Back to Journals » Advances in Medical Education and Practice » Volume 16
Problem-Based Learning and Case-Based Learning in Clinical Practical Teaching for Gynecology Residents: A Narrative Review
Authors Zhu Y, Zhang J, Fei J, Fang H, Zhang Z ![]()
Received 12 April 2025
Accepted for publication 18 July 2025
Published 23 July 2025 Volume 2025:16 Pages 1269—1279
DOI https://doi.org/10.2147/AMEP.S534053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Ying Zhu,* Jiaojiao Zhang,* Jing Fei, Huibin Fang, Zhigang Zhang
Department of Gynecology, The Second Affiliated Hospital, Zhejiang University School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhigang Zhang, Department of Gynecology, The Second Affiliated Hospital, Zhejiang University School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China, Email [email protected]
Background: Gynecology residency training necessitates a robust educational framework to cultivate clinical competency, critical thinking, and problem-solving skills. Traditional lecture-based teaching methods are deficient in fostering active learning and clinical decision-making. Problem-based learning (PBL) and case-based learning (CBL) have emerged as learner-centered approaches that enhance medical education by integrating theoretical knowledge with clinical practice. This review aims to explain the efficacy, implementation frameworks, challenges, and comparative value of PBL and CBL in gynecology residency education, and explores the role of instructional technology integration.
Methods: A systematic literature search was conducted across PubMed, ERIC, Scopus, Embase, and EBSCO (January 2010–January 2025) using keywords: “problem-based learning”, “case-based learning”, “gynecology education”, “residency training”. Inclusion criteria encompassed studies on PBL/CBL interventions in gynecology residency with qualitative/quantitative outcomes. Ten articles met the criteria after screening.
Results: Both PBL and CBL significantly outperform in enhancing clinical decision-making, differential diagnosis, knowledge retention, procedural planning, and long-term knowledge application. PBL utilizes open-ended problems to cultivate self-directed learning, critical thinking, and collaborative problem-solving (eg, managing complex AUB etiologies). CBL employs structured clinical cases to bridge theoretical knowledge with practical application, improving diagnostic reasoning and patient management skills. Key implementation frameworks involve careful pre-session preparation, facilitator-guided discussions on authentic cases, and structured feedback. Challenges include significant faculty time for case design/facilitation, resource intensity, and competency assessment. PBL fosters deep theoretical understanding, while CBL excels in clinical skill translation. Integrating both approaches creates a balanced curriculum. Augmenting PBL/CBL with simulation, flipped classrooms, mobile learning, and AI enhances accessibility, personalization, and procedural skill practice.
Conclusion: PBL and CBL are transformative pedagogical strategies for gynecology residency training, effectively developing competencies needed for complex clinical practice. Successful implementation requires rigorously designed cases, faculty trained in facilitative guidance, and strategic technology integration. These approaches prepare residents not only as skilled technicians but as adaptable, patient-centered practitioners capable of navigating evolving healthcare challenges. Investment in faculty development and technology-enhanced PBL/CBL models is crucial for advancing gynecologic education globally.
Keywords: problem-based learning, case-based learning, gynecology residency, medical education, clinical training, active learning, instructional technology
Background
The scientific rigour and practical nature of gynaecology as a secondary clinical discipline is well-established. It encompasses a wide spectrum of disease types, many of which can be challenging to differentiate, along with intricate physiological and pathological mechanisms. The complexity of these mechanisms and the high demand for professional expertise necessitate rigorous teaching requirements for gynaecology.1 For instance, the intricacies of numerous diseases associated with abnormal uterine bleeding (AUB) necessitate a profound level of comprehension, encompassing not only technical expertise but also the discernment and precise implementation of intricate mechanisms.2 Gynaecological residency training not only contributes to the development of highly skilled clinicians, but also improves the overall skills and service levels of the gynaecological healthcare team, ultimately driving the continued advancement of the specialty. Nonetheless, contemporary clinical teaching methodologies in the field of gynaecology remain predominantly reliant on conventional instructional approaches, predominantly comprising lecture-based learning.3,4 This pedagogical model entails the transmission of knowledge from the instructor to the students within a constrained timeframe in the classroom setting. The utilisation of this traditional teaching method is associated with several limitations, including diminished opportunities for student engagement and practical application. Furthermore, it poses significant challenges in fostering active learning and critical thinking skills.5 It is becoming increasingly apparent that lecture-based learning models are no longer adequate to meet the requirements of teaching gynaecology. In order to develop the ability to think independently and apply knowledge in clinical practice, modern education must emphasise student participation, interaction and practical experience.
