Back to Journals » Clinical Ophthalmology » Volume 20
Prism Success in Patients with Diplopia and Retinal Pathology
Authors Tadross M, Cavuoto KM, Falcone MM
Received 3 February 2026
Accepted for publication 21 April 2026
Published 3 June 2026 Volume 2026:20 586726
DOI https://doi.org/10.2147/OPTH.S586726
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Mariam Tadross, Kara M Cavuoto, Michelle M Falcone
Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA
Correspondence: Michelle M Falcone, Bascom Palmer Eye Institute, 7101 Fairway Dr, Palm Beach Gardens, FL, 33418, USA, Email [email protected]
Purpose: To evaluate the effectiveness of prisms in treating binocular diplopia in patients with retinal pathologies and to evaluate factors associated with treatment success.
Methods: A retrospective chart review was conducted on patients ≥ 18 years with binocular diplopia and retinal pathology presenting between 2012– 2022. Patients prescribed prisms with ≥ 1 follow-up were included. Subjective prism prescriptions were compared to measured deviations. Associations between treatment success and clinical factors were analyzed.
Results: Seventy patients (mean age 73.5 ± 8.6 years) were included, most with epiretinal membranes (54.3%) or prior retinal detachment (14.3%). Diplopia was eliminated in 65.7% of patients with prisms, though 43.5% of these patients required at least 1 prism change. For horizontal deviations, prescribed prisms were lower than measured deviations at both distance (Mean = 3.39 ± 4.23 PD vs. 5.33 ± 6.03 PD, p < 0.001) and near (Mean =1.99 ± 2.35 PD vs. 4.30 ± 6.05 PD, p =0.005). Vertical prism prescriptions were similar to measured deviations at distance (Mean = 2.34 ± 2.96 PD vs. 2.04 ± 2.37 PD, p =0.128), but higher at near (Mean = 1.99 ± 2.35 PD vs. 1.26 ± 2.47 PD, p =0.006). No significant associations were found between treatment success and type of retinal pathology, visual acuity, age, or prism type (Fresnel or ground-in) (all p > 0.05).
Conclusion: Prisms effectively eliminated diplopia in most patients, though adjustments were frequently necessary. Discrepancies between measured and subjectively preferred prism magnitudes highlight the importance of careful, individualized prism trials.
Keywords: prisms, binocular diplopia, diplopia, retinal pathology
Introduction
Patients with retinal pathologies, including epiretinal membrane, macular hole, and macular edema, may develop diplopia and/or strabismus that is related or unrelated to their underlying retinal condition. Evaluating this patient population can pose a challenge due to decreased visual acuity and visual distortion, decreased fusional amplitudes, and monocular diplopia. These factors can also make treating patients with retinal pathology and diplopia challenging.
Diplopia in patients with macular pathologies can stem from binocular misregistration where the distorted image from the affected eye competes with the fellow eye’s image resulting in central-peripheral rivalry-type (CPR-type) diplopia.1 Previous studies have highlighted that CPR-type diplopia occurs in 16% of patients with epiretinal membranes (ERM), and have identified retinal misregistration as the primary mechanism of diplopia in patients with ERMs.1,2 There is data to support that surgical intervention to remove ERMs not only improved diplopia for patients, but also improved retinal misregistration.3 Further research, however, has not explored the success of surgical intervention for alleviating diplopia in other retinal pathologies.
Apart from surgical intervention, prisms are a noninvasive option commonly used for treatment of symptomatic binocular diplopia. The research on prism use for alleviating binocular diplopia in patients with retinal pathologies, however, has been limited and yielded variable effectiveness.4–7 One discrepancy in previous studies has been a lack of use of both objective clinical data and subjective participant feedback to make conclusions about treatment effectiveness. One study in particular tested the success of incorporated and loose prisms, Bangerter filters, translucent tape, iseikonic manipulation, Fresnel prisms, and ERM peeling for patients with CPR-type diplopia who had retinal disease and found the most success with Fresnel prisms in these patients based on a subjective questionnaire following treatment.8 With the unique considerations that must be made to tailor treatment for patients with retinal pathologies, using both measured and subjective types of data to assess treatment success may be pertinent.
