")
Back to Journals » Patient Preference and Adherence » Volume 17
Prioritizing Treatment Goals of People Diagnosed with Bipolar I Disorder in the US: Best–Worst Scaling Results
Authors Bridges JFP, Goldberg JF, Fitzgerald HM , Chumki SR, Beusterien K, Will O , Citrome L
Received 28 April 2023
Accepted for publication 29 September 2023
Published 12 October 2023 Volume 2023:17 Pages 2545—2555
DOI https://doi.org/10.2147/PPA.S419143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
John FP Bridges,1,* Joseph F Goldberg,2,* Heather M Fitzgerald,3,* Sanjeda R Chumki,4,* Kathleen Beusterien,5,* Oliver Will,5,* Leslie Citrome6,*
1Department of Biomedical Informatics, the Ohio State University College of Medicine, Columbus, OH, USA; 2Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 3Medical Affairs, Lundbeck LLC, Deerfield, IL, USA; 4Medical Affairs, Otsuka Pharmaceutical Development & Commercialization Inc, Princeton, NJ, USA; 5Cerner Enviza, North Kansas City, MO, USA; 6Department of Psychiatry & Behavioral Sciences, New York Medical College, Valhalla, NY, USA
*These authors contributed equally to this work
Correspondence: Sanjeda R Chumki, Otsuka Pharmaceutical Development & Commercialization Inc, 508 Carnegie Center Dr, Princeton, NJ, 08540, USA, Tel +1-609-524-6788, Email [email protected]
Purpose: Bipolar I disorder (BP-I) is associated with significant disease burden, but evidence on treatment goals in people diagnosed with BP-I is scarce. This study sought to quantify treatment goals related to the pharmacological management of BP-I in adults in the US and to identify if subgroups of people with similar treatment goals exist.
Patients and Methods: A best–worst scaling (BWS) of treatment goals was developed based on available literature and input from experts and patients and was distributed as part of a survey between August and September 2021. Survey participants were adults with a self-reported diagnosis of BP-I who were recruited via an online panel in the US. Participants were asked to prioritize the importance of 16 treatment goals using BWS. BWS scores were computed using multinomial logistic regression, with the scores across all goals summing to 100 for each participant. Subgroups of people with similar preferences were identified using latent class analysis.
Results: The most important treatment goals for people diagnosed with BP-I (N=255) were “being less impulsive, angry, or irritable” (score: 9.73), or being “able to feel pleasure or happiness” (score: 9.54). Goals related to reducing the incidence of various potential adverse events of medication (scores: ≤ 4.51) or “reducing dependence on others” (score: 3.04) were less important. Two subgroups were identified. One subgroup (n=111) prioritized symptom-focused goals, considering “reducing frequency of mania, depression, and mixed episodes” and “being less impulsive, angry or irritable” the most important (scores: 12.46 and 11.85, respectively). The other subgroup (n=144) placed significantly more importance on social functioning-focused goals, including beginning or maintaining a relationship with a partner/significant other, and with family and/or friends (scores: 8.45 and 7.70, respectively).
Conclusion: People diagnosed with BP-I prioritized emotional improvements. Subgroups of people with BP-I prioritized either symptom-focused or social functioning-focused treatment goals.
Keywords: patient preference, healthcare questionnaire, treatment individualization, social functioning
Introduction
Bipolar I disorder (BP-I) is a lifelong neuroprogressive illness characterized by severe alterations in mood and behavior, manifesting through episodes of mania, hypomania, and/or depression.1–4 Available evidence suggests a global lifetime prevalence of ~1% of BP-I in the general population;5 however, patients with BP-I are often initially misdiagnosed with major depressive disorder, schizophrenia, schizophrenia-related disorders, or substance-induced psychotic disorder, and a diagnosis of BP-I may be delayed for up to 15 years, compounding adverse patient outcomes.6
BP-I is associated with a significant disease burden due to early onset (typically in the early twenties),5 and the chronicity and severity of its symptoms.7 People with BP-I achieving clinical remission continue to experience symptoms such as subsyndromal depression, sleep disturbances, or perceived cognitive impairment during euthymic periods.2,8 These symptoms may act as precursors to mood episode recurrence, and negatively impact people’s functioning and quality of life.8 Moreover, BP-I is linked to high rates of premature mortality from suicide as well as medical comorbidities.9,10
Pharmacological treatment with atypical antipsychotics and mood stabilizers is recommended as the cornerstone of management of BP-I by clinical guidelines, including the American Psychiatric Association (APA) and Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines.11–13 Available evidence suggests that monotherapy with lithium, quetiapine, divalproex, lamotrigine, asenapine, or aripiprazole, or combination therapy should be considered as first‐line treatment for those initiating pharmacotherapy, or for those switching treatment during the maintenance phase.11 Long-acting injectable (LAI) formulations may be used in people who prefer this method of administration or whose history of adherence is erratic.14 Aripiprazole once-monthly 400 mg (AOM 400) and risperidone LAI have the highest level of evidence for use, are the only LAI formulations approved for maintenance monotherapy treatment of BP-I,15,16 and are guideline-recommended for the maintenance treatment of BP-I.11,14
Unmet needs remain for an array of safe therapeutic options that are effective for long-term management of the symptoms of BP-I across different phases of the disorder.11,17,18 Patient-centered care, including shared decision-making (SDM), is recommended as a foundation of BP-I clinical management.11 Possible treatment goals for patients with BP-I have previously been identified, including achieving euthymia and normal levels of functioning, and preventing the recurrence of a depressive or a manic episode.11,19 While treatment goal prioritization from the patients’ perspective has been investigated in other psychiatric conditions, such as schizophrenia,20–22 there is a paucity of literature focused on comparative assessment of treatment goals from the perspective of people diagnosed with BP-I. This paper aimed to quantitatively assess how people in the US diagnosed with BP-I prioritize a variety of treatment goals related to the pharmacological management of their condition. The secondary objective was to identify possible subgroups of people diagnosed with BP-I with similar patterns of treatment goal prioritization. The data and learning from this study could increase awareness of the patient perspective among clinicians working with people diagnosed with BP-I and promote patient-centered care.
