Back to Journals » Cancer Management and Research » Volume 13
Prognostic Impact of Pretreatment Elevated and Normalized Carcinoembryonic Antigen Levels After Neoadjuvant Chemoradiotherapy in Resected Locally Advanced Rectal Cancer Patients
Authors Song J ![]() , Chen Z, Huang D, Xu B
, Chen Z, Huang D, Xu B
Received 27 December 2020
Accepted for publication 18 March 2021
Published 7 May 2021 Volume 2021:13 Pages 3713—3721
DOI https://doi.org/10.2147/CMAR.S299364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eileen O'Reilly
Jianyuan Song,1– 3 Zhuhong Chen,1 Daxin Huang,1 Benhua Xu1– 3
1Department of Radiation Oncology, Fujian Medical University Union Hospital, Fuzhou, Fujian Province, People’s Republic of China; 2Department of Medical Imaging Technology, College of Medical Technology and Engineering, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 3Fujian Medical University Union Clinical Medicine College, Fuzhou, Fujian Province, People’s Republic of China
Correspondence: Benhua Xu
Department of Radiation Oncology, Fujian Medical University Union Hospital, Fuzhou, 350001, People’s Republic of China
Email [email protected]
Purpose: The prognostic significance of pretreatment elevated and normalized CEA after neoadjuvant chemoradiotherapy (nCRT) was evaluated.
Materials and Methods: The characteristics of 951 locally advanced rectal cancer patients with nCRT were retrieved and were analyzed retrospectively. Pretreatment CEA levels were defined as CEA evaluated one week prior to the nCRT. CEA after nCRT was deemed as CEA measured one week before surgery. The normal CEA levels were set at < 5 ng/mL. The normal CEA group was defined as patients with normal pretreatment CEA levels. The normalized CEA group was defined as patients with elevated pretreatment CEA levels and normal CEA levels after nCRT. The elevated CEA group was defined as patients with elevated pretreatment CEA levels and elevated CEA levels after nCRT.
Results: Compared with the elevated CEA group, the normalized CEA group was associated with better overall survival (OS) (HR: 0.625, 95%CI: 0.416– 0.938, P=0.022). There was no difference between the normalized CEA group and the normal CEA group (HR: 1.143, 95%CI: 0.84– 1.557, P=0.395).
Conclusion: In conclusion, the study indicated that OS of the normalized CEA group and the normal CEA group was better than the elevated CEA group.
Keywords: rectal cancer, locally advanced rectal cancer, LARC, carcinoembryonic antigen, CEA
Introduction
Carcinoembryonic antigen (CEA) as one of the tumor markers was carried out to screen for cancer, predict the survival of cancer, and detect the recurrence of rectal cancer.1–3 The screening value of CEA has been studied.1,4,5 The CEA levels were associated with the survival of rectal cancer.6 CEA clearance has an intensive relationship with overall survival of metastatic colorectal cancer.4 CEA was recommended to monitor the recurrence of rectal cancer.7,8 The changes of CEA levels after curative surgery were associated with the survival of rectal cancer.9,10 Neoadjuvant chemoradiotherapy (nCRT) and curative resection for locally advanced rectal cancer (LARC) is recommended.3,11,12 There were few reports related to prognostic impact of the changes of CEA levels after nCRT in LARC. In the present study, the prognostic significance of pretreatment elevated and normalized CEA after nCRT were assessed.
Materials and Methods
Ethics Statement
In this study, all information was retrospectively extracted in the context of compliance with the ethical standards of the institutional and/or national research committees and the principles of the Declaration of Helsinki. Patients’ medical records were analyzed retrospectively. No individual identifiable information was used. Thus, the Fujian Medical University Union Hospital Ethic Review Board considered that the patients’ consent was unnecessary. The study was approved by the Fujian Medical University Union Hospital Ethic Review Board (Number: 2020KY066).
