Back to Journals » Infection and Drug Resistance » Volume 19
Prevalence Trends and Antimicrobial Resistance of Carbapenem-Resistant Gram-Negative Bacteria in Paediatric Patients in Sichuan Province: A Retrospective Study (2021-2025)
Authors You Z ![]() , Huang X, Liu X, Yu H, Long S
, Huang X, Liu X, Yu H, Long S
Received 20 January 2026
Accepted for publication 25 March 2026
Published 31 March 2026 Volume 2026:19 597519
DOI https://doi.org/10.2147/IDR.S597519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Zhuorui You,1 Xiangning Huang,2 Xin Liu,2 Hua Yu,2 Shanshan Long2
1School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2Department of Laboratory Medicine, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, 610072, People’s Republic of China
Correspondence: Shanshan Long, Email [email protected] Hua Yu, Email [email protected]
Objective: Antimicrobial resistance (AMR) represents one of the most pressing global public health threats. This study aimed to analyze the distribution and antimicrobial resistance profiles of Carbapenem-resistant Gram-negative Bacteria (CRGNB) isolated from pediatric patients in Sichuan Province, China, in order to provide evidence to support rational antimicrobial use and infection prevention and control in clinical practice.
Methods: This retrospective study included non-duplicate CRGNB isolates recovered from hospitalized children aged ≤ 14 years in 134 medical institutions across Sichuan Province from 2021 to 2025. Bacterial identification and antimicrobial susceptibility testing were performed according to a unified surveillance protocol. CRGNB was defined, in accordance with CLSI M100, 34th edition (2024), as isolates resistant to at least one carbapenem (imipenem, meropenem, or ertapenem). Data were analyzed using WHONET 5.6.
Results: A total of 2523 CRGNB isolates were collected. Isolates from male patients accounted for 56.4% (1422/2523), and the largest proportion of isolates was from the 29 days to ≤ 1 year age group (41.8%, 1054/2523). The five most frequently isolated species were Klebsiella pneumoniae (41.8%, 1055/2523), Acinetobacter baumannii (22.1%, 558/2523), Escherichia coli (10.0%, 252/2523), Enterobacter cloacae complex (9.3%, 235/2523), and Pseudomonas aeruginosa (6.4%, 162/2523), with respiratory specimens accounting for most isolates (59.6%, 1504/2523). Enterobacterales showed susceptibility rates > 96% to tigecycline and polymyxin B. K. pneumoniae showed 87.5% susceptibility to ceftazidime-avibactam. A. baumannii exhibited low resistance only to polymyxin B and tigecycline (2.3% and 2.5%, respectively). P. aeruginosa showed 100% susceptibility to ceftazidime-avibactam and polymyxin B.
Conclusion: CRGNB infections among children in Sichuan Province remain severe and display marked regional characteristics, with infants constituting a high-risk population. The increasing prevalence of multidrug-resistant organisms poses a substantial challenge to clinical management and warrants close surveillance and targeted intervention.
Keywords: Sichuan Province, China, children, antimicrobial resistance, carbapenem resistance
Introduction
In 2019, the World Health Organization (WHO) identified antimicrobial resistance (AMR) as one of the ten greatest global public health threats facing humanity.1 Modeling studies have projected that between 2025 and 2050, AMR could directly result in more than 39 million deaths and contribute to an additional 169 million deaths, making it the third leading cause of mortality worldwide.2,3 In the WHO Bacterial Priority Pathogens List 2024 (BPPL-2024), Carbapenem-resistant Acinetobacter baumannii (CRAB), Carbapenem-resistant Pseudomonas aeruginosa (CRPA), and Carbapenem-resistant Enterobacterales (CRE) are classified as “critical” and “high-priority” pathogens, with their dissemination closely associated with inappropriate antimicrobial use and inadequate infection control practices.4,5
Children are particularly vulnerable to infections caused by Carbapenem-resistant Gram-negative Bacteria (CRGNB) because of immature immune systems and increased exposure to invasive medical procedures. Consequently, pediatric patients experience higher susceptibility, greater disease severity, and increased mortality following CRGNB infections compared with adults.6,7 However, the distribution and resistance patterns of CRGNB exhibit marked geographic heterogeneity. In Europe, the reported prevalence of Carbapenem-resistant Klebsiella pneumoniae (CRKP) ranges from 0.13% to 22%.8 In China, detection rates of CRKP and CRAB among children reach 35.4% and 56.2%, respectively,9 whereas corresponding resistance rates in the United States remain below 5.5%.10 In Lebanon, the prevalence of carbapenem resistance among pediatric Enterobacterales isolates is only 1.7%,11 while studies from Africa report resistance rates as high as 30.34% in neonatal populations.12
Current antimicrobial drug development lags behind the evolution of resistance, and the approval of new agents for pediatric use is even slower.13 Meanwhile, surveillance data on pediatric CRGNB in Southwest China remain scarce, limiting evidence-based guidance for clinical practice. Therefore, this study was conducted as an isolate-based resistance surveillance study, focusing on CRGNB isolates from pediatric patients to characterize their epidemiological features and antimicrobial resistance patterns. The findings aim to fill the regional data gap and provide evidence to support optimized antimicrobial therapy and targeted infection prevention and control.