Materials and Methods
Study Design
The study comprised a qualitative (survey development) and a quantitative phase (survey implementation). All research was conducted according to best practice guidelines for Conjoint Analyses published by the International Society of Pharmacoeconomics and Outcomes Research (ISPOR),23 in accordance with ethical principles specified in the Declaration of Helsinki, International Conference on Harmonization Good Clinical Practices, Good Pharmacoepidemiology Practice, and the applicable legislation on Non-Interventional Studies, and all patients provided informed consent. The study protocol received exemption status from Pearl Institutional Review Board (03 August 2021; board registration number 00007772).24
A best–worst scaling (BWS) exercise to evaluate prioritization of a draft set of treatment goals was developed and included in a draft survey in June 2021. BWS, sometimes known as MaxDiff, object scaling, or best–worst scaling case 1, is now extensively used to understand the priorities of patients and other stakeholders in healthcare,25,26 and is supported by a growing list of software packages.27,28 BWS can be used in several choice formats for various purposes, including prioritizing items, and involves sets containing at least three options, where the respondent is asked to indicate both best and worst (or most and least) options for certain criteria.26 Econometric or statistical methods can subsequently be used to gain a BWS score by assigning values to the individual items based on the choices.29 Development of the BWS exercise was informed by qualitative research and a focused literature review of important treatment outcomes among people diagnosed with BP-I, and by consultation with a panel of experts.
Cognitive interviewing, a technique used to elucidate participants’ perceptions by inviting them to verbalize thoughts and feelings as they examine information,30 was employed: one-on-one cognitive interviews with 12 people in the US diagnosed with BP-I were held via telephone and a desktop sharing platform to pre-test the final survey design and ensure that content was clear to survey participants, and to obtain feedback on BWS items. Open-ended concept elicitation questions were first asked regarding treatment goals to confirm survey content; the participants were then walked through key components of the BWS exercise to assess question interpretation and rationale for responses. The interviews used a “think-aloud” approach, where the participants answered the survey questions by expressing their thoughts out loud.
The survey was finalized based on participant feedback. The final survey was designed to last approximately 25–30 minutes and included 16 treatment goals for prioritization. In a series of 20 BWS tasks, participants rated 20 subsets of treatment goals; each task presented a different combination of 4 goals. For each task, the participants were asked to indicate the most and least important goals. Experimental design for the BWS was a balanced incomplete block design. Every participant saw a different arrangement of treatment goal sets, with the order of the goals and of the sets sequenced differently for each respondent to eliminate order effects. The survey was distributed online between August and September 2021.
Sample Population
People with a self-confirmed diagnosis of BP-I were recruited via Kantar Profiles, a research panel company that maintains a database of people who have opted into research interviews. Participants from the qualitative phase of the survey were not able to participate in the quantitative phase of the survey. People were eligible to complete the survey if they met all of the following criteria: were aged 18–65 years, had a self-reported diagnosis of BP-I by a physician, were currently prescribed antipsychotic medication for the treatment of BP-I, identified BP-I as their primary condition, had been prescribed medication for mania or a manic episode, had received at least 6 months of antipsychotic treatment for BP-I, resided in the US, and were willing to provide informed consent. People were excluded if they were hospitalized for a manic episode at the time of the survey, had other disorder(s) that could alter BP-I treatment or had diagnoses that conflicted with establishing a diagnosis of BP-I (such as schizophrenia, or schizoaffective disorder), had taken clozapine for the treatment of BP-I, or were currently participating in a clinical trial.
People were able to self-identify with the research criteria and take immediate action to determine their eligibility for participation. Measures were taken to minimize intentionally false reporting; questions were included to help screen out people without a diagnosis of BP-I, such as including a list of health conditions to choose from. Severity of participants’ BP-I was self-reported based on participants’ hospitalization history and number of medications ever taken for the treatment of BP-I, and further assessed through an additional targeted question. The Patient Health Questionnaire-8 (PHQ-8)31 was used as a screening tool to evaluate depressive symptoms in participants; scores of ≥10 indicate a positive screen for depression. All participants who met the study eligibility criteria and completed the full survey were included in the analysis.
Statistical Analysis
Sample size considerations for computation of BWS scores were addressed following Lipovetsky et al (2015).32 Based on the formula provided, to achieve a margin error around the BWS score within ±0.05 where there are 16 BWS goals presented 4 at a time in 20 tasks, a minimum sample size of 154 patients was required. The target sample size for this study of 250 was higher to ensure that it would be robust for conducting a latent class analysis.
Participant characteristic data were collected and summarized descriptively. BWS scores were computed using multinomial logistic regression. The model was fit using maximum likelihood, and one coefficient β was estimated for each of the 16 BWS goals, with coefficients reflecting preference weights. The estimated coefficients were transformed with the logit function and converted into selection probabilities and standardized to 100% for reporting (the BWS scores summed to 100 for each respondent). The rank order, standard errors, and 95% confidence intervals (CIs) were reported for the preference weight of each goal, with the combined importance scores for the 16 treatment goals totaling 100 (the higher the value, the more important the treatment goal). The final score received by any treatment goal was thus indicative of the treatment goal’s relative importance compared with other goals.
Analyses of the study data did not involve adjustment for covariates. Instead, multinomial logistic regression was used for latent class analysis of the preference weights to identify subgroups of people with similar goal prioritizations. Demographic and clinical characteristics were compared between subgroups, using independent sample t-tests or chi-square tests, as appropriate. BWS analysis was performed using Sawtooth’s Lighthouse Studio v9.9. All other analyses were performed using SPSS v28.
Results
Of the 2438 people in the research database who accessed the survey, 263 eligible people completed the survey, 206 people accessed the survey link but did not take the survey, 21 people attempted to access the survey after it had closed, and 1948 people did not meet eligibility criteria. Of the 263 eligible people who completed the survey, 8 were identified as “speeders” in the survey, completing each preference task in less than 5 seconds, and were removed, resulting in an effective sample size of 255 participants.
Most participants were female, Caucasian, and the most common employment status of participants was part-time or full-time employment. At the time of survey, most people self-rated their severity of BP-I as moderate, with a mean (standard deviation [SD]) PHQ-8 score of 12 (6.41). Participant demographic and clinical characteristics are shown in Table 1 and 2.
