Back to Journals » OncoTargets and Therapy » Volume 12
Primary poorly differentiated small cell type neuroendocrine carcinoma of the hypopharynx
Received 30 September 2018
Accepted for publication 17 January 2019
Published 27 February 2019 Volume 2019:12 Pages 1593—1601
DOI https://doi.org/10.2147/OTT.S189241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Yin-Jie Ao, Shui-Hong Zhou
Department of Otolaryngology, The First Affiliated Hospital, College of Medicine, Zhejiang University, Zhejiang Province 310003, China
Abstract: The incidence of primary poorly differentiated neuroendocrine carcinoma (PDNC) of the hypopharynx is ~4%. However, the disease pathogenesis, natural history, and prognostic factors remain poorly understood. We report the case of a 66-year-old man who presented with multiple metastases from primary PDNC of the hypopharynx. Physical examination revealed a ~3×4 cm left cervical mass located at the level III, with tenderness and an unclear boundary. Laryngoscopy revealed a large mass arising from the posterior hypopharynx; glottis and vocal cord movements were invisible. After consultation with our head and neck oncological multidisciplinary team, diagnosis and specific treatment plan were made. Under general anesthesia, a biopsy sample was obtained via suspension laryngoscopy. Routine pathology revealed small cell carcinoma. Immunohistochemical staining identified neoplastic cells that were positive for cytokeratins, CD56, chromogranin A, and synaptophysin. The Ki-67 mitotic index approached 80%. These findings confirmed hypopharyngeal PDNC, and chemotherapy was prescribed. After 7 months, the tumor metastasized to the left side of the anterior chest wall, bilateral lungs, left liver, and skeleton. The soft tissue of the chest wall was biopsied, and pathology revealed PDNC. Subsequent examinations over the next 4 months confirmed multiple liver metastatic lesions. The patient succumbed to the cancer progression a month later. Here, we systematically review the clinical manifestations, pathogenesis, prognostic factors, and treatment of the disease. In conclusion, patients always have a poor prognosis due to a lack of optimal treatment.
Keywords: neuroendocrine carcinoma, hypopharyngeal, Warburg effect, literature review
Introduction
Neuroendocrine carcinoma (NEC) of head and neck is uncommon.1–5 NEC is an aggressive malignant tumor that most commonly affects the larynx.6 The approximate distribution by anatomic site is 9% oral cavity, 12% oropharynx, 35% larynx, 4% hypopharynx, 10% nasopharynx, and 30% nasal cavity and paranasal sinuses.7 Poorly differentiated neuroendocrine carcinoma (PDNC) in the hypopharynx is extremely rare. The 2017 WHO report8 included a section on laryngeal NEC that was a considerable improvement in terminology and classification and divided NEC into well-differentiated, moderately differentiated, and poorly differentiated NEC. Poorly differentiated NEC can be further divided into small cell NEC (SmCC) and large cell NEC (LCNEC).8 The most frequent hypopharyngeal NEC is poorly differentiated. LCNECs or SmCCs are distinct clinicohistopathological entities, but it is unknown which is more common. Only eleven cases engaging the hypopharynx have been described in the English literature. Advanced age, male gender, a history of alcohol consumption, smoking, and irradiation history are inducible etiologic factors.
To date, no treatment for NEC of the hypopharynx has been reported. In addition, recurrence or metastasis needs to be identified through long-term follow-up. Thus, new therapies are essential to improve long-term survival. Although some clinicians have applied targeted therapies to treat NECs of other sites, better targets are needed.
Both conventional oxidative metabolism and glycolytic anaerobic metabolism are available for cancer cells; however, proliferating cancer cells tend to utilize glycolytic anaerobic metabolism even in the presence of abundant oxygen in a concept known as the Warburg effect. The biochemistry underlying the Warburg effect provides a strong explanation for the cause of cancer cell proliferation, and hypoxic markers like glucose transporter-1 (GLUT-1) and hypoxia-inducible factor-1α (HIF-1α) are key factors in this process. Thus, reducing the expression of these markers could be a plausible strategy for treating NEC.
