Back to Journals » Clinical Interventions in Aging » Volume 18
Procedural Intervention for Benign Prostatic Hyperplasia in Men ≥ Age 70 Years – A Review of Published Literature
Authors Codelia-Anjum AJ, Berjaoui MB, Khondker A, Elterman D, Zorn KC, Bhojani N ![]() , Lerner LB, Chughtai B
, Lerner LB, Chughtai B
Received 13 July 2023
Accepted for publication 25 September 2023
Published 11 October 2023 Volume 2023:18 Pages 1705—1717
DOI https://doi.org/10.2147/CIA.S414799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Alia J Codelia-Anjum,1,* Mohamad Baker Berjaoui,2,* Adree Khondker,2 Dean Elterman,2 Kevin C Zorn,3 Naeem Bhojani,3 Lori B Lerner,4 Bilal Chughtai1
1Department of Urology, Weill Cornell Medical College/New York Presbyterian, New York, NY, USA; 2Division of Urology, Department of Surgery, University Health Network, University of Toronto, Toronto, ON, Canada; 3Division of Urology, Centre Hospitalier de l’Université de Montréal, Montreal, QC, Canada; 4Department of Urology, VA Boston Healthcare System, Boston, MA, USA
*These authors contributed equally to this work
Correspondence: Bilal Chughtai, Weill Cornell Medical Center, Department of Urology, 425 East 61st Street, 12th Floor, New York, NY, 10065, USA, Tel +1 646 962-4811, Email [email protected]
Objective: We set out to review studies reporting on the use of surgical intervention to treat Benign Prostatic Hyperplasia in elderly men ≥ 70 years of age.
Methods: A systematic literature search was conducted using Scopus, PubMed-MEDLINE, Cochrane, and Wiley Online Library databases including studies published between January 2012 through December 2022. This 10-year interval was chosen given the recent plethora of new modalities that have entered the BPH armamentarium, many of which have been marketed as appropriate for older and high-risk patients. The following database search words were used either individually or in conjunction: “BPH”, “elderly”, “surgical”, “ablation”, “resection”, “embolization”, and “aging”.
Results: We identified 28 studies for inclusion in this review. The pros and cons of these modalities are presented, specifically as applicable to an older and higher risk population.
Conclusion: There are a wide variety of surgical procedures available for surgically treating BPH in elderly men with varying states of health. Each of these comes with different risks and benefits, supporting that individualized approaches are important. Long-term data and further studies comparing modalities, specifically as regards the elderly and frail, would enhance our approaches to BPH treatment in this patient population.
Keywords: benign prostatic hyperplasia, aging, elderly, surgical
Introduction
Benign prostatic hyperplasia (BPH) is a common, and arguably inevitable, disease in elderly men with a prevalence that increases with age affecting approximately 60% of men by the age of 65.1 BPH involves the progressive benign enlargement of the prostate gland secondary to unregulated hyperplastic growth of epithelial and fibromuscular tissues of transition zone and periurethral area resulting in bladder outlet obstruction (BOO).1
Usually, BOO is clinically correlated with lower urinary tract symptoms (LUTS), classically storage (frequency, urgency, nocturia, incontinence) and voiding symptoms (weak stream, retention). First-line therapy typically involves lifestyle modifications and/or medications; however, the recent AUA BPH guidelines supported that early surgical treatment is also an option: Guideline Statement 2 -
Patients should be counselled on options for intervention, which can include behavioral/lifestyle modifications, medical therapy and/or referral for discussion of procedural options (Expert Opinion).2
For many, lifestyle modifications and medical therapy are often not sustainable, desired by the patient, or tolerable, with poor compliance rates. This can prompt urologists to offer procedural intervention.
Surgically, TURP is the most commonly performed procedure and is often referred to as the gold standard.3 However, the risks, limitations due to prostate morphology, and the side effects of TURP have driven industry and urologists to develop alternate procedural options. As age is the most significant contributor to the prevalence and severity of BPH, special attention must be placed on elderly patients who pursue surgical management. Although efficacy remains important, safety becomes a huge driving point in the treatment of elderly patients due to their prevalence of significant comorbidities. With an increase in life expectancy and aging population, understanding the efficacy and safety of available surgical management for BPH in older, at-risk patients is essential. In this literature review, we present an overview of surgical options for BPH and describe considerations for an elderly population.
Materials and Methods
Literature Search
A systematic literature search was conducted using Scopus, PubMed-MEDLINE, Cochrane, and Wiley Online Library databases, to identify literature over the last 10 years up until December 31st, 2022, to focus on recent surgical procedure studies. The following database search words were used either individually or in conjunction: “BPH”, “elderly”, “surgical”, “ablation”, “resection”, “embolization”, and “aging”. Relevant citations from manuscripts populated during the literature search were also considered. Once studies that correlated to those terms were populated, the full text articles were screened to ensure the median/mean age of the patient population was 70 years or compared surgical outcomes of elderly vs young patient population.
Studies were excluded if they (1) were not published in English, (2) were focused on treatment of prostate cancer, (3) did not specify age of patient population, and/or (4) did not focus on surgical outcomes, as indicated by Figure 1.