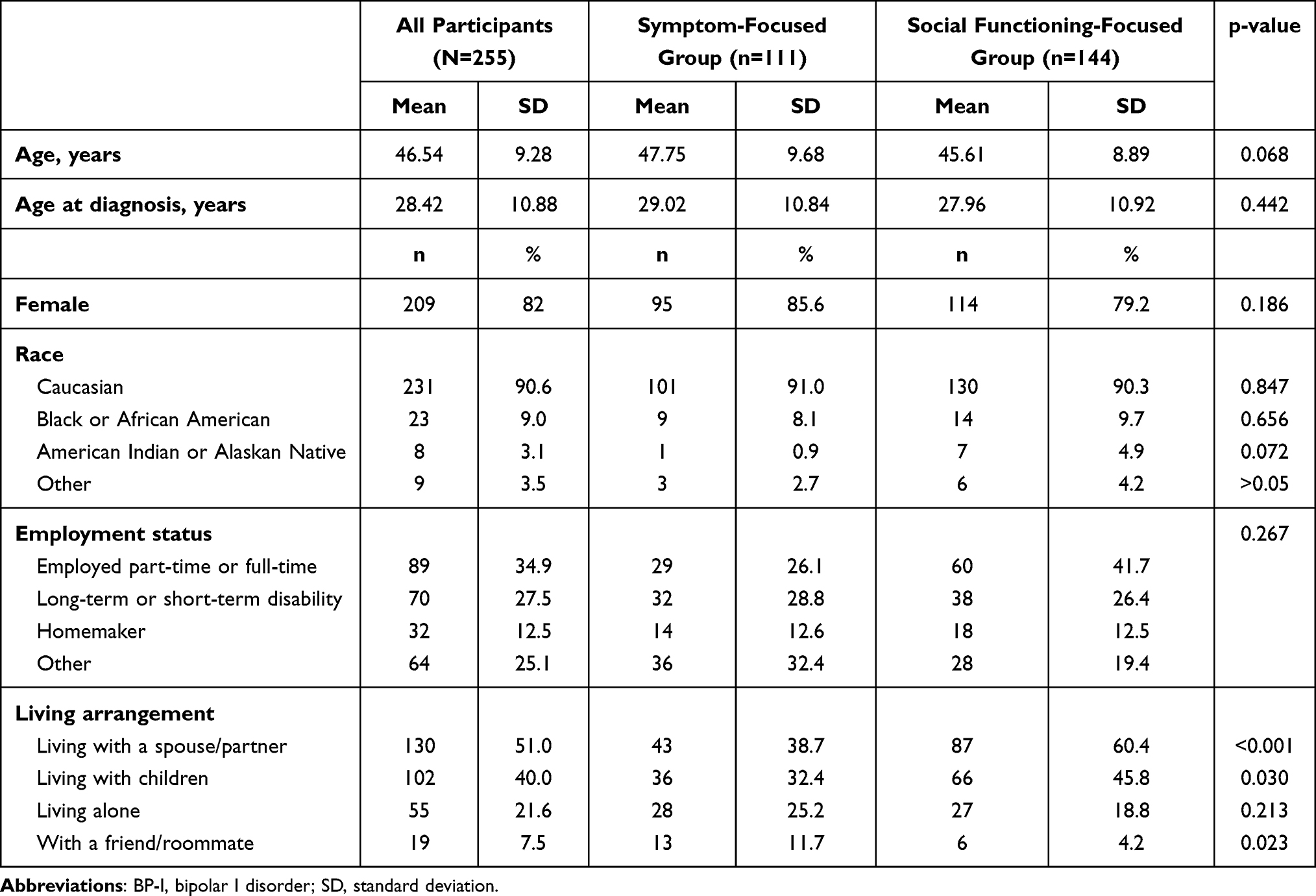 |
Table 1 Demographic Characteristics of Survey Participants Diagnosed with BP-I |
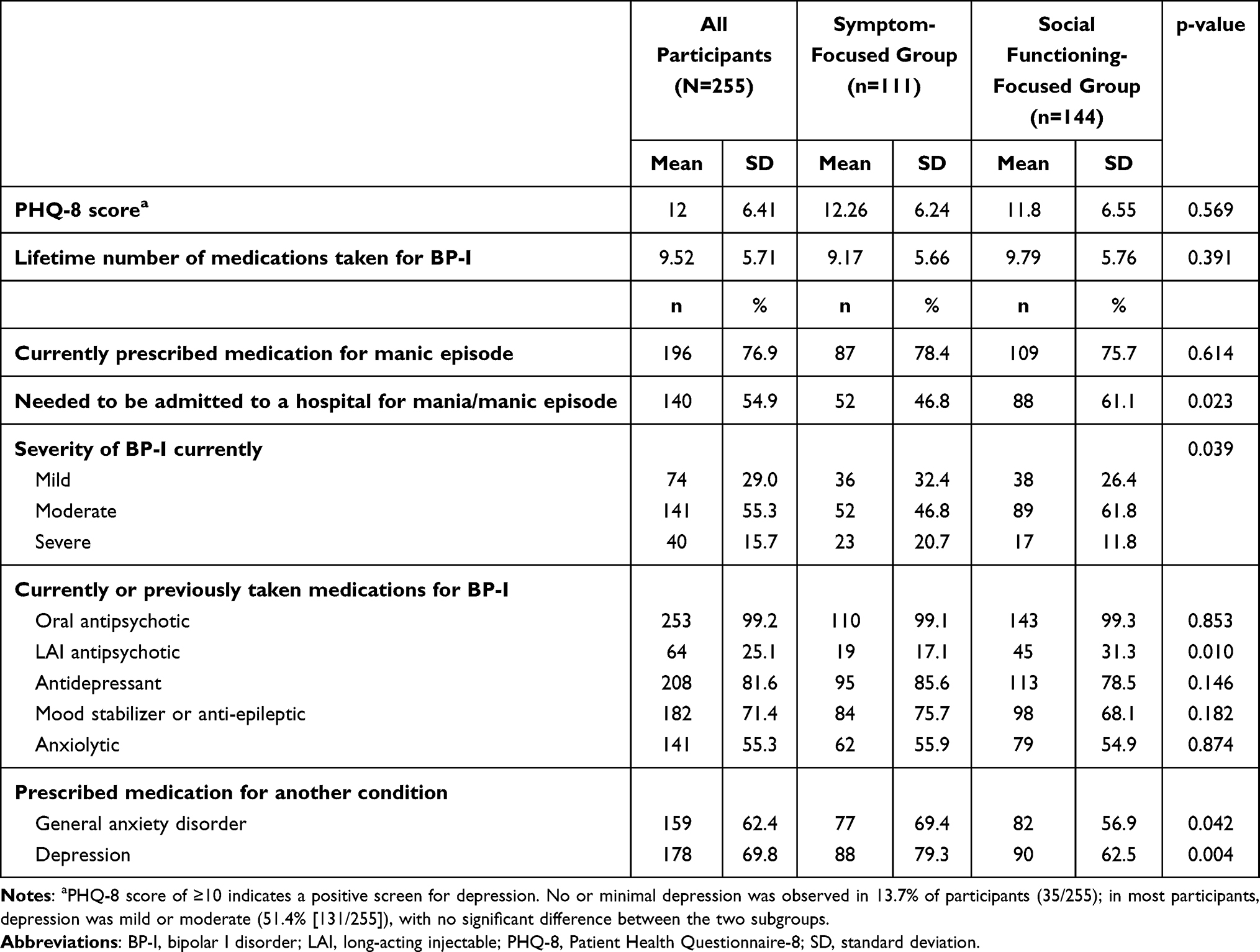 |
Table 2 Clinical Characteristics of Survey Participants Diagnosed with BP-I |
Prioritization of treatment goals by people diagnosed with BP-I is presented in Table 3, ranked from the most to the least important. BWS scores total 100 for each participant. The higher the score for individual goals, the more important the treatment goal relative to other treatment goals included. If all BWS scores were considered equal in importance, they would each have a score of 6.25. Treatment goals shown to be the most important to participants were emotional improvement, such as being less impulsive, angry, or irritable, or being able to feel pleasure or happiness, and reduction in the frequency of mania, depression, or mixed episodes. Reducing the incidence of various potential adverse events (AEs) of medication (eg, “reduced risk of insomnia, restlessness or moving around too much during sleep”, “reduced risk of weight gain” and “reduced risk of excessive sleepiness, drowsiness or being slowed down”) or reducing dependence on others were considered relatively less important.
