Back to Journals » OncoTargets and Therapy » Volume 19
Primary Hepatic Epithelioid Gastrointestinal Stromal Tumor: A Rare Case
Authors Yang Q, Fang X, Wang L, Lu J ![]()
Received 3 April 2026
Accepted for publication 15 May 2026
Published 21 May 2026 Volume 2026:19 613626
DOI https://doi.org/10.2147/OTT.S613626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tohru Yamada
Qijun Yang,1,* Xixi Fang,1,2,* Lingling Wang,3 Jun Lu1,4
1Department of Hepatopancreatobiliary Surgery, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, People’s Republic of China; 2School of Medicine, Hangzhou Normal University, Hangzhou, People’s Republic of China; 3Department of Pathology, Affiliated Hangzhou First People’s Hospital, School of Medicine, Westlake University, Hangzhou, People’s Republic of China; 4School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Lu, Email [email protected]
Abstract: Primary hepatic epithelioid gastrointestinal stromal tumor (GIST) is an extremely rare neoplasm. Due to its non‑specific clinical and radiologic features, it is frequently misdiagnosed as other primary or metastatic hepatic malignancies. Here, we report the case of an 85‑year‑old asymptomatic woman in whom a mass in the left hepatic lobe was incidentally identified during routine examination. Computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography‑CT revealed a well‑defined malignant lesion in the left hepatic lobe without evidence of extrahepatic disease. The patient underwent neoadjuvant transarterial chemoembolization (TACE), followed by left hemihepatectomy one month later. Histopathologic and immunohistochemical analyses confirmed a high‑risk epithelioid GIST. Adjuvant therapy with oral imatinib (400 mg/day) was initiated six weeks postoperatively. At the 10‑month follow‑up, the patient remained free of tumor recurrence. Despite preoperative diagnostic challenges, the combination of neoadjuvant TACE, curative surgical resection, and adjuvant imatinib resulted in favorable short‑term outcomes in this patient.
Keywords: primary hepatic gastrointestinal stromal tumor, epithelioid, extragastrointestinal stromal tumor, imaging features, surgical resection, imatinib
Introduction
Gastrointestinal stromal tumor (GIST) is the most common mesenchymal neoplasm of the gastrointestinal tract, arising from the interstitial cells of Cajal responsible for regulating gastrointestinal motility.1,2 It predominantly occurs in the stomach (60–65%) and the small intestine (20–25%), while stromal tumors arising outside the gastrointestinal tract are defined as extragastrointestinal stromal tumors (EGISTs), accounting for less than 5% of all GISTs.3,4 EGISTs may develop in various intra‑abdominal and extra‑abdominal sites, including the greater omentum, mesentery, retroperitoneum, liver, pelvic cavity, vagina, and abdominal wall.5–7 Among these, primary hepatic epithelioid GIST represents an exceptionally rare subtype, with only a small number of cases documented in the literature.8
In this report, we describe a patient with high‑risk primary hepatic epithelioid GIST who was successfully treated with neoadjuvant TACE, surgical resection, and postoperative adjuvant imatinib, with favorable short‑term outcomes.
Case Report
An 85‑year‑old woman was admitted to our hospital after a hepatic mass was incidentally detected during a routine physical examination. She denied any symptoms, including abdominal pain, nausea, vomiting, fever, fatigue, or unexplained weight loss. The lesion was initially identified by abdominal ultrasound, and subsequent imaging studies were performed for further characterization. The patient had a history of subtotal gastrectomy for gastric ulcer 20 years earlier, with an uneventful postoperative course. She had no known chronic liver disease, viral hepatitis, hypertension, diabetes mellitus, or other chronic medical disorders. She also denied any history of toxic exposure or blood transfusion.
Physical examination revealed stable vital signs. No jaundice was present. A hard, non‑tender, immobile mass was palpable in the left upper quadrant. No superficial lymphadenopathy was identified. The abdomen was non‑tender without rebound tenderness or guarding. Shifting dullness was absent, and no lower extremity edema was noted.
