Back to Journals » Clinical Epidemiology » Volume 14
Profiling Bispebjerg Acute Cohort: Database Formation, Acute Contact Characteristics of a Metropolitan Hospital, and Comparisons to Urban and Rural Hospitals in Denmark
Authors Gregersen R ![]() , Fox Maule C
, Fox Maule C ![]() , Husum Bak-Jensen H, Linneberg A
, Husum Bak-Jensen H, Linneberg A ![]() , Nielsen OW
, Nielsen OW ![]() , Thomsen SF
, Thomsen SF ![]() , Meyhoff CS
, Meyhoff CS ![]() , Dalhoff K, Krogsgaard M, Palm H
, Dalhoff K, Krogsgaard M, Palm H ![]() , Christensen H
, Christensen H ![]() , Porsbjerg C, Antonsen K, Rungby J, Haugaard SB, Petersen J
, Porsbjerg C, Antonsen K, Rungby J, Haugaard SB, Petersen J ![]() , Nielsen FE
, Nielsen FE ![]()
Received 10 September 2021
Accepted for publication 14 February 2022
Published 31 March 2022 Volume 2022:14 Pages 409—424
DOI https://doi.org/10.2147/CLEP.S338149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor H Sorensen
Rasmus Gregersen,1,2 Cathrine Fox Maule,3 Henriette Husum Bak-Jensen,2 Allan Linneberg,3,4 Olav Wendelboe Nielsen,4,5 Simon Francis Thomsen,6 Christian S Meyhoff,2,4,7 Kim Dalhoff,4,8 Michael Krogsgaard,4,9 Henrik Palm,4,9 Hanne Christensen,4,10 Celeste Porsbjerg,4,11 Kristian Antonsen,12 Jørgen Rungby,2,4,13 Steen B Haugaard,2,4,13 Janne Petersen,3,14 Finn E Nielsen1,2
1Department of Emergency Medicine, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 2Copenhagen Center for Translational Research, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 3Center for Clinical Research and Prevention, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 4Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 5Department of Cardiology, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 6Department of Dermatology, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 7Department of Anaesthesia and Intensive Care, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 8Department of Clinical Pharmacology, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 9Department of Orthopedics, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 10Department of Neurology, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 11Department of Respiratory Medicine, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 12Executive Board, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 13Department of Endocrinology, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark; 14Section of Biostatistics, Department of Public Health, University of Copenhagen, Copenhagen, Denmark
Correspondence: Rasmus Gregersen, Department of Emergency Medicine, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, NV, 2400, Denmark, Email [email protected]
Purpose: To present a metropolitan cohort, Bispebjerg acute cohort (BAC), and compare patient characteristics and outcomes with patients from urban and rural hospitals in Denmark.
Patients and Methods: We linked data from seven Danish nationwide registries and included all acute contacts to non-psychiatric hospitals in the years 2016– 2018. Acute hospital contacts to Bispebjerg and Frederiksberg Hospital constituted BAC, representing a solely metropolitan/urban catchment area. Patient characteristics and outcomes were compared to the rest of Denmark in an urban cohort (UrC) and a rural cohort (RuC), stratified by visit and hospitalization contact types.
Results: We identified 4,063,420 acute hospital contacts in Denmark and BAC constituted 8.4% (n=343,200) of them. BAC had a higher proportion of visits (65.1%) compared with UrC (52.1%) and RuC (45.3%). Patients in BAC more often lived alone (visits: BAC: 34.8%, UrC: 30.6%, RuC: 29.2%; hospitalizations: BAC: 50.8%, UrC: 36.7%, RuC: 37.2%) and had temporary CPR number (visits: BAC: 4.4%, UrC: 1.9%, RuC: 1.6%; hospitalizations: BAC: 1.5%, UrC: 0.9%, RuC: 0.8%). Visit patients in BAC were younger (BAC: 36, UrC: 42, RuC: 45 years, median), more often students (BAC: 18.0%, UrC: 14.0%, RuC: 12.5%), and had more contacts due to infectious diseases (BAC: 19.8%, UrC: 14.1%, RuC: 6.2%) but less due to injuries (BAC: 40.0%, UrC: 43.8%, RuC: 60.7%). Hospitalized patients in BAC had higher median age (BAC: 64, UrC: 61, RuC: 64 years) and fewer were in employment than in UrC (BAC: 26.1%, UrC: 32.1%, RuC: 28.1%). BAC Hospitalizations had a lower death rate within 30 days than in RuC (BAC: 3.0% [2.9– 3.1%], UrC: 3.1% [3.0– 3.1%], RuC: 3.4% [3.3– 3.4%]), but a higher readmission-rate (BAC: 20.5% [20.3– 20.8%], UrC: 17.3% [17.2– 17.4%], RuC: 17.5% [17.5– 17.6%]).
Conclusion: Significant differences between BAC, urban, and rural cohorts may be explained by differences in healthcare structure and sociodemographics of the catchment areas.
Keywords: emergency medicine, acute care, urban-rural disparities, registry-based research, Danish national registers, epidemiology
Introduction
In Denmark, acute hospital contacts account for 72% of all inpatient and 8% of all outpatient contacts.1,2 There are 21 hospitals with adult acute care units in Denmark, of which Bispebjerg and Frederiksberg Hospital (BFH), a metropolitan hospital in Copenhagen, the capital of Denmark, is among the largest.3,4 To better understand and improve outcomes of patients with acute hospital needs, we have established a research collaboration called Bispebjerg Acute Cohort (BAC) and a national registry-based database as one of the research initiatives. BFH is notably different from other hospitals in Denmark when considering catchment areas and inhabitants since it is the only hospital covering a solely metropolitan catchment area.1 In preparation for establishing a local, acute cohort with continuous inclusion and collection of extra information and samples, we realized that it has not yet been established how a metropolitan hospital differs from urban hospitals that also have non-urban catchment areas and from hospitals in smaller cities.5 Studies on this subject primarily originate from countries with low population density or a higher degree of rural population, and information from European settings are scarce.6–9 A Scottish study reported more multimorbidity in patients from urban areas than rural areas.10 Age, comorbidity, discharge diagnosis, income, education and employment status, cohabitation, and polypharmacy are associated with mortality or readmission, and we hypothesized that they might vary across different degrees of urbanization.11–17
This study aims to examine patient and hospital contact characteristics and outcomes of BAC compared with an urban cohort (UrC) and a rural cohort (RuC) in Denmark. Further, we will establish the methodology and research perspective of BAC as an ongoing research initiative.
Methods
Design, Study Population, and Data Sources
This is a national, registry-based cohort study of all acute somatic hospital contacts in Denmark during 2016–2018. All hospital contacts with at least one acute contact at BFH were extracted as part of BAC. For comparisons, we defined two other cohorts of the remaining hospital contacts: UrC, consisting of hospital contacts in cities with ≥100.000 inhabitants; and RuC, consisting of hospital contacts in smaller cities (Figure 1, see Supplementary A1 for list of hospitals). BFH covers a solely metropolitan catchment area, UrC covers both urban and suburban or rural catchment areas, while RuC covers smaller cities and rural areas. We considered each hospital contact separately. Therefore, patients could have more than one hospital contact during the period and could be included in more than one of the cohorts (with different hospital contacts).