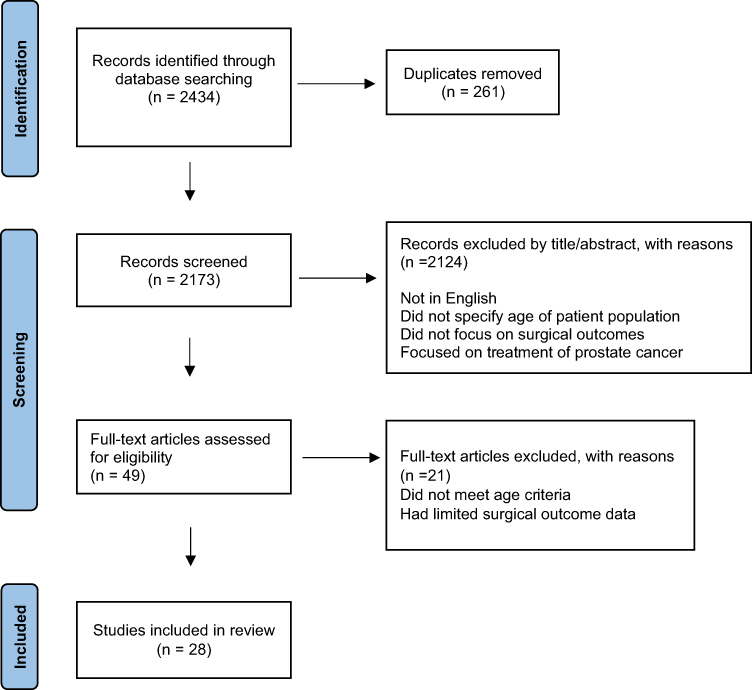 |
Figure 1 Study selection flow diagram. |
Results
Transurethral Resection of the Prostate (TURP) [2 Studies Used]
For patients who have failed medical therapy or have an indication for surgical therapy, TURP continues to be the most commonly performed surgical treatment.2 TURP can be performed with either monopolar or bipolar energy. The use of bipolar energy has addressed some of the complications that were once encountered with monopolar energy, particularly in negating the development of TUR syndrome and its subsequent need to limit operative time, as well as reduce bleeding. Bipolar energy has also pushed the standard admission that often accompanies monopolar TURP. TURP requires spinal or general anesthesia, which carries risks in the elderly population, particularly the elderly and frail. The surgery itself is associated with side effects including retrograde ejaculation, erectile dysfunction, bleeding, and often does require a hospital stay, as shown in Table 1.2 Since these issues are more complex in the elderly population, recent studies have focused on TURP’s safety and efficacy in this patient population, which are reviewed below.
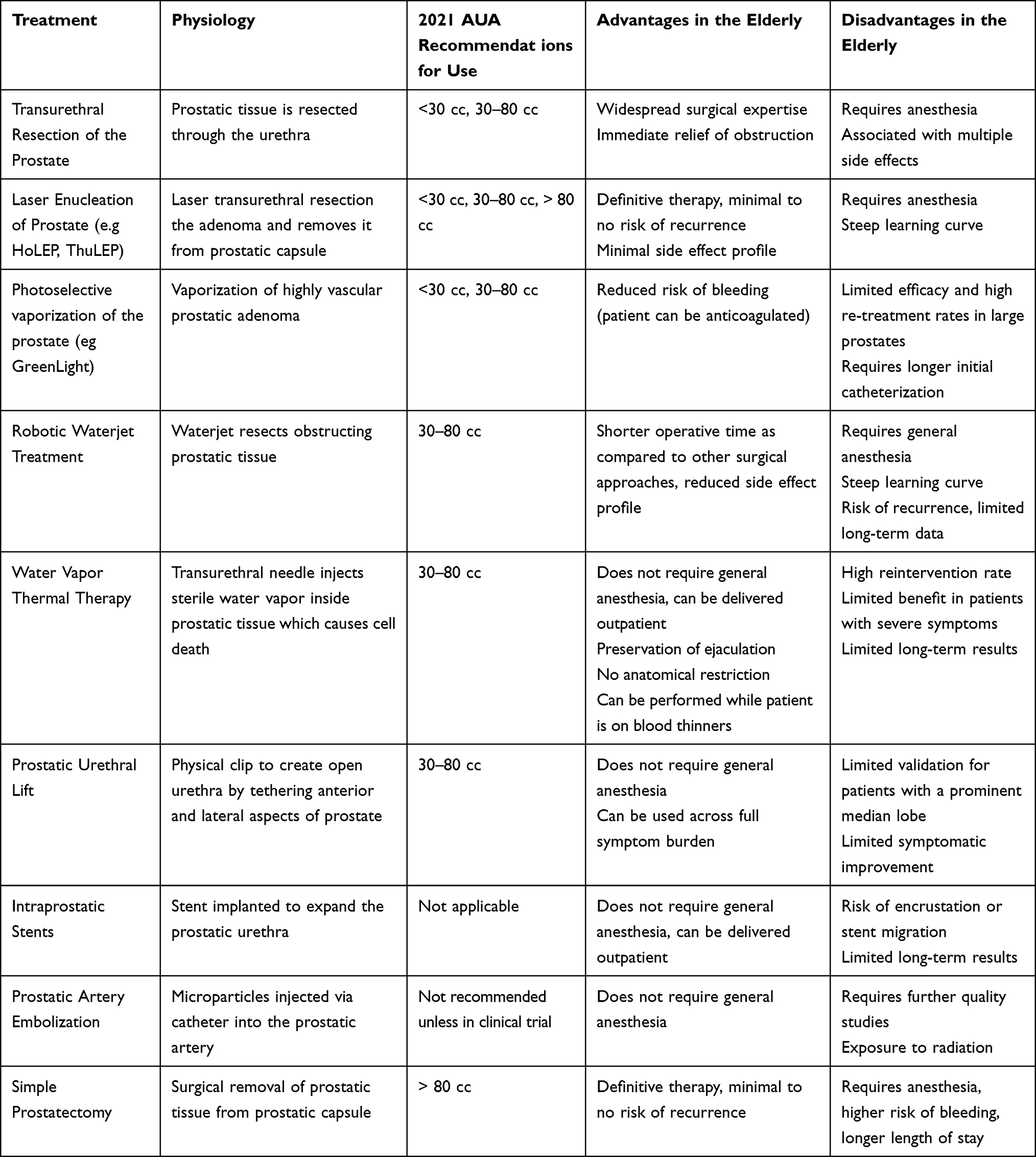 |
Table 1 BPH Surgical Procedures Guidelines and Risks |
A recent multicenter retrospective study aimed to analyze the efficacy of TURP in patients 85 years and older (74% were bipolar, and 26% monopolar).4 In this study, 66.3% of patients had an indwelling catheter pre-operatively due to recurrent urinary retention. Post procedure, 85% of patients were able to spontaneously void, and 85.7% of patients remained catheter free at 12-months. Overall, this study indicated TURP is effective at relieving obstruction with no correlation between age and poor voiding outcomes. They did report an increased transfusion rate with monopolar (16%) over bipolar energy (5%) with a total transfusion rate of 8%. Major complications were low at 3%, with only one death out of 168 patients. This study supports that when TURP is used, bipolar energy is likely safer, especially in older patients at risk for bleeding.
An open-label prospective study by Yang et al further investigated TURP in elderly patients considered high surgical risk, by comparing the effects of bipolar TURP (B-TURP) and monopolar TURP (M-TURP).5 Patients were aged 75 and older with at least one comorbidity. Both B-TURP and M-TURP had similar improvements in IPSS, QoL, Qmax, and PVR one year postoperatively. Similar to the prior study, the authors also concluded that both surgical options are successful in relieving obstruction and addressing symptoms, but bipolar is recommended as superior due to more favorable perioperative factors such as bleeding, irrigation time, Transurethral Resection (TUR) syndrome, length of stay, indwelling catheter time, and overall less adverse effects.