Materials and Methods
Source of Bacterial Isolates
This retrospective study included 2523 non-duplicate CRGNB isolates recovered from hospitalized children (≤14 years) in 134 medical institutions across Sichuan Province from 2021 to 2025. Non-duplicate isolates were defined as follows: when multiple specimens from the same anatomical site (eg, respiratory tract, urine, or blood) were collected from the same patient during a single hospitalization and yielded the same bacterial species, only one isolate was retained as the representative strain, while the others were excluded as duplicates.
Inclusion criteria: (1) pediatric inpatients (≤14 years) treated between 2021 and 2025; (2) CRGNB isolated from clinical specimens collected in the context of suspected infection (sterile or non-sterile sites) and confirmed by culture.
Exclusion criteria: (1) patients with negative CRGNB culture results; (2) cases with incomplete clinical data that precluded analysis; (3) repeat isolation of the same strain from the same patient.
The study protocol was approved by the Institutional Review Boards of Sichuan Provincial People’s Hospital and the University of Electronic Science and Technology of China (Approval No.202617). Given the retrospective design and use of de-identified electronic medical record data, informed consent was waived. All procedures conformed to the principles of the Declaration of Helsinki and applicable national regulations.
Bacterial Identification and Antimicrobial Susceptibility Testing
Bacterial identification was performed using the Vitek 2 automated system (bioMérieux, Inc., Hazelwood, MO, USA) or a MALDI-TOF mass spectrometry system (bioMérieux S.A., Marcy-l’Étoile, France). Antimicrobial susceptibility testing and interpretation were conducted in strict accordance with the CLSI M100-S34 (2024) guidelines.14 Minimum inhibitory concentration (MIC) testing and the Kirby-Bauer (K-B) disk diffusion method were applied, and results were interpreted as susceptible (S), intermediate (I), or resistant (R). Susceptible dose-dependent (SDD) results were grouped with the intermediate category for statistical analysis. For selected isolates, antimicrobial susceptibility results were further verified using the E-test gradient strip method (E-TEST, bioMérieux S.A., Marcy-l’Étoile, France).
CRGNB were defined as Gram-negative bacilli resistant to at least one carbapenem agent, with intermediate (I) interpreted as non-resistant. The specific criteria were as follows:
- Enterobacterales (excluding Proteus, Providencia, and Morganella, for which isolates resistant only to imipenem were not included): resistance to any of ertapenem, imipenem, or meropenem, defined as ertapenem MIC ≥ 2 μg/mL or disk diffusion (DD) ≤ 18 mm; imipenem or meropenem MIC ≥ 4 μg/mL or DD ≤ 19 mm.
- Pseudomonas aeruginosa: resistance to either imipenem or meropenem, defined as MIC ≥ 8 μg/mL or DD ≤ 15 mm for either agent.
- Acinetobacter baumannii: resistance to either imipenem or meropenem, defined as imipenem MIC ≥ 8 μg/mL or DD ≤ 18 mm, or meropenem MIC ≥ 8 μg/mL or DD ≤ 14 mm.
