")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Prognostic Implications of the Admission Cardiac Troponin I Levels and Door-to-Balloon Time on Clinical Outcomes in Patients with ST-Segment Elevation Myocardial Infarction Undergoing Percutaneous Coronary Intervention
Authors Zhao L, Xin M, Piao X, Zhang S, Li Y, Cheng XW
Received 19 August 2021
Accepted for publication 6 December 2021
Published 7 January 2022 Volume 2022:18 Pages 31—45
DOI https://doi.org/10.2147/TCRM.S335045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Deyun Wang
Longguo Zhao, Minglong Xin, Xianji Piao, Shengming Zhang, Yanglong Li, Xian Wu Cheng
Department of Cardiology and Hypertension, Yanbian University Hospital, Yanji, Jilin, 133000, People’s Republic of China
Correspondence: Xian Wu Cheng
Department of Cardiology and Hypertension, Yanbian University Hospital, 1327 Juzijie, Yanji, 133000, People’s Republic of China
Email [email protected]; [email protected]
Minglong Xin
Department of Cardiology and Hypertension, Yanbian University Hospital, 1327 Juzijie, Yanji, 133000, People’s Republic of China
Email [email protected]
Background: The prognostic implications of the admission cTnI level and D2B time combined on in-hospital and 1-year heart failure (HF) and mortality in STEMI patients undergoing a primary percutaneous coronary intervention (PCI) are remain uncertain.
Methods and Results: We divided the consecutive 1485 STEMI patients who underwent PCI from January 2015 to October 2019 at our hospital into three groups based on their admission cTnI levels: normal group (< 0.1 ng/mL), middle group (0.1 to less than 3 ng/mL), and high group (≥ 3 ng/mL) and into two groups by their D2B times: > 90 min (> 90-D2B) and ≤ 90 min (≤ 90-D2B). During the in-hospital and 1-year follow-up periods, the incidence of composite clinical events increased significantly with the increase in the admission cTnI level (p < 0.05). In-hospital, the composite rate of death and HF events was significantly higher in the > 90-D2B group compared to the ≤ 90-D2B group (p = 0.006), but its influence disappeared in the 1-year follow-up (p > 0.05). A multivariable logistic analysis revealed that, in the ≤ 90-D2B group, with the exception of the cTnI ≥ 3 ng/mL patients, the cTnI level had no effect on in-hospital or 1-year outcomes; in > 90-D2B group, cTnI ≥ 3ng/mL increased outcomes in both periods.
Conclusion: High cTnI levels (≥ 3 ng/mL) on admission are independent of the D2B time for predicting in-hospital and 1-year cardiac events in STEMI patients undergoing PCI.
Keywords: cardiac troponin I, acute myocardial infarction, door-to-balloon time, cardiac death, heart failure
Introduction
Cardiac troponin levels are routinely evaluated in the setting of suspected or known acute myocardial infarction (AMI). Recent studies demonstrated that performing an in-practice evaluation of a 0/1-hour high-sensitive cardiac troponin T protocol embedded in emergency department care enabled a more rapid discharge of patients with suspected acute coronary syndrome (ACS)1 but did not reduce ischemic events over a 12-month follow-up.2 Baseline cardiac troponin I (cTnI) levels are frequently measured in an emergency department for an evaluation of suspected ACS,3 but doing so not a part of the formal diagnostic criteria. The release of cTnI exhibits predictable kinetics in the acute onset of an ST-segment elevation myocardial infarction (STEMI), and peak levels of cTnI are associated with both the ischemic quantity and the time of myocardium at risk.4–6 A prospective study demonstrated that low plasma cTnI levels measured at admission identified two-thirds of patients at very low risk of cardiac events.7 Despite the useful value of admission cTnI levels indicating a prehospital ischemic injury, there is limited information about the association between the admission cTnI levels and cardiac outcomes of STEMI patients undergoing a PCI.8 The prognosis after STEMI has improved significantly over the past two decades (even in patients with multivessel disease), due mainly to the use of early reperfusion therapies (ie, thrombolysis and angioplasty/stenting).9,10 Accumulating evidence indicates that early successful reperfusion can rapidly restore coronary artery patency and reduce the incidence of acute complications.11,12
The door-to-balloon (D2B) time is strongly associated with in-hospital and long-term mortality and is essential regardless of the length of time from a patient’s symptom onset and his/her presentation at an emergency department and regardless of the baseline risk of mortality, especially among patients whose anterior wall is infarction and patients who are high-risk patients.11 There is now a consensus regarding the effectiveness of regional medical chest pain centers’ efforts to reduce the D2B time.13 Previous large studies have confirmed that shortening the D2B time can improve the prognosis of patients with STEMI.14,15 However, other researchers observed that shortening the D2B time had no or very limited effect on the long-term mortality of patients with a STEMI,16 and few studies have focused on the evaluation of the combined prognostic implications of the D2B time plus the admission cTnI level on the outcomes of STEMI patients undergoing a PCI.17
In this context, we examined the association between plasma cTnI levels at admission plus the D2B time and the incidence of cardiac death and heart failure (HF) in patients who underwent a primary PCI for the treatment of a STEMI.
Patients and Methods
Patients and Groups
Our study cohort for this retrospective analysis was comprised of patients who presented to the emergency department and/or Chest Pain Center of Yanbian University Hospital (Yanji, Jilin PR. China) and underwent a primary PCI for a STEMI over the 4-year period from January 2015 to October 2019. Yanbian University Hospital Cardiovascular Center performs the PCI treatments for STEMI patients throughout Yanbian Prefecture. The data of the STEMI inpatients were collected from the electronic medical record system of Yanbian University Hospital. The study protocol was approved by the ethics committee of the Yanbian University Hospital, and written informed consent was obtained from all patients.
Inclusion and Exclusion Criteria
We included all of the STEMI patients who were directly admitted to this Center or were transferred to the Center by any of the 12 cooperative medical facilities for the patient’s PCI. We identified the STEMI patients based on their clinical symptoms and standard electrocardiogram (ECG). We excluded STEMI patients who suffered prehospital cardiac arrest or had severe valvular disease or cardiomyopathies, and those with chronic kidney disease on dialysis, or a history of PCI or coronary artery bypass graft (CABG). We also excluded patients without baseline cTnI levels that were obtained at their hospital presentation and those whose cases exceeded the PCI time window or failed the PCI or/and underwent CABG, and patients who received preoperative fibrinolytic therapy or had missing demographic or clinical data for the estimation of predicted mortality risk. The cases of the final total 1485 STEMI patients who underwent a primary PCI within 12 hr of symptom onset and within 6 hr of admission were included in the current analysis (Figure 1).
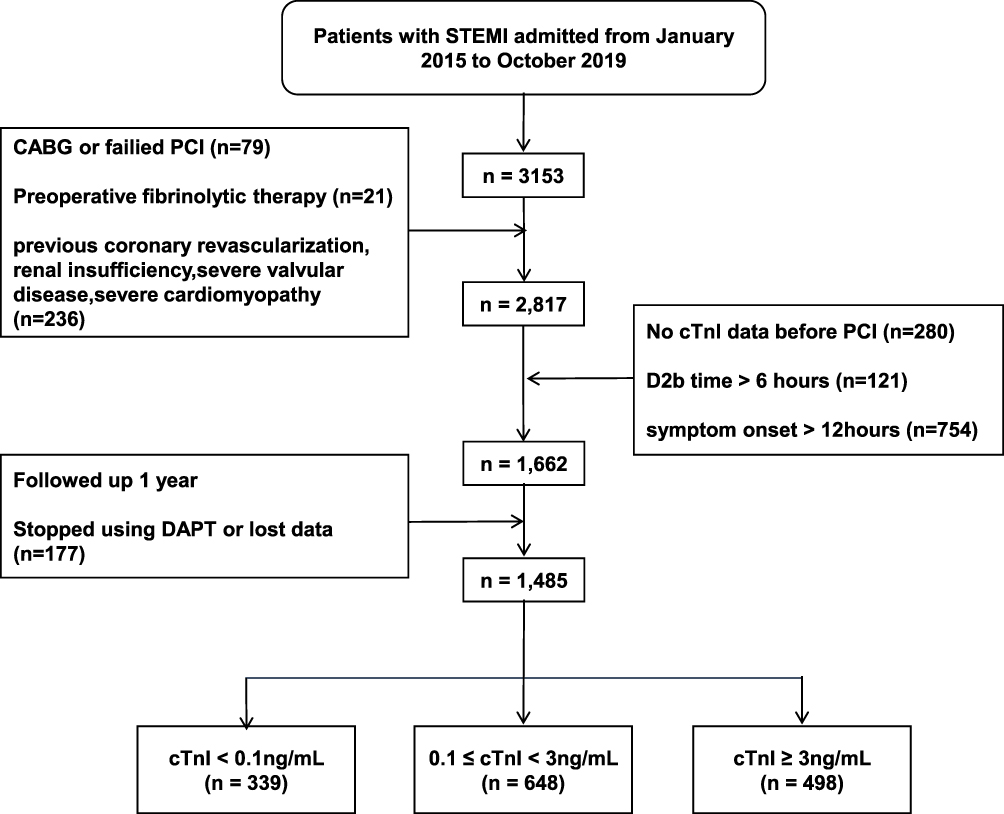 |
Figure 1 Patient inclusion diagram for the study cohort. Abbreviations: CABG, coronary artery bypass graft; cTnI, cardiac troponin I; PCI, primary percutaneous coronary intervention; STEMI, ST-segment-elevation myocardial infarction. |
Definitions
Diabetes mellitus was confirmed if the patient had a fasting plasma glucose concentration >126 mg/dL, hemoglobin A1c level ≥6.5%, and/or a history of a previous diagnosis of diabetes or the use of any anti-hyperglycemic medication. Hypertension was diagnosed as diastolic blood pressure >90 mmHg, systolic blood pressure >140 mmHg, and/or having received treatment for hypertension. “Smoking history” included current smoking (still smoking within the last 1 year) and non-smoking (had quit smoking ≥1 year ago or never smoked). A “family history of ischemic heart disease” included any immediate family member (parent, sibling, or child) with angina, myocardial infarction, sudden cardiac death of no apparent cause, or a history of coronary artery bypass grafting or PCI.
