")
Back to Journals » Clinical Interventions in Aging » Volume 14
Prognostic value of health-related quality of life in elderly patients hospitalized with heart failure
Authors Erceg P , Despotovic N , Milosevic DP, Soldatovic I, Mihajlovic G, Vukcevic V , Mitrovic P, Markovic-Nikolic N , Micovic M, Mitrovic D , Davidovic M
Received 13 January 2019
Accepted for publication 30 April 2019
Published 22 May 2019 Volume 2019:14 Pages 935—945
DOI https://doi.org/10.2147/CIA.S201403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Predrag Erceg,1,2 Nebojsa Despotovic,1,2 Dragoslav P Milosevic,1,2 Ivan Soldatovic,1 Gordana Mihajlovic,1,2 Vladan Vukcevic,1,3 Predrag Mitrovic,1,3 Natasa Markovic-Nikolic,1,4 Milica Micovic,2 Dragica Mitrovic,5 Mladen Davidovic1
1Faculty of Medicine, University of Belgrade, Belgrade, Serbia; 2Clinical Department of Geriatrics, “Zvezdara” University Hospital, Belgrade, Serbia; 3Cardiology Clinic, Clinical Center of Serbia, Belgrade, Serbia; 4Clinical Department of Cardiology, “Zvezdara” University Hospital, Belgrade, Serbia; 5Department of Physical Medicine and Rehabilitation, “Zvezdara” University Hospital, Belgrade, Serbia
Purpose: Previous research has shown that poor health-related quality of life (HRQOL) is associated with adverse long-term prognosis in patients with heart failure (HF); however, there have been inconsistencies among studies and not all of them confirmed the prognostic value of HRQOL. In addition, few studies involved elderly patients and most focused on all-cause mortality and HF-related hospitalization as outcomes. The aim of our study was to determine whether HRQOL is a predictor and an independent predictor of long-term cardiac mortality, all-cause mortality, and HF-related rehospitalization in elderly patients hospitalized with HF.
Patients and methods: This prospective observational study included 200 elderly patients hospitalized with HF in Serbia. HRQOL was measured using the Minnesota Living with Heart Failure questionnaire (MLHFQ). The median follow-up period was 28 months. The primary outcome was cardiac mortality, and all-cause mortality and HF-related rehospitalization were secondary outcomes. Survival analysis was conducted using the Kaplan–Meier method and Cox-proportional hazards regression.
Results: Subjects with poor HRQOL (higher than the median MLHFQ score) had a higher probability of cardiac mortality (P=0.029) and HF-related rehospitalization (P=0.001) during long-term follow-up. Poor HRQOL was an independent predictor of cardiac mortality (HR: 2.051, 95% CI: 1.260–3.339, P=0.004), all-cause mortality (HR: 1.620, 95% CI: 1.076–2.438, P=0.021), and HF-related rehospitalization (HR: 2.040, 95% CI: 1.290–3.227, P=0.002).
Conclusion: HRQOL is an independent predictor of long-term cardiac mortality in elderly patients hospitalized with HF. It also independently predicts all-cause mortality and HF-related rehospitalization. HRQOL could be used as a complementary clinical predictive tool in this patient population.
Keywords: aged, heart disease, self-perception of health, prognosis
Introduction
Heart failure (HF) is a frequent disease in the elderly; its prevalence increases with age and ranges from 4.8% to 13.5% in this population.1 It is associated with high mortality, comparable to the rates of various malignancies, and the 5-year mortality is almost 50%.2–4 The aging of populations worldwide indicates that HF will become a major public health problem in the coming decades,3 and research on HF is currently focusing on improvement in survival and health-related quality of life (HRQOL).5 HRQOL is usually defined as the patient’s self-perceived health status,6 and it may be impaired in HF patients due to their symptoms, functional limitations, and psychological problems.7
Evaluation of prognosis in HF is important because patients at high risk of unfavorable outcomes could benefit from more intensive treatment and more frequent monitoring.5,8 Previous research has shown that numerous factors, including age, sex, New York Heart Association (NYHA) class, and left ventricular ejection fraction (LVEF), influence prognosis in HF patients, and efforts have been made to develop new prognostic models for HF.9
Research indicates that poor HRQOL predicts worse prognosis in HF patients; thus, it could be used as a novel prognostic marker in HF patients.10–13 However, previous studies used different instruments for measuring HRQOL, and a review showed that their results were not consistent enough to reach a definitive conclusion.14 Most of the research on the prognostic value of HRQOL in HF has been conducted in younger subjects.10–14 To our knowledge, there have only been two studies solely on elderly subjects.15,16 Furthermore, most of the previous studies focused on all-cause mortality or HF-related hospitalization as endpoints.10–16 Given that overall long-term survival in elderly HF patients is influenced by multiple other conditions that are common in this age group, such as malignancies and dementia,17,18 we aimed to determine whether HRQOL, as a global measure of overall health state14 including those influences, is a predictor and an independent predictor of long-term cardiac mortality, all-cause mortality, and HF-related rehospitalization in elderly patients hospitalized with HF.
Patients and methods
Study population and design
This prospective observational study included 200 patients aged ≥65 years hospitalized with HF at the Geriatric Department of “Zvezdara” University Hospital in Belgrade, Serbia, between February 2009 and July 2012. HF diagnosis was established by study personnel, using the European Society of Cardiology criteria.19 Exclusion criteria were terminal malignancy, end-stage renal failure, previous stroke with immobility, or advanced dementia. All patients gave written informed consent. The study was approved by the Ethics Committee of “Zvezdara” University Hospital and conducted according to the principles outlined in the Declaration of Helsinki.
Patients were followed up from February 2009 to May 2018, for a median period of 28 months (minimum 1, maximum: 95, IQR: 54), during which time they received standard care from their physicians.
Outcomes
The primary outcome was time until cardiac death. Secondary outcomes were times until all-cause death and HF-related rehospitalization. Data on the outcomes were collected from hospital medical records and/or reports from primary care physicians. Cause of death was obtained from death certificates.