Laser Enucleation (ThuLEP and HoLEP)
The most recent AUA guidelines recommend laser enucleation and photo-selective vaporization of the prostate (PVP) in medically complicated patients with high risk of bleeding.2 Given that elderly patients are often at risk for bleeding secondary to medications and medical comorbidities, laser procedures are attractive procedures in this patient group. Multiple laser modalities have been utilized to perform endoscopic laser enucleation, but the most studied include holmium, and thulium wavelengths.
HoLEP [5 Studies Used]
Holmium laser enucleation of the prostate (HoLEP) is a transurethral technique where obstructing prostatic tissue is resected directly along the prostatic capsule. One of the most rigorously studied and reported procedures, multiple publications have shown similar IPSS improvement, post-void residual, and Qmax after HoLEP between elderly men over the age of 70 as compared to younger patients.6–9
In an age stratified retrospective study by Mmeje et al, the safety and efficacy of HoLEP was assessed in 311 men.6 Across all age groups, rates of morbidity and complication were similar and by the 12 month follow up, all patients showed improvement in IPSS and Qmax, with no significant difference to age. Additionally, intraoperative complication rates were low at 2.2% across 3 of 4 groups, as shown in Table 2. They concluded that age does not impact the safety and efficacy of HoLEP and can be used to treat octogenarians.
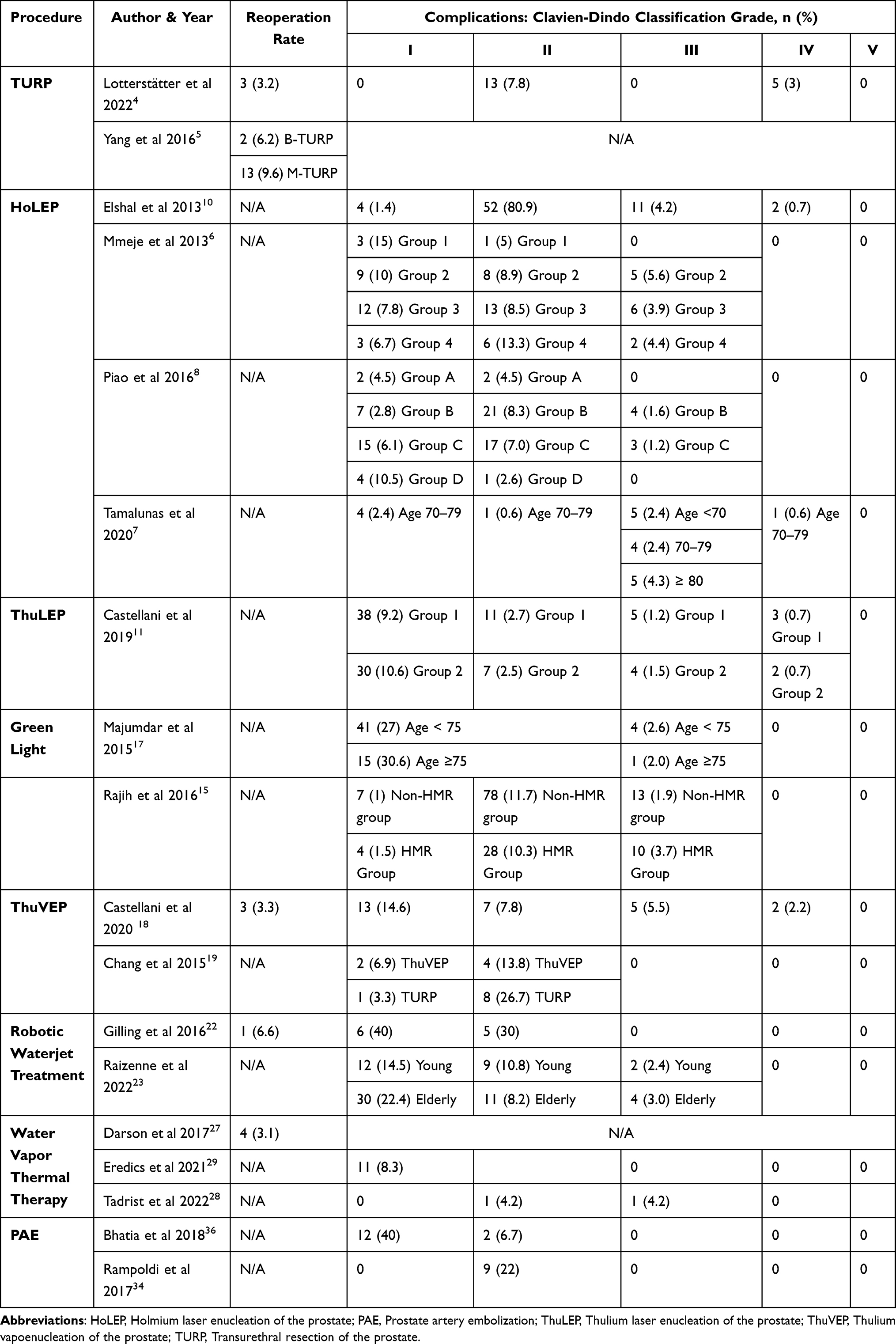 |
Table 2 Studies That Contained Reoperation Rates and Complications According to Clavien-Dindo Classification of Patients |
In a retrospective study of 487 men separated by age, Tamalunas et al evaluated the impact of age on HoLEP outcomes.7 The oldest cohort had a median age of 82 (range 80–85), with 65.2% of patients having an ASA score ≥3. There was no difference in mean operative time, the rate of adverse events, or complication type among patients. All groups experienced improvement in IPSS, QoL, Qmax, and PVR after 4 weeks post-procedure. They determined that HoLEP is safe and effective, regardless of age.
In 2016, Piao et al assessed the impact of age on the safety and efficacy of HoLEP in an age-stratified prospective study of 579 men.8 Octogenarians had higher rates of anticoagulants use, retention, and ASA scores ≥3. Despite this, when compared to the younger cohorts, no difference in complication types and rates were observed. At the 6 month follow up, there was no statistically significant difference in improvement across IPSS, QoL, Qmax, and PVR across all cohorts. They concluded that HoLEP is safe and effective amongst octogenarians.
