Back to Journals » OncoTargets and Therapy » Volume 9
Prognostic value of PD-L1 and PD-1 expression in pulmonary neuroendocrine tumors
Authors Fan Y, Ma K ![]() , Wang C, Ning J, Hu Y, Dong D, Dong X, Geng Q, Li E
, Wang C, Ning J, Hu Y, Dong D, Dong X, Geng Q, Li E ![]() , Wu Y
, Wu Y
Received 15 June 2016
Accepted for publication 31 August 2016
Published 6 October 2016 Volume 2016:9 Pages 6075—6082
DOI https://doi.org/10.2147/OTT.S115054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ingrid Espinoza
Yangwei Fan,1,* Ke Ma,1,* Chuying Wang,1 Jing Ning,1 Yuan Hu,1 Danfeng Dong,1 Xuyuan Dong,1 Qianqian Geng,2 Enxiao Li,1 Yinying Wu1
1Department of Medical Oncology, 2Department of Nuclear Medicine, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Purpose: Programmed death 1 (PD-1) receptor and its ligand, programmed death ligand-1 (PD-L1), play critical roles in the immune invasion of various tumors. This study aimed to explore the clinical significance of PD-L1/PD-1 expression in the progression of pulmonary neuroendocrine tumors (PNETs).
Methods: The expression of PD-L1 and PD-1 in 80 patients diagnosed with PNETs were investigated. Immunohistochemical analysis was performed on 80 formalin-fixed paraffin-embedded tissue specimens from PNETs and 20 corresponding cancer-adjacent tissue specimens.
Results: Tissues from PNETs had higher levels of PD-L1 (58.8%) and PD-1 (51.3%) compared to the cancer-adjacent tissues (25% and 20%, respectively). Meanwhile, PD-L1 expression was associated with PD-1 expression (P=0.007). PD-L1 expression was significantly associated with histological type (P=0.014) and tumor stage (P=0.014). Univariate analyses showed that the overall survival time of PNETs patients was significantly associated with PD-L1 expression in cancer cells (P=0.003), PD-1 expression in tumor-infiltrating lymphocytes (P=0.001), tumor node metastasis stage (P<0.05), and distant metastasis (P<0.001). Additionally, multivariate analysis revealed that PD-L1 expression, PD1 expression, and distant metastasis of PNETs were independently associated with survival time. Moreover, Kaplan–Meier survival curves analysis revealed that patients with negative PD-L1 and PD-1 expression had better prognoses.
Conclusion: Data suggested that PD-L1 and PD-1 can be useful prognostic biomarkers for survival and can pave the way toward new immunotherapy regimens against PNETs through targeting the PD-L1/PD-1 pathway.
Keywords: pulmonary neuroendocrine tumors, PD-L1, PD-1, prognosis
Introduction
Neuroendocrine tumors (NETs) are a diverse group of tumors originating from neuroendocrine cells. Given the wide distribution of the neuroendocrine cells throughout the body, NETs can develop in a variety of organs.
Pulmonary neuroendocrine tumors (PNETs) comprise various heterogeneous tumors, ranging from low-grade, well-differentiated typical carcinoid tumors to intermediate-grade atypical carcinoid tumors and poorly differentiated, highly malignant large-cell neuroendocrine carcinoma (LCNEC) and small cell lung cancer (SCLC).1
The prognosis and the therapy for patients with these tumors depend on the specific subtypes of PNETs. Surgical excision is the optimal choice in the case of chemoresistant carcinoids. On the other hand, patients with highly malignant PNETs usually receive chemotherapy because of tumor metastasis and those patients usually have a poor prognosis due to tumor relapse.2–5 Over the past three decades, while the incidence of PNETs has increased, the associated clinical treatment has remained mostly unchanged. Therefore, there is an urgent need to establish and develop novel approaches against PNETs to improve patient prognosis.6
Cancer-targeted immunotherapies have evolved as a promising strategy for tackling solid tumors. Programmed death-1 (PD-1) and its ligand, programmed death ligand-1 (PD-L1), act as immune checkpoints that downregulate the activation of T cells in the tumor microenvironment.7 Therefore, blocking the PD-1-/PD-L1-mediated coinhibition of T cells will improve the endogenous immune response against tumors.