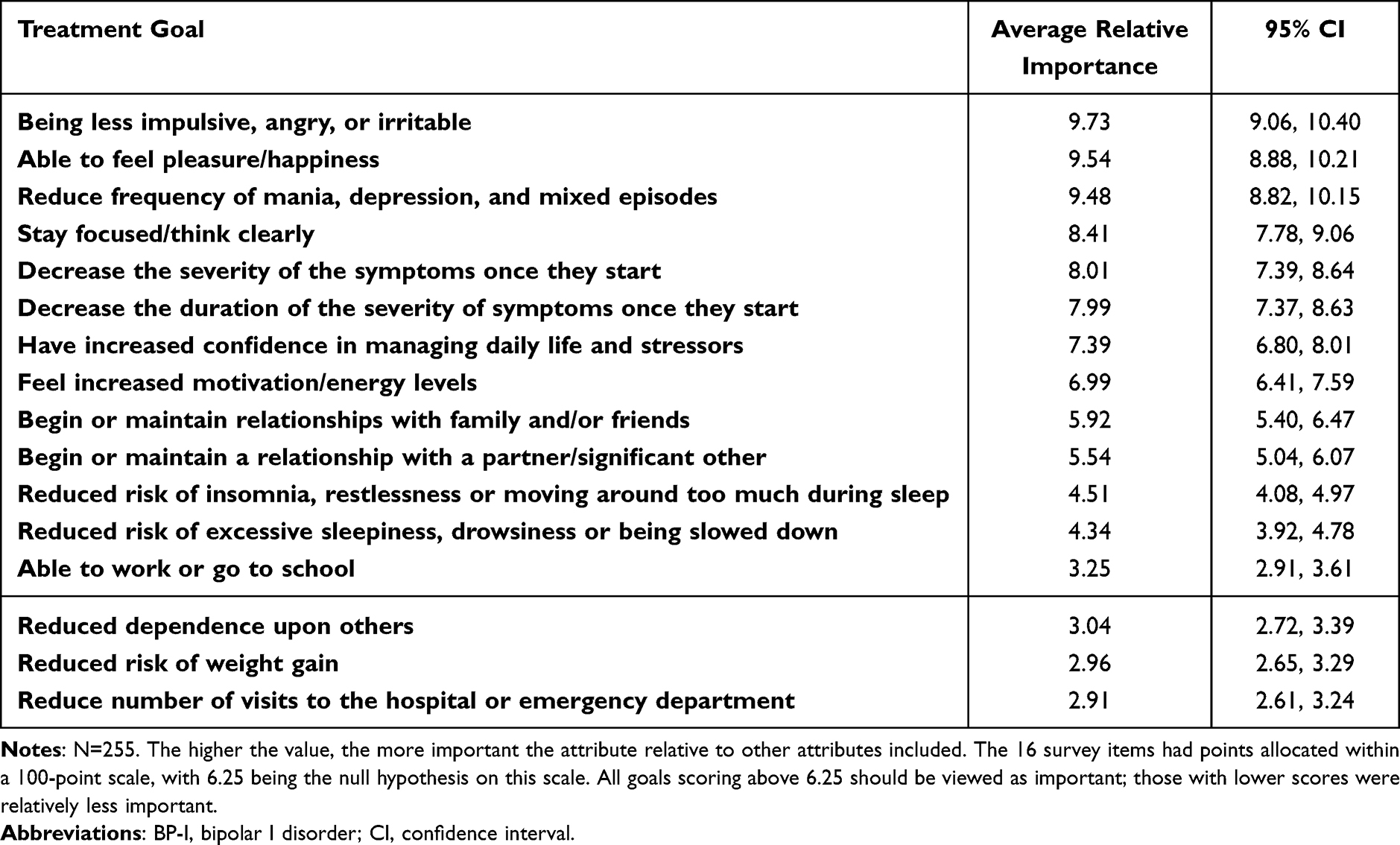 |
Table 3 Treatment Goals and Their Importance to Survey Participants Diagnosed with BP-I |
Latent class analysis of treatment goals identified two groups of people with different distributions of preferences. The first group (n=111) placed more importance on symptom-focused goals (symptom-focused group), while the second group (n=144) placed more emphasis on social functioning-focused goals (social-functioning focused group; Figure 1).