In light of the limitations of traditional teaching models, a comprehensive investigation is being conducted into the evolution of teaching methodologies employed in gynaecology residency training programmes. This study focuses on two pioneering instructional approaches: problem-based learning (PBL) and case-based learning (CBL).6,7
These learner-centred methodologies, which are grounded in constructivist theory, address the identified lacuna by emulating authentic clinical scenarios. PBL is a pedagogical approach that prioritises autonomous learning by facilitating open-ended problem solving. Research has indicated that the PBL teaching mode enhances clinical practice and fosters collaborative learning among dental students.8 Conversely, CBL employs structured clinical cases to establish a contextual framework for knowledge acquisition. It has been demonstrated by preceding studies that CBL is a successful method for enhancing neurology residents’ understanding of and knowledge about professionalism.9 A recent study explored the effectiveness of a teaching model combining PBL and CBL in clinical teaching for fifth-year medical students specializing in clinical medicine, focusing on ectopic pregnancy.6 The findings indicated that the PBL-CBL approach outperformed traditional teaching methods in terms of learning motivation, comprehension ability, teacher-student interaction, communication skills, clinical reasoning ability, self-directed learning ability, knowledge retention, and course satisfaction. However, the application of PBL and CBL in the standardised training of gynaecological residents remains largely unexplored, with limited research on their application models and value. There is an urgent need for the development of teaching models that are consistent and well-defined, as well as value evaluations and research that integrates these emerging teaching methods. Consequently, the present review examines the efficacy, implementation frameworks, challenges, and comparative value of PBL and CBL in gynecology residency education, and explores the role of instructional technology integration.
Methods
Literature Search
A systematic literature search was conducted using the following electronic databases: PubMed, ERIC, Scopus, Embase and EBSCO. The search was conducted on January 16, 2025. And the comprehensive search strategy was employed by utilising boolean operators with keywords encompassing “problem-based learning”, “case-based learning”, “gynecology education” and “residency training”. All articles collected during the literature search were imported into EndNote, a standardized reference management software.
Inclusion Criteria