Monoclonal antibodies targeting PD-L1 or PD-1, called checkpoint inhibitors, are currently being studied in clinical trials, and remarkable response rates have been reported against lung adenocarcinoma, non-Hodgkin lymphoma, malignant melanoma, triple-negative breast cancer, and renal cell carcinoma.8–12 Further, the expression of PD-L1 by tumors is being investigated as a potential biomarker for the efficacy of PD-1/PD-L1 blockade by checkpoint inhibitors. In a recent study performed on 68 patients, preliminary data implied that PD-L1 expression by tumor cells may be related to a higher response rate.13
PD-1 is expressed on B cells, T cells, and myeloid cells. It is a costimulatory molecule that generates an inhibition signal in T-cell activation.14,15 PD-1 is overexpressed in a large proportion of tumor-infiltrating lymphocytes (TILs) in different types of tumors.16–19 PD-L1 (PD-1 ligand, also known as B7-H1) is expressed on the surface of malignant cells in different types of tumors and tumor-associated antigen-presenting cells.20–24
Several studies have shown that during tumor progression, PD-1/PD-L1 interaction leads to T-cell apoptosis and cytokine secretion, which plays a crucial role in tumor-mediated immunosuppression and tumor evasion.24,25 The overexpression of PD-L1 has been observed in tumor cells of the lungs, kidneys, esophagus, gastrointestinal tract, pancreas, ovary, colorectal, head and neck, breast, and skin (melanoma); several studies have illustrated the clinicopathological features of tumors.26–32
To the best of our knowledge, the expression of PD-1 and PD-L1 by PNETs has not yet been the focus of major research. Therefore, in this study, the correlations between PD-L1 and PD-1 expression and the clinicopathological features of PNETs in 80 patients to determine the impact of PD-1 and PD-L1 expression on patient survival were investigated. With this knowledge, the future feasibility of PNETs immunotherapy can be determined.
Materials and methods
Patients and samples
A total of 80 patients – 61 males and 19 females aged between 29 years and 76 years at The First Affiliated Hospital of Xi’an Jiaotong University – were enrolled in this study between January 2005 and December 2014. All the patients were histologically confirmed to have PNETs and their clinical characteristics (including age, gender, histological type, tumor node metastasis (TNM) stage, histological grade, and so on) were collected. The patients’ characteristics are summarized in Table 1. A TNM stage was given to each patient with PNETs according to the American Joint Committee on Cancer (2010) staging criteria.33 Tumor histology for each patient was reviewed according to the current World Health Organization classification and China Consensus Guidelines.34
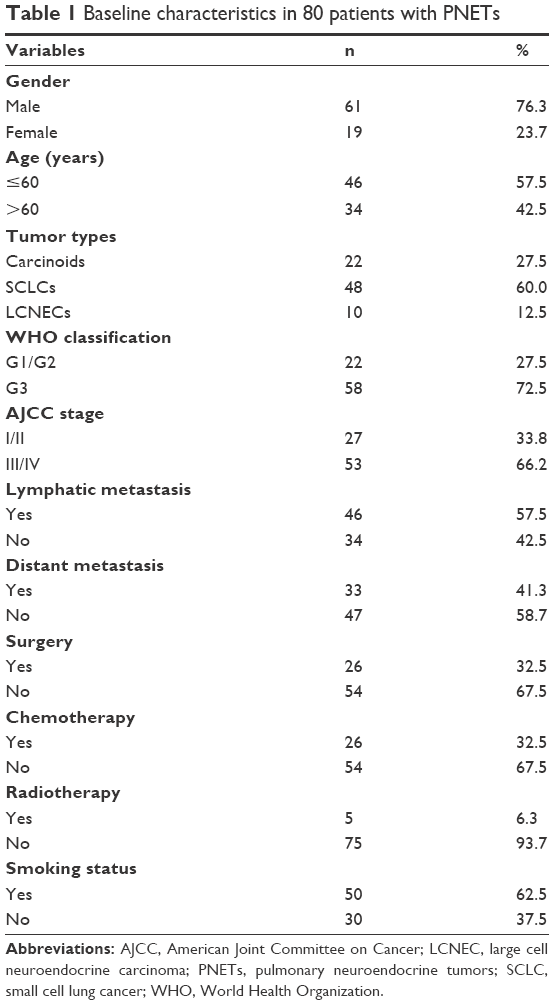 | Table 1 Baseline characteristics in 80 patients with PNETs |
In this study, patients with various types of PNETs such as carcinoids, SCLCs, and LCNECs were included. Most carcinoids received surgery and some high-grade NETs (SCLCs and LCNECs) were treated with chemo/radiation therapy. Patients who underwent surgery did not have adjuvant chemo/radiation therapy in principle. The other patients were treated with supportive therapy.
Overall survival was defined as the period from the day of diagnosis to the end of follow-up. Patients were examined until the end of the follow-up period (March 2016) or until death. Patients whose information was incomplete were excluded from the study. This study was approved by the Ethics Committees of The First Affiliated Hospital of Xi’an Jiaotong University, and all patients signed an informed consent form.
Immunohistochemical staining and scoring
PNETs tissues were fixed in 10% neutral buffered formalin, dehydrated in ethanol series, cleared in xylene, and then embedded in paraffin. Each paraffin block was serially cut to 4 μm thick sections on a microtome. Additionally, corresponding para-carcinoma lung tissues were selected as a control group from 20 cases who underwent surgical excision of PNETs.
