")
Back to Journals » Substance Abuse and Rehabilitation » Volume 12
Problems in Social Medicine Related to Alcohol and Deaths: Autopsy Cases in the Southern Part of Osaka City
Authors Tani N , Ikeda T, Hirokawa T, Aoki Y , Shida A, Ikeda K, Morioka F, Ishikawa T
Received 22 June 2021
Accepted for publication 13 October 2021
Published 27 October 2021 Volume 2021:12 Pages 89—103
DOI https://doi.org/10.2147/SAR.S326020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Naoto Tani,1,2 Tomoya Ikeda,1,2 Tatsuya Hirokawa,1,2 Yayoi Aoki,1 Alissa Shida,1 Kei Ikeda,1 Fumiya Morioka,1 Takaki Ishikawa1,2
1Department of Legal Medicine, Osaka City University Medical School, Osaka, 545-8585, Japan; 2Forensic Autopsy Section, Medico-Legal Consultation and Postmortem Investigation Support Center, C/O Department of Legal Medicine, Osaka City University Medical School, Osaka, 545-8585, Japan
Correspondence: Naoto Tani
Department of Legal Medicine, Osaka City University Medical School, 1-4-3 Asahi-machi, Abeno, Osaka, 545-8585, Japan
Tel +81-6-6645-3767
Fax +81-6-6634-3871
Email [email protected]
Purpose: The purpose of this study was to examine the social and medical background of alcohol dependence and to prevent the abuse of alcohol.
Methods: Alcohol and deaths were retrospectively investigated based on the forensic postmortem data of 1694 decedents ≥ 20 years of age in 2008– 2017. Of these, the 999 cases that could be tested for alcohol within 48 h of death were examined.
Results: The alcohol-positive and alcohol-negative groups included 179 (17.9%) and 820 (82.1%) cases, respectively. In terms of medical issues, compared with the alcohol-negative group, men in the positive group were mostly in their 40s to 60s, whereas women’s age peaked in the 70s. The causes of death included many blunt injuries in men, though there was no difference in women. Underlying diseases were more frequent in men than women, with many of them having heart or liver disease, and the percentage of cases with mental disorders was 16.8% in the alcohol-positive group. In 15 cases of the alcohol-positive group, phenothiazine and barbituric acids were detected in 53.3% and 46.7% of cases, respectively. The incidence of traffic accidents and homicides was higher in the alcohol-positive group than in the alcohol-negative group.
Conclusion: Measures to address social issues based on risk factors for alcohol and deaths are required.
Keywords: forensic autopsy, alcohol, medical issue, socioenvironmental issue, pharmacological issue
Introduction
Excessive or long-term alcohol intake affects the mind and causes hepatic dysfunction and circulatory disorders.1–9 In addition, mental disorders due to alcohol intake may result in work accidents and fights.5,10 Furthermore, the mental disorders due to alcohol may involve other drugs.11,12 Past research regarding alcohol use has been one-dimensional, examining alcohol and illness, alcohol and traffic accidents, etc. However, there have been no reports that examined the general impacts of alcohol use. Specifically, there are complex issues related to the “medical problems” of the diseases due to alcohol, the “social problems” arising from accidents related to alcohol, and the “pharmacological problems” that arise when drugs are taken with alcohol. Therefore, in this study, problems due to alcohol were examined from a multidimensional perspective, and each problem was examined comprehensively. Alcohol can have a pharmacological impact on existing medication use and can potentially lead to deaths due to overdose.12 Alcohol may be involved in the process of various deaths, which is important for specialists in forensic autopsy cases.
There is a scarcity of reports that systematically summarized survey results. The results of existing surveys mentioned above can be classified into medical, socioenvironmental, or pharmacological issues. Thus, the present study presents the results of an interdisciplinary examination.
Materials and Methods
Sample Collection
The legal drinking age in Japan is 20 years. Thus, the present study targeted autopsies performed over a period of 10 years between 2008 and 2017 involving people ≥20 years of age in the Department of Legal Medicine, Osaka City University Medical School. Cases that were examined within 48 h of death were targeted considering the impact of postmortem production of alcohol. Exclusion criteria for the study included cases under 20 years of age, examined 48 h or more after death, blood could not be collected, or alcohol levels were not examined. The number of autopsies performed in 10 years was 1694, with 999 cases suitable for alcohol tests (717 males and 282 females). The causes of death were diagnosed according to the macropathological findings at autopsy and the results of micropathological and toxicological examinations.13 The background data of the patients were recorded in our database for each autopsy. These data were stored in our department and used for the present study. The variables for analysis were determined based on the autopsy record reviews and information obtained from investigations conducted by the authorities.
Study Variable Definitions
To test for alcohol in the blood, cases that could be tested for blood from the right heart, the left heart, or the iliac artery were targeted. The cut-off value for alcohol detection was 0.1 mg/mL.14 Sample information (including age, sex, cause of death, organ disease, mental disorder, occupation, traffic accident, type of death, environmental factors, type of drug, and alcohol concentration) was collected based on postmortem pathological examination, postmortem biochemistry findings, toxicological findings, and information obtained from investigations conducted by the authorities. Blood alcohol concentrations were determined using headspace gas chromatography/mass spectrometry.15 Ethanol levels were measured in cases within 48 h of death taking into account postmortem changes that occur with the passage of time. Toxicological analyses were conducted to identify the drugs that victims had been using. Drug analyses were performed using gas chromatography/mass spectrometry.16 Toxicological analyses were performed on samples of right heart blood. The toxic level of drug concentrations was classified with reference to the report by Winek et al.17
Data Analysis
This study analysed autopsy data and information obtained from investigations by the authorities that were previously recorded at the Department of Legal Medicine, Osaka City University Medical School. Autopsy data were already standardized at the time of recording, and information obtained from the investigations conducted by authorities was reviewed by three forensic doctors and researchers. The flow diagram shows the number of records identified in the search and the number of studies included in the review (Figure 1). Autopsy records were analysed. The groups that tested positive or negative for alcohol in the blood (the alcohol-positive and alcohol-negative groups) were compared by age, sex, cause of death, organ disease, mental disorder, occupation, traffic accident, type of death, death due to accident, manner of death, environmental factors, type of drug, and alcohol concentration. The information was recorded in a Microsoft Excel database for analysis. The results for quantitative and qualitative variables are described as percentages.
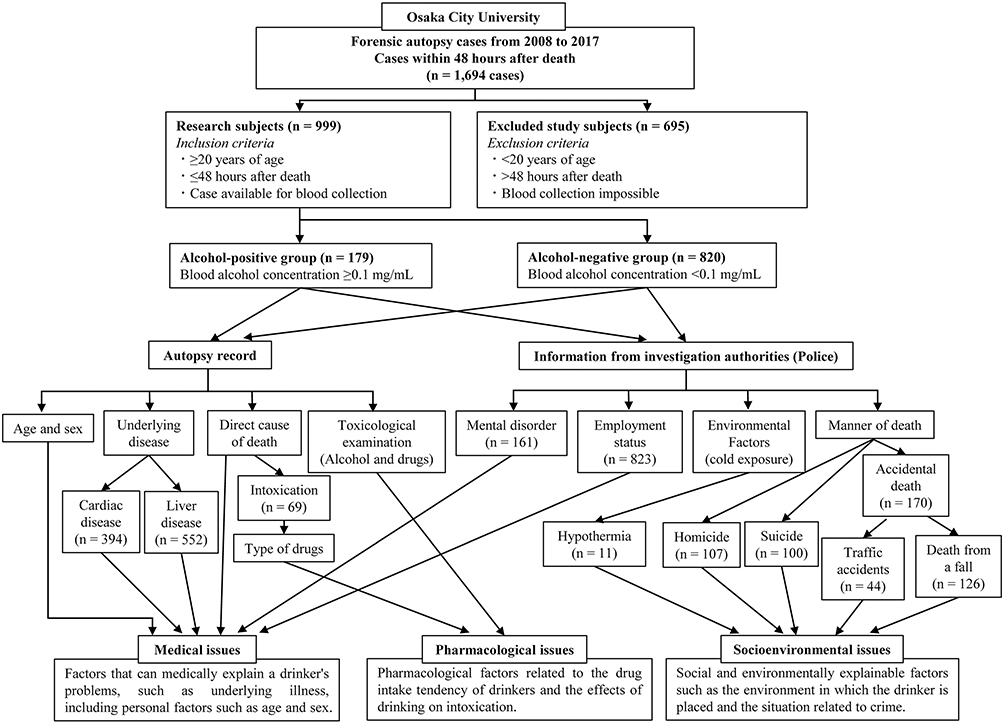 |
Figure 1 Flowchart of the cases. The cases include 1694 cases examined within two days after death from 2008 through 2017. Alcohol was detected in 179 of those 20 years or older and not detected in 820 cases. Autopsy records and the investigation records provided by the police were used for this study. |
Ethics Statement
This study design was approved by the ethics review board of the Osaka City University Medical School.