Health-related quality of life measurement
HRQOL was measured with the Serbian version of the Minnesota Living with Heart Failure questionnaire (MLHFQ).20 The MLHFQ consists of 21 items and reflects the impact of HF on a patient’s everyday life in the previous month. The questions ask the patient to indicate how much a possible effect of HF prevented them from living as they wanted during the past month; responses are graded from 0 (no effect) to 5 (very much). The questionnaire’s total score can range between 0 and 105, with higher values indicating poorer HRQOL. It has two subscales that measure the physical (eight items; range 0–40) and emotional (five items; range 0–25) dimensions of HRQOL. The MLHFQ is a widely used disease-specific tool for measuring HRQOL in patients with HF, with proven validity and reliability.21
Data collection
Demographic data, ie, age, sex, marital status, educational level, living situation (living alone or not), and income, were obtained by interview. Clinical characteristics were collected from medical records and included the length of HF, history of previous myocardial infarction, angina, risk factors for coronary artery disease (CAD), comorbidities (diabetes, hypertension, atrial fibrillation, previous stroke, chronic obstructive pulmonary disease, chronic kidney disease, liver disease, peptic ulcer disease, anemia, malignancies, and dementia), and current medication. All the above-mentioned conditions were taken into comorbidity score. NYHA class was determined based on the patients’ symptoms and functional limitations. LVEF was measured by echocardiography using the modified Simpson’s rule.
Depressive symptoms and cognitive impairment
Symptoms of depression were evaluated using the five-item Geriatric Depression Scale (GDS), which is a validated screening tool for identifying possible depression in the elderly.22 The score can range from 0 to 5 points, where ≥2 indicates potential depression. The Mini-Mental State Examination23 was used to assess cognitive status. Patients who scored <25 were considered to be cognitively impaired.
Statistical analysis
Categorical variables are presented as frequencies and percentages, while continuous variables are presented as mean ± SD. Patients were grouped according to the median total MLHFQ score, and the medians of the physical and emotional scores. Differences between subjects with better and worse HRQOL, grouped according to the median MLHFQ scores (total, physical, and emotional), were tested using the Student’s independent samples t-test for normally distributed continuous variables and the Mann–Whitney U test for non-normally distributed continuous variables. The Chi-square test was performed to compare differences between categorical variables. Testing was performed in order to obtain covariates that could be potential confounders for the observed outcomes. All patients’ data were complete (n=200), except for obesity, family history of CAD, LVEF, hyponatremia and hemoglobin levels, where numbers of missing values were: 1 (0.5%), 4 (2.0%), 3 (1.5%), 2 (1.0%), and 1 (0.5%), respectively. Percentage of data completion was sufficient to perform further analyses. It was not necessary to use missing-data imputation methods.
Survival analysis
Survival analysis was conducted using the Kaplan–Meier method and Cox-proportional hazards regression. The differences in survival times between subjects with better and worse HRQOL in terms of the total score and the physical and emotional dimension scores were tested using the log-rank test based on Kaplan–Meier curves. Cox-proportional hazards models were also constructed in order to determine whether HRQOL and the physical and emotional dimension scores were predictors (in univariate analyses) and independent predictors (in multivariable analyses) of cardiac mortality, all-cause mortality, and HF-related rehospitalization. Multivariable modeling was performed in two steps. First, potential theoretical confounders of mortality in HF patients (age, sex, NYHA class, and LVEF) and MLHFQ score groups were entered in the model. Those variables were obligatory, and the enter method was used in this step. Next, all variables with P<0.10 in the univariate Cox-proportional hazards regression analyses and those that showed a significant difference with P<0.05 between patients with better and worse HRQOL were entered in the model. Last, the backward method with 0.05 entrance and 0.10 probability removal criteria was applied, and obligatory variables and those with P<0.10 were retained in the final model.
All statistical tests were two-tailed, and P<0.05 was considered statistically significant. Statistical analysis was performed with the IBM SPSS Statistics® software version 20.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline patient characteristics
The baseline characteristics of all patients and those with better and worse HRQOL are presented in Table 1. The patients had a mean age of 77.5 years, 51% were male, 68.5% were in NYHA classes III–IV, and the mean LVEF was 42.1%. Patients with worse HRQOL were significantly more likely to be in NYHA classes III–IV, take diuretics and digoxin, take more drugs, and have depressive symptoms, and significantly less likely to have hypertension. The mean total MLHFQ score in the entire group of subjects was 47.4±18.8, while the mean physical and emotional dimension scores were 23.8±9.3 and 9.8±6.1, respectively.