We conducted a retrospective review of patients with binocular diplopia and retinal pathologies to evaluate the success of prisms in treating diplopia in patients with retinal pathology and to assess for variables associated with increased likelihood for treatment success. Subjective data on patient-reported diplopia, the amount of prism prescribed based on patient preference, and the amount of prism necessary to eliminate diplopia were collected and compared to objective data on the magnitude of strabismus measured in clinic, which to our knowledge, has not been assessed in prior studies.
Methods
The study received institutional review board approval by the University of Miami Institutional Review Board and adhered to the tenets of the Declaration of Helsinki. A retrospective chart review was conducted for patients who presented to Bascom Palmer Eye Institute between 1/1/2012 and 12/31/2022. Patients were included if they were 18 years or older, had binocular diplopia, and had a history of unilateral retinal pathology including macular hole, epiretinal membrane, macular edema, or prior retinal detachment. Patients with a history of retinal detachment were only included if the macula was involved or if they had other macular pathology. Patients who were prescribed prisms and had at least 1 follow up visit after they were prescribed were included. Patients were excluded if they had no retinal pathology, bilateral retinal pathology, inability to provide reliable subjective data regarding diplopia symptoms, inability to undergo sensorimotor testing by cover/alternate cover due to poor vision, a neurological condition that could otherwise explain their diplopia, prior strabismus surgery, diplopia presumed to be secondary to a scleral buckle (i.e. underlying mechanical or restrictive cause), or were prescribed a Fresnel prism at an angle due to the variability of quantifying how much prism they were receiving at the horizontal and vertical axes.
Ocular alignment was assessed using standard sensorimotor examination techniques. Objective measurement of strabismus was performed using cover–uncover and alternate cover testing at both distance and near fixation, with prism neutralization to quantify the magnitude of deviation in prism diopters (PD). Measurements in primary gaze were used for this study. Diplopia was assessed subjectively through patient report during testing, including identification of diplopia presence and direction. The amount of prism required to eliminate diplopia was determined using prism trial in free space or in a trial frame, with adjustments made based on patient feedback until single binocular vision was achieved.
Continuous variables were compared using two-tailed paired t-tests when assessing differences between measured deviations and prescribed prism values within the same patients, and independent t-tests when comparing continuous variables between independent groups (e.g., patients with versus without diplopia resolution). Categorical variables, such as type of prism used or retinal pathology type, were compared using two-tailed chi-square tests. Effect sizes were calculated as Cohen’s d for t-tests and Cramer’s V for chi-square analyses. Statistical significance was defined at p <0.05. All analyses were completed in SPSS (IBM Corp., Chicago, Illinois, 2021).
Results
A total of 70 patients (51.4% male) with a mean age of 73.5 ± 8.6 years met the inclusion criteria. The retinal pathologies of the patients are summarized in Table 1. The most common pathologies were epiretinal membrane (54.3%) and prior retinal detachment (14.3%). Patients with multiple retinal pathologies comprised 17.1% of the cohort. The median baseline visual acuity of the eyes affected by the retinal pathology was .18 LogMAR (20/30 Snellen equivalent), [range: 0 to 1.6 logMAR (20/20 to 20/800 Snellen equivalent)]. Monocular distortion was reported in 30.0% of patients. Most patients (44.3%) had combined vertical and horizontal strabismus, whereas 37.1% had only horizontal strabismus and 18.6% had only vertical strabismus. Further details regarding the specific types of deviations are summarized in Table 2.
