic monitoring tool to early alert for the risk of tumor recurrence and guide the timing of imaging reexamination. Moreover, this nomogram model can also help facilitate communication between doctors and patients through an intuitive visual approach, enabling patients to better understand their individualized recurrence risk and survival expectations, thereby formulating personalized follow-up plans and providing objective basis for patient stratification in clinical trials, ultimately achieving the precision and individualization of postoperative management for colon cancer.
Methods
Research Participants
Based on the previous research data, the overall 5-year survival rate of the patients was 50%, with HR = 2, α = 0.05 and β = 0.1. The sample size was calculated asn = [(Zα/2 + Zβ)2] / [p(1-p)(lnHR)2], which resulted in a sample size of 176 cases. Therefore, the clinical and pathological data of 227 colon cancer patients who underwent radical surgery for colon cancer at The Affiliated Wuxi People’s Hospital of Nanjing Medical University from July 1, 2017, to July 1, 2019, were collected as the training set. Similarly, the clinical and pathological data of 117 colon cancer patients who underwent radical surgery at Affiliated Hospital of Jiangnan University during the same period were collected and used as the validation set.
The inclusion criteria were as follows: (1) pathologically confirmed diagnosis of colon cancer; (2) TNM stage II–III; (3) complete clinical laboratory tests and pathological data; (4) no preoperative neoadjuvant radiotherapy or chemotherapy; (5) underwent radical R0 resection; and (6) postoperative treatment with oxaliplatin-based chemotherapy.
The exclusion criteria were as follows: (1) severe postoperative complications resulting in a survival time of less than 30 days; (2) recurrent cancer or concurrent colon cancer; (3) a history of other malignant tumors; (4) evidence or history of inflammatory disease infection that affects blood test results; (5) a history of psychiatric disorders or other severe internal medical conditions.
This study was approved by the Medical Ethics Committees of The Affiliated Wuxi People’s Hospital of Nanjing Medical University (KY24326, Approval date:2024.1.4). All patients provided signed informed consent. Our study complies with the Declaration of Helsinki.
General Information Questionnaire
The general and clinicopathological data of all patients were collected. General information included age, gender, medical history, and laboratory test results one week before surgery. Medical history included smoking history, drinking history, hypertension history, diabetes history, etc. The results of laboratory examination included carcinoembryonic antigen (CEA), carbohydrate antigen 199 (CA199), ferritin, platelets, neutrophils, lymphocytes, etc. The clinicopathological data included TNM classification, lesion location, the maximum diameter of the lesion, degree of tumor differentiation, pathological type, classification, vascular tumor thrombus, and nerve invasion.
Systemic Immune-Inflammation Indices
The system immune-inflammation index (SII) integrates three indicators, including neutrophils, lymphocytes, and platelets, which can more comprehensively reflect the inflammatory and immune status of the body. It is a new inflammatory biomarker. SII = platelet count (109/L) × neutrophil count (109/L)/lymphocyte count (109/L). The best cutoff values for the SII and ferritin (F) for predicting the overall survival (OS) of patients with colon cancer after radical resection were calculated using the X-Tile software. According to the best cutoff values of 687.7 and 195.7, the patients were divided into low-SII (SII ≤ 687.7) and high-SII (SII > 687.7) groups and low-ferritin (F ≤ 195.7) and high-ferritin (F > 195.7) groups. Low SII and low F were defined as Grade 1, while high SII and high F were defined as Grade 2. A low SII combined with low F was defined as FS grade 1, a high SII combined with high F was defined as FS grade 3, and all other combinations of SII and F were defined as FS grade 2.
Follow-Up
The patients were followed up once a month after surgery and then once every six months through telephone calls and outpatient review. The follow-up data included the results of routine blood and serum tumor marker analyses, abdominal ultrasound, and enhanced abdominal computed tomography; the follow-up was conducted on July 1, 2024. The endpoint of this study was OS, which was defined as the interval from radical resection to the last follow-up date or death.