Gild et al performed a retrospective analysis of 1816 men with a median age of 71, range 66–76, with a focus on peri-operative outcomes.9 Perioperative transfusions occurred in 2.4% of all patients and postoperative complications with a Clavien-Dindo grade of ≥ III, occurred in 3.3% of all patients. In patients undergoing HoLEP, this study showed no differences in the rate of blood transfusions or complications due to age.
A 2013 retrospective review by Elshal et al assessed the peri-operative outcomes and morbidity of 264 octogenarians who underwent various Holmium laser procedures.10 One hundred and seventy-one men were treated using HoLEP with a mean age of 83.9. Their baseline characteristics included 38.5% on anticoagulation therapy, 52% in urinary retention, and 60.8% with an ASA score ≥3. In the 30 days post-procedure, 138 experienced no complications. At 1 year follow up they found improvement in IPSS, QoL, Qmax, PVR with average scores of 4.7, 1.2, 18 mL/s, and 39 mL, respectively. While the patients did well from a voiding perspective post procedure, 18% had ≥ Clavien-Dindo grade III complications. This underscores the potential operative risk in the older patient population.
Despite the identified risks in older patients, HoLEP has arguably undergone the most rigorous validation and secondary analysis for applicability in this patient population. Given its advantages in comorbid patients and success in reducing some risks, such as bleeding, it should be considered first line was offered as an option. If HoLEP is not available, consider referral to a center with the capability to perform the procedure in high-risk patients.
ThuLEP [2 Studies Used]
In a retrospective study, Castellani et al found that the difference in complication or re-treatment rates in older and younger patients, in age-adjusted comparisons, was due to baseline rates of urinary retention and disease burden, rather than a consequence of the intervention.11 In a balanced group of patients undergoing ThuLEP, the outcomes were compared using a propensity score matching in the elderly versus younger men with an age cut-off of 75. After ThuLEP, the length of hospital stays, indwelling catheterization time, and complication types were comparable amongst both groups. Both cohorts showed improvement and by the 12 month follow up, there was no statistical difference in the change of IPSS, QoL, and Qmax, between both groups.
In a single center study by Hou et al, the outcomes of two groups of men who underwent either ThuLEP or B-TURP were compared.12 Both groups had nearly identical baseline characteristics including age, comorbidities, functional outcome scores, and use of BPH medication. The B-TURP group consisted of 141 men, mean age 68, and the ThuLEP group consisted of 135 men, mean age 70. Neither group required blood transfusions during or after their procedures. Post procedure there were no statistically significant differences in the length of hospital stay, rate of re-catheterization, rate of complication, or complication type. At the 2 week and 3-month visits, ThuLEP patients showed a higher improvement of outcomes in a shorter duration than B-TURP patients. By the 6 month follow up, both procedures were equally effective, as indicated by IPSS, QoL, and Qmax. However, ThuLEP patients had better post-operative pain scores and only 5.2% of patients required narcotic pain relief, as opposed 30.6% of TURP patients. This study concludes that both ThuLEP and B-TURP and effective treatments of BPH, however those undergoing ThuLEP experience less post-operative pain.
Vaporization (Greenlight and ThuVEP)
In photo-selective vaporization of the prostate (PVP), laser energy is applied to and absorbed by highly vascular prostatic tissue, resulting in tissue damage. The AUA BPH Guidelines suggest the use of PVP in medically complex patients, particularly those at risk for bleeding.6 Bouhadana et al looked specifically at multi-morbid and elderly individuals aged ≥75. They compared PVP to TURP and found that laser vaporization procedures have lower rates of both long-term and short-term complications, however the reoperation rate was higher.13 This is consistent with other studies comparing TURP to laser vaporization.14
Greenlight Photovaporization of the Prostate (PVP) [3 Studies Used]
In a study by Rajih et al, a multi-center retrospective analysis was performed comparing PVP 180W system outcomes of patients classified as high medical risk (HMR) versus those who were low risk.15 HMR was determined if patient had an ASA score ≥3. The HMR cohort consisted of 273 men with a mean age of 72.3, and the non-HMR cohort consisted of 668 men with a mean age of 67.1. HMR patients had a higher use of anticoagulants and increased prevalence of one or more comorbidities. Despite the HMR cohort having a higher operative and laser time (secondary to larger prostate size), there were no differences in adverse events or complication rates between the two groups. By the 6 months follow up, both groups experienced significant improvement from baseline assessment across IPSS, QoL, Qmax, and PVR. They concluded that in high-risk patients, Greenlight was safe and provided symptom alleviation similar to patients not deemed HMR.
Another multi-center study assessed Greenlight outcomes in HMR patients with an ASA score ≥3 versus those who were low risk.16 The HMR cohort consisted of 626 men with a mean age of 75.9, and the non-HMR cohort consisted of 1514 men with a mean age of 68. HMR patients tended to be older, required anticoagulant therapy, and had smaller prostates (in contrast to the prior study with larger prostates in the HMR group). Perioperatively, 2.6% of HMR patients required transfusions as opposed to 0.14% of non-HMR patients. However, both groups experienced similar rates of hematuria (non-HMR patients 10.5% and HMR patients 12.7%). During the 12-month visit, both groups experienced improvement in IPSS, QoL, PVR and Qmax. This study also indicates that Greenlight is an effective treatment in high-risk patients.
In 2014, Majumdar et al compared the use Greenlight in an age-stratified prospective study of 202 men.17 The elderly cohort consisted of 49 men aged ≥75 who had a higher prevalence of anticoagulants use, urinary retention, and comorbidities, such as heart disease. Despite this, when compared to the younger cohort of 153 men <75 years old, there was no statistical difference in rates of serious complications or need for blood transfusion. Additionally, by the 9-month visit, there was no significant difference in IPSS and QoL scores between both groups. They concluded that Greenlight is safe and just as effective for the elderly.
ThuVEP [3 Studies Used]
A retrospective single-center study by Castellani et al assessed the safety and efficacy of ThuVEP in 88 men, mean age 74.7 with high cardiovascular risk and taking continuous antithrombotic therapy.18 69.3% of the patients had an ASA score ≥3. Postoperative complications occurred in 26.1% of patients, with later complications occurring in 3.8% of patients. The majority of complications were minor, but 2 patients suffered cardiac events, 4 required continuous bladder irrigation, 2 received blood transfusions, and one was brought back to the OR for control of bleeding. Compared to baseline, they found significant improvement across IPSS, QoL, and Qmax by the 12 month follow up. They concluded that ThuLEP resulted in improvement of symptoms and while not without risk, was relatively safe in patients at risk of bleeding.
