Back to Journals » Infection and Drug Resistance » Volume 8
Profile and microbiological isolates of asymptomatic bacteriuria among pregnant women in Abakaliki, Nigeria
Authors Onu F, Ajah L ![]() , Ezeonu P, Umeora O, Ibekwe P, Ajah M
, Ezeonu P, Umeora O, Ibekwe P, Ajah M
Received 21 April 2015
Accepted for publication 3 June 2015
Published 24 July 2015 Volume 2015:8 Pages 231—235
DOI https://doi.org/10.2147/IDR.S87052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Fidelis Agwu Onu,1 Leonard Ogbonna Ajah,1 Paul Olisaemeka Ezeonu,1 Odidika Ugochukwu Joannes Umeora,1 Perpetus Chudi Ibekwe,1 Monique Iheoma Ajah2
1Department of Obstetrics and Gynaecology, Federal Teaching Hospital, 2Department of Microbiology, Ebonyi State University, Abakaliki, Nigeria
Background: Detecting and treating asymptomatic bacteriuria (ASB) prevents urinary tract infection and its consequences. The cost-effectiveness of routine screening for ASB in pregnancy is controversial. In populations with high prevalence, however, it is worthwhile and justifiable.
Aim: To determine the profile, prevalence, microbiological isolates, and risk factors of ASB among booking antenatal clinic attendees in Abakaliki, Nigeria.
Materials and methods: This was a cross-sectional study involving booking antenatal clinic attendees at the Federal Teaching Hospital, Abakaliki, who met the inclusion criteria. This study occurred between January and December, 2012. The midstream urine samples of these women were subjected to microscopy, culture, and sensitivity.
Results: A total of 300 randomly selected booking antenatal clinic attendees participated in the study; 74 of them had ASB, giving a prevalence of 24.7%. With the exception of rural residence, sociodemographic and obstetric characteristics did not influence the risk of ASB among the participants in this study. Staphylococcus aureus was the commonest organism isolated. The majority of the organisms were sensitive to ofloxacin and ceftriaxone.
Conclusion: There is a high prevalence of ASB among pregnant women in Abakaliki. With the exception of rural dwelling, sociodemographic and obstetric characteristics did not significantly influence the risk of ASB among these pregnant women. Therefore, routine ASB screening of pregnant women is recommended in our environment.
Keywords: asymptomatic bacteriuria, pregnant women, Abakaliki
Introduction
Asymptomatic bacteriuria (ASB) is defined as the presence of actively multiplying bacteria in the urinary tract, excluding the distal urethra, in a patient without obvious urinary symptoms.1 Profound physiologic and anatomic changes of the urinary tract during pregnancy contribute to the increased risk of ASB.2 ASB is a major risk factor for developing symptomatic urinary tract infections during pregnancy, and may be associated with adverse effects on maternal and fetal health.2 These adverse effects include pyelonephritis and adverse obstetric outcomes, such as prematurity, low birth weight, and higher fetal mortality rates. ASB is common in women, and increases in prevalence with age and/or sexual activity.3 The impact of ASB on pregnancy outcome has been a focus of controversy since the development of the quantitative urine-culture technique in the mid-1950s made it possible to differentiate women with bacteriuria from those without.2 These controversies center on the fact that even though it is generally accepted that ASB is detrimental to pregnancy, data available to support this contention are limited. Randomized controlled trials and cohort studies have shown that the detection and treatment of ASB can decrease the occurrence of acute pyelonephritis later in pregnancy and intrauterine growth restriction.2
The prevalence of ASB in pregnancy in developed countries varies from 4% to 7%, and may or may not be similar to that observed in nonpregnant women.4–6 Prevalent rates among pregnant Nigerian women have been variously reported to be between 4% and 78.7%.7–11 It is twice as common in pregnant women with sickle-cell trait, and three times as common in pregnant women with diabetes mellitus as in normal pregnant women.1 Other risk factors include increased age, high parity, poor perineal hygiene, history of recurrent urinary tract infection, neurogenic bladder, anatomic or functional urinary tract abnormality, increased frequency of sexual activity, and presence of vesicoureteric reflux.1 When ASB is untreated, 25%–40% of pregnant women, especially multiparous patients, will develop symptomatic urinary tract infection, including acute pyelonephritis.4 ASB has also been shown to be an important risk factor for preterm labor, perinatal mortality, preeclampsia, and anemia in pregnancy.3,4 The incidence of all the complications associated with ASB are significantly decreased with appropriate treatment.5