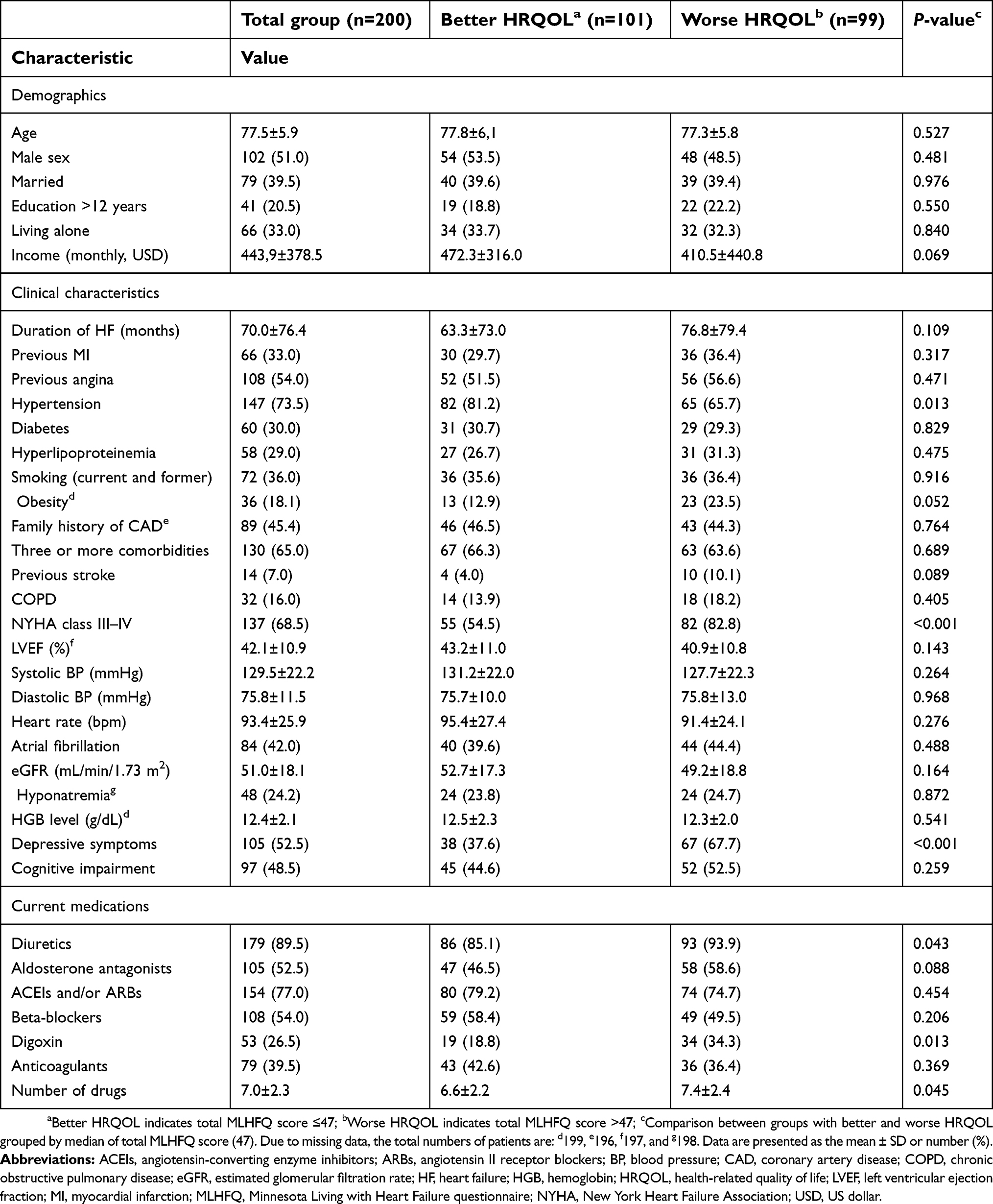 | Table 1 Baseline patient characteristics according to HRQOL |
Follow-up
After discharge from the hospital, 169 out of 194 survivors (87.1%) were followed up for a median period of 28 months. Twenty-five patients (12.9%) were lost to follow-up. During the follow-up period, 110 patients (65.1%) died, with cardiac death occurring in 78 patients (46.2%), and 105 patients (62.1%) experienced HF-related rehospitalization.
Survival analysis
Kaplan–Meier survival analysis showed that patients with worse HRQOL had a significantly higher probability of cardiac death (X2=4.754; P=0.029) and HF-related rehospitalization (X2=10.665; P=0.001) than those with better HRQOL. There was no significant difference in the probability of all-cause death (X2=2.596; P=0.107) between the patients with better and worse HRQOL. Kaplan–Meier curves showing the probability of cardiac death, all-cause death, and HF-related rehospitalization in patients with better and worse HRQOL are presented in Figure 1.
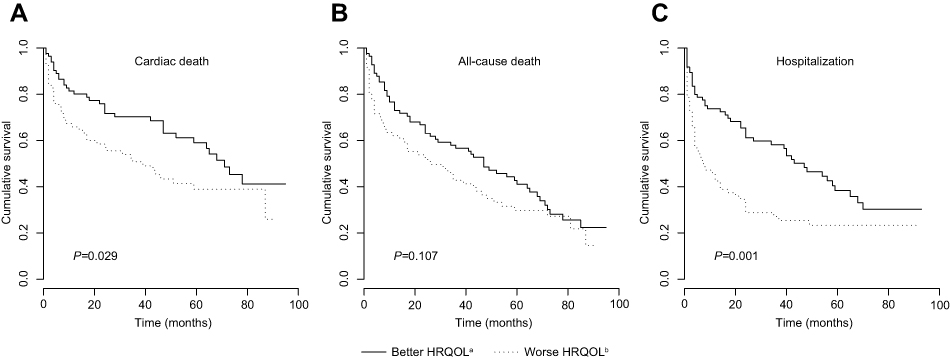 | Figure 1 Kaplan–Meier curves showing probability of cardiac death, all-cause death, and HF-related rehospitalization in patients with better and worse HRQOL. aBetter HRQOL indicates total MLHFQ score ≤47; bWorse HRQOL indicates total MLHFQ score >47. Each P-value indicates whether the probability of the event (eg, cardiac death) at any time point was significantly different between the two groups (according to the log-rank test). Abbreviations: HF, heart failure; HRQOL, health-related quality of life; MLHFQ, Minnesota Living with Heart Failure questionnaire. |
Patients with a worse HRQOL physical dimension score had a significantly higher probability of cardiac death (X2=5.199; P=0.023) and HF-related rehospitalization (X2=7.552; P=0.006) than those with a better HRQOL physical dimension score. There was no significant difference in the probability of all-cause death between patients with better and worse HRQOL physical dimension scores (X2=3.464; P=0.063). Kaplan–Meier curves showing the probability of cardiac death, all-cause death, and HF-related rehospitalization in patients with better and worse HRQOL physical dimension scores are presented in Figure 2.