Results
General Information and Clinicopathological Data
In total, 227 patients were included in the training set, and 117 were included in the validation set. The mean age of the training cohort was 75.19 ±6.50 years, and the median survival time (range) was 1889 (950, 2201) days. The mean age of the patients in the training set was 74.17 ±6.05 years, and the median survival time (range) was 1962 (983, 2258) days. The mean value of ferritin in the training set was 198.20 ±50.62 ng/mL, which included 119 Grade I patients and 108 Grade II patients. The mean value of the SII was 667.45 ±320.91, of which 136 were Grade I and 91 were Grade II. TNM stage II included 102 cases, while TNM stage III included 125 cases. There were 105 cases of FS grade I, 45 cases of FS grade II, and 77 cases of FS grade III. The average value of ferritin in the validation set was 208.12 ±49.29 ng/mL, with 52 cases in Grade I and 65 cases in Grade II. The average value of the SII was 676.35 ±219.49, with 64 cases in Grade I and 53 cases in Grade II, 56 cases in TNM Stage II and 61 cases in TNM Stage III, 43 cases in FS Grade I, 30 cases in Grade II, and 44 cases in Grade III. No significant differences were recorded in the general and pathological data between the training and validation sets (P ≥ 0.05) (Table 1).
 |
Table 1 Clinical Characteristics of Patients in Training Set and Validating Set |
Analysis of Factors Affecting OS in Colorectal Cancer Patients After Curative Resection
The training set was used to construct univariate and multifactorial Cox regression models. Univariate Cox regression analysis revealed that, compared to highly differentiated tumors, poorly differentiated tumors, hazard ratio (HR)= 24.932, 95% CI = 5.865–105.976; moderately differentiated tumors, HR = 6.235, 95% CI = 1.530–25.419; vascular cancer thrombi, HR = 5.252, 95% CI = 3.424–8.055; nerve infiltration, HR = 2.342, 95% CI = 1.553–3.532; and FS grade I and grade II tumors, HR = 6.218, 95% CI = 2.682–14.416; and grade III tumors, HR = 31.766, 95% CI = 15.041–67.088. The multivariate Cox regression results revealed the degree of tumor differentiation (moderately differentiated versus well-differentiated, HR = 4.413, 95% CI = 1.058–18.403; poorly differentiated versus well-differentiated, HR = 10.868, 95% CI = 2.496–47.318); vascular cancer thrombus, HR = 1.706, 95% CI = 1.082–2.689; nerve infiltration, HR = 1.634, 95% CI = 1.070–2.495; and FS grading (compared to Grade I, Grade II, HR = 6.375, 95% CI = 2.725–14.911; Grade III, HR = 21.623, 95% CI = 9.897–47.240) were all independent influencing factors for the OS of patients with colon cancer after radical resection (P < 0.05) (Table 2).
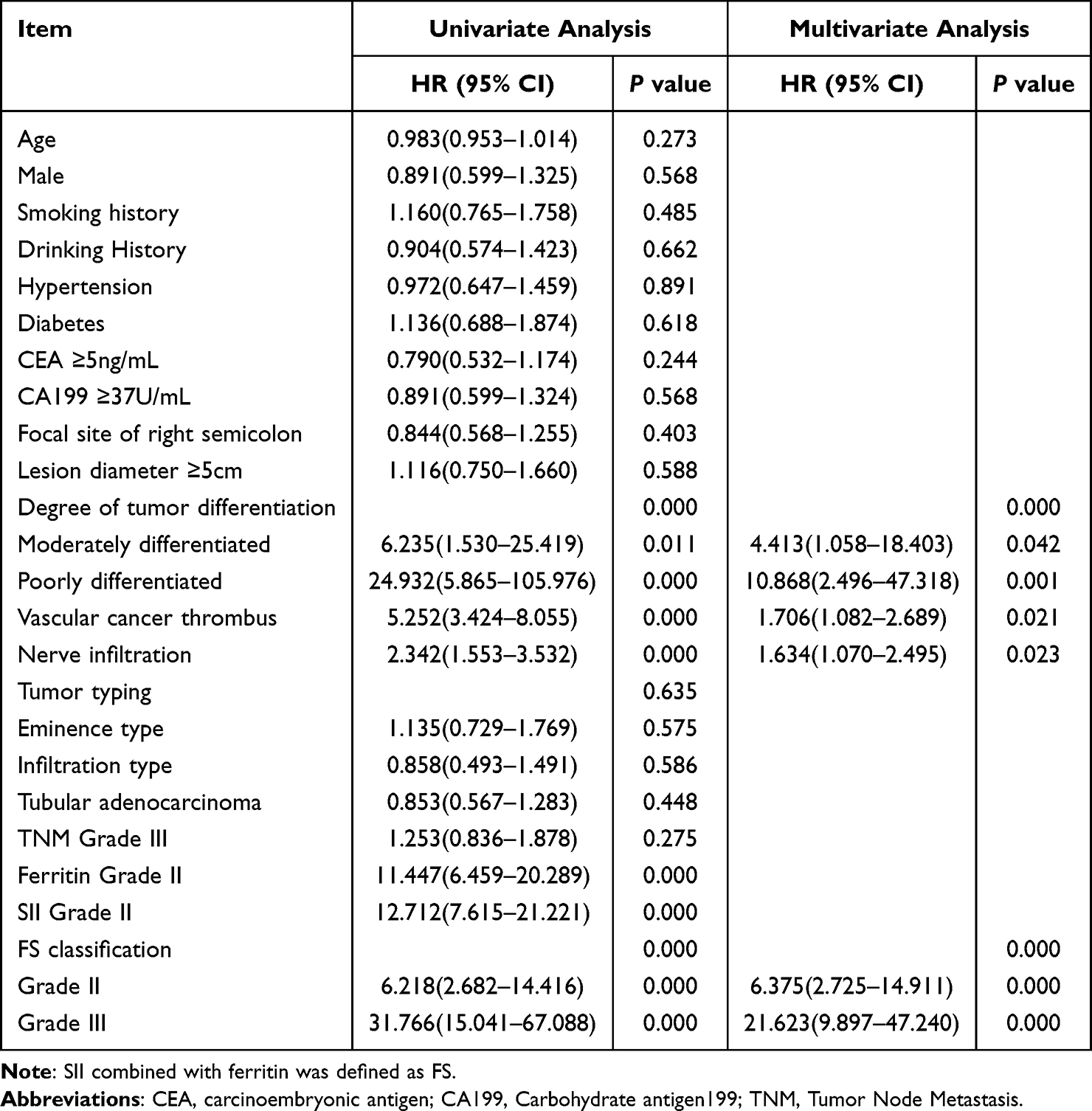 |
Table 2 Univariate and Multivariate Cox Regression Analysis of Patients |
As shown in Figure 1, the Kaplan-Meier survival curve analysis of the training set and verification set revealed that the five-year OS rates of patients in the training set and verification set were 56.8% and 57.3%, respectively. The survival rates of FS grades I, II, and III in the training set were 42.73%, 12.33%, and 1.76%, respectively. The survival rates of SII grades I and II were 51.54% and 5.29%, respectively. The survival rates of ferritin grades I and II were 46.26% and 10.57%, respectively. The survival rates of patients with FS grades I, II, and III were 34.19%, 17.09%, and 5.98%, respectively. The survival rates of patients with SII grades I and II were 47.86% and 9.41%, respectively. The survival rates of patients with ferritin grades I and II were 37.61% and 19.66%, respectively. There were significant differences among all groups (P < 0.05).
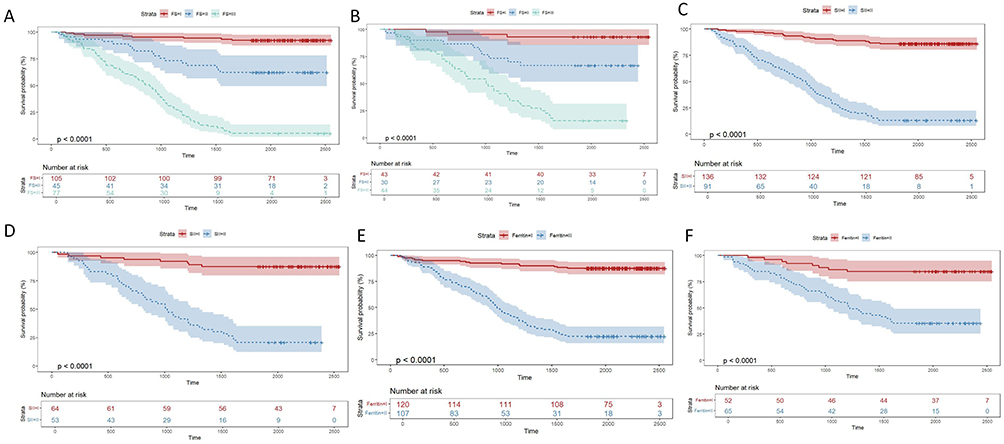 |
Figure 1 Kaplan-Meier survival curve of colon cancer patients after radical resection ((A, C, E) Training set; (B, D, F) Validating set). |
ROC Curve Analysis of the SII, Ferritin Level, and FS
ROC analysis revealed that the areas under the curve (AUCs) of the SII, F, and FS in the training set for predicting the survival status of patients after radical resection of colon cancer were 0.913 (95% CI = 0.876–0.950), 0.865 (95% CI = 0.815–0.916), and 0.939 (95% CI = 0.908–0.969), respectively. In the validation set, the AUCs of the SII, F, and FS for predicting the survival status of patients after radical resection of colon cancer were 0.900 (95% CI = 0.844–0.956), 0.810 (95% CI = 0.731–0.889), and 0.915 (95% CI = 0.863–0.966), respectively. The results showed that the predictive ability of FS was better than that of SII and F (Figure 2).