Patients and Clinical Parameters
The database of our institution was reviewed. The data of LARC patients was retrieved, who were treated with nCRT and curative surgery from September 2006 to October 2017. TNM was used on the basis of The Union for International Cancer Control (UICC) eighth edition. The information relating to characteristics of patients and and tumor were collected, including age, gender, CEA levels, postneoadjuvant TNM (ypTNM), clinical TNM (cTNM), the total number of retrieved lymph node (TLN), surgery, the neoadjuvant radiotherapy regimen, the nCRT regimens, consolidation chemotherapeutic regimens, adjuvant chemotherapy and the interval between neoadjuvant therapy and surgery. Pretreatment CEA levels were defined as CEA evaluated one week prior to the nCRT. CEA after nCRT was deemed as CEA measured one week before surgery. The normal CEA levels were set at <5 ng/mL. The normal CEA group was defined as patients with normal pretreatment CEA levels. The normalized CEA group was defined as patients with elevated pretreatment CEA levels and normal CEA levels after nCRT. The elevated CEA group was defined as patients with elevated pretreatment CEA levels and elevated CEA levels after neoadjuvant chemoradiotherapy. A history and physical examination, including endoscopic ultrasonography and magnetic resonance imaging, was carried out to define clinical T and N stages. The exclusion criteria were as follows: (a) histologically proven signet-ring cell carcinoma or other carcinoma; (b) age at diagnosis <18 years; (c) previous or concurrent other malignancies; (d) patients with inadequate clinicopathological information; (e) presence of unresectable cancer; (f) previous history of chemotherapy or pelvic radiation.
Neoadjuvant Chemoradiotherapy and Surgery
In the capecitabine regimen, patients received capecitabine with 825 mg/m2 twice daily, day 1–14, every 21 days one cycle. In the oxaliplatin plus leucovorin and 5-fluorouracil 5-FU (FOLFOX4) regimen, patients received oxaliplatin with 85 mg/m2, day 1, leucovorin with 200 mg/m2, day 1–2, 5-FU with 400 mg/m2, days 1–2, 600 mg/m2, days 3–4, every 14 days one cycle. In the capecitabine plus oxaliplatin (CapeOX) regimen, patients received oxaliplatin with 130 mg/m2, day 1, capecitabine with 825 mg/m2 twice daily, days 1–14, every 21 days one cycle. In the modified oxaliplatin plus leucovorin and 5-FU (mFOLFOX6) regimen, patients received oxaliplatin with 85 mg/m2, day 1, leucovorin 400 mg/m2, day 1, 5-FU 400 mg/m2, day 1, 1200 mg/m2, day 2–3, every 14 days one cycle. The 5-FU-based nCRT includes FOLFOX4 and mFOLFOX6 regimens. The nCRT was initiated at the beginning of radiotherapy. The planning target volume (PTV) of clinical target volume was treated with 45 Gy. The PTV of gross tumor volume was treated with 50.4 Gy in 3-dimensional conformal radiotherapy (3DRT) cohort or 50 Gy in intensity-modulated radiation therapy (IMRT) cohort. The resection was performed 6–12 weeks after nCRT. The operation was carried out on the basis of the tumor-specific mesorectal excision or total mesorectal excision principle. The excision was completed by abdominoperineal resection (APR) or other resection.
Follow-up
The frequency of regular follow-up was once every three months within the first two years, once every six months in the next three years, and annually thereafter.
Data Analysis
The differences between the variable groups were analyzed with the Pearson's chi-squared test or Student's t-test. The interval between neoadjuvant therapy and surgery was dichotomized for OS before the log rank test by using optimal cutoff values determined by the “surv_cutpoint” function of the “survminer” R package. The survival-analyses were performed using the Kaplan–Meier method with the log rank test. Multivariate analysis were examined by the Cox proportional hazards model. Statistical analysis were performed with R software 3.6.2 and the SPSS software 25.0 (IBM Corporation, Armonk, NY, USA). P-value <0.05 was considered statistically significant.
Results
Clinical Characteristics
In total, the characteristics of 951 LARC patients with nCRT were collected. Among the patients, 621 (65.3%) were male, and 330 (34.7%) were female. The mean age was 55.2 years. The mean of pretreatment CEA level was 13.44 ng/mL. The mean of CEA level after nCRT was 4.2 ng/mL. One hundred and eighty-four patients (19.3%) achieved pCR. There are 531 patients, 303 patients and 117 patients in the normal CEA group, normalized CEA group, and elevated CEA group, respectively. The percentage of male in normal CEA group, normalized CEA group and elevated CEA group was 59.5%, 21.3% and 78.6% separately. The mean age of the normal CEA group, normalized CEA group, and elevated CEA group was 54.6 years, 55.4 years and 58.3 years, respectively. The percentage of clinical positive lymph node in the normal CEA group, normalized CEA group, and elevated CEA group was 87.4%, 92.1% and 94% respectively. The percentage of pathologic stage III in the normal CEA group, normalized CEA group, and elevated CEA group was 24.7%, 28.4% and 35%, respectively. The patients in the elevated CEA group were male, older, with the status of more clinically positive lymph node, more postneoadjuvant advanced tumor stage (P<0.05). There are no differences in gender, clinical stage T, the total number of retrieved lymph node, surgery regimens, the neoadjuvant radiotherapy regimen, the neoadjuvant chemotherapeutic regimens, consolidation chemotherapeutic regimens, adjuvant chemotherapy and the interval between neoadjuvant therapy and surgery between the normal CEA group, normalized CEA group, and elevated CEA group (P>0.05).The median follow-up period for all eligible patients was 57 (range: 4–158) months. The detail characteristics were showed in Tables 1 and 2.