Our previous study9,10 used positron emission tomography/computed tomography (PET/CT) to detect high-level [18F]-fluoro-2-deoxy-D-glucose ([18F]-FDG) uptake in laryngeal NECs, as occurs with other head and neck cancers. Various studies have shown that FDG uptake is associated with metastasis and poor prognosis of many human cancers. Therefore, we proposed that FDG uptake may be useful for the treatment of hypopharyngeal NECs.
Here, we report a patient exhibiting multiple metastases from a primary hypopharyngeal NEC and review the clinical manifestations, possible pathogenesis, clinicopathology, immunohistochemistry, diagnosis, prognostic factors, and therapeutic approaches. The appearance of HIF-1α and GLUT-1 within the carcinoma is also discussed. Finally, we explore the value of [18F]-FDG PET/CT in the diagnosis of hypopharyngeal NECs.
Case report
Presenting concerns
A 66-year-old man presented with a 2-month history of sustained hoarseness, sore throat, and dysphagia. The syndromes progressed 1 month later, and a left neck mass was found accidentally. His past medical history included 20 years of hypertension that was controlled by oral irbesartan (one tablet per day) and 20 years of atrial fibrillation and coronary artery disease (one tablet of metoprolol and warfarin once a day, respectively, and half a tablet of digoxin once a day). He also suffered from pulmonary tuberculosis 40 years ago, which was cured (there were no active tuberculosis lesions on a lung CT, and blood test and sputum cultures were negative).
Clinical findings
On physical examination, a tender 3×4 cm left cervical mass with an unclear boundary was found at the level III. A strobolaryngoscope revealed a large mass arising from the posterior hypopharynx, and movements of both the glottis and vocal cords were invisible (Figure 1). MRI revealed a 28×14 mm mass located in the left hypopharyngeal region, and multiple lymph nodes of the left neck were integrated. T1-weighted images were hypointense, T2-weighted images were hyperintense, and diffusion-weighted imaging was hyperintense. The lesion underwent heterogeneous enhancement following administration of gadolinium-DTPA; the mass was strongly enhanced and the integrated lymph node was peripherally enhanced (Figure 2A and B). PET/CT showed high standardized uptake values (SUVs) of FDG in the left hypopharyngeal regions (SUVmax=8.9) and left cervical lymph node (SUVmax=9.5), but there were no high FDG lesions in other parts of the body (Figure 3A and B).
 | Figure 1 Strobolaryngoscope revealed a large mass arising from the posterior hypopharynx (red arrow). |
 | Figure 2 (A, B) MRI revealed the mass (red arrow) was strongly enhanced and the integrated lymph node (blue arrow) was peripherally enhanced. |
 | Figure 3 (A, B) PET/CT showed high SUV of FDG in the left hypopharyngeal regions (SUVmax=8.9) (red arrow) and left cervical lymph node (SUVmax=9.5) (blue arrow), but there were no high FDG lesions in other parts of the body. |
Therapeutic focus and assessment
Our head and neck oncological multidisciplinary team (MDT; Department of Otolaryngology Head-Neck Surgery, Maxillofacial Surgery, Radiology, Radiotherapy, Microsurgery, Thoracic Surgery, and Vascular Surgery) discussed the preoperative possible diagnosis, therapeutic modalities, and whether further postoperative treatment was needed if surgery was performed. The MDT reached a consensus that the diagnosis was hypopharyngeal carcinoma with cervical lymph node metastasis (T2N2M0) and that the treatment would be determined according to frozen section results. If the frozen sections showed small cell carcinoma/malignant tumor or poorly differentiated carcinoma, the patient would first receive concurrent chemoradiotherapy (CCRT). If the frozen section results suggested other type carcinomas, treatment would be partial laryngopharyngectomy plus bilateral neck dissection (II–VI) with postoperative chemoradiotherapy according to NCCN guidelines regarding hypopharyngeal carcinoma. Under general anesthesia, a biopsy sample was obtained via suspension laryngoscopy. Analysis of the frozen section suggested the presence of a small cell malignant tumor (most likely small cell carcinoma).