To detect PD-L1 and PD-1 expression, immunostaining was performed with an immunohistochemical kit (SP-9001; Beijing Zhongshan Golden Bridge Biotechnology Co, Ltd, Beijing, China) according to the manufacturer’s instructions. Briefly, the sections were dried for 30 minutes at 60°C before deparaffinization in xylene and rehydration in ethanol series. Next, antigen retrieval was performed using 10 mM citrate buffer (pH 6.0) at 95°C for 5 minutes followed by incubation with 3% hydrogen peroxide in methanol for 10 minutes to quench endogenous peroxidase activity.
The sections were treated with reagent A (5% bovine serum albumin) for 30 minutes at room temperature to reduce nonspecific binding. Subsequently, the sections were incubated with rabbit monoclonal anti-PD-L1 antibody (ab205921; Abcam) at 1:50 dilution, or rabbit monoclonal anti-PD-1 antibody (ab137132; Abcam, Cambridge, UK) at 1:50 dilution, in a moist chamber at 4°C overnight. Later, the sections were incubated with reagent B and C (horseradish peroxidase-labeled rabbit anti-rabbit monoclonal antibodies), respectively, for 15 minutes at 37°C. They were then visualized by diaminobenzidine tetrahydrochloride (ZLI-9018; Beijing Zhongshan Golden Bridge Biotechnology Co, Ltd), counterstained with hematoxylin, dehydrated, cleared, and mounted. For the negative control, phosphate buffered saline was used instead of the primary antibody, and the sections were incubated at 4°C overnight.
For each section, the approximate percentage of positive tumor cells and staining intensity determined the PD-L1 staining score. Three independent pathologists observed five different high-power fields at the hot-spot areas of each slide in a blinded manner (400× magnification). The proportion of stained cells in each field were assessed as follows: 0 for <5% stained cells; 1 for 5%–25% stained cells; 2 for 26%–50% stained cells; and 3 for >50% stained cells. Intensity of overall staining was graded as follows: 0 for negative staining; 1 for light staining; 2 for moderate staining; and 3 for intense staining. The staining intensity distribution (SID) for one field was obtained by multiplying the score of the proportion of stained cells by the score of the staining intensity. Then, the mean of the five fields in each section was the final SID score for that sample. SID was finally judged as 0–2 for negative and ≥3 for positive.35 As for PD-1 in TILs, sections were scored at 5% intervals, and specimens with ≥5% staining were considered positive.11
Statistical analysis
SPSS software (Statistical Package for the Social Sciences, version 18.0, SPPS, Inc, Chicago, IL, USA) was used to carry out the statistical analysis. Depending on the data type, chi-squared (χ2) test or Student’s t-test was used to analyze the differences between groups. Survival analysis was performed by Kaplan–Meier plot and log-rank tests. Multivariate analyses according to the Cox proportional hazards regression model were performed. All statistical tests were two-sided, and P<0.05 was considered statistically significant.
Results
Immunohistochemical analysis of the expression PD-L1 or PD–1 and the association with clinicopathological characteristics
In tissues of PNETs, PD–L1 immunostaining was observed in the cytoplasm and on the plasma membrane of cancer cells, and PD-1 immunostaining was observed in the cytoplasm and on the plasma membrane of TILs. In corresponding paracarcinoma lung tissues, PD–L1 and PD-1 immunostaining was observed in the cytoplasm and on the plasma membrane in normal lung tissue cells, like non-neoplastic alveolar pneumocytes, bronchial epithelial cells, pulmonary macrophages, and so on, which was hypochromic obviously. Representative images are shown in Figure 1A–H.
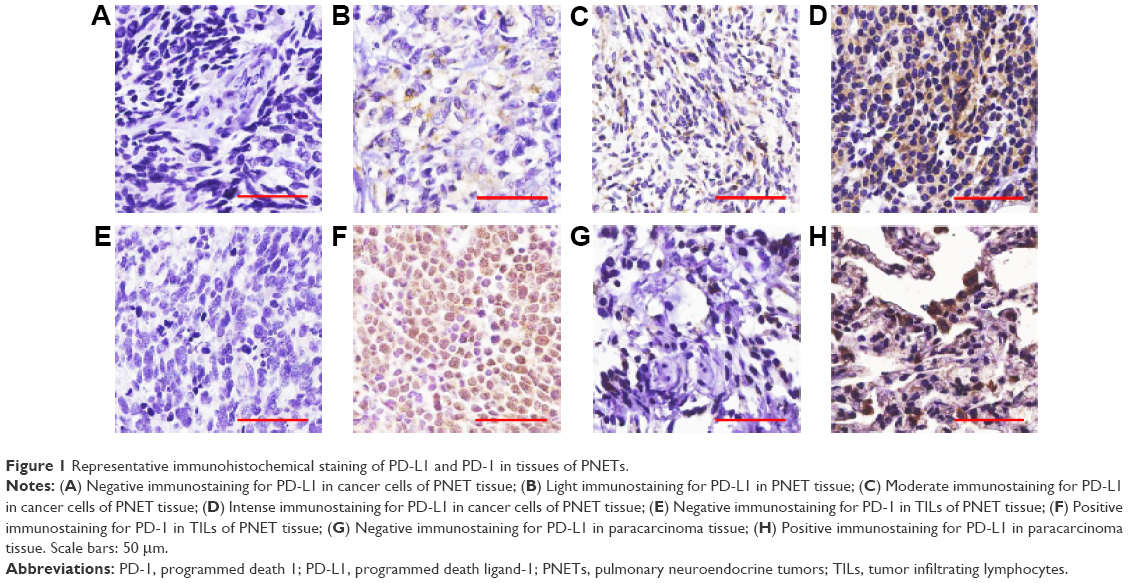 | Figure 1 Representative immunohistochemical staining of PD-L1 and PD-1 in tissues of PNETs. |
Positive PD-1 expression in TILs was observed in the PNET tissue specimens of 41 cases (51.3%) and in the paracarcinoma tissues of four cases (20%). The difference between the two groups was found to be significant (P=0.012). The incidence rate of PD-L1 in tissue specimens of PNETs was 58.8% (47/80), while the incidence rate in paracarcinoma tissues was 25% (5/20). The difference was statistically significant (P=0.007).
