Back to Journals » OncoTargets and Therapy » Volume 8
Prognostic role of apoptosis-related gene functional variants in advanced non-small-cell lung cancer patients treated with first-line platinum-based chemotherapy
Authors Tao K, Li X, Xu W, Wang Y, Zhu S, Xie H, Luo W, Xu Y, Xu X
Received 24 September 2014
Accepted for publication 19 December 2014
Published 14 January 2015 Volume 2015:8 Pages 147—155
DOI https://doi.org/10.2147/OTT.S74855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr William C. Cho
Kai-Yi Tao,1 Xian-Xing Li,2 Wei-Zhen Xu,3 Yin Wang,4 Shuang-Mei Zhu,5 Hua-Xia Xie,3 Wen-Hua Luo,6 Yan-Jun Xu,7 Xiao-Ling Xu3,7
1Department of Thoracic Surgery, 2Department of Radiology, 3Key Laboratory on Diagnosis and Treatment Technology on Thoracic Cancer, Zhejiang Cancer Hospital (Zhejiang Cancer Research Institute), 4Physical Examination Center, Zhejiang Provincial People’s Hospital, Hangzhou, 5Department of Radio-Chemotherapy Oncology, Lishui People’s Hospital, Sixth Affiliated Hospital of Wenzhou Medical University, 6Department of Radio-Chemotherapy Oncology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 7Department of Medical Oncology, Zhejiang Cancer Hospital, Hangzhou, People’s Republic of China
Background: Single-nucleotide polymorphisms in apoptosis-related genes have been shown to play a role in the efficacy of platinum-based chemotherapy and may influence clinical outcomes. Our study aimed to evaluate the correlations of four functional single-nucleotide polymorphisms – FAS −670 A>G, FAS ligand −844 T>C, survivin −31 G>C, and survivin 9386 C>T – with drug response and clinical outcomes in advanced non-small-cell lung cancer patients who received platinum-based chemotherapy.
Materials and methods: Polymorphisms were evaluated using the polymerase chain reaction-based restriction fragment-length polymorphism technique.
Results: Patients with the CC genotype of FAS −670 A>G had worse overall survival (OS) than those with the CT or TT genotype (P=0.044), with median OS values of 20.1 months, 22.8 months, and 26.0 months, respectively. Furthermore, progression-free survival was associated with the FAS −670 A>G polymorphism (P=0.032). In addition, patients with the TC and CC genotypes of survivin 9386 C>T experienced improved survival compared with patients with the TT genotype (median OS 31.4 months and 22.8 months, respectively).
Conclusion: The functional FAS −670 A>G and survivin 9386 C>T polymorphisms are potential independent prognostic factors in advanced non-small-cell lung cancer patients treated with platinum-based chemotherapy.
Keywords: lung cancer, FAS −670 A>G, survivin 9386 C>T, polymorphism, chemotherapy response
Introduction
Lung cancer is the most common cancer in males worldwide, being responsible for 17% of total new cancer cases and resulting in 23% of cancer-related deaths. Among females, lung cancer mortality accounts for nearly 11% of total cancer-related deaths in developing countries.1 Non-small-cell lung cancer (NSCLC) accounts for approximately 80%–85% of all lung cancer cases, and nearly 45% of cases present with advanced-stage disease.2 Surgical resection is the most common treatment option for early stage lung cancer, with a high 5-year survival rate and an optimistic outcome. For patients with advanced lung cancer, combinatorial treatment is becoming a standard treatment strategy, and platinum-based chemotherapy is one of the most effective therapeutic strategies for advanced NSCLC, with an objective response rate of approximately 40%.3 However, drug resistance limits the therapeutic efficacy of platinum-based regimens.
Apoptosis is a physiological process that regulates programmed cell death in multicellular organisms,4–6 and plays an important role in development and homeostasis.6 Accumulating evidence indicates that the inappropriate regulation of apoptosis contributes to human disorders, including cancer.5 Interaction of the FAS receptor, a cell-surface death receptor, with its natural ligand (FASL), plays a crucial role in apoptotic signaling in many cell types, including cells of the immune system,7,8 through both extrinsic (death receptor) and intrinsic apoptosis (mitochondrial apoptosis) pathways by inhibiting initiator (caspase 9) and effector (caspase 3 and 7) caspases.9,10 There is increasing evidence that single-nucleotide polymorphisms (SNPs) in apoptosis-related genes11–14 may be involved in clinically meaningful variations in platinum-based chemotherapy response or prognosis.
Indeed, functional SNPs in FAS, FASL, and survivin can alter gene expression, and may influence the response to chemotherapy and prognosis in patients harboring these SNPs. Although the survivin −31 G>C mutation has been linked to susceptibility in various cancer types,10,15–21 the prognostic and therapeutic implications of this SNP remain inconclusive.
As SNPs in apoptosis-related genes may be involved in platinum-based chemotherapy response and may influence clinical outcome, we prospectively evaluated four functional SNPs – FAS −670 A>G (rs1800682), FASL −844 T>C (rs763110), survivin −31 G>C (rs9904341), and survivin 9386 C>T (rs2239680) – by a polymerase chain-reaction (PCR) restriction fragment-length polymorphism (RFLP) assay in 146 patients with advanced NSCLC who received platinum-based chemotherapy to identify correlations with drug response and survival.