Many studies favor routine screening in pregnancy as opposed to screening only women at high risk for developing urinary tract infection.2,3 Patterson and Andriole recommended that all pregnant women be screened at the first antenatal visit, and this could be reliably done with a dipstick culture. This is because bacteriuria typically presents at the time of first prenatal visit, and only 1%–2% of pregnant women who are not bacteriuric at initial screening early in pregnancy will develop bacteriuria later in pregnancy.2 Screening for ASB is cost-effective, and can therefore be recommended.12–14
A high proportion of the women in Ebonyi State belong to the low socioeconomic class, have high parity, and reside in rural areas. These risk factors for ASB have been identified in previous studies.1,4,6 Even though a previous study in the subject matter was done in Abakaliki before,14 it was done 10 years ago, and the antibiotic sensitivity pattern was not determined then. It was because of this that this study was embarked upon. This study aimed to determine the profile, prevalence, microbiological isolates, and risk factors of ASB among pregnant women in Abakaliki. The findings from this study may encourage the commencement of routine urine microscopy, culture, and sensitivity at booking in the study center. It may also help determine the types of antibiotics to be used on pregnant women who have ASB.
Materials and methods
Study area
Ebonyi State has an estimated population of 4.3 million and occupies a land mass of 5,935 km2. Approximately 75% of the population of Ebonyi State dwell in rural areas with farming as the major occupation.15 The Federal Teaching Hospital, Abakaliki, is the only tertiary hospital in Ebonyi State. It receives referrals from all parts of the state and the neighboring states of Benue, Enugu, Cross River, and Abia. The hospital runs antenatal clinic from Monday through Friday every week.
Study design
This was a cross-sectional study of pregnant women who came for booking at the antenatal clinic of the Federal Teaching Hospital, Abakaliki, Ebonyi State between January and December, 2012. For subject selection, systematic random sampling was done. Here, every third of the women in the attendance register was picked after an initial random start. The inclusion criteria involved the booking of apparently healthy antenatal clinic attendees who gave their informed consent to participate in the study. However, the women excluded from the study were those who had features of urinary tract infection, fever, had taken antibiotics within 4 weeks of the study, had medical diseases like diabetes mellitus, retroviral disease, and sickle cell anemia, patients on steroid therapy, and those who declined consent despite adequate counseling.
All pregnant women booking at the antenatal clinic, who met the inclusion criteria, were counseled on how to collect midstream urine. This involved initial instructions by the female research assistants comprising two trained nurses and one house officer. The research assistants supervised the urine-sample collection. This involved initial cleaning of the vulva with clean running water. The first part of the urine was voided, and approximately 10–15 mL of midstream urine was collected in a sterile universal bottle containing 0.5 g boric acid crystal that had been correctly labeled and given to the patients. The urine samples in the sterile universal bottles were taken to the laboratory for processing within 1 hour. These samples were subjected to microscopy, culture, and sensitivity according to standard practice by two laboratory scientists. Analysis was done by the same pair of laboratory scientists for quality control.