In a prospective study, Chang et al compared the use of ThuVEP versus TURP in patients >70 years.19 Most baseline characteristics of both groups were similar; however, the ThuVEP group consisted of 29 men with a mean age of 76.1 while the TURP group consisted of 30 men with a mean age of 72.6. Post-operatively, the ThuVEP group experienced a shorter catheterization time and hospital stay. Additionally, patients who underwent ThuVEP had a lower complication rate of 20.7% compared to 30% of TURP patients. Compared to baseline, they found significant improvement across IPSS, QoL, and Qmax by the 12 month follow up, with no difference between the two cohorts. They concluded that in elderly patients, ThuVEP was better tolerated than TURP and had similar efficacy.
Becker et al assessed the durability of ThuVEP in a prospective study of 90 patients with a median age of 71 (IQR 66–75.25) and prostates ≥85 mL.20 They found significant improvement across IPSS, QoL, PVR, and Qmax by the 12 month follow up, when compared to baseline. Though only data from 29 patients were available at the 2-year visit, these patients continued to experience improvement in urinary outcomes with only 1 patient requiring reoperation. This study shows ThuVEP is an effective means of treatment for elderly patients with large prostates.
Robotic Waterjet Treatment [2 Studies Used]
Robotic Waterjet Treatment is a transurethral procedure that uses targeted high velocity saline to resect tissue.21 While this procedure still requires anesthesia, it is shorter than traditional transurethral prostate procedures, can treat large glands quickly, and can preserve ejaculatory function.
Though not specifically focused on the elderly, an initial single-center trial of robotic waterjet treatment with a mean age of 73 years, studied the procedure’s safety and outcomes.22 Most notably, no patients required blood transfusions. Despite the occurrence of postoperative complications in 53.3% of patients, the complications were minor, with 5 patients in urinary retention requiring re-catheterization, 3 with hematuria, and 3 with dysuria. All patients experiencing hematuria and dysuria did not require medical intervention. From the baseline to six month follow up, there were significant improvements across IPSS, QoL, Qmax, and PVR. Due to a shorter resection time, time spent under general anesthesia was reduced, making this procedure attractive for those patients where anesthesia time should be limited.
A recent retrospective analysis by Raizenne et al studied outcomes after robotic waterjet treatment between men ≥65 (defined as “elderly”) and men less than 65 years of age (“young”).23 In both groups, post-operative catheterization and lengths of stay were similar. There was no statistical difference in adverse events. Additionally, there was a similar reduction of IPSS scores, Qmax, ejaculatory dysfunction, and annual re-treatment rates between both groups. The authors also extend that robotic waterjet treatment offers higher IPSS improvement rates when compared to non-ablative office-based surgical procedures, such as Water Vapor Thermal Therapy and PUL. This study showed that age does not impact outcome.
Water Vapor Thermal Therapy (WVTT) [5 Studies Used]
This minimally invasive method uses sterile water vapor injected directly into the prostate to destroy prostatic adenoma.3 There are multiple advantages with water vapor thermal therapy including short procedural time, reduced hospital stay, and patients can safely maintain their anticoagulant or antiplatelet therapy prior to treatment, which is significant in the elderly population.24 However, there is limited long-term data and the procedure is not well suited for those with severe symptom burden.
In a retrospective chart review, McVary et al assessed 38 men with a mean age of 76 who were catheter dependent.25 Water vapor thermal therapy proved effective as 70.3% were ultimately able to void spontaneously. Mild adverse events were reported and occurred in only 13% of patients, supporting that this is a safe procedure, as well.
In a retrospective review, Bassily et al assessed the efficacy of water vapor thermal therapy in a study of 49 men, median age 73 (IQR 65–82) who were catheter dependent.26 Procedures were done under monitored anesthesia care (59%) or general anesthesia (41%). Post procedure, 27% of patients experienced minor adverse events including continued urinary retention, UTI, and penoscrotal edema. They found statistical improvement across IPSS, QoL, and PVR. Most notably, PVR was reduced from 900 mL to 78 mL and 87.8% of patients no longer experienced retention following water vapor thermal therapy.
In a multicenter retrospective analysis by Darson et al, 131 men, mean age 70.9 who were catheter dependent, showed significant improvement across functional outcomes after being treated with water vapor thermal therapy.27 Patients were treated under various methods of anesthesia including IV sedation (86%), general anesthesia (41%), or prostatic block (6%). No transfusions were noted and only minor adverse events occurred. By the 12 month follow up, IPSS, QoL, and PVR improved by 45.2%, 37.8%, and 34.9%, respectively. Additionally, there was no reported impact on sexual function.
In a small, single-center study consisting of 24 men with a median age of 77 (IQR 67–86), who were considered frail and catheter dependent, the efficacy of water vapor thermal therapy was assessed.28 After 1-year post-op, all patients maintained spontaneous voiding and did not require surgical retreatment. Only two adverse events occurred: one bleeding event that was treated with PAE; and another patient treated for prostatitis.
Eredics et al retrospectively analyzed 136 men with a mean age of 80.3 who were multimorbid, experiencing urinary retention, and considered unfit for surgery.29 After water vapor thermal therapy (performed under local anesthesia with a periprostatic block), 78.6% of patients were able to void spontaneously and by 12 months post-op, 90% of all patients remained catheter free. Additionally, only 11 patients experienced minor complications that were easily resolved. They concluded that water vapor thermal therapy was safe and effective in treating patients suffering from urinary retention who may not be surgical candidates.