Materials and methods
Patients and clinical samples
A total of 146 patients with primary NSCLC who registered at the Zhejiang Cancer Hospital between April 2008 and September 2012 were enrolled in this study. All of the patients were confirmed using histopathology or cytology, and peripheral blood samples from the patients were collected prior to treatment with chemotherapy. Their disease was classified and staged according to World Health Organization criteria and the American Joint Committee on Cancer TNM classification. Patients were included according to the following criteria: 1) no previous radiotherapy or chemotherapy, 2) life expectancy of more than 4 weeks, 3) age of no more than 80 years, 4) stage IIIB or IV disease, and 5) Eastern Cooperative Oncology Group performance status of 2 or less. Patients were excluded according to the following criteria: 1) previously receiving chemotherapy or radiotherapy, 2) suffering from symptomatic brain metastasis, 3) diagnosed with other malignancies within the last 5 years, 4) stage I or II disease, and 5) Eastern Cooperative Oncology Group performance status of 3 or more. None of the patients underwent surgical resection during treatment.
This study was approved by the ethics and scientific committees of Zhejiang Cancer Hospital. Written informed consent was obtained from all patients involved in this study.
Chemotherapy regimens and other therapy
The chemotherapy regimens that the patients with NSCLC received were as follows: carboplatin on day 1 plus gemcitabine on days 1 and 8 every 3 weeks or carboplatin replaced with cisplatin on day 1; and pemetrexed on day 1 plus carboplatin or cisplatin. Each treatment was repeated for two to six cycles, interrupted only by disease progression, unacceptable toxicity, or the patient’s refusal to continue treatment. When the disease progressed, some patients received radiotherapy or EGFR-inhibitor therapy, such as gefitinib 150 mg/day, icotinib 125 mg three times a day, or erlotinib 150 mg/day.
Tumor response was evaluated according to the Response Evaluation Criteria in Solid Tumors, and all responses were evaluated at least 6 weeks after the initial assessment. Tumor response was categorized as complete response, partial response, stable disease, or progressive disease on the basis of changes in lesion size according to computed tomography scans.
DNA extraction and genotyping
Genomic deoxyribonucleic acid (DNA) samples were extracted from the peripheral blood of all subjects using a blood genomic DNA-isolation kit (Axygen Scientific, CA, USA). All genotypes were analyzed using a PCR-based RFLP assay.
The primers used to amplify the target DNA fragment containing the FAS −670 A>G polymorphism were 5′-CCTTGGCTAATTGCTGGAGT-3′ (forward) and 5′-GGAAATAATGAGTAACGAAGGACA-3′ (reverse), which produced a fragment of 283 bp. The primers designed for the FASL −844 T>C polymorphism were 5′-GCAACATAGCAAGTCCCCATC-3′ (forward) and 5′-ATTTACCCTGACCTGCCGAT-3′ (reverse), which produced a fragment of 368 bp. The primer pairs used to amplify DNA containing the survivin −31 G>C and 9386 C>T sites were 5′-GCCATTAACCGCCAGATTTGA-3′ (forward) and 5′-GAGATGCGGTGGTCCTTGAGA-3′ (reverse) and 5′-AAATTAGATGTTTCAACTGTGGTC-3′ (forward) and 5′-CAAAACAGCAAAAATGAGCC-3′ (reverse), respectively. Restriction enzymes MvaI, BseMI, MspI, or AvaII (Fermentas, Vilnius, Lithuania) were used to distinguish the FAS −670 A>G, FASL −844 T>C, survivin −31 G>C, or survivin 9386 C>T genotypes, respectively.
PCR was performed in a 15 μL reaction mixture containing 50 ng of DNA, 2.5 mM dNTP, 0.5 U Taq DNA polymerase (Sangon Biotech, Shanghai, People’s Republic of China), 1.2 mM MgCl2, 1.5 μL 10× Taq buffer and 10 pmol forward and reverse primers. The PCR conditions consisted of an initial melting step at 95°C for 5 minutes, 40 cycles of 95°C for 30 seconds, 58°C for 30 seconds for annealing, and 72°C for 40 seconds and a final extension step at 72°C for 6 minutes.
Statistical analysis
The associations between the SNPs and clinicopathological characteristics were assessed by the χ2 test, as was the connection between the SNPs and chemotherapeutic sensitivity. The Kaplan–Meier method and the log-rank test were used to estimate overall survival (OS) and progression-free survival (PFS). The unadjusted and adjusted 95% confidence intervals (CIs) of survival were calculated, and are reported for univariate and multivariate statistical models. All statistical tests were two-sided, P<0.05 was considered statistically significant, and all analyses were performed using SPSS software (version 18.0; SPSS, Chicago, IL, USA).