Group Dividing
According to the cut-off values of admission cTnI levels (0.1 and 3.0 ng/mL), we divided the 1485 patients were divided into the following three groups: the Normal group (NG), in which the patient’s admission cTnI level was below the upper reference limit of <0.1 ng/mL; the Middle group (MG), with a cTnI level that was higher than the upper reference limit and less than 3 ng/mL; and the High group (HG), in which the cTnI level was ≥3 ng/mL. We further divided the patients into two groups based on their D2B times on admission: the more-than 90 min (>90-D2B) group and the ≤90 min (≤90-D2B) group.
A blood sample was collected prior to any endovascular intervention for an elevation of a patient’s lipid profile, inflammatory profile, or hemoglobin A1c (HbA1c). The gender, age, body mass index, smoking history, systolic and diastolic blood pressure values, disease(s), and medication histories were recorded for each patient.
Laboratory Parameters
Baseline cTnI levels were evaluated for all patients at their admission (before PCI) with the use of Yanbian University Hospital’s standard clinical troponin I assay (#1100, GeTein Biomedical, Nanjing, China). Values of cTnI from a transferring facility were not included in the study. Serum creatinine, low-density lipoprotein (LDL), high-density lipoprotein (HDL), N-terminal pro-B-type natriuretic peptide (NT-proBNP), creatine kinase-MB (CK-MB), and CK, and HbA1c were measured in the clinical laboratory of Yanbian University Hospital. Two-dimensional and Doppler echocardiography was performed within the first 72 hr in the critical care unit and/or the department of cardiology to determine the patient’s left ventricular ejection fraction.
Angiographic Analysis and PCI Treatment Strategy
All patients received a loading dose of dual anticoagulation drugs (300 mg of aspirin and 600 mg of clopidogrel or 180 mg of ticagrelor) before their PCI and were administered an intravenous injection of unfractionated heparin, which is a conventional treatment followed by PCI to achieve adequate blood flow of the infarct-related artery. The other stenotic coronary arteries were not targeted for any intervention, unless the arter(ies) were affected by cardiogenic shock. Procedural decisions such as the size and length of the stent (a drug-eluting stent) and the use of adjunctive pharmacotherapy (including glycoprotein (Gp) IIb/IIIa receptor antagonists) were made by the hospital’s cardiac interventional therapy physicians. A successful PCI was defined as residual stenosis <20% without major complications (eg, stent thrombosis, need for emergent CABG or repeat PCI, coronary dissection or rupture, and death). An antiplatelet regimen was prescribed to all patients: lifelong aspirin (100 mg/d) and clopidogrel (75 mg/d) or ticagrelor (90 mg/d) for ≥12 months. Telephone interviews were carried out to determine both the use and the duration of dual antiplatelet therapy (DAPT), and patients who did not meet the standard usage of drugs were removed from the present analyses.
Follow-Up
Clinical follow-up data were obtained from hospital records and telephone interview records with the patients and/or their relatives. Regular outpatient clinic visits were performed at 1, 3, 6, and 12 months after discharge, and if a patient did not visit on the scheduled date, a telephone interview was conducted to assess adverse outcomes. Causes of death were determined by the medical record or death certificate.
End Points
The study’s primary major adverse cardiovascular events were a heart failure (HF) event and cardiovascular mortality during the 1-year follow-up period. We defined HF as admission to a hospital for worsening HF requiring intravenous drug treatment. Cardiac death was defined as having been caused by life-threatening arrhythmia, myocardial infarction (MI), cardiac arrest, or congestive HF or other cardiac events. We also calculated the in-hospital HF and mortality rates.
Statistical Analyses
Categorical variables are expressed as frequencies and proportions and were compared by Pearson’s chi-square or Fisher’s exact test. Continuous variables with normal distribution are presented as the mean and standard deviation (SD), and variables that did not fit a normal distribution are presented as the median and interquartile range (IQR). Data with a normal distribution were compared by unpaired Student’s t-test or a one-way analysis of variance (ANOVA), and non-normally distributed variables were compared by the Mann–Whitney U-test or Kruskal–Wallis H-test.
We performed a multivariate analysis with a Cox proportional hazard model to analyze the prognostic effects of both the baseline troponin I and the baseline D2B time for different time-periods. The factors that related at the p<0.1 level were selected as independent variable candidates [ie age, sex, Chinese Korean, Killip class, hypertension, current smoke, NT-proBMP, left ventricular ejection fraction (LVEF), infarct-related artery (IRA): left main/left anterior descending artery (LAD), MVD, multi-vessel disease, no flow, Gensini score, O2B time, D2B time ≤ 90 min, cTnI ≥ 3 ng/mL] for a multiple logistic regression analysis, which was used to evaluate the independent contributions of clinical parameters to 30-day and 1-year composite events (death/HF). Multiple regression model includes all variables at baseline with p<0.05 by univariable analysis. The results are presented as the adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) and p-values. The incidence of composite outcomes in each group during the different time-periods was compared by a Kaplan-Meier survival curve analysis with a stratified Log rank test. All analyses were two-tailed, with clinical significance defined as p<0.05. All statistical analyses were performed with SPSS 26.0 software (SPSS, Chicago, IL).
Results
Baseline Characteristics of the Study Population
A total of 3153 patients with a STEMI were transferred (45.9%) or admitted (54.1%) directly to the PCI-capable emergency department/Chest Pain Center of Yanbian University Hospital and underwent a primary PCI. Patients were excluded if they had a treatment delay of symptom onset-to-door (O2D) >12 hr (thus exceeding the PCI time window, n=754) or a D2B time >6 hr (n=121), and if they failed a PCI or/and underwent CABG (n=79) or received thrombolysis therapy (n=21). A total of 516 patients met one of the other exclusion criteria (no cTnI data, n=280; had one of the indicated disease histories, n=236), and thus the final cohort was 1485 patients. Figure 1 provides the patient inclusion flow diagram.
The median cTnI level for all of the patients was 3.2 ng/mL (IQR: 1.3–15.9 ng/mL). Of this cohort, 339 (22.8%) patients had initial cTnI levels that were undetectable (<0.1 ng/mL). The baseline characteristics, laboratory findings, and angiographic characteristics of the patients according to their admission cTnI levels are summarized in Table 1. The overall mean age was 59.5 ± 11.3 years; 1138 patients (76.6%) were men, and 481 were Chinese Korean (32.4%). The median O2D time was 5.3 hr (IQR: 3.9–7.1 hr). The median D2B time was 89 min (65–134 min).