Results
Medical Issues
Age and Sex
The alcohol-positive and alcohol-negative groups included 179 and 820 cases, respectively. Among the 717 males, alcohol was detected and not detected in 136 (19.0%) and 581 (81.0%) cases, respectively. Among the 282 females, alcohol was detected and not detected in 43 (15.2%) and 239 (84.8%) cases, respectively. The details of the 179 cases in the alcohol-positive group (mean age, 56 years; median age, 58 years) were as follows: eight (4.5%) cases in their 20s (4 males and 4 females), 22 (12.3%) cases in their 30s (14 males and 8 females), 32 (17.9%) cases in their 40s (27 males and 5 females), 32 (17.9%) cases in their 50s (27 males and 5 females), 45 (25.1%) cases in their 60s (38 males and 7 females), 30 (16.8%) cases in their 70s (19 males and 11 females), eight (4.5%) cases in their 80s (5 males and 3 females), and 2 (1.1%) cases in their 90s (2 males) (Figure 2A). The details of the 820 cases in the alcohol-negative group (mean age, 61 years; median age, 64 years) were as follows: 48 (5.9%) cases in their 20s (32 males and 16 females), 65 (7.9%) cases in their 30s (47 males and 18 females), 110 (13.4%) cases in their 40s (81 males and 29 females), 111 (13.5%) cases in their 50s (89 males and 22 females), 194 (23.7%) cases in their 60s (157 males and 37 females), 144 (17.6%) cases in their 70s (107 males and 37 females), 124 (15.1%) cases in their 80s (56 males and 68 females), 23 (2.8%) cases in their 90s (12 males and 11 females), and one (0.1%) case in the 100s (1 female) (Figure 2B). Among males in the alcohol-positive group, 67.6% (92/136 cases) were in their 40s to 60s. Females in the alcohol-positive group showed a bimodal distribution with a peak in their 30s (18.6%, 7/43 cases) and a peak in their 70s (25.6%, 11/43 cases).
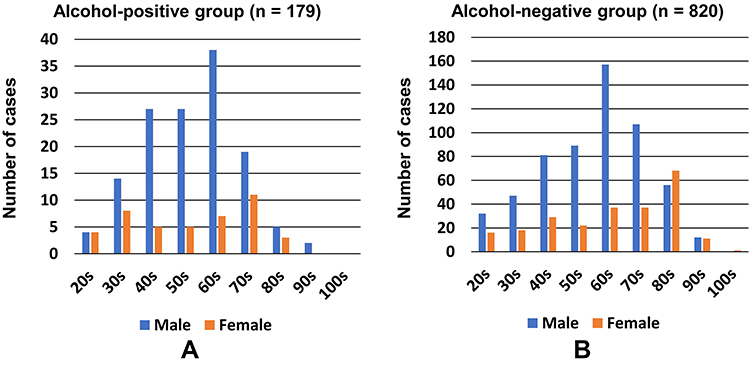 |
Figure 2 The graph shows the age-specific number of cases in the alcohol-positive group (A) and the alcohol-negative group (B), for men and women. In the alcohol-positive group, men in their 60s accounted for 27.9% (38/136), whereas women were in their 30s (18.6%, 8/43) and 70s (25.6%, 11/43). |
Cause of Death
The causes of death for 179 cases in the alcohol-positive group were as follows: 53 (29.6%) cases of blunt injury (43 males and 10 females), 27 (15.1%) cases of fire-related death (21 males and 6 females), 21 (11.7%) cases of sharp instrument injury (19 males and 2 females), 18 (10.1%) cases of asphyxia (11 males and 7 females), 15 (8.4%) cases of intoxication (8 males and 7 females), 13 (7.3%) cases of drowning (11 males and 2 females), 5 (2.8%) cases of hyperthermia (2 males and 3 females), 3 (1.6%) cases of hypothermia (3 males), and 1 (0.6%) case of gunshot wound (1 male). Among deaths caused by illnesses, 11 (6.1%) were heart disease (6 males and 5 females), 2 (1.1%) were central nervous system disorder (1 male and 1 female), and 10 (5.6%) were other natural death (10 males) (Figure 3A). The causes of death for 179 cases in the alcohol-negative group were as follows: 256 (31.2%) cases of blunt injury (204 males and 52 females), 189 (23.0%) cases of fire-related death (132 males and 57 females), 81 (9.9%) cases of asphyxia (50 males and 31 females), 52 (6.3%) cases of intoxication (34 males and 18 females), 34 (4.1%) cases of drowning (20 males and 14 females), 28 (3.4%) cases of sharp instrument injury (20 males and 8 females), 22 (2.7%) cases of hyperthermia (13 males and 9 females), 11 (1.3%) cases of hypothermia (5 males and 6 females), 6 (0.7%) cases of gunshot wound (5 males and 1 female), and 2 (0.2%) cases of electrocution (2 males). Among deaths caused by illnesses, 45 (5.5%) cases were heart disease (38 males and 7 females), 19 (2.3%) cases were central nervous system disorder (11 males and 8 females), and 75 (9.1%) cases were other natural death (29 males and 46 females) (Figure 3B).
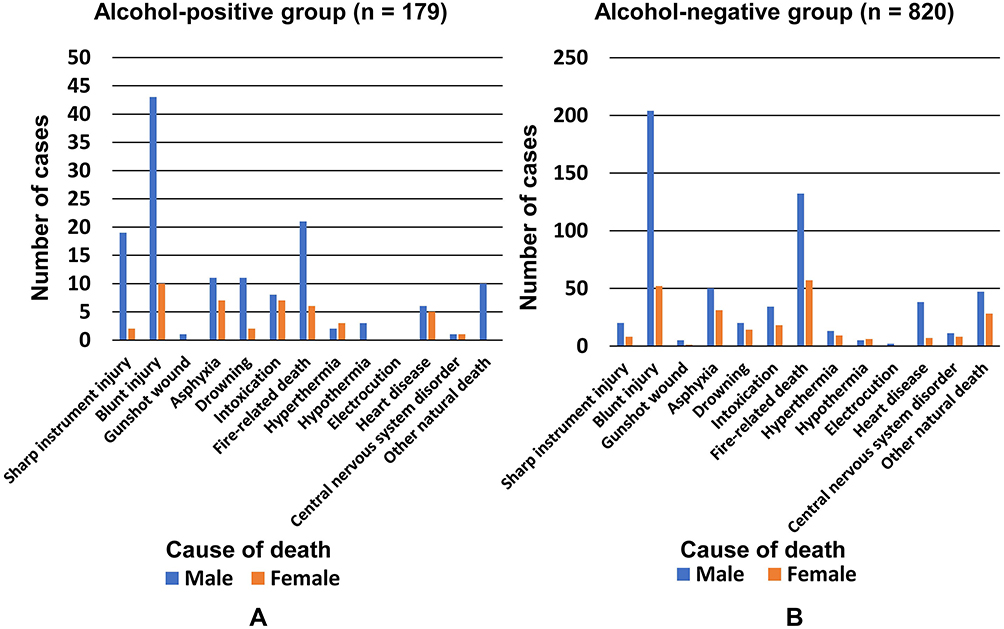 |
Figure 3 The graph indicates the number of cases by cause of death in the alcohol-positive group (A) and the alcohol-negative group (B). In all of groups (A and B), blunt injury ((A) 29.6% (53/179), (B) 15.1% (274/179)) and fire-related deaths ((A) 31.2% (256/820), (B) 23.0% (189/820)), respectively, were common. Although there is a marked difference between groups (A and B) in men, there is no difference in the causes of death in women. |
Organ Disease
Among the 179 cases in the alcohol-positive group, 90 (50.3%) cases of underlying heart disease (eg, ischemic heart disease and congestive heart failure; 70 males and 20 females), 76 (42.5%) cases of liver disease (eg, cirrhosis and fatty liver; 59 males and 17 females), 61 (34.1%) cases of pulmonary disease (eg, aspiration pneumonia and emphysema; 51 males and 10 females), 33 (18.4%) cases of pancreatic disease (eg, pancreatic fibrosis and fatty degeneration; 27 males and 6 females), 22 (12.3%) cases of cranial nerve disease (eg, cerebral infarction and cerebral atrophy; 16 males and 6 females), and 18 (10.1%) cases of kidney disease (eg, nephritis and renal insufficiency; 13 males and 5 females) were noted (Figure 4A). Among the 820 cases in the alcohol-negative group, 462 (56.3%) cases of heart disease (330 males and 132 females), 318 (38.8%) cases of pulmonary disease (230 males and 88 females), 223 (27.2%) cases of liver disease (166 males and 57 females), 168 (20.5%) cases of kidney disease (124 males and 44 females), 160 (19.5%) cases of pancreatic disease (112 males and 48 females), and 141 (17.2%) cases of cranial nerve disease (85 males and 56 females) were noted (Figure 4B).
