Back to Journals » Clinical Ophthalmology » Volume 18
Prevalences of Other Non-Thyroid Autoimmune Diseases and Factor Associated with Their Presence in Ocular Myasthenia Gravis
Authors Anutraungkool T, Padungkiatsagul T ![]() , Jindahra P
, Jindahra P ![]() , Vanikieti K
, Vanikieti K
Received 10 January 2024
Accepted for publication 17 April 2024
Published 25 April 2024 Volume 2024:18 Pages 1125—1132
DOI https://doi.org/10.2147/OPTH.S458979
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Thanathon Anutraungkool,1 Tanyatuth Padungkiatsagul,1 Panitha Jindahra,2 Kavin Vanikieti1
1Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Kavin Vanikieti, Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Bangkok, 10400, Thailand, Tel +662 201 1526, Email [email protected]
Purpose: To report the prevalences of other non-thyroid autoimmune diseases and identify factors associated with their presence in ocular myasthenia gravis (OMG) subjects.
Subjects and Methods: A total of 208 subjects with OMG diagnosis were included. Demographic data, clinical characteristics, the ice-pack test, the acetylcholine receptor (AChR) antibody test, electrophysiology tests (single-fiber electromyography and repetitive nerve stimulation), the presence of thymoma, generalized myasthenia gravis conversion, and the presence of other non-thyroid autoimmune diseases (defined as the presence of at least one other non-thyroid autoimmune disease) were retrospectively reviewed. Factors associated with the presence of other non-thyroid autoimmune diseases were analyzed by univariate and multivariate logistic regression.
Results: Of the total 208 subjects, 21 (10.10%) exhibited the presence of other non-thyroid autoimmune diseases (19 subjects (9.14%) and 2 subjects (0.96%) had one and two other non-thyroid autoimmune diseases, respectively), and systemic lupus erythematosus (SLE) was diagnosed in 9 subjects, followed by Sjogren’s syndrome (7 subjects), rheumatoid arthritis (6 subjects), and ankylosing spondylitis (1 subject). Therefore, the prevalences of SLE, Sjogren’s syndrome, rheumatoid arthritis, and ankylosing spondylitis in OMG subjects were estimated to be 4.33% (95% confidence interval (CI): 2.29– 8.02%), 3.37% (95% CI: 1.64– 6.79%), 2.88% (95% CI: 1.33– 6.14%), and 0.48% (95% CI: 0.08– 2.67%), respectively. Positivity of the AChR antibody was the only significant factor associated with the presence of other non-thyroid autoimmune diseases (odds ratio 4.10, 95% CI: 1.11– 15.21, p = 0.035).
Conclusions: The presence of other non-thyroid autoimmune diseases was found in approximately 10% of OMG patients, with SLE displaying the highest prevalence. We recommend screening and monitoring for other non-thyroid autoimmune diseases in OMG patients, particularly those with positivity of the AChR antibody.
Keywords: ocular myasthenia gravis, autoimmune diseases, systemic lupus erythematosus, Sjogren’s syndrome, rheumatoid arthritis, ankylosing spondylitis
Introduction
Myasthenia gravis (MG) is an autoimmune disease in which autoantibodies develop against the postsynaptic membrane at the neuromuscular junction, resulting in fluctuation of muscle weakness and fatigability.1 Approximately 50% of the patients present with pure ocular symptoms (ptosis and/or diplopia), classified as ocular MG (OMG), that is, Myasthenia Gravis Foundation of America clinical classification class I. The remaining 50% present with symptoms of generalization, for example, limb weakness, difficulty with speech, and dysphagia, classified as generalized MG (GMG), that is, Myasthenia Gravis Foundation of America clinical classification class II–V.2,3
The diagnosis of OMG is challenging because patients with OMG can present with various ocular manifestations mimicking other conditions such as cranial nerve palsy, internuclear ophthalmoplegia, or thyroid eye disease. Moreover, the acetylcholine receptor (AChR) antibody test, which is one of the diagnostic tests, was reported to be 50–71% sensitive in OMG.2,4 Therefore, OMG is normally diagnosed based on a combination of clinical presentations and other diagnostic tests, including the ice-pack test, the AChR antibody test, and electrophysiology tests.