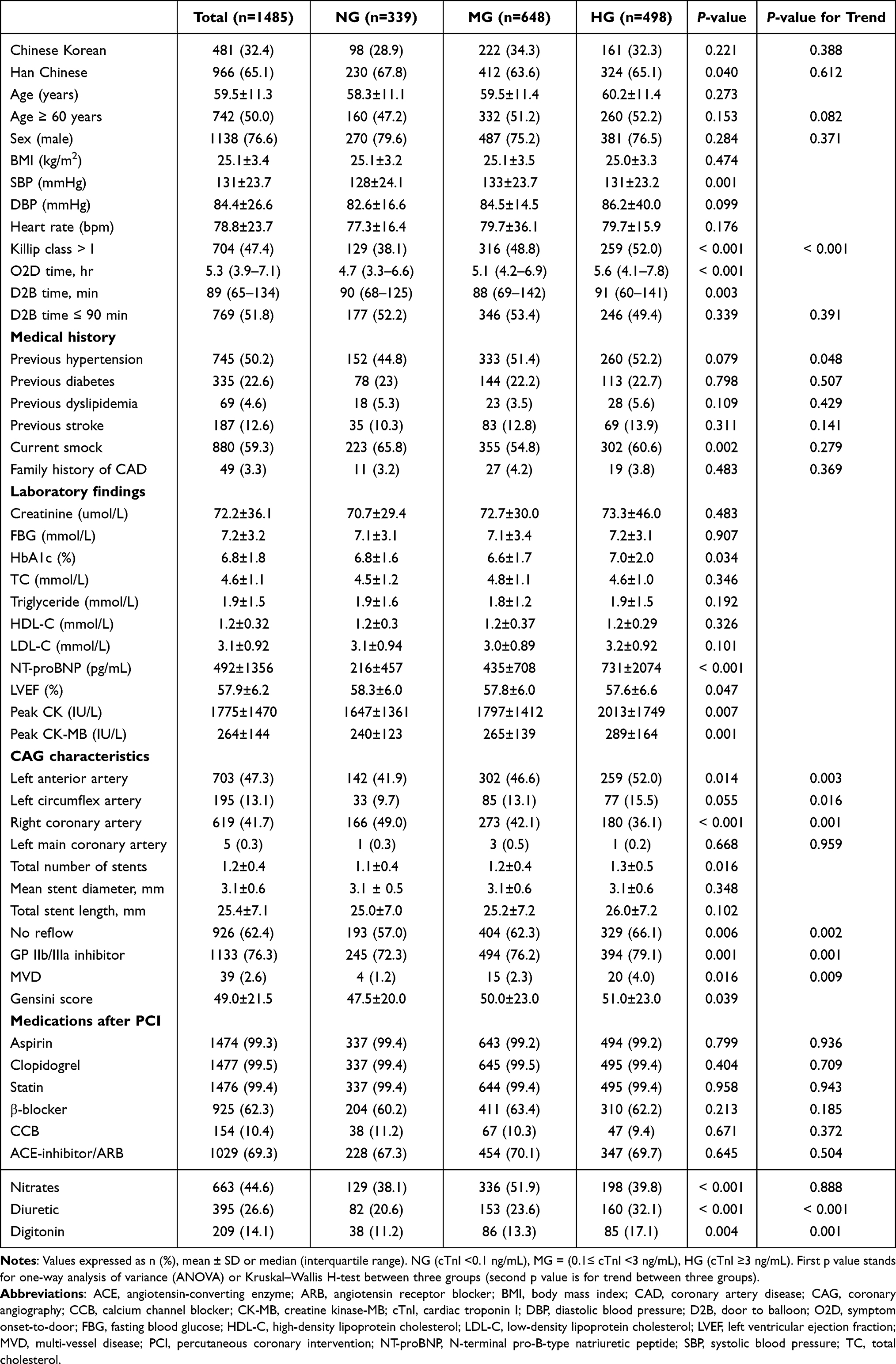 |
Table 1 Baseline Demographic and Clinical Characteristic of Patients with Presentation cTnI Levels |
The patients’ admission levels of NT-proBNP, peak CK, and peak CK-MB, and peak CK-MB increased with the increase in the admission cTnI level. The rates of patients with LAD disease, two or three-vessel disease, the total number of stents, no reflow, and Killip class >I from initial angiography were all higher in the High (admission cTnI level) group. The rates of DAPT and statins use were >99% in all three cTnI groups and both D2B groups. There were differences in the usages of diuretics, digitonin, and nitrates due to the occurrence of complications such as HF and cardiogenic shock during hospitalization between three experimental groups. The baseline characteristics of the patients according to D2B times are summarized in Table 2. With exception of NT-proBNP, there were no significant differences in other parameters between the two D2B groups.
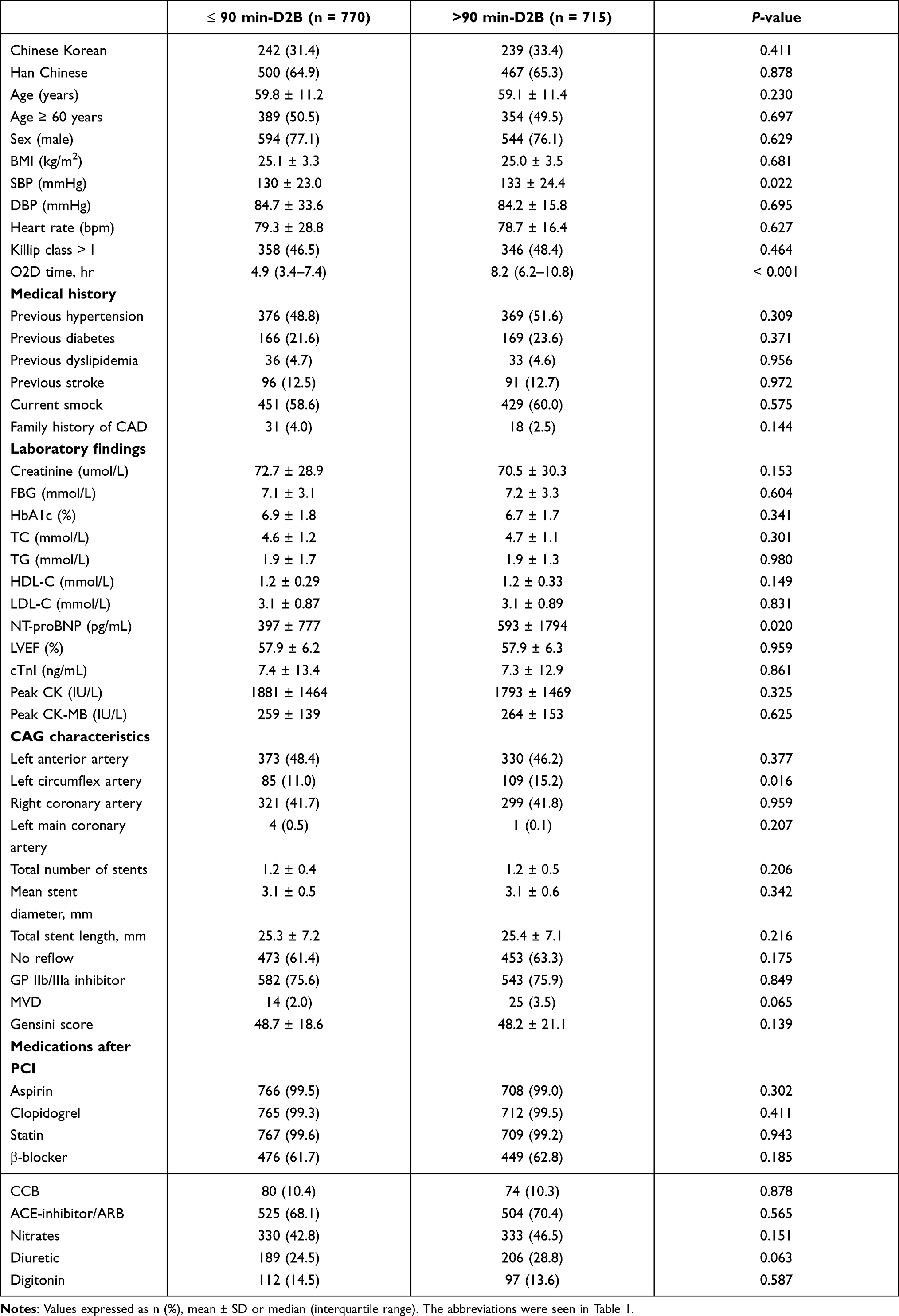 |
Table 2 Baseline Characteristics of the Patients with D2B Time |
Clinical Outcomes
During the 1-year follow-up, 177 patients who stopped using DAPT due to side effects or other reasons and those with lost data were excluded from the analysis of the follow-up data. The composite clinical events that occurred during the in-hospital period and during the 1-year follow-up stratified by the admission cTnI levels are presented in Figure 2. The following were significantly increased with the increase in the admission cTnI level: the incidence of 30-day mortality and HF (Normal, 3.5% vs Middle, 6.0% vs High, 10.2%) and the incidence of the overall 12-month cardiac death plus HF hospitalization (8.3% vs 9.6% vs 15.4%) (log-rank p<0.001 for each, Figure 2).