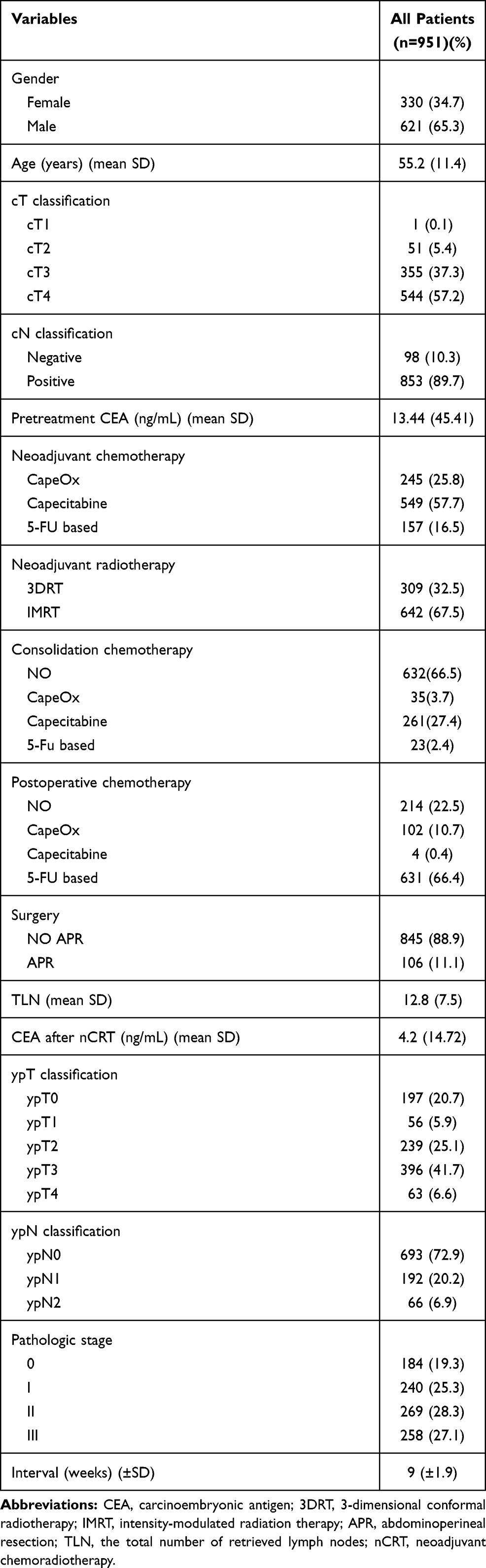 |
Table 1 Baseline Characteristics of Rectal Cancer Patients |
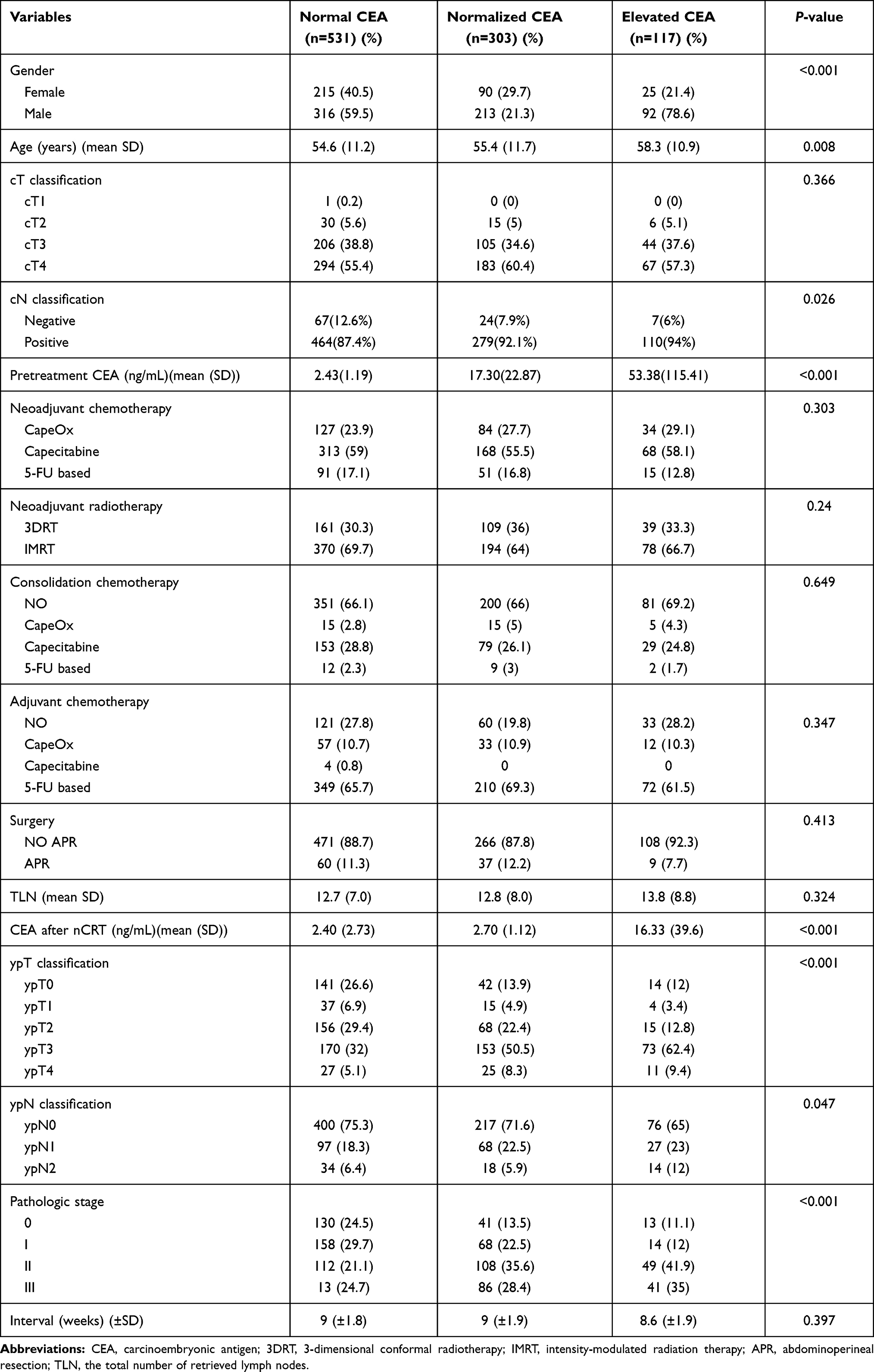 |
Table 2 Baseline Characteristics of Different CEA Group |
Factors Affecting Overall Survival of Resected Locally Advanced Rectal Cancer with Neoadjuvant Chemoradiotherapy
Univariate analyses demonstrated that pathologic stage (P<0.001) and CEA classification were significantly associated with overall survival (OS) (P=0.010). Age, gender, TLN, surgery, radiotherapy regimens, chemotherapeutic regimens, consolidation chemotherapy, adjuvant chemotherapy and the interval were not significantly associated with OS. Multivariate analyses revealed that pathologic stage was an independent prognostic factor (Table 3).The survival curves showed differences of CEA classification. Compared with elevated CEA group, normalized CEA group was associated with better OS (HR: 0.625, 95%CI: 0.416–0.938, P=0.022). There are no differences between the normalized CEA group and normal CEA group (HR: 1.143, 95%CI: 0.84–1.557, P=0.395) (Figure 1). Compared with patients with normal CEA levels after nCRT, patients with CEA ≥5 ng/mL got worse OS (HR: 1.663, 95%CI: 1.18–2.344, P=0.003) (Figure 2).