Regarding concomitant autoimmune diseases, although other thyroid autoimmune diseases (eg, Graves’ disease and Hashimoto’s thyroiditis) are frequently associated with MG, other non-thyroid autoimmune diseases can coexist with MG.5–7 Prevalences of other non-thyroid autoimmune diseases in OMG patients have been rarely reported in the Thai population.8 Moreover, to the best of our knowledge, no studies have been performed to identify factors associated with the presence of other non-thyroid autoimmune diseases in OMG patients in the Thai population. Therefore, this study aimed to report the prevalences of other non-thyroid autoimmune diseases and identify factors associated with their presence in OMG subjects.
Materials and Methods
This study followed the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand (IRB number: COA. MURA2023/527), which waived the need for written informed consent from the subjects due to the retrospective nature of the study. De-identified data were used in this study. All data were kept confidentially in our database. Electronic medical records were reviewed to identify all MG subjects in the Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, from January 2013 to December 2020.
Subject Selection
Subjects who met all of the following criteria were included: (1) age at onset ≥ 18 years; (2) had pure ocular symptoms of fluctuating ptosis and/or diplopia at onset and were diagnosed with OMG based on at least one of the following: (2.1) positivity of the ice-pack test, (2.2) positivity of the AChR antibody, (2.3) positivity of electrophysiology tests: single-fiber electromyography (SFEMG) or repetitive nerve stimulation (RNS); and (3) exhibited pure ocular symptoms for at least 2 years from the onset of symptoms unless there was GMG conversion within 2 years from the onset of symptoms. We excluded subjects who presented with GMG at the initial visit.
Data Collection
Demographic data and clinical characteristics, including age at onset, sex, underlying diseases (hypertension, type 2 diabetes mellitus, and thyroid autoimmune diseases), and initial ocular signs (ptosis, lid fatigability, Cogan’s lid twitch, orbicularis oculi weakness, and duction limitation) were reviewed.
Regarding the diagnostic tests, the ice-pack test, the AChR antibody test which was performed by an ELISA method (EUROIMMUN Analyzer I, Seekamp, Lübeck, Germany), and electrophysiology tests (SFEMG and RNS) were reviewed. Definitions of positivity of each diagnostic test are summarized in Table 1.
 |
Table 1 Definitions of Positivity of Each Diagnostic Test |
The presence of thymoma was defined as its radiological presence as based on thoracic computed tomography, which was performed within 1 month after the initial visit.
Regarding GMG conversion, this was defined as the presence of at least one of the following symptoms during follow-up: hoarseness, dysarthria, dysphagia, dyspnea, and weakness of extremities and the neck, predominantly at proximal muscles. The diagnosis of GMG conversion was confirmed by neurologists.
Other non-thyroid autoimmune diseases were identified from the ICD-10 (International Statistical Classification of Diseases and Related Health Problems 10th Revision) codes and the diagnosis was confirmed by actual specialists, meeting the international criteria established for each disease.9–12 Of note, in subjects who displayed GMG conversion, other non-thyroid autoimmune diseases as well as underlying diseases (hypertension, type 2 diabetes mellitus, and thyroid autoimmune diseases) that were diagnosed after GMG conversion were not taken into consideration.
The presence of other non-thyroid autoimmune diseases was defined as the presence of at least one other non-thyroid autoimmune disease. The timing of the diagnosis of other non-thyroid autoimmune diseases relative to OMG diagnosis was classified into the three categories of prior to OMG diagnosis, concurrent with OMG diagnosis, and after OMG diagnosis.
Statistical Analysis
Continuous variables were expressed using the mean or median, with normally distributed results shown as mean ± standard deviation (SD) and non-normally distributed results shown as median and range. Independent t-test or Mann–Whitney U-test, where appropriate, were applied to compare continuous variables. Categorical variables were expressed as frequency and percentage. These variables were compared using Chi-squared or exact test where appropriate. For multivariate analysis, logistic regression was applied, to simultaneously regress outcomes with variables whose p-values in univariate analysis were <0.1. Statistical analyses were performed using STATA software, version 18.0 (StataCorp LLC, College Station, TX, USA). Differences were reported with the 95% confidence interval (CI). P-values < 0.05 were considered to be statistically significant.
Results
A total of 208 subjects with an OMG diagnosis were included in the study. The mean age at onset was 48.16 ± 17.82 years. Of these 208 subjects, 160 (76.92%) were female. Ptosis was the most common initial ocular sign, which was presented in 175 subjects (84.13%).