Two reviewers independently screened and applied inclusion criteria to the collected articles gathered from the literature search (JF and JJZ). Titles and abstracts were initially screened for the scope and relevance of the research aim. All discrepancies were resolved from team consensus. The inclusion criteria for the study were as follows: 1) Full text was provided, 2) Published between January 2010 to January 2025, 3) English, 4) involved qualitative, quantitative, or mixed methods study design, and 5) studies reporting PBL or CBL interventions in gynecologic residency training programs, qualitative or quantitative outcomes, and reviews that engage with pedagogical frameworks. Exclusion criteria included non-English articles and studies not related to clinical skills.
The initial search yielded 146 articles. Following this, the literature was screened, the rigorous screening process resulted in the inclusion of 10 articles10–19 (Figure 1 and Table 1), which will serve as the foundation for subsequent analysis and synthesis.
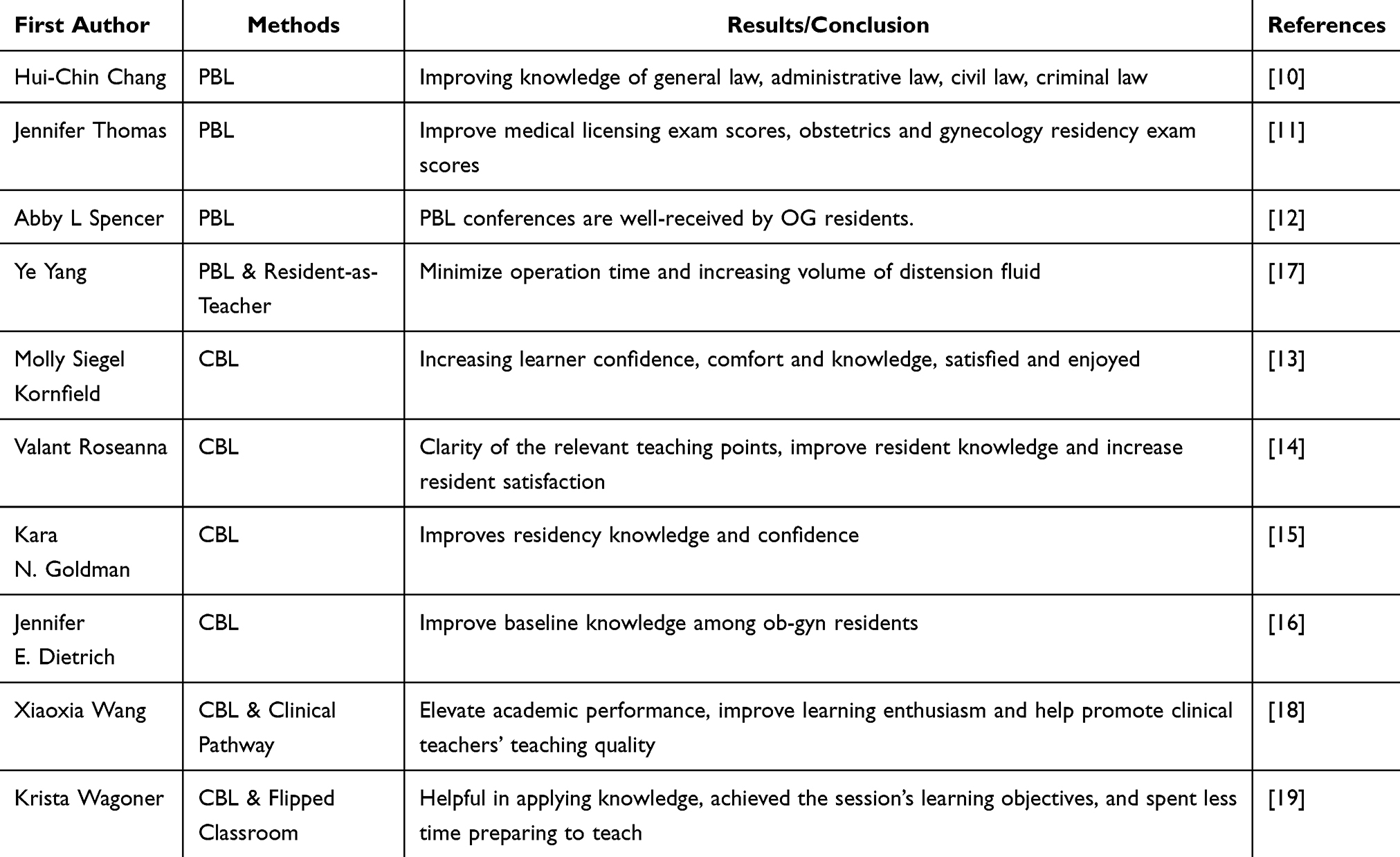 |
Table 1 Studies Assessing the Application of PBL and CBL in Gynecology Residency Programs, Including Educational Outcomes: Summarizes Research on PBL and CBL Methodologies in Gynecology Residency Training, Highlighting Improvements in Knowledge, Exam Performance, Learner Confidence, and Satisfaction |
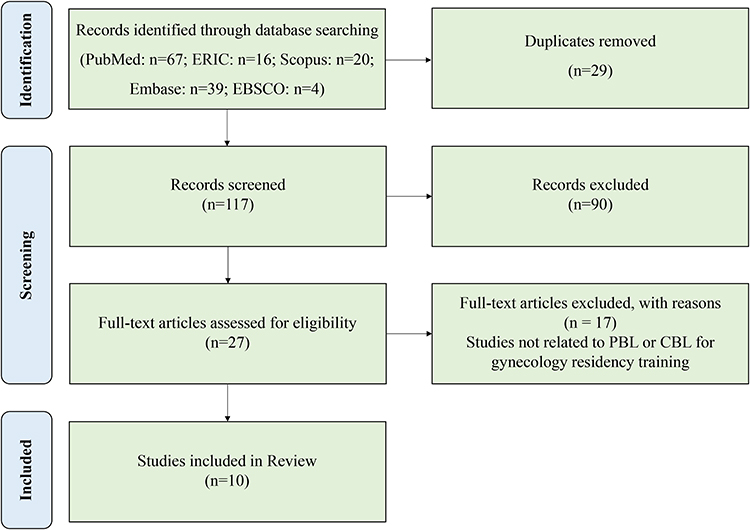 |
Figure 1 PRISMA flow diagram of the study. |
Data Extraction, Quality Assessment, and Analysis
Research data were extracted using Microsoft Excel. The extracted content included author, year, training population, teaching model, research results, and conclusions. Data extraction was performed by two researchers (JJZ or HBF). In case of discrepancies, the data were reviewed by the other researcher (ZGZ) to ensure accuracy and completeness.
PBL in Gynecology Residency Training
PBL is a student-centered teaching model that utilizes a variety of materials, including literature, monographs, and papers, to guide students in reviewing and discussing problems. This dynamic teaching strategy integrates theoretical knowledge with clinical practice, with the aim of developing students’ critical thinking and adaptive skills in gynecology residency training. By integrating authentic clinical scenarios with a collaborative learning environment, PBL prepares residents to address complex challenges in women’s health. PBL pedagogy fosters clinical thinking by enhancing students’ capacity to actively acquire knowledge and analyze problems. The model emphasizes faculty-designed questions that prompt faculty to pose relevant inquiries based on the syllabus and typical cases, thereby guiding students to acquire knowledge.
PBL Framework (eg Abnormal Uterine Bleeding) (Figure 2)
Pre-Instructional Phase
Instructor compiles educational materials (case studies, guidelines, literature), designs discussion questions, and outlines lesson structure. Learners (individually/in small groups) research AUB topics: pathophysiology, diagnostic criteria/tests, medical/surgical management, and clinical outcomes supported by current evidence.