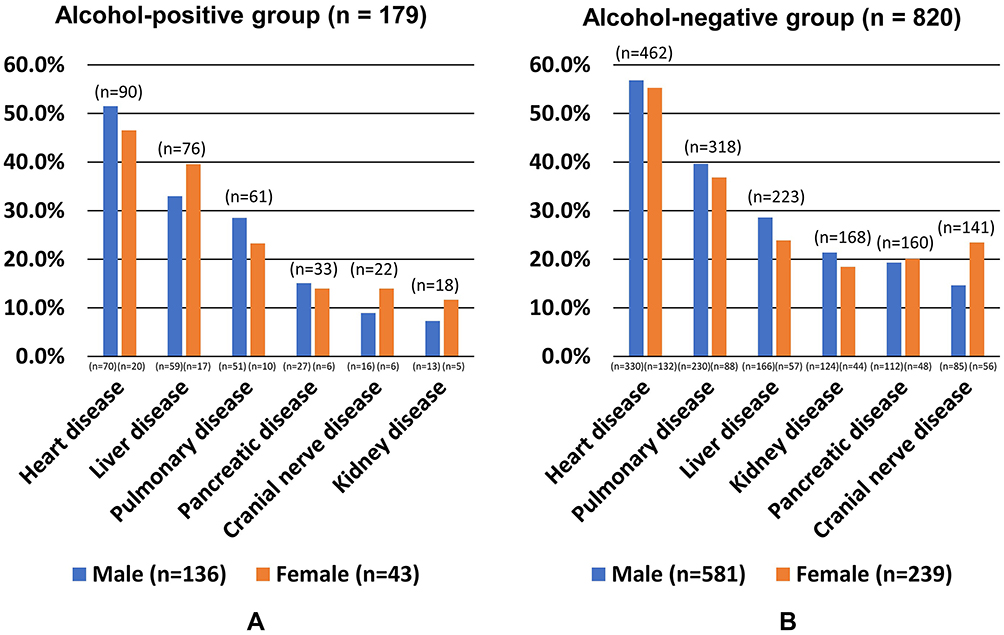 |
Figure 4 The graph shows the number of cases according to the existing medical history in the alcohol-positive (A) and alcohol-negative groups (B). In group (A), cardiac disease (50.3%, 90/179), liver disease (42.5%, 76/179), and pulmonary disease (38.8%, 318/820) are common. In group (B) cardiac disease, liver disease, and pulmonary disease are common, in that order. In group (A), more women than men have liver disease, whereas more men than women have liver disease in group (B). In addition, in group (A) and group (B), more men than women have cardiac disease and pulmonary disease, respectively. |
The classification of liver diseases showed the differences between the alcohol-positive and alcohol-negative groups. The alcohol-positive group included 43 (51.8%) cases of cirrhosis (34 males and 9 females), 37 (44.6%) cases of fatty liver (31 males and 6 females), and 12 (14.5%) cases of hepatitis (8 males and 4 females). Moreover, among the 820 cases in the alcohol-negative group, 114 (37.3%) cases of cirrhosis (92 males and 22 females), 78 (25.5%) cases of fatty liver (52 males and 26 females), 64 (20.9%) cases of hepatitis (51 males and 13 females), and 3 (1.0%) cases of liver cancer (3 males) were noted (Figure 5A).
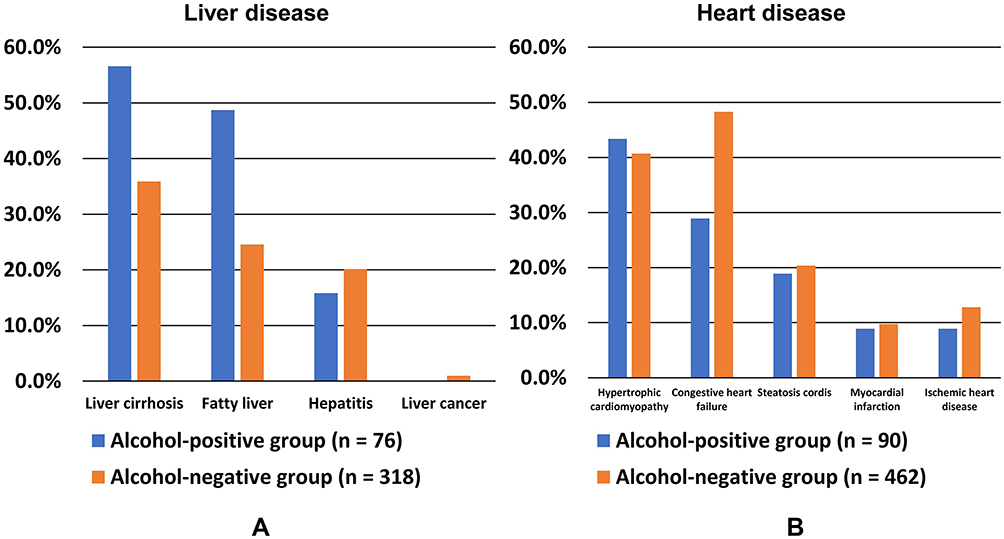 |
Figure 5 This figure shows the details of liver disease (A) and heart disease (B) in the alcohol-positive group and alcohol-negative group, respectively. There are more cases of cirrhosis (56.6%, 43/79) and fatty liver (48.7%, 37/76) in the alcohol-positive group. In addition, hypertrophic cardiomyopathy (43.3%, 39/90) is slightly more common in the alcohol-positive group. However, congestive heart failure (48.3%, 223/462) is more common in the alcohol-negative group than in the alcohol-positive group. |
The details of heart disease, which was the most common underlying condition in the present study, are also shown. The alcohol-positive group included 39 (43.3%) cases of hypertrophic cardiomyopathy (35 males and 4 females), 26 (28.9%) cases of congestive heart failure (18 males and 8 females), 17 (18.9%) cases of steatosis cordis (11 males and 6 females), 8 (8.9%) cases of myocardial infarction (8 males), and 80 (8.9%) cases of ischemic heart disease (8 males). Among the 820 cases in the alcohol-negative group, 188 (40.7%) cases of hypertrophic cardiomyopathy (146 males and 42 females), 223 (48.3%) cases of congestive heart failure (155 males and 68 females), 94 (20.3%) cases of steatosis cordis (54 males and 40 females), 45 (9.7%) cases of myocardial infarction (37 males and eight females), and 59 (12.8%) cases of ischemic heart disease (43 males and 16 females) were noted (Figure 5B).