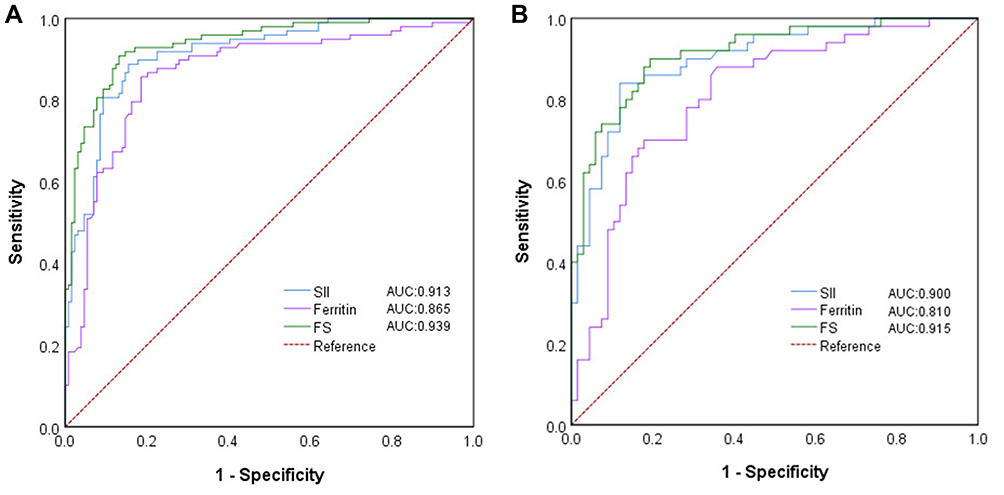 |
Figure 2 SII, ferritin, and FS combined to predict overall survival after radical resection in patients with colon cancer ((A) Training set; (B) Validating set). Abbreviation: SII, systemic immune-inflammation index. |
Construction and Validation of the Nomogram Model
The above independent influencing factors included tumor differentiation, vascular tumor thrombus, nerve invasion, and FS to construct a nomogram model (Figure 3). The consistency indices of the training set and the validation set based on the column line model were 0.850 (95% CI = 0.817–0.883) and 0.810 (95% CI = 0.757–0.862), respectively. The survival rate calibration curves of the training set and the validation set were close to the reference line, and the nomogram model had a good predictive ability in the training set and the validation set (Figure 4).
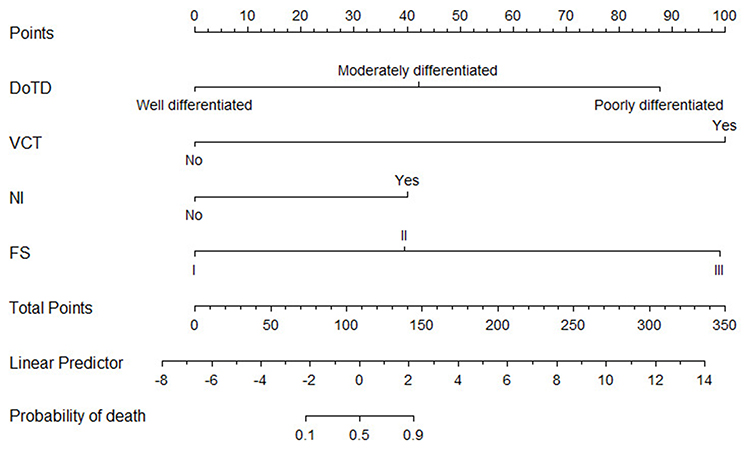 |
Figure 3 A nomogram model for predicting prognosis of colon cancer patients after radical resection. |
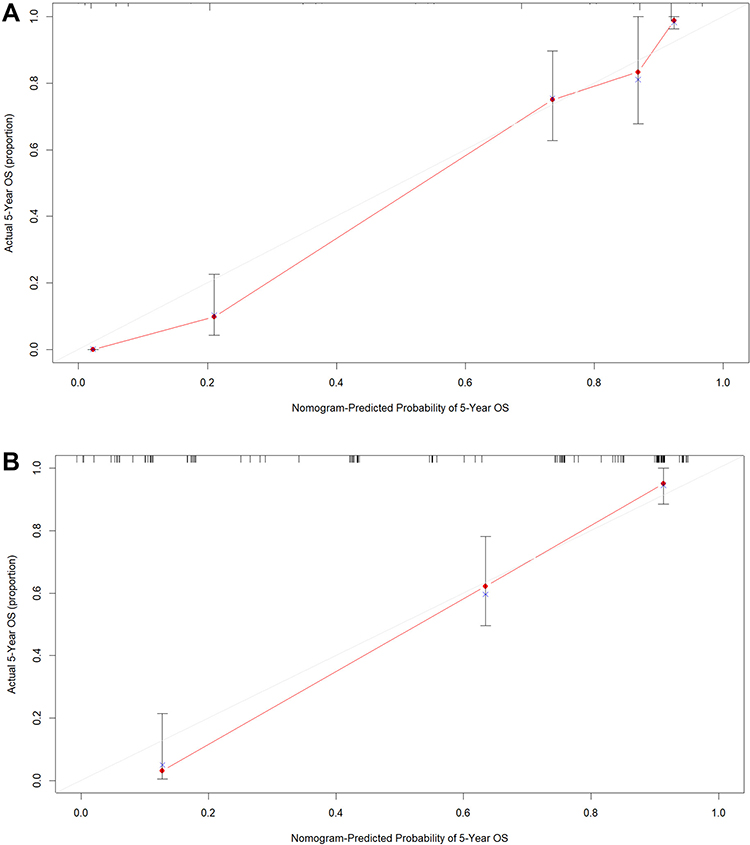 |
Figure 4 Calibration curve of survival rate of colon cancer patients predicted by the histogram model after radical surgery ((A) Training set; (B) Validating set). |
Discussion
The occurrence and development of cancer are closely related to the tumor immune and inflammatory microenvironments.16 In recent years, the SII has been widely used in the prognostic evaluation of patients with malignant tumors and has shown a good prognostic predictive value. Biological marker testing should be recommended as part of the standard screening for colon cancer.17 More and more evidence indicates that inflammation is the driving factor in the development of this disease. Therefore, many studies have investigated the predictive and prognostic roles of various blood-based inflammatory markers (including NLR, PLR18 and LMR19). Furthermore, among the several major genetic mutations in colon cancer, RAS mutations are associated with the aggressiveness of the tumor and the pathological