Back to Journals » International Medical Case Reports Journal » Volume 17
Primary Omentum Malignant Hemangiopericytoma Present with Acute Abdomen
Authors Nasr B ![]() , Gazem SK, Al-Gahafy RS, Al-Hawbani MA
, Gazem SK, Al-Gahafy RS, Al-Hawbani MA
Received 19 April 2024
Accepted for publication 16 June 2024
Published 3 July 2024 Volume 2024:17 Pages 653—657
DOI https://doi.org/10.2147/IMCRJ.S469084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Burkan Nasr,1 Sameh Khalil Gazem,2 Rashad Saleh Al-Gahafy,3 Mohammed A Al-Hawbani3
1Department of General Surgery, University of Aden, Aden, Yemen; 2Department of General Surgery, Al-Hawbani Hospital, Bajel, Al-Hodeidah, Yemen; 3Department of Radiology, Al-Hawbani hospital, Bajel, Al-Hodeidah, Yemen
Correspondence: Burkan Nasr, Email [email protected]
Abstract: The greater omentum primary malignant tumors are rare, with less than 50 cases reported. Malignant hemangiopericytomas constitute only four of these cases. The common clinical manifestations of a malignant omental tumor are abdominal mass and pain. We report on a woman 38 years old who came to the hospital’s emergency department with a finding consisting of intestinal obstruction (abdominal pain, constipation, abdominal distention, and vomiting), and during a clinical examination a mass was discovered in the lower half of her abdomen. She had been experiencing these symptoms for three days before her arrival. During a clinical examination, a large size, hard mobile mass was discovered in the lower half of her abdomen. The patient underwent an abdominal CT scan which indicated the presence of a sizable, soft tissue mass located within the abdominal and pelvic region, exerting pressure on the small bowel loops, with mild free ascites. Due to the patient’s acute abdomen, an exploration laparotomy was performed, revealing a large mass in the omentum measuring 20× 20× 10 cm and weighing 3 kg. The mass, along with the omentum, was completely removed, and histopathology confirmed a malignant hemangiopericytoma.
Keywords: omental cancer, acute abdomen, surgical exploration
Introduction
Primary omental malignancies include liposarcoma, hemangiopericytoma, fibrosarcoma, leiomyosarcoma, mesothelioma, desmoid tumor, and malignant fibrous histiocytoma. They are rare, making their diagnosis quite challenging. They are usually found in people in their 50s or 60s.1,2
In 1942 Stout and Murray described hemangiopericytoma as a distinctive soft tissue neoplasm. Hemangiopericytoma is a type of tumor thought to come from Zimmerman pericytes displaying signs of myoid or myofibroblast differentiation.3–5 The World Health Organization has classified hemangiopericytoma as a solitary fibrous tumor (SFT) that occurs outside the pleura as either benign or malignant with an overall incidence of 0.6%. While there have been twenty documented instances of hemangiopericytoma, the literature only mentions four cases of hemangiopericytoma.2,6
Case Presentation
A woman aged 38 arrived at the emergency department of our hospital with symptoms including abdominal pain, constipation, vomiting, and abdominal distension. These symptoms had started three days earlier. However, the patient had a history of abdominal discomfort and distension due to swelling that began in the epigastric area five years earlier. As the patient lives far away, the patient had been taking pain relievers on her own after going to a peripheral rural clinic for assistance. During our examination the patient was fully conscious but seemed unwell and dehydrated. A mass was discovered across the lower half of her abdomen, causing abdominal distention. The mass measured 20×20 cm in size and was hard, non-pulsatile, and tender to palpation. It disappeared when the patient raised her head against resistance and was mobile. The laboratory result complete blood counted HP 7,5 WBC 14. An abdominal ultrasound revealed a large, pelvic-abdominal, heterogeneous, hypoechoic, and highly vascularized soft tissue mass measuring 20×18×10 cm in size, showing high blood flow on color Doppler study. Multiple tortuous, dilated blood vessels with mild to moderate free fluid were also detected in the peritoneal cavity. After receiving intravenous fluids containing ranger lactate, the patient underwent an abdominal CT scan with IV contrast. The results of the scan revealed a clear, large, well-defined, heterogeneous soft tissue mass lesion measuring 20×16×9 cm, found in the lower abdomen and pelvis. These findings were similar to those of a gastrointestinal stromal tumor (GIST) or desmoid tumor [Figure 1].