According to the preoperative plan developed by the MDT, CCRT was performed. Routine pathology (Figure 4) revealed that the small tumor cells were uniform in size, exhibited marked heteromorphy, and were arranged into nests and cords with sparse cytoplasm. Immunohistochemical staining revealed that the primary tumor was positive for cytokeratins (Figure 5A), CD56 (Figure 5B), chromogranin A (Figure 5C), and synaptophysin (Syn; Figure 5D) and negative for p63, CK7, and CD45. The Ki-67 (Figure 5E) mitotic index approached 80%. These histopathological features confirmed the presence of hypopharyngeal PDNC. The patient received six cycles of chemotherapy.
 | Figure 4 Routine pathological image. |
 | Figure 5 Immunohistochemical staining revealed that the primary tumor was positive for cytokeratins (A), CD56 (B), chromogranin A (C), synaptophysin (D), and Ki-67 (E). |
Follow-up and outcomes
The patient received regular follow-ups. On March 14, 2017, CT revealed that the lesion in the hypopharynx had shrunk markedly and the metastatic left lymph nodes had disappeared (Figure 6). On March 21, 2017, CT revealed the presence of irregular soft tissue in the left side of the anterior chest wall, sized ~2.7×4.7 cm, invading the corresponding ribs, and multiple high-density nodules in the bilateral lungs (Figure 7). Ultrasonography revealed a hypoechoic lesion in the left liver (Figure 8). Whole body bone imaging revealed tracer concentrated in the right skull, left rib 4, left rib 8, rib 9, right scapula, the vertebral body of lumbar 5, the left superior iliac spine, and right sacroiliac joint (Figure 9). Then, a left chest nodule was biopsied. Immunohistochemical staining revealed that the nodule was positive for chromogranin A, CD56, and Syn. The Ki-67 mitotic index approached 80%. These findings confirmed metastatic PDNC. On April 8, 2017, CT revealed multiple liver metastatic lesions, and swollen metastatic lymph nodes appeared in the hepatogastric gap and porta (Figure 10). On June 14, 2017, CT revealed no invisible swollen lymph nodes bilaterally (Figure 11). No further treatments were given, and the patient died of multiple metastases on August 2017.
 | Figure 6 CT revealed that the lesion in the hypopharynx had shrunk markedly and the metastatic left lymph nodes had disappeared. |
 | Figure 7 CT revealed the presence of irregular soft tissue in the left side of the anterior chest wall (red arrow), sized ~2.7×4.7 cm, invading the corresponding ribs, and multiple high-density nodules (blue arrow) in the bilateral lungs. |
 | Figure 8 Ultrasonography revealed a hypoechoic lesion in the left liver (red arrow). |
 | Figure 9 Whole body bone imaging revealed tracer concentrated in the right skull, left rib 4, left rib 8, rib 9, right scapula, the vertebral body of lumbar 5, the left superior iliac spine, and right sacroiliac joint. |
