Back to Journals » Clinical Ophthalmology » Volume 17
Primary Posterior Continuous Circular Capsulorhexis without the Use of Ophthalmic Viscosurgical Device
Received 11 October 2022
Accepted for publication 10 January 2023
Published 2 February 2023 Volume 2023:17 Pages 441—444
DOI https://doi.org/10.2147/OPTH.S386925
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Primary posterior continuous circular capsulorhexis without OVD" [ID 386925].
Views: 142
Pavel Studeny,1,2 Tomas Benda1,2
1Ophthalmology Department, University Clinic Kralovske Vinohrady and 3rd Faculty of Medicine, Charles University, Prague, Czech Republic; 2Eye Centrum SOMICH, Karlovy Vary, Czech Republic
Correspondence: Pavel Studeny, Šípková 36, Karlovy Vary, 36007, Czech Republic, Email [email protected]
Abstract: Performing primary posterior capsulorhexis (PPCCC) during cataract surgery is an effective prevention of secondary cataracts. It is important not to damage the anterior vitreous membrane to minimize the possible complications and adverse side effects of this step of the surgery. Most authors use a viscoelastic material to protect the anterior vitreous membrane, injected into the space between the posterior lens capsule and the vitreous membrane through a small hole in the posterior capsule. The creation of posterior capsulorhexis using 25G forceps under an implanted intraocular lens while continuously filling the anterior chamber with irrigation fluid from an irrigation cannula, without the use of a viscoelastic material is, in our opinion, a safe, fast and cheap technique of PPCCC. This technique could theoretically lead to a lower incidence of postoperative complications such as higher postoperative intraocular pressure or anterior segment inflammatory response.
Keywords: primary posterior continuous curvilinear capsulorhexis, secondary cataract, hydroimplantation
Introduction
Opacification of the posterior lens capsule (PCO) is the most common postoperative complication in patients after cataract surgery.1,2 Its incidence is reported in the literature between 10% and 50%.3,4 The central part of the posterior capsule plays a key role in the development of secondary cataracts, which acts as a surface (scaffold), along which epithelial cells migrate (between the posterior capsule and posterior surface of the artificial IOL), and subsequently cause a proliferative or fibrotic form of cataract. Therefore, the most effective way to prevent secondary cataract is to remove the central part of the posterior capsule.5,6 Yu et al, using Scheimpflug imaging, also observed faster postoperative posterior capsule adhesion to the IOL and stabilization in eyes with PPCCC than in the control group, without PPCCC.7
Primary posterior continuous curvilinear capsulorhexis (PPCCC) was described in an experiment by Castaneda in 1992, followed by Galand and co-authors who suggested the routine use of PPCCC in children as well as adult patients.8,9 Gimbel proposed to combine this technique with the implantation of the optical part of the IOL under the posterior capsule (optic capture).10,11 However, these techniques are not very common in adult patients due to the risk of possible serious complications such as anterior hyaloid membrane disruption, vitreous prolapse, postoperative inflammatory reaction, or macular oedema.12 Some of these postoperative complications (higher postoperative intraocular pressure, postoperative irritation) may be related to the use of the ophthalmic viscosurgical device (OVD) during PPCCC and its insufficient removal from the retrolental space at the end of the surgery.
Although other PPCCC techniques were later described, both before and after implantation of the IOL, most of them use the OVD as protection against anterior vitreous membrane rupture and vitreous prolapse.13–17 Performing PPCCC with 23 G forceps under the IOL with continuous anterior chamber irrigation could theoretically lead to a lower incidence of postoperative complications such as higher postoperative intraocular pressure (IOP) or anterior segment inflammatory response.
Surgical Technique
Written informed consent was obtained from all patients. The procedure was approved by an institutional Ethics committee (EK FN Kralovske Vinohrady, Praha) and followed the tenets of the Declaration of Helsinki.