response to chemotherapy. The presence of RAS mutations may indicate a poor prognosis.20 MiRNA (microRNA) has the functions of tumor suppressor genes and oncogenes.21 The diagnostic, prognostic and predictive significance of it is currently also being explored. For example, the SII can predict the prognosis of patients with malignant tumors, such as non-small cell lung cancer, gastric cancer, and hepatocellular carcinoma.22–24 The results of this study revealed that patients with an SII of 2 had shorter OS than those with an SII of 1. The SII, a new biomarker that integrates three indicators of neutrophils, lymphocytes, and platelets, can more comprehensively reflect the inflammatory and immune status of the body. Neutrophils are involved mainly in the immune response of the body, which involves swallowing and killing bacteria and defending against diseases.25 Additionally, studies have shown that newly diagnosed tumor patients often exhibit thrombocytosis, which can promote tumor growth and metastasis, enable tumor cells to escape killing by the immune system, and promote tumor angiogenesis, thus increasing the possibility of tumor growth and recurrence.26 Lymphocytes are cell lines with specific immune recognition functions in the body. They play important roles in immune processes, such as anti-infection and anti-tumor effects. Therefore, the number of lymphocytes in patients with tumors often decreases.27 Therefore, these findings may explain why patients with SII grade 2 colon cancer are more likely to have a poor prognosis after radical resection. Our results were similar to those of previous studies. Zhang et al28 confirmed that the preoperative SII can predict the disease-free survival (DFS) of patients with colon cancer undergoing radical surgery and is an independent influencing factor for the prognosis of patients with colon cancer after radical resection. The SII reflects the prognosis of patients with colon cancer undergoing radical surgery more accurately than other inflammatory markers.