Results
Patient characteristics and clinical predictors
The general clinical characteristics of the patients are listed in Table 1. We recruited 146 cases of advanced lung cancer, consisting of 94 (64.4%) males and 52 (35.6%) females. The mean age of all patients was 56.6±0.7 years, ranging from 35.0 to 78.0 years old. There were 69 (50.7%) never-smokers and 72 (49.3%) smokers. Among them, 25 (17.1%) had stage IIIB disease and 121 (82.8%) had stage IV disease. The median PFS and OS values were 8.27 months (95% CI 6.4–10.1) and 25.7 months (95% CI 23.1–28.2), respectively. The median follow-up time was 17.1 months (range 5.1–56.0). The pathological type of the majority of patients was squamous cell carcinoma (87 cases, 60.3%), whereas a small percentage of patients had adenocarcinoma (24 cases, 16.4%). The others (34 cases, 23.3%) exhibited other subtypes, such as adenosquamous carcinoma or only could be diagnosed as NSCLC.
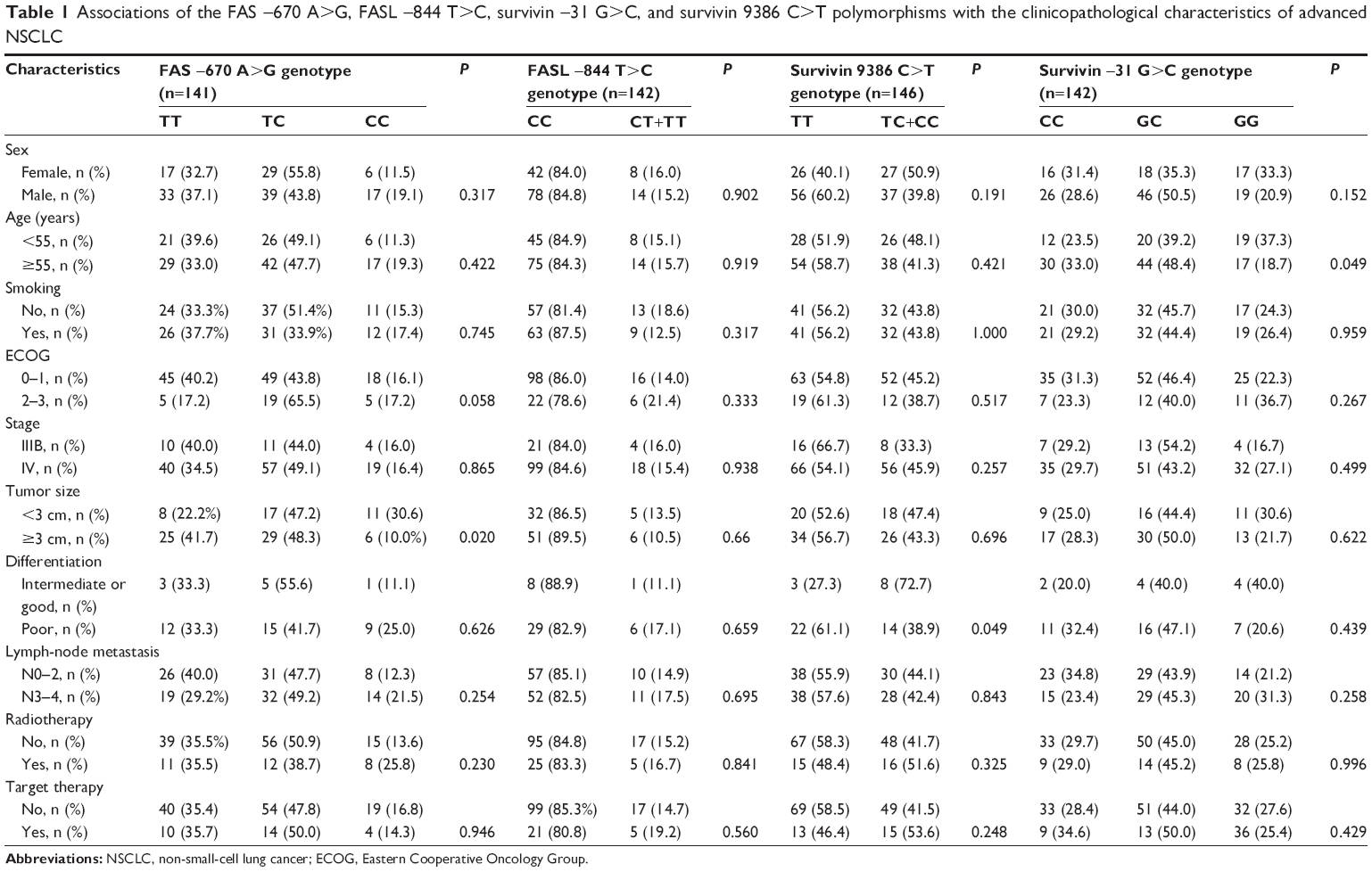 | Table 1 Associations of the FAS −670 A>G, FASL −844 T>C, survivin −31 G>C, and survivin 9386 C>T polymorphisms with the clinicopathological characteristics of advanced NSCLC |
As presented in Table 1, the observed FAS −670 A>G polymorphism frequencies were 35.5% (50 cases) for the TT genotype, 48.2% (68 cases) for the CT heterozygous genotype, and 16.3% (23 cases) for the CC genotype. The frequencies conformed to the Hardy–Weinberg equilibrium (χ2=0.0, P=0.095). The genotypic frequencies of the FASL −844 T>C polymorphism were 84.5% (120 cases), 13.4% (19 cases), and 2.1% (3 cases) for the CC, CT, TT genotypes, respectively, also conforming to the Hardy–Weinberg equilibrium (χ2=3.1, P=0.250). The frequencies of TT, TC, and CC for survivin the 9386 C>T polymorphism were 56.2% (82 cases), 37.7% (55 cases), and 6.2% (9 cases), respectively, and these frequencies also conformed to the Hardy–Weinberg equilibrium (χ2=0.0, P=0.975), as did the genotype frequencies of the survivin −31 G>C polymorphism (χ2=1.3, P=0.500).