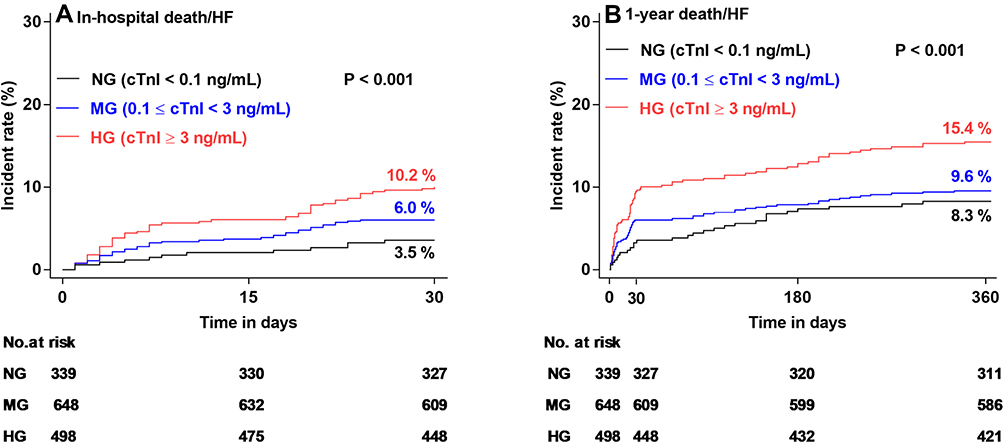 |
Figure 2 The incidence of death/HF (heart failure) composite events during the in-hospital and follow-up time-periods and the patients’ baseline troponin I levels. (A) In-hospitalization (30 days). (B) The 1-year follow-up. |
Consistently, we observed that the incidence of individual clinical events was also markedly increased with the increase in the patients’ admission cTnI levels (Table 3). Compared to the Normal and Middle cTnI groups (<0.3 ng/mL), the Cox regression analysis revealed that the composite and individual clinical events were significantly increased in the High cTnI group, and the overall 30-day in-hospital (p=0.002) and 1-year composite outcomes (p<0.001) were significantly increased by 2.3- or 2.7-times in the High group (Table 3), suggesting that STEMI patients’ admission cTnI levels are closely correlated with composite and individual clinical events.
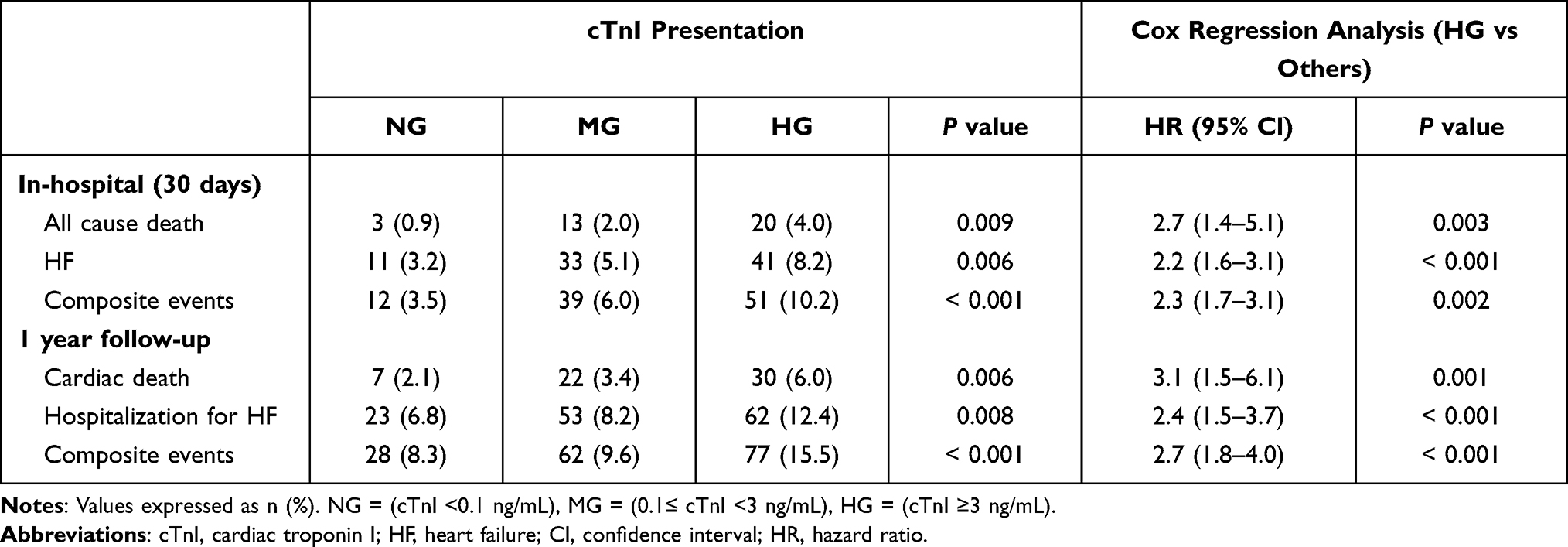 |
Table 3 30-Day and 1-Year Clinical Outcomes Stratified by Admission cTnI Groups and Cox Regression Analysis |
We next evaluated the impact of the D2B time on the composite clinical outcomes. Compared to the ≤90-min D2B group, the >90-min D2B group had significantly increased mortality and HF during the in-hospital period (5.2% vs 8.5%, log-rank p=0.006, Figure 3A). In contrast, there is no significant difference in mortality or HF between the D2B groups during the 1-year follow-up (10.1% vs 12.4%, log-rank p=0.146, Figure 3B). The data of individual clinical events yielded the same conclusion (Table 4). The areas under the curve (AUCs), the measures of each model’s predictive ability, and the receiver operator characteristic curve (ROC) of the potential models are presented in Figure 4. The ROC data show that the cTnI level and the D2B time can predict the 30-day composite incidence (AUC: 0.63, p<0.001; AUC: 0.58, p=0.001) (Figure 4A). As shown in Figure 4B, the cTnI level still has predictive value for the incidence of 1-year composite events, whereas the D2B time exhibits very limit predictive value on it.
