Back to Journals » Cancer Management and Research » Volume 12
Procalcitonin Levels in Post TACE Infection
Authors Han S, Ye Y, Wu J, Li B, Zhang G ![]() , Jin K, Tang R, Huang W, Chao M, Ding K
, Jin K, Tang R, Huang W, Chao M, Ding K
Received 15 September 2020
Accepted for publication 15 November 2020
Published 26 November 2020 Volume 2020:12 Pages 12197—12203
DOI https://doi.org/10.2147/CMAR.S281667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Shugao Han,1 Yao Ye,2 Jianjun Wu,1 Bin Li,1 Guangqiang Zhang,1 Kai Jin,1 Rui Tang,1 Wei Huang,1 Ming Chao,1 Kefeng Ding2
1Department of Radiology, Second Affiliated Hospital of School of Medicine, Zhejiang University, Hangzhou 310009, Zhejiang Province, People’s Republic of China; 2Department of Surgical Oncology, Second Affiliated Hospital of School of Medicine, Zhejiang University, Hangzhou 310009, Zhejiang Province, People’s Republic of China
Correspondence: Kefeng Ding Department of Surgical Oncology
Second Affiliated Hospital, Zhejiang University School of Medicine, Jiefang Road 88, Hangzhou 310009, Zhejiang Province, People’s Republic of China
Tel/Fax +86 57187784820
Email [email protected]
Purpose: This study aimed to evaluate the value of serum procalcitonin (PCT) levels in the diagnosis of abscess and sepsis following transarterial chemoembolization (TACE) therapy among patients with hepatocellular carcinoma (HCC).
Patients and Methods: In this study, a retrospective review of patient charts was performed in 2221 patients who suffered from hepatocellular carcinoma and had undergone 8656 TACE procedures from January 2012 to January 2018. According to the diagnosis of infection and abscess after TACE, these participants were divided into infection group (group A, n=48) and abscess group (group B, n=35). Group B included subgroup B1 (suffered from liver abscess but no sepsis, n=16) and subgroup B2 (suffered from liver abscess and sepsis, n=19). The main observational indexes included sociodemographic characteristics and laboratory and clinical parameters.
Results: The results showed that the mean PCT and C-reactive protein (CRP) levels were higher in group B, but receiver-operating characteristic (ROC) analysis showed low sensitivity and specificity. Only the mean PCT level was higher in subgroup B2 than in subgroup B1 (P< 0.001); the ROC analysis had high sensitivity and specificity. However, all other data such as NEUT (neutrophil count) and NEUTP (neutrophil percentage) showed no significant differences.
Conclusion: Serum PCT level was a promising inexpensive marker for the diagnosis of liver abscess and sepsis following TACE therapy among patients with primary liver cancer. A cutoff level of 5.1 ng/mL for PCT had high sensitivity and specificity in predicting liver abscess with sepsis.
Keywords: hepatocellular carcinoma, abscess, C-reactive protein, procalcitonin, sepsis, transarterial chemoembolization
Introduction
Transarterial chemoembolization (TACE) is one of the most effective treatments for managing primary malignant liver tumors. Many studies have shown that TACE prolongs survival.1,2 Although this treatment modality is a minimally invasive procedure, it can sometimes lead to serious complications. The formation of abscesses after TACE is one of the most serious complications of TACE.3 Previous studies have shown that the incidence of abscess formation after TACE varies between 0.1% and 4.5%.4 Early identification of abscess and sepsis is very important following TACE in patients with primary liver cancer. Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection.5
Biomarkers play a vital role in the early diagnosis of sepsis, predicting sepsis-related complications, including developing multiple-organ dysfunctions, guiding antimicrobial therapy, and assessing the response to therapy and recovery from sepsis.5 Computed Tomography (CT) is very important for the diagnosis of liver abscess, but sometimes it is difficult to detect sepsis. Therefore, this study was conducted to evaluate the value of serum procalcitonin (PCT) levels in the diagnosis of abscess and sepsis following TACE therapy among patients with HCC.
Materials and Methods
Ethics Statement
Patients with primary liver tumors were obtained from the Second Affiliated Hospital of Zhejiang University School of Medicine with written informed consent of each individual and approval by the Research Ethics Board of the Second Affiliated Hospital of Zhejiang University. Data were collected anonymously and the clinical study was carried out in accordance with the Declaration of Helsinki.