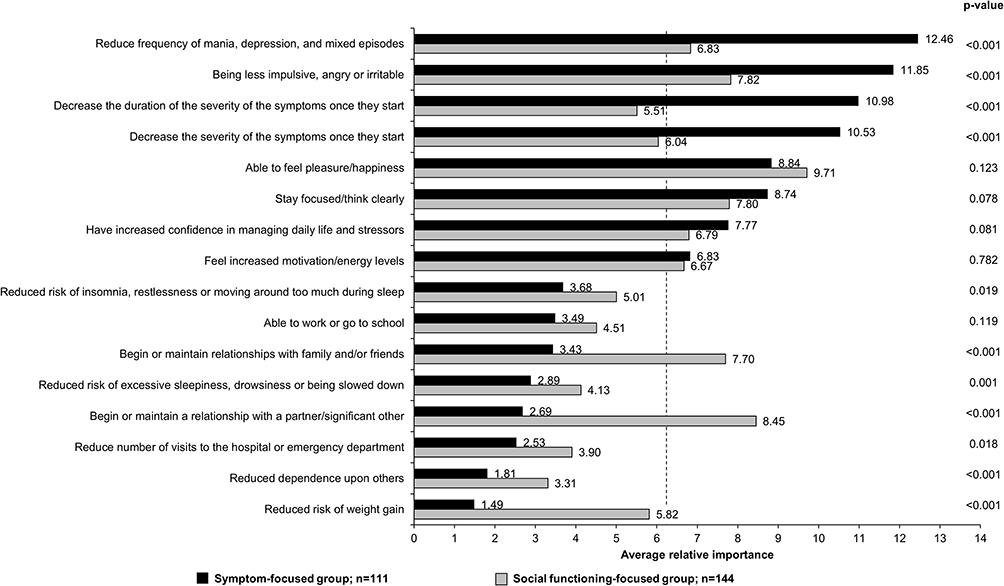 |
Figure 1 Latent class analysis of the importance of treatment goals for different subgroups of participants, listed from most important to least important according to the symptom-focused group. The 16 survey items had points allocated within a 100-point scale, with 6.25 being the null hypothesis on this scale, representing an item in the middle of a scale from most important to least important. All goals scoring above 6.25 (denoted by the dashed line) should be viewed as important. The higher the value, the more important the attribute relative to the other attributes included in the exercise. P-values were derived from an independent samples t-test. |
The most important treatment goals for the symptom-focused group included reducing the frequency of mania, depression, and mixed episodes (score: 12.46), being less impulsive, angry, or irritable (score: 11.85), and decreasing the severity and duration of severity of symptoms once they start (scores: 10.53 and 10.98, respectively). These goals were statistically significantly more important for the symptom-focused group than for the social functioning-focused group (p<0.001; Figure 1).
Compared with the symptom-focused group, the social functioning-focused group placed significantly more importance on beginning or maintaining a relationship with a partner or significant other (score: 8.45), and with family and/or friends (score: 7.70) (p<0.001; Figure 1). The most important goal for the social functioning-focused group was being able to feel pleasure/happiness (score: 9.71), but the difference in treatment preference weight for this goal did not reach statistical significance when compared with the symptom-focused group (p=0.123; Figure 1).
Compared with the social functioning-focused group, the symptom-focused group was significantly more likely to have a higher overall BP-I severity (p=0.039; Table 2), a concomitant diagnosis of depression (p=0.007; data not shown), to have been prescribed medication for depression (p=0.004) or general anxiety disorder (p=0.042; Table 2), and to live with a friend or roommate (p=0.023; Table 1).
Compared with the symptom-focused group, the social functioning-focused group was more likely to have been hospitalized in the past for mania/manic episode (p=0.023; Table 2), live with a spouse/partner (p<0.001) or children (p=0.030; Table 1), and more likely to have used an LAI treatment (p=0.010; Table 2).
Most people reported that BP-I impacted their career or finances, with the impacts of BP-I being generally similar in the symptom-focused and social functioning-focused groups (Figure 2). Compared with the social functioning-focused group, the symptom-focused group was more likely to have been declared bankrupt (p=0.007; data not shown).
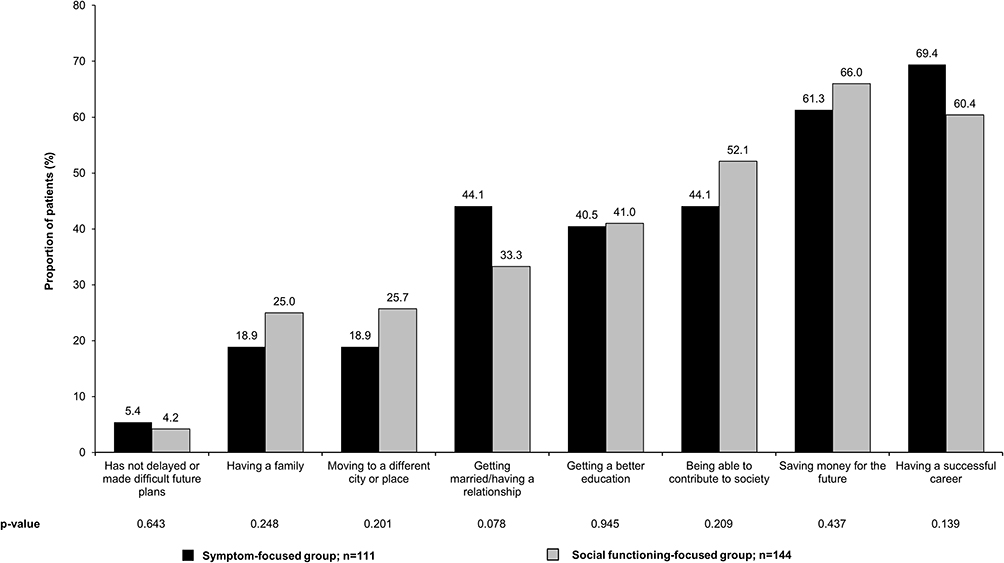 |
Figure 2 Future plans made difficult by BP-I. P-values for the between-group difference were derived from independent sample tests of proportions. Abbreviation: BP-I, bipolar I disorder. |
Discussion
The results of the survey showed that treatment goals considered the most important by people diagnosed with BP-I include emotional improvement, and reduction in the frequency of episodes of mania, depression, or mixed episodes. Social functioning goals, such as the ability to stay focused/think clearly, and having increased confidence in managing daily life and stressors, were also considered important. This treatment goal prioritization is broadly in line with previous research showing that the treatment goals considered the most important by people diagnosed with BP-I include avoiding severe depression and mania, increasing quality of life, and improving school, occupational, and social functioning,33 and reflects the significant disease burden many people diagnosed with BP-I face. Impulsive and aggressive behavior during manic episodes can have disastrous consequences for people,2,7 while depressive episodes are disabling and may be associated with chronicity.3 Greater severity of depressive and irritability symptoms has also been associated with lower quality of life and higher functional impairment in people with bipolar disorder.34 Functional impairment affects up to 75% of patients with bipolar disorders,35 with only 40% of patients with BP-I achieving functional recovery within two years following their first manic or mixed episode.36 However, functional impairment often receives insufficient clinical attention, with some clinicians arguing that the most common unmet need in patients with residual symptoms is access to a wider spectrum of psychosocial interventions.17 This is especially concerning given the results of an online survey of patient and caregiver perspectives on unmet needs in the treatment of bipolar disorder, where 43.2% of the 433 respondents identified life stressors as the most common cause of relapse.37
Our results also show that there may be subgroups of people with BP-I with different priorities regarding the goals of BP-I treatment, with some patients prioritizing symptom-focused goals, and others placing more emphasis on social functioning-focused goals. The difference between the average relative importance of the goals ranked as the most and least important was almost 11 BWS score points in the symptom-focused group, compared with a difference of 6.4 BWS score points in the social functioning-focused group, suggesting a more equal distribution of treatment goal importance in the social functioning-focused group compared with the symptom-focused group. The existence of subgroups of people with different treatment priorities suggests that treatment of BP-I may need to be tailored to the specific needs of individual patients and highlights the crucial role of shared decision-making in the clinical management of BP-I to ensure the treatment approach is in line with patients’ needs and priorities. Our results also highlight a need for psychological support among patients with BP-I, and a variation in the required focus of such support, to restore the quality of life of individual patients with BP-I and their families.11