Laboratory examinations, including complete blood count, liver and renal function tests, coagulation profile, and serum tumor markers (alpha‑fetoprotein, carcinoembryonic antigen, carbohydrate antigen 19‑9), were all within normal limits. Serologic testing for hepatitis B and C viruses was negative.
Abdominal CT demonstrated a well‑defined mass in the left hepatic lobe. The lesion was slightly hypodense relative to the surrounding hepatic parenchyma and contained central hypodense areas (Figure 1a). In the arterial phase, the tumor exhibited marked heterogeneous enhancement with intratumoral strand‑like vascular structures, known as the “thread and streak sign” (Figure 1b).9 Progressive washout of contrast was observed in the portal venous and delayed phases, consistent with a typical “fast wash‑in, fast wash‑out” enhancement pattern (Figure 1c and d).
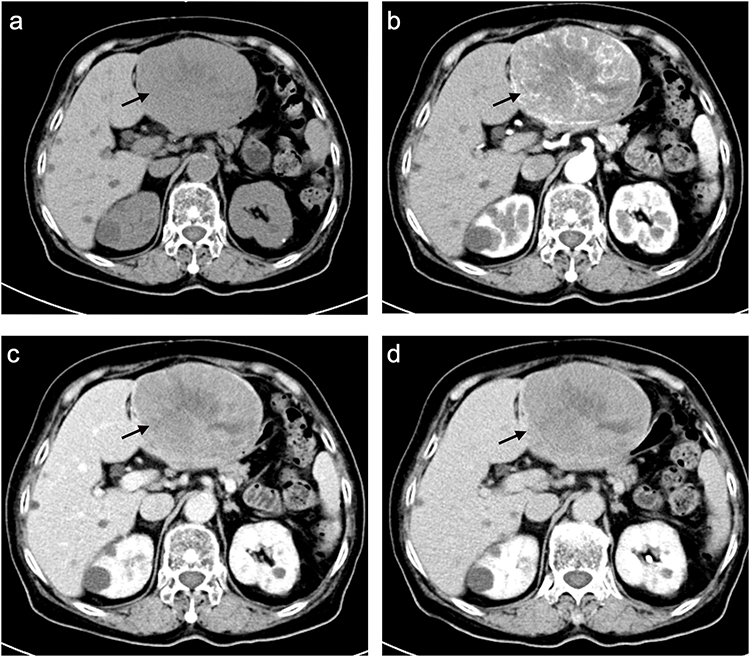 |
Figure 1 Preoperative contrast-enhanced computed tomography (CT) features of the primary hepatic epithelioid GIST. (a) Unenhanced CT demonstrates a well-defined, slightly hypodense mass in the left hepatic lobe with central hypodense areas suggestive of necrosis or hemorrhage (arrow). (b) Arterial-phase CT shows marked heterogeneous enhancement with characteristic intratumoral strand-like vascular structures (“thread and streak sign”, arrow). (c) Portal venous-phase image shows progressive contrast washout of the tumor (arrow). (d) Delayed-phase image shows further washout with clear demarcation from the surrounding hepatic parenchyma (arrow). |
Contrast‑enhanced MRI showed that the solid components of the tumor were heterogeneously isointense to hyperintense on T2‑weighted imaging (Figure 2a). After contrast administration, intense heterogeneous enhancement was seen in the arterial phase (Figure 2b). In the portal venous and delayed phases, the tumor became more homogeneously enhanced with gradual signal reduction (Figure 2c and d). The lesion displayed restricted diffusion on diffusion‑weighted imaging (Figure 2e). No significant contrast uptake was observed in the hepatobiliary phase following Gd‑EOB‑DTPA administration (Figure 2f).