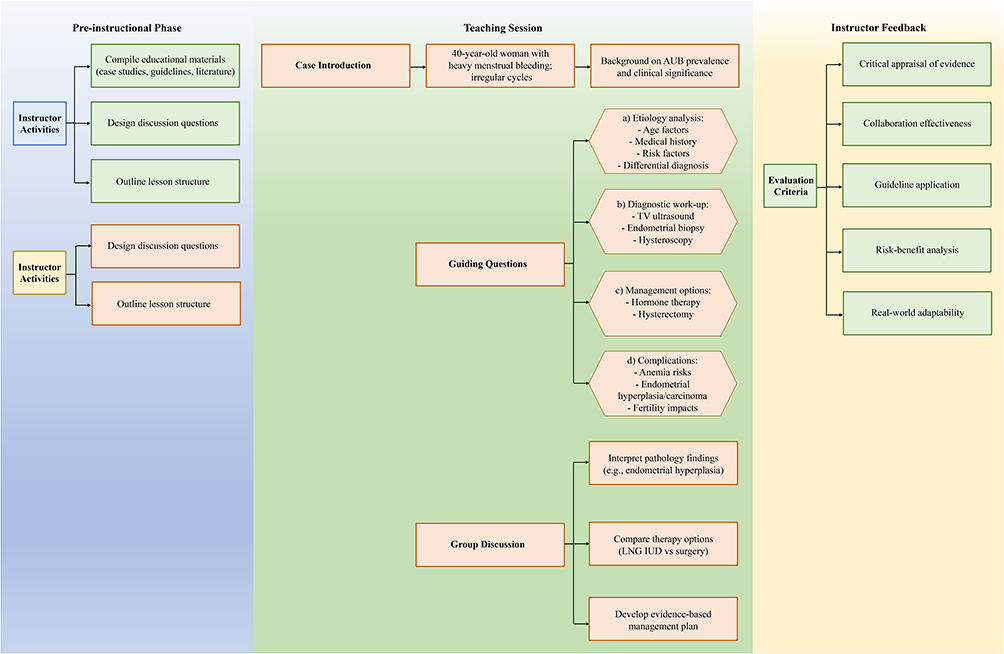 |
Figure 2 PBL framework for gynecology residents (eg abnormal uterine bleeding). |
Teaching Session
Case Introduction: A 40-year-old woman presents with heavy menstrual bleeding and irregular cycles. Background on the prevalence and clinical significance of AUB is provided.
Guiding questions: a) Etiology: How do age, medical history, and risk factors inform the differential diagnosis (eg, structural lesion vs ovulatory dysfunction?) b) Diagnostic work-up: Rationale for selection of tests (transvaginal ultrasound, endometrial biopsy, hysteroscopy). c) Management: Indications/risks of hormone therapy, or hysterectomy. d) Complications: Risks of anemia, endometrial hyperplasia/carcinoma, and effects on fertility.
Group Discussion: Learners propose evidence-based management plans that address: a) Interpretation of pathology findings (eg, endometrial hyperplasia). b) Personalized therapy selection (eg, LNG IUD vs surgery).
Instructor Feedback
Evaluates learners’ ability to critically appraise evidence, collaborate, and apply guidelines to clinical decisions. Emphasizes logical reasoning, risk-benefit analysis, and real-world adaptability.
Evidence of Efficacy
PBL has demonstrated its efficacy in gynecology residency training, as evidenced by educational research and clinical outcomes. Studies have highlighted its impact on knowledge retention, clinical reasoning, and skill acquisition in comparison to traditional lecture-based methods. The implementation of PBL in various disciplines has been shown to enhance clinical competence and decision-making abilities. A study by Tullius et al examined the impact of PBL in obstetrics and gynecology residency on interdisciplinary communication, critical thinking, and collaboration. Furthermore, from the students’ perspective, PBL has been found to increase interest and satisfaction in learning.
Challenges
While PBL offers significant benefits, its implementation in gynecology residency programs faces several challenges. First, designing high-quality, multidimensional cases that balance complexity with educational objectives requires substantial time and expertise. Second, facilitator training is critical; inexperienced mentors may struggle to guide discussions effectively, leading to superficial analyses or missed learning opportunities. Third, time constraints in busy clinical environments limit dedicated PBL sessions, risking inconsistent participation or rushed deliberations. Finally, the assessment of competency in PBL remains subjective, as traditional metrics may not fully capture nuanced skills such as collaborative decision-making or empathy.
CBL in Gynecology Residency Training
Case-Based Learning (CBL) is a novel teaching method that is centered on “case-oriented, problem-based, student-oriented, and teacher-led” principles. A significant number of teaching hospitals are progressively incorporating the CBL teaching method into their obstetrics and gynecology curricula. This approach utilizes authentic case studies to enhance students’ comprehension of diseases, refine their comprehensive analysis of clinical scenarios, and cultivate a profound understanding of the clinical manifestations, diagnosis, and differential diagnosis of diseases. Furthermore, it fosters the development of independent clinical thinking skills among students.