Associations between clinicopathologic characteristics (sex, age, smoking status, stage, tumor size, differentiation, chemotherapy regimens, radiotherapy, or target therapy) of the patients and SNPs (FAS −670 A>G, FASL −844 T>C, survivin 9386 C>T, and survivin −31 G>C) are shown in Table 1. In addition, a representative gel showing the PCR-RFLP analysis of the FAS −670 A>G, FASL −844 T>C, survivin 9386 C>T, and survivin −31 G>C polymorphisms is shown in Figure 1. The FAS −670 A>G polymorphism was found to be correlated with tumor size (P=0.020), with patients harboring the CC genotype having a larger tumor size. The patients with the TT genotype of the survivin 9386 C>T polymorphism had tumors with poorer differentiation than those with the TC or TT genotype. The survivin −31 G>C polymorphism was associated with age (P=0.049). In contrast, the FASL −844 T>C polymorphism had no correlation with any clinicopathologic parameters.
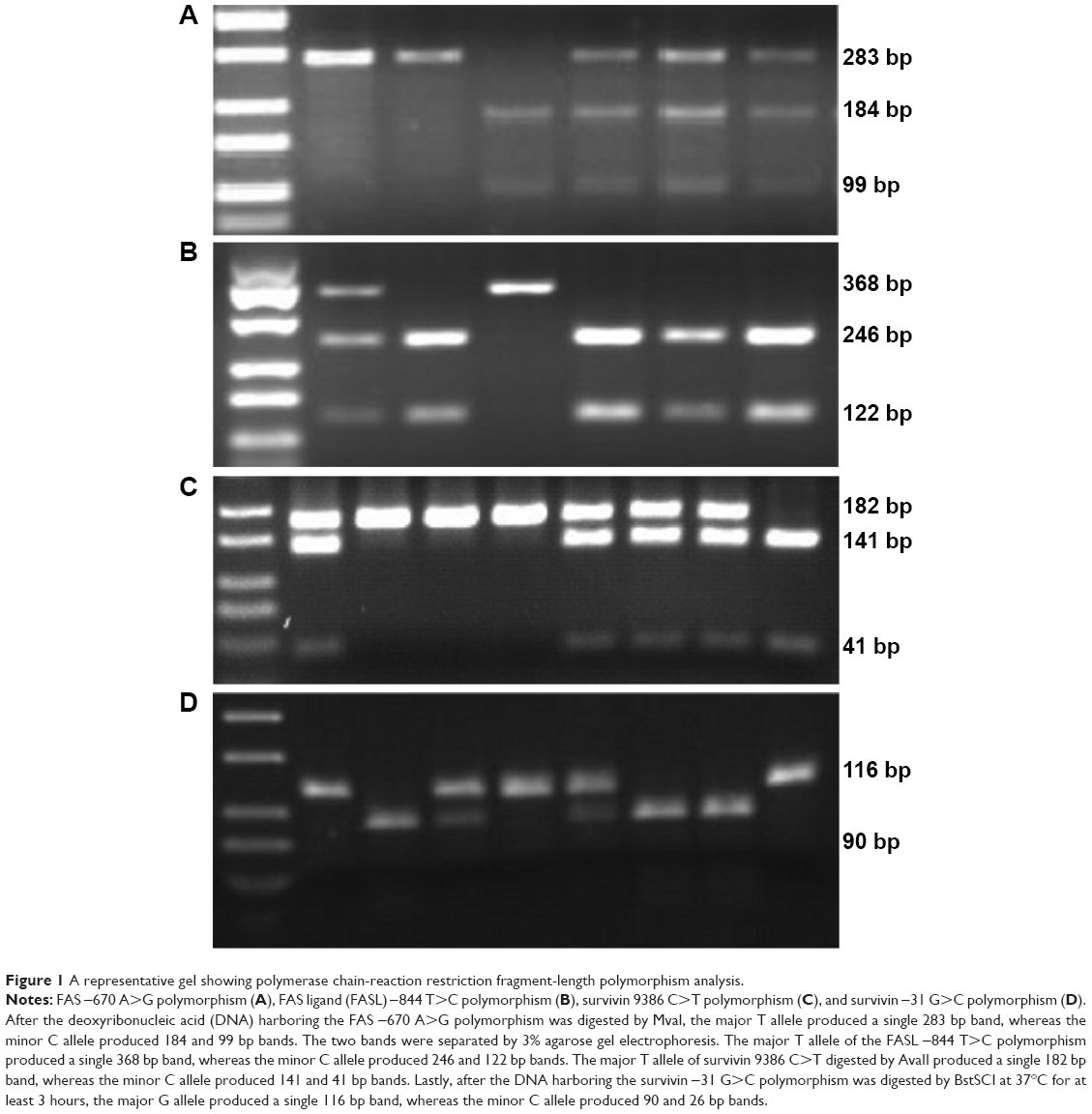 | Figure 1 A representative gel showing polymerase chain-reaction restriction fragment-length polymorphism analysis. |
Genotypes and therapeutic sensitivity
All of the 146 patients received platinum-based chemotherapy. Among them, 98 (71.0%) patients were treated with gemcitabine plus platinum chemotherapy, and 31 (22.5%) patients were treated with pemetrexed plus platinum chemotherapy. Moreover, 31 cases received radiotherapy, and 28 cases received EGFR-inhibitor therapy. There were 145 patients whose response to chemotherapy was successfully evaluated. None of the patients had a complete response, though 63 patients had a partial response, 71 had stable disease, and eleven had progressive disease. However, there were no significant associations between the four SNPs and chemotherapeutic sensitivity (data not shown).