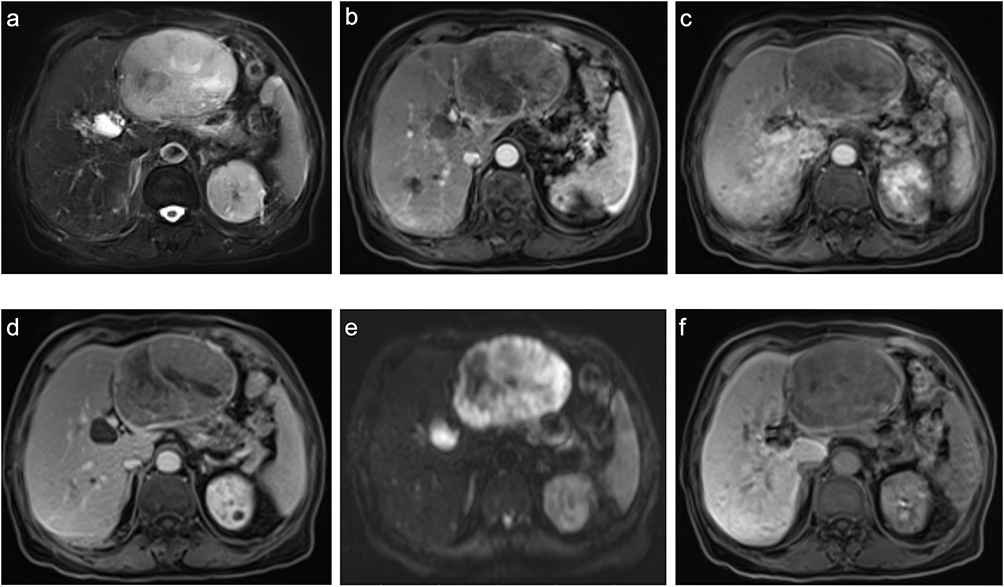 |
Figure 2 Magnetic resonance imaging (MRI) features of the hepatic mass. (a) T2-weighted image shows heterogeneous isointense to hyperintense signal within the solid components of the tumor. (b) Arterial-phase contrast-enhanced MRI shows intense heterogeneous enhancement. (c) Portal venous-phase image shows more homogeneous enhancement with decreasing signal intensity. (d) Delayed-phase image shows further reduction in enhancement. (e) Diffusion-weighted imaging shows marked restricted diffusion (high signal). (f) Hepatobiliary-phase image (Gd-EOB-DTPA) shows no significant uptake within the tumor, consistent with non-hepatocellular origin. |
PET‑CT demonstrated markedly increased glucose metabolism within the left hepatic mass, with no abnormal foci detected elsewhere in the body.
Based on these imaging features, the lesion was regarded as a highly suspicious hepatocellular carcinoma (HCC) in the left hepatic lobe. Given the large tumor size and advanced patient age, neoadjuvant therapy was administered. TACE was performed to reduce tumor volume and increase the likelihood of complete surgical resection.
Left hemihepatectomy was performed one month after TACE. Intraoperatively, a well‑circumscribed mass was confirmed in the left hepatic lobe. No enlarged lymph nodes or additional lesions were identified in the abdominal cavity or the remaining liver parenchyma. The operation proceeded uneventfully without intraoperative complications.
Gross examination of the resected specimen showed a well‑demarcated solid tumor measuring 12 cm × 10 cm × 7 cm. The cut surface was grayish‑white to dark red and fleshy, with multifocal hemorrhage (Figure 3a). The postoperative course was uncomplicated, without bleeding, infection, or liver dysfunction. Follow‑up CT on postoperative day 4 confirmed complete tumor resection with good perfusion of the remnant liver and no significant fluid collection (Figure 3b).
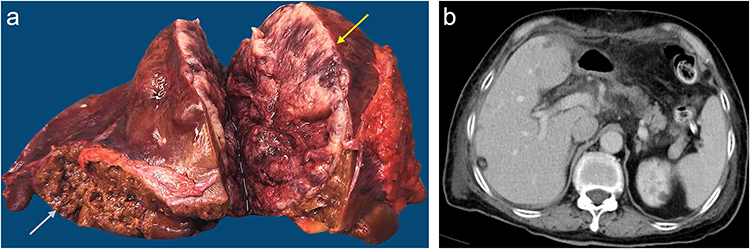 |
Figure 3 Gross pathological appearance and postoperative imaging evaluation. (a) Resected left hemihepatectomy specimen shows a well-circumscribed solid tumor (12 cm × 10 cm × 7 cm) with a gray-white to dark red fleshy cut surface and multifocal hemorrhage (yellow arrow). The hepatic resection margin is free of tumor involvement (white arrow). (b) Postoperative CT (day 4) confirms complete resection of the hepatic mass, with satisfactory perfusion of the remnant liver and no significant fluid collection or complication. |
Histopathologic examination revealed an epithelioid GIST with mild‑to‑moderate nuclear atypia and an infiltrative growth pattern. The mitotic count was 8 per 5 mm2, consistent with a high‑risk tumor. Vascular invasion was identified within the tumor. Surgical margins were negative, and no lymph node metastasis was observed. Hematoxylin and eosin staining showed that the tumor was composed predominantly of round epithelioid cells (Figure 4a).