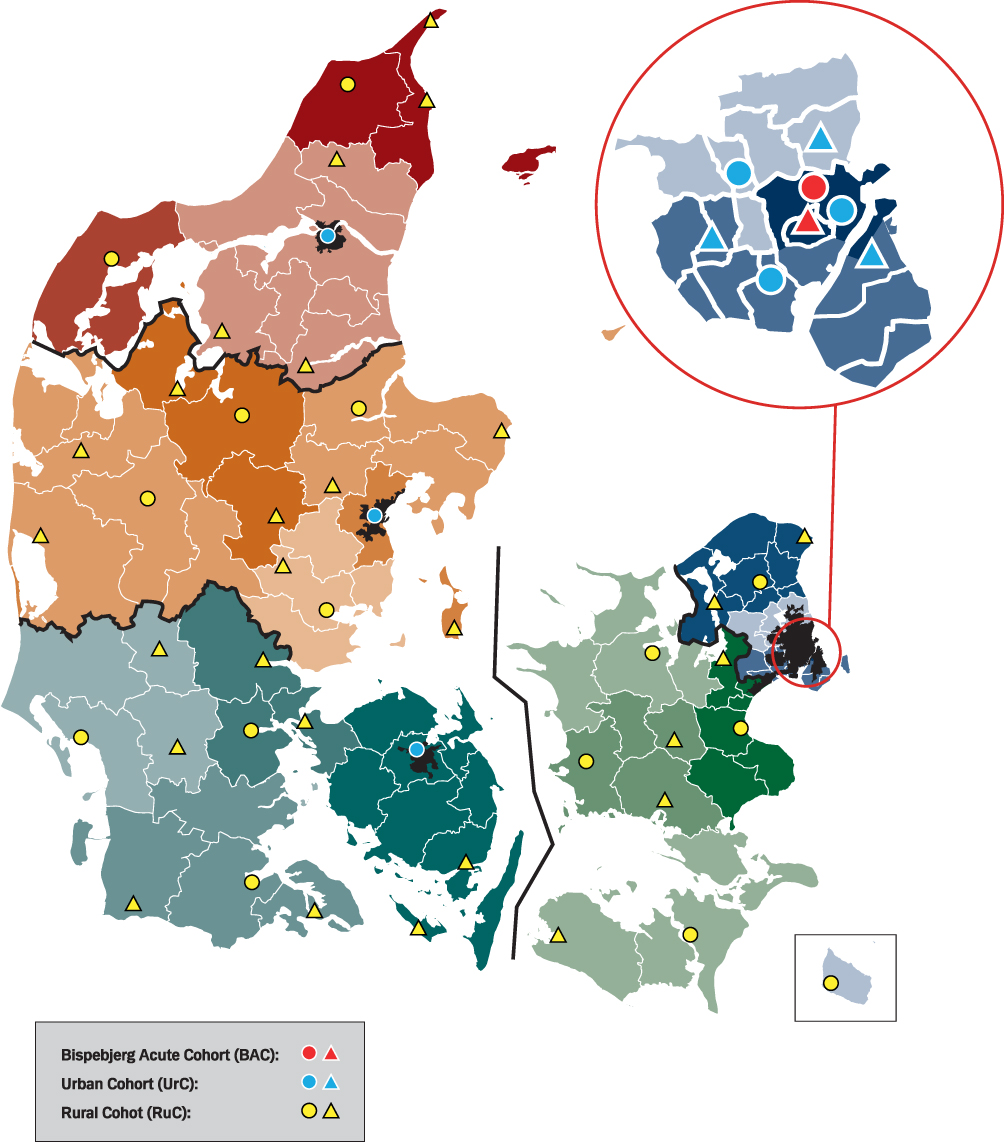 |
Figure 1 Map of hospitals with acute functions in Denmark and related catchment areas. Notes: Hospitals involved in acute care are marked with circles and triangles. A circle indicates that the hospital has an emergency department or trauma center. A triangle indicates that the hospital has no emergency department but receives patients with minor problems in emergency clinics or departments receiving transfers from acute hospitals. The catchment area of each acute hospital is represented by the extent of the colored area the hospital is placed in. Catchment areas are related to hospitals with emergency departments and mostly follow municipality borders (marked with white lines), except for central Copenhagen. Bispebjerg Acute Cohort (BAC) is marked with red, the urban cohort (UrC) is marked with blue, and the rural cohort (RuC) is marked with yellow. The city boundaries for the four largest cities are drawn with black to show that the catchment areas of UrC extend outside the cities. Black line and change of color palette marks regional borders. |
The database was established at Statistics Denmark by linkage of data from the Danish National Patient Registry (DNPR),18 the Danish National Prescription Registry,19 the Register of Laboratory Results for Research (RLRR),20 the Central Person Register,21 the Income Statistics Register,22 the Danish Education Register,23 and the Building and Housing Register24 for the years 2003–2018. Data was available nationally, except for RLRR data from the Central Denmark Region. Information was linked by CPR number (“Det Centrale Personregister”), a unique, lifelong identifier provided at birth and used for registration of all healthcare and societal information. Persons <18 years were excluded, since they are usually treated in pediatric emergency departments.
In DNPR, a new contact is registered for each visit (eg, visits to the emergency department [ED], hospital ambulatories, or short stays at hospital wards) or Department stay, and a new contact is recorded each time a patient is transferred to a new department.18 Each contact is registered by contact type (visit or hospitalization) and urgency (acute/unplanned or elective/planned), separately for somatic and psychiatric departments. We considered all somatic and psychiatric contacts, in all variations of acute, elective, visits, and hospitalization contact types and formed hospital contacts of coherent contacts within four hours. Thereby, hospital contacts consist of one or more contacts; either visit contact(s), hospitalization contact(s), or a combination of them reflecting the total course from arrival at a hospital until discharge. Exclusively elective or psychiatric hospital contacts were not included. We stratified hospital contacts into hospitalizations (at least one hospitalization contact) and visits (See Supplementary A2 for further definitions). Notably, acute visit contacts can be either visits at the ED or acute visits at outpatient clinics (ambulatories located at the hospital) or hospital wards.
Setting
Denmark has a tax-funded, universal healthcare and welfare system, where hospital diagnostics and treatments are carried out without direct expenses of the patient.3,18,25 Access to acute care at hospitals requires a referral from either general practitioners (GP) or Emergency Medical Services (EMS), and each region operates an independent EMS organization.3,26 In 2014, the Capital Region implemented a new system, where patients who are assessed by out-of-hours GPs in other regions, are handled in separate ED fast tracks.2,4,26 These ED fast tracks are registered in the DNPR as ED visits, which consequently increases the number of ED visits in the Capital Region compared with other regions.2 Persons with Danish citizenship or a permanent address in Denmark (eg, foreigners working or studying in Denmark, along with legal immigrants) are provided with a CPR number, whereas visitors (tourists among others) and illegal immigrants are given a temporary CPR number if they need healthcare services.
BFH is located at two different locations in central Copenhagen and covers a solely metropolitan/urban catchment area, whereas other urban hospitals cover both urban/suburban and rural areas (Figure 1). BFH receives about 120,000 acute contacts per year and has a catchment area of 52.8 km2, covering most of central Copenhagen with about 483,000 inhabitants from two municipalities.4,27 While most of central Copenhagen is a part of the BFH catchment area, Rigshospitalet, the national hospital for highly specialized treatments also has an Emergency Clinic for minor traumas in a small catchment area and Amager and Hvidovre Hospital, besides covering Southern and Western Copenhagen, also covers parts of Central Copenhagen (Figure 1). BFH has a level II trauma center, and all severe cases are prehospitally referred to the level I center at Rigshospitalet. Patients with acute ST-elevation myocardial infarction are referred to specialized centers outside BFH. Rigshospitalet and BFH are regional stroke centers, providing reperfusion treatment on alternating dates.
The ED at BFH has a short-stay (<6 hours) unit and an Emergency Medical Ward for up to 48-hour stays at the Bispebjerg site, along with an Emergency Clinic at the Frederiksberg site. While most patients were initially examined at the ED prior to admission, patients could also be directly admitted to acute units at the Emergency Medical Ward, Cardiology Department, Neurology Department, and Surgical Department.1 Since BFH did not provide general gynecology, obstetrical, neonatal, or pediatric care services in the study period, pregnant women were referred to other hospitals in the Capital Region and children were only referred to BFH with minor to moderate trauma or mild diseases.
Characteristics
We examined patient characteristics, medication prior to acute hospital contact, characteristics of the hospital contact, the primary diagnoses, and abnormal laboratory results. Patient characteristics consisted of age, sex, CPR status (permanent or temporary), and comorbidity measured as Charlson Comorbidity Index (CCI) score by the Quan 2011 modification, with a 5-year lookback period.28,29 Socioeconomic data were assessed at the calendar year before each hospital contact and consisted of educational level by the International Standard Classification of Education (ISCED) 2011,30 personal income (divided by quintiles of the general population), employment status, civil status, and cohabitation (see Supplementary A3–A5 for groupings). Medication was defined from redeemed prescriptions within four months prior to the hospital contact. We identified the 15 most frequent medications among all included hospital contacts at the therapeutic subgroup (2nd Anatomical Therapeutic Chemical Classification [ATC] level) and assessed the proportion of patients with at least one redemption of these, along with polypharmacy and hyperpolypharmacy (5+ and 10+ different medications [5th ATC-level], respectively). Patients with temporary CPR were censored from socioeconomic and medication assessments due to missing data. Characteristics of the hospital contacts include the time of day and day of the week for the start of each hospital contact, number of transfers if the hospital contact involved contacts in another region, and involved psychiatric contacts. The primary diagnosis was assessed at the last contact in a hospital contact and grouped as proposed by Vest-Hansen et al,31 with some modifications (see Supplementary A6 for grouping and modifications). We chose the blood, blood gas, urine, and cerebrospinal fluid laboratory results most relevant for acute contacts and assessed the proportion of abnormal results (values outside reference intervals). We only investigated the first of each result during each hospital contact. For results without defined reference intervals, such values were defined when appropriate; otherwise the results were excluded.
