")
Back to Journals » International Medical Case Reports Journal » Volume 13
Primary Pure Squamous Cell Carcinoma of Kidney Associated with Multiple Stag Horn Stones
Authors Hosseinzadeh M, Mohammadzadeh S
Received 8 May 2020
Accepted for publication 25 June 2020
Published 9 July 2020 Volume 2020:13 Pages 261—263
DOI https://doi.org/10.2147/IMCRJ.S261022
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Massood Hosseinzadeh, Sahand Mohammadzadeh
Department of Pathology, Shiraz University of Medical Sciences, Shiraz, Iran
Correspondence: Sahand Mohammadzadeh
Department of Pathology, Shiraz University of Medical Sciences, Shiraz, Iran
Tel +989173078147
Fax +9871323017
Email [email protected]
Abstract: Primary Squamous cell carcinoma (SCC) of the kidney is rarely reported in the literature. It is usually associated with renal stone, and due to lack of clinical symptoms and radiological diagnostic features, patients often present at the late stages of the disease. We reported a 59-year-old woman presented with a longstanding history of flank pain and hematuria. Imaging techniques revealed enlargement of the right kidney associated with multiple staghorn stones. The patient subsequently underwent right radical nephrectomy, and histopathological examination of the mass revealed well-differentiated keratinized squamous cell carcinoma. There was no primary source for her SCC. Although the primary SCC of the kidney is a rare entity, it should be considered in patients with longstanding renal calculi, particularly for large staghorn stones of renal pelvis. On the other hand, conventional imaging could not detect this type of malignancy. In most cases, CT and MRI play an essential role in the diagnosis of such tumors.
Keywords: squamous cell carcinoma, kidney, staghorn stone
Introduction
Primary squamous cell carcinoma of the kidney is rare cancer with poor prognosis at the time of presentation.1 There are only a few case reports in the literature, and urinary bladder and male urethra involve by SCC more frequently than the kidney.2 Although the incidence of this tumor in the kidney is rare, when a renal mass is accompanied by a longstanding renal stone, this differential diagnosis should be considered. Factors that increase the probability of SCC caused by a renal stone include chronic irritation, inflammation, and infection, which can cause squamous metaplasia in the renal pelvis epithelium.3 We reported a case of incidentally detected primary renal SCC associated with staghorn stones and severe hydronephrosis. Ultrasound (US), computed tomography (CT) characteristics are discussed along with histopathologic findings.
Case Presentation
A 59-year-old female patient presented at the hospital with flank pain and hematuria since three months ago. General and physical examinations were normal. Local examination revealed a slight tenderness on the right flank. Examination of the abdomen was unremarkable. The patient had a history of hypertension. The serum urea and creatinine levels were 14 and 1 mg/dl. Urine examination revealed a 4+ hematuria and a 1+ proteinuria. She had no history of prior surgery.
Ultrasound (US) evaluation revealed that the right kidney is enlarged with severe hydronephrosis and thin cortex. Shadow of multiple variable size staghorn stones demonstrated over projection of lower, mid, and upper pole and also in the renal pelvis. Shadow of two isolated solid parts measuring 55 and 35 mm showed within the renal pelvis and attached to the anterior wall. Renal CT revealed a 40 mm staghorn stone in the right renal pelvis with soft tissue mass measured 45mm surrounding the mentioned staghorn stone (Figure 1). Subsequently, the right radical nephrectomy was performed.
 |
Figure 1 Renal CT scan revealed a 40 mm staghorn stone (arrow) in the right renal pelvis. Soft tissue mass measured 45mm is seen surrounding the mentioned staghorn stone. |
Gross examination of the radical nephrectomy specimen revealed enlargement of the right kidney (25x14x13cm). Cut section showed a brown colored staghorn stone in the renal calyces (Figure 2). There was ill-defined gray-white solid cystic mass replacing the renal parenchyma and renal pelvis. The mass was found invading to the perinephric fat. The rest of the kidney appeared cystic and distorted.
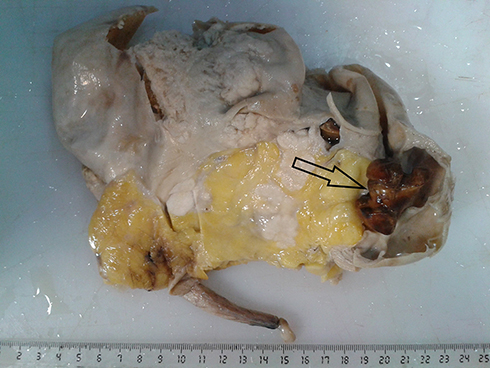 |
Figure 2 On gross examination of radical nephrectomy specimen, the right kidney was enlarged in size, measured 25x14x13cm, and a staghorn stone (arrow) was found in cut sections. |
The microscopic examination of the hematoxylin and eosin-stained tissue revealed that a well-differentiated SCC was infiltrating the renal parenchyma, capsule, and perirenal fat (Figure 3).