The mean SID score of PD-L1 staining was 3.4750±2.6143 (mean ± standard deviation) in PNET tissues and 1.6500±2.2775 (mean ± standard deviation) in paracarcinoma tissues (P=0.005). Additionally, PD-L1 expression was observed to correlate with the PD-1 expression (P=0.007); see Table 2.
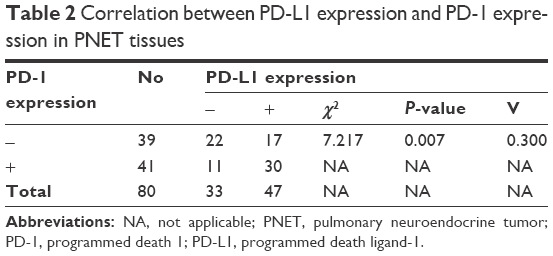 | Table 2 Correlation between PD-L1 expression and PD-1 expression in PNET tissues |
Data showing the association between PD-L1 or PD-1 expression and various clinicopathological characteristics of patients with PNETs is shown in Table 3. Results indicated that the PD-L1 expression was significantly related to the tumor stage (P=0.014) and histological type (P=0.014).
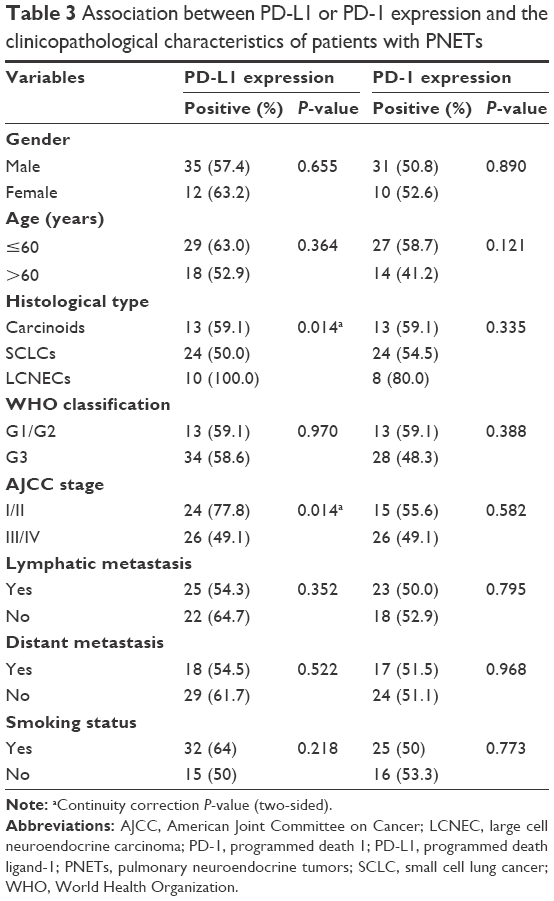 | Table 3 Association between PD-L1 or PD-1 expression and the clinicopathological characteristics of patients with PNETs |
Survival analysis for patients with PNETs using the Kaplan–Meier method and Cox proportional hazards regression model
Univariate analyses showed that overall survival of patients with PNETs was significantly associated with four prognostic factors: PD-L1, PD-1 expression, tumor TNM stage, and distant metastasis (Table 4). Therefore, these prognostic factors were subjected to multivariate analysis using a Cox proportional hazard model. Multivariate analysis revealed that the expression of PD-L1 in cancer cells (hazard ratio, 0.345; 95% confidence interval, 0.194–0.614; P<0.001); the expression of PD1 in TILs (hazard ratio, 0.367; 95% confidence interval, 0.206–0.652; P=0.001); and distant metastasis of PNETs all remained independently associated with the survival time (Table 5).