Ferritin can better reflect the whole-body iron reserve, and it is often used as an index of iron metabolism homeostasis in clinical practice. Immunohistochemical staining for ferritin is often positive in colon cancer, and the intensity of ferritin expression is related to the degree of interstitial infiltration of mononuclear inflammatory cells.29 Other studies have shown that ferritin levels are elevated in most colon cancer patients. For example, in a study involving 94 colon cancer patients, Tingting et al30 reported that only about 14.9% of patients had hypoferritinemia. Recent studies have shown that ferritin can be used as an indicator of the poor prognosis of some malignant tumors. For example, a meta-analysis by Lin et al31 confirmed that elevated ferritin in patients with malignant biliary tract tumors often indicates a poor prognosis. Similarly, elevated ferritin was found to be associated with shorter OS in patients with colon cancer in our study; other researchers32 also confirmed this conclusion. The ferritin level is closely related to the prognosis of patients with stage II–III nonmetastatic and metastatic colon cancer. The specific mechanism related to the relationship between elevated ferritin and poor prognosis in colon cancer patients is unclear. However, there is some evidence. For example, studies have shown that iron plays an important role in cellular DNA synthesis and proliferation; thus, the demand for iron in hyperplastic tumor cells is often greater than that in normal cells.33 Additionally, ferritin is involved in pathophysiological processes such as immune regulation, angiogenesis, and the promotion of tumor cell proliferation.34
In this study, we merged the SII with ferritin to form FS and classified it into grades 1, 2, and 3 to assess the systemic immune status of colon cancer patients more comprehensively. Because FS is a joint index of the SII and ferritin, only FS was included in the multivariate Cox regression analysis, and the SII and ferritin levels were excluded. The lower the FS grade, the better the prognosis of colon cancer patients after radical resection. The results of the ROC analysis revealed that FS had better prognostic prediction ability in both the training and validation sets. Therefore, FS can be used as a combined index of the SII and ferritin rather than FS. Hence, only FS was included in the multivariate Cox regression analysis, as it is a more practical and reliable method to evaluate the prognosis of patients with colon cancer after radical resection. Additionally, multivariate Cox regression analysis revealed that tumor differentiation, vascular tumor thrombus, and nerve invasion were also independent influencing factors for the OS of patients with colon cancer after radical resection. The third level of the FS classification represents the highest risk, indicating that the prognosis of the patients is often worse. Such patients may require more intensive adjuvant therapy (for example, combined chemotherapy with immunomodulators), while lower levels can guide the downgrading of treatment to avoid unnecessary toxicity. Therefore, in this study, we established an effective and practical nomogram model for predicting prognosis based on FS, tumor differentiation, vascular tumor thrombus, and nerve invasion; the model had a good prognostic value and predictive ability.
To summarize, in this study, we investigated the significance of the SII combined with ferritin and pathological features in the prognostic evaluation of patients with colon cancer after radical resection. The AUC of the combination of the SII and ferritin for identifying the prognostic outcome of patients was greater than that of a single indicator, indicating that the combined application helps improve the accuracy of the assessment. The nomogram based on the SII, ferritin level, and pathological features also revealed that the model constructed in this study had a good predictive ability. At the first follow-up after the surgery, the clinical doctor can obtain a visualized individualized recurrence risk score (ranging from 0 to 100 points) and the corresponding risk stratification by inputting the patient’s pathological indicators, preoperative SII and ferritin values. This result will serve as an important basis for multidisciplinary consultation and guide the formulation of differentiated treatment plans. At the same time, the model can also correspond to differentiated follow-up strategies, ranging from the 6-month routine follow-up for the low-risk group to the monthly monitoring combined with ctDNA dynamic assessment for the high-risk group, contributing to the greatest improvement in the patient’s prognosis.
This study had several limitations. It included only patients with stage II and III colon cancer after radical resection; the included population was relatively limited, and the sample size was relatively small. Further studies with a larger sample size and external multi-center validations are needed to confirm the results. Additionally, the retrospective design increases the possibility of selection bias and unmeasured confounding factors in the study, which is also one of the limitations of this research.