Outcomes
Outcomes consisted of length of stay (length of hospital contact in total hours), in-hospital mortality (dying during a hospital contact), and all-cause mortality and readmission within 30 days from discharge (only including patients discharged alive and with a permanent CPR number). Readmission was defined as a hospitalization beginning with an acute contact within 30 days from discharge, with one exception: if the hospital contact ended with a referral to a hospital Department, and the next contact both started within 24 hours and was registered as referred from the hospital, it was not considered a readmission.
Statistical Methods
Since there were notable differences between visits and hospitalizations in patient characteristics and causes of contacts, we performed all analyses stratified by hospital contact type. Characteristics and outcomes are presented by frequency (%) if categorical and by median (first quartile [Q1]-third quartile [Q3]) if continuous. Outcomes after discharge were assessed by cumulative incidence function at 30 days (95% CI) with death as a competing risk for readmission, and censoring at the end of follow-up on the 31st of December 2018.
It was not the purpose of the study to test specific hypotheses. Further, due to the large sample size, it would be possible to identify even small, statistically significant results. Therefore, we have refrained from using classical statistical methods to compare the groups. Instead, we compared UrC and RuC to BAC, and highlighted relative differences of at least 10% at a 95% confidence interval. Smaller differences or even lack of differences might also be worth considering when comparing cohorts, but it is beyond the scope of this paper to discuss such differences in detail. Comparisons were not performed for the cumulative incidence function analyses.
We performed subgroup analyses excluding patients <40 years of age and patients with a temporary CPR number. The cut-off at 40 years was chosen after reviewing the data since we observed an overrepresentation of young persons in the metropolitan and urban cohorts. This overrepresentation is presumably caused by students who often finish their studies and move away from the big cities before the age of 40. By excluding patients <40 years of age, we obtained a comparable age-distribution between the three cohorts, both regarding visits and hospitalizations.
Data analyses were performed with SAS Enterprise Guide (version 9.04, SAS Institute, USA). Reporting adhered to Reporting of Studies Conducted using Observational Routinely-collected Data (RECORD).32
Results
There were 4.82 million citizens with permanent CPR number aged ≥18 years in Denmark during the study period. We identified 4.06 million acute hospital contacts in the entire country, consisting of 6.06 million individual contacts. Hospitalizations represented 2.04 mio (50.3%) of these acute hospital contacts (Table 1). Of all adult citizens with permanent CPR number in Denmark, 38.9% (1.88 million persons) had at least one acute hospital contact over the 3-year period.
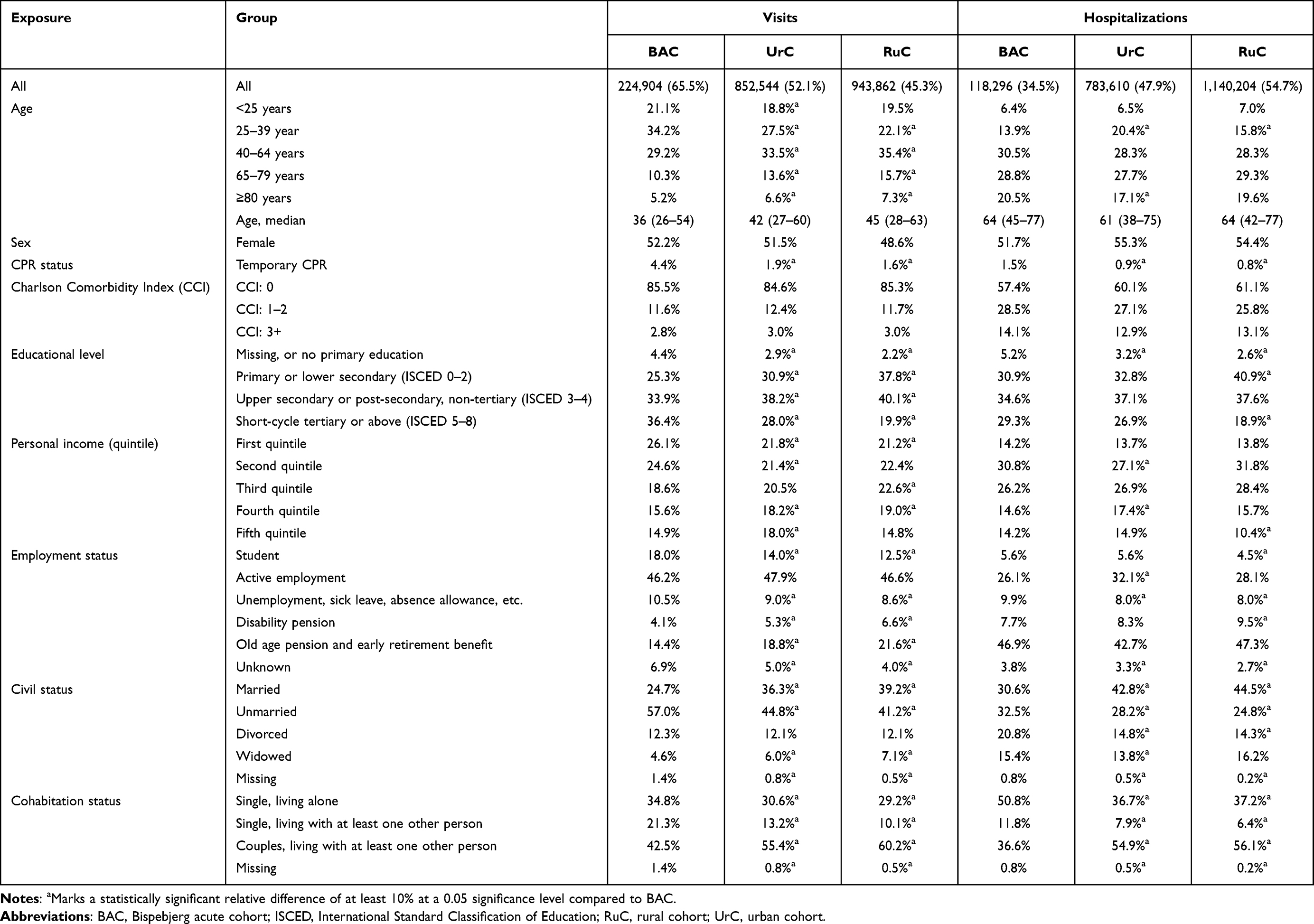 |
Table 1 Patient Characteristics at Each Acute Hospital Contact |
When stratified into the three cohorts, BAC constituted 8.4% (n=343,200), UrC 40.3% (n=1,636,154), and RuC 51.3% (n=2,084,066) of all hospital contacts (Table 1). When comparing contact type distribution, BAC had a higher proportion of visits at 65.5% compared with 52.1% for UrC and 45.3% for RuC. Thereby, BAC constituted 11.1% of all visits in the country but only 5.8% of all hospitalizations. In BAC, 6.7% of visit contacts were registered at other departments than the ED units. Of the 200,299 unique patients included in BAC, 35.7% also had one or more contacts in the other cohorts (at other hospitals) during the study period.