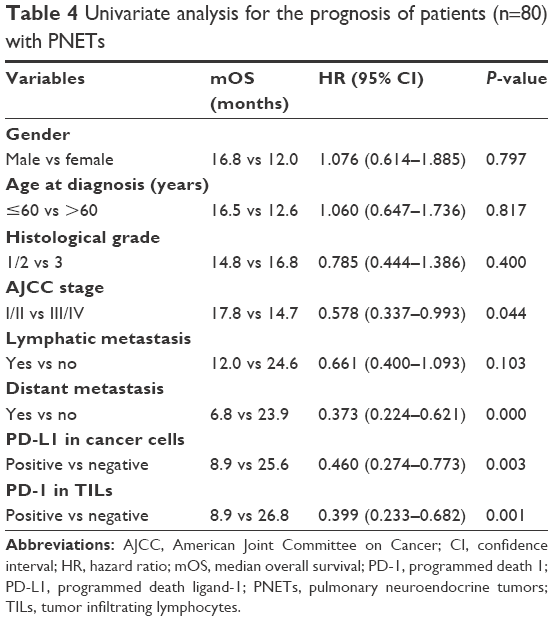 | Table 4 Univariate analysis for the prognosis of patients (n=80) with PNETs |
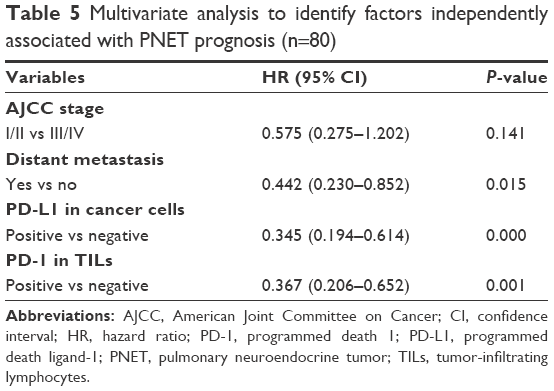 | Table 5 Multivariate analysis to identify factors independently associated with PNET prognosis (n=80) |
The Kaplan–Meier survival curves for PD-L1, PD-1, and distant metastasis positive and negative cases are shown in Figure 2, which reveals that patients with negative metastasis as well as PD-L1 and PD-1 expression had better prognoses.
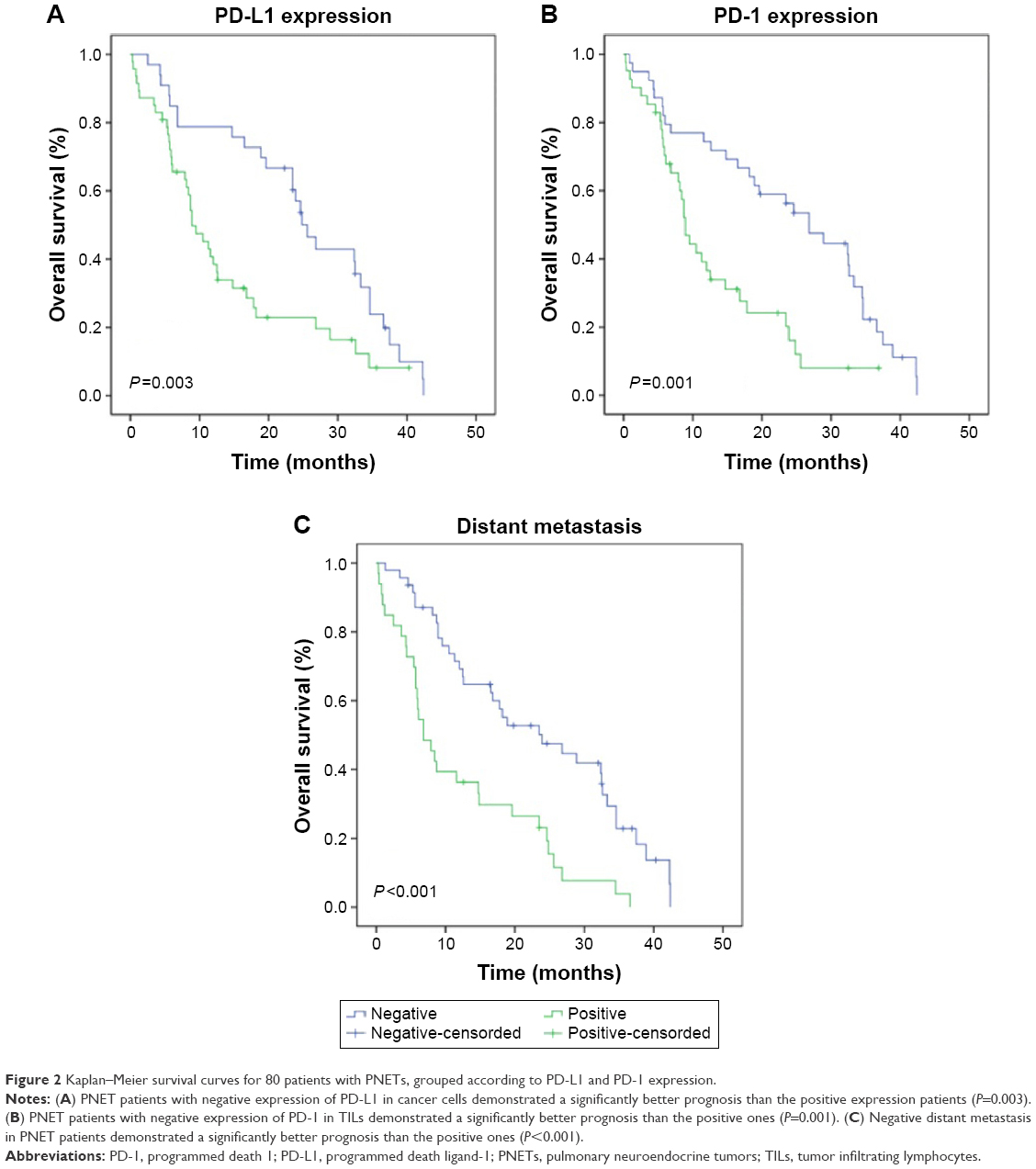 | Figure 2 Kaplan–Meier survival curves for 80 patients with PNETs, grouped according to PD-L1 and PD-1 expression. |
Discussion
The rise in the incidence of PNETs and the limited available therapeutic options have created an urgent demand for new treatment strategies. Cancer immunotherapy is a promising new treatment strategy that will soon be an integral part of the comprehensive tumor therapy. Indeed, checkpoint inhibitors targeting PD-1, pembrolizumab, and nivolumab were recently approved by the US Food and Drug Administration in 2014 and 2015, respectively.36 Moreover, the efficacy of several monoclonal antibodies toward PD-1 or PD-L1 was investigated in Phase I trials, and continue to be assessed in Phase II and III clinical trials.
Checkpoint inhibitors targeting PD-1 (nivolumab and pembrolizumab) and PD-L1 (MPDL3280A and BMS-936559) have achieved promising antitumor effect without serious adverse reactions.37 Moreover, it has been reported that the overexpression of PD-L1 in tumors was associated with a higher response to anti-PD-L1 therapy.13
In this study, the aim was to prove the role of PD-L1 and PD-1 as predictive or prognostic biomarkers for survival in patients with PNETs. Therefore, PD-L1 or PD-1 expression were analyzed by immunohistochemistry (IHC) in 80 patients with PNETs, and investigated possible correlations between their expression and patients’ clinicopathological parameters and overall survival.
First, the rate of positive PD-L1 expression in PNET tissues was proved to increase compared with the paracarcinoma tissues, and the study verified that PD-L1 was highly expressed in PNETs. PD-L1 overexpression in various tumors was associated with a higher response to anti-PD-L1 therapy.13 Thus the PD-L1 molecule can act as a potential biomarker for detecting the efficacy of immunotherapy in patients with PNETs.