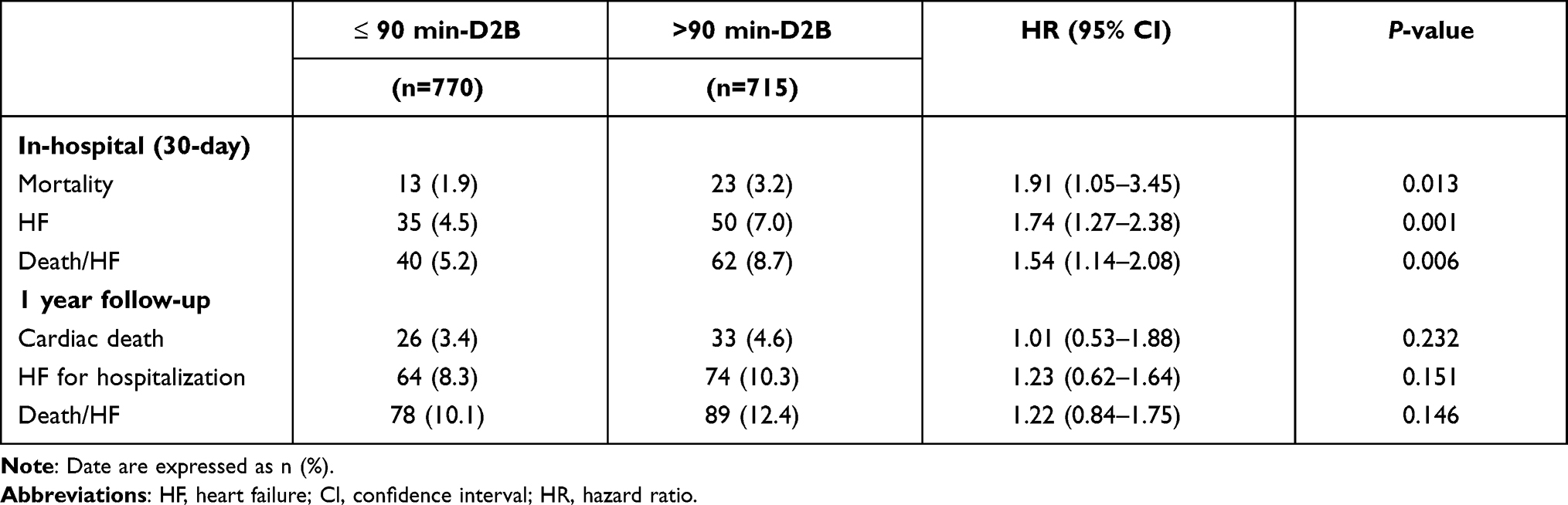 |
Table 4 30-Day and 1-Year Individual and Composite Clinical Event of Groups According to D2B Time |
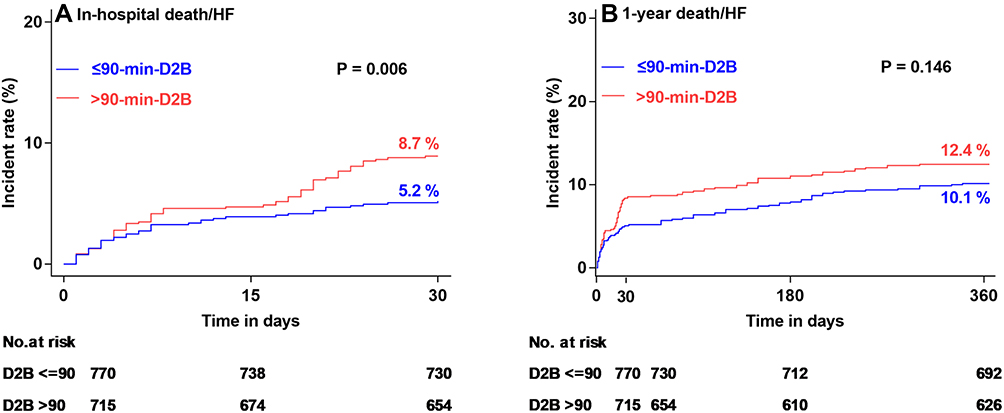 |
Figure 3 The incidence of composite events during the (A) 30-day-hospitalization and (B) 1-year follow-up according to D2B time groups. |
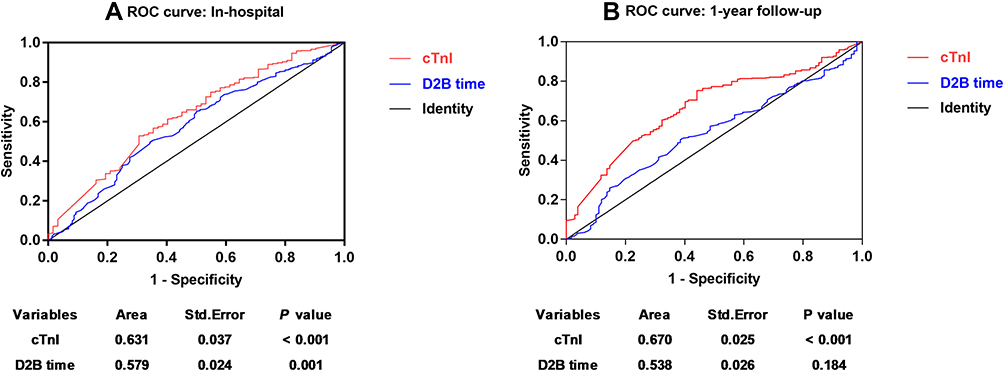 |
Figure 4 Receiver-operating curve (ROC) analysis showing the predictive cutoff value of troponin I/D2B time for hospitalization and 1-year death/HF composite events. (A) In-hospitalization (30 days). (B) The 1-year follow-up. |
The unadjusted estimated risk for composite clinical events during the pre-specified times and according to the admission cTnI level and D2B time is illustrated in Figure 5. When the D2B time was ≤90-min, even an elevated high admission cTnI level was not effective for predicting 30-day hospital composite events (Figure 5A). When the follow-up time was extended to 1 year, D2B time can predict outcomes (HR 2.8, 95% CI: 1.25–5.99, p=0.01). In the >90-min-D2B group analysis, this prognostic impact on composite clinical events by a high cTnI level was present not only for the in-hospital period (HR 2.9, 95% CI: 1.57–5.56, p<0.001) but also for the 1-year follow-up period (HR 3.0, 95% CI: 1.26–7.41, p=0.008) after STEMI (Figure 5B).
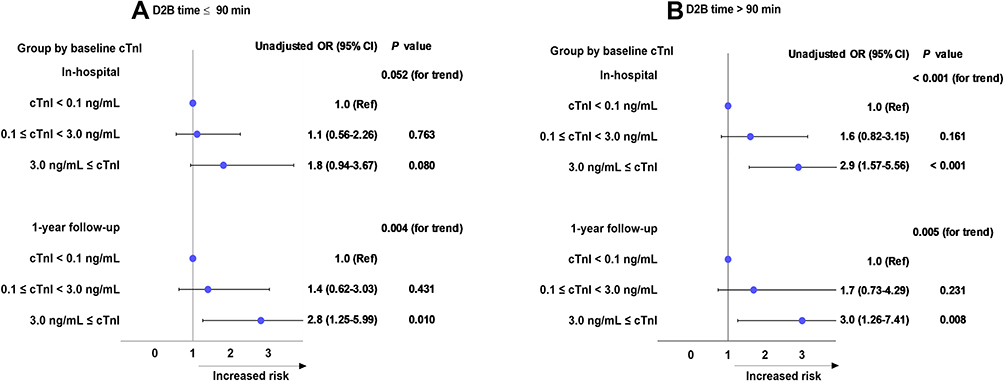 |
Figure 5 Unadjusted estimated risk for composite clinical events during the in-hospitalization and follow-up periods according to admission cTnI. (A) D2B time ≤90 min. (B) D2B time >90 min. |
Univariate and Multivariate Analysis
We performed univariate and multivariate analyses to determine the correlation between several variables and the 30-day and 1-year composite events. The results are presented in Table 5. With the exception of the Gensini scores and multi-vessel disease numbers, the investigated demographic and biological parameters exhibited predictive value for the incidence of 30-day composite events: sex, age ≥60 yrs, Chinese Korean, Killip class >I, hypertension, current smoking, NT-proBNP, LVEF, IRA-left main/LAD, no flow, O2D time, D2B ≤90 min, and cTnI (Table 5). The results of the multivariate analysis demonstrated that among those positive parameters, the cTnI level as well as age ≥60 yrs, Killip class >I, NT-proBNP, LVEF, IRA-left main/LAD, no flow, and D2B ≤90 min can be used to predict 30-day composite events.