Microscopy involved centrifugation of approximately 10 mL of urine sample in a test tube at 1,500 rpm. The sediments were poured on a clean slide and observed under a microscope for casts, pus cells, and red blood cells. Culture of the urine was carried out by inoculating a portion of the urine samples, which had been well mixed unto cysteine lactose electrolyte-deficient or MacConkey agar and blood agar plates (both Lab M Ltd, Heywood, UK) using a standard wire loop. The specimens were well streaked on the plates to allow for discrete colonies. Inoculated agar plates were incubated at 37°C overnight and read after 24 hours to access growth for significant bacteriuria. Significant bacteriuria is the presence of at least 105 single bacteria colonies per milliliter of urine and microscopy of three to five pus cells per high-power field. Suspected pathogens were identified using standard biochemical and sugar utilization tests.16 Following identification, the isolated microbes were subjected to antibiotic sensitivity testing using the disk diffusion technique. Multidisk (Oxoid; Thermo Fisher Scientific, Waltham, MA, USA) was used and interpreted in accordance with the zone-size interpretative chart using the Kirby–Bauer method.16
A questionnaire was used to obtain information from the study participants. The information obtained consisted of identification number, age, address, phone number, educational qualification, occupation of the participants, occupation of their partners, parity, gestational age, hemoglobin genotype, human immune virus status, fasting blood sugar and 2-hour postprandial result, urine microscopy, culture, and sensitivity result. The social class of the participants was determined based on the criteria by Olusanya et al.17
Sample-size estimation
The minimum sample size for the study was calculated based on the formula for estimating sample size for cross-sectional studies described by Daniel:18 n = z2P(1−P)/d2, where n = sample size, z = z-statistic for 95% level of confidence, P = expected prevalence or proportion, and d = precision. With z=1.96, P=0.787,14 and d=0.05, and adding an assumed attrition rate of 10%, the calculated minimum sample size was 284.
Data analysis
Data analysis was both descriptive and inferential at the 95% confidence level using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). Tests of significance were done with χ2 or Fischer’s exact test where appropriate. A P-value of less than or equal to 0.05 was considered statistically significant.
Ethical clearance
Ethical clearance for this study was obtained from the Ethics Committee of Federal Teaching Hospital, Abakaliki.
Results
A total of 300 booking antenatal clinic attendees who met the inclusion criteria participated in the study. The mean age of the women was 28.6±4.5 years, with age ranging from 19 to 44 years. A total 74 of the participants had ASB, giving a prevalence of 24.7%. Table 1 shows the influence of demographic characteristics, parity, and gestational age of the participants on ASB. The age, parity, social class, and gestational age of the participants did not have any statistical significant influence on ASB. However, women who resided in rural areas were more likely to have ASB when compared to urban dwellers. Table 2 contains the frequency distribution of the bacterial isolates from urine culture. The commonest bacteria isolated was Staphylococcus aureus. This was followed by Escherichia coli, unspecified coliform, and Proteus mirabilis, respectively. Table 3 shows the antibiotic sensitivity pattern of the organisms. The majority of the organisms (32.7%) were sensitive to ofloxacin. This was followed by ceftriaxone (23.1%). Moderate sensitivities were noticed in nitrofurantoin and gentamicin. Co-amoxiclav, cefuroxime, and cotrimoxazole were the least sensitive.