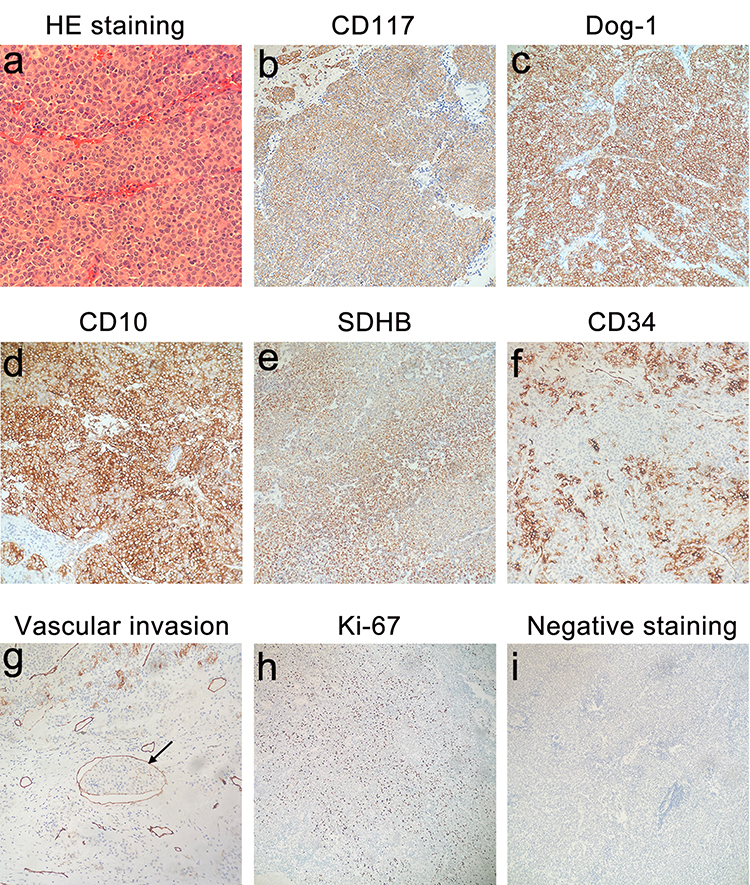 |
Figure 4 Histopathological and immunohistochemical features of the tumor. (a) Hematoxylin and eosin staining reveals a monotonous population of round epithelioid cells. (b-e) Tumor cells show diffuse immunoreactivity for CD117, Dog-1, CD10, and SDHB. (f) Focal CD34 expression is noted in the tumor cells. (g) Vascular tumor thrombus is also positive for CD34 (arrow). (h) Ki-67 proliferation index is approximately 30%. (i) Tumor cells are negative for a broad panel of lineage-specific markers including PDGFRα, SMA, Desmin, S-100, cytokeratins, hepatocellular markers, and neuroendocrine markers. |
Immunohistochemically, the tumor cells were diffusely positive for CD117, Dog‑1, SDHB, and CD10 (Figure 4b–e), and focally positive for CD34 (Figure 4f). Vascular tumor thrombus was also positive for CD34 (Figure 4g). P53 showed a wild‑type expression pattern, and the Ki‑67 proliferation index was 30% (Figure 4h). The tumor cells were negative for a broad panel of lineage‑specific markers, including PDGFRα, SMA, Desmin, S‑100, pan‑CK, CK7, CK18, CK19, HepPar‑1, Arg‑1, AFP, CEA, Glypican‑3, LCA, Syn, CgA, and CD56 (Figure 4i). The final diagnosis was high‑risk primary hepatic epithelioid GIST.