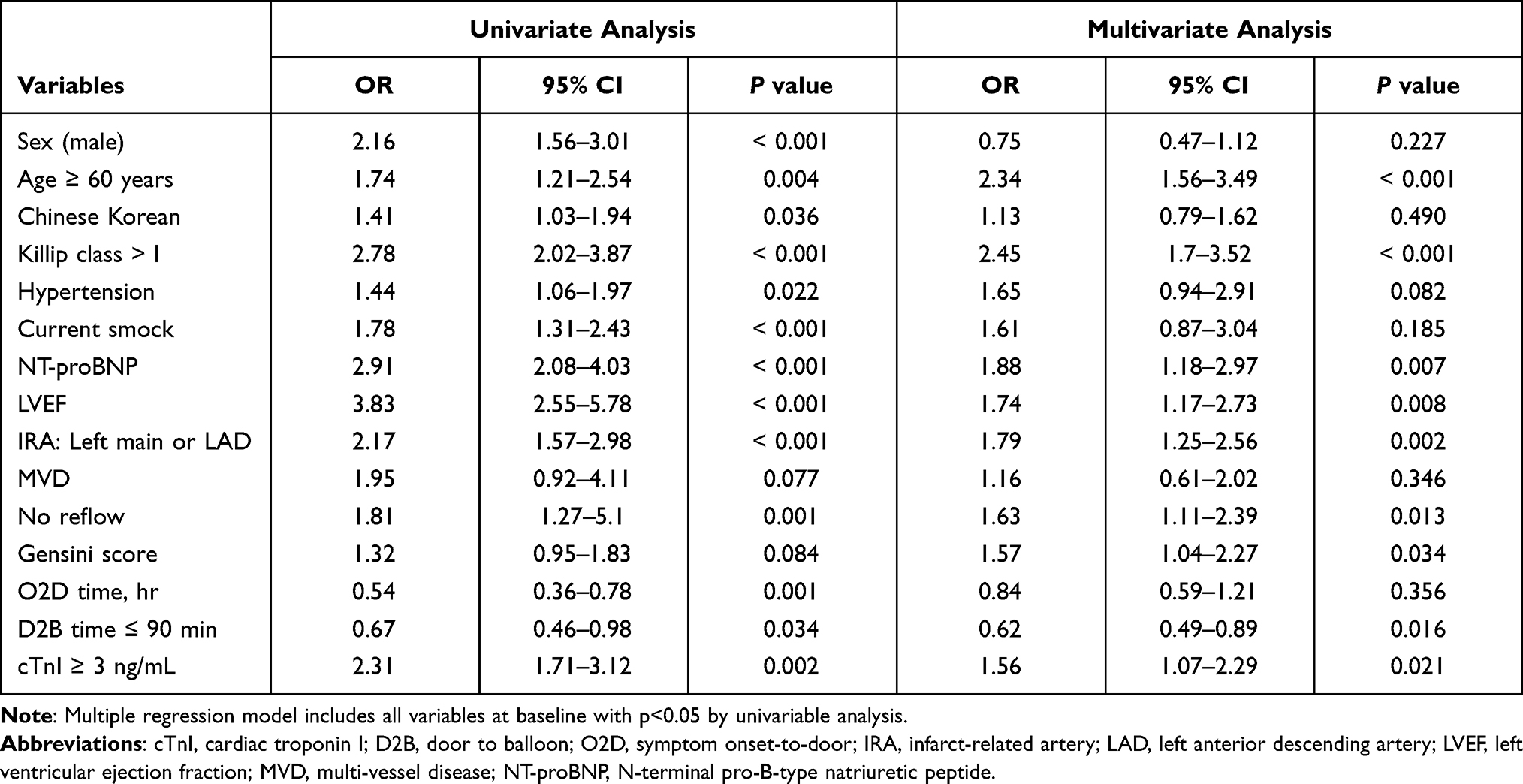 |
Table 5 Independent Effects of 30-Day Composite Events (Death/HF) According to Multivariable Logistic Regression Analysis |
During the 1-year follow-up period, as shown in Table 6, with the exceptions of Chinese Korean status, Gensini score, MVD number, O2D time and D2B time, 10 demographic and cardiac laboratory parameters exhibited predictive value for the composite events: sex, age ≥60 yrs, Killip class >I, hypertension, current smoking, NT-proBNP, LVEF, IRA-left main/LAD, no flow and cTnI. However, the multivariate analysis demonstrated that only the cTnI level and four other parameters (age ≥60 yrs, NT-proBNP, LVEF, and IRA-left main/LAD) have predictive value.
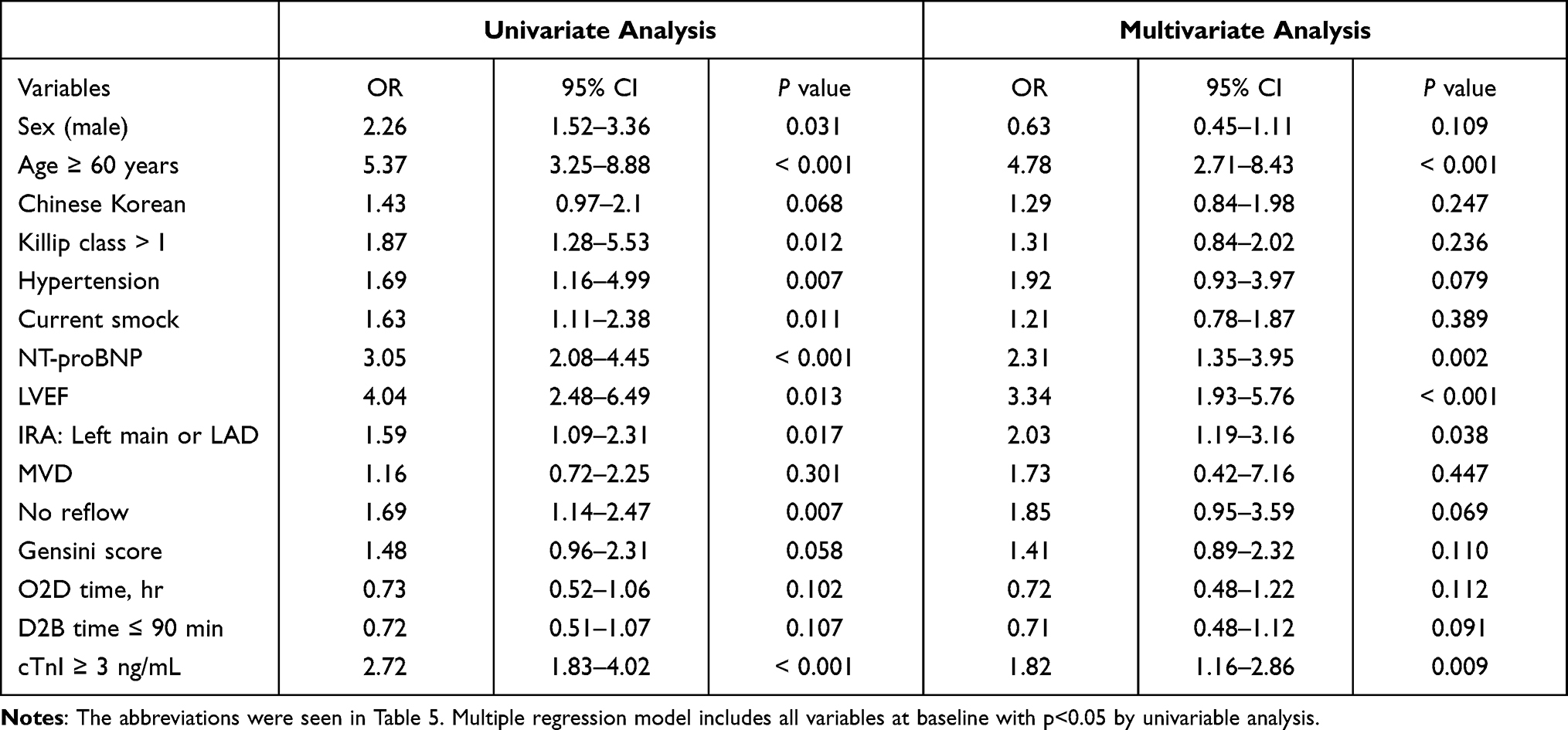 |
Table 6 Independent Effects of 1-Year Composite Events (Death/HF) According to Multivariable Logistic Regression Analysis |
The adjusted estimated risks for composite clinical events during the pre-specified time-periods and according to the patients’ admission cTnI levels and D2B times are depicted in Figure 6. As anticipated, an increased admission cTnI level can be used to predict the occurrence of composite clinical events during the 30-day in-hospital period and the 1-year follow-up period after STEMI (Figure 6A). As shown in Figure 6B, in the analysis of the D2B times (≤90 min vs >90 min), the prognostic impact of a shorter D2B time on composite mortality and HF by the admission cTnI level was present only for the 30-day in-hospital period in STEMI patients undergoing a primary PCI; its prognostic impact disappeared during the 1-year follow-up period.