After standard phacoemulsification, final cleaning of the lens capsule (especially in the periphery) by irrigation/aspiration, and hydroimplantation of the IOL, we continue to perform PPCCC without using any OVD. The stability of the anterior chamber was maintained by an irrigation cannula inserted via one lateral paracentesis. Subsequently, a 23 G curved forceps with a sharp tip (Alio Iridectomy Forceps 23 G, Asiko, USA) was inserted into the paracentesis on the other side. After slightly displacing the IOL in the bag, the end of the forceps was moved under the IOL. The small tearing was made about 2–3 mm from the centre. In our case, we performed tearing in the lower left quadrant. Since the surgeon was sitting behind the patient’s head, the paracentesis was usually performed at No. 3 and 9, and the forceps were held in the surgeon’s dominant (right) hand. Subsequently, the edge of the flap formed was grasped in the forceps, and a circular hole was created by a circular motion of the instruments. The edge of the flap was grasped and re-grasped every quarter-circle similarly to the anterior circular capsulorhexis. Usually, it was necessary to re-capture the fold of the posterior capsule during capsulorhexis about 2–3 times so that manoeuvring with forceps did not occur too much in the periphery. The size of the posterior capsulorhexis was about 4–5 mm so that the edge did not exceed the edge of the optical part of the IOL (a little bit smaller than anterior capsulorhexis). The torn-out central part of the posterior capsule was removed with forceps, and the IOL was returned to its original central position. Finally, the irrigation cannula was pulled out, the wounds were hydrated, and antibiotics injected into the anterior chamber (Supplementary Video).
We have been performing this technique routinely at our clinic for more than two years. For the purposes of this publication, we monitored the occurrence of possible complications in a group of consecutive patients operated on at our clinic in the period May – December 2021. We had no age, gender or type of cataract limitation. We recorded all complications during the PPCCC (Table 1). In total, we performed cataract surgery in 775 patients during this period. The age in our group of patients was 72.5 (± 4.19) in average (min, 49, max 82).
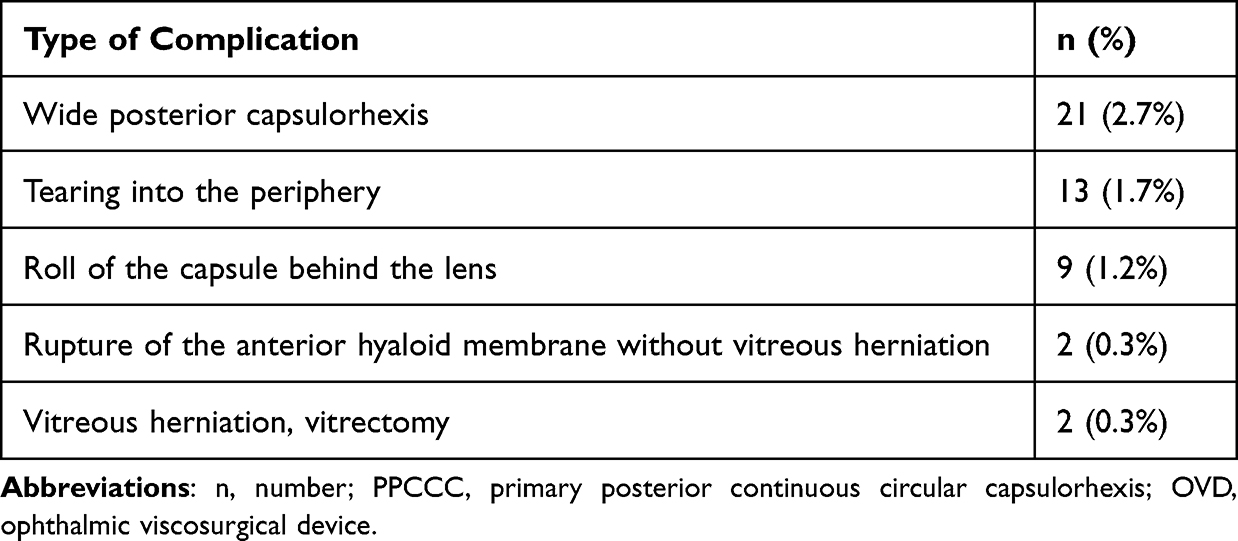 |
Table 1 Number of Complications in a Group of 755 Performed PPCCC Without OVD |
We noticed the following complications: widening of the posterior CCC beyond the edge of the optical part of the IOL (21 cases), tearing the posterior capsule into the periphery (13 cases), leaving part or all of lamella roll of the posterior capsule behind the intraocular lens (9 cases), visible disruption of the anterior hyaloid (vitreous) membrane without vitreous herniation (2 cases), prolapse of the vitreous in front of the intraocular lens and subsequent anterior vitrectomy (2 cases). None of these complications had a major impact on the outcome of the operation, and in none of the cases, we have noticed problems with the position of the lens or other more serious complications. For comparison, all complications in the formation of anterior CCC were also recorded. Capsulorhexis enlargement (larger than optical part of the IOL) was noticed in 6 cases (0.8%), tearing of the capsulorhexis into the periphery in 7 cases (0.9%).