Visits
Characteristics and Outcomes
BAC patients were younger, more often had a temporary CPR number, had a higher education level and a lower income compared with UrC and RuC (Table 1). They were more likely to be studying or unemployed but less likely to be on a pension. They were more often unmarried and living alone but had a similar comorbidity burden. Polypharmacy and hyperpolypharmacy, along with all medication groups, except for psycholeptics, drugs for obstructive airway diseases, and sex hormones and modulators of the genital system, were more frequent in UrC and RuC (Table 2). Visits in BAC less often started as a planned contact, were more often initiated during the evening, nighttime, and weekend, had fewer transfers and were more likely to involve patients living in other regions of Denmark (Table 3). RuC had a high proportion of injuries, whereas BAC and UrC had more visits due to infectious diseases, poisoning and intoxication, and unspecific symptoms (Table 4). A sensitivity analysis showed that injuries were registered for 40.3% and infectious diseases for 19.5% of visits in the Capital Region compared with 63.1% and 2.4%, respectively, for the other four regions combined. Abnormal laboratory results of blood tests for haemoglobin, leukocytes, creatinine, albumin, bilirubin, glucose, and lactate; as well as urine leukocytes and erythrocytes were more frequent in BAC than in the other two cohorts (Table 5).
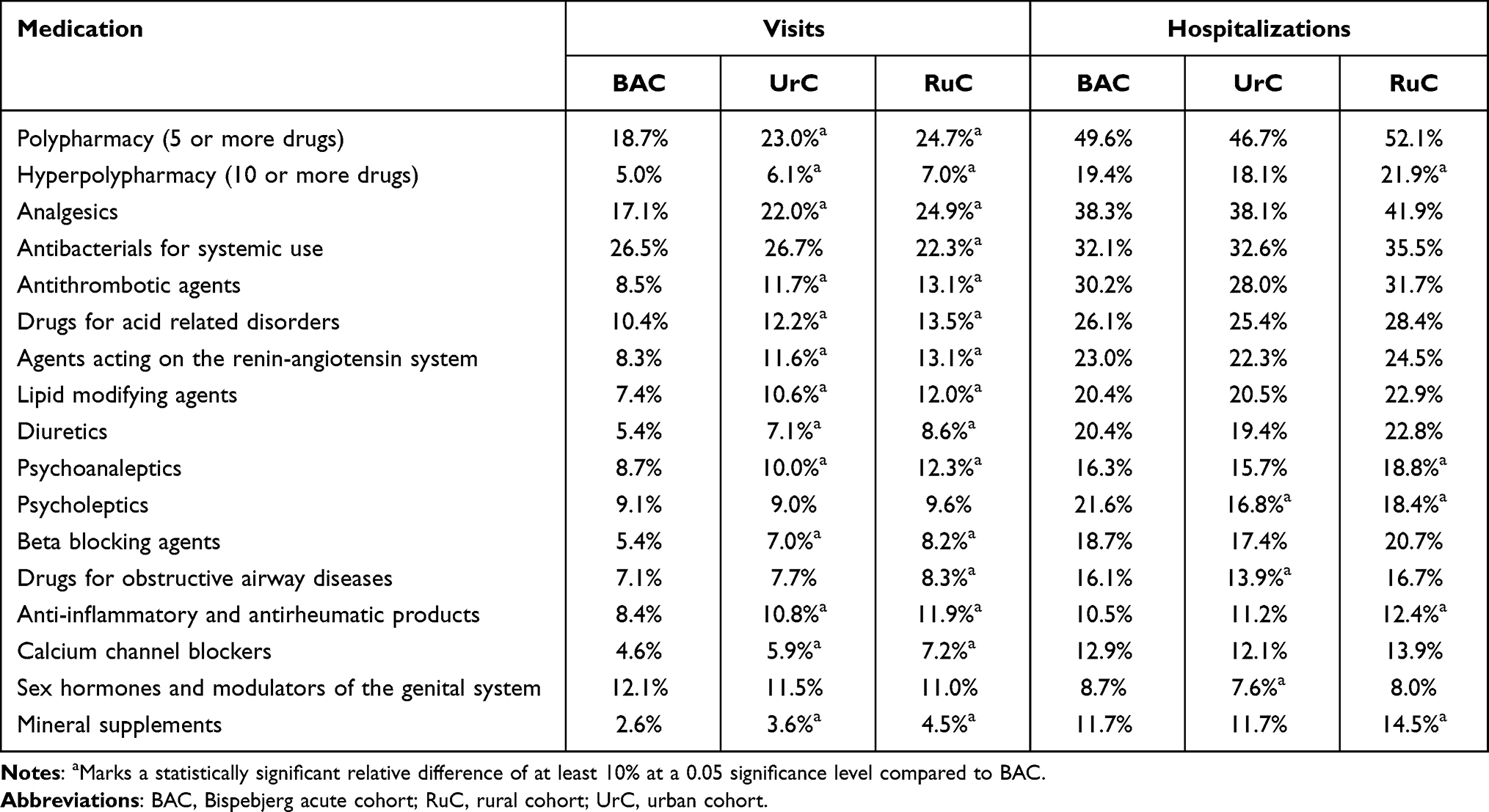 |
Table 2 Proportions of Patients with Medication Prescriptions Prior to Each Acute Hospital Contact |
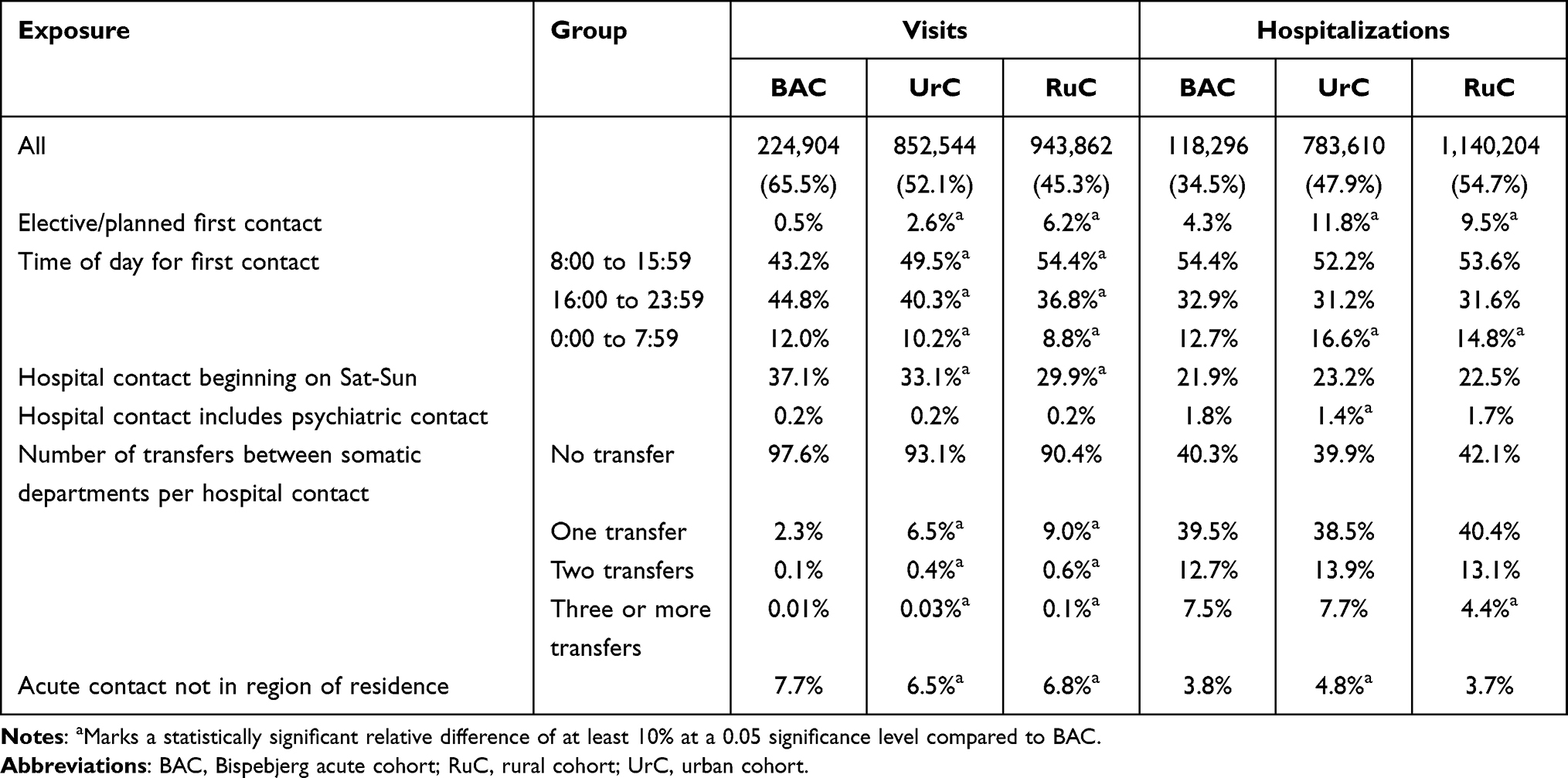 |
Table 3 Hospital Contact Characteristics |
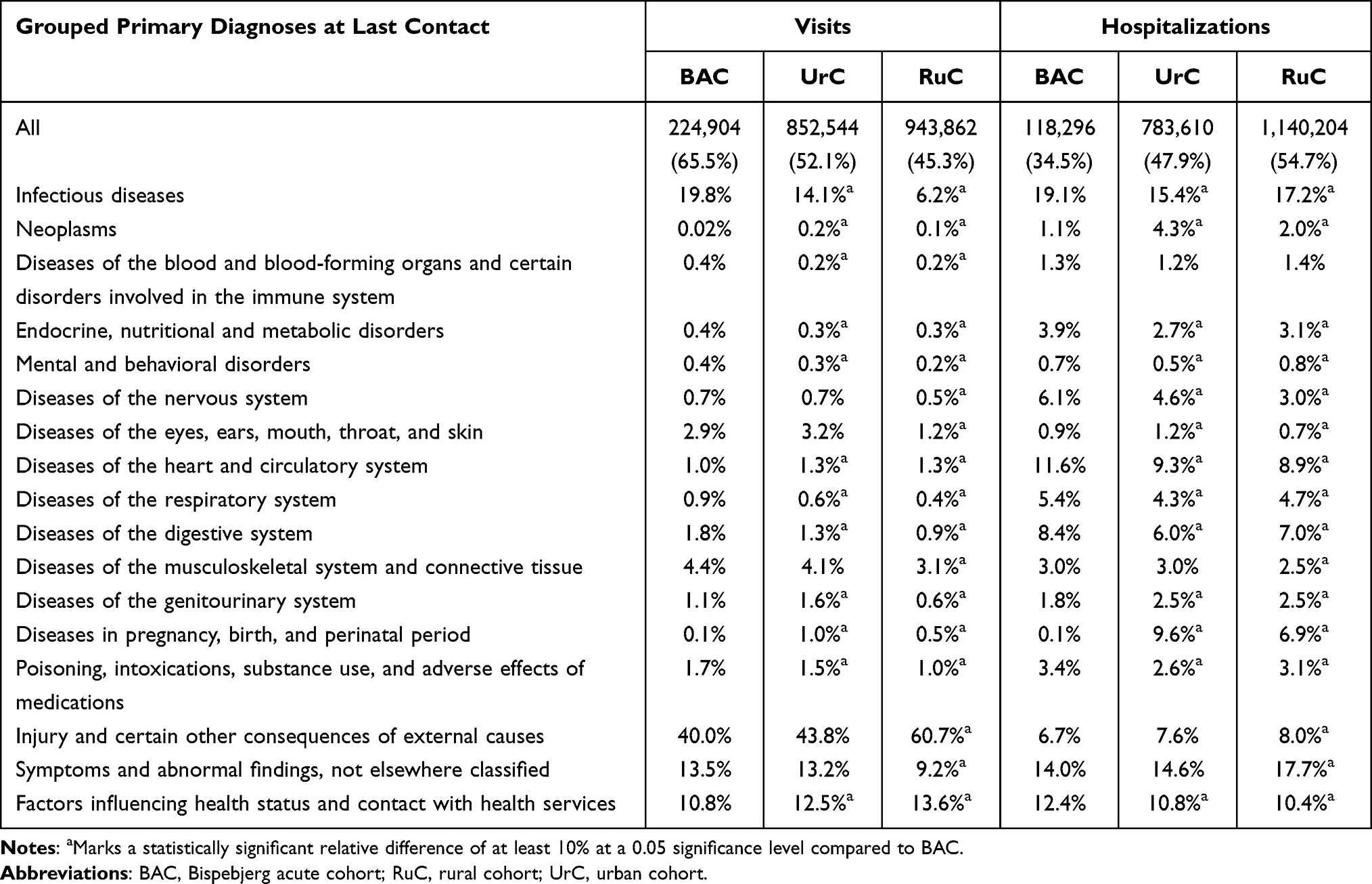 |
Table 4 Grouped Primary Diagnoses for Patients at Last Contact in a Hospital Contact |
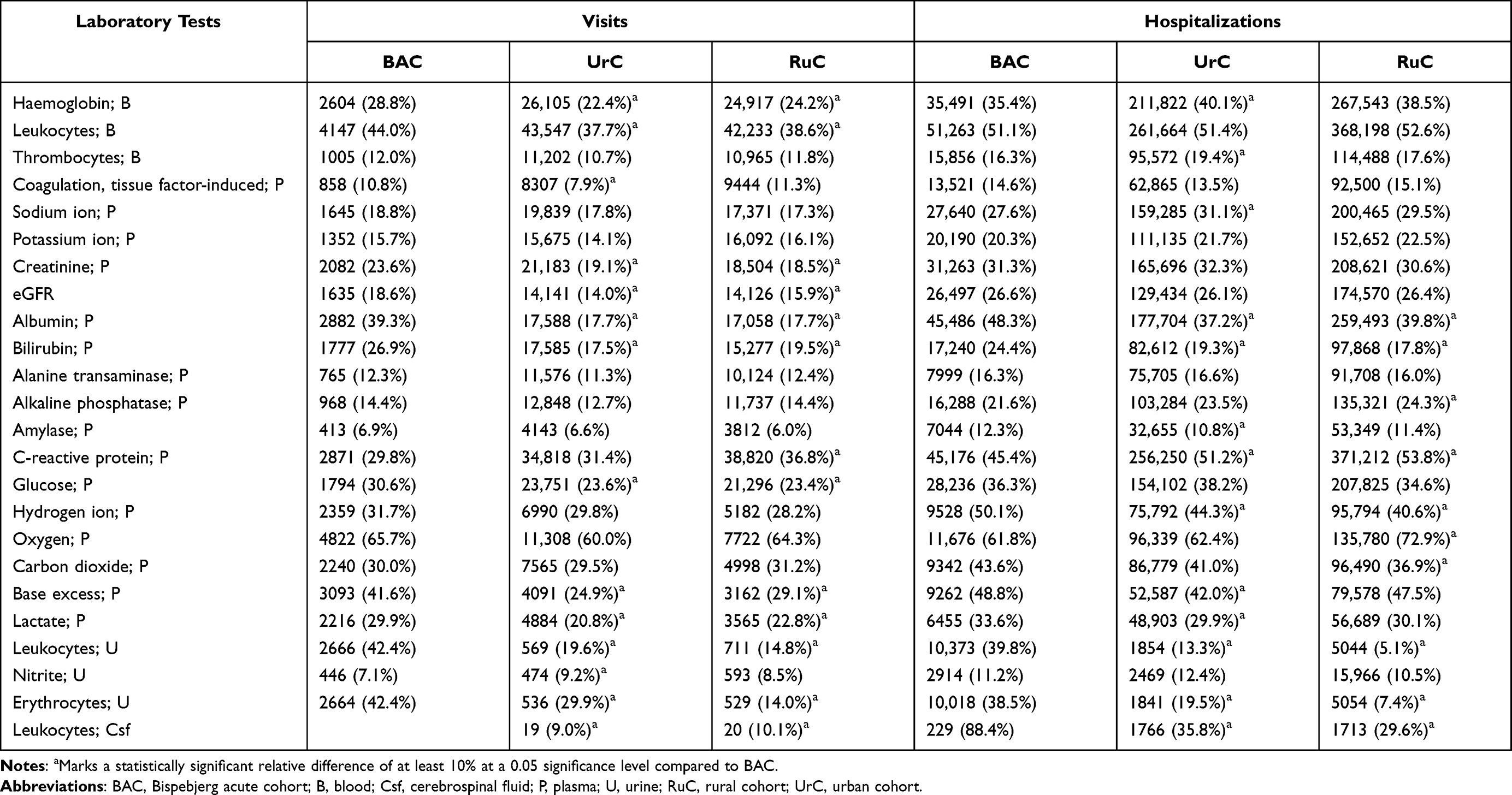 |
Table 5 Proportion of Abnormal Results for the First of Each Laboratory Tests |
Length of stay was similar in all three cohorts (Table 6). For patients discharged alive, the risk of 30-day mortality was similar across the cohorts, and BAC had a 30-day risk of readmission comparable to UrC, but higher than RuC.
 |
Table 6 Outcomes During and Following Hospital Contacts |
Subgroup
When patients <40 years or without permanent CPR were excluded, the differences in age, income, employment status, polypharmacy, medication groups, and primary diagnosis results diminished or disappeared, whereas differences in education, civil status, cohabitation, contact characteristics, and abnormal laboratory results remained almost unchanged (Supplementary B1–B6). Further, most differences in medication groups between BAC and UrC disappeared but remained more prevalent for RuC in most groups. Differences in length of stay and in-hospital mortality were unchanged, but the risk of readmission was higher for BAC than for the other cohorts.