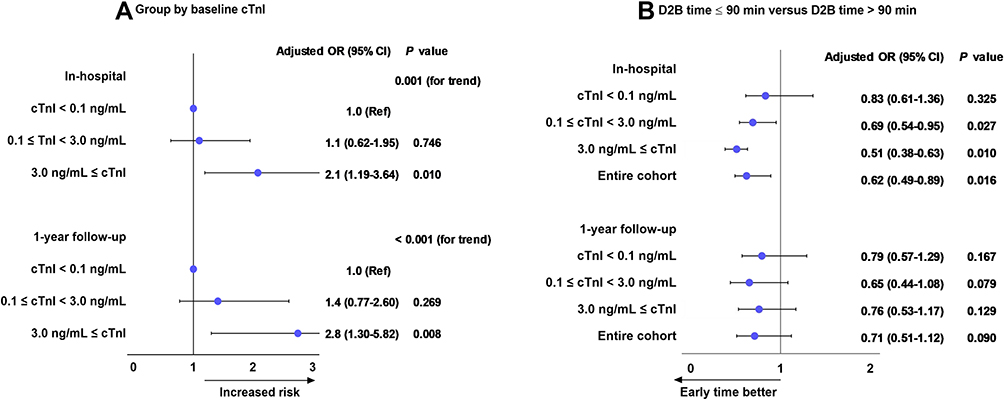 |
Figure 6 Adjusted estimated risk for composite clinical events during in-hospitalization and follow-up periods time-periods according to admission cTnI levels (A) and D2B time (B). Results are adjusted for the following variables: sex, age ≥60 years, nationality (Chinese Korean), Killip class >I, previous hypertension, current smoking, NT-proBNP, LVEF, IRA (infarct-related artery) as the left main artery or LAD (left anterior descending artery), no-reflow, Gensini score, O2D (symptom onset-to-door) time, and D2B (door to balloon) time ≤90 min. |
Discussion
The results of our study confirm that an elevated/high troponin I concentration at admission is a strong predictor of increased 30-day and 1-year death/HF composite events in patients with STEMI undergoing a primary PCI. Our analyses also revealed that (i) the effect of the D2B time on the prognosis was limited to the 30-day in-hospital period, and (ii) early revascularization attenuated the incidence of individual and composite clinical outcomes. After a coronary artery’s occlusion, the main pathogeneses are myocardial necrosis, myocardial interstitial congestion, edema, and a massive infiltration of inflammatory cells. The infarct size is an important indicator for predicting the prognosis of patients with a myocardial infarction. The patient-level analysis of 10 randomized primary PCI trials (total 2632 patients) sought to determine the strength of the relationship between infarct size assessed early after primary PCI in STEMI and subsequent all-cause-mortality, reinfarction, and hospitalization for HF by either technetium-99m sestamibi single-photon emission CT or cardiac MRI and to all-cause mortality and hospitalization for HF within 1 year.18 Other studies have shown that the cumulative release of troponin (a specific and sensitive index of the myocardium) into the circulation is closely related to the infarct size.4–6,8
In addition, the data from the US National Cardiovascular Data Registry (NCDR) Cath PCI database of 14,061 patients showed that the admission troponin level was an effective tool for the prediction of in-hospital death.19 This is consistent with our present results. Although we did not have the patients’ cardiac MRI data, our analyses revealed that the peak CK-MB level, Gensini score, no reflow, and LAD lesions in the High cTnI group were significantly higher than those in the Normal and Middle groups. These results suggest that an elevated/high cTnI level is closely related to more extensive myocardial damage.
It is thought that cTnT and cTnI levels rise 3–4 hr after the onset of an AMI. The kinetics of troponin release dictate that the levels observed in the early acute phase are closely dependent on the time of myocardial ischemia.2 The O2B time was reported to be associated with troponin elevation, though only modestly.20,21 The determination of the ischemic time based on diseases and medication histories can be problematic for some patient groups (eg, older individuals, women, and diabetic individuals) who are more likely to present with atypical symptoms.22,23 Mahmoud et al showed that the “cardiac biochemical ischemic time” based on troponin levels frequently disagreed with — and was substantially longer than — the conventional cardiac ischemic time derived from the patients’ symptom records in their retrospective cohort.24 In our present cohort, the median O2D time in the patients with a cTnI level below the detection limit was 4.7 hr. Moreover, the median time difference between the other groups was <1 hr. The poor reliability of symptom duration as an indicator of the cardiac ischemic time may, in part, explain why several previous clinical studies did not show a close link between mortality and the O2B time in patients with STEMI.11,14 Accumulating evidence indicates that the progression to STEMI in many patients may occur by a more dynamic and prolonged process of atherosclerotic plaque instability, thrombosis/distal embolization, and the restoration of flow, which is better appreciated with objective admission biomarker data.25,26
The importance of the prompt restoration of coronary patency in STEMI patients is well known. However, there have been conflicting results about the relative prognostic importance of the O2B and D2B times. The US National Registry of Myocardial Infarction, which has enrolled >20,000 patients, reported that a shorter D2B time but not a shorter O2B time was associated with lower in-hospital mortality.11 A study of 5243 patients with STEMI treated at 20 tertiary hospitals in Korea reported that shortening of the D2B time was significantly associated with reduced 1-year mortality.12 In contrast, in the CREDO-Kyoto (Coronary Revascularization Demonstrating Outcome Study in Kyoto) MI registry (n=3391), an O2B time >3 hr was associated with a higher risk of a composite of death and congestive HF, whereas a shorter D2B time was associated with a lower risk of death and congestive HF, only in patients with early presentation (O2D time <2 hr). There is a large body of literature on the relationship between the D2B time and mortality.11–13 Two types of clinical study design have been used. In patient-level investigations, the risk of mortality was examined using large-scale observational cohorts, and a positive correlation was consistently observed between a lower risk of mortality and shorter D2B times.11–13 The other type of investigation design is population-level studies in which institution-wide and nation-wide differences in clinical outcomes were evaluated during the application of national programs to decrease the 30-day hospital delay, with the D2B time as the target quality examination. Some population-based studies showed that reducing the D2B time in STEMI patients undergoing primary PCI was not associated with an amelioration of mortality.19,27,28 These findings raised questions about the value of reducing the D2B time. Some positive observations have indicated that a shorter D2B time might be a surrogate marker for low-risk patients or may reflect the operator and/or institutional expertise. In retrospective analyses of the US National Cardiovascular Data Registry, Nallamothu et al reported that although shorter D2B times were consistently associated with lower mortality in a population-based cohort, an increasing proportion of high-risk patients undergoing a primary PCI might have largely contributed to secular trends of improved mortality rates.19 The results of our present analyses demonstrated that a D2B time <90 min has a prognostic impact on composite and individual clinical events during the 30-day in-hospital period but not during the 1-year follow-up period. The Cox regression and ROC analysis yielded the same conclusion, suggesting that reducing the D2B time can provide a greater cardiovasculoprotective benefit in STEMI patients undergoing a primary PCI. This notion was further supported by the data from univariate and multivariate analyses revealing that the shorter D2B time (≤90-min) was effective for predicting composite event development during the 30-day in-hospital period, whereas this prognostic impact on death/HF was no longer present at 1 year after the patients’ AMIs.
Patient- and population-level clinical studies have focused on the admission cTnI level or the D2B time alone to evaluate the prognostic impact on all-cause mortality and major adverse cardiac events during the in-hospital and long-term follow-up periods, and they achieved a degree of consensus.12–14 To the best of our knowledge, the present study is the first to evaluate the combines prognostic implications of the admission cTnI level and the D2B time on in-hospital and 1-year mortality and HF hospitalizations in STEMI patients undergoing a primary PCI. Our observation of the unadjusted estimated risk for composite clinical events during the pre-specified times and according to the admission cTnI level and D2B time indicates that when the D2B time is ≤90 min, even an elevated high admission cTnI level was not effective for predicting 30-day hospital composite events, whereas this shorter D2B time can predict 1-year composite outcomes after PCI. In the >90-min D2B subgroup analysis, this prognostic impact on composite clinical events was present for both the in-hospital and 1-year follow-up periods. Interestingly, the results of the present evaluation of the adjusted estimated risk for composite clinical events demonstrated that the protective effect of even a shorter D2B time on composite mortality and HF by the admission cTnI level was present only for the 30-day hospital period in STEMI patients undergoing a primary PCI, and this protective impact disappeared during the 1-year follow-up period. Collectively, the combined evaluation of the admission cTnI level and D2B time could be more objective and suitable to evaluate the prognoses of STEMI patients after PCI. We do not believe that these findings are sufficient to recommend this combined evaluation as better than the single-variable analyses at present, but further prospective studies are warranted.
Study Limitations
Our study has several limitations that should be addressed. (1) The admission cTnI levels were collected from 1485 participates with STEMIs. The release of troponin in a STEMI involves hemodynamic changes, and the measurement of the cTnI level at a single time point is not sufficient or accurate enough to determine the cardiac ischemic time and infarct size. We hope that our findings will spur further investigation using the cTnI levels obtained at multiple time points as an objective tool for comparison. (2) Because of the non-randomized nature of the registry data, the characteristics of the groups divided by the admission cTnI level and D2B time showed substantial differences at the baseline. The determination of treatment strategies based on the attending physicians’ discretion also introduced a possibility of selection bias. (3) In the present cohort, 43.9% of the patients were transported to our hospital from one of 12 cooperating medical facilities, and 1050 patients with a treatment delay of O2D >12 hr or D2B time >6 hr were excluded. More than 800 patients met one of the other exclusion criteria and were also excluded from the cohort. These factors may have influenced our results and conclusions. (4) We did not conduct a comparison between the impacts of the O2D time and the D2B time on composite clinical events in this cohort. (5) Our analyses were based on observational data, and there is no definite ground to claim causality. We attempted to reduce the confounding effects through vigorous risk adjustment; however, we could not preclude the possibility of non-measured confounding factors (eg, prehospital system delay, prior peripheral vascular disease, and the index of failed reperfusion other than epicardial TIMI [thrombolysis in MI] flow). Further large-scale prospective studies of both STEMI and non-STEMI patients are warranted to explore these issues.