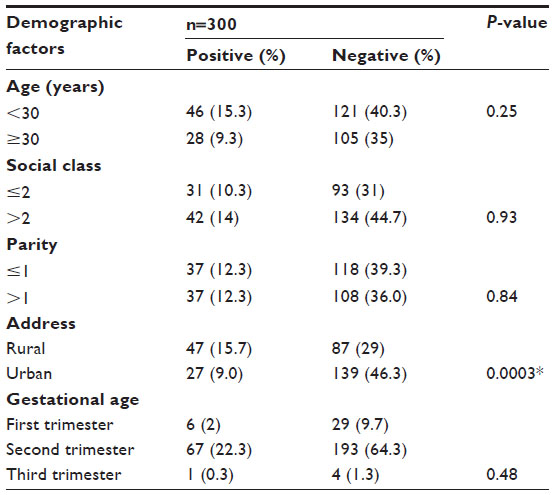 | Table 1 Influence of demographic characteristics, parity, and gestational age on asymptomatic bacteriuria |
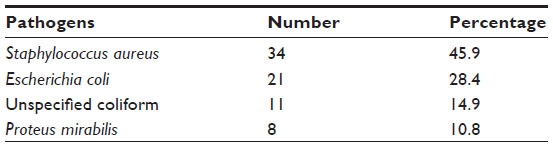 | Table 2 Frequency of pathogenic isolates |
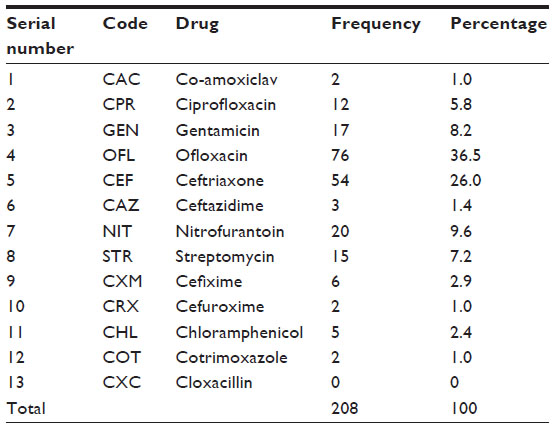 | Table 3 Antibiotic sensitivity pattern of the uropathogens |
Discussion
The principal findings from this study showed that the prevalence of ASB among women booking for antenatal care in Abakaliki was 24.7%. The age, parity, social class, and gestational age of the participants did not have any statistical significant influence on ASB. However, the pregnant women who resided in rural areas were more likely to have ASB. The bacteria isolated from urine culture were S. aureus (45.9%), E. coli (28.4%), unspecified coliform (14.9%), and P. mirabilis (10.8%). Majority of the organisms were sensitive to ofloxacin (32.7%) and ceftriaxone(23.1%). Moderate sensitivities were noticed in nitrofurantoin and gentamicin. Co-amoxiclav, cefuroxime, and cotrimoxazole were least sensitive.
The 24.7% prevalence of ASB recorded in this study is higher than the 15.1% reported in Enugu.9 It is however lower than the 78.7% and 86.6% previously reported at Abakaliki and Benin, respectively.14,19 This variability in rates may be influenced by the method of urine collection, which may be contaminated if not done properly. More so, the exclusion of pregnant women who had features of urinary tract infection, fever, diabetes mellitus, sickle-cell anemia, and retroviral disease and those on steroid therapy in this study might have made the prevalence of ASB less than the previous reports from Abakaliki and Benin.
The age distribution of the participants in this study appeared not to have any significant effect on ASB. This is contrary to a previous report in which advancing maternal age was linked with high prevalence of ASB. This could be because increasing maternal age was believed to be associated with comorbid conditions like neurogenic bladder and increased residual urine volume or urinary reflux.20 The absence of a significant effect of age on ASB in this study may have been due to the exclusion of certain medical disorders that predispose to ASB and are commoner at an advanced age. Educational level attained may be an indicator of the socioeconomic status of the women. Lower levels of education and low socioeconomic status have been related to higher prevalence of ASB in many studies and reports.21,22 This is because education improves the attitudes and beliefs of women and has a protective role against most of these morbidities.23 However, the social class of the participants in this study did not have any significant effect on ASB, which is contrary to previous reports.21–23 The significant association of ASB among rural dwellers in this study is supported by a previous report in India.24 This may be because of poor hygienic conditions and a lack of social amenities in rural areas.