Hospitalizations
Characteristics and Outcomes
Hospitalizations in BAC had higher median age than in UrC but were similar to RuC (Table 1). Temporary CPR and living alone were more common in BAC than in other cohorts, and fewer were married in BAC. Patients in BAC had a higher educational level than in RuC but comparable to UrC. Income was similar for BAC and the other cohorts. BAC had more unemployed, UrC had more in employment, and RuC had more disability pensioners. Hyperpolypharmacy was more common in RuC (Table 2). The frequencies of most medication groups were similar, except for psycholeptics, which were more common in BAC; psychoanaleptics, anti-inflammatory drugs, and mineral supplements, which were more common in RuC; and drugs for obstructive airway diseases, which were less common in UrC. Hospitalizations in BAC were less often initiated with a planned contact or during nighttime (Table 3). Hospital contact involving a psychiatric Department was more frequent for BAC than for UrC but was similar to RuC. UrC had more hospitalization patients from other regions. BAC had a higher proportion of infectious, endocrine, cardiovascular, respiratory, digestive, and neurological diseases, and a considerably lower proportion of diseases regarding pregnancy, birth, and perinatal period than UrC and RuC (Table 4). The proportion of abnormal laboratory results was similar for most tests, except for a predominance of abnormal plasma albumin, bilirubin, and hydrogen ion (pH); urine erythrocytes and leukocytes; and cerebrospinal fluid leukocytes, and at the same time fewer abnormal C-reactive protein results in BAC compared to UrC and RuC (Table 5). Compared to BAC, RuC had an overweight of abnormal blood haemoglobin and thrombocytes.
The median length of stay was higher for UrC than for BAC and RuC, and UrC had a higher risk of in-hospital mortality than BAC and RuC but slightly below our pre-defined level of relevance (Table 6). Risk of 30-day mortality after discharge was higher for RuC than BAC and UrC, but BAC had an increased risk of 30-day readmission compared with UrC and RuC.
Subgroup
Subgroup analyses of patients >40 years and patients with a permanent CPR leveled out age differences, while differences in employment status, contact characteristics, and discharge diagnoses decreased (Supplementary B1–B6). Differences in education level increased, while differences in income, civil status, cohabitation, hyperpolypharmacy, medication groups, and abnormal laboratory results were largely unchanged. The proportion of female patients remained unchanged for BAC but decreased considerably for the other cohorts. Differences of length of stay, in-hospital mortality, and risk of readmission were unaffected, but risk of mortality after being discharged was lower for BAC compared with UrC and RuC.
Discussion
We have presented patient characteristics, prescription groups, contact characteristics, primary diagnoses, laboratory results, and outcomes for a metropolitan acute cohort, BAC, constituting more than eight percent of all acute hospital contacts in Denmark. We compared patient characteristics and outcomes with other hospital cohorts to examine differences across the regions that may affect generalizability. To our knowledge, this is the first nationwide comparative study between a metropolitan hospital, hospitals in large cities, and hospitals in smaller cities. Our study revealed partly age-dependent differences in characteristics regarding visits between BAC and the other two comparison cohorts and, to a lesser degree, hospitalizations, where BAC and UrC were almost similar. Risk of in-hospital mortality was higher for UrC than for BAC and RuC in both regular and subgroup analyses. RuC had a higher risk of 30-day mortality after hospitalizations than BAC and UrC, but in subgroup analysis BAC had a lower risk than both UrC and RuC. Opposingly, BAC had a higher risk of readmission.
Visits
Comparisons of visits were primarily reflected by differences in healthcare structure since DNPR acute visits in the Capital Region also include contacts which are handled by out-of-hours GPs in other regions. After the 2014 Capital Region reorganization, patients with mild diseases were seen in ED fast tracks instead of by out-of-hours GPs, a drastic increase in the total number of acute contacts and a doubling of discharge diagnoses with infectious diseases has been observed.2 In agreement with this, we found significant differences in injury-related primary diagnoses (60.7% for RuC compared with 40.0% for BAC), showing that the causes of visits differ between the cohorts. Our sensitivity analysis showed that this difference was mainly between the Capital Region and the other regions.
Further, BAC visit patients were substantially younger than those in UrC and RuC. The age difference was in concordance with the average age differences across catchment areas, where the two municipalities (out of 98) in BAC have the lowest and fifth-lowest average age.5 The disparities in age and causes of contact may result in differences in all other compared characteristics since they are largely age-dependent. Our subgroup analyses reduced some, but not all, of these differences. Due to these national differences in healthcare structure, it is challenging to establish if metropolitan acute visits are different from urban and rural acute visits. It appears that there are both regional and local variations that should be considered when comparing visit contacts.
Hospitalizations
There were fewer but important differences between BAC and the comparison cohorts. Most notably, patients in UrC were younger than in BAC and RuC, which could also cause differences in other patient characteristics, if correlated with age. Hospitalized patients in BAC lived alone considerably more often, which may increase the risk of readmission and mortality.17,33
A Scottish study discovered a significant association between multimorbidity and living area among hospitalized patients, with less frequent multimorbidity in remote rural areas (22.0%), but otherwise comparable proportions between urban and small-town areas (27.8–29.1%).10 In agreement with these findings, comorbidity in the present study was more common in BAC (42.6%) than in UrC (39.9%) and RuC (38.9%), although the median age was comparable between BAC and RuC, and higher for UrC. Opposingly, hyperpolypharmacy was more common in RuC. The identified differences in discharge diagnoses largely reflect the specialties present at our hospitals.
A US study including both acute and planned hospitalizations showed a difference in mortality between urban and rural groups,7 and another US study found that this difference is increasing over time.9 In contrast, we discovered a lower in-hospital mortality for BAC and RuC compared with UrC, although UrC had lower age and comorbidity burden. This suggests that the excess mortality found in rural US is not present in Denmark when considering acute care – and might even be the opposite, with a higher risk for urban patients. Except for a Swedish two-center investigation of patients with acute chest pain that showed no difference in mortality between an urban and rural setting, no large-scale comparisons have been conducted in a European setting.34
Perspectives
Perspectives of Current Findings
Differences between metropolitan, urban, and rural hospitals can be caused by differences on several levels, eg, local variations in medical specialties, transfers, and patient flow; regional differences in the handling of patients with mild symptoms; and both local and regional differences in demographics and socioeconomics of the inhabitants.1,2,5 Regarding acute visits, our comparisons are influenced mainly by the differences in healthcare structure. However, comparisons of hospitalizations were only to a minor degree affected by healthcare structure, and highlighted that a metropolitan cohort is different from urban and rural cohorts, and that BAC might not be completely representative of all acute contacts in Denmark. The present study provides important, potential confounders when comparing acute contacts of metropolitan, urban, and rural catchment areas. Many of the characteristics are internally correlated, and thereby differences in one characteristic (eg age) can cause differences in other characteristics. Demographics of the general population have previously been compared between the five regions of Denmark, showing a large degree of homogeneity, except for differences in urbanization and population density.35 This study highlights that there may be differences in patient characteristics within the same region and across regions, especially since there are differences in the healthcare organization. We found that during the three-year study period, more than a third of all adult inhabitants had at least one acute contact. However, for this study, we included all types of acute hospital contacts, which besides trauma and acute diseases in emergency departments or hospital wards, also included acute visits at hospital ambulatories, acute pregnancy- and birth-related contacts, and out-of-hours GP contacts (only for the Capital Region).