Conclusion
The prognostic impact of the baseline cTnI level at the time of admission in STEMI patients after a PCI was evident not only for the in-hospital period but also for the 1-year follow-up period, and the critical value of cTnI ≥3 ng/mL can be used to evaluate the patient’s prognosis at the first medical contact. At the same time, shortening the D2B time is still beneficial for the prognosis, although in this study the benefit was limited to the 30-day in-hospital period. The combined evaluation of the admission cTnI level and D2B time might be more objective and useful to predict the prognoses of STEMI patients after a PCI.
Ethical Approval
The Ethics Committee of Yanbian University Hospital consented to review the anonymous clinical data retrospectively and approved the study (2019-76). This study was conducted in accordance with the Declaration of Helsinki. All patient data was guaranteed to be confidential, and the researchers were committed to protecting the privacy and personal identity information of patients.
Funding
This work was supported in part by grants from the National Natural Science Foundation of China (nos. 81560240 and 81770485).
Disclosure
The authors declare that they have no conflicts of interest to disclose with respect to this manuscript.
References
1. Chew DP, Lambrakis K, Blyth A, et al. A randomized trial of a 1-hour troponin t protocol in suspected acute coronary syndromes: the rapid assessment of possible acute coronary syndrome in the emergency department with high-sensitivity troponin t study (rapid-tnt). Circulation. 2019;140:1543–1556. doi:10.1161/CIRCULATIONAHA.119.042891
2. Lambrakis K, Papendick C, French JK, et al. Late outcomes of the rapid-tnt randomized controlled trial: 0/1-hour high-sensitivity troponin t protocol in suspected acs. Circulation. 2021;144:113–125. doi:10.1161/CIRCULATIONAHA.121.055009
3. Morrow DA, Cannon CP, Jesse RL, et al. National academy of clinical biochemistry laboratory medicine practice guidelines: clinical characteristics and utilization of biochemical markers in acute coronary syndromes. Clin Chem. 2007;53:552–574. doi:10.1373/clinchem.2006.084194
4. Huang ZS, Zheng ZD, Zhang JW, et al. Association of major adverse cardiovascular events and cardiac troponin-i levels following percutaneous coronary intervention: a three-year follow-up study at a single center. Eur Rev Med Pharmacol Sci. 2020;24:3981–3992. doi:10.26355/eurrev_202004_20868
5. Chia S, Senatore F, Raffel OC, Lee H, Wackers FJ, Jang IK. Utility of cardiac biomarkers in predicting infarct size, left ventricular function, and clinical outcome after primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. JACC Cardiovasc Interv. 2008;1:415–423. doi:10.1016/j.jcin.2008.04.010
6. Hall TS, Hallen J, Krucoff MW, et al. Cardiac troponin i for prediction of clinical outcomes and cardiac function through 3-month follow-up after primary percutaneous coronary intervention for ST-segment elevation myocardial infarction. Am Heart J. 2015;169(257–265):e251. doi:10.1016/j.ahj.2014.10.015
7. Shah AS, Anand A, Sandoval Y, et al. High-sensitivity cardiac troponin i at presentation in patients with suspected acute coronary syndrome: a cohort study. Lancet. 2015;386:2481–2488.
8. Wanamaker BL, Seth MM, Sukul D, et al. Relationship between troponin on presentation and in-hospital mortality in patients with ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention. J Am Heart Assoc. 2019;8:e013551. doi:10.1161/JAHA.119.013551
9. Pavasini R, Biscaglia S, Barbato E, et al. Complete revascularization reduces cardiovascular death in patients with ST-segment elevation myocardial infarction and multivessel disease: systematic review and meta-analysis of randomized clinical trials. Eur Heart J. 2020;41:4103–4110. doi:10.1093/eurheartj/ehz896
10. Mehta SR, Wood DA, Storey RF. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019;381:1411–1421. doi:10.1056/NEJMoa1907775
11. McNamara RL, Wang Y, Herrin J, et al. Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2006;47:2180–2186. doi:10.1016/j.jacc.2005.12.072
12. Park J, Choi KH, Lee JM, et al. Prognostic implications of door-to-balloon time and onset-to-door time on mortality in patients with ST -segment-elevation myocardial infarction treated with primary percutaneous coronary intervention. J Am Heart Assoc. 2019;8:e012188. doi:10.1161/JAHA.119.012188
13. Bradley EH, Nallamothu BK, Herrin J, et al. National efforts to improve door-to-balloon time results from the door-to-balloon alliance. J Am Coll Cardiol. 2009;54:2423–2429. doi:10.1016/j.jacc.2009.11.003
14. Cannon CP, Gibson CM, Lambrew CT, et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA. 2000;283:2941–2947. doi:10.1001/jama.283.22.2941
15. Shiomi H, Nakagawa Y, Morimoto T, et al. Association of onset to balloon and door to balloon time with long term clinical outcome in patients with ST elevation acute myocardial infarction having primary percutaneous coronary intervention: observational study. BMJ. 2012;344:e3257. doi:10.1136/bmj.e3257
16. Lee WC, Fang HY, Chen HC, et al. Effect of improved door-to-balloon time on clinical outcomes in patients with ST segment elevation myocardial infarction. Int J Cardiol. 2017;240:66–71. doi:10.1016/j.ijcard.2017.02.156
17. Qin X, Fang E, Narisawa M, Cheng XW. Alternating p wave morphology. Circulation. 2019;139:1225–1227. doi:10.1161/CIRCULATIONAHA.118.038396
18. Stone GW, Selker HP, Thiele H, et al. Relationship between infarct size and outcomes following primary PCI: patient-level analysis from 10 randomized trials. J Am Coll Cardiol. 2016;67:1674–1683. doi:10.1016/j.jacc.2016.01.069
19. Nallamothu BK, Normand SL, Wang Y, et al. Relation between door-to-balloon times and mortality after primary percutaneous coronary intervention over time: a retrospective study. Lancet. 2015;385:1114–1122. doi:10.1016/S0140-6736(14)61932-2
20. Giannitsis E, Lehrke S, Wiegand UK, et al. Risk stratification in patients with inferior acute myocardial infarction treated by percutaneous coronary interventions: the role of admission troponin t. Circulation. 2000;102:2038–2044. doi:10.1161/01.CIR.102.17.2038
21. Kurowski V, Hartmann F, Killermann DP, et al. Prognostic significance of admission cardiac troponin t in patients treated successfully with direct percutaneous interventions for acute ST-segment elevation myocardial infarction. Crit Care Med. 2002;30:2229–2235. doi:10.1097/00003246-200210000-00009
22. Brieger D, Eagle KA, Goodman SG, et al. Acute coronary syndromes without chest pain, an underdiagnosed and undertreated high-risk group: insights from the global registry of acute coronary events. Chest. 2004;126:461–469. doi:10.1378/chest.126.2.461
23. Canto JG, Rogers WJ, Goldberg RJ, et al. Association of age and sex with myocardial infarction symptom presentation and in-hospital mortality. JAMA. 2012;307:813–822.
24. Mahmoud KD, Hillege HL, Jaffe AS, Lennon RJ, Holmes DR
25. Leibundgut G, Gick M, Morel O, et al. Discordant cardiac biomarker levels independently predict outcome in ST-segment elevation myocardial infarction. Clin Res Cardiol. 2016;105:432–440.
26. Rittersma SZ, van der Wal AC, Koch KT, et al. Plaque instability frequently occurs days or weeks before occlusive coronary thrombosis: a pathological thrombectomy study in primary percutaneous coronary intervention. Circulation. 2005;111:1160–1165.
27. Menees DS, Peterson ED, Wang Y, et al. Door-to-balloon time and mortality among patients undergoing primary PCI. N Engl J Med. 2013;369:901–909. doi:10.1056/NEJMoa1208200
28. Flynn A, Moscucci M, Share D, et al. Trends in door-to-balloon time and mortality in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Arch Intern Med. 2010;170:1842–1849. doi:10.1001/archinternmed.2010.381
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.