Parity, not having an influence on ASB, in this study is similar to previous reports in Ibadan, Nigeria, and Ghana.7,25 However, this differed from another study where ASB in pregnancy was associated with increasing parity.26 The prevalence of ASB across the trimesters in this study showed no consistent pattern of influence. It did not tally either with observations by Awonuga et al, who found increasing prevalence with gestational age, or Nnatu et al, who found decreasing prevalence with duration of pregnancy.7,27 Trimester not having a significant effect on ASB in this study is similar to a previous report in Benin.27 S. aureus as the commonest bacteria isolated from urine culture in this study is consistent with studies in Nigeria and other places, where it is emerging as a common causative agent of ASB among pregnant women.14,20 However, this is contrary to reports in Benin, Nigeria, and Kumasi, Ghana, in which E. coli was the commonest bacteria isolated from culture.25,28 The highest sensitivity pattern exhibited by ofloxacin and ceftriaxone to the uropathogens in this study is similar to previous reports in Benin and Ekiti, where quinolones and cephalosporins had the highest sensitivity pattern to the bacterial isolates.28,29 This sensitivity pattern may help policy makers in determining the drugs to be provided for the treatment of ASB and urinary tract infections in this environment.
This study is weakened by its hospital-based design, which may not be a true reflection of what is happening in this society. However, it is strengthened by the randomization.
In conclusion, there is a high prevalence of ASB among pregnant women in Abakaliki. With the exception of rural dwelling, demographic and obstetric characteristics did not significantly influence the risk of ASB in this study population. S. aureus and E. coli were the dominant uropathogens isolated among the pregnant women. Ofloxacin and ceftriaxone had the highest sensitivity pattern to these uropathogens. In view of the high prevalence of ASB, routine urine microscopy, culture, and sensitivity testing are recommended for booking antenatal clinic attendees in this region. Health education on ASB and social amenities should be provided, especially in rural areas, to help stem the tide of this public health problem. A community-based study in this subject matter and in the puerperium is recommended.
Acknowledgments
The authors wish to acknowledge the two laboratory scientists – Mr Ibeagi and Mr Akan – for doing the urine microscopy, culture, and sensitivity of the study participants. The authors funded the project.
Disclosure
The authors report no conflicts of interest in this work.
References
Grewal M, Biswas MK. Cardiac, hematologic, pulmonary, renal and urinary tract disorders in pregnancy. In: A DeCherney AH, Nathan L, editors. Current Obstetric and Gynecologic Diagnosis and Treatment. 9th ed. New York: McGraw-Hill; 2003:387–427. | |
Patterson TF, Andriole VT. Bacteriuria in pregnancy. Infect Dis Clin North Am. 1987;1:807–822. | |
Patterson TF, Andriole VT. Detection, significance and therapy of bacteriuria in pregnancy: update in the managed health care era. Infect Dis Clin North Am. 1997;11(3):593–608. | |
Arias F, Daftary SN, Bhide AG. Abnormalities of the urinary system during pregnancy. In: Arias F, Daftary SN, Bhide AG, editors. Practical Guide to High-Risk Pregnancy and Delivery: A South Asian Perspective. 3rd ed. New Delhi: Elsevier; 2008:489–505. | |
Smaill F, Vazquez JC. Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane Database Syst Rev. 2007 Apr 18;(2):CD000490. | |
Peterside N, Adegoke AO. Asymptomatic Bacteriuria in pregnant and non-pregnant women at University of Port Harcourt Teaching Hospital. J Med Lab Sci. 2007;16(1):40–40. | |