Moreover, coronary artery lesions (eg, stenosis due to atherosclerosis and intimal thickening) were observed in 12 (6.7%) cases in the alcohol-positive group (11 males and 1 female) and 77 (9.4%) cases in the alcohol-negative group (63 males and 14 females).
Mental Disorder
Of the 999 cases, 161 (16.1%) had underlying mental disorders. Moreover, among the 179 and 820 cases in the alcohol-positive and alcohol-negative groups, 36 (20.1%) and 125 (15.2%) had mental disorders, respectively. The alcohol-positive group had cases with multiple mental disorders classified as depression (13 cases, 36.1%), schizophrenia (12 cases, 33.3%), alcohol dependence (11 cases, 30.5%), psychotic disorders excluding depression and schizophrenia (5 cases, 13.8%), insomnia (5 cases, 13.8%), anxiety disorder (3 cases, 8.3%), and eating disorder (1 case, 2.8%). In addition, the alcohol-negative group had 125 cases with mental disorders, including depression (44 cases, 35.2%), schizophrenia (40 cases, 32.0%), psychotic disorders excluding depression and schizophrenia (22 cases, 17.6%), insomnia (22 cases, 17.6%), alcohol dependence (16 cases, 12.8%), anxiety disorder (12 cases, 9.6%), and eating disorder (2 cases, 1.6%).
Employment Status
Employment status was identified in 144 of 179 cases in the alcohol-positive group; 45 (31.3%) cases (37 males and 8 females) and 99 (68.7%) cases (71 males and 28 females) were employed and unemployed, respectively (Figure 6A). Moreover, 8 (8.1%) cases were receiving government welfare. Furthermore, employment status was determined in 679 of the 820 cases in the alcohol-negative group. Of the cases, 187 (27.5%) cases (152 males and 35 females) and 492 (72.5%) cases (315 males and 177 females) were employed and unemployed, respectively (Figure 6B); 32 cases were receiving government welfare.
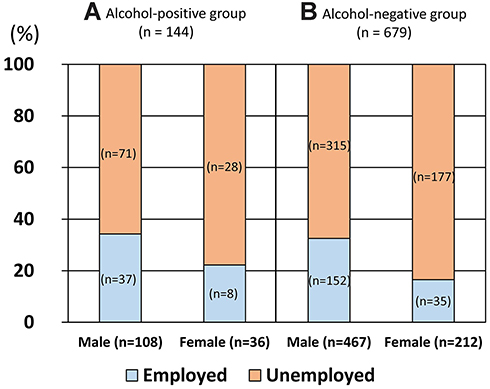 |
Figure 6 The graph shows men’s and women’s employment status in the alcohol-positive group (A) and alcohol-negative group (B). In the alcohol-positive group, 31.3% (45/144) are employed compared to 27.5% (187/679) in the alcohol-negative group. |
Socioenvironmental Issues
Type of Death
This study classified and examined the types of death as pathological deaths (161 cases: 16.1%), deaths due to accident (170 cases: 17.0%), suicide (100 cases: 10.0%), homicide (107 cases: 10.7%), and unexpected and unknown external causes (461 cases: 46.1%) (Figure 7).
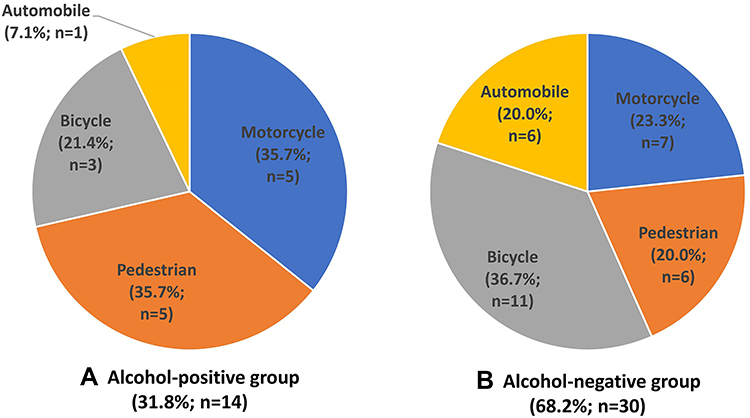 |
Figure 7 The graph shows the manner of death in the alcohol-positive group (A) and the alcohol-negative group (B). In the alcohol-positive group, there are many accidental deaths (18.4%, 33/179). In the alcohol-negative group (B), there are many pathological deaths (16.8%, 138/820) and accidental deaths (16.7%, 137/820). |
Details of Deaths Due to Accidents
There were 44 cases of deaths that were clearly attributed to traffic accidents. Among the 44 cases, alcohol was detected and not detected in 14 (31.8%) cases and 30 (68.2%) cases, respectively. In the alcohol-positive group, 5 (35.7%) cases of motorcycle accidents, 5 (35.7%) cases of pedestrian accidents, 3 (21.4%) cases of bicycle accidents, and 1 (7.1%) case of automobile accident were noted (Figure 8A). Moreover, 11 (36.7%) cases of bicycle accidents, 7 (23.3%) cases of motorcycle accidents, 6 (20.0%) cases of pedestrian accidents, and 6 (20.0%) cases of automobile accidents were noted in the alcohol-negative group (Figure 8B).
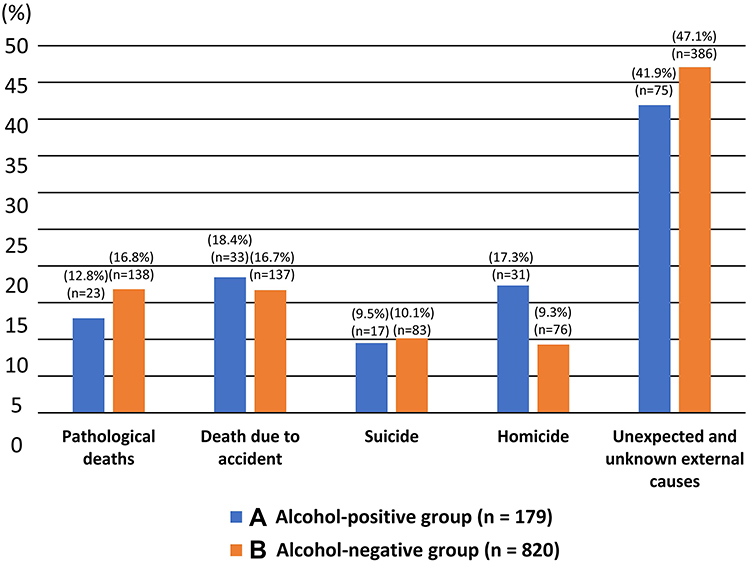 |
Figure 8 The graph shows the frequency according to the kind of traffic accident in the alcohol-positive group (A) and the alcohol-negative group (B). In the alcohol-positive group, motorcycle (37.5%, 5/14) and pedestrian accidents (35.7%, 5/14) account for 70% or more of cases. Bicycle accidents are uncommon in the alcohol-positive group (21.4% 3/14), whereas there are many bicycle accidents (36.7%, 11/30) in the alcohol-negative group. |
Details of the Deaths Due to Homicide and Suicide
In the alcohol-positive (179 cases) and alcohol-negative groups (820 cases), 31 (17.3%) cases and 76 (9.3%) cases were homicides, and 17 (9.5%) cases and 83 (10.1%) cases were suicides, respectively. The homicides in the alcohol-positive group (n = 31) were classified as stab wound (18 cases, 58.1%), violence (8 cases, 25.8%; 2 cases head injury and 6 cases other than head injury), asphyxia (5 cases, 16.1%; 4 cases of strangulation, and 1 case of hanging; Figure 9A). Moreover, the details of the causes of death for 26 cases of violence and stab wound were exsanguination and haemorrhagic shock (22 cases, 86.3%), acute subdural haematoma (1 case, 3.8%), traumatic shock (1 case, 3.8%), pulmonary contusion (1 case, 3.8%), and asphyxiation by aspiration of blood from the nasal cavity and lip mucosal tear injuries (1 one case, 3.8%). In the alcohol-negative group, 33 cases of violence (43.4%; 20 cases of head injury and 13 cases other than head injury), 20 (26.3%) cases of asphyxia (17 cases of strangulation, 1 case of hanging, and 2 cases of obstruction to nose and mouth), 17 (22.4%) cases of stab wound, 2 (2.6%) cases of drowning, 2 (2.6%) cases of arson, 1 (1.3%) case of gunshot wound, and 1 (1.3%) case of burn were noted (Figure 9B). The details of the causes of death for the 50 cases of violence and stab wound were 13 (26.0%) cases of acute subdural haematoma, 20 (40.0%) cases of exsanguination and haemorrhagic shock, 6 (12.0%) cases of traumatic shock, 4 (8.0%) cases of traumatic subarachnoid haemorrhage, 4 (8.0%) cases of cerebral contusion/haemorrhage/swelling, 1 (2.0%) case of a cervical injury, 1 (2.0%) case of asphyxiation by aspiration of blood from a left lung injury, and 1 (2.0%) case of pulmonary hilar laceration.