There were 150 subjects with available ice-pack test data, of whom 93 (62.00%) displayed positivity in this test. AChR antibody tests were performed in all subjects, with 117 (56.25%) revealing positivity of the AChR antibody. SFEMG and RNS data were only available for 69 subjects (33.17%) and 71 subjects (34.13%), respectively. Therefore, these variables were excluded from the comparative, univariate, and multivariate analyses. Of the aforementioned available SFEMG and RNS data, positivity of SFEMG and RNS was demonstrated in 52 subjects (75.36%) and 5 subjects (7.04%), respectively. Of the 163 subjects with available thoracic computed tomography data, 19 (11.66%) displayed the presence of thymoma. GMG conversion was observed in 17 subjects (8.17%).
Of the total 208 subjects, 21 (10.10%) exhibited the presence of other non-thyroid autoimmune diseases (19 subjects (9.14%) had one other non-thyroid autoimmune disease and 2 subjects (0.96%) had two other non-thyroid autoimmune diseases (1 subject displayed systemic lupus erythematosus (SLE) and Sjogren’s syndrome (SS), while the other had rheumatoid arthritis (RA) and SS)). SLE was diagnosed in 9 subjects (4.33%), followed by SS (7 subjects, 3.37%), RA (6 subjects, 2.88%), and ankylosing spondylitis (AS) (1 subject, 0.48%). Therefore, the prevalences of SLE, SS, RA, and AS in OMG subjects were estimated to be 4.33% (95% CI: 2.29–8.02%), 3.37% (95% CI: 1.64–6.79%), 2.88% (95% CI: 1.33–6.14%), and 0.48% (95% CI: 0.08–2.67%), respectively.