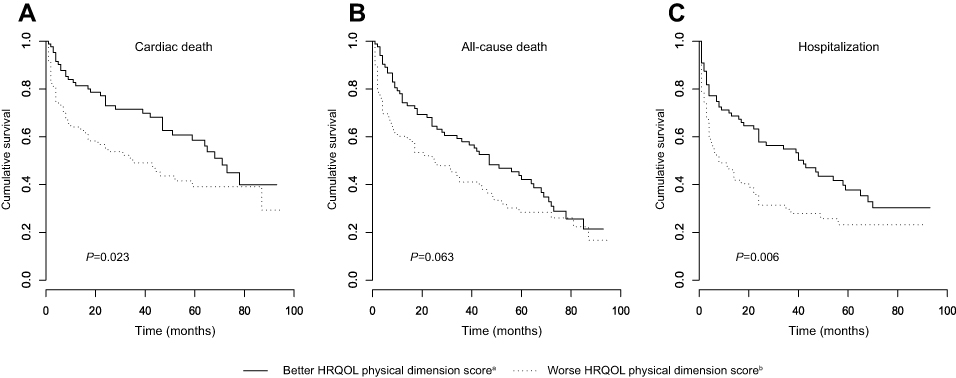 | Figure 2 Kaplan–Meier curves showing probability of cardiac death, all-cause death, and HF-related rehospitalization in patients with better and worse HRQOL physical dimension scores.aBetter HRQOL physical dimension score indicates physical MLHFQ score ≤24; bWorse HRQOL physical dimension score indicates physical MLHFQ score >24. Each P-value indicates whether the probability of the event (eg, cardiac death) at any time point was significantly different between the two groups (according to the log-rank test). Abbreviations: HF, heart failure; HRQOL, health-related quality of life; MLHFQ, Minnesota Living with Heart Failure questionnaire. |
There were no differences in probability of cardiac death (X2=0.533; P=0.465), all-cause death (X2=0.456; P=0.500), or HF-related rehospitalization (X2=0.560; P=0.454) between patients with better and worse HRQOL emotional dimension scores. Kaplan–Meier curves showing the probability of cardiac death, all-cause death, and HF-related rehospitalization in patients with better and worse HRQOL emotional dimension scores are presented in Figure 3.
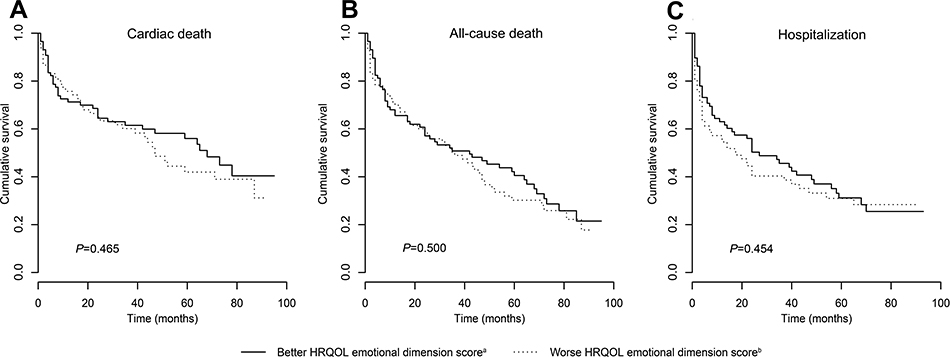 | Figure 3 Kaplan–Meier curves showing probability of cardiac death, all-cause death, and HF-related rehospitalization in patients with better and worse HRQOL emotional dimension scores. aBetter HRQOL emotional dimension score indicates emotional MLHFQ score ≤9; bWorse HRQOL emotional dimension score indicates emotional MLHFQ score >9. Each P-value indicates whether the probability of the event (eg, cardiac death) at any time point was significantly different between the two groups (according to the log-rank test). Abbreviations: HF, heart failure; HRQOL, health-related quality of life; MLHFQ, Minnesota Living with Heart Failure questionnaire. |
Univariate Cox-proportional hazards regression analyses showed that worse HRQOL was significantly associated with increased risk of cardiac mortality and HF-related rehospitalization, but not with all-cause mortality. A worse HRQOL physical dimension score predicted cardiac mortality and HF-related rehospitalization, but not all-cause mortality. There were no associations between the HRQOL emotional dimension score and the observed outcomes. The results of the univariate Cox-proportional hazards regression models of HRQOL and the physical and emotional dimension scores regarding the time until cardiac death, all-cause death, and HF-related rehospitalization are presented in Table 2.
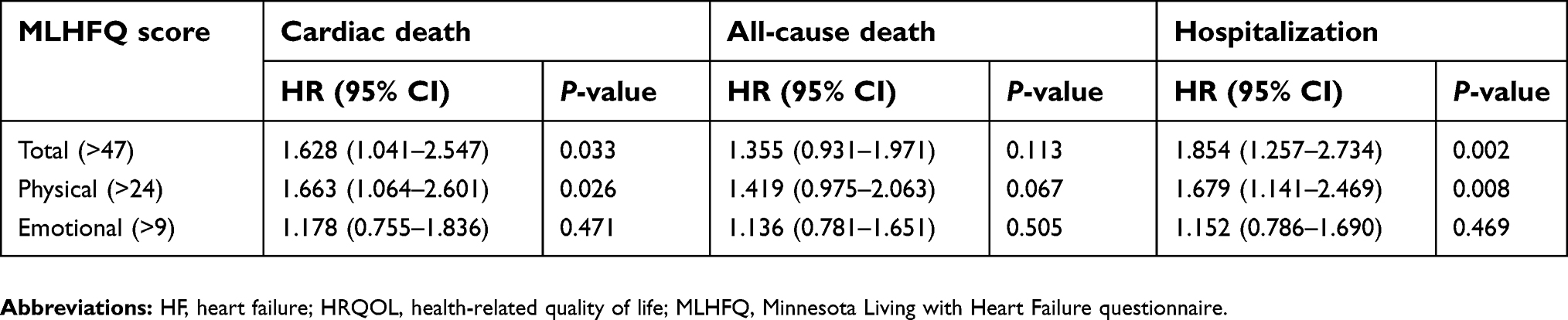 | Table 2 Univariate Cox-proportional hazards regression of HRQOL and subscales regarding the time until cardiac death, all-cause death, and HF-related rehospitalization |
Multivariable Cox-proportional hazards regression analyses showed that worse HRQOL was significantly independently associated with increased cardiac mortality, all-cause mortality, and HF-related rehospitalization. A worse HRQOL physical dimension score was a significant independent predictor of cardiac and all-cause mortality, but not HF-related rehospitalization. The HRQOL emotional dimension score was not an independent predictor of any of the observed outcomes. The results of the multivariable Cox-proportional hazards regression models of the HRQOL and the physical and emotional dimension scores regarding the time until cardiac death, all-cause death, and HF-related rehospitalization are presented in Table 3.