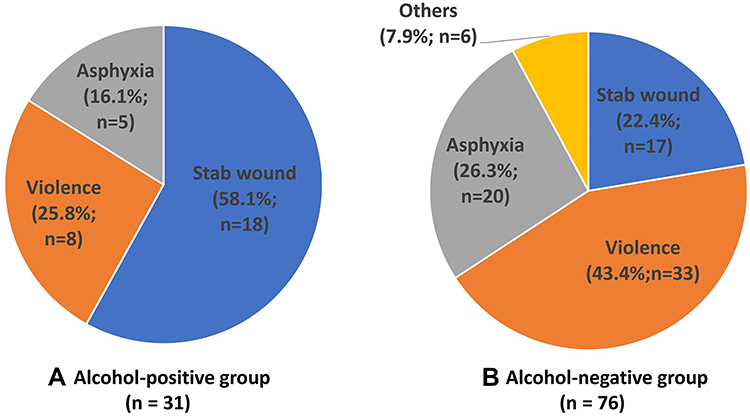 |
Figure 9 The graph shows the frequency according to the method of homicide (n=107) in the alcohol-positive group (A) and the alcohol-negative group (B). In the alcohol-positive group (A), stab wound accounts for 58.1% (18/31), whereas violence accounts for 43.4% (33/76) in the alcohol-negative group. |
Among suicide cases in the alcohol-positive group, 12 (70.6%) cases of asphyxia (hanging, 11 cases; obstruction of the nose and mouth with plastic around the nose and mouth, 1 case), 2 (11.8%) cases of sharp instrument injury, 1 (5.9%) case of gunshot wounds, 1 (5.9%) case of drowning, and 1 (5.9%) case of acute alcohol poisoning were noted (Figure 10A). Among suicide cases in the alcohol-negative group, 36 (43.4%) cases of asphyxia (34 cases of hanging, 2 cases of obstruction to the nose and mouth with a bag over the head and an obstacle stuffed in the throat), 21 (25.3%) cases of jumping, 5 (6.0%) cases of burns, 5 (6.0%) cases of gunshot wound, 4 (4.8%) cases of sharp instrument injury, 4 (4.8%) cases of carbon monoxide intoxication, 3 (3.6%) cases of jumping in front of a train, 3 (3.6%) cases of drug intoxication, and 2 (2.4%) cases of drowning were noted (Figure 10B).
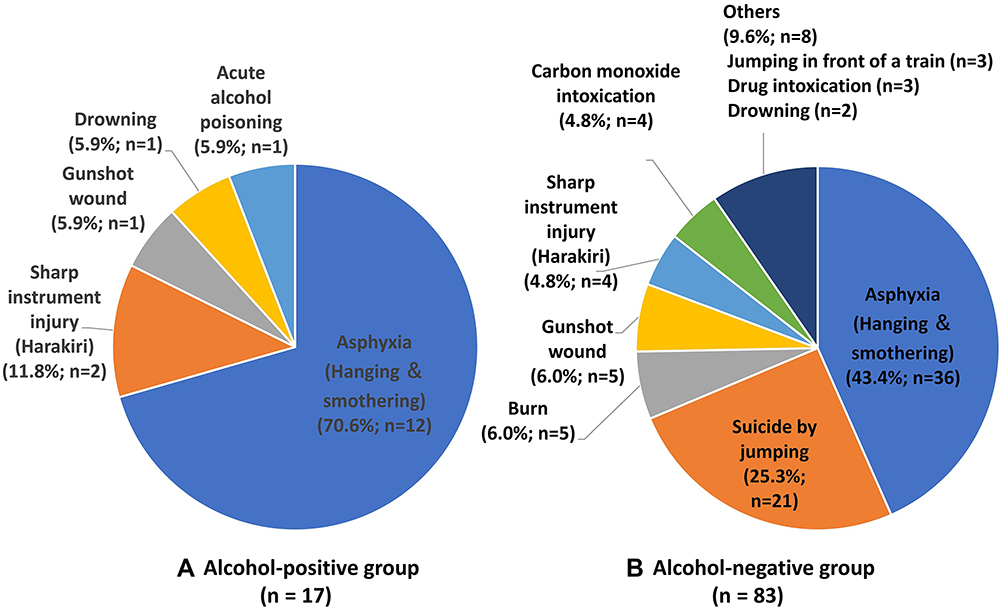 |
Figure 10 The graph shows the method of suicide (n = 100) in the alcohol-positive group (A) and the alcohol-negative group (B). Asphyxia accounts for 70.6% (12/17) of cases in the alcohol-positive group and 43.4% (36/86) in the alcohol-negative group. |
Environmental Factors
Among the 11 cases of deaths caused by hypothermia in the alcohol-negative group, 8 (72.7%) cases and 3 (27.3%) cases were found indoors and outdoors, respectively. However, all 3 (100%) cases of hypothermia in the alcohol-positive group were discovered outdoors on the street.
Pharmacological Issues
Intoxication
The classification of the cause of death due to intoxication in 15 cases in the alcohol-positive group was 7 (46.7%) cases of psychotropic poisoning, 5 (33.3%) cases of alcohol poisoning, 2 (13.3%) cases of methamphetamine poisoning, and 1 (6.7%) case of surfactant poisoning with detergent. The classification of the cause of death in 54 cases due to intoxication in the alcohol-negative group was 24 (44.4%) cases of methamphetamine poisoning, 21 (38.9%) cases of psychotropic poisoning, 4 (7.4%) cases of carbon monoxide poisoning, 2 (3.7%) cases novel psychoactive substance poisoning, 1 (1.9%) case of alcohol poisoning, 1 (1.9%) case of noninsulin diabetic drug poisoning, and 1 (1.9%) case of vecuronium poisoning.
Types of Drugs
Drugs that caused intoxication in the alcohol-positive group were classified by type, with 2 (13.3%) cases of methamphetamine (1 case of toxic dose and 1 case below the toxic dose), 1 (6.7%) case of narcotics (1 case below the toxic dose), 8 (53.3%) cases of phenothiazines (1 case of fatal dose, 6 cases of toxic dose, and 1 case below the toxic dose), 7 (46.7%) cases of barbituric acids (7 cases below the toxic dose), 3 (20.0%) cases of benzodiazepines (3 cases below the toxic dose), 1 (6.7%) case of tetracyclic antidepressant (1 case of toxic dose), and 3 (20.0%) cases of other psychotropics (2 cases of fatal dose and 1 case of toxic dose).