Interpretive criteria for tigecycline followed the recommendations of the U.S. Food and Drug Administration (FDA),15 while polymyxin B susceptibility was interpreted according to the standards of the European Committee on Antimicrobial Susceptibility Testing (EUCAST; https://www.eucast.org).
Quality Control
Quality control strains were included weekly in accordance with CLSI guidance: Escherichia coli ATCC 25922, Klebsiella pneumoniae ATCC 700603, and Pseudomonas aeruginosa ATCC 27853. These controls were used to verify the accuracy and reproducibility of species identification and susceptibility testing.
Data Management and Statistical Analysis
Laboratory data were entered and managed using WHONET version 5.6. Data entry included isolate identifiers, specimen source, species, antimicrobial agents tested, and susceptibility results. Analytical procedures comprised selection of appropriate WHONET modules for resistance and susceptibility analyses and construction of resistance profiles according to study objectives. Key parameters (isolate source, organism type, and target antimicrobials) were defined a priori. Outputs were exported as standardized reports and data tables for further interpretation in the clinical context. Descriptive analyses were performed to summarize isolate distribution and resistance patterns.
Results
Isolate Distribution and Specimen Sources
From 2021 to 2025, a total of 2523 CRGNB isolates were identified. The five most frequently detected species were Klebsiella pneumoniae (41.8%), Acinetobacter baumannii (22.1%), Escherichia coli (10.0%), Enterobacter cloacae (9.3%), and Pseudomonas aeruginosa (6.4%). Among these isolates, 56.4% were recovered from male patients. The highest isolation rate was observed in the 29 days to ≤1 year age group (41.8%), whereas the lowest rate occurred in the <3 to ≤14 years age group (17.2%). The majority of isolates were obtained from respiratory specimens (59.6%), followed by urine (6.1%), wound secretions (5.9%), and blood (5.7%) (Tables 1 and 2). Temporal trends in the detection of the five most common CRGNB species are shown in Figure 1, and their distribution across major specimen sources is presented in Figure 2.