CBL Framework (eg Abnormal Uterine Bleeding) (Figure 3)
Pre-Instructional Phase
In order to facilitate a comprehensive differential diagnosis, teachers must first clarify their teaching objectives and select typical cases that are representative of the common etiologies associated with multiple AUBs. To illustrate, a case of a 40-year-old woman with both a structural etiology, such as fibroids, and a nonstructural etiology, such as a hormonal imbalance, would be a suitable example. Another case may involve a postmenopausal woman with heavy bleeding, which may suggest endometrial cancer. Students are required to read the literature related to AUB, including etiology, diagnostic approaches, treatment options, and management strategies. In particular, the most recent clinical guidelines and retrospective studies will help them understand the common causes of AUB (eg, fibroids, endometrial hyperplasia, endometrial cancer, etc.)
 |
Figure 3 CBL framework for gynecology residents (eg abnormal uterine bleeding). |
Teaching Session
Case Introduction: Woman presents with irregular menstrual cycles and heavy bleeding for the past six months. Introduce AUB as the overarching clinical topic. Briefly explain that AUB encompasses a variety of causes, ranging from benign conditions like fibroids and polyps to more serious conditions such as endometrial cancer. Clarify that the learners will focus on understanding the diagnosis, differential diagnosis, and management of AUB.
Prompt Initial Questions: Encourage learners to think about the following questions ahead of the case discussion: What are the common causes of AUB in women of reproductive age? How would you approach the differential diagnosis of AUB in a patient like the one described? What diagnostic steps would you take first in evaluating a case of AUB? Clarify Roles and Expectations: If students are working in groups, clarify the roles each member will play (eg, leader, recorder, presenter). Set expectations for collaboration, including active participation and respect for diverse opinions.
Group Discussion and Clinical Decision-Making: Allow the group to discuss their findings, diagnostic steps, and management plans. Encourage students to justify their decisions with evidence-based guidelines or literature. Guide the discussion to ensure comprehensive coverage of relevant topics and steer learners toward evidence-based conclusions. Resolve the case by discussing the final diagnosis (eg, fibroids causing AUB) and the recommended management plan (eg, medical management with progesterone or surgical intervention). Reflect on the case to reinforce key learning points, such as the importance of considering a broad differential diagnosis and tailoring management to individual patient needs.
Instructor Feedback
Assess how well learners interpreted clinical data, formulated a differential diagnosis, and justified their management choices. Ask students to reflect on their approach to this case and consider how they would apply these skills to future cases of AUB or similar clinical situations.
Evidence of Efficacy
CBL has been demonstrated to be an effective pedagogical tool for promoting clinical reasoning and diagnostic skills, particularly in complex cases, and for enhancing residents’ clinical competence and patient management skills. It has been shown to significantly increase satisfaction with learning, improve long-term memory, and facilitate the application of knowledge regarding gynecologic disorders. Additionally, CBL has been shown to promote teamwork and communication skills.
Challenges
CBL necessitates a considerable investment of time, encompassing preparation, case development, and discussion. This commitment is further compounded by the existing demands on residents and faculty, who are already encumbered by extensive clinical and didactic schedules within the context of their demanding residency training programs. To ensure the effective facilitation of CBL, instructors must possess not only clinical expertise but also the competencies to guide discussions, facilitate critical thinking, and manage group dynamics. The active engagement of residents in case discussions is paramount to the efficacy of CBL. However, some residents may experience discomfort in participating, particularly if they lack confidence in their knowledge or find the case too complex. It is imperative to design cases that are appropriately challenging and relevant to the resident’s level of training, as cases that are too simple or too advanced may not offer a conducive learning experience.
Comparative Analysis of PBL and CBL
PBL and CBL are two important pedagogical approaches to gynecology residency training, each with its own unique strengths and challenges (Table 2). PBL is a method of instruction that emphasizes critical thinking and independent learning by encouraging residents to work in groups to solve complex clinical problems. It enhances problem-solving skills, but requires significant time for preparation and instruction and can be resource intensive. Conversely, CBL emphasizes the application of theoretical knowledge to real-world clinical scenarios, fostering the development of clinical decision-making and practical skills. However, the quality and diversity of available cases may constrain the efficacy of this approach. PBL fosters profound learning and theoretical comprehension, while CBL is more directly associated with enhanced clinical proficiency. The success of both approaches hinges on the expertise of the instructors and the meticulous design of the curriculum. While PBL offers a more expansive and adaptable educational experience, CBL focuses on experiential learning, providing a more immersive and practical training environment. The integration of these two methodologies can create a balanced educational experience, catering to the necessity of theoretical knowledge and hands-on clinical experience in gynecology residency training.