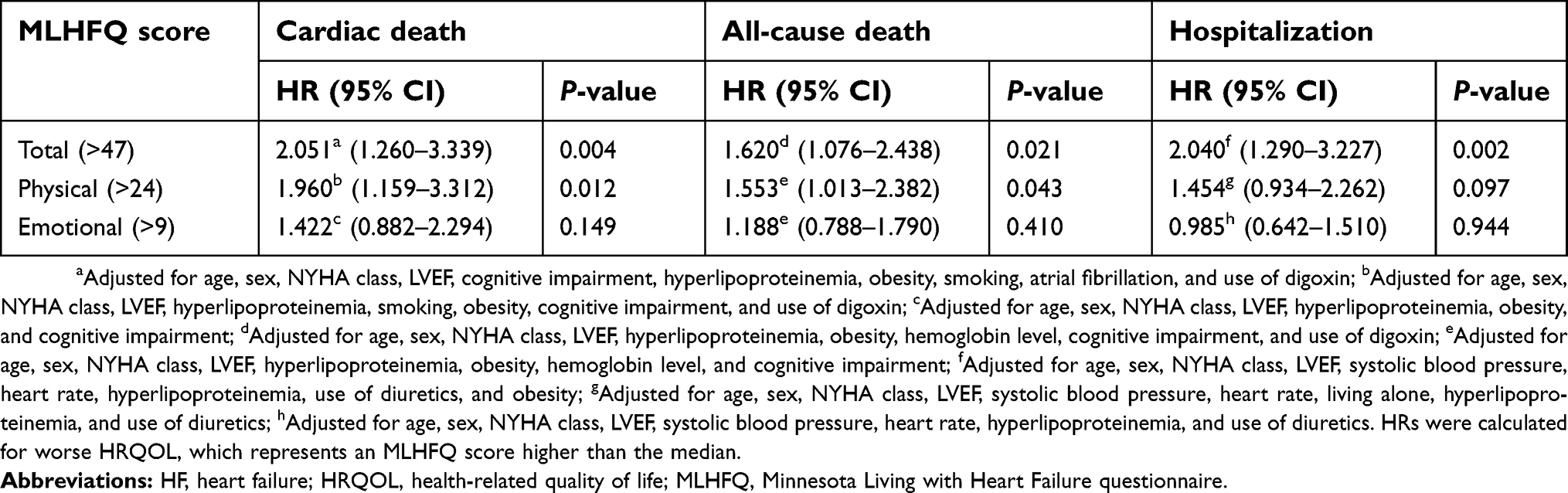 | Table 3 Multivariable Cox-proportional hazards regression of HRQOL and subscales regarding the time until cardiac death, all-cause death, and HF-related rehospitalization |
Discussion
The main finding of our study is that poor HRQOL is an independent predictor of increased long-term cardiac mortality, all-cause mortality, and HF-related rehospitalization in elderly patients hospitalized with HF. A novel finding of our research is that HRQOL independently predicts cardiac mortality in elderly HF patients. Most of the previous research on the associations between HRQOL and long-term prognosis in HF patients focused on all-cause mortality or HF-related hospitalization as outcomes.10–16 Only a few studies used the combined endpoint of cardiac death and HF-related hospitalization or cardiac event-free survival as an outcome.24–26 In our study, we used MLHFQ, which is a disease-specific instrument that measures HRQOL in HF and reflects how the disease affects everyday life and functioning of patients.20 We believe that if HRQOL is a predictor of the long-term prognosis of elderly HF patients, using cardiac death as a primary endpoint better reflects the real prognostic value of HRQOL in HF than all-cause death, especially in the elderly, many of whom have multiple comorbidities that could influence all-cause mortality.17,18,27
Our subjects were older than the patients included in most of the previous studies that assessed the prognostic value of HRQOL in HF.10–14,24,28 According to the available literature, there have been only two studies that included solely elderly patients,15,16 and the mean age of subjects in each of these studies was similar to that in our study. Approximately half of our patients were male, in contrast to the studies of younger subjects, in which males were a majority,10,11,13,24,28 and the two studies of elderly subjects, which reported a higher frequency of women.15,16 More than two-thirds of our subjects were in NYHA classes III–IV. This is in contrast to most of the previous studies in younger and older populations, which reported that up to 50% of patients were in these higher NYHA classes,10,11,13,15,16,24,28 indicating that our patients had more functional limitations. The mean LVEF in our study was 42%, similar to the value reported in the two studies of elderly subjects,15,16 while studies involving younger subjects reported a wide range of mean LVEF values, from 22% to 51%.10,11,13,24,28,29 The mean total MLHFQ score in our patients was 47.4, higher than the scores reported in the majority of studies in younger subjects,10,11,24,26 indicating worse HRQOL in our subjects. This could be explained by the fact that our subjects were older, had higher NYHA classes, were hospitalized, and were more likely to have symptoms of depression, which could all contribute to poor HRQOL.25,30–33 However, each of the two studies involving elderly subjects had a total MLHFQ score similar to ours.15,16
When we compared the baseline characteristics of patients with better and worse HRQOL, the latter were significantly more likely to be in NYHA classes III–IV, take diuretics and digoxin, take more drugs and have depressive symptoms, and significantly less likely to have hypertension. Previous studies also found that poor HRQOL was associated with higher NYHA class, more frequent use of diuretics and digoxin, and polypharmacy.24,28,34 Many studies found that depression was strongly associated with poor HRQOL,25,34,35 consistent with our findings. Hypertension has been shown to negatively influence quality of life in a general population,36 but studies conducted in HF patients found no association with HRQOL,10,32 contrary to our results.