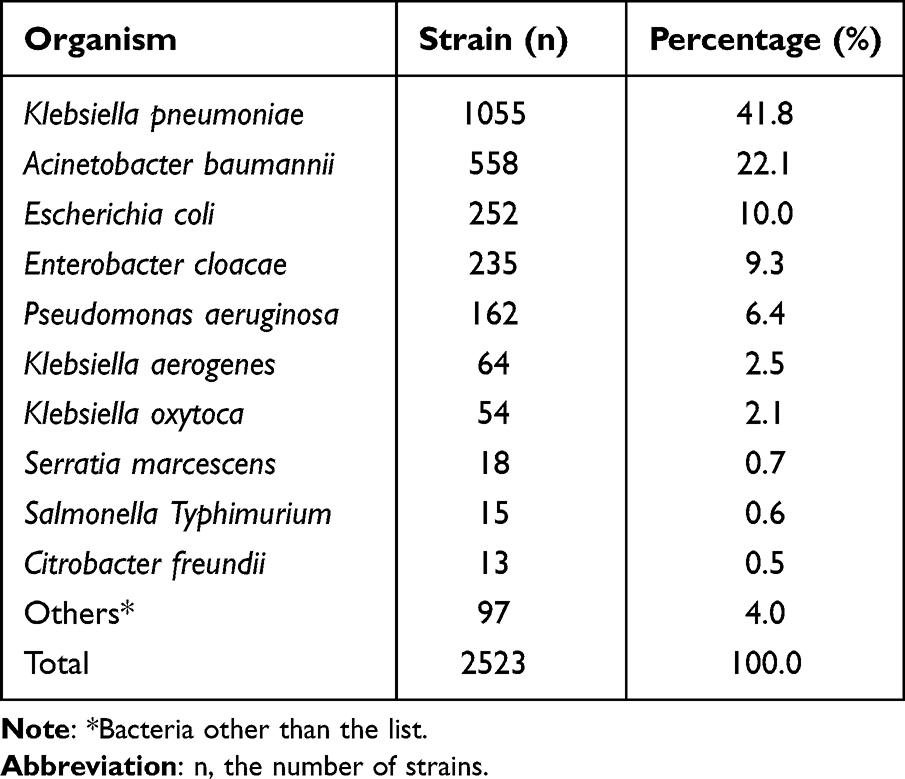 |
Table 1 Distribution of Major Pathogens in CRGNB Isolates |
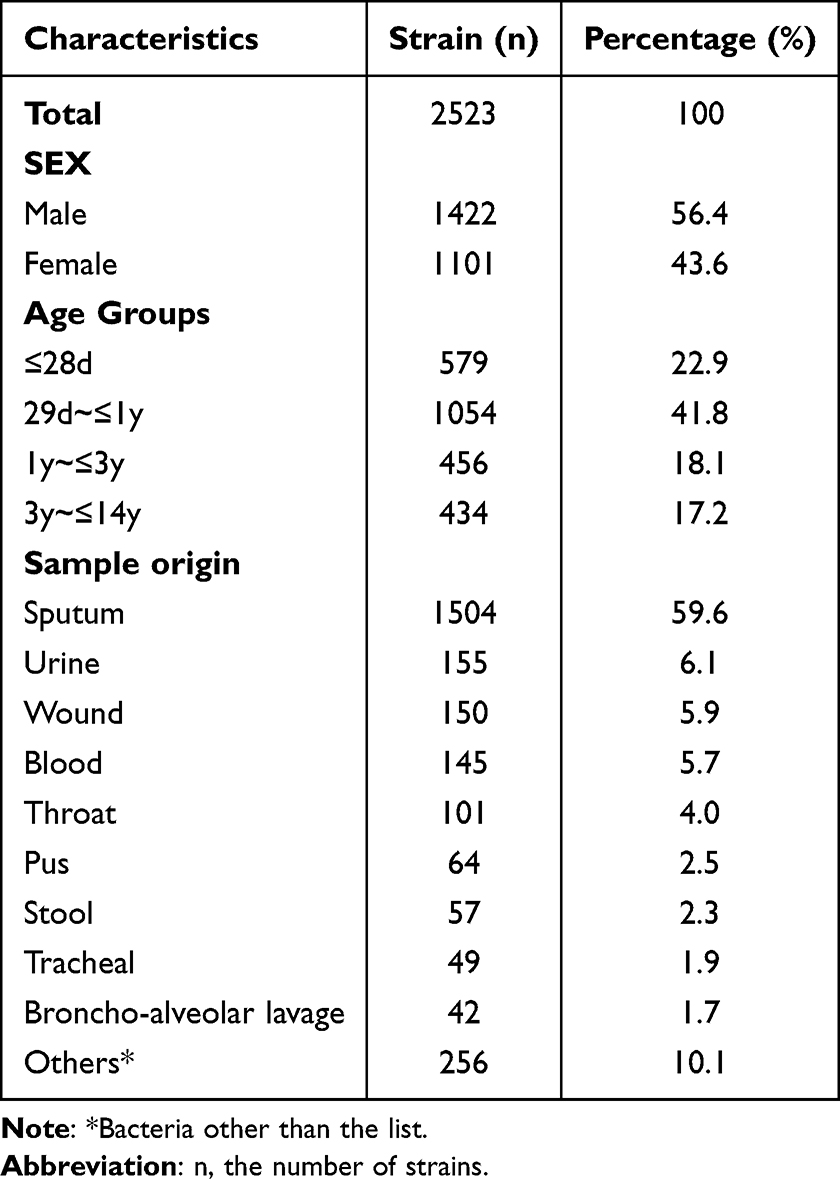 |
Table 2 Distribution Characteristics of CRGNB Isolates by Gender, Age Group and Specimen Source |
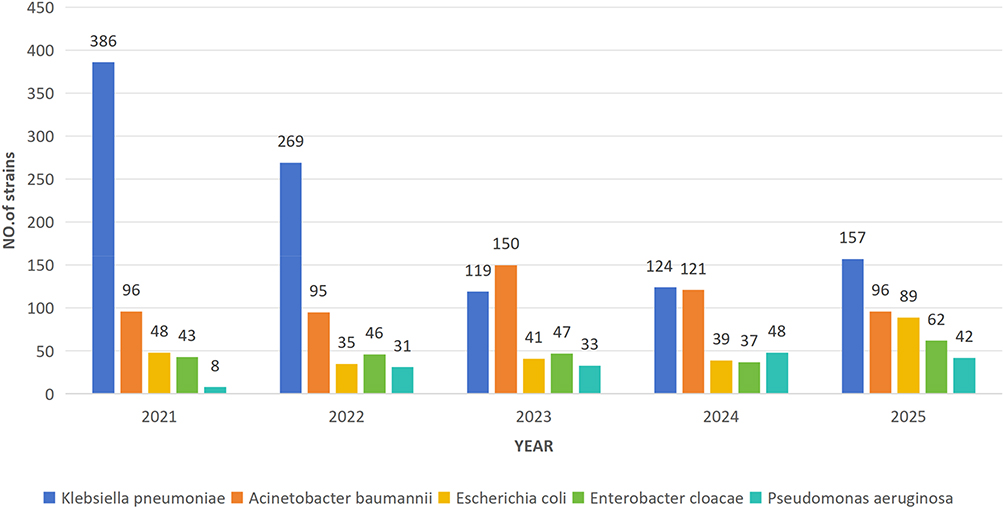 |
Figure 1 Detection trends of the top five CRGNB species. |
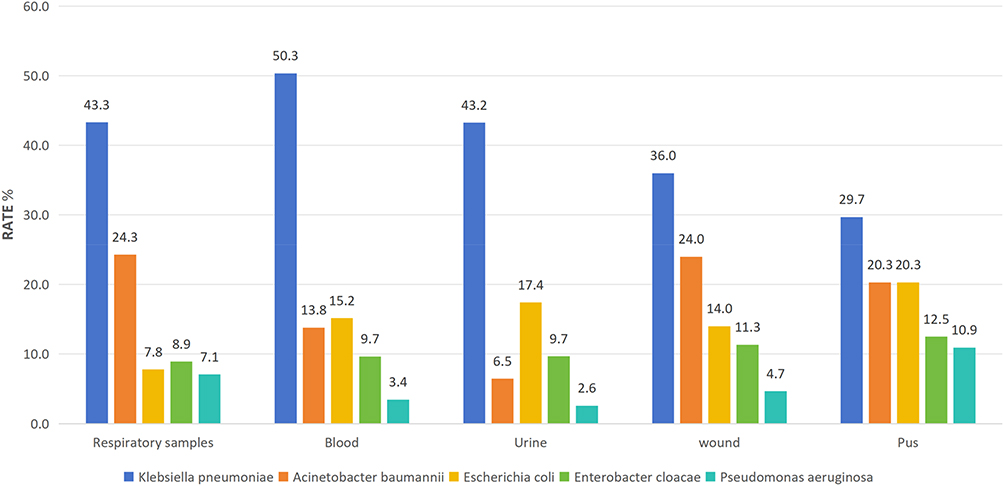 |
Figure 2 Proportional distribution of the top five CRGNB species across major specimen sources. |
Resistance and Susceptibility Among Major Enterobacterales
Resistance rates to β-lactam antibiotics among Carbapenem-resistant E. coli (CRECO), Carbapenem-resistant K. pneumoniae (CRKP), and Carbapenem-resistant E. cloacae (CRECL) ranged from 63.9% to 100.0%. Susceptibility to tigecycline was 100.0% for CRECO and 98.4% for both CRKP and CRECL. All three Enterobacterales species demonstrated polymyxin B susceptibility exceeding 96.0%. Susceptibility to ceftazidime-avibactam differed markedly by species: CRKP 87.5%, CRECO 6.9%, and CRECL 5.6% (Table 3).