 | Figure 10 CT revealed multiple liver metastatic lesions (red arrow), and swollen metastatic lymph nodes appeared in the hepatogastric gap and porta (blue arrow). |
 | Figure 11 CT revealed no invisible swollen lymph nodes bilaterally. |
Discussion
In 1972, Olofsson and van Nostrand6 reported the first case of primary extrapulmonary NEC arising in the head and neck. Since then, it has been reported at multiple sites of the head and neck throughout the upper aerodigestive tract, including the larynx, paranasal sinuses, and salivary glands.11 However, the hypopharynx is an unusual site for this tumor. In 1980, Ferlito and Polidoro12 reported the first case of primary NEC in the hypopharynx. We performed a clinical review of the English language literature and found 12 cases (including the current case) that have been documented (Table 1). Most predominant cases occurred in males: ten patients were male and two were female (male:female ratio, 5:1). The mean age was 61.9 years (range, 35–75 years). There was a history of cigarette smoking in nine patients and alcohol consumption in ten patients. Most tumors were located in the pyriform sinus, apart from one case located in the base of the tonsil to the pyriform sinus. Neck mass and dysphagia were the most frequently documented symptoms; both occurred in 50% (6/12) of cases. Other symptoms included weight loss (33.3%, 4/12 cases), dyspnea (25%, 3/12), hoarseness (16.8%, 2/12 cases), and throat pain (8.3%, 1/12 cases). Histologically, half of the cases (6/12) were pure SmCCs with classical macroscopic features and the remaining half (50%, 6/12) were SmCCs combined with squamous cell carcinoma. Of all patients, seven (58.3%) received radiotherapy. Of these, five (71.4%) received a radical operation plus postoperative radiotherapy and two (28.5%) received only radiotherapy. Two patients (16.6%) had incomplete operative excision, one of whom accepted chemotherapy afterward. Of the remaining patients, one (8.3%) received only a radical operation, one (8.3%) received chemotherapy exclusively, and one (8.3%) died without any treatment. Six (50%) patients died within a year, four (33.3%) patients died within 2 years, and the other two patients lived for 55 months and 26 months, respectively. Lymph node metastases are the most common; five (41.6%) cases had lymph node metastases alone and five (41.6%) cases had lymph node metastases together with bone, soft tissue, liver, or lung metastases. The other patients had only bone metastases or bone combined with liver metastases. Death was always caused by metastatic disease rather than by local recurrence. Systematic analyses of the clinical manifestations and treatment of metastases are rarely reported. Clues regarding the appearance of distant metastasis and local recurrence are vague, even though it is a relevant prognostic factor.