Awonuga DA, Fawole AO, Dada-Adegbola HA, Olola FA, Awonuga OM. Predictors of asymptomatic bacteriuria among obstetric population in Ibadan. Niger J Med. 2010;19:188–193. | |
Onyemelukwe NF, Obi SN, Ozumba BC. Significant bacteriuria in pregnancy in Enugu, Nigeria. Int J Med Health Dev. 2003;8:20–22. | |
Ikeme AC, Ezeome IV, Okezie OA, Onyebueke EA. Asymptomatic bacteriuria in pregnant women in Enugu, Nigeria. Trop J Obstet Gynaecol. 2006;23:12–13. | |
Oyetunji JA, Ahmed Y, Nwobodo IE, Airede LR, Ekele BA. Asymptomatic bacteriuria in pregnancy in Sokoto. Sahel Med J. 2006;9(1):1–6. | |
Oli AN, Okafor CI, Ibezim EC, Akujiobi CN, Onwunzo MC. The prevalence and bacteriology of asymptomatic bacteriuria among antenatal patients in Nnamdi Azikiwe University Teaching Hospital Nnewi, South East Nigeria. Niger J Clin Pract. 2010;13:409–412. | |
US Preventive Services Task Force. Screening for Asymptomatic Bacteriuria: Recommendation Statement. Rockville (MD): Agency for Healthcare Research and Quality; 2004. | |
US Preventive Services Task Force. Screening for Asymptomatic Bacteriuria: Guide to Clinical Preventive Services. 2nd ed. Washington: US Department of Health and Human Services, Office of Disease Prevention and Health Promotion; 1996. | |
Amadi ES, Enemuo OB, Uneke CJ, Nwosu OK, Onyeagba RA, Ugbogu OC. Asymptomatic bacteriuria among pregnant women in Abakaliki, Ebonyi State Nigeria. J Med Sci. 2007;7:698–700. | |
Ezegwui HU, Onoh RC, Ikeako LC, et al. Investigating maternal mortality in a public teaching hospital, Abakaliki, Ebonyi State, Nigeria. Ann Med Health Sci Res. 2013;3:75–80. | |
Cheesbrough M. District Laboratory Practice in Tropical Countries: Part 2. Cambridge, UK: Cambridge University Press; 2004. | |
Olusanya O, Okpere E, Ezimokhai M. The importance of social class in voluntary fertility control in a developing country. West Afr J Med.1985;4:205–212. | |
Daniel WW. Biostatistics: A Foundation for Analysis in the Health Sciences. 7th ed. New York: John Wiley & Sons; 1999. | |
Akerele J, Abhulimen P, Okonufua F. Prevalence of asymptomatic bacteriuria among pregnant women in Benin City, Nigeria. J Obstet Gynaecol. 2001;21:141–144. | |
Tungrul S, Oral O, Kumru P, Köse D, Alkan A, Yildirim G. Evaluation and importance of asymptomatic bacteriuria in pregnancy. Clin Exp Obstet Gynecol. 2005;32:237–240. | |
Faro S, Fenner DE. Urinary tract infections. Clin Exp Obstet Gynecol. 1998;41:744–754. | |
Younis N, Khattab H, Zurayk H, El-Mouelhy M, Amin MF, Faray AM. A community study of gynaecological and related morbidities in rural Egypt. Stud Fam Plann. 1993;24:175–186. | |
Cline MK, Bailey-Dorton C, Cayelli M. Maternal infections: diagnosis and treatment. Prim Care. 2000;27:13–33. | |
Lallar M, ul Haq A, Nandal R. Asymptomatic bacteriuria: predisposing factors and correlation with preterm labor in low resource settings. Int J Reprod Contracept Obstet Gynecol. 2014;3:403–408. | |
Obirikorang C, Quaye L, Bio FY, Amidu N, Acheampong I, Addo K. Asymptomatic bacteriuria among pregnant women attending antenatal clinic at the University Hospital, Kumasi, Ghana. J Med Biomed Sci. 2012;1:38–44. | |
Stenqvist K, Dahlén-Nilsson I, Lidin-Janson G, et al. Bacteriuria in pregnancy: frequency and risk of acquisition. Am J Epidemiol. 1989;192:372–379. | |
Nnatu S, Essien EE, Akinkugbe A, Odum CU. Asymptomatic bacteriuria in pregnant Nigerian patients. Clin Exp Obstet Gynaecol. 1989;16:126–129. | |
Imade PE, Izekor PE, Eghafona NO, Enabulele OI, Ophori E. Asymptomatic bacteriuria among pregnant women. N Am J Med Sci. 2010;2:263–266. | |
Ade-Ojo IP, Oluyege AO, Adegun PT, Akintayo AA, Aduloju OP, Olofinbiyi BA. Prevalence and antimicrobial suseptibility [sic] of asymptomatic significant bacteriuria among new antenatal enrollees in Southwest Nigeria. Int Res J Microbiol. 2013;4:197–203. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.