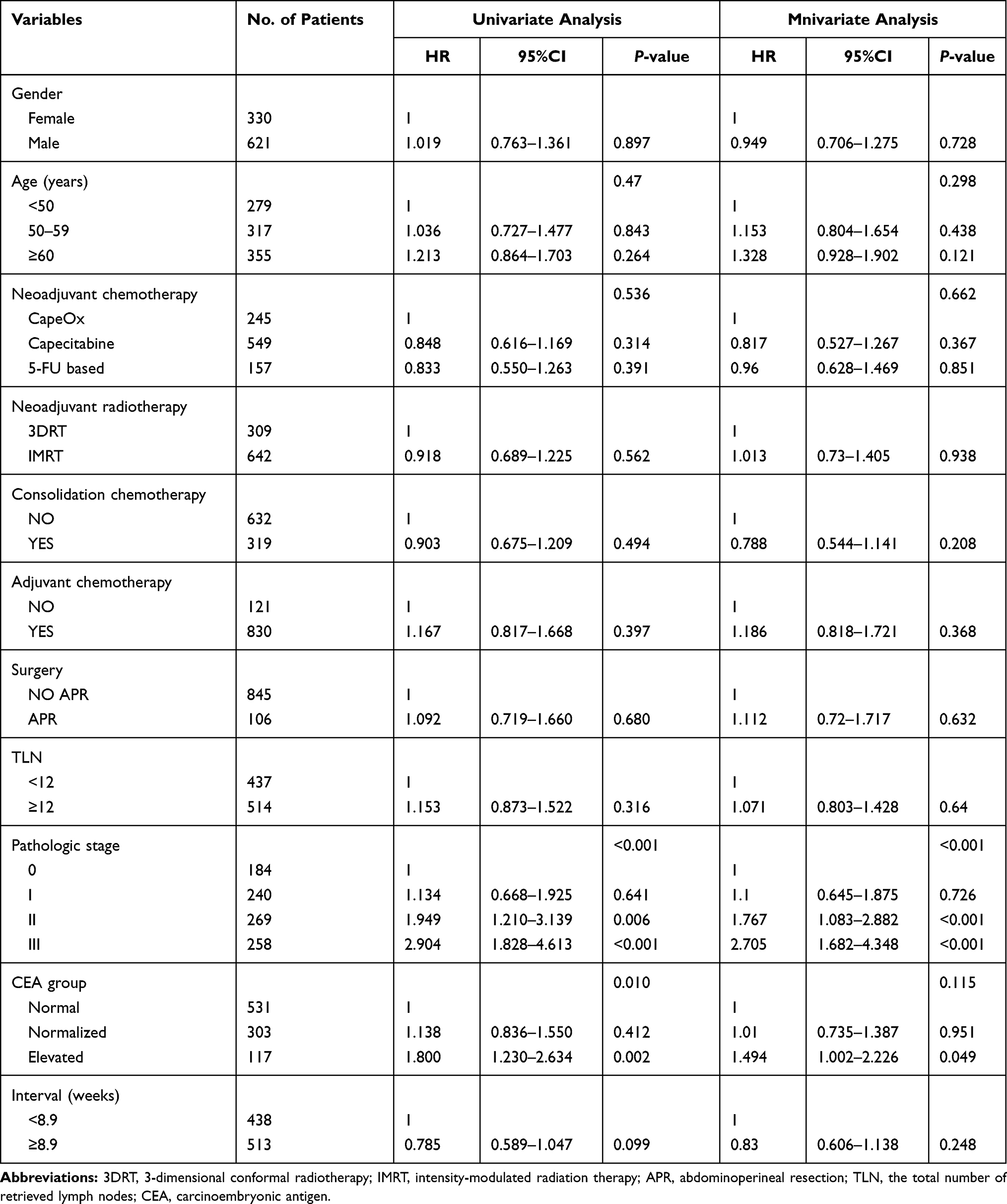 |
Table 3 Univariate and Multivariate Analysis of Prognostic Factors for Overall Survival |
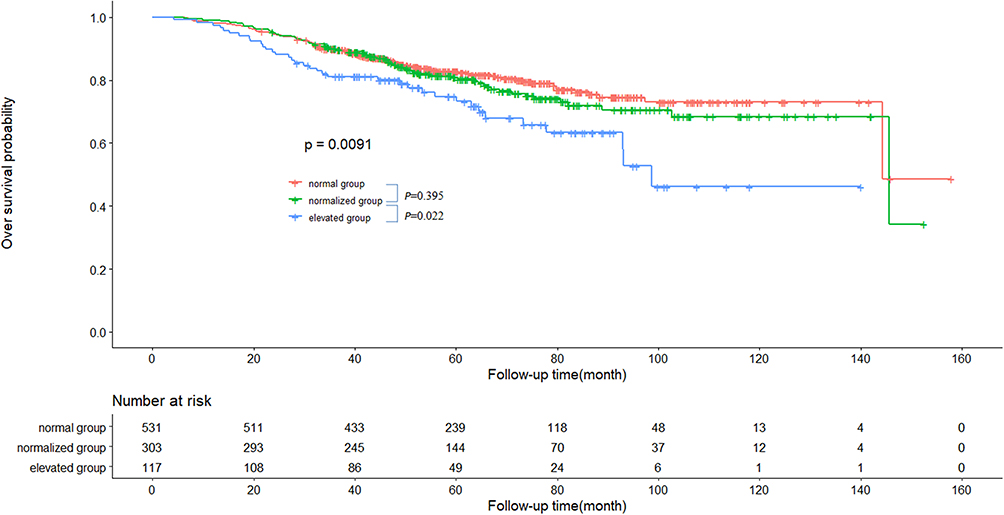 |
Figure 1 Overall survival curves for the normal CEA group, normalized CEA group and elevated CEA group. |
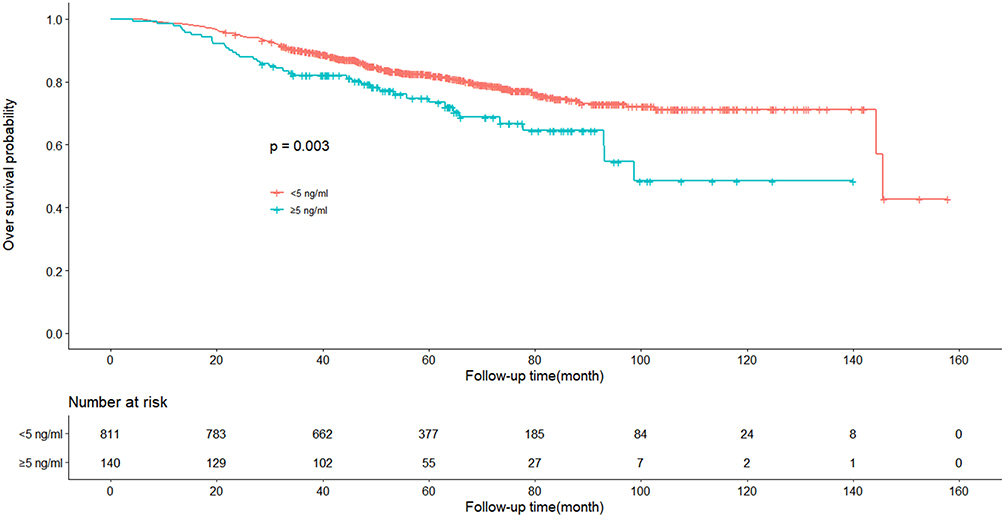 |
Figure 2 Overall survival curves for patients with the different CEA levels after neoadjuvant chemoradiotherapy. |
Discussion
The American Joint Committee on Cancer (AJCC) TNM staging system is the most commonly used algorithm in clinical practice. Currently, the individual survival of rectal cancer is usually predicted using the TNM staging system.13 In our study, the TNM staging system is an independent prognostic factor. Surgery is conventionally performed approximately six to eight weeks after nCRT. Ryan et al showed that minimum eight-week interval from the end of nCRT to TME increases pCR and downstaging rates, and improves recurrence-free survival without compromising surgical morbidity.14 Gambacorta et al reported that the best time to achieve pCR in LARC is at 10 weeks and that the lengthening of interval is not detrimental concerning survival outcomes.15 Du et al demonstrated that there were no significant differences in overall survival, disease-free survival in the interval of ≥8 weeks group and the interval of <8 weeks group.16 The study also provided evidence of the fact that the interval did not impact patient outcomes. The consolidation chemotherapy demonstrated the improvement in the downstaging rate for locally advanced rectal cancer.17,18 Our retrospective data illustrated consolidation chemotherapy did not impact the oncological outcomes of patients. And a future prospective, randomized trial is necessary to evaluate it. In locally advanced rectal cancer with nCRT, adjuvant chemotherapy remains controversial.19–21 The controversy is largely reflected by the differences in the strength of the recommendation from international clinical guidelines. Our retrospective data showed that adjuvant chemotherapy is not beneficial to patients who have received nCRT.