 |
Table 1 Retinal Pathologies Among Study Participants |
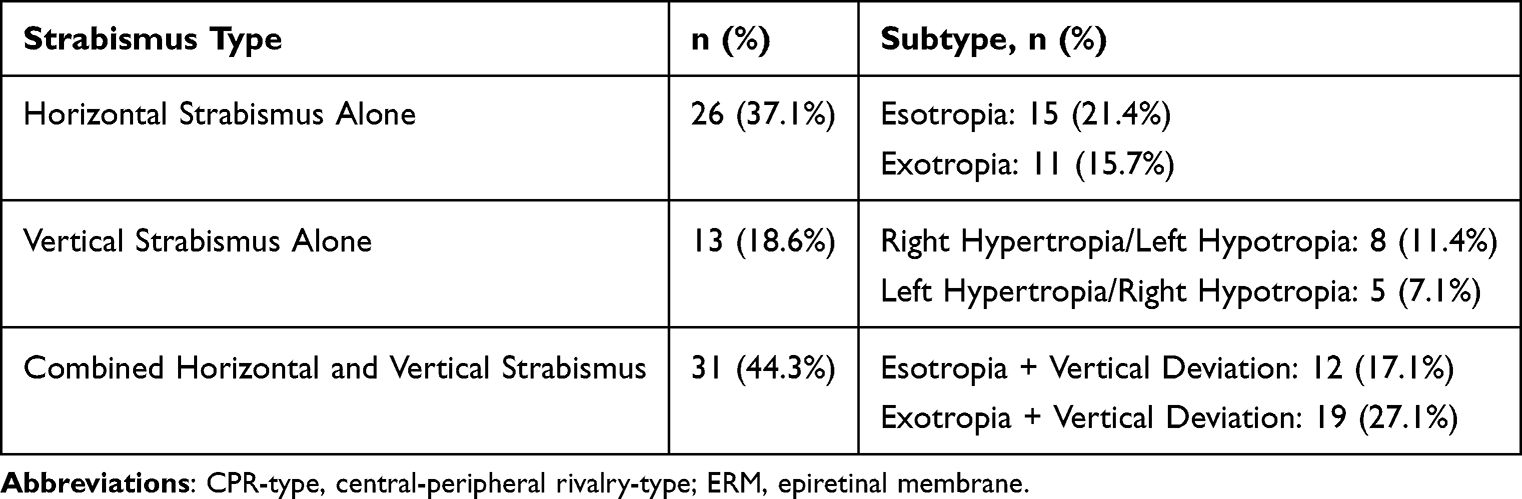 |
Table 2 Characteristics of Strabismus Among Study Participants (N = 70) |
All patients (n = 70) were prescribed prisms, of which 16 (22.9%) received a Fresnel prism. 26 patients (37.1%) had resolution of diplopia at the first follow-up with the initial prism prescription. Nearly two-thirds (65.7%, n= 46/70) had their diplopia eliminated with any prism prescription, with 43.5% (n= 20/46) of those who had diplopia eliminated requiring at least 1 prism prescription change. The number of prescription changes necessary to alleviate diplopia in patients whose initial prescription did not work ranged from 1–4 with an average of 1.4. Only one patient included in the study underwent subsequent strabismus surgery and did not require post-operative prisms as diplopia was eliminated. The remainder of the patients (34.3%) were not able to achieve resolution of diplopia with any prism prescription.
The discrepancy between the measured deviation in primary gaze and the amount of prism prescribed based on subjective patient feedback was assessed using paired t-tests, and the distribution of these differences for horizontal and vertical deviations at both distance and near is shown in Figures 1a–d. For patients with combined horizontal and vertical strabismus, the magnitude of the horizontal and vertical deviation was recorded and combined with those who had horizontal-only and vertical-only deviations for this part of the data analysis (n = 57 horizontal deviations, n = 44 vertical deviations). For vertical deviations at distance, no significant difference was found between the measured deviation (Mean = 2.34 ± 2.96 PD) and the prescribed vertical prism (Mean = 2.04 ± 2.37 PD) (paired t-test, p =0.128, Cohen’s d = 0.11). At near, patients required significantly more vertical prism prescribed (Mean = 1.99 ± 2.35 PD) than what was measured in primary gaze (Mean = 1.26 ± 2.47 PD) (paired t-test, p =0.006, Cohen’s d = 0.30). For horizontal deviations at distance, however, patients required significantly less prism prescribed (Mean = 3.39 ± 4.23 PD) than the deviation measured in primary gaze (Mean = 5.33 ± 6.03 PD) (paired t-test, p <0.001, Cohen’s d = 0.37). A similar trend was found for horizontal deviations at near with the amount of prescribed prism being significantly lower than the measured deviation (1.99 ± 2.35 PD vs. 4.30 ± 6.05 PD) (paired t-test, p =0.005, Cohen’s d = 0.49). No consistent pattern in these differences was identified based on the type of strabismus (vertical-only, horizontal-only, or combined horizontal and vertical deviations).