Discussion
Stifter and co-authors proved the safety of the PPCCC, but they did not find higher intraocular pressure, greater inflammatory reaction in the anterior chamber, or a more significant effect on postoperative macular changes compared to eyes in which the posterior capsule was left intact.18–20 However, it is essential that the anterior hyaloid membrane does not get damaged during PPCCC.21 The techniques described so far have been recommended using a OVD to separate the posterior capsule and anterior hyaloid membrane. The IOL is then implanted after the creation of PPCCC. Subsequently, an intraocular lens is implanted. However, this technique can be somewhat stressful, where the surgeon implants the lens into a bag with the back cap open. In addition, leaving part of the OVD under the intraocular lens can theoretically lead to other problems, such as the subjective perception of floaters in the vitreous cavity, a temporary displacement of the intraocular lens towards in conjunction with refractive shift, or an increase of intraocular pressure. Performing PPCCC under an already implanted lens without using a OVD can eliminate these problems.
Most of the complications that occurred in our group were relatively benign and did not affect the outcome of the operation (larger size of the capsulorhexis, tearing into the periphery leaving the torn part of the capsule in the vitreous space). More serious complications, such as anterior vitreous membrane rupture or vitreous herniation, which could theoretically lead to other complications (such as cystoid macular oedema or retinal tear), were relatively low and did not exceed the frequency of complications described after Nd: YAG capsulotomy.22 The authors believe that the low frequency of anterior vitreous membrane rupture or vitreous loss was caused by an irrigation fluid that maintains a positive pressure in the anterior chamber during the procedure. This fluid is likely to fill the space between the posterior capsule and the anterior vitreous membrane, pushes posteriorly the anterior vitreous membrane and prevents vitreous prolapse (Figure 1). After the irrigation, the cannula was extended, the entire PPCCC area was occluded by the optical part of the intraocular lens, and the two spaces were separated. This can explain why the rupture in our group of patients was so rare (only 0.6%). Hence, from this point of view, our technique of PPCCC under the implanted IOL without OVD seems effective, easy, and safe. At this moment in our we routinely doing the PPCCC at our clinics.
 |
Figure 1 Detachment of the anterior vitreous membrane after intraocular lens implantation (intraoperative OCT). Note: 1, back surface of intraocular lens; 2, posterior capsule; 3, anterior vitreous membrane. |
In this work, we describe the modification of surgical technique (PPCCC), its safety and efficiency. We evaluated the preoperative complications, not postoperative complications but generally we did not mark any serious complications after surgery (postoperative IOP rise, pupilary problems or increased anterior chamber inflammation), also any PCO, but this information is only of secondary importance, as within this study, we did not specifically monitor these parameters. It will be the part of our next prospective study.
Conclusion
The creation of posterior capsulorhexis using 25G forceps under an implanted intraocular lens while continuously filling the anterior chamber with irrigation fluid from an irrigation cannula, without the use of a viscoelastic material is a safe, fast and cheap technique of PPCCC.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDonnell PJ, Zarbin MA, Green WR. Posterior capsule opacification in pseudophakic eyes. Ophthalmology. 1983;1983:901548–901553.
2. Kappelhof JP, Vrensen GFJM. The pathology of after cataract; a minireview. Acta Ophthalmol Suppl. 1992;1992:20513–20524.
3. Sundelin K, Almarzouki N, Soltanpour Y, Petersen A, Zetterberg M. Five-year incidence of Nd: YAGlaser capsulotomy and association with in vitro proliferation of lens epithelial cells from individual specimens: a case control study. BMC Ophthalmol. 2014;14:116. doi:10.1186/1471-2415-14-116
4. Ursell PG, Dhariwal M, O’Boyle D, Khan J, Venerus A. 5-year incidence of YAG capsulotomy and PCO after cataract surgery with single-piece monofocal intraocular lenses: a real-world evidence study of 20,763 eyes. Eye. 2020;34(5):960–968. doi:10.1038/s41433-019-0630-9
5. Menapace R. Routine posterior optic buttonholing for eradication of posterior capsule opacification in adults: report of 500 consecutive cases. J Cataract Refract Surg. 2006;32(6):929–943. doi:10.1016/j.jcrs.2006.02.046
6. Menapace R, Schriefl S, Lwowski C, Leydolt C. Impact of primary posterior capsulorhexis on regeneratory after-cataract and YAG laser rates with an acrylic micro-incision intraocular lens with plate haptics: 1-year and 3-year results. Acta Ophthalmol. 2019;97(8):e1130–e1135. doi:10.1111/aos.14156
7. Yu M, Huang Y, Wang Y, Xiao S, Wu X, Wu W. Three-dimensional assessment of posterior capsule-intraocular lens interaction with and without primary posterior capsulorrhexis: an intraindividual randomized trial. Eye. 2022;36(11):2130–2136. doi:10.1038/s41433-021-01815-4
8. Castaneda VE, Legler UF, Tsai JC, et al. Posterior continuous curvilinear capsulorhexis. An experimental study with clinical applications. Ophthalmology. 1992;99(1):45–50.