Of the 21 subjects with the presence of other non-thyroid autoimmune diseases, 11 (52.38%) were diagnosed prior to OMG diagnosis (median 81 (3–90) months), 3 (14.29%) were diagnosed concurrent with OMG diagnosis, and 7 (33.33%) were diagnosed after OMG diagnosis (median 38 (3–86) months). Of note, the two other non-thyroid autoimmune diseases in each of the two subjects who had two other non-thyroid autoimmune diseases were diagnosed concurrent with OMG diagnosis.
Detailed demographic data, clinical characteristics, diagnostic tests, presence of thymoma, GMG conversion, presence of other non-thyroid autoimmune diseases and their timing of the diagnosis relative to OMG diagnosis, and the diagnosis and prevalences of other non-thyroid autoimmune diseases of the study subjects are summarized in Table 2.
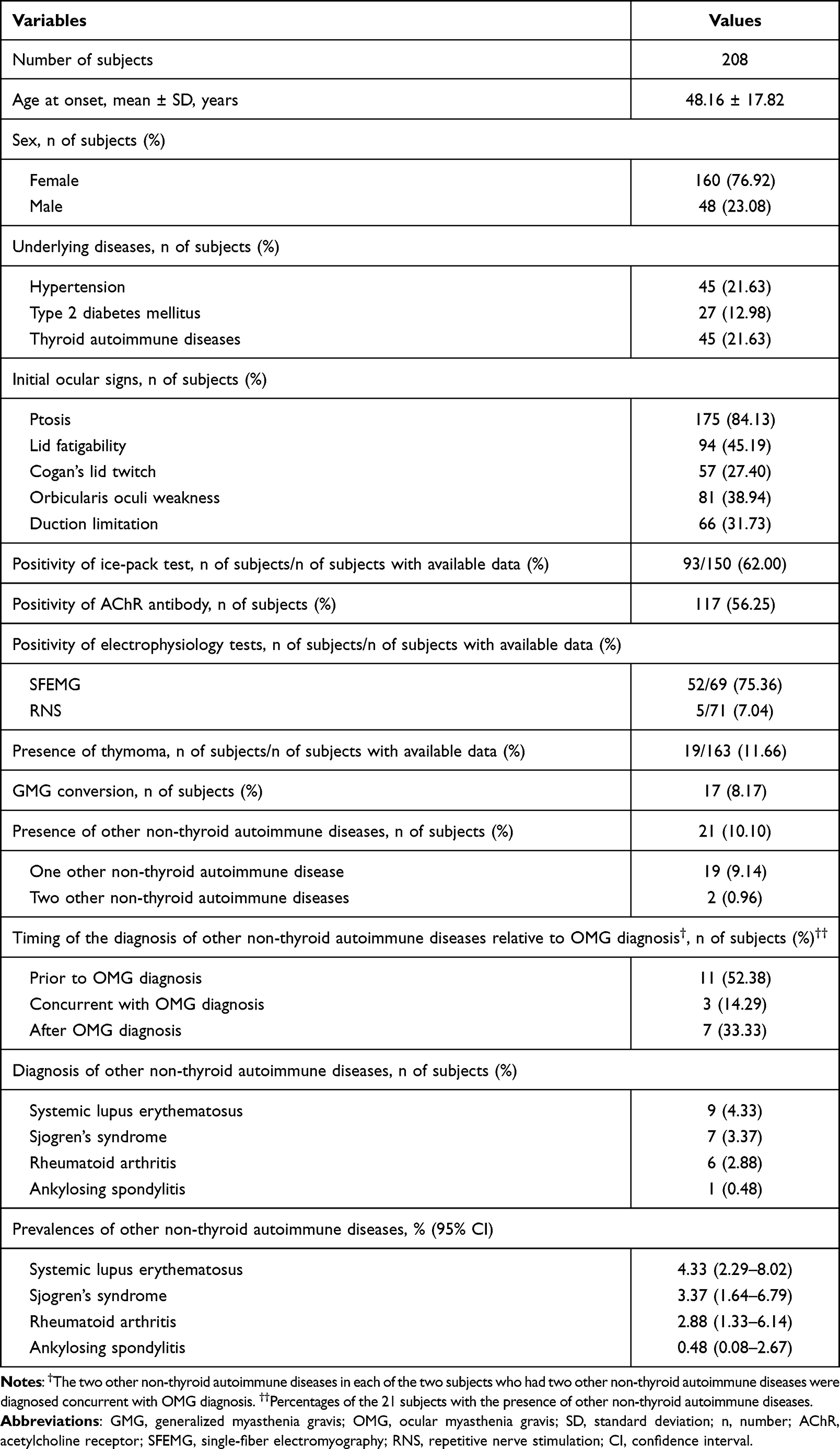 |
Table 2 Detailed Demographic Data, Clinical Characteristics, Diagnostic Tests, Presence of Thymoma, GMG Conversion, Presence of Other Non-Thyroid Autoimmune Diseases and Their Timing of the Diagnosis Relative to OMG Diagnosis, and the Diagnosis and Prevalences of Other Non-Thyroid Autoimmune Diseases of the Study Subjects |