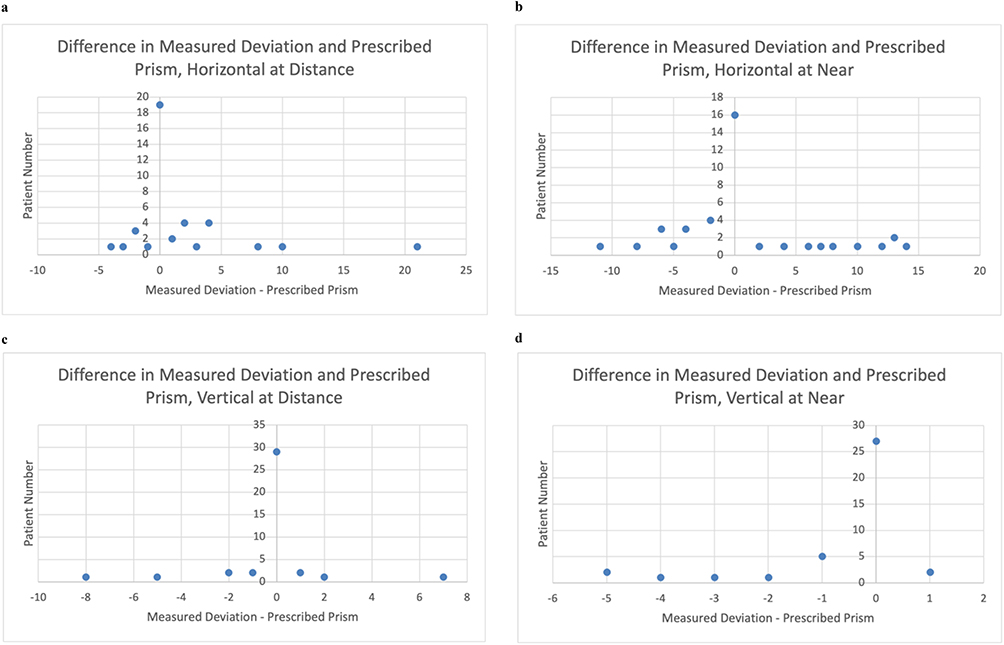 |
Figure 1 (a) The difference of measured deviation and prescribed prism in patients with horizontal deviations at distance, range: [−4, 21]. (b) The difference of measured deviation and prescribed prism in patients with horizontal deviations at near, range: [−12, 14]. (c) The difference of measured deviation and prescribed prism in patients with vertical deviations at distance, range: [−8, 7]. (d) The difference of measured deviation and prescribed prism in patients with vertical deviations at near, range: [−5, 1]. |
Multiple factors were evaluated to assess for an association with the ability to have diplopia eliminated at follow-up with prism glasses. The type of retinal pathology (chi-square test, p =0.055), baseline visual acuity (independent t-test, p =0.280, Cohen’s d = 0.18), age at presentation (independent t-test, p =0.567, Cohen’s d = 0.10), or type of prism prescribed (Fresnel or ground-in) (chi-square test, p =0.771) did not significantly impact the success of diplopia elimination with prisms. There was also no significant difference by type of strabismus (esotropia, exotropia, vertical deviation only, esotropia + vertical deviation, and exotropia + vertical deviation) in the ability of prisms to eliminate diplopia (chi-square test, p =0.095). Patients with esotropia or exotropia alone had similar prism success compared to those with combined horizontal and vertical deviations (chi-square test, p =0.661), as did patients with vertical deviations alone (chi-square test, p =0.180) when compared to patients with combined deviations. There was also no association between retinal pathology type and the type of deviation at presentation (chi-square test, p =0.747). Observed effect sizes for these analyses were small.