9. Galand A, Cauwenberge F, Moosavi J. Posterior capsulorhexis in adult eyes with intact clear capsules. J Cataract Refract Surg. 1996;1996:22458–22461.
10. Gimbel HV. Posterior continuous curvilinear capsulorhexis and optic capture of the intraocular lens to prevent secondary opacification in pediatric cataract surgery. J Cataract Refract Surg. 1997;23(Suppl 1):652–656. doi:10.1016/S0886-3350(97)80049-1
11. Mohan A, Sen P, Jain R, Shah C, Jain E, Sen A. Posterior optic buttonholing of intraocular lens implantation through posterior capsulorrhexis margin: a technique of intraocular lens implantation in cases of anterior capsulorrhexis extension in pediatric cataract surgery. Indian J Ophthalmol. 2021;69(4):974–977. doi:10.4103/ijo.IJO_1622_20
12. Van Cauwenberge F, Rakic JM, Galand A. Complicated posterior capsulorhexis: aetiology, management, and outcome. Br J Ophthalmol. 1997;81(3):195–198. doi:10.1136/bjo.81.3.195
13. Hazirolan DO, Altiparmak UE, Aslan BS, Duman S. Vitrectorhexis versus forceps capsulorhexis for anterior and posterior capsulotomy in congenital cataract surgery. J Pediatr Ophthalmol Strabismus. 2009;46:104–107. doi:10.3928/01913913-20090301-12
14. Hugkulstone CE. Intraoperative and early postoperative results of suction posterior capsulorhexis. J Cataract Refract Surg. 2002;28:126–130. doi:10.1016/S0886-3350(01)01129-4
15. Eid AM. Abd-Elhamid Mehany Elwan S, Sabry AM, Moharram HM, Bakhsh AM. Novel technique of pneumatic posterior capsulorhexis for treatment and prevention of posterior capsular opacification. J Ophthalmol. 2019;21(2019):3174709.
16. Gibran SK, Jungkim S, Patil B, Cleary PE. Primary posterior continuous capsulorhexis; a new technique. Br J Ophthalmol. 2006;90(5):655–656. doi:10.1136/bjo.2005.074872
17. Arbisser LB. Review of primary posterior capsulorhexis in cataract surgery. Saudi J Ophthalmol. 2022;36(2):149–156. doi:10.4103/sjopt.sjopt_183_21
18. Stifter E, Menapace R, Neumayer T, Luksch A. Macular morphology after cataract surgery with primary posterior capsulorhexis and posterior optic buttonholing. Am J Ophthalmol. 2008;146(1):15–22. doi:10.1016/j.ajo.2008.02.022
19. Stifter E, Luksch A, Menapace R. Postoperative course of intraocular pressure after cataract surgery with combined primary posterior capsulorhexis and posterior optic buttonholing. J Cataract Refract Surg. 2007;33(9):1585–1590. doi:10.1016/j.jcrs.2007.04.038
20. Stifter E, Menapace R, Luksch A, Neumayer T, Vock L, Sacu S. Objective assessment of intraocular flare after cataract surgery with combined primary posterior capsulorhexis and posterior optic buttonholing in adults. Br J Ophthalmol. 2007;91(11):1481–1484. doi:10.1136/bjo.2007.120535
21. Groot V, Hubert M, Van Best JA, Engelen S, Van Aelst S, Tassignon M-J. Lack of fluorophotometric evidence of aqueous–vitreous barrier disruption after posterior capsulorhexis. J Cataract Refract Surg. 2003;29:2330–2338. doi:10.1016/S0886-3350(03)00341-9
22. Burq MA, Taqui AM. Frequency of retinal detachment and other complications after neodymium: yaglaser capsulotomy. J Pak Med Assoc. 2008;58(10):550–552.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.