Prostatic Urethral Lift (PUL) [1 Study Used]
A Prostatic Urethral Lift (PUL) is performed by inserting implants from the anterior and lateral aspects of the prostate, to extend the anterior prostatic urethral channel. PUL can be done without general anesthesia and has been shown to preserve sexual function.2,30 According to the AUA guidelines, PUL is recommended in patients with a prostate volume of less than 80 cc and absence of a median lobe.2
Lehner et al performed a retrospective review of high-risk patients with a mean age of 70 and average ASA score ≥3, who underwent PUL.31 Patients were treated under various methods of anesthesia including general anesthesia (58.2%%), IV sedation and localized lidocaine (38.5%), or spinal block (3.3%). Post operative adverse events included hematuria (not requiring re-operation), dysuria, pelvic pain, UTI, and acute retention. Prior to procedure, 44 (48%) of patients were in complete urinary retention, with that number dropping to 17 (18%). There was significant improvement in IPSS, SHIM, PVR, and Qmax of 42.9%, 12.3%, 43.5%, and 34.4%, respectively. Over the 4.5 year follow up, the surgical retreatment rate was 11%, averaging a 2.4% retreatment rate per year. This study found that PUL was an acceptable treatment for patients with high surgical risk, severe LUTS, and multiple comorbidities. Further research on PUL in elderly patients is required.
Prostatic Stents
Intraprostatic stents have long been used as a treatment for relieving BOO secondary to BPH by expanding the prostatic urethra.32 Since minimal anesthesia is required, stents are an alternative for patients that have a high anesthetic risk or are unfit for surgery. However, there is a risk of stent migration and/or encrustation. Currently, there are no guidelines for the use of intraprostatic stents in treating patients with BPH. However, stents remain an attractive option for patients, particularly those who are elderly and/or frail. Ideally, stents could be deployed in an office setting and would relieve obstruction sufficiently enough to improve symptoms and reduce risk for retention. There are several stents currently in trials and it is anticipated that at least 3 will be marketed in the near future.
Prostatic Artery Embolization (PAE) [4 Studies Used]
Prostatic artery embolization (PAE) is a minimally invasive technique that is performed via catheter through either the femoral or radial artery and does not require general anesthesia. Microparticles are injected into the blood vessel to reduce blood supply to the prostate, thus reducing its size over time.2 There have been multiple studies assessing the efficacy and safety of PAE in elderly patients.
A recent prospective single-center study by Wang et al compared the use of PAE to treat BPH in men ≥75 defined as “elderly” and men less than 75 years of age.33 At baseline, differences were noticed between the two groups in PVR, Qmax, and IIEF-5 scores. During PAE, there were no differences in technical success rates, despite the elderly cohort having a longer procedure time. There were no complications ≥ Clavien-Dindo grade II, and both groups experienced only minor adverse events. Post-procedural follow up showed that both groups had similar improvement in IPSS, QoL, Qmax, and PVR, and that there was no statistically significant difference in rate of clinical success (90.4% elderly versus 95.2% young). Most notably, the elderly cohort had a larger reduction of prostate volume than the young group.
A 2017 prospective study assessed the use of PAE in patients who were not fit for surgery due to significant comorbidities and required an indwelling bladder catheterization.34 The cohort had a mean age of 77.9, one or more comorbidities, and required catheterization for at least a month. Post procedure 9 patients (22%) had Clavien-Dindo grade II complications including acute retention requiring temporary catheterization and urinary tract infections. Additionally, 9 patients (22%) experienced mild to moderate post-embolization syndrome. After PAE, 80.5% of patients had their catheter removed, experienced a reduction in prostate size, and showed improvement in IPSS and QoL.
Gabr et al focused on PAE in high-risk patients in a prospective study of 22 men with a mean age 72.5 who presented with urinary retention.35 No peri- or post operative complications were noted, and patients showed improvement of 48.61%, 31.19%, and 97.77% in IPSS, QoL, and Qmax, respectively. They concluded PAE was safe and did not include complications such as urethral stricture, need for blood transfusion, or Transurethral Resection (TUR) syndrome that can occur in TURP.
In a retrospective single-center review by Bhatia et al, of 30 men with a mean age of 73.1 (range 48 −94) with large prostates and in urinary retention underwent PAE.36 Despite the occurrence of postoperative complications in 47% of patients, only 6.7% were classified as Clavien-Dindo grade II, with the majority being grade I. They found 86.7% men were able to void independently by 3 months post-procedure and had a decrease in prostate average volume from 167.3 at baseline to 94.1 by the 12-month visit. Additionally, when compared to baseline values, significant improvement in IPSS and QoL was observed. They concluded that PAE is an effective treatment for patients with urinary retention and large prostates.
These studies support the use of PAE in patients with significant comorbidities, presenting with urinary retention, and large prostates. At this time, the AUA does not support the use of PAE as a means of treating BPH as further studies must be performed to weigh the benefits and risks.2
Simple Prostatectomy [1 Study Used]
Simple prostatectomy involves removal of the complete prostatic tissue within the prostatic capsule. While open simple prostatectomy provides definitive treatment for BPH, there is a higher rate of perioperative complications compared to TURP.27 At this time, the AUA recommends the use of simple prostatectomy for BPH in patients with very large prostates.2
In an analysis of the National Inpatient Sample, Pariser et al focused on the outcomes and risk of simple prostatectomy to treat BPH in a study of 35,171 men, median age 72 (IQR 66–77), from 2002 through 2012.37 Simple prostatectomy was associated with a 28% complication rate, with bleeding being the most prevalent. During the study period, use of simple prostatectomy steadily decreased, associated with the introduction of novel minimally invasive procedures. Additionally, patients who were ≥75 years of age or had at least one comorbidity were independently associated with an increased risk of complication after simple prostatectomy.
Discussion
As one of the first surgical treatments for BPH, TURP has been extensively studied for its safety and efficacy throughout the years, with most urologists having an extensive clinical experience with this therapy.2,3 Multiple studies have shown that bipolar TURP has superior perioperative outcomes compared to monopolar TURP; however, both surgical options carry the risk of retrograde ejaculation, and erectile dysfunction.2 More so, the use of spinal or general anesthesia to perform this procedure carries greater risk in the elderly population. In addition, this procedure cannot be performed while on active anticoagulant therapy which has led to the search for safer alternatives to TURP.