Kaplan–Meier survival analysis showed that our patients with worse HRQOL had higher probabilities of cardiac death and HF-related rehospitalization compared with those with better HRQOL. We found no difference in the probability of all-cause death between the two groups. We also found that patients with a worse HRQOL physical dimension score had a higher probability of cardiac death and HF-related rehospitalization than those with a better HRQOL physical dimension score. There were no differences in the probabilities of cardiac death, all-cause death, or HF-related rehospitalization between patients with better and worse HRQOL emotional dimension scores.
Previous studies that used the same method of survival analysis (Kaplan–Meier) and the same instrument for measuring HRQOL (MLHFQ) found that worse HRQOL was associated with a higher probability of all-cause death,11,13,24 in contrast to our findings. Possible explanation for discrepancies between our results and the findings of above-mentioned studies comes from the fact that in these studies patients were younger, predominantly male, in a lower NYHA classes, and recruited mostly from outpatient clinics. Heidenreich et al,28 using the Kansas City Cardiomyopathy Questionnaire (KCCQ)37 as a disease-specific instrument for assessing HRQOL in HF, reported that subjects with poor HRQOL had a higher probability of all-cause death, which differs from our results. However, they included younger subjects from outpatient clinics who were predominantly male with lower LVEF, which could possibly explain the variable findings. Studies that used HF-related hospitalization as one of the endpoints revealed that poor HRQOL is linked to a higher probability of hospitalization, in accordance with our results.11,28,29 Kato et al24 found that subjects with poor HRQOL had a higher probability of the combined endpoint of cardiac death and HF-related hospitalization, which partly fits with our findings. Hoekstra et al10 reported that patients with worse physical functioning and general health subscale scores measured by a generic HRQOL instrument, the Medical Outcomes Study Short-Form 36 (SF-36)38 questionnaire, had a higher probability of all-cause death, which differs from our findings. These differences could be explained with the use of SF-36, designed to measure health status across various conditions and in healthy people,38 and a different sample which in their study included younger, predominantly male patients with lower LVEF.
Using Cox-proportional hazards regression survival analysis, we found that worse HRQOL is a predictor of cardiac mortality and HF-related rehospitalization, and an independent predictor of cardiac mortality, all-cause mortality, and HF-related rehospitalization. In addition, we revealed that a poor HRQOL physical dimension score is a predictor of cardiac mortality and HF-related rehospitalization, and an independent predictor of cardiac mortality and all-cause mortality. Studies using the MLHFQ in elderly subjects found that poor HRQOL was a predictor of all-cause mortality and HF-related hospitalization,15 and that a poor HRQOL physical dimension score was an independent predictor of all-cause mortality,15,16 partly consistent with our findings. Several studies that included younger patients with HF showed that HRQOL was an independent predictor of all-cause mortality and HF-related hospitalization,11,13,24,28,29 which is consistent with our findings. The HRQOL emotional dimension score was not a predictor or an independent predictor of any of the observed endpoints in our study, consistent with the findings of most previous studies.14
Previous studies that assessed the prognostic value of HRQOL in HF patients reported inconsistent results due to differences in HRQOL definitions, measuring instruments, sample sizes and populations, time of baseline measurement, endpoints, and follow-up duration.14 There is no consensus about the definition of HRQOL, and the term is often interchangeably used with quality of life and health status.6 In addition, researchers often define quality of life and choose questionnaires for its measurement according to the purpose of their study, making cross-study comparison difficult.39 There are several generic questionnaires designed for measuring the quality of life in the elderly, such as World Health Organization’s Quality of Life measure for older people (WHOQOL-OLD),40 but to our knowledge, there is still no disease-specific instrument for measuring HRQOL in elderly patients with HF. Future research should focus on developing such a questionnaire, and the process should involve both experts in the field and elderly people.41 Given that HRQOL is a subjective concept,6 we propose that asking older people to help defining the concept of HRQOL and develop appropriate questionnaires for its measurement would lead to more valid and reliable tools for assessing HRQOL and its predictive value in this population.
Our findings and those from previous research indicate that worse HRQOL is an independent predictor of poor long-term prognosis in HF patients.11,13,15,16,24,28,29 The advantage of our study is that we showed that HRQOL is an independent predictor of cardiac mortality in elderly patients hospitalized with HF. As mentioned before, we suggest that cardiac death and HF-related rehospitalization are better endpoints to evaluate the prognostic value of HRQOL in HF than all-cause mortality. There are several reasons that could possibly explain this hypothesis. First, we assessed HRQOL with MLHFQ, which is a disease-specific instrument for HF and does not reflect general HRQOL. Second, if we hypothesize that HRQOL measured by this questionnaire could be a predictor of poor prognosis of HF patients, it is more important to assess cardiac mortality than all-cause mortality, because only cardiac death should be an event of interest. In other words, we think that the quality of life of HF patients is not theoretically related to the likelihood of any fatal outcome, as death may be a consequence of, for example, a fall and subsequent fracture of the hip, malignancy, or dementia, which are all common causes of mortality in the elderly.17,18,27,42 Thus, prediction of all-cause mortality should not be linked to HRQOL in HF, especially if it is measured by a disease-specific instrument.
Clinical implications
The most important goals in the treatment of HF patients are reducing mortality, preventing hospitalization, and improving HRQOL.5 Findings from previous research and those of our study indicate that poor HRQOL is associated with unfavorable long-term prognosis in elderly patients with HF.15,16 Consequently, assessing HRQOL in elderly HF patients could be a simple and cost-effective complementary method for risk stratification in this population. Patients at high risk of unfavorable outcomes could benefit from specific interventions targeting the improvement of HRQOL,43 as well as from more intensive treatment and more frequent monitoring.5
Pharmacological interventions modestly improve HRQOL in HF.43 Treatment with angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and ivabradine increased HRQOL in older subjects.43,44 Cardiac resynchronization therapy in selected patients also resulted in improvement in HRQOL,5 but the benefits of such a procedure have not yet been proven in the elderly.45 Specific multidisciplinary HF management and monitoring programs could also improve HRQOL in HF patients.5,43,45 Cardiac rehabilitation and exercise training programs appear to be among the most promising interventions for improving HRQOL in elderly HF patients.43,46
Considering that elderly patients with HF are often frail and have multiple comorbidities, depression, cognitive impairment, and issues with polypharmacy,27,35,47,48 future interventions to improve HRQOL in this vulnerable group should focus on identification and treatment of these conditions.