In contrast to the results, Schultheis et al analyzed 94 clinical cases of small cell carcinomas (61 pulmonary tumors and 33 extrapulmonary tumors) and found that no PD-L1 overexpression was observed on the neoplastic cells of small cell carcinoma cases by IHC. However, they detected PD-L1 expression in the tumor-infiltrating macrophages and revealed activated PD-1/PD-L1 pathway in a fraction of small cell carcinomas.38 The contradiction can be attributed to the fact that the study used anti-PD-L1-antibodies with different immunogenic domains in both studies. Further, it was observed that PD-1 was highly expressed in TILs and the expression of PD-L1 was directly associated with PD-1 expression (P=0.007).
A previous study also reported that the expression of PD-L1 was inversely related to TILs, particularly CD8+ T cells.29 Therefore, it can be speculated that the induced PD-L1 on tumor cells interacts with PD-1 on TILs and that these interactions can regulate the effector function of TILs resulting in immune invasion and tumor progression. Thus, monoclonal antibodies against PD-L1 or PD-1 molecule may ultimately benefit patients with PNETs.
The above-mentioned assumption is supported by the fact that PD-L1 was significantly related to the tumor stage (P=0.014) and histological type (P=0.014). As the American Joint Committee on Cancer tumor staging system is recognized as a pivotal prognostic factor in human tumor progression, PD-L1 expression may also be associated with tumor development. Indeed, the univariate analyses in this study revealed that the overall survival time of patients with PNETs was significantly associated with PD-L1 expression in cancer cells. Further, multivariate analysis by a Cox proportional hazards model revealed that PD-L1 expression in PNETs remained independently associated with the survival time. This undoubtedly proved that PD-L1 took part in the occurrence and progression of PNETs; therefore, PD-L1 can be used as a predictive and prognostic biomarker for patients’ survival.
Interestingly, there was no significant association between PD-1 expression and the clinicopathological characteristics when the correlation between PD-1 expression and clinicopathological characteristics of patients with PNETs were explored. However, the univariate analyses exhibited a significant association between the overall survival time of patients with PNETs and PD-1 expression, which was proven to exist independently. Thus, PD-1 can also be used as a potential biomarker for survival. Moreover, these results imply that PD-1 and PD-L1 interaction can lead to tumor progression.