There are a wide variety of surgical procedures available for treating BPH in elderly men with varying states of health, as shown in Table 1 and Table 2. Each of these comes with different risks and benefits, supporting that individualized approaches are essential in surgical management. For patients at a greater anesthesia risk, water vapor thermal therapy is a minimally invasive option that can be performed in an office setting using local anesthesia.2,3,19,26–30The prostatic urethral lift can preserve sexual function and can also be performed in-office, though limitations include prostate size and may be challenging with a middle lobe.2,31 For medically complex patients with higher bleeding risk, the AUA suggests the use of procedures such as HoLEP, ThuLEP, Greenlight, and ThuVEP, as they have shown promising improvement in functional urinary outcomes in the elderly and avoid the morbidity of simple prostatectomy.2,6–16,20,22,24,2523 Robotic waterjet treatment has been shown to preserve ejaculatory function and while it requires the use of general anesthesia, it has a shorter operative time compared to other traditional transurethral procedures which makes it preferable for patients with a high anesthesia risk.218,19,21 PAE is a minimally invasive procedure that has undergone multiple clinical trials with promising results in terms of efficacy and safety in elderly men.2,16,36,37
While improvement in BPH symptoms is the main priority, there are a multitude of factors and lifestyle choices that patients consider when deciding upon surgical intervention. Multiple studies have shown that the preservation of sexual function is just as important to the elderly as it is in younger patients. In a study by Helgason et al, they identified that the preservation of sexual function is important even in men older than 70.38
This literature review is limited by the small number of studies available focusing on surgical interventions in patients older than 70. Furthermore, new studies may have been published outside the timeframe of the review. The strengths of this comprehensive literature review include 28 papers and included data from 2012 to 2022. The studies were selected to include the appropriate population and are applicable to the elderly population.
Conclusion
With the wide array of surgical treatments for BPH available, understanding the efficacy and safety profiles of each procedure is essential in older, at-risk patients. Novel technologies and new minimally invasive approaches are available to urologists, with even more coming down the pike. These approaches, combined with careful patient selection, may offer similar symptomatic improvement with a reduced risk profile. Long-term data and further studies to determine which approaches are preferred in the elderly population will help to streamline surgical management. Shared decision-making and individualized approaches based on risk and patient characteristics are necessary prior to determining the appropriate treatment option.
Disclosure
Bilal Chughtai is a consultant for Olympus, Boston Scientific, Ferring Pharmaceuticals, and Allergan. Dean Elterman reports grants, personal fees from Boston Scientific, grants from Olympus, grants from Urotronic, grants from Procept Biorobotics, grants from Zenflow, outside the submitted work. Kevin C. Zorn is a consultant and proctor for Boston Scientific, Procept BioRobotics, and investigator for Zenflow. Naeem Bhojani is a consultant for Olympus, Boston Scientific, and Procept BioRobotics. Lori Lerner reports Uncompensated - Chair of the Clinical Events Committee (CEC) from Proverum, outside the submitted work. The authors declare that they have no other known competing interests.
References
1. Bushman W. Etiology, epidemiology, and natural history. Urol Clin North Am. 2009;36(4):403–415. doi:10.1016/j.ucl.2009.07.003
2. Lerner LB, McVary KT, Barry MJ, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA GUIDELINE PART II—surgical evaluation and treatment. J Urol. 2021;206(4):818–826. doi:10.1097/ju.0000000000002184
3. Bortnick E, Brown C, Simma-Chiang V, Kaplan SA. Modern best practice in the management of benign prostatic hyperplasia in the elderly. Ther Adv Urol. 2020;12. doi:10.1177/1756287220929486
4. Lotterstätter M, Seklehner S, Wimpissinger F, et al. Transurethral resection of the prostate in 85+ patients: a retrospective, multicentre study. World J Urol. 2022;40(12):3015–3020. doi:10.1007/s00345-022-04179-w
5. Yang EJ, Li H, Sun XB, et al. Bipolar versus monopolar transurethral resection of the prostate for benign prostatic hyperplasia: safe in patients with high surgical risk. Sci Rep. 2016;6(1). doi:10.1038/srep21494
6. Mmeje CO, Nunez-Nateras R, Warner JN, Humphreys MR. Age-stratified outcomes of holmium laser enucleation of the prostate. BJU Int. 2013;35(5). doi:10.1111/bju.12063
7. Tamalunas A, Westhofen T, Schott M, et al. The clinical value of holmium laser enucleation of the prostate in octogenarians. LUTS. 2020;13(2):279–285. doi:10.1111/luts.12366
8. Piao S, Choo MS, Kim M, Jeon HJ, Oh SJ. Holmium laser enucleation of the prostate is safe for patients above 80 years: a prospective study. Int Neurourol J. 2016;20(2):143–150. doi:10.5213/inj.1630478.239
9. Gild P, Lenke L, Pompe RS, et al. Assessing the outcome of holmium laser enucleation of the prostate by age, prostate volume, and a history of blood thinning agents: report from a single-center series of >1800 consecutive cases. J Endourol. 2021;35(5):639–646. doi:10.1089/end.2020.0605
10. Elshal AM, Elmansy HM, Elhilali MM. Transurethral laser surgery for benign prostate hyperplasia in octogenarians: safety and outcomes. Urology. 2013;81(3):634–639. doi:10.1016/j.urology.2012.11.042
11. Castellani D, Pirola GM, Gasparri L, et al. Are outcomes of thulium laser enucleation of the prostate different in men aged 75 and over? A propensity score analysis. Urology. 2019;132:170–176. doi:10.1016/j.urology.2019.06.025
12. Hou CP, Lin YH, Juang HH, et al. Clinical outcome of transurethral enucleation of the prostate using the 120-W thulium Laser (VelaTM XL) compared to bipolar transurethral resection of the prostate (TURP) in aging male. Aging. 2020;12(2):1888–1898. doi:10.18632/aging.102720