Study limitations
Our study had several limitations. First, it was a relatively small, single-center study performed only in hospitalized patients, and its results may not be generalizable. Second, the median follow-up of our patients was relatively short (28 months), considering that other studies had follow-up periods of 3–7 years.10,11,13,16 Third, 25 (12.9%) of our patients were lost to follow-up, which could have influenced the validity of our results. However, the loss was <20%, which is considered to be the maximum value for a study to be valid.49 Fourth, we assessed only baseline HRQOL. Serial measurements of HRQOL during the follow-up period would give us more information about how temporal changes in HRQOL influence prognosis.11 Finally, we used only MLHFQ, which is a disease-specific instrument for measuring HRQOL, with proven validity and reliability.21 It is among the three most recommended questionnaires for use in HF patients,21,50 together with KCCQ37 and Chronic Heart Failure Questionnaire (CHFQ),51 and all three have good psychometric properties.21,50 Complementary use of other questionnaires, such as the generic SF-36 questionnaire,38 could have given us more information about the HRQOL of our patients and its prognostic value.
Conclusion
HRQOL is an independent predictor of long-term cardiac mortality in elderly patients with HF. It also independently predicts all-cause mortality and HF-related rehospitalization. Assessment of HRQOL in this population of patients could be a simple and useful clinical tool for additional evaluation of their prognosis. It could identify a subgroup of elderly HF patients with high risk of poor prognosis and help clinicians make decisions about more intensive treatment and more frequent monitoring.
Acknowledgments
This manuscript was edited for English language by Charlesworth Author Services.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mozaffarian D, Benjamin EJ, Go AS, et al.;
2. Díez-Villanueva P, Alfonso F. Heart failure in the elderly. J Geriatr Cardiol. 2016;13(2):115–117.
3. Danielsen R, Thorgeirsson G, Einarsson H, et al. Prevalence of heart failure in the elderly and future projections: the AGES-Reykjavík study. Scand Cardiovasc J. 2017;51(4):183–189. doi:10.1080/14017431.2017.1311023
4. Askoxylakis V, Thieke C, Pleger ST, et al. Long-term survival of cancer patients compared to heart failure and stroke: a systematic review. BMC Cancer. 2010;10:105. doi:10.1186/1471-2407-10-663
5. Ponikowski P, Voors AA, Anker SD, et al.;
6. Karimi M, Brazier J. Health, health-related quality of life, and quality of life: what is the difference? Pharmacoeconomics. 2016;34(7):645–649. doi:10.1007/s40273-016-0389-9
7. Rector TS. A conceptual model of quality of life in relation to heart failure. J Card Fail. 2005;11(3):173–176. doi:10.1016/j.cardfail.2005.03.005
8. Crişan S, Petrescu L, Lazăr MA, et al. Reduced ejection fraction heart failure - new data from multicenter studies and national registries regarding general and elderly populations: hopes and disappointments. Clin Interv Aging. 2018;13:651–656. doi:10.2147/CIA.S161385
9. Pocock SJ, Ariti CA, McMurray JJ, et al.;
10. Hoekstra T, Jaarsma T, van Veldhuisen DJ, Hillege HL, Sanderman R, Lesman-Leegte I. Quality of life and survival in patients with heart failure. Eur J Heart Fail. 2013;15(1):94–102. doi:10.1093/eurjhf/hfs148
11. Lupón J, Gastelurrutia P, de Antonio M, et al. Quality of life monitoring in ambulatory heart failure patients: temporal changes and prognostic value. Eur J Heart Fail. 2013;15(1):103–109. doi:10.1093/eurjhf/hfs133
12. Allen LA, Gheorghiade M, Reid KJ, et al. Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life. Circ Cardiovasc Qual Outcomes. 2011;4(4):389–398. doi:10.1161/CIRCOUTCOMES.110.958009
13. Iqbal J, Francis L, Reid J, Murray S, Denvir M. Quality of life in patients with chronic heart failure and their carers: a 3-year follow-up study assessing hospitalization and mortality. Eur J Heart Fail. 2010;12(9):1002–1008. doi:10.1093/eurjhf/hfq042
14. Mommersteeg PM, Denollet J, Spertus JA, Pedersen SS. Health status as a risk factor in cardiovascular disease: a systematic review of current evidence. Am Heart J. 2009;157(2):208–218. doi:10.1016/j.ahj.2008.09.020
15. Rodríguez-Artalejo F, Guallar-Castillón P, Pascual CR, et al. Health-related quality of life as a predictor of hospital readmission and death among patients with heart failure. Arch Intern Med. 2005;165(11):1274–1279. doi:10.1001/archinte.165.11.1274
16. Zuluaga MC, Guallar-Castillón P, López-García E, et al. Generic and disease-specific quality of life as a predictor of long-term mortality in heart failure. Eur J Heart Fail. 2010;12(12):1372–1378. doi:10.1093/eurjhf/hfq042
17. Newson RS, Witteman JC, Franco OH, et al. Predicting survival and morbidity-free survival to very old age. Age (Dordr). 2010;32(4):521–534. doi:10.1007/s11357-010-9131-2
18. Ferrer A, Formiga F, Sanz H, Almeda J, Padrós G. Multimorbidity as specific disease combinations, an important predictor factor for mortality in octogenarians: the Octabaix study. Clin Interv Aging. 2017;12:223–231. doi:10.2147/CIA.S123173
19. Dickstein K, Cohen-Solal A, Filippatos G, et al.;
20. Rector TS, Kubo SH, Cohn JN. Patients’ self-assessment of their congestive heart failure, part 2: content, reliability and validity of a new measure, the Minnesota living with heart failure questionnaire. Heart Failure. 1987;3:198–209.