Participants
This study was a retrospective trial. From January 2012 to January 2018, patients with HCC who underwent TACE at the Department of Interventional Radiology in Second Affiliated Hospital of School of Medicine were recruited in this study. The medical records of these patients were reviewed and analyzed. Among the 2221 patients, 83 patients with suspected infection symptoms and temperature higher than 38.5°C after TACE were included in the study.
According to the diagnosis of infection and abscess after TACE, these participants were divided into infection group (group A, n=48) and abscess group (group B, n=35). Group B included subgroup B1 (suffered from liver abscess but no sepsis, n=16) and subgroup B2 (suffered from liver abscess and sepsis, n=19). The main observational indexes included sociodemographic characteristics and laboratory and clinical parameters. This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the hospital.
Diagnosis of Abscess and Sepsis
After TACE, the patients were closely observed for TACE related complications. Patients suspected infection symptoms after TACE were included in the study, with temperature higher than 38.5°C.
Liver abscess was diagnosed in CT images showing a peripheral rim contrast enhancement, with or without an air–fluid level abscess, and with hypoattenuation in the treated segment. Moreover, any one of the following conditions was included: Blood or aspirate culture revealed bacteria; aspirate from percutaneous drainage had a purulent appearance; and temperature higher than 38.5°C lasted for more than 5 days with the leukocyte count >12 × 109 per L without other causes.
Sepsis was diagnosed using the standard of the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis 3) as a reference.5
Infection was diagnosed in patients suspected infection symptoms with temperature higher than 38.5°C, but there was no evidence of an abscess and sepsis.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) patients diagnosed with hepatocellular carcinoma (diagnosed in accordance with the recommendations of the American Association for the Study of Liver Diseases) and TACE has been done; (2) suspected infection symptoms after TACE; (3) patients with age more than 18 years; and (4) patients whose data were complete.
The exclusion criteria were as follows: (1) patients who inconsistent with the criteria of HCC or refused to undergo TACE; (2) without suspected infection symptoms after TACE; (3) patients with age under 18 years; (4) patients whose data were incomplete.
Treatment of Abscess and Sepsis
CT-guided percutaneous catheter drainage therapy was carried out in patients who had abscesses; 10 mL of the aspirate was obtained for bacterial culture and antibiogram tests.
When the diagnosis of liver abscess was confirmed, broad-spectrum antibiotics were empirically administered until the results of the antibiogram were collected.
Statistical Analysis
The continuous variables with a normal distribution were expressed as mean ± standard deviation, the continuous variables with a non-normal distribution were expressed as median (interquartile range), and the categorical variables were expressed as frequency [percentage (%)]. Differences between the two groups were assessed using the χ2 test or Fisher exact test for categorical variables, the Student t test for continuous variables with a normal distribution, and the non-parametric rank-sum test for non-normally distributed continuous and ordinal variables. Receiver-Operating Characteristic (ROC) curves were drawn, and diagnostic efficacies were determined by comparing the Areas under the Curves (AUC). Subsequently, optimal cutoff values were selected according to the Youden index. The sensitivity and specificity for differential diagnosis were assessed. A two-tailed P value less than 0.05 was considered statistically significant. SPSS version 25 (SPSS Inc., IL, USA) and the R version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria) were applied to perform all statistical analyses.
Results
General Characteristics
A total of 83 patients with HCC and suspected infection symptoms were included in the study. According to the diagnosis, these participants were divided into infection group (group A, n=48) and abscess group (group B, n=35). Group B included subgroup B1 (suffered from liver abscess but no sepsis, n=16) and subgroup B2 (suffered from liver abscess and sepsis, n=19). The results showed that age, sex, size, extrahepatic metastases, vascular invasion, number of TACE and tumor staging had no significant differences, which are shown in Table 1.