Owing to the benefits of immunotherapy, several potential predictive biomarkers are currently being investigated for efficacy. Among these, PD-L1 expression is one of the most promising predictors of response to immune checkpoint inhibitors. Robert et al’s (2014) Phase I study demonstrated a 36% response rate to nivolumab in PD-L1 positive tumors, including advanced melanoma, non-small cell lung cancer, and renal cell carcinoma.39 Further, Carbognin et al observed that the activity of nivolumab, pembrolizumab, and MPDL3280A varied according to PD-L1 expression in tumor cells.40 However, the involved molecular mechanism remains poorly understood and more future studies are required to determine the relationship between PD-L1 expression and response rate.
In addition, there is also a high percentage of patients with no PD-L1 expression who respond to anti-PD-L1 immunotherapy. However, the point is that a patient with positive PD-L1 expression is more likely to be sensitive to anti-PD-L1 immunotherapy. Many other immune-related biomarkers exist. For instance, biomarkers including T-cell-specific, antigen presentation-related, and interferon gamma signaling-related genes, may allow for improved selection for patients who are likely to respond to anti-PD-1 therapy with pembrolizumab.41 The combination of multiple immune-related biomarkers need to be used in taking immunotherapy into consideration.
In conclusion, this study identified correlations between PD-L1/PD-1 expression and clinicopathological variables and/or survival time. Data provided by this study sheds light on the importance of PD-L1/PD-1 pathway for tumor progression, which will help to pave the way for new immunotherapy regimens against PNETs.
This study had some limitations including small sample size and the sole dependence on immunohistochemical analysis of PD-1 and PD-L1 expression. Schultheis et al recently showed that RNA sequencing (RNA-seq) and IHC yielded highly comparable results, although RNA-seq yielded more PD-L1 positive cases than IHC.38
In future studies, the results need to be reconfirmed in a large multicenter study with RNA-seq and immunohistochemical analyses.
Acknowledgment
The authors thank Medjaden Bioscience Ltd (http://www.medjaden.com/index.html) for providing English language editing services.
Disclosure
The authors report no conflicts of interest in this work.
References
Travis WD, Brambilla E, Nicholson AG, et al. The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015;10(9):1243–1260. | ||
Gridelli C, Rossi A, Airoma G, et al. Treatment of pulmonary neuroendocrine tumours: state of the art and future developments. Cancer Treat Rev. 2013;39(5):466–472. | ||
Swarts DR, Ramaekers FC, Speel EJ. Molecular and cellular biology of neuroendocrine lung tumors: evidence for separate biological entities. Biochim Biophys Acta. 2012;826(2):255–271. | ||
Metro G, Duranti S, Fischer MJ, Cappuzzo F, Crino L. Emerging drugs for small cell lung cancer – an update. Expert Opin Emerg Drugs. 2012;17(1):31–36. | ||
Oberg K, Hellman P, Ferolla P, Papotti M; ESMO Guidelines Working Group. Neuroendocrine bronchial and thymic tumors: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23(Suppl 7):vii120–vii123. | ||
Yao JC, Hassan M, Phan A, et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008;26(18):3063–3072. | ||
He J, Hu Y, Hu M, Li B. Development of PD-1/PD-L1 pathway in tumor immune microenvironment and treatment for non-small cell lung cancer. Sci Rep. 2015;5:13110. | ||
Brahmer JR, Drake CG, Wollner I, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010;28(19):3167–3175. | ||
Brahmer JR, Tykodi SS, Chow LQ, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012;366(26):2455–2465. | ||
Topalian SL, Sznol M, McDermott DF, et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J Clin Oncol. 2014;32(10):1020–1030. | ||
Taube JM, Klein A, Brahmer JR, et al. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin Cancer Res. 2014;20(19):5064–5074. | ||
Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–2454. | ||
Powles T, Eder JP, Fine GD, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014;515(7528):558–562. | ||
Ishida Y, Agata Y, Shibahara K, Honjo T. Induced expression of PD-1, a novel member of the immunoglobulin gene superfamily, upon programmed cell death. EMBO J. 1992;11(11):3887–3895. | ||
Nishimura H, Honjo T. PD-1: an inhibitory immunoreceptor involved in peripheral tolerance. Trends Immunol. 2001;22(5):265–268. | ||
Dong H, Zhu G, Tamada K, Chen L. B7-H1, a third member of the B7 family, co-stimulates T-cell proliferation and interleukin-10 secretion. Nat Med. 1999;5(12):1365–1369. | ||