The patient was discharged in good condition two weeks after surgery. Targeted therapy with oral imatinib mesylate (400 mg daily) was initiated six weeks postoperatively. At the 10‑month follow‑up, the patient remained asymptomatic, and imaging studies showed no evidence of tumor recurrence or distant metastasis. The patient was advised to receive adjuvant imatinib for a minimum of 3 years and to undergo surveillance with contrast-enhanced CT or MRI at least every 6 months.
Based on the above case report, we constructed a timeline diagram to facilitate readers’ understanding of the clinical course (Figure 5).
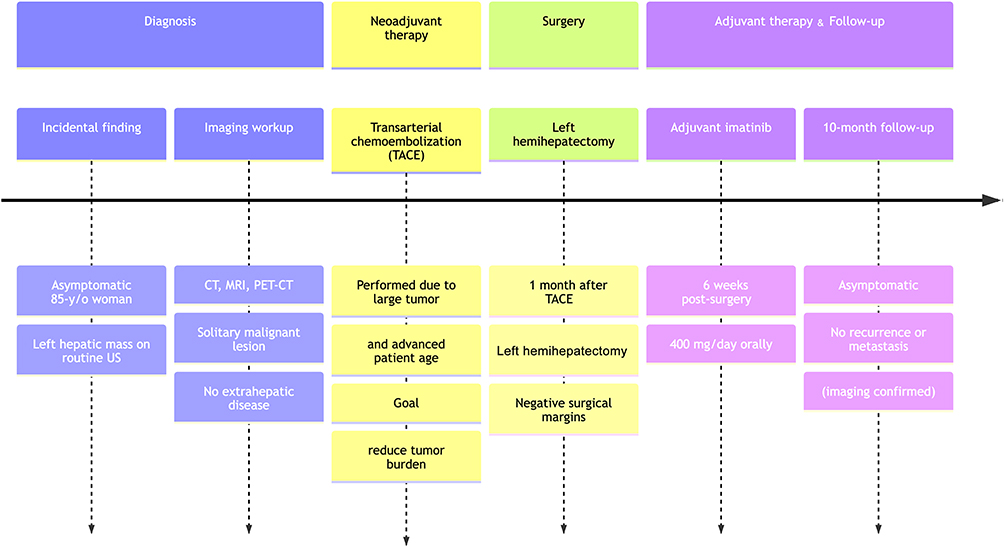 |
Figure 5 Timeline of the sequence of diagnosis, TACE treatment, surgery, and follow-up. |
Discussion
Primary hepatic GIST is an extremely rare neoplasm. A 2025 review by Usama et al included 22 cases, with a male-to-female ratio of 1.3:1 and mean age at diagnosis of 57.6±15.5 years10. Among these 22 cases, only 2 were epithelioid cell subtype. Of these two cases, one was a low‑risk GIST harboring a PDGFRA mutation. This patient received no targeted therapy after curative resection, and the postoperative survival duration was not reported.8 The other was a high‑risk GIST that was also preoperatively misdiagnosed as HCC or adrenal tumor. It was wild‑type for c-KIT/PDGFRA, and imatinib was considered ineffective; thus, no adjuvant targeted therapy was administered. This patient died of widespread tumor metastasis 11 months after surgery.11
The pathogenesis of GIST remains unclear, although emerging evidence suggests a potential role for c-KIT and PDGFRA mutations.12 c-KIT/PDGFRA mutation analysis is crucial for GIST diagnosis and targeted therapy decision-making. Mutation status is particularly important for prognostication and predicting imatinib sensitivity in this rare primary hepatic epithelioid GIST. In this case, genetic testing was not performed due to objective reasons—the patient refused further c-KIT/PDGFRA mutation analysis because of poor economic conditions.