Correlations between polymorphisms and prognosis
Kaplan–Meier survival curves were used to analyze the tumor-specific PFS and OS for the FAS −670 A>G SNP. As shown in Figure 2A, advanced NSCLC patients with the CC genotype of FAS −670 A>G had a worse OS than those with the CT or TT genotype (P=0.044), with median OS values being 20.1 months, 22.8 months and 26.0 months, respectively.
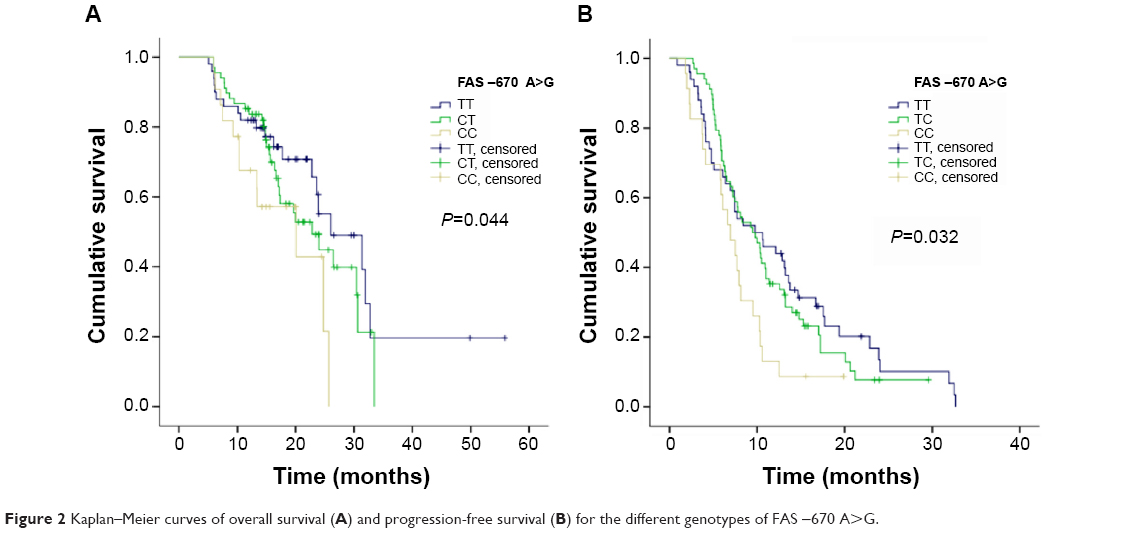 | Figure 2 Kaplan–Meier curves of overall survival (A) and progression-free survival (B) for the different genotypes of FAS −670 A>G. |
Furthermore, PFS was associated with the FAS −670 A>G polymorphism, as shown in Figure 2B. A log-rank test showed that patients with the CT genotype (median PFS 9.5 months, 95% CI 6.9–12.0) or TT genotype (median PFS 9.8 months, 95% CI 4.3–15.2) experienced better survival than patients with the CC genotype (median PFS 8.3 months, 95% CI 6.3–10.2; P=0.032).
Moreover, the survivin 9386 C>T polymorphism was associated with OS in advanced NSCLC patients (Figure 3). Those patients with the TC and CC genotypes experienced improved survival compared with those with the TT genotype (median OS 31.4 months and 22.8 months, respectively; P=0.006). However, no connection was observed between FASL −844 T>C or survivin −31 G>C and prognosis in patients with advanced NSCLC. In addition, radiotherapy and response to chemotherapy had an impact on PFS, whereas none of the clinicopathologic parameters had an impact on OS in a univariate analysis.