Freeman GJ, Long AJ, Iwai Y, et al. Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J Exp Med. 2000;192(7):1027–1034. | ||
Zhang Y, Huang S, Gong D, Qin Y, Shen Q. Programmed death-1 upregulation is correlated with dysfunction of tumor-infiltrating CD8+ T lymphocytes in human non-small cell lung cancer. Cell Mol Immunol. 2010;7(5):389–395. | ||
Lyford-Pike S, Peng S, Young GD, et al. Evidence for a role of the PD-1:PD-L1 pathway in immune resistance of HPV-associated head and neck squamous cell carcinoma. Cancer Res. 2013;73(6):1733–1741. | ||
Sfanos KS, Bruno TC, Meeker AK, De Marzo AM, Isaacs WB, Drake CG. Human prostate-infiltrating CD8+ T lymphocytes are oligoclonal and PD-1+. Prostate. 2009;69(15):1694–1703. | ||
Ahmadzadeh M, Johnson LA, Heemskerk B, et al. Tumor antigen-specific CD8 T cells infiltrating the tumor express high levels of PD-1 and are functionally impaired. Blood. 2009;114(8):1537–1544. | ||
Zou W, Chen L. Inhibitory B7-family molecules in the tumour microenvironment. Nat Rev Immunol. 2008;8(6):467–477. | ||
Zang X, Allison JP. The B7 family and cancer therapy: costimulation and coinhibition. Clin Cancer Res. 2007;13(18 Pt 1):5271–5279. | ||
Freeman GJ, Long AJ, Iwai Y, et al. Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J Exp Med. 2000;192(7):1027–1034. | ||
Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus Docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373(17):1627–1639. | ||
Badoual C, Hans S, Merillon N, et al. PD-1-expressing tumor-infiltrating T cells are a favorable prognostic biomarker in HPV-associated head and neck cancer. Cancer Res. 2013;73(1):128–138. | ||
Droeser RA, Hirt C, Viehl CT, et al. Clinical impact of programmed cell death ligand 1 expression in colorectal cancer. Eur J Cancer. 2013;49(9):2233–2242. | ||
Konishi J, Yamazaki K, Azuma M, Kinoshita I, Dosaka-Akita H, Nishimura M. B7-H1 expression on non-small cell lung cancer cells and its relationship with tumor-infiltrating lymphocytes and their PD-1 expression. Clin Cancer Res. 2004;10(15):5094–5100. | ||
Nomi T, Sho M, Akahori T, et al. Clinical significance and therapeutic potential of the programmed death-1 ligand/programmed death-1 pathway in human pancreatic cancer. Clin Cancer Res. 2007;13(7):2151–2157. | ||
Ohigashi Y, Sho M, Yamada Y, et al. Clinical significance of programmed death-1 ligand-1 and programmed death-1 ligand-2 expression in human esophageal cancer. Clin Cancer Res. 2005;11(8):2947–2953. | ||
Spranger S, Spaapen RM, Zha Y, et al. Up-regulation of PD-L1, IDO, and T(regs) in the melanoma tumor microenvironment is driven by CD8(+) T cells. Sci Transl Med. 2013;5(200):200ra116. | ||
Thompson RH, Dong H, Lohse CM, et al. PD-1 is expressed by tumor-infiltrating immune cells and is associated with poor outcome for patients with renal cell carcinoma. Clin Cancer Res. 2007;13(6):1757–1761. | ||
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. | ||
Schnabel PA, Junker K. Pulmonale neuroendokrine Tumoren in der neuen WHO-Klassifikation 2015 [Pulmonary neuroendocrine tumors in the new WHO 2015 classification: start of breaking new grounds?]. Pathologe. 2015;36(3):283–292. Greek. | ||
Ye Y, Zhou L, Xie X, Jiang G, Xie H, Zheng S. Interaction of B7-H1 on intrahepatic cholangiocarcinoma cells with PD-1 on tumor-infiltrating T cells as a mechanism of immune evasion. J Surg Oncol. 2009;100(6):500–504. | ||
Lee J, Kefford R, Carlino M. PD-1 and PD-L1 inhibitors in melanoma treatment: past success, present application and future challenges. Immunotherapy. 2016;8(6):733–746. | ||
Ohaegbulam KC, Assal A, Lazar-Molnar E, Yao Y, Zang X. Human cancer immunotherapy with antibodies to the PD-1 and PD-L1 pathway. Trends Mol Med. 2015;21(1):24–33. | ||
Schultheis AM, Scheel AH, Ozretic L, et al. PD-L1 expression in small cell neuroendocrine carcinomas. Eur J Cancer. 2015;51(3):421–426. | ||
Robert C, Ribas A, Wolchok JD, et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet. 2014;384(9948):1109–1117. | ||
Carbognin L, Pilotto S, Milella M, et al. Differential activity of nivolumab, pembrolizumab and MPDL3280A according to the tumor expression of programmed death-ligand-1 (PD-L1): sensitivity analysis of trials in melanoma, lung and genitourinary cancers. PLoS One. 2015;10(6):e0130142. | ||
Antoni R, Caroline R F. Stephen H, et al. Association of response to programmed death receptor 1 (PD-1) blockade with pembrolizumab (MK-3475) with an interferon-inflammatory immune gene signature. 2015 ASCO Annual Meeting. J Clin Oncol. 2015(suppl: abstr3001). |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.