It is worth noting that people’s priorities may differ between genders and in different phases of the disorder.17,18 Different episodes or stages of BP-I are often handled as almost independent from each other; the development of an overall therapeutic strategy, therefore, remains an unmet need in BP-I.18 Research has shown that people diagnosed with bipolar disorder desire greater involvement in decisions regarding their care.38 The data reported here show differences in the prioritization of treatment goals between symptom-focused and social functioning-focused people diagnosed with BP-I, who may differ in their demographic and clinical characteristics, as well as in their symptomatic presentation and where they are in their treatment journey. These findings may facilitate the development of strategies for individualizing treatment plans. Clinicians can use this information to help patients explore their preferences and make informed treatment choices in line with the principles of SDM.39 By ensuring that patient perspectives are adequately considered,40 and enhancing the therapeutic alliance, treatment adherence and outcomes in BP-I may be improved.41,42
Available data on the perception of people diagnosed with BP-I of the importance of avoiding AEs of medication compared with the aforementioned goals are contradictory, with some studies showing that avoidance of AEs is considered more important than symptom- or functioning-related goals, and other studies suggesting the opposite.33,43,44 AEs previously reported to have the greatest influence on treatment choice among people diagnosed with bipolar disorder include weight gain, sleeping difficulties, suicidal thoughts, and sedation.45,46 In the present survey, feeling increased levels of energy was an important treatment goal for people diagnosed with BP-I, while reducing weight gain was found to be relatively less important to them. It is, however, worth noting that compared with symptom-focused participants who had a higher overall severity of BP-I, reducing weight gain was significantly more important to social functioning-focused participants, who in the present study were significantly more likely to be living with their spouse or children, and who tended to have higher rates of full- or part-time employment.
The current survey design has several potential limitations. Firstly, the people with BP-I included in this survey may not be representative of the broader population of people diagnosed with BP-I – the proportion of participants receiving LAIs (25.1%) may be much higher than is usual in current clinical practice. In a 2019 online poll of 130 clinicians, only one fifth of respondents stated that they treat >5% of their patients with BP-I with LAIs, whereas a third stated that they treat <1% of their patients with BP-I with LAIs.2 Results of another survey, distributed between April and November 2016 to 34 experts in the US, indicated that only 11% of patients with bipolar disorders were being treated with LAIs.47 In addition, in current clinical practice, LAIs are often reserved for people with greater disease severity or adherence concerns.2 In the present survey, the participants who were treated with LAIs were more likely to have a lower overall severity of BP-I. The survey may have had a selection bias toward recruiting people interested in and able to participate in research studies, potentially under-representing more severely ill, elderly, or institutionalized people. Additionally, as a means of ensuring a more homogenous sample, the study included patients receiving an antipsychotic but not those receiving only a mood stabilizer, thus excluding a potentially important population. For these reasons, the exploration of the priorities of people with BP-I in a real-world patient population without such restrictive selection criteria, eg, by healthcare providers during clinical appointments with patients with BP-I, would be beneficial to evaluate treatment goal prioritization in a broader group of patients with BP-I with less risk of sampling bias.
Secondly, the survey was not designed to assess how subgroups of people with different treatment goal prioritization may be identified in clinical practice, or how treatment goal prioritization could be used in SDM in people diagnosed with BP-I, eg, through a BP-I-specific equivalent of an instrument such as the Outcome Prioritization Tool48 or through an integrated, goal-based, visualization SDM tool such as the Goal Board, aligning prioritized goals to interventional options.49
Thirdly, the survey’s reliance on participants’ self-reported data is inherently susceptible to response bias (eg, recall bias or self-presentation bias), which may influence study results. Additionally, while the BWS approach may allow for the consideration of more goals than other methods such as discrete choice exercises, it may fail to capture additional attributes influencing participant preferences. Lastly, in the treatment goals BWS exercise, the wording of goals related to reducing the incidence of AEs of medication did not explicitly make a link to medication; as such, it is conceivable that AEs were perceived as disease symptoms independent of medication. For example, patients may have rated the insomnia or excessive sleepiness goals in the context of their wish to minimize those items as symptoms of their illness (ie, insomnia as a symptom of mania, or sleepiness as a symptom of depression), rather than wanting to minimize them as potential side effects of medication.
Conclusion
This survey contributes to knowledge on treatment goal prioritization by people diagnosed with BP-I. Treatment goals prioritized by people diagnosed with BP-I include emotional improvement and reduction in the symptomatic burden of BP-I. However, subgroups of people with differences in perceived importance of individual treatment goals may exist, and should be considered when discussing treatment options with people diagnosed with BP-I.
Acknowledgments
This work was supported by Otsuka Pharmaceutical Development & Commercialization Inc. (Princeton, NJ, USA) and Lundbeck LLC (Deerfield, IL, USA). The sponsors were involved in the design of the study, the collection, analysis and interpretation of data, the writing and reviewing of this article, and the decision to submit the article for publication.
Writing support was provided by Babette Jamieson, assisted by her colleagues at Cambridge – a Prime Global Agency (Knutsford, UK), and funded by Otsuka Pharmaceutical Development & Commercialization Inc. and H. Lundbeck A/S.
The authors would like to thank Maxine Chen, who contributed to developing the project concept, the Protocol, and the Statistical Analysis Plan, and to analysis of topline results.
Some of the data in this manuscript have previously been reported in a poster presented at Psych Congress 2022, New Orleans, LA, USA, 17–20 September 2022; Poster 142.