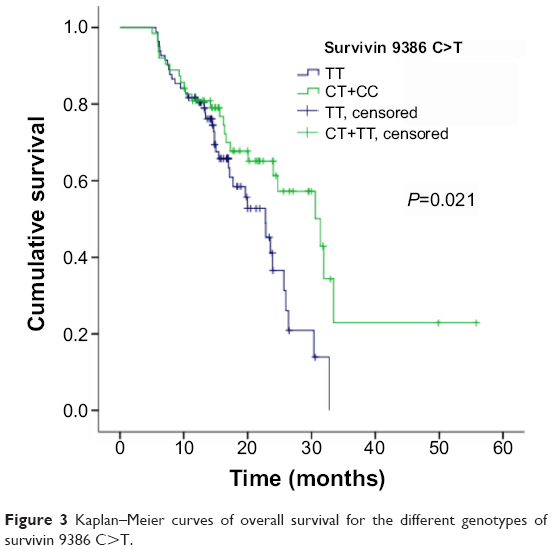 | Figure 3 Kaplan–Meier curves of overall survival for the different genotypes of survivin 9386 C>T. |
The Cox proportional hazard model was used in a multivariate analysis. The FAS −670 A>G polymorphism and radiotherapy were significant variables in determining PFS (hazard ratio 2.2, P=0.030; hazard ratio 1.6, P=0.025; respectively). Furthermore, the multiplicative interaction term for survivin 9386 C>T and differentiation (hazard ratio 0.1, 95% CI 0.1–0.9; P=0.042) were found to be independent prognostic factors for OS in patients with NSCLC, as was tumor response to chemotherapy (hazard ratio 0.3, 95% CI 0.1–0.8; P=0.022) (Table 2). Finally, a subgroup analysis was conducted according to different clinical characteristics, and the conclusion was the same.
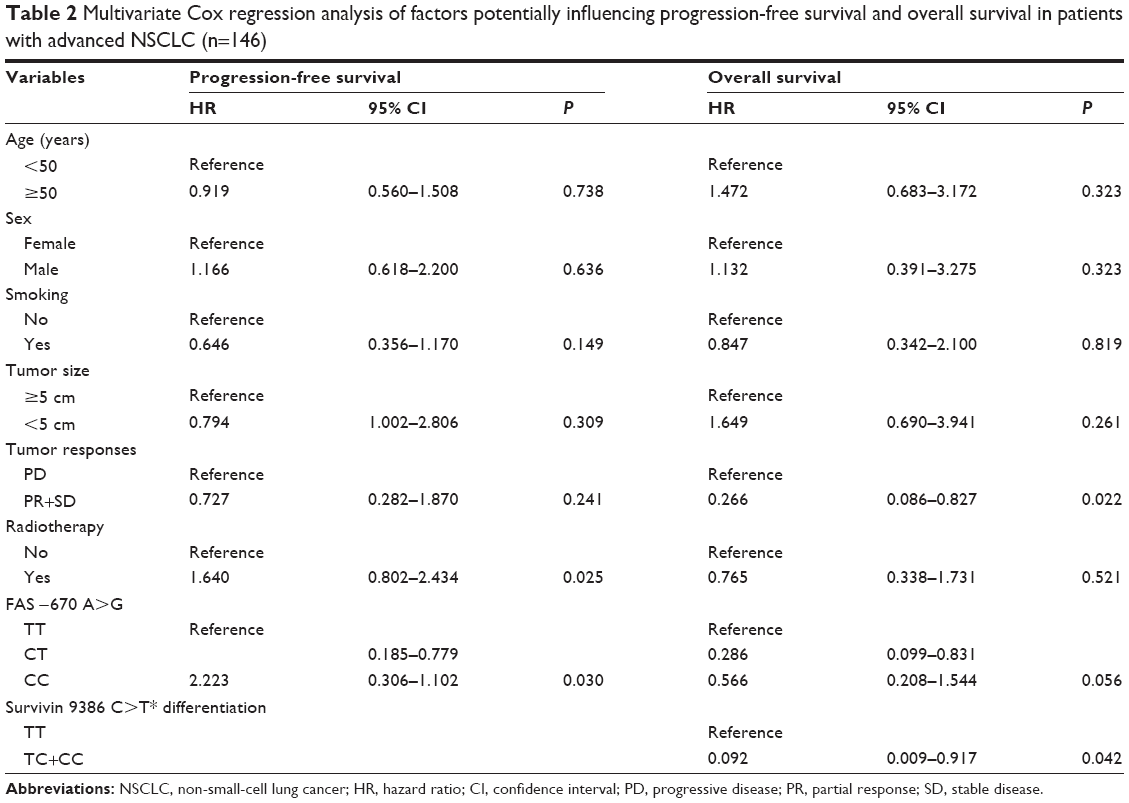 | Table 2 Multivariate Cox regression analysis of factors potentially influencing progression-free survival and overall survival in patients with advanced NSCLC (n=146) |
Discussion
Lung cancer is a health-threatening cancer that is highly malignant and responds poorly to existing treatments, especially in advanced-stage tumors. Unfortunately, only a small portion of patients show a good outcome after chemotherapy and other treatments. Therefore, in the present study, we sought to identify predictive and/or prognostic markers that could distinguish individuals who would benefit from chemotherapy treatment. Previous studies have confirmed that apoptosis plays an important role in cancer initiation and progression. Interestingly, SNPs within FAS, FASL, and survivin, which play a crucial role in the apoptosis pathway, have been associated with susceptibility to many cancers.8,17,19,22,23 Moreover, it has been demonstrated that an intact apoptotic pathway is associated with improved survival after platinum-based chemotherapy.24 Our study systematically evaluated the relationship between four functional SNPs in genes important for apoptosis – FAS −670 A>G, FASL −844 T>C, survivin −31 G>C, and survivin 9386 C>T – and chemotherapeutic response and prognosis in patients with advance NSCLC treated with platinum-based first-line chemotherapy.