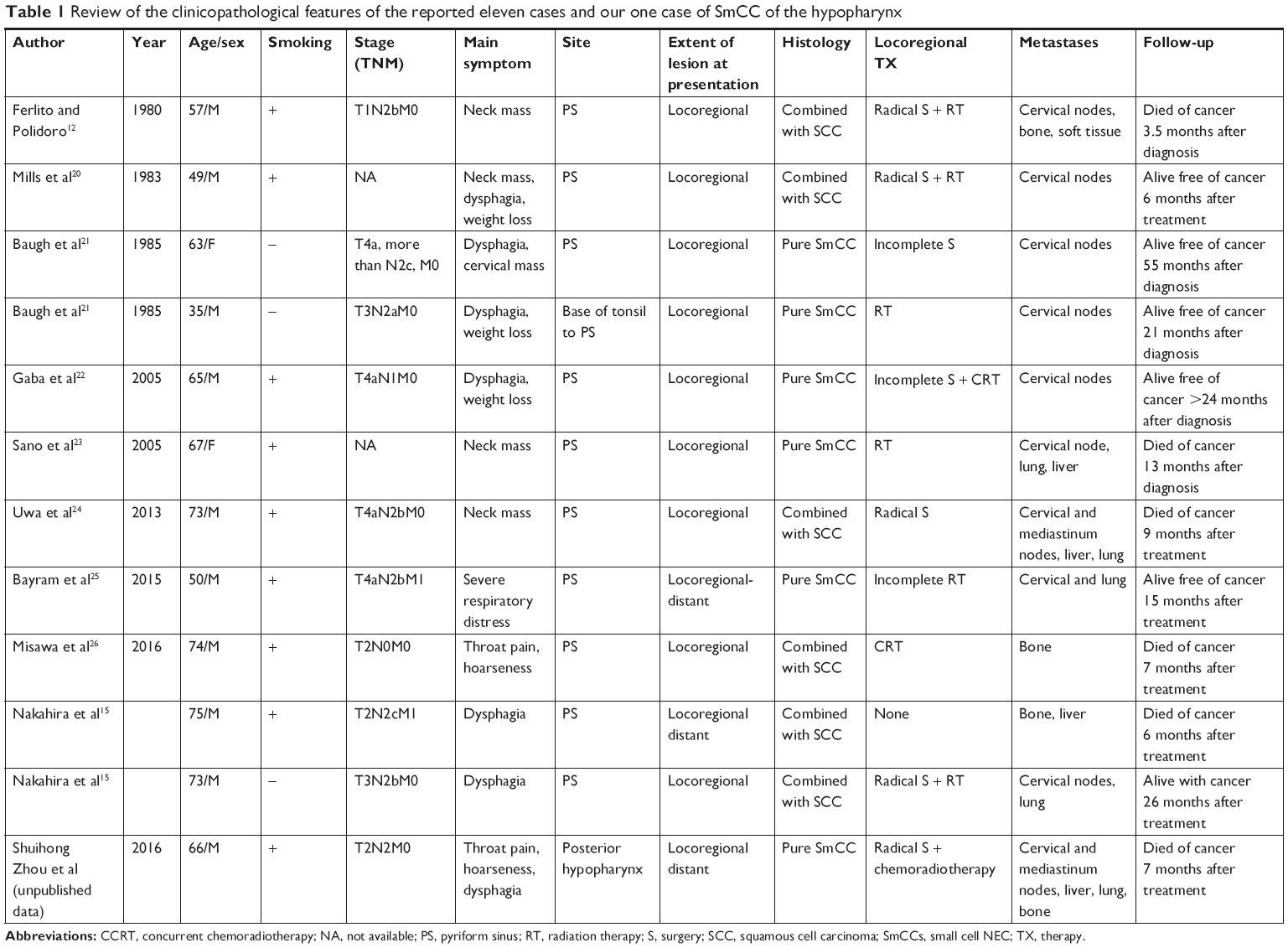 | Table 1 Review of the clinicopathological features of the reported eleven cases and our one case of SmCC of the hypopharynx |
There is no consensus on the treatment of NEC of the hypopharynx. Surgical operation is not always preferable because it decreases the quality of postoperative life severely. Therefore, combined chemoradiotherapy aiming at organ preservation is preferred.13 However, in patients whose deglutition has been severely invaded by advanced hypopharyngeal tumors, radical surgery needs to be implemented rather than chemoradiotherapy. In a study by Takagawa et al,13 the primary lesion was unknown and appropriate surgery was possible because the metastases occurred in one organ at a time. Kuan et al14 divided NEC of the head and neck into sinonasal and nonsinonasal, according to the site of the primary tumor. They reported that patients with sinonasal primary tumors experienced improved survival with surgery, whereas those with nonsinonasal tumors had better survival with radiation therapy.14 In contrast, Nakahira et al15 successfully achieved local control in all patients, regardless of the therapeutic modality used for the primary tumor. This suggests that an organ preservation strategy with platinum-based chemotherapy and concurrent radiotherapy for the primary lesion is also reasonable for SmCC of the hypopharynx.15 However, in contrast to SmCC of the larynx, there is a higher risk of failed completion of chemoradiotherapy in patients whose deglutition has been already severely compromised by advanced hypopharyngeal tumors, and these patients might be candidates for radical surgery, if possible, instead of chemoradiotherapy.15 In the current case, we selected chemotherapy after the diagnosis of SmCCs. After treatment, the primary lesion was controlled and the neck showed no enlarged lymph nodes at follow-up. Unfortunately, the patient revealed metastatic disease after chemotherapy.
In this literature review, we reviewed the eleven cases of primary SmCC of the hypopharynx documented to date and combined the data with those from the current patient. The mean length of follow-up was 16.4 months (range, 3.5–55 months). All patients died during follow-up. The 1- and 2-year survival rates were 33.3% (four cases) and 16.7% (two cases), respectively. A total of 41.6% of the patients (five cases) died within 1 year. Overall, NEC of the hypopharynx has an extremely poor outcome; nevertheless, the small number of reported cases means that these statistics may not be reliable. Therefore, it is essential that additional cases are collected to calculate an accurate survival rate and determine appropriate prognostic factors and treatments.