CEA is one of the commonly used tumor biomarkers in rectal cancer. CEA has been recommended to predict tumor response following nCRT and outcomes of rectal cancer.22–26 Serum CEA level is one of the significant predicting factors, which can reflect responses to nCRT in locally advanced rectal cancer.22,27 Pretreatment higher CEA level is associated with worse overall survival and disease-free survival of stage I to III rectal cancer.25 Preoperative serum CEA elevation is correlated with worse outcomes of T1N0M0 rectal cancer.26 As part of a follow-up regimen, CEA is also recommended by the National Comprehensive Cancer Network (NCCN) to detect tumor recurrence.12 Prognostic significance of preoperative and early postoperative serum CEA was reported.23 Some studies have published that CEA after nCRT is in connection with response and prognosis of rectal cancer.27–30 Song et al showed that posttreatment CEA level was significantly correlated with downstaging.27 Perez et al supported the idea that postchemoradiotherapy CEA levels <5 ng/mL has correlation with better clinical response, pathologic response, overall survival and disease-free survival.28 In this study, the data also illustrated that postchemoradiotherapy CEA levels <5 ng/mL has better overall survival. Huh et al showed that postchemoradiotherapy CEA level was an independent prognostic factor for overall survival.30 In our study, the CEA levels was associated with age, ypT classification, cN classification, ypN classification, pathologic stage. However, few studies reported prognostic significance of pretreatment serum CEA and the CEA levels following nCRT, especially for pretreatment of elevated and normalized CEA after nCRT. In this study, in comparison with the elevated CEA group, the patients in the normalized CEA group had better outcomes. There are no differences in the outcomes between the normalized CEA group and the normal CEA group.