 |
Table 2 Advantages and Disadvantages of PBL and CBL in the Context of Gynecology Residency Education: Summarizes the Key Strengths and Limitations of PBL and CBL Methodologies as Applied to Gynecology Residency Training, Focusing on Aspects Such as Self-Directed Learning, Clinical Reasoning, Collaboration, and Practical Challenges |
Instructional Technology Integration and Innovation in Gynecology Residency Training
The integration of instructional technology into gynecology residency training represents a significant advancement, improving the quality and efficiency of medical education. By utilizing innovative technologies, residency programs can enhance learning experiences, bridge knowledge gaps, and better prepare residents for real-world clinical scenarios. The following are some key approaches and innovations in the integration of instructional technology:
Simulation-Based Learning
Simulation technologies, including high-fidelity mannequins, virtual reality (VR), and augmented reality (AR), provide immersive and risk-free environments for residents to practice clinical skills and procedures, such as laparoscopic surgery or obstetric management. Simulation helps develop technical skills, decision-making, and teamwork in a controlled setting without putting patients at risk. It allows for repeated practice and exposure to rare or complex cases that residents may not encounter frequently.20,21
Flipped Classroom Model
The flipped classroom model involves residents learning theoretical content outside of class via online modules, lectures, or reading materials. In-class time is then used for active learning, such as case discussions, group problem-solving, and hands-on practice. This model allows for more interactive, focused, and personalized learning during class time. It can enhance residents’ problem-solving skills and encourage deeper engagement with the material.22,23
Mobile Learning (mLearning)
mLearning involves the use of mobile devices (smartphones, tablets) to access educational content, such as videos, articles, and quizzes, anytime and anywhere. This method offers flexibility and convenience, allowing residents to access learning materials on-the-go, improving knowledge retention, and enabling just-in-time learning.24,25
Artificial Intelligence (AI) and Machine Learning
AI can be used to create adaptive learning systems that personalize education based on residents’ progress. Machine learning algorithms can also help analyze clinical data, identify patterns in patient care, and improve diagnostic accuracy. AI-powered platforms provide tailored learning experiences for residents, enabling them to focus on areas where they need improvement. It also enhances decision-making by providing evidence-based recommendations and identifying subtle clinical patterns.26,27
The integration of instructional technology and innovation in gynecology residency training has the potential to significantly enhance learning outcomes, improve clinical skills, and provide residents with a comprehensive education. Technologies such as simulation, virtual patient encounters, mobile learning, AI, and data analytics offer diverse, flexible, and personalized approaches to residency education, bridging the gap between theoretical knowledge and clinical application. The combined use of these tools in conjunction with traditional educational methods, like PBL and CBL, creates a dynamic and effective learning environment for future gynecologists.
Discussion
This review constitutes the inaugural comprehensive study to explore the application of PBL and CBL in gynecology residency education. Utilising the term “abnormal uterine bleeding” as a case study, the review outlines educational modules and evaluates the value, challenges, and comparative differences of these two teaching models based on a comprehensive review of the extant literature. Furthermore, the study systematically analyses the application value of combining PBL and CBL with other emerging teaching models in gynaecology residency training.
PBL and CBL represent transformative paradigms in gynecology residency education, aligning pedagogical strategies with the dynamic, multifaceted demands of clinical practice. PBL fosters self-directed learning and critical thinking by immersing trainees in authentic, open-ended problems, while CBL bridges theoretical knowledge and clinical application through structured, patient-centered scenarios. Together, these approaches cultivate competencies in differential diagnosis, procedural planning, and interdisciplinary collaboration—skills essential for managing conditions ranging from routine obstetric emergencies to complex oncologic cases.
The integration of PBL and CBL into residency curricula addresses longstanding gaps in traditional didactic models, particularly in nurturing adaptability and resilience amidst clinical uncertainty. However, their success hinges on deliberate implementation: faculty must be equipped to facilitate rather than direct learning, cases must evolve to reflect emerging challenges (eg, telemedicine, health equity), and assessments should prioritize competency milestones over rote knowledge. While challenges such as resource constraints and facilitator training persist, innovations like AI-generated cases, virtual simulations, and global health-oriented adaptations offer scalable solutions.
Ultimately, the value of PBL and CBL lies in their capacity to prepare gynecologists not merely as technicians but as thoughtful, patient-centered practitioners. By embedding iterative problem-solving into training, these methods empower residents to navigate evolving medical landscapes, advocate for vulnerable populations, and lead multidisciplinary teams. Institutions must champion these approaches through sustained investment in faculty development, technology integration, and outcome-driven curricular reform. The future of obstetrics and gynecology education will be defined by its ability to balance innovation with evidence, ensuring trainees graduate not only competent but confident in their capacity to transform women’s health care globally.