The proportion of positivity of the AChR antibody was significantly higher in subjects with the presence of other non-thyroid autoimmune diseases than in subjects with their absence (80.95% versus 53.48%, p = 0.016). There were no significant differences in terms of age at onset, sex, underlying diseases (hypertension, type 2 diabetes mellitus, and thyroid autoimmune diseases), initial ocular signs, positivity of the ice-pack test, presence of thymoma, or GMG conversion, as shown in Table 3.
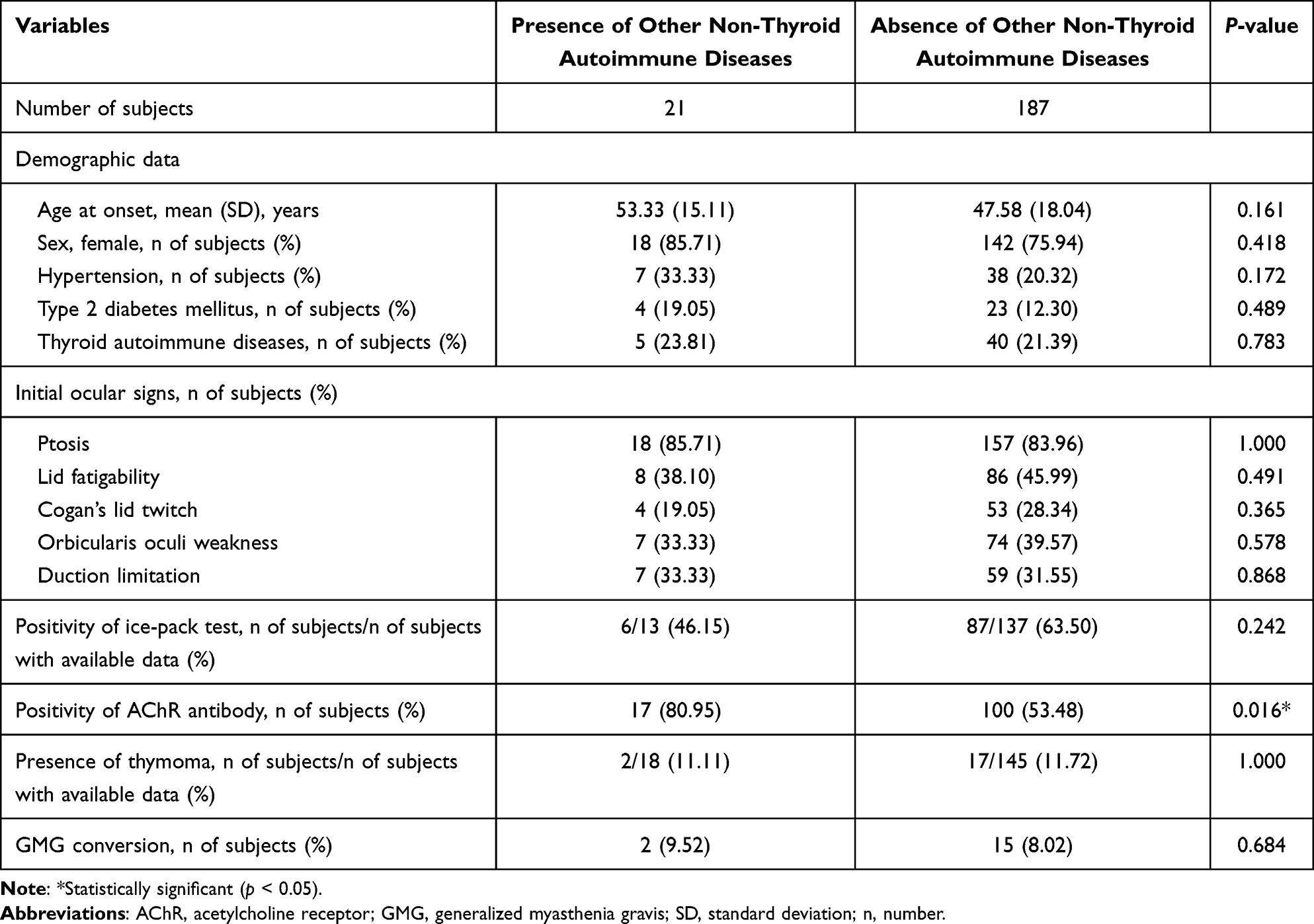 |
Table 3 Comparison of Demographic Data, Clinical Characteristics, Ice-Pack Test, AChR Antibody Test, Presence of Thymoma, and GMG Conversion Between Subjects with the Presence of Other Non-Thyroid Autoimmune Diseases and the Absence of Other Non-Thyroid Autoimmune Diseases |
Given the higher incidence and prevalence of autoimmune diseases in females and increasing evidence of thymoma producing various autoantibodies,13,14 these two factors were also included in the multivariate analysis despite their p-values of ≥0.1 in univariate analysis. Nevertheless, positivity of the AChR antibody (odds ratio 4.10, 95% CI: 1.11–15.21, p = 0.035) was the only significant factor associated with the presence of other non-thyroid autoimmune diseases in multivariate analysis, as shown in Table 4.