However, the study has some limitations. Firstly, the study has selection bias of retrospective analysis, in which some factors associated with survival were unavailable, such as smoking status, genetic alterations, lymphovascular invasion and so on. Furthermore, due to the data being relatively small, large-scale investigations are necessary. Moreover, the study is based on a single institution, more institutions are necessary for external validations.
Conclusion
In conclusion, the study revealed that OS of the normalized CEA group and the normal CEA group was better than in the elevated CEA group.
Funding
The study was supported by the Natural Science Foundation of Fujian province (No. 2019J01149) and Fujian provincial health technology project (Grant No. 2019-ZQN-44).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Song WY, Zhang X, Zhang Q, Zhang PJ, Zhang R. Clinical value evaluation of serum markers for early diagnosis of colorectal cancer. World J Gastrointest Oncol. 2020;12:219–227. doi:10.4251/wjgo.v12.i2.219
2. Baca B, Beart RW, Etzioni DA. Surveillance after colorectal cancer resection: a systematic review. Dis Colon Rectum. 2011;54:1036–1048. doi:10.1007/DCR.0b013e31820db364
3. Glynne-Jones R, Wyrwicz L, Tiret E, et al. Rectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28:iv22–iv40. doi:10.1093/annonc/mdx224
4. Colloca GA, Venturino A, Guarneri D. Carcinoembryonic antigen reduction after medical treatment in patients with metastatic colorectal cancer: a systematic review and meta-analysis. Int J Colorectal Dis. 2019;34:657–666. doi:10.1007/s00384-018-03230-w
5. Schaap DP, de Valk KS, Deken MM, et al. Carcinoembryonic antigen-specific, fluorescent image-guided cytoreductive surgery with hyperthermic intraperitoneal chemotherapy for metastatic colorectal cancer. Br J Surg. 2020;107:334–337. doi:10.1002/bjs.11523
6. Cho WK, Choi DH, Park HC, et al. Elevated CEA is associated with worse survival in recurrent rectal cancer. Oncotarget. 2017;8:105936–105941. doi:10.18632/oncotarget.22511
7. Nicholson BD, Shinkins B, Pathiraja I, et al. Blood CEA levels for detecting recurrent colorectal cancer. Cochrane Database Syst Rev;2015:CD011134. doi:10.1002/14651858.CD011134.pub2
8. Primrose JN, Perera R, Gray A, et al. Effect of 3 to 5 years of scheduled CEA and CT follow-up to detect recurrence of colorectal cancer: the FACS randomized clinical trial. JAMA. 2014;311:263–270. doi:10.1001/jama.2013.285718
9. Yang KM, Park IJ, Kim CW, Roh SA, Cho DH, Kim JC. The prognostic significance and treatment modality for elevated pre- and postoperative serum CEA in colorectal cancer patients. Ann Surg Treat Res. 2016;91:165–171. doi:10.4174/astr.2016.91.4.165
10. Woo J, Kim J, Park I, et al. Perioperative serum carcinoembryonic antigen ratio is a prognostic indicator in patients with stage II colorectal cancer. Ann Coloproctol. 2018;34:4–10. doi:10.3393/ac.2018.34.1.4
11. Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized Phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;30:1926–1933. doi:10.1200/JCO.2011.40.1836
12. National Comprehensive Cancer Netowrk. NCCN Clinical Practice Guidelines in Oncology Rectal Cancer. Version 1; 2020. Available from: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf. Accessed May 04, 2021.
13. Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177–193. doi:10.3322/caac.21395
14. Ryan ÉJ, O’Sullivan DP, Kelly ME, et al. Meta-analysis of the effect of extending the interval after long-course chemoradiotherapy before surgery in locally advanced rectal cancer. Br J Surg. 2019;106:1298–1310. doi:10.1002/bjs.11220
15. Gambacorta MA, Masciocchi C, Chiloiro G, et al. Timing to achieve the highest rate of pCR after preoperative radiochemotherapy in rectal cancer: a pooled analysis of 3085 patients from 7 randomized trials. Radiat Oncol. 2020;154:154–160. doi:10.1016/j.radonc.2020.09.026
16. Du D, Su Z, Wang D, Liu W, Wei Z. Optimal interval to surgery after neoadjuvant chemoradiotherapy in rectal cancer: a systematic review and meta-analysis. Clin Colorectal Cancer. 2018;17:13–24. doi:10.1016/j.clcc.2017.10.012
17. Zhai Z, Zhang K, Wang C, et al. Adding three cycles of CAPOX after neoadjuvant chemoradiotherapy increases the rates of complete response for locally advanced rectal cancer. Curr Oncol. 2021;28:283–293. doi:10.3390/curroncol28010033
18. Kim SY, Joo J, Kim TW, et al. A randomized phase 2 trial of consolidation chemotherapy after preoperative chemoradiation therapy versus chemoradiation therapy alone for locally advanced rectal cancer: KCSG CO 14-03. Int J Radiat Oncol Biol Phys. 2018;101:889–899. doi:10.1016/j.ijrobp.2018.04.013
19. Seddik Y, Brahmi SA, Afqir S. Does adjuvant chemotherapy for locally advanced resectable rectal cancer treated with neoadjuvant chemoradiotherapy have an impact on survival? A single moroccan institute retrospective study. Gulf J Oncolog. 2019;1:29–32.
20. Chung MJ, Lee JH, Lee JH, et al. Adjuvant chemotherapy in rectal cancer patients treated with preoperative chemoradiation and total mesorectal excision: a multicenter and retrospective propensity-score matching study. Int J Radiat Oncol Biol Phys. 2019;103:438–448. doi:10.1016/j.ijrobp.2018.09.016
21. Bregni G, Akin Telli T, Camera S, et al. Adjuvant chemotherapy for rectal cancer: current evidence and recommendations for clinical practice. Cancer Treat Rev. 2020;83:101948. doi:10.1016/j.ctrv.2019.101948
22. Kim CH, Huh JW, Yeom SS, Kim HR, Kim YJ. Predictive value of serum and tissue carcinoembryonic antigens for radiologic response and oncologic outcome of rectal cancer. Pathol Res Pract. 2020;216:152834. doi:10.1016/j.prp.2020.152834
23. Nakamura Y, Shida D, Tanabe T, et al. Prognostic impact of preoperatively elevated and postoperatively normalized carcinoembryonic antigen levels following curative resection of stage I-III rectal cancer. Cancer Med. 2020;9:653–662. doi:10.1002/cam4.2758
24. Restivo A, Delrio P, Deidda S, et al. Predictors of early distant relapse in rectal cancer patients submitted to preoperative chemoradiotherapy. Oncol Res Treat. 2020;43:146–152.
25. Cai D, Huang ZH, Yu HC, et al. Prognostic value of preoperative carcinoembryonic antigen/tumor size in rectal cancer. World J Gastroenterol. 2019;25:4945–4958. doi:10.3748/wjg.v25.i33.4945
26. Wu S, Gu W. Association of T stage and serum CEA levels in determining survival of rectal cancer. Front Med. 2019;6:270. doi:10.3389/fmed.2019.00270
27. Song J, Huang X, Chen Z, et al. Predictive value of carcinoembryonic antigen and carbohydrate antigen 19-9 related to downstaging to stage 0-I after neoadjuvant chemoradiotherapy in locally advanced rectal cancer. Cancer Manag Res. 2018;10:3101–3108. doi:10.2147/CMAR.S166417
28. Perez RO, Sao Juliao GP, Habr-Gama A, et al. The role of carcinoembriogenic antigen in predicting response and survival to neoadjuvant chemoradiotherapy for distal rectal cancer. Dis Colon Rectum. 2009;52:1137–1143. doi:10.1007/DCR.0b013e31819ef76b
29. Jang NY, Kang SB, Kim DW, et al. The role of carcinoembryonic antigen after neoadjuvant chemoradiotherapy in patients with rectal cancer. Dis Colon Rectum. 2011;54:245–252. doi:10.1007/DCR.0b013e3181fcee68
30. Huh JW, Yun SH, Kim SH, et al. Prognostic role of carcinoembryonic antigen level after preoperative chemoradiotherapy in patients with rectal cancer. J Gastrointest Surg. 2018;22:1772–1778. doi:10.1007/s11605-018-3815-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.