Conclusion
Based on the systematic review, PBL and CBL significantly outperform traditional teaching in gynecology residency training, enhancing clinical decision-making, differential diagnosis, and practical skills. PBL cultivates self-directed learning and critical thinking through open-ended problem-solving, while CBL bridges theoretical knowledge and clinical application via structured cases. Their integration balances deep analytical engagement with procedural proficiency. Successful implementation hinges on three pillars: rigorously designed authentic cases, faculty trained in facilitative guidance, and technology augmentation (eg, simulation/AI tools). Together, these approaches develop globally competent gynecologists equipped to navigate complexity with humanistic care, establishing them as core drivers of transformative specialty education.
Ethics Approval and Consent to Participate
An ethics statement is not applicable because this study is based exclusively on published literature. The selection of articles has been based on a scientific search strategy and is free from bias.
Funding
This study was supported by 2023 Teaching reform research and cultivation project of The Second Affiliated Hospital of Zhejiang University School of Medicine (20230203).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Recker F, Scheele F. Editorial: education in obstetrics and gynecology. Front Med. 2024;11:1490673. doi:10.3389/fmed.2024.1490673
2. Marnach ML, Laughlin-Tommaso SK. Evaluation and management of abnormal uterine bleeding. Mayo Clin Proc. 2019;94(2):326–335. doi:10.1016/j.mayocp.2018.12.012
3. Royce CS, Morgan HK, Baecher-Lind L, et al. The time is now: addressing implicit bias in obstetrics and gynecology education. Am J Obstet Gynecol. 2023;228(4):369–381. doi:10.1016/j.ajog.2022.12.016
4. Harris E. Online abortion care training now available for ob-gyn residents. JAMA. 2023;330(10):905. doi:10.1001/jama.2023.15445
5. Zhang SL, Ren SJ, Zhu DM, et al. Which novel teaching strategy is most recommended in medical education? A systematic review and network meta-analysis. BMC Med Educ. 2024;24(1):1342. doi:10.1186/s12909-024-06291-4
6. Xie W, Li Y, Liu X. Application of problem-based learning and case-based learning in teaching ectopic pregnancy to fifth-year medical students. BMC Med Educ. 2024;24(1):1346. doi:10.1186/s12909-024-06327-9
7. Shang Y, Cao KF, Yue JY, et al. Comparative effectiveness of various teaching modes, including PBL, CBL, and CTTM in paediatric medical education with combined online and offline approaches. BMC Med Educ. 2025;25(1):8. doi:10.1186/s12909-024-06267-4
8. Bai X, Zhang X, Wang X, Lu L, Liu Q, Zhou Q. Follow-up assessment of problem-based learning in dental alveolar surgery education: a pilot trial. Int Dent J. 2017;67(3):180–185. doi:10.1111/idj.12275
9. Alrawdhan N, Althubaiti A, Alzahem A, Alqahtani S, Baarmah D, Alrumayyan A. Cultivating professionalism in Saudi Arabian neurology residency programs: the impact of case-based learning. Adv Med Educ Pract. 2025;16:287–295. doi:10.2147/AMEP.S499212
10. Chang HC, Wang NY, Ko WR, Yu YT, Lin LY, Tsai HF. The effectiveness of clinical problem-based learning model of medico-jurisprudence education on general law knowledge for Obstetrics/Gynecological interns. Taiwan J Obstet Gynecol. 2017;56(3):325–330. doi:10.1016/j.tjog.2017.04.011
11. Jennifer Thomas TA, Kamikawa G, Kaneshiro B, Kaneshiro B. Problem based learning and academic performance in residency. Hawaii Med J. 2009;68(10):246–248.