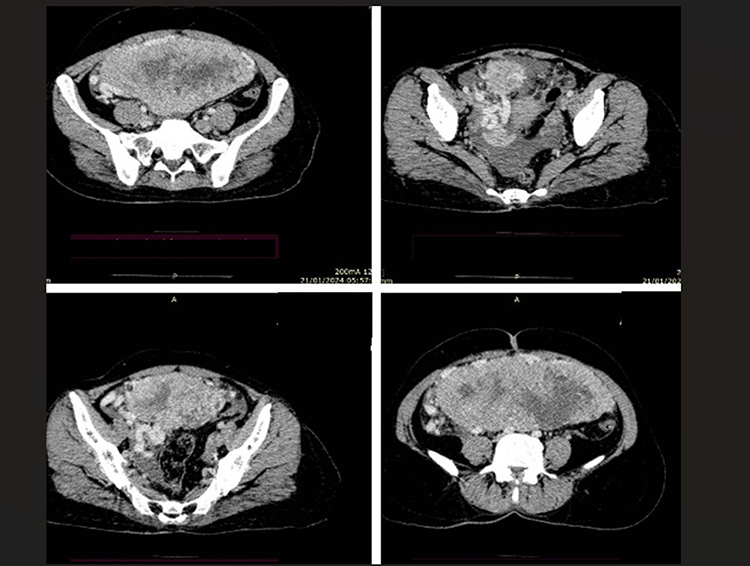 |
Figure 1 Abdominal CT scan with IV contrast, revealing a large, well-defined, heterogeneous soft tissue mass lesion measuring 20×16×9 cm, in the lower abdomen and pelvis. |
As the patient had an acute abdomen, we decided on exploration laparotomy. During the surgery, a large mass was discovered that infiltrated the greater omentum, measuring about 20×20×10 cm and weighing 3 kg. The mass was close to and compressing the small bowel loops and was associated with mild ascites. There was also free blood in the peritoneal cavity. The mass, along with the omentum, was completely excised and sent for histopathology, while also ensuring a safe margin was maintained during the excision [Figure 2].
 |
Figure 2 During the surgery, a large mass was discovered that infiltrated the greater omentum. |
The patient was discharged four days after the operation with good general condition. However, the histopathology results revealed that the mass under the microscope was a tumor growth formed of a sheet of spindle cells having oval-shaped nuclei and an eosinophilic to clear cytoplasm, with foci of moderate nuclear atypia and foci of necrosis also seen. Also noted was separate omental fatty tissue, showing patchy mild mixed inflammation. Mitotic figures were not encountered, and the examination of the immunoassayed section showed the following: CD34, diffuse positive; CD99, weak positive; CD117 and Dog-1, negative; ki67, low proliferation index less than 1%; and SMA, DESMIN, S-100.STAT6 CD31, D2-40, HMB-45, ER, MDM2CDK4, and Bc12, negative. The result of analysis was that the tumor is a malignant hemangiopericytoma. Therefore, the patient was referred to an oncology center for further follow-up.
Discussion
Primary benign hemangiopericytomas of the omentum make up a fraction less than 2% of all soft tissue tumors, while malignant hemangiopericytomas constitute less than 1% of all hemangiopericytomas.4,7 There have been only four instances recorded of this condition [Table 1]. In hemangiopericytoma cells it is uncommon to find markers, such as desmin and actin, which makes immunohistochemistry not always a reliable diagnostic tool.5 On the other hand, hemangiopericytoma cells express antigens such as CD34 (100%), CD99, and Bcl-2 (70–90%).1,4,8 STAT6 serves as a reliable immunohistochemical indicator for diagnostic purposes,9 but in our case CD34 was present, whereas STAT6 was not present. In order to identify hemangiopericytoma it is essential to conduct an assessment including running necessary laboratory tests and carrying out imaging studies.10 Magnetic resonance imaging (MRI) is a more effective tool than using a computer tomographic (CT) scan to assess the size of the tumor and how it interacts with tissues. In our case, we proceeded with the surgery after reviewing the CT scan results as the size of the lesion necessitated surgery due to rupture of tumor with intra-peritoneal bleeding regardless of the result of tumor type. Additionally, our hospital is currently experiencing resource constraints, and many patients are unable to afford extra investigations.