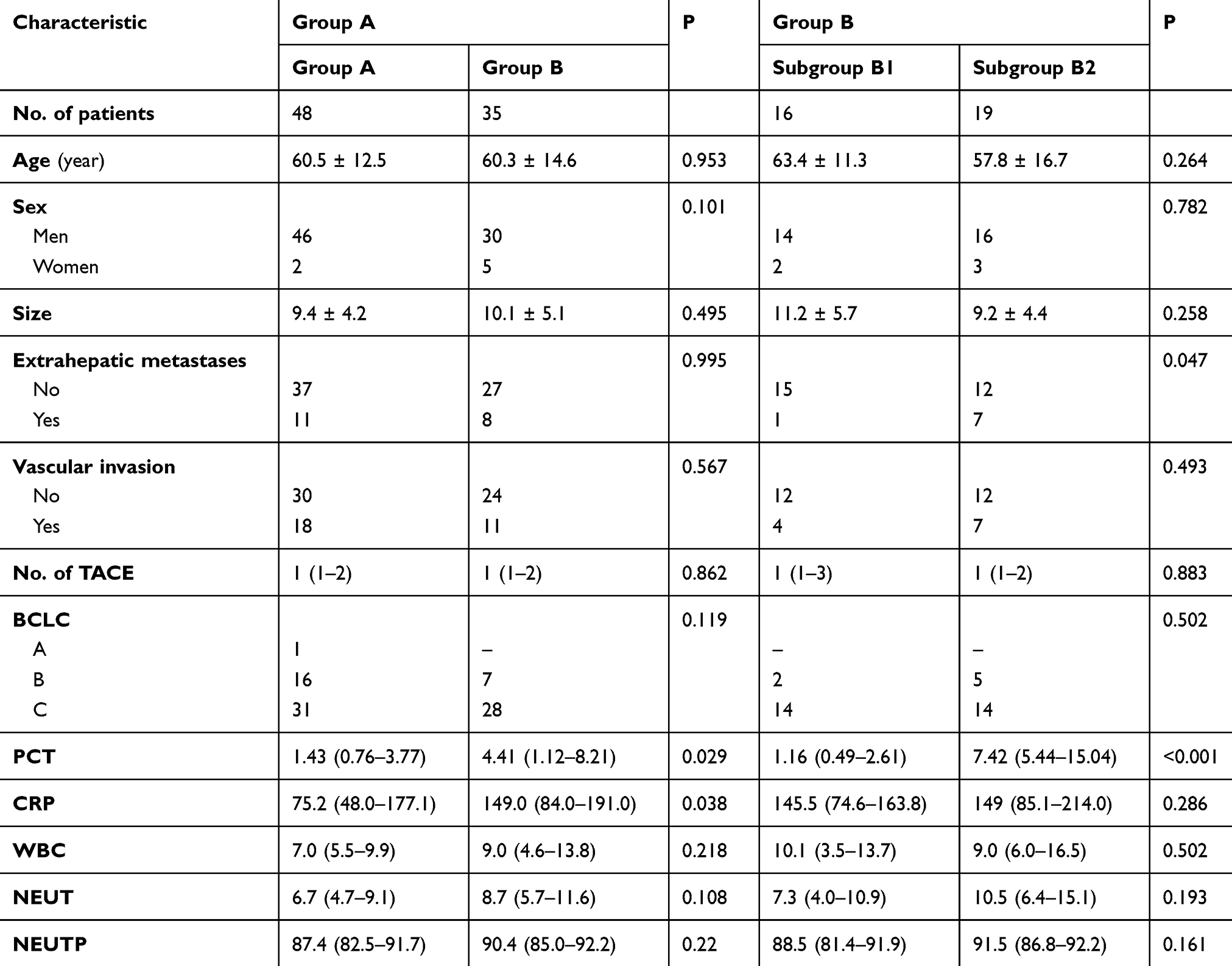 |
Table 1 Characteristics of the Two Groups of Patients (P<0.05) |
Levels of PCT, CRP, NEUT, and NEUTP
PCT (serum procalcitonin) and CRP (C-reactive protein) levels were higher in group B, but the mean NEUT (neutrophil count) and NEUTP (neutrophil percentage) levels showed no significant differences between groups A and B. White Blood Cell (WBC) count and the levels of PCT, CRP, NEUT, and NEUTP showed low sensitivity and specificity to identify groups A and B (Figure 1).