While national healthcare structures, policies, and population demographics differ between countries and affect international generalization, the current results are also relevant in other countries. Based on population Denmark is a medium-sized European country (no. 25 of 51)36 and Copenhagen is medium-sized capital city and metropole (the 34th largest urban agglomeration in Europe 2020 with 1.35mio inhabitants).37 Thereby our findings should be relevant for most of Europe and possibly also non-European settings with comparable living standards and healthcare structure. Among others, our study shows that acute patients in a metropolitan catchment area more often have a temporary CPR number (not permanent address), more often live alone, and have a higher comorbidity burden, but also have a higher educational level. These differences can be relevant to consider in the interpretation of research findings in other countries or cities (both metropolitan, urban, or rural) or organizational when planning healthcare structure for acute patients.
Perspectives of the Database
BAC comprises almost 10% of the total acute hospital contacts in Denmark and enables research on the entirety of acute patients, with a focus on a single metropolitan hospital and with the possibility of assessing differences across hospitals and regions. While the Danish national registers include large amounts of relevant data, other supplementary data could be of importance. For specific research hypotheses, it is possible to obtain permission to merge clinical information (such as symptoms, triage, and vitals which unfortunately are not registered in DNPR) from the EMS databases and from the electronic patient record Sundhedsplatformen (Epic) with our database.3,26 Thereby, we will obtain substantial information about the patient at arrival and during stay, providing new research possibilities. Further, some of the existing Danish clinical quality databases can provide detailed information on predefined groups of patients.3,38 Other external databases, such as the Danish Poison Information Center, may add valuable information. The Register of Hospital Medication will become available soon and provides information on medication during hospital stay. Further on, BAC is in the process of establishing an infrastructure for collection of biological material and relevant clinical information that may not be obtained otherwise.
With the addition of clinical information from different sources, many major limitations usually associated with research based on the Danish national registers could be minimized. A focus, among others, will be the investigation of the prevalence of inter- and intrahospital transfers and their consequences; differences in unplanned readmission rates across diagnoses and specialties; cooperation between GPs, EMS, and hospitals; and the impact of different patient sociodemographics. To our knowledge, this is the first hospital-wide examination of all acute hospital contacts, and as such, it hopefully could serve as a point of reference for other studies.
Strengths and Limitations
The strength of this study is the use of prospectively collected nationwide data on all adult acute patients and access to high-quality and well-described information from the CPR number based national Danish registers. Large epidemiological studies with long-term and complete follow-up on the Danish population are used in many studies and have been considered an invaluable data resource.3
The current study also has limitations. The database is based on administrative data, which may cause bias, eg, bias of misclassification or selection. Acute hospitalization contacts in DNPR have a high validity,39 but the accuracy of acute visit contacts is undetermined – and should be topic for future research. Comorbidity was defined from all previous DNPR contacts, but thereby missing for patients at their first contact. Primary discharge diagnoses are coded by the physician responsible for discharging the patient and might be subject to personal or regional variation and preference.3 RLRR does not include information from the Central Denmark Region, which caused missing information.20 However, we primarily analyzed proportions of abnormal results from those who had analyses registered. RLRR might be subject to local differences in registration of point-of-care analyses and selection of patients to examine. For patients in BAC, some analyses (most notably urine erythrocytes and leukocytes, but also plasma albumin and bilirubin) were much more often abnormal than the other cohorts, supporting differences in registration.
All acute visit contacts, regardless of whether the contact was in an ED, hospital ward or ambulatory clinic, were included in this study. Consequently, 6.7% of the visits in BAC were outside the ED. We included combined contacts rather than individuals so that patients with several hospital contacts affect the averages more than patients with just one hospital contact. Our algorithm for combining contacts in DNPR differs from others.2,4,29,40 Based on our previous experience with DNPR coding, we chose a 4-hour window.41 Fløjstrup et al have only found minor differences between a 3-, 6- and 12-hour window in sensitivity analyses.2 We included planned contacts and contacts at psychiatric departments to investigate how often these were present in acute hospital contacts. Acute hospital contacts started with a planned contact in 4.3–11.8% of hospital contacts, and 1.4–1.8% of hospitalizations included contacts at the psychiatric departments. Patients with temporary CPR were not excluded, and we showed that they represent a considerable proportion of the work with acute patients, especially in urban hospitals. Due to the large sample-size, we were able to identify even small, statistically significant results, and therefore highlighted only difference with a 99% confidence interval difference of 10%. However, smaller or lack of differences are also worth considering.
Conclusion
The study outlines the establishment and research perspectives of BAC, a metropolitan and national acute hospital contact database. The presentation of patient characteristics, hospital course, and outcomes in BAC and comparing them to acutely admitted patients from urban and rural catchment areas revealed important differences between the catchment areas. Healthcare structure influenced the comparison of visits, but differences were also present among hospitalizations. This shows that acute contacts in metropolitan hospitals are different and not always representative of the general population, which should be considered when evaluating findings on local cohorts. It is also worth considering when planning healthcare structure since metropolitan acute care hospitals should expect more younger patients with different contact characteristics, more visiting tourists, and patients more often living alone, possibly with limited social support.
Abbreviations
BAC, Bispebjerg acute cohort; BFH, Bispebjerg and Frederiksberg Hospital; CPR, Det Centrale Personregister; DNPR, Danish National Patient Registry; ED, emergency department; GPs, general practitioners; RLRR, Register of Laboratory Results for Research; RuC, rural cohort; UrC, urban cohort.
Data Sharing Statement
Since the data is protected by Danish legislations, it cannot be made available neither publicly, nor privately. Approved Danish research institutions can apply for an equivalent data material through Statistics Denmark and the Danish Health Data Authority.
Ethics Approval and Informed Consent
According to Danish law, ethical approval is not needed for registry-based studies. The project was approved by Statistics Denmark (project number: 707838) and the Data Protection Agency (P-2019-616).
Acknowledgments
We would like to express our thanks to Diana Kali for providing linguistic support. Further, we thank Karina Aaroe Grossmeyer at RegionH Design for producing Figure 1.
Author Contributions
Initial conceptualization: Finn E. Nielsen, Janne Petersen, Rasmus Gregersen, Henriette Husum Bak-Jensen, Allan Linneberg, Olav Wendelboe Nielsen, Simon Francis Thomsen, Christian S. Meyhoff, Kim Dalhoff, Michael Krogsgaard, Henrik Palm, Hanne Christensen, Celeste Porsbjerg, Kristian Antonsen, Steen B. Haugaard, and Jørgen Rungby. Data acquisition and methodology: Rasmus Gregersen, Cathrine Fox Maule, Henriette Husum Bak-Jensen, Janne Petersen, and Finn E. Nielsen. Data management and formal analysis: Rasmus Gregersen and Cathrine Fox Maule. Primary investigator and writing initial draft: Rasmus Gregersen. Primary supervision and revision: Janne Petersen and Finn E. Nielsen Visualization: RegionH Design, under instructions from Rasmus Gregersen. Funding acquisition: Finn E. Nielsen, Janne Petersen, Henriette Husum Bak-Jensen, Allan Linneberg, Olav Wendelboe Nielsen, Simon Francis Thomsen, Christian S. Meyhoff, Kim Dalhoff, Michael Krogsgaard, Henrik Palm, Hanne Christensen, Celeste Porsbjerg, Steen B. Haugaard, and Kristian Antonsen. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; all authors have agreed upon submission to Clinical Epidemiology, have provided final approval, and take full responsibility for all aspects and contents of the work.
Funding
The project was financed by the Bispebjerg and Frederiksberg Hospital Research Committee Fund, the Center for Translational Research, and the Department of Emergency Medicine.
Disclosure
Professor Olav Wendelboe Nielsen reports speaker fees from Novartis and Roche, outside the submitted work. Dr Christian S Meyhoff reports indirect research grants from Boehringer Ingelheim to his department, research grants from Merck, Sharp & Dohme to his department, personal fees for research and lecture from Radiometer, outside the submitted work; In addition, Dr Christian S Meyhoff has a patent “Wireless Assessment of Respiratory and circulatory Distress (WARD) – Clinical Support System (CSS) - an automated clinical support system to improve patient safety and outcomes” pending to WARD 247 ApS, which he is a co-founder. The authors report no other conflicts of interest in this work.