Ioannou et al16 immunostained 30 NEC biopsy samples with antibodies against HIF-1α and found that HIF-1α overexpression is common in multiple types of carcinomas and is associated with aggressive tumor behavior and overall poor prognosis. Lee et al17 collected SCNEC samples from 111 patients treated with platinum-based chemotherapy as a front-line regimen between January 2002 and December 2009. They found that low expression of HIF-1α may be a useful predictor of better prognosis in NEC patients treated with front-line platinum-based chemotherapy. GLUT-1 overexpression is frequently observed in cancer, and it is associated with a high metabolic rate and rapid growth of cells in often-hypoxic tumor areas.14 Increased GLUT-1 expression is associated with a range of carcinomas, including pulmonary NECs, and is strongly correlated with neuroendocrine differentiation/grade.14 Miyoshi et al18 found that NECs generally had similar genomic profiles and promising therapeutic targets such as the PI3K/Akt/mammalian target of rapamycin (mTOR) pathway. For example, genetic alterations in the PI3K/Akt/mTOR pathway were reported in NEC,18 suggesting that this pathway may play a critical role in NEC tumorigenesis.18 In the present patient, immunohistochemistry also showed that the hypopharyngeal NEC was positive for GLUT-1 and HIF-1α. Thus, we propose that a poor prognosis in PDNC may be related to markers such as HIF-1α, GLUT-1, and mTOR. Targeted therapies for these markers may improve the progression-free survival time of patients.
According to immunohistochemical staining in the current case, the Ki-67 mitotic index approached 80%, which confirmed the presence of hypopharyngeal PDNC. Patients with a high Ki-67 proliferation index always exhibit highly proliferative tumors. Proliferating cells express Ki-67, which also provides criteria to determine the growth fraction of individual tissues and tumors. Takagawa et al13 reported high Ki-67 positivity in a patient with primary hypopharyngeal NEC with distant metastases. Lee et al19 reported the case of a patient with a Ki-67 mitotic index that approached 70% and made the diagnosis of LCNEC of the hypopharynx. Nakahira et al15 also reported two cases of primary small cell carcinoma of the hypopharynx with high Ki-67 positivity. This high Ki-67 expression is consistent with the current case.
Conclusion
In conclusion, SmCCs of the hypopharynx are rare, and prognoses are poor. Prognostic factors include GLUT-1 and Ki-67 levels, alcohol consumption, smoking history, and distant metastasis. No optimal treatment for such disease has yet been established.
Ethics approval
The case report was approved by the Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University (approval no. 2018011). Written informed consent was obtained from the patient’s next of kin.
Acknowledgments
This research was supported by the National Natural Science Foundation of China (grant no. 81372903) and Science and Technology Department of Zhejiang Province, China (no. 2016C33144).
Disclosure
The authors report no conflicts of interest in this work.
References
Ying HF, Bao YY, Zhou SH, Chai L, Zhao K, Wu TT. Submucosal small-cell neuroendocrine carcinoma of the larynx detected using 18F-fluorodeoxyglucose positron emission tomography/computed tomography: a case report and review of the literature. Oncol Lett. 2014;8(3):1065–1069. | ||
Chai L, Ying HF, Wu TT, et al. Clinical features and hypoxic marker expression of primary sinonasal and laryngeal small-cell neuroendocrine carcinoma: a small case series. World J Surg Oncol. 2014;12(1):199. | ||
Chen XH, Bao YY, Zhou SH, Wang QY, Zhao K. Palatine tonsillar metastasis of small-cell neuroendocrine carcinoma from the lung detected by FDG-PET/CT after tonsillectomy: a case report. Iran J Radiol. 2013;10(3):148–151. | ||
Qiu J, Lin W, Zhou ML, Zhou SH, Wang QY, Bao YY. Primary small cell cancer of cervical trachea: a case report and literature review. Int J Clin Exp Pathol. 2015;8(6):7488–7493. | ||