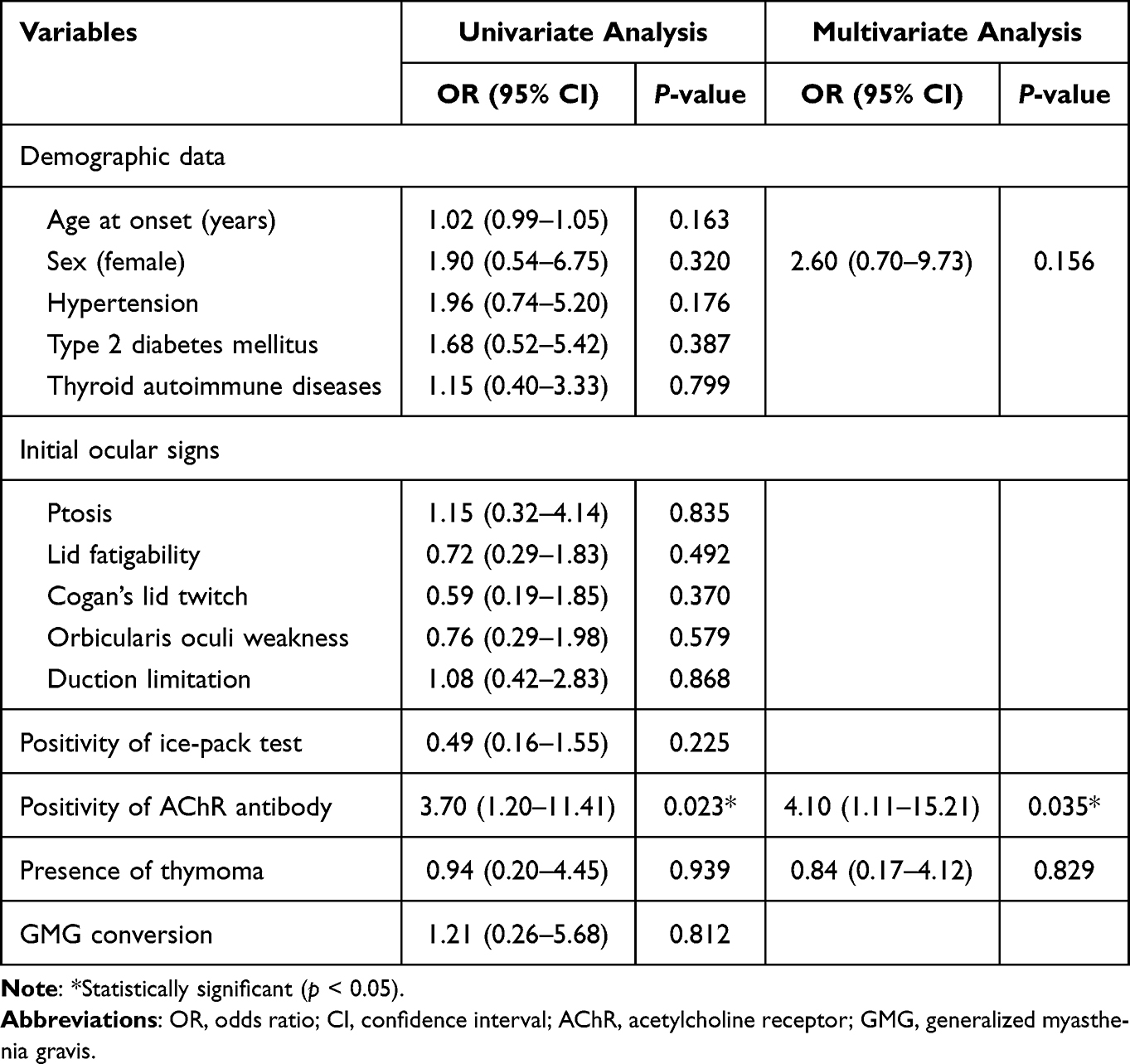 |
Table 4 Factors Associated with the Presence of Other Non-Thyroid Autoimmune Diseases |
Discussion
In this study, we retrospectively reviewed electronic medical records of 208 OMG subjects, aiming to report the prevalences of other non-thyroid autoimmune diseases and identify factors associated with their presence in OMG subjects.
We reported that the prevalences of SLE, SS, RA, and AS in OMG subjects were estimated to be 4.33% (95% CI: 2.29–8.02%), 3.37% (95% CI: 1.64–6.79%), 2.88% (95% CI: 1.33–6.14%), and 0.48% (95% CI: 0.08–2.67%), respectively. By contrast, the prevalences of SLE, SS, RA, and AS in the general Asian population are reported to be approximately 0.07%, 0.04%, 0.07%, and 0.07%, respectively, such that each prevalence lies outside the lower limit of the 95% CI of each corresponding prevalence calculated for our subjects.15–18 Therefore, the prevalences of SLE, SS, RA, and AS in OMG subjects in our study appear to be higher than in the general Asian population. These findings may be the result of chemokine (C-X-C motif) ligand 13, which is the factor that stimulates B and T cell lymphocytes and consequently promotes the pathogenesis of MG and other autoimmune diseases.19–22 Furthermore, we hypothesized that a common genetic background may also contribute to the coexistence of MG and other autoimmune diseases, for example, variations of human leukocyte antigen (HLA) loci (HLA-B8, HLA-DRB1, and HLA-DR3).23–26
The prevalences of other non-thyroid autoimmune diseases in our study were higher compared with the study of Kemchoknatee et al with 155 OMG subjects in Thailand.8 In their study, the prevalences of SLE and RA in OMG subjects were estimated to be 1.29% and 0.65%, respectively. Moreover, none of the OMG subjects in their study exhibited SS or AS. These different findings between these two studies may be explained by the larger number of subjects enrolled in our study and unlike our study, their study did not evaluate other non-thyroid autoimmune diseases after OMG diagnosis.