12. Spencer AL, McNeil M. Interdisciplinary curriculum to train internal medicine and obstetrics gynecology residents in ambulatory women’s health: adapting problem based learning to residency education. J Women’s Health. 2009;18(9):1369–1375. doi:10.1089/jwh.2008.1253
13. Kornfield MS, Rubin E, Parker P, et al. Strengthening the reproductive endocrinology and infertility curriculum through three interactive cases. MedEdPORTAL. 2023;19:11375. doi:10.15766/mep_2374-8265.11375
14. Valant R, Grigorescu B, Benerofe S, Lazarou G. Improved understanding of female pelvic medicine and reconstructive surgery concepts through targeted case-based educational intervention: a pilot study. Female Pelvic Med Reconstr Surg. 2020;26(12):723–725. doi:10.1097/SPV.0000000000000691
15. Goldman KN, Tiegs AW, Uquillas K, et al. Interactive case-based learning improves resident knowledge and confidence in reproductive endocrinology and infertility(). Gynecol Endocrinol. 2017;33(6):496–499. doi:10.1080/09513590.2017.1290075
16. Dietrich JE, De Silva NK, Young AE. Reliability study for pediatric and adolescent gynecology case-based learning in resident education. J Pediatr Adolesc Gynecol. 2010;23(2):102–106. doi:10.1016/j.jpag.2009.09.002
17. Yang Y, Li LY, Sang LW, et al. An observation of a resident-as-teacher combined with tutor guided hysteroscopy teaching program for standardized residency training (SRT) in obstetrics and gynecology. J Healthc Eng. 2020;2020:8855099. doi:10.1155/2020/8855099
18. Wang X, Che X, Tang X, Xu Z. Application of combined teaching method of case-based-learning and clinical pathway in practical gynecological teaching. PeerJ. 2024;12:e17813. doi:10.7717/peerj.17813
19. Wagoner K, Dempsey A, Dunn F, Hemphill A. Normal pregnancy care and physiology and select pregnancy complications: a flipped classroom case for the OB/GYN clerkship. MedEdPORTAL. 2024;20:11413. doi:10.15766/mep_2374-8265.11413
20. He Y, Wang Z, Sun N, et al. Enhancing medical education for undergraduates: integrating virtual reality and case-based learning for shoulder joint. BMC Med Educ. 2024;24(1):1103. doi:10.1186/s12909-024-06103-9
21. Ma L, Yan R, Wang X, et al. Enhancing surgical nursing student performance: comparative study of simulation-based learning and problem-based learning. J Multidiscip Healthc. 2024;17:991–1005. doi:10.2147/JMDH.S440333
22. de Jong N, van Rosmalen P, Brancaccio MT, Bleijlevens MHC, Verbeek H, Peeters IGP. Flipped classroom formats in a problem-based learning course: experiences of first-year bachelor European public health students. Public Health Rev. 2022;43:1604795. doi:10.3389/phrs.2022.1604795
23. Wagoner K, Dempsey A, Wade J, Dunn F. Evaluation and management of early pregnancy: a flipped classroom case for OB/GYN clerkship students. MedEdPORTAL. 2023;19:11297. doi:10.15766/mep_2374-8265.11297
24. Hamad F, AlMuhaissen S, Urquhart C, Tarawneh R, Asaad M, Abu-Ajamieh M. Attitudes and perceptions of health schools’ students toward mobile learning: a cross-sectional study. BMC Med Educ. 2024;24(1):1558. doi:10.1186/s12909-024-06394-y
25. Yalcinkaya T, Cinar yucel S. Mobile learning in nursing education: a bibliometric analysis and visualization. Nurse Educ Pract. 2023;71:103714. doi:10.1016/j.nepr.2023.103714
26. Popenici SAD, Kerr S. Exploring the impact of artificial intelligence on teaching and learning in higher education. Res Pract Technol Enhanc Learn. 2017;12(1). doi:10.1186/s41039-017-0062-8
27. Naseer MA, Saeed S, Afzal A, Ali S, Malik MGR. Navigating the integration of artificial intelligence in the medical education curriculum: a mixed-methods study exploring the perspectives of medical students and faculty in Pakistan. BMC Med Educ. 2025;25(1):273. doi:10.1186/s12909-024-06552-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Facilitating Active Collaborative Learning in Medical Education; a Literature Review of Peer Instruction Method
Fakoya AOJ, Ndrio M, McCarthy KJ
Advances in Medical Education and Practice 2023, 14:1087-1099
Published Date: 3 October 2023
A Comparison of the Academic Achievement at the End of the Medicine Undergraduate Degree Program Between Students Who Only Used the University Admission Test and Those Who Used the University Admission Test Plus Marks from the High School National Exam (ENEM) at a Single Brazilian Center
Bestetti RB, Durand MT, Couto LB, Faria-Jr M, Fumagalli HF, Silva VMR, Romão GS, Furlan-Daniel R, Garcia ME, Ferri SMN, Reis ACS, Jorge-Neto SD, Geleilete TJM
Advances in Medical Education and Practice 2023, 14:1185-1190
Published Date: 21 October 2023
Pathology as a Basic Medical Subject: Its Relevance and Application During Clinical Practice in Jordanian MD Programs, Interns’ and Residents’ Perspectives
Al-Saghbini MS, Fayyad MA, Gharaibeh L
Advances in Medical Education and Practice 2024, 15:627-635
Published Date: 4 July 2024
Artificial Intelligence in Medical Education: Promise, Pitfalls, and Practical Pathways
Saroha S
Advances in Medical Education and Practice 2025, 16:1039-1046
Published Date: 14 June 2025
Student Perceptions and Effectiveness of Video-Based Flipped Classroom for Improving Medical Physiology Teaching at AUSOM
Kottath Veetil P, Kollukkad Mani M, Arja SB, Paramban S, Kattambally PA, Fatteh R, Arja SB
Advances in Medical Education and Practice 2025, 16:1159-1167
Published Date: 3 July 2025