Conclusion
Preoperative FS grading is an effective and practical method to predict the OS of patients with colon cancer after radical resection. Compared to the SII and ferritin alone, the FS grade has a better predictive value for the prognosis of patients. This model is applicable to Chinese patients with stage II–III colon cancer. The FS-based nomogram model can more accurately identify the high-risk population for postoperative recurrence of colon cancer, achieve early warning of tumor recurrence, and provide a scientific basis for the selection of imaging re-examination timing. This model significantly improves the efficiency of doctor-patient communication through an intuitive visual presentation, helping patients better understand their individualized risk level of recurrence and survival prognosis, and thus formulate targeted follow-up plans. At the same time, this model can also serve as an objective standard for stratifying clinical trial subjects, promoting the advancement of postoperative treatment for colon cancer towards precision and individualization.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Chen H, Luo J, Guo J. Development and validation of a five-immune gene prognostic risk model in colon cancer. BMC Cancer. 2020;20(1):395. doi:10.1186/s12885-020-06799-0
2. Adeleke S, Haslam A, Choy A, et al. Microsatellite instability testing in colorectal patients with Lynch syndrome: lessons learned from a case report and how to avoid such pitfalls. Per Med. 2022;19(4):277–286. doi:10.2217/pme-2021-0128
3. Xie F, Lu P, Chen Y, et al. Laparoscopic radical surgery for locally advanced T4 transverse colon cancer and prognostic factors analysis: evidence from multi-center databases. Medicine. 2023;102(48):e36242. doi:10.1097/MD.0000000000036242
4. Spurgeon L, Mitchell C, Cook N, et al. Cancer of unknown primary: the hunt for its elusive tissue-of-origin - is it time to call off the search? Br J Cancer. 2025;133(6):733–742. doi:10.1038/s41416-025-03073-7
5. Su Y, Tian X, Gao R, et al. Colon cancer diagnosis and staging classification based on machine learning and bioinformatics analysis. Comput Biol Med. 2022;145:105409. doi:10.1016/j.compbiomed.2022.105409
6. Mocan L. Laparoscopic surgery for the treatment of colon cancer: the new standard? Eur Rev Med Pharmacol Sci. 2021;25(12):4228–4235. doi:10.26355/eurrev_202106_26128
7. Osterman E, Glimelius B. Recurrence risk after up-to-date colon cancer staging, surgery, and pathology: analysis of the entire Swedish population. Dis Colon Rectum. 2018;61(9):1016–1025. doi:10.1097/DCR.0000000000001158
8. Sheng XH, Gao CF, Ji XQ, et al. Comparative study of recurrent colon cancer and recurrent rectal cancer after radical resection. Zhonghua wei chang wai ke za zhi. 2010;13(6):409–412.
9. Wang Q, Zhu D. The prognostic value of systemic immune-inflammation index (SII) in patients after radical operation for carcinoma of stomach in gastric cancer. J Gastrointest Oncol. 2019;10(5):965–978. doi:10.21037/jgo.2019.05.03
10. Ding P, Guo H, Sun C, et al. Combined systemic immune-inflammatory index (SII) and prognostic nutritional index (PNI) predicts chemotherapy response and prognosis in locally advanced gastric cancer patients receiving neoadjuvant chemotherapy with PD-1 antibody sintilimab and XELOX: a prospective study. BMC Gastroenterol. 2022;22(1):121. doi:10.1186/s12876-022-02199-9
11. Chen JH, Zhai ET, Yuan YJ, et al. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J Gastroenterol. 2017;23(34):6261–6272. doi:10.3748/wjg.v23.i34.6261
12. Cui Z, Li W, Wang Y, et al. M2 macrophage-derived exosomal ferritin heavy chain promotes colon cancer cell proliferation. Biol Trace Elem Res. 2023;201(8):3717–3728. doi:10.1007/s12011-022-03488-w
13. Prutki M, Poljak-Blazi M, Jakopovic M, et al. Altered iron metabolism, transferrin receptor 1 and ferritin in patients with colon cancer. Cancer Lett. 2006;238(2):188–196. doi:10.1016/j.canlet.2005.07.001
14. Demir H, Beypinar I, Urvay S, et al. Prognostic role of pre-operative serum ferritin level in stage 2 colon cancer. Eur Rev Med Pharmacol Sci. 2021;25(21):6473–6479. doi:10.26355/eurrev_202111_27091
15. Fan XJ, Wan XB, Fu XH, et al. Phosphorylated p38, a negative prognostic biomarker, complements TNM staging prognostication in colorectal cancer. Tumour Biol. 2014;35(10):10487–10495. doi:10.1007/s13277-014-2320-3
16. Rui R, Zhou L, He S. Cancer immunotherapies: advances and bottlenecks. Front Immunol. 2023;14:1212476. doi:10.3389/fimmu.2023.1212476
17. Uludag SS, Sanli AN, Zengin AK, Ozcelik MF. Systemic inflammatory biomarkers as surrogate markers for stage in colon cancer. Am Surg. 2022;88(6):1256–1262. doi:10.1177/0003134821995059
18. Ramesh SK, Swain SK, Munikrishnan V, Jameel JKA. Can the inflammatory cell ratio nlr and plr be used as a reliable marker in colon cancer? A prospective study. Euroasian J Hepatogastroenterol. 2023;13(2):61–65. doi:10.5005/jp-journals-10018-1399
19. Huang L, Hu Z, Luo R, et al. Predictive values of the selected inflammatory indexes in colon cancer. Cancer Control. 2022;29:10732748221091333. doi:10.1177/10732748221091333