13. Bouhadana D, Nguyen DD, Zhang X, et al. Safety and efficacy of TURP vs. laser prostatectomy for the treatment of benign prostatic hyperplasia in multi-morbid and elderly individuals aged ≥ 75. World J Urol. 2021;39(12):4405–4412. doi:10.1007/s00345-021-03779-2
14. Stoddard MD, Zheng X, Mao J, Te A, Sedrakyan A, Chughtai B. Safety and efficacy of outpatient surgical procedures for the treatment of benign prostatic enlargement in New York state and California (2005–2016). J Urol. 2021;205(3):848–854. doi:10.1097/ju.0000000000001401
15. Rajih E, Tholomier C, Hueber PA, et al. Evaluation of surgical outcomes with photoselective greenLight XPS laser vaporization of the prostate in high medical risk men with benign prostatic enlargement: a multicenter study. J Endourol. 2017;31(7):686–693. doi:10.1089/end.2016.0782
16. Nguyen DD, Deyirmendjian C, Law K, et al. GreenLight photovaporization of the prostate in high-medical-risk patients: an analysis of the Global GreenLight Group (GGG) database. World J Urol. 2022;40(7):1755–1762. doi:10.1007/s00345-022-03986-5
17. Majumdar R, Mirheydar HS, Palazzi KL, Lakin CM, Albo ME, Parsons JK. Prostate laser vaporization is safe and effective in elderly men. Urol Ann. 2015;7(1):36. doi:10.4103/0974-7796.148595
18. Castellani D, Di Rosa M, Gasparri L, Pucci M, Dellabella M. Thulium laser vapoenucleation of the prostate (ThuVEP) in men at high cardiovascular risk and on antithrombotic therapy: a single-center experience. J Clin Med. 2020;9(4):917. doi:10.3390/jcm9040917
19. Chang CH, Lin TP, Chang YH, Huang WJ, Lin AT, Chen KK. Vapoenucleation of the prostate using a high-power thulium laser: a one-year follow-up study. BMC Urol. 2015;15(1). doi:10.1186/s12894-015-0032-7
20. Becker B, Orywal AK, Gross AJ, Netsch C. Thulium vapoenucleation of the prostate (ThuVEP) for prostates larger than 85 mL: long-term durability of the procedure. Lasers Med Sci. 2019;34(8):1637–1643. doi:10.1007/s10103-019-02760-1
21. Taktak S, Jones P, Haq A, Rai BP, Somani BK. Aquablation: a novel and minimally invasive surgery for benign prostate enlargement. Ther Adv Urol. 2018;10(6):183–188. doi:10.1177/1756287218760518
22. Gilling P, Reuther R, Kahokehr A, Fraundorfer M. Aquablation - image-guided robot-assisted waterjet ablation of the prostate: initial clinical experience. BJU Int. 2016;117(6):923–929. doi:10.1111/bju.13358
23. Raizenne BL, Bouhadana D, Zorn KC, et al. Functional and surgical outcomes of Aquablation in elderly men. World J Urol. 2022;40(10):2515–2520. doi:10.1007/s00345-022-04137-6
24. Cantrill CH, Zorn KC, Elterman DS, Gonzalez RR. The Rezūm system - A minimally invasive water vapor thermal therapy for obstructive benign prostatic hyperplasia. Can J Urol. 2019;26(3):9787–9793.
25. McVary KT, Holland B, Beahrs JR. Water vapor thermal therapy to alleviate catheter-dependent urinary retention secondary to benign prostatic hyperplasia. Prostate Cancer Prostatic Dis. 2019;23:303–308. doi:10.1038/s41391-019-0187-5
26. Bassily D, Wong V, Phillips JL, et al. Rezūm for retention—retrospective review of water vaporization therapy in the management of urinary retention in men with benign prostatic hyperplasia. Prostate. 2021;81(14):1049–1054. doi:10.1002/pros.24201
27. Darson MF, Alexander EE, Schiffman ZJ, et al. Procedural techniques and multicenter postmarket experience using minimally invasive convective radiofrequency thermal therapy with Rezūm system for treatment of lower urinary tract symptoms due to benign prostatic hyperplasia. Res Rep Urol. 2017;9:159–168. doi:10.2147/rru.s143679
28. Tadrist A, Baboudjian M, Bah MB, et al. Water vapor thermal therapy for indwelling urinary catheter removal in frail patients. Int Urol Nephrol. 2022;55:249–253. doi:10.1007/s11255-022-03408-w
29. Eredics K, Wehrberger C, Henning A, et al. Rezūm water vapor therapy in multimorbid patients with urinary retention and catheter dependency. Prostate Cancer Prostatic Dis. 2021;25(2):302–305. doi:10.1038/s41391-021-00462-w
30. Garcia C, Chin P, Rashid P, Woo HH. Prostatic urethral lift: a minimally invasive treatment for benign prostatic hyperplasia. Prost Inter. 2015;3(1):1–5. doi:10.1016/j.prnil.2015.02.002
31. Lehner K, Popat S, Utech K, Taylor J, Brooks M and Jones J. Outcomes of prostatic urethral lift in a medically complex population at a veterans affairs hospital. BJUI Compass, (2022). 3(3), 214–219. 10.1002/bco2.126
32. Papatsoris A, Zachou, Kachrilas, Masood, Buchholz and Junaid. New developments in the use of prostatic stents. OAJU, (2011). 63 10.2147/OAJU.S11752
33. Wang MQ, Wang Y, Yan JY, et al. Prostatic artery embolization for the treatment of symptomatic benign prostatic hyperplasia in men ≥75 years: a prospective single-center study. World J Urol. 2016;34(9):1275–1283. doi:10.1007/s00345-016-1771-0
34. Rampoldi A, Barbosa F, Secco S, et al. Prostatic artery embolization as an alternative to indwelling bladder catheterization to manage benign prostatic hyperplasia in poor surgical candidates. Cardiovasc Intervent Radiol. 2017;40(4):530–536. doi:10.1007/s00270-017-1582-8
35. Gabr AH, Gabr MF, Elmohamady BN, Ahmed A. Prostatic artery embolization: a promising technique in the treatment of high-risk patients with benign prostatic hyperplasia. Urol Int. 2016;97(3):320–324. doi:10.1159/000447360
36. Bhatia S, Sinha VK, Kava BR, et al. Efficacy of prostatic artery embolization for catheter-dependent patients with large prostate sizes and high comorbidity scores. J Vasc Interv Radiol. 2018;29(1):78–84.e1. doi:10.1016/j.jvir.2017.08.022
37. Pariser JJ, Pearce SM, Patel SG, Bales GT. National trends of simple prostatectomy for benign prostatic hyperplasia with an analysis of risk factors for adverse perioperative outcomes. Urology. 2015;86(4):721–726. doi:10.1016/j.urology.2015.06.04
38. Helgason ÁR, Adolfsson J, Dickman P, et al. Sexual desire, erection, orgasm and ejaculatory functions and their importance to elderly Swedish men: a population-based study. Age Ageing. 1996;25(4):285–291. doi:10.1093/ageing/25.4.285
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treating and Managing Laryngopharyngeal Reflux Disease in the Over 65s: Evidence to Date
Lechien JR
Clinical Interventions in Aging 2022, 17:1625-1633
Published Date: 15 November 2022
How to Effectively Monitor Aging Patients with Chronic Hepatitis B: A Review
Kang CK, Brennan PN, Dillon JF
Clinical Interventions in Aging 2022, 17:1811-1820
Published Date: 9 December 2022