We demonstrated that positivity of the AChR antibody was the only significant factor associated with the presence of other non-thyroid autoimmune diseases. A systematic review conducted by Mao et al also revealed that positivity of the AChR antibody was associated with the coexistence of other autoimmune diseases in MG (pooled odds ratio 3.68, 95% CI: 1.52–8.89; p = 0.004).27 Nevertheless, unlike our study, they excluded studies that were limited to specific patient characteristics, such as OMG in particular. Furthermore, they mainly focused on other autoimmune diseases overall, unlike specifically other non-thyroid autoimmune diseases as in our study.
Therefore, from our results, we indicated the coexistence of other non-thyroid autoimmune diseases in OMG. Furthermore, we recommend screening and monitoring for other non-thyroid autoimmune diseases in OMG patients, particularly those with positivity of the AChR antibody. These may support an early diagnosis and prompt treatment of other non-thyroid autoimmune diseases in OMG patients, which may consequently decrease further complications and progression of other non-thyroid autoimmune diseases.
There were some strengths in our study. First, to the best of our knowledge, this study enrolled the largest number of OMG subjects for any such study in Thailand. Second, to the best of our knowledge, this is the first study performed to identify factors associated with the presence of other non-thyroid autoimmune diseases in particular OMG subjects in the Thai population.
Our study had some limitations. First, it had a retrospective design, which resulted in some data loss. Second, we did not stratify the cohort with the presence of other non-thyroid autoimmune diseases into separate other non-thyroid autoimmune diseases due to the sample size, resulting in the lack of further specific findings for each subgroup.
Conclusions
The presence of other non-thyroid autoimmune diseases was found in approximately 10% of OMG patients, with SLE displaying the highest prevalence. We recommend screening and monitoring for other non-thyroid autoimmune diseases in OMG patients, particularly those with positivity of the AChR antibody.
Acknowledgments
The authors would like to thank Ms. Sasiporn Sitthisorn, Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, for her advice on the statistical analysis. We thank Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Dresser L, Woldarski R, Rezania K, et al. Myasthenia gravis: epidemiology, pathophysiology and clinical manifestations. J Clin Med. 2021;10(11):2235. doi:10.3390/jcm10112235
2. Peeler CE, Lott LBD, Eggenberger ER, et al. Clinical utility of acetylcholine receptor antibody testing in ocular myasthenia gravis. JAMA Neurol. 2015;72(10):1170–1174. doi:10.1001/jamaneurol.2015.1444
3. Jaretzki AIII, Barohn RJ, Sanders DB, et al. Myasthenia gravis: recommendations for clinical research standards. task force of the medical scientific advisory board of the myasthenia gravis foundation of America. Neurology. 2000;55(1):16–23. doi:10.1212/WNL.55.1.16
4. Gabriele M, Gregorio S, Valentina D, et al. Acetylcholine receptor antibody positivity rate in ocular myasthenia gravis: a matter of age? J Neurol. 2021;268(5):1803–1807. doi:10.1007/s00415-020-10342-3
5. Amin S, Aung M, Malik H, et al. Myasthenia gravis and its association with thyroid diseases. Cureus. 2020;12(9):e10248. doi:10.7759/cureus.10248
6. Zhu Y, Wang B, Hao Y, et al. Clinical features of myasthenia gravis with neurological and systemic autoimmune diseases. Front Immunol. 2023;14:e1223322. doi:10.3389/fimmu.2023.1223322
7. Vincenzo DS, Salvatore I, Massimiliano M, et al. Comorbidity in myasthenia gravis: multicentric, hospital-based, and controlled study of 178 Italian patients. Neurol Sci. 2024. doi:10.1007/s10072-024-07368-0
8. Kemchoknatee P, Arepagorn A, Srisombut T. Ocular manifestation and generalization after ocular onset in ocular myasthenia gravis: a 5-year analysis. Asian Pac J Allergy Immunol. 2021. doi:10.12932/AP-260521-1141
9. Petri M, Orbai AM, Alarcon GS, et al. Derivation and validation of the systemic lupus international collaborating clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012;64(8):2677–2686. doi:10.1002/art.34473
10. Shiboski SC, Shiboski CH, Criswell L, et al. American college of rheumatology classification criteria for sjogren’s syndrome: a data-driven, expert consensus approach in the sjogren’s international collaborative clinical alliance cohort. Arthritis Care Res. 2012;64(4):475–487.