21. Garin O, Ferrer M, Pont A. Disease-specific health-related quality of life questionnaires for heart failure: a systematic review with meta-analyses. Qual Life Res. 2009;18(1):71–85. doi:10.1007/s11136-009-9478-y
22. Rinaldi P, Mecocci P, Benedetti C, et al. Validation of the five-item geriatric depression scale in elderly subjects in three different settings. J Am Geriatr Soc. 2003;51(5):694–698. doi:10.1034/j.1600-0579.2003.00216.x
23. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
24. Kato N, Kinugawa K, Seki S, et al. Quality of life as an independent predictor for cardiac events and death in patients with heart failure. Circ J. 2011;75(7):1661–1669. doi:10.1253/circj.CJ-10-1308
25. Lee KS, Lennie TA, Wu JR, Biddle MJ, Moser DK. Depressive symptoms, health-related quality of life, and cardiac event-free survival in patients with heart failure: a mediation analysis. Qual Life Res. 2014;23(6):1869–1876. doi:10.1007/s11136-014-0636-5
26. Wu JR, Lennie TA, Frazier SK, Moser DK. Health-related quality of life, functional status, and cardiac event-free survival in patients with heart failure. J Cardiovasc Nurs. 2016;31(3):236–244. doi:10.1097/JCN.0000000000000248
27. Murad K, Goff DC
28. Heidenreich PA, Spertus JA, Jones PG, et al.;
29. Alla F, Briançon S, Guillemin F, et al.;
30. Masoudi FA, Rumsfeld JS, Havranek EP, et al. Age, functional capacity, and health-related quality of life in patients with heart failure. J Card Fail. 2004;10:368–373. doi:10.1016/j.cardfail.2004.01.009
31. Gott M, Barnes S, Parker C, et al. Predictors of the quality of life of older people with heart failure recruited from primary care. Age Ageing. 2006;35(2):172–177. doi:10.1093/ageing/afj040
32. Franzén K, Saveman BI, Blomqvist K. Predictors for health related quality of life in persons 65 years or older with chronic heart failure. Eur J Cardiovasc Nurs. 2007;6(2):112–120. doi:10.1016/j.ejcnurse.2006.06.001
33. Creditor MC. Hazards of hospitalization of the elderly. Ann Intern Med. 1993;118(3):219–223.
34. Erceg P, Despotovic N, Milosevic DP, et al. Health-related quality of life in elderly patients hospitalized with chronic heart failure. Clin Interv Aging. 2013;8:1539–1546. doi:10.2147/CIA.S53305
35. Bekelman DB, Havranek EP, Becker DM, et al. Symptoms, depression, and quality of life in patients with heart failure. J Card Fail. 2007;13(8):643–648. doi:10.1016/j.cardfail.2007.05.005
36. Carvalho MV, Siqueira LB, Sousa AL, Jardim PC. The influence of hypertension on quality of life. Arq Bras Cardiol. 2013;100(2):164–174. doi:10.5935/abc.20130030
37. Green CP, Porter CB, Bresnahan DR, Spertus JA. Development and evaluation of the Kansas City cardiomyopathy questionnaire: a new health status measure for heart failure. J Am Coll Cardiol. 2000;35(5):1245–1255. doi:10.1016/S0735-1097(00)00531-3
38. McHorney CA, Ware JE
39. Mollenkopf H, Walker A, eds. Quality of Life in Old Age. Dordrecht: Springer; 2007.
40. Power M, Quinn K, Schmidt S;
41. Hickey A, Barker M, McGee H, O’Boyle C. Measuring health-related quality of life in older patient populations: a review of current approaches. Pharmacoeconomics. 2005;23(10):971–993. doi:10.2165/00019053-200523110-00006
42. Schnell S, Friedman SM, Mendelson DA, Bingham KW, Kates SL. The 1-year mortality of patients treated in a hip fracture program for elders. Geriatr Orthop Surg Rehabil. 2010;1(1):6–14. doi:10.1177/2151458510378105
43. Morgan K, McGee H, Shelley E. Quality of life assessment in heart failure interventions: a 10-year (1996-2005) review. Eur J Cardiovasc Prev Rehabil. 2007;14(5):589–607. doi:10.1097/HJR.0b013e32828622c3
44. Zachariah D, Stevens D, Sidorowicz G, et al.;
45. Grady KL, Halvey K. Quality of life in elderly heart failure patients. J Geriatr Cardiol. 2006;3(4):227–236.
46. Antonicelli R, Spazzafumo L, Scalvini S, et al. Exercise: a “new drug” for elderly patients with chronic heart failure. Aging (Albany NY). 2016;8(5):860–872. doi:10.18632/aging.100901
47. Denfeld QE, Winters-Stone K, Mudd JO, Gelow JM, Kurdi S, Lee CS. The prevalence of frailty in heart failure: A systematic review and meta-analysis. Int J Cardiol. 2017;236:283–289. doi:10.1016/j.ijcard.2017.01.153
48. Lazzarini V, Mentz RJ, Fiuzat M, Metra M, O’Connor CM. Heart failure in elderly patients: distinctive features and unresolved issues. Eur J Heart Fail. 2013;15(7):717–723. doi:10.1093/eurjhf/hft028
49. Sacket DL, Richardson WS, Rosenberg W. Evidence-Based Medicine: How to Practice and Teach EBM. New York: Churchill Livingstone; 1997.
50. Garin O, Herdman M, Vilagut G, et al. Assessing health-related quality of life in patients with heart failure: a systematic, standardized comparison of available measures. Heart Fail Rev. 2014;19(3):359–367. doi:10.1007/s10741-013-9394-7
51. Guyatt GH, Nogradi S, Halcrow S, Singer J, Sullivan MJ, Fallen EL. Development and testing of a new measure of health status for clinical trials in heart failure. J Gen Intern Med. 1989;4(2):101–107. doi:10.1007/BF02602348
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.