Drugs that caused intoxication in the alcohol-negative group were classified according to types, with 24 (46.2%) cases of methamphetamine (6 cases of fatal dose, 12 cases of toxic dose, and 6 cases below the toxic dose), 18 (34.6%) cases of phenothiazines (4 cases of fatal dose, 9 cases of toxic dose, and 5 cases below the toxic dose), 22 (42.3%) cases of barbituric acids (1 case of fatal dose, 3 cases of toxic dose, and 18 cases below the toxic dose), 6 (11.5%) cases of tricyclic antidepressants (1 case of fatal dose, 1 case of toxic dose, and 4 cases below the toxic dose), 17 (32.7%) cases of benzodiazepines (3 cases of fatal dose, 1 case of toxic dose, 9 cases below the toxic dose, and 4 unknown cases), 3 (5.8%) cases of tetracyclic antidepressants (2 cases of fatal dose and 1 case below the toxic dose), 5 (9.6%) cases of nonbenzodiazepines (1 case below the toxic dose and 4 unknown cases), 2 (3.8%) cases of antiseizure drugs (1 case of fatal dose and 1 case below the toxic dose), 8 (5.8%) cases of other psychotropics (2 cases of fatal dose, 5 cases of toxic dose, and 1 case below the toxic dose), and 5 (9.6%) cases of other drugs (1 case of fatal dose, 2 cases of toxic dose, and 2 cases below the toxic dose) (Tables 1 and 2).
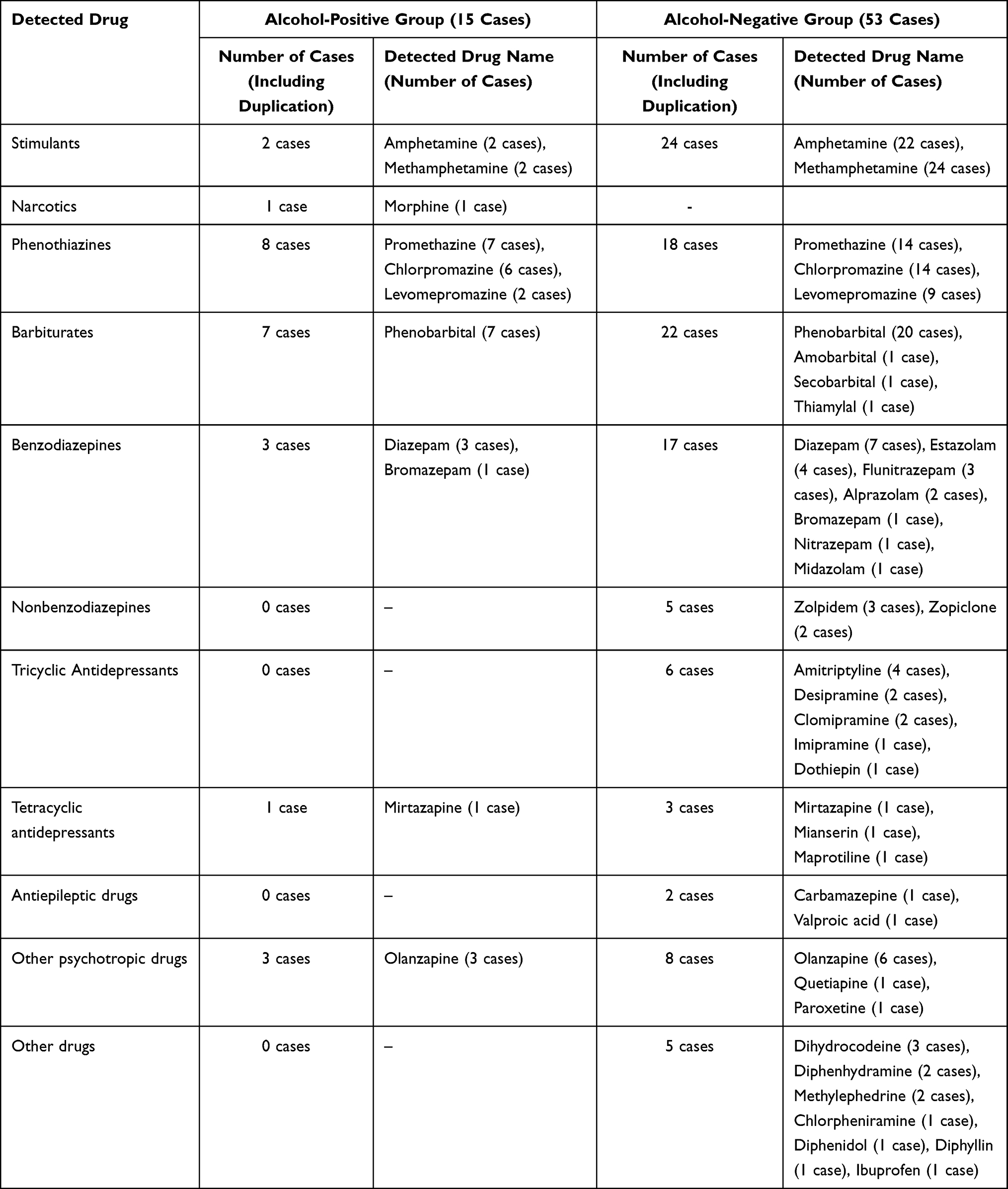 |
Table 1 Drugs Detected in Blood in Intoxication Cases in the Alcohol-Positive and Alcohol-Negative Groups |
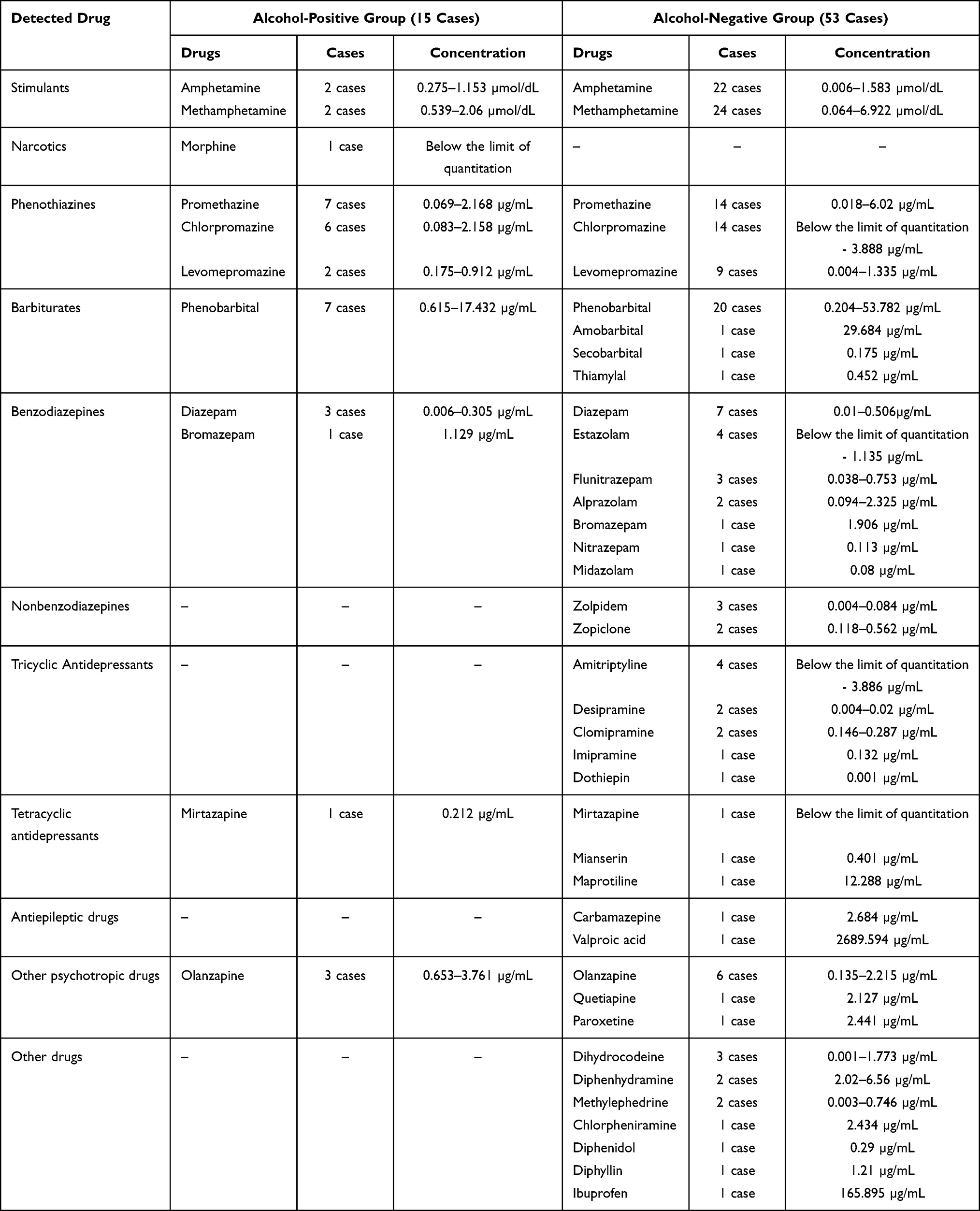 |
Table 2 Concentrations of Drugs Detected in the Blood in Overdose Cases in the Alcohol-Positive and Alcohol-Negative Groups |
Alcohol Concentrations
Ethanol concentrations could be measured in the blood from the right heart in 138 of 179 cases in the alcohol-positive group. Ethanol concentrations in right endocardial blood were 0.1–0.5 mg/mL in 49 cases, 0.5–1.0 mg/mL in 22 cases, 1.0–1.5 mg/mL in 24 cases, 1.5–2.0 mg/mL in 13 cases, 2.0–2.5 mg/mL in 12 cases, 2.5–3.0 mg/mL in 5 cases, and 3.0–3.5 mg/mL in 5 cases. Moreover, ethanol concentrations could be measured in the blood from the left heart in 134 cases. Ethanol concentrations in left endocardial blood were 0.1–0.5 mg/mL in 39 cases, 0.5–1.0 mg/mL in 24 cases, 1.0–1.5 mg/mL in 20 cases, 1.5–2.0 mg/mL in 12 cases, 2.0–2.5 mg/mL in 10 cases, 2.5–3.0 mg/mL in 5 cases, 3.0–3.5 mg/mL in 4 cases, and 3.5–4.0 mg/mL in 2 cases. Furthermore, ethanol concentrations could be measured in the blood from the common iliac vein in 82 cases. Ethanol concentrations in common iliac vein blood were 0.1–0.5 mg/mL in 19 cases, 0.5–1.0 mg/mL in 10 cases, 1.0–1.5 mg/mL in 12 cases, 1.5–2.0 mg/mL in 9 cases, 2.0–2.5 mg/mL in 6 cases, 2.5–3.0 mg/mL in 2 cases, and 3.0–3.5 mg/mL in 2 cases. Many cases had ethanol concentrations within 0.1–0.5 mg/mL in all sampled sites.
Discussion
Medical, socioenvironmental, and pharmacological factors were examined in the alcohol-positive group with the purpose of preventing deaths due to drinking. Alcohol was detected most frequently in males in their 40s to 60s, whereas females showed a bimodal distribution with peaks in their 30s and 70s, although no sex-based difference was noted between the alcohol-positive and alcohol-negative groups. This study could not provide a detailed explanation for the difference in alcohol detection by age group between males and females. However, in the problems related to drinking, a mixture of socioeconomic and medical factors is assumed.18–20 In the alcohol-positive group, 16.8% of cases had mental disorders. In addition, blunt force trauma and fire were common causes of death in the alcohol-positive group, indicating that alcohol consumption may impair the ability to foresee the consequences of their actions and inhibiting the ability to avoid risks.
In terms of underlying diseases, heart disease was the most common, followed by liver disease, respiratory disease, and central nervous system disorders. The onset of myocardial infarction and ischemic heart disease is known to have a negative correlation with alcohol consumption.21 Four possible reasons exist. The first reason is the inhibitory effect of alcohol on platelet aggregation.22 The second reason is that alcohol consumption increases the secretion of tissue plasminogen activator from vascular endothelial cells, which in turn promotes the fibrinolytic system.23,24 These two actions are known to be thrombolytic in the hyperacute phase, which is caused by intravascular ischemic action by thrombi. The third reason is alcohol consumption leading to an increased high-density lipoprotein cholesterol level (increased HDL2 and HDL3 levels), which is negatively correlated with the frequency of ischemic heart disease. Thus, ischemic heart disease is prevented.25,26 The fourth reason is not the action of alcohol itself, but the existence of strong platelet aggregation inhibitors by antioxidants such as polyphenols.27 However, the correlations of alcohol, heart disease, and sex in the present study may indicate the impact of alcohol on hypertension onset. According to Klatsky et al, ethanol consumption of 36 g or more per day is a risk factor for hypertension. Ethanol specifically contributes to the increase in systolic blood pressure.28 This contribution is independent of other risk factors for hypertension.29 The linking of alcohol consumption, age, and heart disease in the present study indicates that abstinence would lead to lower blood pressure, as previously reported.30