FAS and FASL play important roles in carcinogenesis and cancer progression. When FAS binds to FASL expressed on cytotoxic T lymphocytes and natural killer cells, the extrinsic pathway of apoptosis is triggered in cancer cells. These molecules have been shown to be aberrantly expressed in many types of cancer,25 including cervical,22 esophageal,26 breast,23 and bladder cancer.27 To the best of our knowledge, this is the first study showing that patients with the CC genotype of the FAS −670 A>G polymorphism had a worse prognosis (PFS and OS) than those with a CT or TT genotype. These findings suggest that this SNP can serve as an indicator of prognosis. In addition, the CC genotype of FAS −670 A>G was associated with larger tumors.
The survivin gene, BIRC5, consists of four exons spanning 14.7 kb of chromosome 17q25,28 and is also a powerful prognostic marker in NSCLC.29 The aberrant overexpression of survivin inhibits normal immunosurveillance by decreasing tumor-cell apoptosis and thus favoring cell proliferation and tumor growth.30 Several studies15–19,21 have shown that SNPs found in the survivin gene-promoter region, such as 9386 C>T (rs2239680), are associated with risk for a variety of cancers. Our study also indicates that the survivin 9386 C>T polymorphism is a powerful prognostic marker in advanced NSCLC patients who were treated with platinum-based chemotherapy.
The FASL −844 T>C (rs763110) transition in the promoter region is located in a binding motif for the transcription factor CAAT/EBPβ,31 and increased FASL expression is strongly associated with FASL −844 T>C transition. However, this polymorphism had no impact on chemotherapy response or prognosis in patients with advanced NSCLC in our study, which may have been due to the small sample size. Additionally, among the four SNPs, the most widely studied SNP is the −31 G>C polymorphism (rs9904341),20 which has been associated with increased risk for various types of cancers.10,15–21 However, no connection of this polymorphism with chemotherapeutic response or prognosis in advanced NSCLC patients treated with platinum-based chemotherapy was found in our study.
One of the most important strengths of this study is that none of the patients had previously received chemotherapy or radiotherapy, which may have an influence on SNP genotypes. However, the patients did receive radiotherapy and target therapy postchemotherapy in the case of tumor progression. There are several limitations to this study. One limitation is that a portion of patients (approximately 20%) received radiotherapy or target therapy because of tumor progression, but there was no significant difference in the different genotypes of the four SNPs. Furthermore, although the association between the selected genetic variants and clinical outcome was adjusted by these covariates in the multivariate analysis, the FAS −670 A>G and survivin 9386 C>T polymorphisms were still powerful prognosis biomarkers for NSCLC patients treated with first-line platinum-based chemotherapy. Another limitation is that this study comprised retrospective research at a single hospital, and multicenter, large-scale, prospective research is needed to investigate these associations further.
In conclusion, the functional FAS −670 A>G and survivin 9386 C>T polymorphisms were associated with prognosis in advanced NSCLC patients treated with platinum-based chemotherapy. Our study provides novel insight into advanced NSCLC tumorigenesis, and reveals potential implications for individual treatment of lung cancer patients who carry different genotypes for these functional SNPs. However, the prognostic value of the two SNPs needs to be further validated in large, multicenter, randomized, controlled cohorts. Further investigation should evaluate potential strategies for altering FAS or survivin function to improve prognosis in patients with advanced NSCLC.
Acknowledgments
This work was supported by the Natural Science Foundation of Heilongjiang Province (grant Q14h160013), the Province of Important Technology and Science (2011C13039-1), and the National Natural Science Foundation of China (grant 81172081).