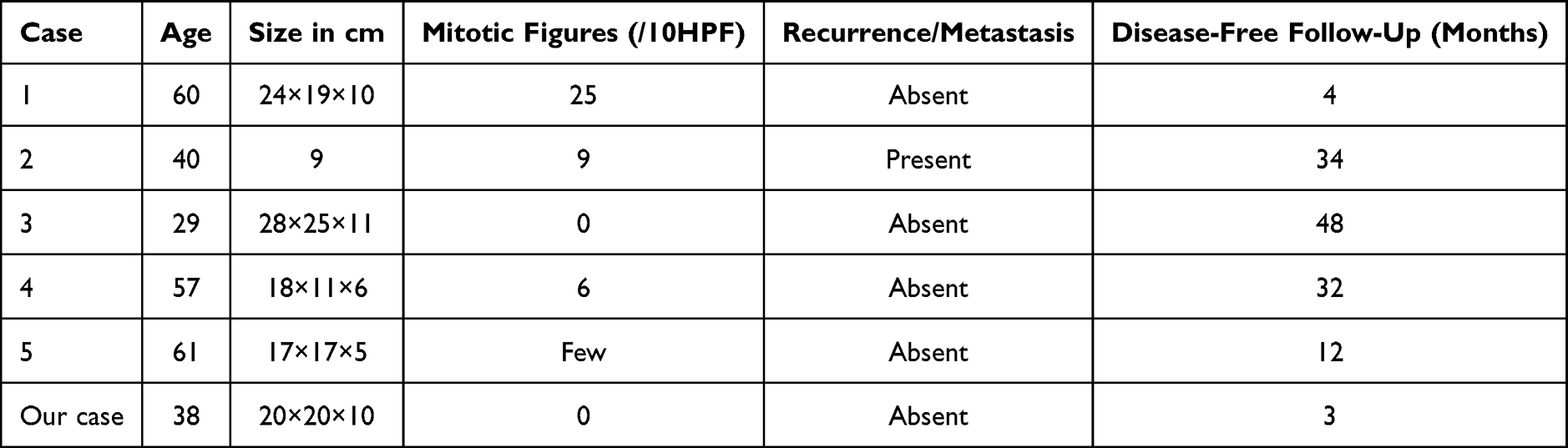 |
Table 1 The Five Cases Recorded with This Condition |
The vascular tumor under consideration necessitates a treatment regimen that involves surgical intervention, chemotherapy, and radiotherapy to achieve good outcomes.
The primary method of treatment is en-bloc surgical excision11 When surgery is not feasible, radiotherapy is often the option. According to the literature, there is not support for the use of adjuvant chemotherapy.10,1213 Before proceeding with surgery, it is advisable to conduct a CT or ultrasound-guided biopsy along with staining for diagnosis and treatment. This aids not only in confirming the diagnosis, but also in comprehending the dimensions and prognosis of the mass.10,14,15
Conclusion
This report describes a rare case of primary omental malignant hemangiopericytoma with acute abdomen. The surgery to remove the tumor only effected part of management. Early detection is important with this kind of tumor, for early surgical intervention, and to improve the prognosis.
Statement of Ethics and Informed Consent
Written informed consent was obtained from the patient, including for the publication of the paper and its content, and approval by Institutional Al-Hawbani hospital, Bajel, Al-Hodeidah, Yemen, was obtained for the publication of this work.
Acknowledgments
The authors would like to express their utmost gratitude to the patient in their involvement in this scientific work.