Wang KR, Jia YJ, Zhou SH, et al. Cutaneous and subcutaneous metastases from atypical laryngeal carcinoids: case report and review of the literature. Medicine. 2016;95(7):e2796. | ||
Olofsson J, van Nostrand AW. Anaplastic small cell carcinoma of larynx. Case report. Ann Otol Rhinol Laryngol. 1972;81(2):284–287. | ||
Pointer KB, Ko HC, Brower JV, et al. Small cell carcinoma of the head and neck: an analysis of the National Cancer Database. Oral Oncology. 2017;69:92–98. | ||
Gale N, Poljak M, Zidar N. Update from the 4th edition of the World Health organization classification of head and neck tumours: what is new in The 2017 who blue book for tumours of the hypopharynx, larynx, trachea and parapharyngeal space. Head Neck Pathol. 2017;11(1):23–32. | ||
Zhao K, Luo XM, Zhou SH, et al. 18F-fluorodeoxyglucose positron emission tomography/computed tomography as an effective diagnostic workup in cervical metastasis of carcinoma from an unknown primary tumor. Cancer Biother Radiopharm. 2012;27(10):685–693. | ||
Zhao K, Yang SY, Zhou SH, Dong MJ, Bao YY, Yao HT. Fluorodeoxyglucose uptake in laryngeal carcinoma is associated with the expression of glucose transporter-1 and hypoxia-inducible-factor-1α and the phosphoinositide 3-kinase/protein kinase B pathway. Oncol Lett. 2014;7(4):984–990. | ||
Renner G. Small cell carcinoma of the head and neck: a review. Semin Oncol. 2007;34(1):3–14. | ||
Ferlito A, Polidoro F. Simultaneous primary oat cell carcinoma (apudoma) and squamous cell carcinoma of the hypopharynx. ORL J Otorhinolaryngol Relat Spec. 1980;42(3):146–157. | ||
Takagawa R, Tanaka K, Yamada M, et al. Primary neuroendocrine carcinoma of the hypopharynx: a case report. Dis Esophagus. 2011;24(3):E26–E31. | ||
Kuan EC, Alonso JE, Tajudeen BA, Arshi A, Mallen-St Clair J, St John MA. Small cell carcinoma of the head and neck: a comparative study by primary site based on population data. Laryngoscope. 2017;127(8):1785–1790. | ||
Nakahira M, Kuba K, Matsumura S, Sugasawa M. Primary small cell carcinoma of the hypopharynx: a report of two cases and review of nine additional cases. Case Rep Otolaryngol. 2017;2017(1):1–7 Article ID 8143145. | ||
Ioannou M, Papamichali R, Kouvaras E, et al. Hypoxia inducible factor-1 alpha and vascular endothelial growth factor in biopsies of small cell lung carcinoma. Lung. 2009;187(5):321–329. | ||
Lee GW, Go SI, Cho YJ, et al. Hypoxia-inducible factor-1α and excision repair cross-complementing 1 in patients with small cell lung cancer who received front-line platinum-based chemotherapy: a retrospective study. J Thorac Oncol. 2012;7(3):528–534. | ||
Miyoshi T, Umemura S, Matsumura Y, et al. Genomic profiling of large-cell neuroendocrine carcinoma of the lung. Clin Cancer Res. 2017;23(3):757–765. | ||
Lee WI, Ameratunga M, du Plessis J, Gan H. Hypopharyngeal large cell neuroendocrine carcinoma. BMJ Case Rep. 2015;2015:bcr2015211908. | ||
Mills SE, Cooper PH, Garland TA, Johns ME. Small cell undifferentiated carcinoma of the larynx: report of two patients and review of 13 additional cases. Cancer. 1983;51(1):116–120. | ||
Baugh RF, Wolf GT, McClatchey KD. Small cell carcinoma of the head and neck. Head & Neck Surgery. 1986;8(5):343–354. | ||
Gaba A, Mbaoma R, Breining D, Smith RV, Beitler JJ, Haigentz Jr M. Unusual sites of malignancies: case 1. Small-cell carcinoma of the hypopharynx. Journal of Clinical Oncology. 2005;23(9):2094–2096. | ||
Sano M, Kitahara N, Toma M. Hypopharyngealsmallcell carcinoma: acasereport. Auris Nasus Larynx. 2005;32(3):319–322. | ||
Uwa N, Terada T, Mohri T, et al. Combined small cell carcinoma of the hypopharynx. Auris Nasus Larynx. 2013;40(1):106–109. | ||
Bayram A, Akay E, Göksu SS, Ozcan I, Primary small cell carcinoma of the hypopharynx: a case report of a rare tumor. Case Reports in Otolaryngology. 2015:1–4. | ||
Misawa K, Kawasaki H, Endo S, et al. Primary combined small and squamous cell carcinoma of the hypopharynx: a case report. Molecular and Clinical Oncology. 2016;4(5):709–714. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.