20. Rodenhuis S. Ras and human tumors. Semin Cancer Biol. 1992;3(4):241–247.
21. Yang F, Bian Z, Xu P, Sun S, Huang Z. MicroRNA-204-5p: a pivotal tumor suppressor. Cancer Med. 2023;12(3):3185–3200. doi:10.1002/cam4.5077
22. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
23. Guo W, Cai S, Zhang F, et al. Systemic immune-inflammation index (SII) is useful to predict survival outcomes in patients with surgically resected non-small cell lung cancer. Thoracic Cancer. 2019;10(4):761–768. doi:10.1111/1759-7714.12995
24. Zhu Z, Cong X, Li R, et al. Preoperative Systemic Immune-Inflammation Index (SII) for predicting the survival of patients with stage I-III Gastric Cancer with a Signet-Ring Cell (SRC) component. Biomed Res Int. 2020;2020:5038217. doi:10.1155/2020/5038217
25. Sasaki K, Morioka D, Conci S, et al. The tumor burden score: a new “metro-ticket” prognostic tool for colorectal liver metastases based on tumor size and number of tumors. Ann Surg. 2018;267(1):132–141. doi:10.1097/SLA.0000000000002064
26. Tao DL, Tassi Yunga S, Williams CD, et al. Aspirin and antiplatelet treatments in cancer. Blood. 2021;137(23):3201–3211. doi:10.1182/blood.2019003977
27. Li Q, Chen C, Zhang J, et al. Prediction efficacy of prognostic nutritional index and albumin-bilirubin grade in patients with intrahepatic cholangiocarcinoma after radical resection: a multi-institutional analysis of 535 patients. Front Oncol. 2021;11:769696. doi:10.3389/fonc.2021.769696
28. Zhang L, Zhang Z, Guo H, et al. Systemic immune-inflammation index: a new indicator of predicting 1-, 2-and 3-year disease-free survival of patients with colon cancer. Adv Clin Exp Med. 2023;32(1):13–22. doi:10.17219/acem/152826
29. Hsu PI, Chow NH, Lin XZ, et al. Prognostic significance of ferritin expression in colorectal adenocarcinoma. Anticancer Res. 1995;15(3):1087–1093.
30. Tingting H, Di S, Xiaoping C, et al. High preoperative serum ferritin predicted poor prognosis in non-metastatic colorectal cancer. Saudi Med J. 2017;38(3):268–275. doi:10.15537/smj.2017.3.16110
31. Lin S, Fang Y, Lin Y, et al. Meta-analysis of the prognostic value of pretreatment serum ferritin in hepatobiliary and pancreas (HBP) cancers. BMJ open. 2021;11(5):e040801. doi:10.1136/bmjopen-2020-040801
32. Lee S, Song A, Eo W. Serum ferritin as a prognostic biomarker for survival in relapsed or refractory metastatic colorectal cancer. J Cancer. 2016;7(8):957–964. doi:10.7150/jca.14797
33. Surguladze N, Thompson KM, Beard JL, et al. Interactions and reactions of ferritin with DNA. J Biol Chem. 2004;279(15):14694–14702. doi:10.1074/jbc.M313348200
34. Alkhateeb AA, Connor JR. The significance of ferritin in cancer: anti-oxidation, inflammation and tumorigenesis. BBA. 2013;1836(2):245–254. doi:10.1016/j.bbcan.2013.07.002
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.