Disclosure
The authors report no conflicts of interest in this work.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. | ||
Bülzebruck H, Bopp R, Drings P, et al. New aspects in the staging of lung cancer. Prospective validation of the International Union Against Cancer TNM classification. Cancer. 1992;70:1102–1110. | ||
Schiller JH, Harrington D, Belani CP, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346:92–98. | ||
Hacker G, Vaux DL. A chronology of cell death. Apoptosis. 1997;2: 247–256. | ||
Thompson CB. Apoptosis in the pathogenesis and treatment of disease. Science. 1995;267:1456–1462. | ||
Zörnig M, Hueber A, Baum W, Evan G. Apoptosis regulators and their role in tumorigenesis. Biochim Biophys Acta. 2001;1551:F1–F37. | ||
Nagata S. Fas and Fas ligand: a death factor and its receptor. Adv Immunol. 1994;57:129–144. | ||
Xerri L, Devilard E, Hassoun J, Mawas C, Birg F. Fas ligand is not only expressed in immune privileged human organs but is also coexpressed with Fas in various epithelial tissues. Mol Pathol. 1997;50:87–91. | ||
Ambrosini G, Adida C, Altieri DC. A novel anti-apoptosis gene, survivin, expressed in cancer and lymphoma. Nat Med. 1997;3:917–921. | ||
Li F, Ambrosini G, Chu EY, et al. Control of apoptosis and mitotic spindle checkpoint by survivin. Nature. 1998;396:580–584. | ||
Khrunin AV, Khokhrin DV, Moisseev AA, Gorbunova VA, Limborska SA. Pharmacogenomic assessment of cisplatin-based chemotherapy outcomes in ovarian cancer. Pharmacogenomics. 2014;15:329–337. | ||
Kim JC, Ha YJ, Roh SA, et al. Novel single-nucleotide polymorphism markers predictive of pathologic response to preoperative chemoradiation therapy in rectal cancer patients. Int J Radiat Oncol Biol Phys. 2013;86:350–357. | ||
Shi TY, Cheng X, Yu KD, et al. Functional variants in TNFAIP8 associated with cervical cancer susceptibility and clinical outcomes. Carcinogenesis. 2013;34:770–778. | ||
Coulthard LR, Taylor JC, Eyre S, et al. Genetic variants within the MAP kinase signalling network and anti-TNF treatment response in rheumatoid arthritis patients. Ann Rheum Dis. 2011;70:98–103. | ||
Borbély AA, Murvai M, Szarka K, et al. Survivin promoter polymorphism and cervical carcinogenesis. J Clin Pathol. 2007;60:303–306. | ||
Hsieh YS, Tsai CM, Yeh CB, Yang SF, Hsieh YH, Weng CJ. Survivin T9809C, an SNP located in 3′-UTR, displays a correlation with the risk and clinicopathological development of hepatocellular carcinoma. Ann Surg Oncol. 2012;19 Suppl 3:S625–S633. | ||
Jaiswal PK, Goel A, Mandhani A, Mittal RD. Functional polymorphisms in promoter survivin gene and its association with susceptibility to bladder cancer in North Indian cohort. Mol Biol Rep. 2012;39: 5615–5621. | ||
Jang JS, Kim KM, Kang KH, et al. Polymorphisms in the survivin gene and the risk of lung cancer. Lung Cancer. 2008;60:31–39. | ||
Kawata N, Tsuchiya N, Horikawa Y, et al. Two survivin polymorphisms are cooperatively associated with bladder cancer susceptibility. Int J Cancer. 2011;129:1872–1880. | ||
Xu Y, Fang F, Ludewig G, Jones G, Jones D. A mutation found in the promoter region of the human survivin gene is correlated to overexpression of survivin in cancer cells. DNA Cell Biol. 2004;23:419–429. | ||
Yang X, Xiong G, Chen X, et al. Polymorphisms of survivin promoter are associated with risk of esophageal squamous cell carcinoma. J Cancer Res Clin Oncol. 2009;135:1341–1349. | ||
Sun T, Zhou Y, Li H, et al. FASL −844C polymorphism is associated with increased activation-induced T cell death and risk of cervical cancer. J Exp Med. 2005;202:967–974. | ||
Zhang B, Sun T, Xue L, et al. Functional polymorphisms in FAS and FASL contribute to increased apoptosis of tumor infiltration lymphocytes and risk of breast cancer. Carcinogenesis. 2007;28:1067–1073. | ||
Kim JG, Sohn SK, Chae YS, et al. TP53 codon 72 polymorphism associated with prognosis in patients with advanced gastric cancer treated with paclitaxel and cisplatin. Cancer Chemother Pharmacol. 2009;64: 355–360. | ||
Desmots F, Russell HR, Michel D, McKinnon PJ. Scythe regulates apoptosis-inducing factor stability during endoplasmic reticulum stress-induced apoptosis. J Biol Chem. 2008;283:3264–3271. | ||
Sun T, Miao X, Zhang X, Tan W, Xiong P, Lin D. Polymorphisms of death pathway genes FAS and FASL in esophageal squamous-cell carcinoma. J Natl Cancer Inst. 2004;96:1030–1036. | ||
Li C, Wu W, Liu J, et al. Functional polymorphisms in the promoter regions of the FAS and FAS ligand genes and risk of bladder cancer in south China: a case-control analysis. Pharmacogenet Genomics. 2006; 16:245–251. | ||
Ambrosini G, Adida C, Sirugo G, Altieri DC. Induction of apoptosis and inhibition of cell proliferation by survivin gene targeting. J Biol Chem. 1998;273:11177–11182. | ||
Rosato A, Menin C, Boldrin D, et al. Survivin expression impacts prognostically on NSCLC but not SCLC. Lung Cancer. 2013;79:180–186. | ||
Altieri DC. Survivin, cancer networks and pathway-directed drug discovery. Nat Rev Cancer. 2008;8:61–70. | ||
Sasaki T, Gan EC, Wakeham A, Kornbluth S, Mak TW, Okada H. HLA-B-associated transcript 3 (Bat3)/Scythe is essential for p300-mediated acetylation of p53. Genes Dev. 2007;21:848–861. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.