Discussion
In this retrospective review evaluating patients with retinal pathology and diplopia who were prescribed prisms, the majority (65.7%) had elimination of diplopia with prism glasses. The findings of this study apply to a range of retinal pathologies associated with diplopia, including epiretinal membrane, macular hole, macular edema, and macula-involving retinal detachment, although some pathologies were more represented in this cohort compared to others. The type of retinal pathology, type of strabismus (horizontal vs. vertical vs. combined), baseline visual acuity, and age were not associated with the ability to eliminate diplopia with prisms. While the literature assessing the role of prisms in this patient population has had variable results, with success rates ranging from 9% to 57%, this outcome yields a more promising role for prisms as a treatment option for these patients.4,8
Despite the majority of patients achieving diplopia resolution with prism correction, approximately one-third of patients did not experience symptomatic improvement. Several factors may account for treatment failure in this population. Structural alterations of the macula, including distortion of the foveal architecture, may result in retinal misregistration that cannot be fully corrected with prisms alone. Additionally, prolonged duration of disease or macular pathology causing distortion/blurred vision may lead to reduced fusional capacity, limiting the ability to achieve stable binocular single vision even with appropriate prism correction.
Although approximately two-thirds of patients reported diplopia elimination with prisms, many required a change to their prism prescription, with some requiring multiple changes, before reporting diplopia elimination. While the reason for this has not yet been delineated, Bixenmen’s study also reported that patients with retinal pathologies reported an improvement in their diplopia when placed in spectacles containing the appropriately measured prism strength, but later reported that the superimposition of the two images was transient with longer prism use.6 Their study, however, did not include data on prism success after making prescription changes for patient preference. This finding highlights that prescribing prisms for patients with retinal pathology can be a matter of trial-and-error, which emphasizes the importance of prism trial in a trial frame and consideration of a more prolonged simulation with patients performing their typical activities of daily living, such as reading and walking around, in the clinic before being given a final prescription. Patients can also be given the option to trial a Fresnel prism before commitment to a ground-in prescription, as prescription changes may be expected in this population. With this in mind, patient expectations should be appropriately set with proper counseling that they may require multiple prescription trials to alleviate their diplopia.
For horizontal deviations at distance and near, patients tended to report diplopia resolution with prism strengths lower than the measured deviation, while for vertical deviations at near, they required stronger prism than objectively indicated. These findings suggest that patients’ subjective responses during in-office prism testing often did not align with the magnitude of their measured deviations. We suspect that the difference in prescribed and measured horizontal prisms is likely related to horizontal fusional amplitudes, which are variable but generally larger for convergence compared to divergence.9 In contrast, vertical fusional amplitudes are limited and typically less than horizontal amplitudes. There may be several factors that contribute to patients subjectively requiring a different amount of prism to eliminate diplopia then what is objectively measured. Patients with retinal pathology may have eccentric fixation, those with poor visual acuity may have poor fixation during cover testing, and there may be anomalous retinal correspondence.10 Depending on the degree of foveal misalignment and the length of time that patients have had their retinal pathologies, those with anomalous retinal correspondence may require less prism to correct their diplopia. Thus, it is important to incorporate subjective feedback during prism refractions with attention to where patients perceive the second image.
An additional important consideration when interpreting these findings is the optical and physical limitations of prism correction. In clinical practice, prisms may be less effective than expected due to off-axis viewing through spectacle lenses, which induces variable prismatic effects according to Prentice’s rule.11 Despite these known limitations, our study demonstrates a relatively high rate of diplopia resolution in patients with retinal pathology, suggesting that patient’s may be able to adapt to the inherent limitations of prism glasses over time.