As for socioenvironmental issues, deaths due to traffic accidents and homicide were more common in the alcohol-positive than in the alcohol-negative group. The most common kinds of traffic accidents in the alcohol-positive group were motorcycle and pedestrian accidents. Moreover, not many accidents that involved automobiles and bicycles were noted. Perhaps no difference existed in the frequency of alcohol-related accidents with motorcycles, automobiles, and pedestrians. However, motorcycles and pedestrian accidents were more likely to cause a higher degree of damage, leading to a higher mortality rate when compared with the mortality rate of automobile accidents.
In the classification of alcohol-related homicides, many cases of haemorrhagic shock due to sharp instrument injuries incurred during a fight and subdural haematoma from being punched were noted. This indicates that alcohol consumption lowers emotional inhibition,31 blood coagulation,32 and the ability of the cervical muscles to hold the head, which could lead to haemorrhagic shock and subdural haematoma. Thus, medical and pharmacological factors are likely to be involved in addition to socioenvironmental issues.
Under pharmacological issues, antipsychotic (phenothiazines) and psychotropic (barbituric acids) drugs were detected most often in alcohol-related overdose deaths. The frequently detected drugs, chlorpromazine, promethazine, and phenobarbital, are components of Vegetamin (Shionogi Co., Ltd., Tokyo, Japan), and their interaction with alcohol was confirmed in the present survey. However, the sale of Vegetamin has been discontinued since December 2016 as requested by The Japanese Society of Psychiatry and Neurology to the seller, Shionogi Co., Ltd., to prevent substance abuse. Phenobarbital is especially dangerous because it is highly addictive.33 The present survey showed that 16.8% of cases in the alcohol-positive group had mental disorders. This strongly suggests that a causal relationship exists between mental disorders and alcohol use, which strongly depresses the central nervous system. Moreover, the number of cases positive for methamphetamine was limited in the alcohol-positive group, similar to the results of previous studies. This is consistent with previous survey results showing that methamphetamine users do not use alcohol, and these two substances compete pharmacologically with each other.34
From these findings, a multidimensional analysis of alcohol use was performed with 3 factors, the socioenvironmental factor, the pharmacological factor, and the medical factor. As a medical factor, those from 60 to 70 years of age could work, and there were many of them in the alcohol-positive group. In the alcohol-positive group, there were many with liver and cardiac diseases as underlying diseases. From the perspective of the socioenvironmental factor, there were many accidents related to walking and involving motorcycles in the alcohol-positive group. From the pharmacological perspective, the use of psychotropic drugs to control mental symptoms caused by drinking or stimulants was considered. Overall, these results suggest that scientific evidence to reduce the risks of drinking can be accumulated by examining the characteristics of deaths related to drinking.
This study has some limitations. The normal human does not present with symptoms of alcohol poisoning at an ethanol level of 0.02 g/100mL of blood (0.2 mg/mL). In the present study, an ethanol level of 0.01 g/100mL of blood (0.1 mg/mL) was used as a cut-off based on an international standard.35 In addition, alcohol is known to be produced by an increase of postmortem microbiota. In postmortem toxicology, a blood alcohol concentration less than 0.1 mg/mL should be reported as negative.36 Furthermore, the items examined in this investigation were classified as medical, socioenvironmental, and pharmacological problems. However, within this classification, it was impossible to examine each problem separately. When examining the results, it was necessary to recognize that they overlapped.