Disclosure
John F. P. Bridges has previously served as a consultant for Otsuka and Lundbeck. Joseph F. Goldberg has served as a consultant for BioXcel, Jazz Pharmaceuticals, Lundbeck, Neumora, Neurelis, Otsuka, Sage Pharmaceuticals, Sunovion, Supernus, and Takeda. He is on the Speakers’ bureau for AbbVie, Alkermes, Axsome, Intra-Cellular Therapies, and Sunovion. He has received royalties from American Psychiatric Publishing and Cambridge University Press. At the time of the survey, Heather M. Fitzgerald was a full-time employee of Lundbeck LLC, Deerfield, IL, USA. Sanjeda R. Chumki is a full-time employee of Otsuka Pharmaceutical Development & Commercialization Inc, Princeton, NJ, USA. Kathleen Beusterien and Oliver Will are employees of Cerner Enviza, which provides consulting services to Lundbeck and Otsuka. Leslie Citrome has served as consultant to AbbVie/Allergan, Acadia, Adamas, Alkermes, Angelini, Astellas, Avanir, Axsome, BioXcel, Boehringer Ingelheim, Cadent Therapeutics, Cerevel, Clinilabs, COMPASS, Eisai, Enteris BioPharma, HLS Therapeutics, Idorsia, Impel, INmune Bio, Intra-Cellular Therapies, Janssen, Karuna, Lundbeck, Lyndra, Marvin, Medavante-ProPhase, Merck, Mitsubishi-Tanabe Pharma, Neurelis, Neurocrine, Novartis, Noven, Otsuka, Ovid, Praxis, Recordati, Relmada, Reviva, Sage, Sunovion, Supernus, Teva, University of Arizona, Vanda, and one-off ad hoc consulting for individuals/entities conducting marketing, commercial, or scientific scoping research. He has served as speaker for AbbVie/Allergan, Acadia, Alkermes, Angelini, Axsome, BioXcel, Eisai, Idorsia, Intra-Cellular Therapies, Janssen, Lundbeck, Neurocrine, Noven, Otsuka, Recordati, Sage, Sunovion, Takeda, Teva, and CME activities organized by medical education companies such as Medscape, NACCME, NEI, Vindico, and universities and professional organizations/societies. He holds a small number of shares of common stock with Bristol-Myers Squibb, Eli Lilly, Johnson & Johnson, Merck, and Pfizer (purchased >10 years ago) and currently has options for acquiring stocks with Reviva. He has received royalties or income from publishing from Taylor & Francis (Current Medical Research and Opinion, 2022–date), Wiley (International Journal of Clinical Practice, through end 2019), UpToDate, Springer Healthcare, Elsevier (Psychiatry, Clinical Therapeutics). The authors report no other conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Tohen M, Goldberg JF, Hassoun Y, Sureddi S. Identifying profiles of patients with bipolar I disorder who would benefit from maintenance therapy with a long-acting injectable antipsychotic. J Clin Psychiatry. 2020;81(4):OT19046AH1. doi:10.4088/JCP.OT19046AH1
3. Serafini G, Pardini M, Monacelli F, et al. Neuroprogression as an illness trajectory in bipolar disorder: a selective review of the current literature. Brain Sci. 2021;11(2):276. doi:10.3390/brainsci11020276
4. Vázquez GH, Holtzman JN, Lolich M, Ketter TA, Baldessarini RJ. Recurrence rates in bipolar disorder: systematic comparison of long-term prospective, naturalistic studies versus randomized controlled trials. Eur Neuropsychopharmacol. 2015;25(10):1501–1512. doi:10.1016/j.euroneuro.2015.07.013
5. Rowland TA, Marwaha S. Epidemiology and risk factors for bipolar disorder. Ther Adv Psychopharmacol. 2018;8(9):251–269. doi:10.1177/2045125318769235
6. Lublóy Á, Keresztúri JL, Németh A, Mihalicza P. Exploring factors of diagnostic delay for patients with bipolar disorder: a population-based cohort study. BMC Psychiatry. 2020;20(1):75. doi:10.1186/s12888-020-2483-y
7. Ferrari AJ, Stockings E, Khoo J-P, et al. The prevalence and burden of bipolar disorder: findings from the Global Burden of Disease Study 2013. Bipolar Disord. 2016;18(5):440–450. doi:10.1111/bdi.12423
8. Grunze H, Born C. The impact of subsyndromal bipolar symptoms on patient’s functionality and quality of life. Front Psychiatr. 2020;11:510. doi:10.3389/fpsyt.2020.00510
9. Hayes JF, Miles J, Walters K, King M, Osborn DPJ. A systematic review and meta‐analysis of premature mortality in bipolar affective disorder. Acta Psychiatr Scand. 2015;131(6):417–425. doi:10.1111/acps.12408
10. Crump C, Sundquist K, Winkleby MA, Sundquist J. Comorbidities and mortality in bipolar disorder: a Swedish national cohort study. JAMA Psychiatry. 2013;70(9):931–939. doi:10.1001/jamapsychiatry.2013.1394
11. Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. 2018;20(2):97–170. doi:10.1111/bdi.12609
12. Verdolini N, Hidalgo-Mazzei D, Del Matto L, et al. Long-term treatment of bipolar disorder type I: a systematic and critical review of clinical guidelines with derived practice algorithms. Bipolar Disord. 2021;23(4):324–340. doi:10.1111/bdi.13040
13. American Psychiatric Association. Practice Guideline for the Treatment of Patients with Bipolar Disorder.
14. Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: revised third edition recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2016;30(6):495–553. doi:10.1177/0269881116636545
15. Otsuka America Pharmaceutical, Inc. Abilify Maintena® (Aripiprazole) for Extended-Release Injectable Suspension, for Intramuscular Use [Prescribing Information]. Rockville: Otsuka America Pharmaceutical, Inc; 2020.
16. Janssen Pharmaceuticals, Inc. Risperdal Consta® (Risperidone) Long-Acting Injection [Prescribing Information]. Titusville: Janssen Pharmaceuticals, Inc; 2021.