Limited sample size in this study may have interfered with detection of modest associations, such as between deviation type and ability to eliminate diplopia that may have yielded a trend in a larger dataset. This study had a variety of retinal pathologies included, but the relative volume of some of the less represented pathologies may limit the ability to account for other clinical factors, which may also yield an association in a larger sample size. Given the retrospective nature, there was no standardized assessment of subjective improvement after patients received their prism glasses, but rather, diplopia elimination was detected based on clinical documentation.
Given the promising results of prism use for diplopia in patients with retinal pathologies in our study, future studies should aim to prospectively evaluate the relationship between measured deviation and optimal prism correction based on subjective patient reports using more standardized prescribing protocols and consistent long-term follow-up. Inclusion of a greater variety of retinal pathologies and larger patient cohorts could help identify predictors of successful prism adaptation in this population.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the University of Miami Institutional Review Board, approval reference number 20230785.
Consent for Publication
Consent for publication of this study is not applicable due to IRB waiver of consent.
Acknowledgments
We wish to recognize Nathalie Perez, MD for her role in collecting background research for this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare they have no competing interests related to this study.
References
1. Veverka KK, Hatt SR, Leske DA, et al. Prevalence and associations of central-peripheral rivalry-type diplopia in patients with epiretinal membrane. JAMA Ophthalmol. 2017;135(12):1303–6. doi:10.1001/jamaophthalmol.2017.4350
2. Veverka KK, Hatt SR, Leske DA, Brown WL, Iezzi R, Holmes JM. Causes of diplopia in patients with epiretinal membranes. Am J Ophthalmol. 2017;179:39–45. doi:10.1016/j.ajo.2017.04.014
3. Mirzaei A, Akbari MR, Amini A, Mirmohammadsadeghi A, Khojasteh H. Retinal misregistration and effect of surgery on its improvement in patients with epiretinal membrane. J AAPOS. 2022;26(4):179e1–179e5. doi:10.1016/j.jaapos.2022.05.002
4. Burgess D, Roper-Hall G, Burde RM. Binocular diplopia associated with subretinal neovascular membranes. Arch Ophthalmol. 1980;98(2):311–317. doi:10.1001/archopht.1980.01020030307014
5. Barton JJ. “Retinal diplopia” associated with macular wrinkling. Neurology. 2004;63(5):925–927. doi:10.1212/01.wnl.0000137045.33870.9e
6. Bixenman WW, Joffe L. Binocular diplopia associated with retinal wrinkling. J Pediatr Ophthalmol Strabismus. 1984;21(6):215–219. doi:10.3928/0191-3913-19841101-04
7. De Pool ME, Campbell JP, Broome SO, Guyton DL. The dragged-fovea diplopia syndrome: clinical characteristics, diagnosis, and treatment. Ophthalmology. 2005;112(8):1455–1462. doi:10.1016/j.ophtha.2005.01.054
8. Hatt SR, Leske DA, Klaehn LD, Kramer AM, Iezzi R, Holmes JM. Treatment for central-peripheral rivalry-type diplopia (“Dragged-Fovea Diplopia Syndrome”). Am J Ophthalmol. 2019;208:41–46. doi:10.1016/j.ajo.2019.06.030
9. Lanca CC, Rowe FJ. Measurement of fusional vergence: a systematic review. Strabismus. 2019;27(2):88–113. doi:10.1080/09273972.2019.1583675
10. Simonsz HJ. First description of anomalous retinal correspondence by Johannes Peter Muller in 1826. Strabismus. 2010;18(3):116. doi:10.3109/09273972.2010.506406
11. Irsch K. Optical issues in measuring strabismus. Middle East Afr J Ophthalmol. 2015;22(3):265–270. doi:10.4103/0974-9233.159691
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Results According to Inferior Oblique Manipulation in Patients with Inferomedial Blowout Fracture Involving the Orbital Strut
Park J, Jo S, Choi HY
Clinical Ophthalmology 2022, 16:4263-4272
Published Date: 21 December 2022