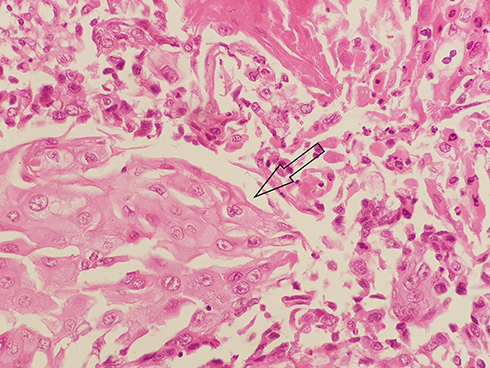 |
Figure 3 Microscopic examination of the hematoxylin and eosin-stained tissue revealed a well-differentiated SCC (arrow). |
Our patient in the present case developed liver metastasis after six months of primary surgical treatment, and one year after pathologic diagnosis, she died because of progressive diseases.
Discussion
The SCC is a rare malignancy of kidney, mostly present in advanced stages which its incidence is 1.4% of all renal malignancies. The literature contains few case reports, so most of the current data about SCC of the kidney are derived from small case series. In general, these tumors have a poor prognosis compare to other urinary tract malignancies. The lack of definite clinical presentation and inconclusive imaging features result in an advanced stage of presentation.4
Clinically, the SCC presents in middle age, its incidence among males and females is almost equal. Presenting symptoms include flank pain, hematuria, and abdominal mass. Significantly, due to nonspecific clinical signs and lack of specific radiological diagnostic features, most cases of the primary renal SCC are underdiagnosed.5,6
Radiologically, the primary SCC of the renal pelvis appears as a solid mass with hydronephrosis. The differential diagnosis of the SCC includes primary and secondary renal neoplasms. CT and MRI can play a better role in the diagnosis of these tumors, particularly in cases with renal stones.2
Histologically, the squamous cell carcinoma presents with extensive squamous differentiation, keratin pearls, and may accompany extensive necrosis. In a large case-series study, Other features such as solid and papillary patterns are observed.7
Radical nephroureterectomy is the treatment of choice in patients with tumors limited to the kidney; however, parenchyma sparing surgeries is also proposed. Available medical literature on this rare malignant entity revealed a poor prognosis, as seen in our case.8
Conclusion
Primary squamous cell carcinoma of the kidney should be considered in patients with staghorn stones. In this setting, imaging techniques such as CT scan and MRI can help clinicians to better diagnose the tumor along with histopathological examination for confirmation.
Ethics
The study was approved by the Iran National Committee for Ethics in Biomedical Research. The patient provided written informed consent before her inclusion within the study and agreed that case details and any accompanying images could be published.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jain A, Mittal D, Jindal A, et al. Incidentally detected squamous cell carcinoma of renal pelvis in patients with staghorn calculi: case series with review of the literature. ISRN Oncol. 2011;2011:1–6. doi:10.5402/2011/620574
2. Mardi K, Kaushal V, Sharma V. Rare coexistence of keratinizing squamous cell carcinoma with xanthogranulomatous pyelonephritis in the same kidney: report of two cases. J Cancer Res Ther. 2010;6(3):339. doi:10.4103/0973-1482.73351
3. Karabulut A, Emir L, Gonultas M, Incel N, Germiyanoglu C, Erol DE. Squamous cell carcinoma located in the renal caliceal system: A case report and review of the literature. Turk J Cancer. 2002;32(1):20–24.
4. Berz D, Rizack T, Weitzen S, Mega A, Renzulli J, Colvin G. Survival of patients with squamous cell malignancies of the upper urinary tract. Clin Med Insights Oncol. 2012;6:CMO–S8103.
5. Palmer CJ, Atty C, Sekosan M, Hollowell CM, Wille MA. Squamous cell carcinoma of the renal pelvis. Urology. 2014;84(1):8–11. doi:10.1016/j.urology.2013.11.020
6. Verma N, Yadav G, Dhawan N, Kumar A. Squamous cell carcinoma of kidney co-existing with renal calculi: a rare tumour. BMJ Case Rep. 2011;2011(mar01 1):bcr1020103388. doi:10.1136/bcr.10.2010.3388
7. Diwan AK, Kabre RS. Primary squamous cell carcinoma of kidney: A rare case report. Int J Med Sci Res Pract. 2015;2(1):49–53.
8. Singh V, Sinha RJ, Sankhwar SN, Mehrotra B, Ahmed N. Squamous cell carcinoma of the kidney–rarity redefined: case series with review of literature. J Cancer Sci Ther. 2010;2:082–085. doi:10.4172/1948-5956.1000028
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.