 |
Figure 1 Diagnostic efficacies of abscess formation were determined by comparing the areas under the curves (AUC). |
Only the mean PCT level was higher in subgroup B2 than in subgroup B1 (P<0.001), and the ROC analysis had high sensitivity and specificity. However, all other data, such as WBC count and the levels of CRP, NEUT, and NEUTP, showed no significant differences and low sensitivity and specificity (Figure 2). A cutoff level of 5.1 ng/mL for PCT revealed high sensitivity and specificity in predicting liver abscess with sepsis.
 |
Figure 2 Diagnostic efficacies of sepsis were determined by comparing the areas under the curves (AUC). |
Clinical Prognosis
In group A, only antibiotics were used, all patients were discharged, and no recurrence or abscess was found during follow-up. In group B, antibiotic was the first treatment, and all the patients underwent abscess drainage. In subgroup B2, two patients died of sepsis and septic shock, although antibiotics were used and drainage operations were performed.
Discussion
The present study demonstrated that serum PCT level had a potential diagnostic value for liver abscess and sepsis following TACE. WBC count and the levels of PCT, CRP, NEUT, and NEUTP were examined as markers to differentiate abscess from suspicious cases after TACE to clarify the effect of PCT on liver abscess. The mean PCT level was higher in subgroup B2 than in subgroup B1 (P<0.001), and the ROC analysis had high sensitivity and specificity. Collectively, the serum PCT level was a promising inexpensive marker for the diagnosis of liver abscess and sepsis following TACE therapy among patients with HCC.
The formation of liver abscesses after TACE is a rare, but serious, complication.6–8 Physicians should be aware of the predisposing risk factors for TACE because of the possibility of death. The formation of abscesses after TACE is one of the most serious complications of TACE.3 The indication for antibiotic treatment and drainage has therefore been a challenge for many years.9
In the present study, WBC count, the levels of NEUT and NEUTP showed no significant differences and low sensitivity and specificity (Figure 2). After TACE, chemotherapy drugs may cause bone marrow suppression. Also, infection can cause an increase in inflammatory cells, and, therefore, the WBC count is not reliable to predict infection. The CRP level rises even if no infection develops after TACE. Hence, the CRP level is not very helpful for the diagnosis of abscess and sepsis.
Specific biomarkers for abscess are lacking. A previous study showed that CRP and calprotectin had moderate specificity and sensitivity for the diagnosis of abscess.10 No reports on specific biomarkers and liver abscess and sepsis after TACE are currently available. However, PCT has been evaluated in cases of intra-abdominal sepsis or injury where it showed a strong diagnostic value if abscess formation or perforation occurred.11 CRP has been used to indicate the presence of inflammatory disease because its levels rise during acute infection.12 PCT is superior to CRP in terms of accuracy at diagnosis and prognosis of sepsis. It is also a more sensitive and specific biomarker in the diagnosis of sepsis compared with other biomarkers, including the levels of tumor necrosis factor-alpha, lactate, Interleukin (IL)-2, IL-6, IL-8, and IL-10.13,14 Most patients with postoperative infection were treated with antibiotics, and patients with liver abscess were treated with antibiotics and drainage. The results indicated that PCT might be more useful to differentiate abscess with sepsis from abscess only compared with the gold standard of abdominal CT scans.
The present study found that the amount of antibiotics could be reduced according to the PCT level, regardless of the formation of liver abscess indicated by CT. The surviving sepsis campaign added CRP and PCT to the definition of sepsis in 2003. Then, in the early part of the last decade, the surviving sepsis campaign approved the early goal-directed therapy.15,16 The treatment and clinical course of liver abscesses after TACE have some similarities with intra-abdominal sepsis or injury. Even if PCT is not superior to other biomarkers in abdominal infections, it may have its place in the case of liver abscesses after TACE, especially for patients with bacteremia. A total of 33 studies explored CRP as a marker for abdominal infection or complications after surgery.17–19 Persistent CRP levels of more than 100 mg/L 5 days after the surgery indicate abscess formation or other septic complications.20,21 However, other studies reported a limited role of CRP in diagnosing sepsis or predicting outcomes in other clinical scenarios.22–24 This study showed a difference in CRP levels between groups with and without an abscess, but no statistically significant difference was found in the differential diagnosis of sepsis in patients with abscess.