Conclusion
As a medical factor, inability to take action caused by drinking may be the reason for deaths by accident and fire. As socioenvironmental problems, there were many traffic accident deaths after drinking. From a pharmacological perspective, the drinker often took other drugs. Social problems are caused by the medical factor, as various diseases develop due to drinking, and the medical and social factors include a pharmacological problem, which is the taking of other drugs.
Ethical Consideration
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The independent Ethics Committee at Osaka City University Graduate School of Medicine approved this study with informed consent from opt-out for the autopsy data analysis (Authorization No. 2001). The authors have confirmed that the data accessed complied with data protection and privacy regulations. All participant data has been anonymized, and privacy and confidentiality were ensured throughout the process of the study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare no conflicts of interest associated with this paper.
References
1. Gardner JD, Mouton AJ. Alcohol effects on cardiac function. Compr Physiol. 2015;5:791–802.
2. Mann RE, Smart RG, Govoni R. The epidemiology of alcoholic liver disease. Alcohol Res Health. 2003;27:209–219.
3. Irving HM, Samokhvalov AV, Rehm J. Alcohol as a risk factor for pancreatitis. A systematic review and meta-analysis. JOP. 2009;10:387–392.
4. Boffetta P, Hashibe M. Alcohol and cancer. Lancet Oncol. 2006;7:149–156. doi:10.1016/S1470-2045(06)70577-0
5. Boden JM, Fergusson DM. Alcohol and depression. Addiction. 2011;106:906–914. doi:10.1111/j.1360-0443.2010.03351.x
6. Fujita Y, Inoue K, Sakuta A, Seki N, Miyazawa T, Eguchi K. An epidemiological analysis of drunken driving accidents in Kagawa Prefecture - comparison of 1997–2000 and 2003–2006. J Forensic Leg Med. 2008;15:469–470. doi:10.1016/j.jflm.2008.03.004
7. Nakamura K, Tanaka A, Takano T. The social cost of alcohol abuse in Japan. J Stud Alcohol. 1993;54:618–625. doi:10.15288/jsa.1993.54.618
8. Sudhinaraset M, Wigglesworth C, Takeuchi DT. Social and cultural contexts of alcohol use: influences in a social-ecological framework. Alcohol Res. 2016;38:35–45.
9. National Health and Nutrition Survey 2018. [homepage on the Internet]. Government of Japan, portal site of official statistics of Japan. Available from: http://www.e-stat.go.jp.
10. Takatsu M. Kenshi Handbook.
11. Matsushita S, Higuchi S. [Alcohol-related disorders and suicide]. Seishin Shinkeigaku Zasshi. 2009;111:1191–1202. Japanese.
12. Ciraulo DA, Barnhill J. Pharmacokinetic mechanisms of ethanol-psychotropic drug interactions. NIDA Res Monogr. 1986;68:73–88.
13. Tani N, Ikeda T, Michiue T, Oritani S, Morioka F, Ishikawa T. Analysis of psychotropic drug-related deaths in south Osaka. Subst Abuse Rehabil. 2018;9:79–90. doi:10.2147/SAR.S163491
14. Kinoshita H, Ameno K, Jamal M. Ethanol, methanol, and toluene. Jpn J Forensic Pathol. 2009;15:37–44. Japanese.
15. Maeda H, Zhu BL, Ishikawa T, et al. Evaluation of post-mortem ethanol concentrations in pericardial fluid and bone marrow aspirate. Forensic Sci Int. 2006;161:141–143. doi:10.1016/j.forsciint.2006.01.016
16. Tominaga M, Michiue T, Oritani S, Ishikawa T, Maeda H. Evaluation of postmortem drug concentrations in bile compared with blood and urine in forensic autopsy cases. J Anal Toxicol. 2016;40:367–373. doi:10.1093/jat/bkw028
17. Winek CL, Wahba WW, Winek CL
18. Sadakane A, Gotoh T, Ishikawa S, Nakamura Y, Kayaba K. Amount and frequency of alcohol consumption and all-cause mortality in a Japanese population: the JMS Cohort Study. J Epidemiol. 2009;19:107–115. doi:10.2188/jea.JE20081003
19. Saito E, Inoue M, Sawada N, et al. Impact of alcohol intake and drinking patterns on mortality from all causes and major causes of death in a Japanese population. J Epidemiol. 2018;28:140–148. doi:10.2188/jea.JE20160200
20. Erol A, Ho AM, Winham SJ, Karpyak VM. Sex hormones in alcohol consumption: a systematic review of evidence. Addict Biol. 2019;24:157–169. doi:10.1111/adb.12589
21. Marmot MG, Rose G, Shipley MJ, Thomas BJ. Alcohol and mortality: a U-shaped curve. Lancet. 1981;1:580–583. doi:10.1016/S0140-6736(81)92032-8
22. Meade TW, Vickers MV, Thompson SG, Stirling Y, Haines AP, Miller GJ. Epidemiological characteristics of platelet aggregability. Br Med J. 1985;290:428–432. doi:10.1136/bmj.290.6466.428
23. Laug WE. Ethyl alcohol enhances plasminogen activator secretion by endothelial cells. JAMA. 1983;250:772–776. doi:10.1001/jama.1983.03340060050025
24. Ridker PM, Vaughan DE, Stampfer MJ, Glynn RJ, Hennekens CH. Association of moderate alcohol consumption and plasma concentration of endogenous tissue-type plasminogen activator. JAMA. 1994;272:929–933. doi:10.1001/jama.1994.03520120039028
25. Fraser GE, Anderson JT, Foster N, Goldberg R, Jacobs D, Blackburn H. The effect of alcohol on serum high density lipoprotein (HDL). A controlled experiment. Atherosclerosis. 1983;46:275–286. doi:10.1016/0021-9150(83)90178-8
26. Gaziano JM, Buring JE, Breslow JL, et al. Moderate alcohol intake, increased levels of high-density lipoprotein and its subfractions, and decreased risk of myocardial infarction. N Engl J Med. 1993;329:1829–1834. doi:10.1056/NEJM199312163292501
27. Renaud S, de Lorgeril M. Wine, alcohol, platelets, and the French paradox for coronary heart disease. Lancet. 1992;339(8808):1523–1526. doi:10.1016/0140-6736(92)91277-F
28. Klatsky AL, Friedman GD, Siegelaub AB, Gérard MJ. Alcohol consumption and blood pressure. Kaiser-permanente multiphasic health examination data. N Engl J Med. 1977;296(21):1194–1200. doi:10.1056/NEJM197705262962103
29. Intersalt Cooperative Research Group. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. BMJ. 1988;297:319–328. doi:10.1136/bmj.297.6644.319
30. Potter JF, Bannan LT, Beevers DG. Alcohol and hypertension. Br J Addict. 1984;79:365–372. doi:10.1111/j.1360-0443.1984.tb03882.x
31. Oscar-Berman M, Marinković K. Alcohol: effects on neurobehavioral functions and the brain. Neuropsychol Rev. 2007;17:239–257.
32. Miceli M, Alberti L, Bennardini F, et al. Effect of low doses of ethanol on platelet function in long-life abstainers and moderate-wine drinkers. Life Sci. 2003;73:1557–1566. doi:10.1016/S0024-3205(03)00473-9
33. Tanikawa A, Seki S, Yasuda T, Hasegawa E. Successful use of the two-tube approach for the treatment of phenobarbital poisoning without hemodialysis. Am J Emerg Med. 2019;37:
34. Tani N, Chen JH, Michiue T, Oritani S, Ishikawa T. [Retrospective investigation of psychostimulant-related fatalities in forensic autopsy during 10 years in the southern half of Osaka city and surrounding areas]. Jpn J Forensic Pathol. 2016;22:13–20. Japanese.
35. Dubowski KM. Alcohol determination in the clinical laboratory. Am J Clin Pathol. 1980;74:747–750. doi:10.1093/ajcp/74.5.747
36. Kugelberg FC, Jones AW. Interpreting results of ethanol analysis in postmortem specimens: a review of the literature. Forensic Sci Int. 2007;165:10–29.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.