Clinical manifestations of primary hepatic GIST are nonspecific. Most patients are asymptomatic, and lesions are discovered incidentally during routine examinations.10 No specific serum biomarkers are available for this entity; tumor markers including AFP and CEA are typically normal, which helps distinguish primary hepatic GIST from hepatocellular carcinoma and metastatic gastrointestinal malignancies.10
Imaging plays a critical role in the preoperative evaluation of primary hepatic GIST, but radiologic features are often non‑specific and may lead to misdiagnosis. In our case, the tumor displayed a “fast wash‑in, fast wash‑out” enhancement pattern on dynamic CT and MRI, mimicking HCC and resulting in preoperative diagnostic uncertainty. To the best of our knowledge, the present study is the first to report the “thread and streak sign” observed in the arterial phase on CT in a GIST. Whether this imaging characteristic is common in primary hepatic epithelioid GIST warrants further verification in larger cohorts.
Definitive diagnosis relies on histopathological and immunohistochemical examinations.3 Histologically, GISTs are categorized into spindle‑cell, epithelioid, and mixed types. The epithelioid variant is rare and associated with higher malignant potential.3 Risk stratification is based on tumor size, mitotic index, and anatomic location. Tumors with a mitotic rate ≥ 5 per 5 mm2 or large dimensions are classified as high‑risk, with an increased risk of recurrence and metastasis.13 In this case, the tumor measured 12 cm × 10 cm × 7 cm with a mitotic count of 8 per 5 mm2, fulfilling high‑risk criteria. The presence of vascular invasion further indicated aggressive biological behavior.
Immunohistochemistry is indispensable for the diagnosis of GIST. CD117 and Dog‑1 are the most sensitive and specific markers, with positivity rates exceeding 95%.14 In the present case, diffuse expression of CD117 and Dog‑1 confirmed the diagnosis. Preserved SDHB expression excluded the rare SDHB‑deficient subtype, which is associated with poor prognosis.15
Surgical resection with negative margins remains the first‑line curative treatment for localized primary hepatic GIST.16 For large or high‑risk HCC, neoadjuvant TACE may be used to reduce tumor burden and improve resectability.17 In this case, we initially diagnosed the lesion as HCC preoperatively, therefore, the patient received neoadjuvant TACE. At present, there are only sporadic reports on the use of TACE in the treatment of primary hepatic GIST.18 Whether TACE offers beneficial effects in primary hepatic GIST requires further validation with more cases and clinical studies.
For high‑risk GIST, adjuvant imatinib therapy is recommended for at least three years postoperatively, as it significantly reduces recurrence and improves survival.19 Our patient was started on adjuvant imatinib (400 mg/day) six weeks after surgery and remained disease‑free at the 10‑month follow‑up, indicating a favorable short‑term response. Given the high‑risk features, prolonged adjuvant treatment and close long‑term surveillance are warranted.
This report is limited by its nature as a single case with relatively short follow‑up. Long‑term prognosis remains to be determined. In addition, the absence of c‑KIT and PDGFRA mutational analysis limits prediction of imatinib sensitivity and prognostic stratification. Future studies involving larger cohorts, comprehensive molecular profiling, and extended follow‑up are needed to establish standardized diagnostic and therapeutic algorithms for this rare tumor.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics
No ethical clearance required as it only involves a case report.
Informed Consent Statement
Informed written consent was obtained from the patient for publication of this case report and all accompanying images.
Consent for Publication
Written informed consent was obtained from the patient for publication of clinical details, including radiological and procedure images. A copy of the consent can be provided upon request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Construction Fund of Key Medical Disciplines of Hangzhou (OO20200093 and 2025HZGF05).
Disclosure
The authors declare that they have no conflicts of interest to disclose in this work.