The authors also would like to express their utmost gratitude to the admin team of Al-Hawbani hospital for their help to collect data and in the use of figures to publish this case report.
Disclosure
The authors declare no competing interests or conflicts in this work.
References
1. Fischerova D, Indrielle-Kelly T, Burgetova A. Yolk sac tumor of the Omentum: a Case Report and Literature Review. Diagnostics. 2022;12(2):304. doi:10.3390/diagnostics12020304
2. Jung C-Y, Bae J-M. Primary omental malignant solitary fibrous tumour, an extremely rare malignancy: a case report and review of the literature. Arab J Gastroenterol. 2019;20(2):114–116. doi:10.1016/j.ajg.2018.12.001
3. Gengler C, Guillou L. Solitary fibrous tumour and haemangiopericytoma: evolution of a concept. Histopathology. 2006;48(1):63–74. doi:10.1111/j.1365-2559.2005.02290.x
4. Radulescu D, Pripon S, Ciuleanu TE, Radulescu LI. Malignant primary pulmonary tumor with hemangiopericytoma-like features: conventional hemangiopericytoma versus solitary fibrous tumor. Clin Lung Cancer. 2007;8(8):504–508. doi:10.3816/CLC.2007.n.037
5. Espat NJ, Lewis JJ, Leung D. Conventional hemangiopericytoma: modern analysis of outcome. Cancer. 2002;95(8):1746–1751. doi:10.1002/cncr.10867
6. Zong L. Giant solitary fibrous tumor arising from greater omentum. World J Gastroenterol. 2012;18(44):6515. doi:10.3748/wjg.v18.i44.6515
7. Pasquali S, Gronchi A, Strauss D. Resectable extra-pleural and extra-meningeal solitary fibrous tumours: a multi-centre prognostic study. Eur J Surg Oncol. 2016;42(7):1064–1070. doi:10.1016/j.ejso.2016.01.023
8. Fletcher CDM, Unni K, Mertens F. World Health Organization classification of tumours. Pathology and genetics of tumours of soft tissue and bone. IARC press, 2002.
9. Doyle LA, Vivero M, Fletcher CD, Mertens F, Hornick JL. Nuclear expression of STAT6 distinguishes solitary fibrous tumor from histologic mimics. Mod Pathol. 2014;27(3):390–395. doi:10.1038/modpathol.2013.164
10. Shahid S, Khan H, Mehmood M, Rage KA, Saeed S. Malignant haemangiopericytomas of omentum presenting as left inguinal hernia: a case report. Ann Med Surg. 2021;62:298–301. doi:10.1016/j.amsu.2021.01.070
11. Rajeev R, Patel M, Jayakrishnan TT, Johnston FM, Bedi M, Charlson J, Turaga KK. Retroperitoneal solitary fibrous tumor: surgery as first line therapy. Clin Sarcoma Res. 2015;5:1–7. doi:10.1186/s13569-015-0034-y
12. Perdikakis E, de Bree E, Giannikaki E, Chryssou EG, Valatsou C, Karantanas A. Pelvic hemangiopericytoma: the role of diffusion weighted imaging in targeting the biopsy site and in monitoring the tumour response to radiotherapy. Radiol Oncol. 2011;45(1):22–26. doi:10.2478/v10019-010-0045-5
13. Penel N, Amela EY, Decanter G, Robin YM, Marec-Berard P. Solitary fibrous tumors and so-called hemangiopericytoma. Sarcoma. 2012;2012:690251. doi:10.1155/2012/690251
14. Errani C, Traina F, Perna F, Calamelli C, Faldini C. Current concepts in the biopsy of musculoskeletal tumors. Sci World J. 2013;2013:538152. doi:10.1155/2013/538152
15. Soudack M, Nachtigal A, Vladovski E, Brook O, Gaitini D. Sonographically guided percutaneous needle biopsy of soft tissue masses with histopathologic correlation. J Ultrasound Med. 2006;25(10):1271–1277. doi:10.7863/jum.2006.25.10.1271
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.