References
1. Danske Regioner, Sundhedsstyrelsen, Sundheds- og Ældreministeriet. De Danske Akutmodtagelser - Status 2016 [Danish Regions, The National Board of Health and Ministry of Health: the Danish Emergency Departments - Status 2016]; 2016. Available from: https://www.ft.dk/samling/20161/almdel/SUU/bilag/121/1706332.pdf.
2. Fløjstrup M, Bogh SB, Henriksen DP, Bech M, Johnsen SP, Brabrand M. Increasing emergency hospital activity in Denmark, 2005–2016: a nationwide descriptive study. BMJ Open. 2020;10(2):2. doi:10.1136/bmjopen-2019-031409
3. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
4. Lassen AT, Jørgensen H, Jørsboe HB. Databasen for Akutte Hospitalskontakter - årsrapport 2018 [The Danish database for acute and emergency hospital contacts - Annual Report 2018]. Clin Epidemiol. 2016;8:1–56. doi:10.2147/CLEP.S95847
5. Danmarks Statistik. Gennemsnitsalder efter kommune og tid, år 2016–2018. [Statistics Denmark. Average age by municipality and year, years 2016–2018]. Available from: www.statistikbanken.dk/BY2. Accessed September 9, 2021
6. Lower T, Kinsman L, MM D, et al. Patterns of emergency department use in rural and metropolitan New South Wales from 2012 to 2018. Aust J Rural Health. 2020;28(5):1–10. doi:10.1111/ajr.12668
7. Elson LE, Luke AA, Barker AR, McBride TD, Joynt Maddox KE. Trends in hospital mortality for uninsured rural and urban populations, 2012–2016. J Rural Health. 2020;37:1–10. doi:10.1111/jrh.12425
8. Yi JY, Kim H, Chi I. Urban–rural differences in multimorbidity and associated factors in China and Korea: a population-based survey study. Geriatr Gerontol Int. 2019;19(11):1157–1164. doi:10.1111/ggi.13771
9. Villapiano N, Iwashyna TJ, Davis MM. Worsening rural-urban gap in hospital mortality. J Am Board Fam Med. 2017;30(6):816–823. doi:10.3122/jabfm.2017.06.170137
10. Robertson L, Ayansina D, Johnston M, Marks A, Black C. Urban–rural and socioeconomic status: impact on multimorbidity prevalence in hospitalized patients. J Comorbidity. 2020;10:2235042X1989347. doi:10.1177/2235042x19893470
11. Klinge M, Aasbrenn M, Aasbrenn M, et al. Readmission of older acutely admitted medical patients after short-term admissions in Denmark: a nationwide cohort study. BMC Geriatr. 2020;20(1):1–10. doi:10.1186/s12877-020-01599-4
12. Tanderup A, Lassen AT, Rosholm JU, Ryg J. Disability and morbidity among older patients in the emergency department: a Danish population-based cohort study. BMJ Open. 2018;8(12):12. doi:10.1136/bmjopen-2018-023803
13. Osler M, Mårtensson S, Prescott E, Carlsen K. Impact of gender, co-morbidity and social factors on labour market affiliation after first admission for acute coronary syndrome. A cohort study of Danish patients 2001–2009. PLoS One. 2014;9(1):e86758. doi:10.1371/journal.pone.0086758
14. Brockhattingen KK, Anru PL, Masud T, Petrovic M, Ryg J. Association between number of medications and mortality in geriatric inpatients: a Danish nationwide register-based cohort study. Eur Geriatr Med. 2020;11(6):1063–1071. doi:10.1007/s41999-020-00390-3
15. Demir TA, Yılmaz F, Sönmez BM, Karadaş MA, Okudan RN, Keskin O. Association of optic nerve sheath diameter measurement with hyponatremia in emergency department. Am J Emerg Med. 2019;37(10):1876–1879. doi:10.1016/j.ajem.2018.12.054
16. Obermeyer Z, Cohn B, Wilson M, Jena AB, Cutler DM. Early death after discharge from emergency departments: analysis of national US insurance claims data. BMJ. 2017;356. doi:10.1136/bmj.j239
17. Aminzadeh F, Dalziel WB. Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med. 2002;39(3):238–247. doi:10.1067/mem.2002.121523
18. Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
19. Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish national prescription registry. Int J Epidemiol. 2017;46(3):798. doi:10.1093/ije/dyw213
20. Arendt JFH, Hansen AT, Ladefoged SA, Sørensen HT, Pedersen L, Adelborg K. Existing data sources in clinical epidemiology: laboratory information system databases in Denmark. Clin Epidemiol. 2020;12:469–475. doi:10.2147/CLEP.S245060
21. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
22. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7):103–105. doi:10.1177/1403494811405098
23. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7):91–94. doi:10.1177/1403494810394715
24. Christensen G. The building and housing register. J Public Health. 2011;39:106–108. doi:10.1177/1403494811399168
25. Ministry of Health. Healthcare in Denmark: an overview; 2017. Available from: http://www.sum.dk.
26. Lindskou TA, Mikkelsen S, Christensen EF, et al. The Danish prehospital emergency healthcare system and research possibilities. Scand J Trauma Resusc Emerg Med. 2019;27(1):1–7. doi:10.1186/s13049-019-0676-5
27. Region Hovedstaden. Hospitals- og Psykiatriplan 2020. [The Capital Region of Denmark. Plan for Hospitals and Psychiatry 2020]. 2015:1–93.
28. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
29. Lassen AT, Jørgensen H, Jørsboe HB, et al. The Danish database for acute and emergency hospital contacts. Clin Epidemiol. 2016;8:469–474. doi:10.2147/CLEP.S99505
30. UNESCO Institute for Statistics. United Nations Educational Scientific and Cultural Organization (UNESCO) institute for statistics. ISCED. 2011;2012. doi:10.1007/BF02207511
31. Vest-Hansen B, Riis AH, Sørensen HT, Christiansen CF. Acute admissions to medical departments in Denmark: diagnoses and patient characteristics. Eur J Intern Med. 2014;25(7):639–645. doi:10.1016/j.ejim.2014.06.017
32. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):1–22. doi:10.1371/journal.pmed.1001885
33. Laugesen K, Baggesen LM, Schmidt SAJ, et al. Social isolation and all-cause mortality: a population-based cohort study in Denmark. Sci Rep. 2018;8(1):4–11. doi:10.1038/s41598-018-22963-w
34. Karlson BW, Karlsson T, Kalin B, Svensson L, Zehlertz E, Herlitz J. Patients admitted to the emergency department with acute chest pain–is there a difference between patients in an urban and a rural area? Eur J Emerg Med. 2000;7(4):277–286. doi:10.1097/00063110-200012000-00005
35. Henriksen DP, Rasmussen L, Hansen MR, Hallas J, Pottegård A. Comparison of the five Danish regions regarding demographic characteristics, healthcare utilization, and medication use - A descriptive cross-sectional study. PLoS One. 2015;10(10):1–12. doi:10.1371/journal.pone.0140197
36. Wikipedia The Free Encyclopedia. List of European countries by population. Available from: https://en.wikipedia.org/wiki/List_of_European_countries_by_population.
37. Statista. Largest urban agglomerations in Europe in 2020; 2022. Available from: https://www.statista.com/statistics/1101883/largest-european-cities/.
38. Sørensen HT, Pedersen L, Jørgensen J, Ehrenstein V. Danish clinical quality databases – an important and untapped resource for clinical research. Clin Epidemiol. 2016;8:425–427. doi:10.2147/CLEP.S113265
39. Vest-Hansen B, Hammerich riis A, Fynbo christiansen C. Registration of acute medical hospital admissions in the Danish National Patient Registry: a validation study. Clin Epidemiol. 2013;5(1):129–133. doi:10.2147/CLEP.S41905
40. Hansen KM, Nielsen H, Vest-Hansen B, et al. Readmission and mortality in patients discharged with a diagnosis of medical observation and evaluation (Z03*-codes) from an acute admission unit in Denmark: a prospective cohort study. BMC Health Serv Res. 2017;17(1):1–7. doi:10.1186/s12913-017-2156-9
41. Klausen HH, Petersen J, Bandholm T, et al. Association between routine laboratory tests and long-term mortality among acutely admitted older medical patients: a cohort study. BMC Geriatr. 2017;17(1):1–14. doi:10.1186/s12877-017-0434-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.