A glycoprotein precursor of calcitonin, PCT, is produced by C cells of the thymus and also by leucocytes, liver, kidney, adipose, and muscle tissue.25 In healthy individuals, the serum levels are usually below 0.1 mg/dL, but can rise within 2 h to 4 h of the inflammatory surge and fall rapidly after halting the primary insult.26–28 Persistently high levels correlated well with increased mortality and severity scores.29 In the present study, a cutoff level of 5.1 ng/mL for PCT revealed high sensitivity and specificity in predicting liver abscess with sepsis; it was more reliable than the WBC count and the levels of NEUT and NEUTP. According to our experience, we suggest routine examination of PCT 1 day after TACE. For the patients with temperature higher than 38.5°C, it is suggested to reexamine every 1–2 days, which can screen out the patients with liver abscess as soon as possible, and can prompt the curative effect of treatment.
Limitations
This study had several limitations. First, this trial was not a randomized controlled trial. Second, this study was a single-center trial and the sample size was limited. Third, further studies should be performed to investigate the use of antibiotics under the guidance of PCT.
Conclusion
Serum PCT was a promising inexpensive marker for the diagnosis of liver abscess and sepsis following TACE therapy among patients with primary liver cancer. A cutoff level of 5.1 ng/mL for PCT revealed high sensitivity and specificity in predicting liver abscess with sepsis.
Acknowledgments
We thank Dr. Jie Min from the Department of Radiology for analysing CT images, Dr. Yan Wang from the Department of Radiology for collecting laboratory and clinical parameters and Dr. Zexin Chen from the Center of Clinical Epidemiology and Biostatistics for statistical analysis.
Disclosure
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article and report no conflicts of interest for this work.
References
1. Yang HT, Zhou SJ, Shen RF, et al. Evaluation on efficacy and safety of arsenic trioxide plus transcatheter arterial chemoembolization versus transcatheter arterial chemoembolization alone for unresectable primary liver cancer. Asian Pac J Cancer Prev. 2017;18(10):2695–2701.
2. Ako S, Nakamura S, Nouso K, et al. Transcatheter arterial chemoembolization to reduce size of hepatocellular carcinoma before radiofrequency ablation. Acta Med Okayama. 2018;72(1):47–52.
3. Lv WF, Lu D, He YS, Xiao JK, Zhou SH, Cheng DL. Liver abscess formation following transarterial chemoembolization: clinical features, risk factors, bacteria spectrum, and percutaneous catheter drainage. Medicine. 2016;95(17):3503. doi:10.1097/MD.0000000000003503
4. Woo S, Chung JW, Hur S, et al. Liver abscess after transarterial chemoembolization in patients with bilioenteric anastomosis: frequency and risk factors. AJR Am J Roentgenol. 2013;200(6):1370–1377. doi:10.2214/AJR.12.9630
5. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis 3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
6. Son DJ, Hong JY, Kim KH, et al. Liver abscess caused by Clostridium haemolyticum infection after transarterial chemoembolization for hepatocellular carcinoma: a case report. Medicine. 2018;97(19):0688. doi:10.1097/MD.0000000000010688
7. Wagnetz U, Jaskolka J, Yang P, Jhaveri KS. Acute ischemic cholecystitis after transarterial chemoembolization of hepatocellular carcinoma. J Comput Assist Tomogr. 2010;34(3):348–353. doi:10.1097/RCT.0b013e3181caaea3
8. Shibata T, Yamamoto Y, Yamamoto N, et al. Cholangitis and liver abscess after percutaneous ablation therapy for liver tumors: incidence and risk factors. J Vasc Interv Radiol. 2003;14(12):1535–1542.
9. Arslan M, Degirmencioglu S. Liver abscesses after transcatheter arterial embolization. J Int Med Res. 2019;47(3):1124–1130. doi:10.1177/0300060518816875
10. Patel PB, Shah J, Baria S. A profile study of 50 cases of liver abscess treated by percutaneous catheter drainage. Int J Surg. 2017;4(8):2490–2494. doi:10.18203/2349-2902.isj20173381
11. Anderson R, Schmidt R. Clinical biomarkers in sepsis. Front Biosci (Elite Ed). 2010;2:504–520.
12. Xiao Z, Wilson C, Robertson HL, et al. Inflammatory mediators in intra-abdominal sepsis or injury – a scoping review. Crit Care. 2015;19:373.