17. Hajda M, Prasko J, Latalova K, et al. Unmet needs of bipolar disorder patients. Neuropsychiatr Dis Treat. 2016;12:1561–1570. doi:10.2147/NDT.S105728
18. Fountoulakis KN, Vieta E, Young A, et al. The International College of Neuropsychopharmacology (CINP) treatment guidelines for bipolar disorder in adults (CINP-BD-2017), Part 4: unmet needs in the treatment of bipolar disorder and recommendations for future research. Int J Neuropsychopharmacol. 2017;20(2):196–205. doi:10.1093/ijnp/pyw072
19. Shah N, Grover S, Rao GP. Clinical practice guidelines for management of bipolar disorder. Indian J Psychiatry. 2017;59(Suppl 1):S51–S66. doi:10.4103/0019-5545.196974
20. Kinter ET, Schmeding A, Rudolph I, dosReis S, Bridges JFP. Identifying patient-relevant endpoints among individuals with schizophrenia: an application of patient-centered health technology assessment. Int J Technol Assess Health Care. 2009;25(1):35–41. doi:10.1017/S0266462309090059
21. Bridges JFP, Slawik L, Schmeding A, Reimer J, Naber D, Kuhnigk O. A test of concordance between patient and psychiatrist valuations of multiple treatment goals for schizophrenia. Health Expect. 2013;16(2):164–176. doi:10.1111/j.1369-7625.2011.00704.x
22. Bridges JFP, Beusterien K, Heres S, et al. Quantifying the treatment goals of people recently diagnosed with schizophrenia using best–worst scaling. Patient Prefer Adherence. 2018;12:63–70. doi:10.2147/PPA.S152870
23. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
24. Pearl Institutional Review BoardTM. Statement of Compliance. Indianapolis: Pearl IRB, LLC. Available from: https://www.pearlirb.com/statement-of-compliance/.
25. Lipovetsky S, Conklin M. Best-worst scaling in analytical closed-form solution. J Choice Model. 2014;10:60–68. doi:10.1016/j.jocm.2014.02.001
26. Hollin IL, Paskett J, Schuster ALR, Crossnohere NL, Bridges JFP. Best–worst scaling and the prioritization of objects in health: a systematic review. Pharmacoeconomics. 2022;40(9):883–899. doi:10.1007/s40273-022-01167-1
27. White MH. bwsTools: an R package for case 1 best-worst scaling. J Choice Model. 2021;39:100289. doi:10.1016/j.jocm.2021.100289
28. Aizaki H, Fogarty J. R packages and tutorial for case 1 best–worst scaling. J Choice Model. 2023;46:100394. doi:10.1016/j.jocm.2022.100394
29. McFadden D. Conditional logit analysis of qualitative choice behavior. In: Zarembka P, editor. Frontiers in Econometrics. New York: Academic Press; 1973:105–142.
30. Centers for Disease Control and Prevention: Cognitive Interviewing. Maryland: National Center for Health Statistics; 2014; Available from: https://www.cdc.gov/nchs/ccqder/evaluation/CognitiveInterviewing.htm.
31. Kroenke K, Strine TW, Spitzer RL, et al. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. 2009;114(1–3):163–173. doi:10.1016/j.jad.2008.06.026
32. Lipovetsky S, Liakhovitski D, Conklin M. What is the right size for my MaxDiff study?
33. Eiring Ø, Nylenna M, Nytrøen K. Patient-important outcomes in the long-term treatment of bipolar disorder: a mixed-methods approach investigating relative preferences and a proposed taxonomy. Patient. 2016;9(2):91–102. doi:10.1007/s40271-015-0128-x
34. Sylvia LG, Montana RE, Deckersbach T, et al. Poor quality of life and functioning in bipolar disorder. Int J Bipolar Disord. 2017;5(1):10. doi:10.1186/s40345-017-0078-4
35. Burdick KE, Millett CE, Yocum AK, et al. Predictors of functional impairment in bipolar disorder: results from 13 cohorts from seven countries by the global bipolar cohort collaborative. Bipolar Disord. 2022;24(7):709–719. doi:10.1111/bdi.13208
36. Tohen M, Hennen J, Zarate CM, et al. Two-year syndromal and functional recovery in 219 cases of first-episode major affective disorder with psychotic features. Am J Psychiatry. 2000;157(2):220–228. doi:10.1176/appi.ajp.157.2.220
37. Masand PS, Tracy N. Results from an online survey of patient and caregiver perspectives on unmet needs in the treatment of bipolar disorder. Prim Care Companion CNS Disord. 2014;16(4):
38. Fisher A, Manicavasagar V, Kiln F, Juraskova I. Communication and decision-making in mental health: a systematic review focusing on bipolar disorder. Patient Educ Couns. 2016;99(7):1106–1120. doi:10.1016/j.pec.2016.02.011
39. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
40. Verwijmeren D, Grootens KP. Shared decision making in pharmacotherapy decisions, perceived by patients with bipolar disorder. Int J Bipolar Disord. 2018;6(1):21. doi:10.1186/s40345-018-0129-5
41. Sylvia LG, Hay A, Ostacher MJ, et al. Association between therapeutic alliance, care satisfaction, and pharmacological adherence in bipolar disorder. J Clin Psychopharmacol. 2013;33(3):343–350. doi:10.1097/JCP.0b013e3182900c6f
42. Strauss JL, Johnson SL. Role of treatment alliance in the clinical management of bipolar disorder: stronger alliances prospectively predict fewer manic symptoms. Psychiatry Res. 2006;145(2–3):215–223. doi:10.1016/j.psychres.2006.01.007
43. Johnson FR, Özdemir S, Manjunath R, Hauber AB, Burch SP, Thompson TR. Factors that affect adherence to bipolar disorder treatments: a stated-preference approach. Med Care. 2007;45(6):545–552. doi:10.1097/MLR.0b013e318040ad90
44. Revicki DA, Hanlon J, Martin S, et al. Patient-based utilities for bipolar disorder-related health states. J Affect Disord. 2005;87(2–3):203–210. doi:10.1016/j.jad.2005.03.017
45. Ng-Mak D, Poon J-L, Roberts L, Kleinman L, Revicki DA, Rajagopalan K. Patient preferences for important attributes of bipolar depression treatments: a discrete choice experiment. Patient Prefer Adherence. 2018;12:35–44. doi:10.2147/PPA.S151561
46. McIntyre RS. Understanding needs, interactions, treatment, and expectations among individuals affected by bipolar disorder or schizophrenia: the UNITE global survey. J Clin Psychiatry. 2009;70(Suppl 3):5–11. doi:10.4088/JCP.7075su1c.02
47. Sajatovic M, Ross R, Legacy SN, et al. Initiating/maintaining long-acting injectable antipsychotics in schizophrenia/schizoaffective or bipolar disorder – expert consensus survey part 2. Neuropsychiatr Dis Treat. 2018;14:1475–1492. doi:10.2147/NDT.S167485
48. Fried TR, Tinetti ME, Iannone L, O’Leary JR, Towle V, Van Ness PH. Health outcome prioritization as a tool for decision making among older persons with multiple chronic conditions. Arch Intern Med. 2011;171(20):1854–1856. doi:10.1001/archinternmed.2011.424
49. Elwyn G, Vermunt NPCA. Goal-based shared decision-making: developing an integrated model. J Patient Exp. 2020;7(5):688–696. doi:10.1177/2374373519878604
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.