11. Aletaha D, Neogi T, Silman AJ, et al. Rheumatoid arthritis classification criteria: an American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
12. Rudwaleit M, Heijde DVD, Landewe R, et al. The development of assessment of spondyloarthritis international society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis. 2009;68(6):777–783. doi:10.1136/ard.2009.108233
13. Angum F, Khan T, Hussain A, et al. The prevalence of autoimmune disorders in women: a narrative review. Cureus. 2020;12(5):e8094. doi:10.7759/cureus.8094
14. Song Y, Zhou L, Chen Z, et al. Increased frequency of thymic T follicular helper cells in myasthenia gravis patients with thymoma. J Thorac Dis. 2016;8(3):314–322. doi:10.21037/jtd.2016.03.03
15. Tian J, Zhang D, Yao X, et al. The global epidemiology of systemic lupus erythematosus: a comprehensive systematic analysis and modeling study. Ann Rheum Dis. 2023;82(3):351–356. doi:10.1136/ard-2022-223035
16. Qin B, Wang J, Yang Z, et al. Epidemiology of primary Sjögren’s syndrome: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74(11):1983–1989. doi:10.1136/annrheumdis-2014-205375
17. Black RJ, Cross M, Haile LM, et al. Global, regional, and national burden of rheumatoid arthritis, 1990–2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5(10):e594–e610. doi:10.1016/S2665-9913(23)00211-4
18. Stolwijk C, Onna MV, Boonen A, et al. Global prevalence of spondyloarthritis: a systematic review and meta-regression analysis. Arthritis Care Res. 2016;68(9):1320–1331. doi:10.1002/acr.22831
19. Bekircan-Kurt CE, Kurne AT, Erdem-Ozdamar S, et al. The course of myasthenia gravis with systemic lupus erythematosus. Eur Neurol. 2014;72(5–6):326–329. doi:10.1159/000365568
20. Hrycek A. Systemic lupus erythematosus and myasthenia gravis. Pol Arch Med Wewn. 2009;119(9):582–585.
21. Meraouna A, Cizeron-Clairac G, Panse RL, et al. The chemokine CXCL13 is a key molecule in autoimmune myasthenia gravis. Blood. 2006;108(2):432–440. doi:10.1182/blood-2005-06-2383
22. Ali M, Riad M, Adhikari P, et al. Association between myasthenia gravis and systemic lupus erythematosus as a comorbid state. Cureus. 2021;13(4):e14719. doi:10.7759/cureus.14719
23. Xue K, Niu WQ, Cui Y. Association of HLA-DR3 and HLA-DR15 polymorphisms with risk of systemic lupus erythematosus. Chin Med J. 2018;131(23):2844–2851.
24. Kwon YC, Chun S, Kim K, et al. Update on the genetics of systemic lupus erythematosus: genome-wide association studies and beyond. Cells. 2019;8(10):1180. doi:10.3390/cells8101180
25. Bubuioc AM, Kudebayeva A, Turuspekova S, et al. The epidemiology of myasthenia gravis. J Med Life. 2021;14(1):7–16. doi:10.25122/jml-2020-0145
26. Avidan N, Panse RL, Berrih-Aknin S, et al. Genetic basis of myasthenia gravis – a comprehensive review. J Autoimmun. 2014;52:146–153. doi:10.1016/j.jaut.2013.12.001
27. Mao ZF, Yang LX, Mo XA, et al. Frequency of autoimmune diseases in myasthenia gravis: a systematic review. Int J Neurosci. 2011;121(3):121–129. doi:10.3109/00207454.2010.539307
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.