13. Dahan E, Dichtwald S, Amar E, Sorkine P, Weinbroum AA. Low plasma C-reactive protein level as an early diagnostic tool for heatstroke vs. central nervous system–associated infection in the ED. Am J Emerg Med. 2013;31(8):1176–1180. doi:10.1016/j.ajem.2013.04.030
14. Wacker C, Prkno A, Brunkhorst F, Schlattmann P. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis. Lancet Infect Dis. 2013;13(5):426–435. doi:10.1016/S1473-3099(12)70323-7
15. Nargis W, Ibrahim M, Ahamed BU. Procalcitonin versus C-reactive protein: usefulness as biomarker of sepsis in ICU patient. Int J Crit Illn Inj Sci. 2014;4(3):195–199. doi:10.4103/2229-5151.141356
16. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–1377. doi:10.1056/NEJMoa010307
17. Kanno N, Hayakawa N, Suzuki S, Harada Y, Yogo T, Hara Y. Changes in canine C-reactive protein levels following orthopaedic surgery: a prospective study. Acta Vet Scand. 2019;61(1):33. doi:10.1186/s13028-019-0468-y
18. Facy O, Paquette B, Orry D, et al. Inflammatory markers as early predictors of infection after colorectal surgery: the same cut-off values in laparoscopy and laparotomy? Int J Colorectal Dis. 2017;32(6):1–7. doi:10.1007/s00384-017-2805-9
19. Lu J, Zheng L, Li R, et al. Diagnostic value of dynamic monitoring of C-reactive protein in drain drainage to predict early anastomotic leakage after colorectal cancer surgery. Zhonghua Wei Chang Wai Ke Za Zhi. 2017;20(9):1055–1059.
20. Almeida AB, Faria G, Moreira H, Pinto-de-Sousa J, Correia-da-Silva P, Maia JC. Elevated serum C-reactive protein as a predictive factor for anastomotic leakage in colorectal surgery. Int J Surg. 2012;10(2):87–91. doi:10.1016/j.ijsu.2011.12.006
21. Witczak A, Juralowicz P, Modzelewski B, Gawlik M. C-reactive protein as a marker of postoperative septic complications. Pol Przegl Chir. 2012;84(2):93–98. doi:10.2478/v10035-012-0015-2
22. Scepanovic MS, Kovacevic B, Cijan V, et al. C-reactive protein as an early predictor for anastomotic leakage in elective abdominal surgery. Tech Coloproctol. 2013;17(5):541–547.
23. Reith HB, Mittelkotter U, Wagner R, Thiede A. Procalcitonin (PCT) in patients with abdominal sepsis. Intensive Care Med. 2000;26(Suppl 2):165–169. doi:10.1007/s001340051137
24. Ravishankaran P, Shah AM, Bhat R. Correlation of Interleukin-6, Serum Lactate, and C-reactive protein to inflammation, complication, and outcome during the surgical course of patients with acute abdomen. J Interferon Cytokine Res. 2011;31(9):685–690. doi:10.1089/jir.2011.0021
25. Tschaikowsky K, Hedwig-Geissing M, Braun GG, Troeger MR. Predictive value of procalcitonin, interleukin-6, and C-reactive protein for survival in postoperative patients with severe sepsis. J Crit Care. 2011;26(1):54–64. doi:10.1016/j.jcrc.2010.04.011
26. Andrejaitiene J, Sirvinskas E, Zebrauskiene I. Procalcitonin: a new infection marker. Its use in intensive care. Medicina. 2002;38(5):491–498.
27. Wong HR. Sepsis biomarkers. J Pediatr Intensive Care. 2019;8(1):11–16. doi:10.1055/s-0038-1677537
28. Zhang T, Wang Y, Yang Q, Dong Y. Procalcitonin-guided antibiotic therapy in critically ill adults: a meta-analysis. BMC Infect Dis. 2017;17(1):514. doi:10.1186/s12879-017-2622-3
29. Martiny P, Goggs R. Biomarker guided diagnosis of septic peritonitis in dogs. Front Vet Sci. 2019;6:208. doi:10.3389/fvets.2019.00208
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.