References
1. Gheorghe G, Bacalbasa N, Ceobanu G, et al. Gastrointestinal stromal tumors-a mini review. J Pers Med. 2021;11:694. doi:10.3390/jpm11080694
2. Kelly CM, Gutierrez Sainz L, Chi P. The management of metastatic GIST: current standard and investigational therapeutics. J Hematol Oncol. 2021;14:2. doi:10.1186/s13045-020-01026-6
3. Blay JY, Kang YK, Nishida T, et al. Gastrointestinal stromal tumours. Nat Rev Dis Primers. 2021;7:22. doi:10.1038/s41572-021-00254-5
4. Cheng M, Liu CH, Horng HC, et al. Gastrointestinal stromal tumor presenting as a rectovaginal septal mass: a case report and review of literature. Medicine. 2019;98:e15398. doi:10.1097/MD.0000000000015398
5. El-Helou E, Chamma L, Mazraani HB, et al. Extra-Gastrointestinal Stromal Tumor (EGIST) in the pelvis mimicking retroperitoneal sarcoma. Surg J. 2022;8:e266–7. doi:10.1055/s-0042-1757335
6. Hanayneh W, Starr J, George TJ, et al. Extragastrointestinal stromal tumors of the pelvic cavity and the vagina: two case reports and review of the literature. Gynecol Oncol Rep. 2018;25:3–7. doi:10.1016/j.gore.2018.04.006
7. Schaefer IM, DeMatteo RP, Serrano C. The GIST of advances in treatment of advanced gastrointestinal stromal tumor. ASCO Educ Book. 2022;42:885–899. doi:10.1200/EDBK_351231
8. Yamamoto H, Miyamoto Y, Nishihara Y, et al. Primary gastrointestinal stromal tumor of the liver with PDGFRA gene mutation. Hum Pathol. 2010;41(4):605–609. doi:10.1016/j.humpath.2009.09.016
9. Sivaramalingam S, Ethiraj D, Srinivas S, et al. Thread and streak sign in hepatocellular carcinoma. QJM. 2021;114(2):134–135. doi:10.1093/qjmed/hcaa317
10. Usama F, Rasikh R, Hassam K, et al. An update on gastrointestinal stromal tumors (GISTs) with a focus on extragastrointestinal stromal tumors (EGISTs). Gastroenterol Rep. 2025;13:goaf068. doi:10.1093/gastro/goaf068
11. Xu LL, Zhang M, Xu MQ. Primary hepatic gastrointestinal stromal tumor with right adrenal gland invasion: a case report and systematic literature review. Medicine. 2019;98(20):e15482. doi:10.1097/MD.0000000000015482
12. Chen Q, Li R, Zhang ZG, et al. Oncogene mutational analysis in Chinese gastrointestinal stromal tumor patients. Onco Targets Ther. 2018;11:2279–2286. doi:10.2147/OTT.S155214
13. Trinh VQH, Dashti NK, Cates JMM. A proposed risk assessment score for gastrointestinal stromal tumors based on evaluation of 19,030 cases from the national cancer database. J Gastroenterol. 2021;56(11):964–975. doi:10.1007/s00535-021-01831-x
14. Wu CE, Tzen CY, Wang SY, et al. Clinical Diagnosis of Gastrointestinal Stromal Tumor (GIST): from the molecular genetic point of view. Cancers. 2019;11(5):679. doi:10.3390/cancers11050679
15. da Silva Gomes S, Oliveira CS, de Almeida Furtado T, et al. Recurrence of fusocellular subtype GIST with SDHB mutation: a case of SDHB-loss and therapeutic challenges. J Surg Oncol. 2024;130(4):741–742. doi:10.1002/jso.27727
16. Qian XH, Yan YC, Gao BQ, et al. Prevalence, diagnosis, and treatment of primary hepatic gastrointestinal stromal tumors. World J Gastroenterol. 2020;26(40):6195–6206. doi:10.3748/wjg.v26.i40.6195
17. Chan KS, Tay WX, Cheo FY, et al. Preoperative transarterial chemoembolization (TACE) + liver resection versus upfront liver resection for large hepatocellular carcinoma (≥5 cm): a systematic review and meta-analysis. Acta Chir Belg. 2023;123(6):601–617. doi:10.1080/00015458.2023.2256539
18. Fernandes MR, Ghezzi CLA, Grezzana-Filho TJ, et al. Giant hepatic extra-gastrointestinal stromal tumor treated with cytoreductive surgery and adjuvant systemic therapy: a case report and review of literature. World J Gastrointest Surg. 2021;13(3):315–322. doi:10.4240/wjgs.v13.i3.315
19. Gao ZD, Li J, Wang C, Ye YJ. Disparities in management guidelines for gastrointestinal stromal tumors: a comparison of recommendations from the Chinese society of clinical oncology, national comprehensive cancer network, and European society for medical oncology. Cancer. 2025;131(Suppl 3):e70153. doi:10.1002/cncr.70153
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.