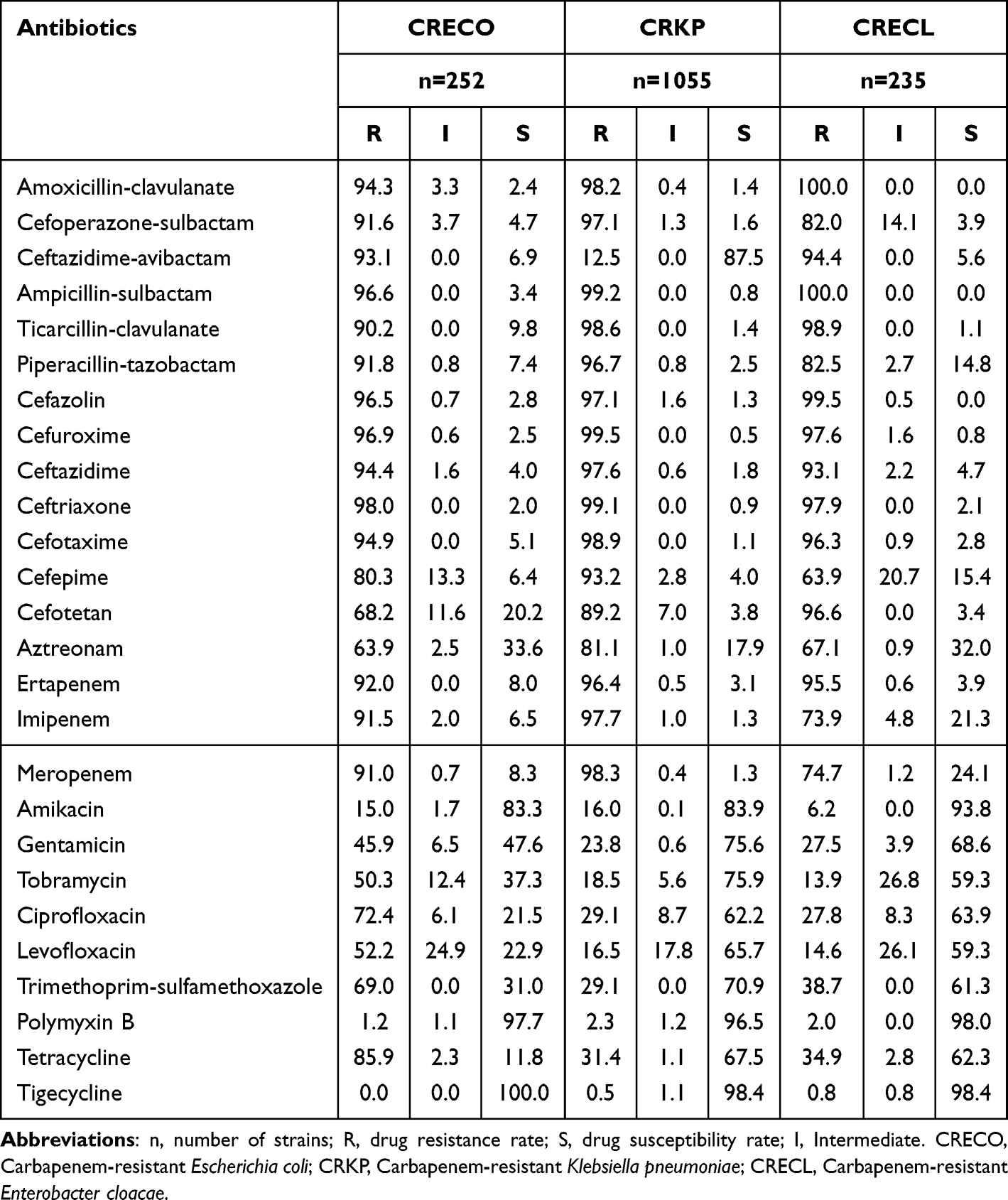 |
Table 3 Antimicrobial Resistance Profiles of CRECO, CRKP, and CRECL (%) |
Resistance and Susceptibility Among Major Non-Fermenters
Acinetobacter baumannii (CRAB) exhibited high resistance rates to the majority of tested antimicrobials (55.9–99.4%), while resistance to polymyxin B and tigecycline was low (2.3% and 2.5%, respectively) (Table 4). Pseudomonas aeruginosa (CRPA) showed 100.0% susceptibility to both ceftazidime-avibactam and polymyxin B; resistance rates to amikacin, tobramycin, and cefepime were all below 13.0% (Table 5).
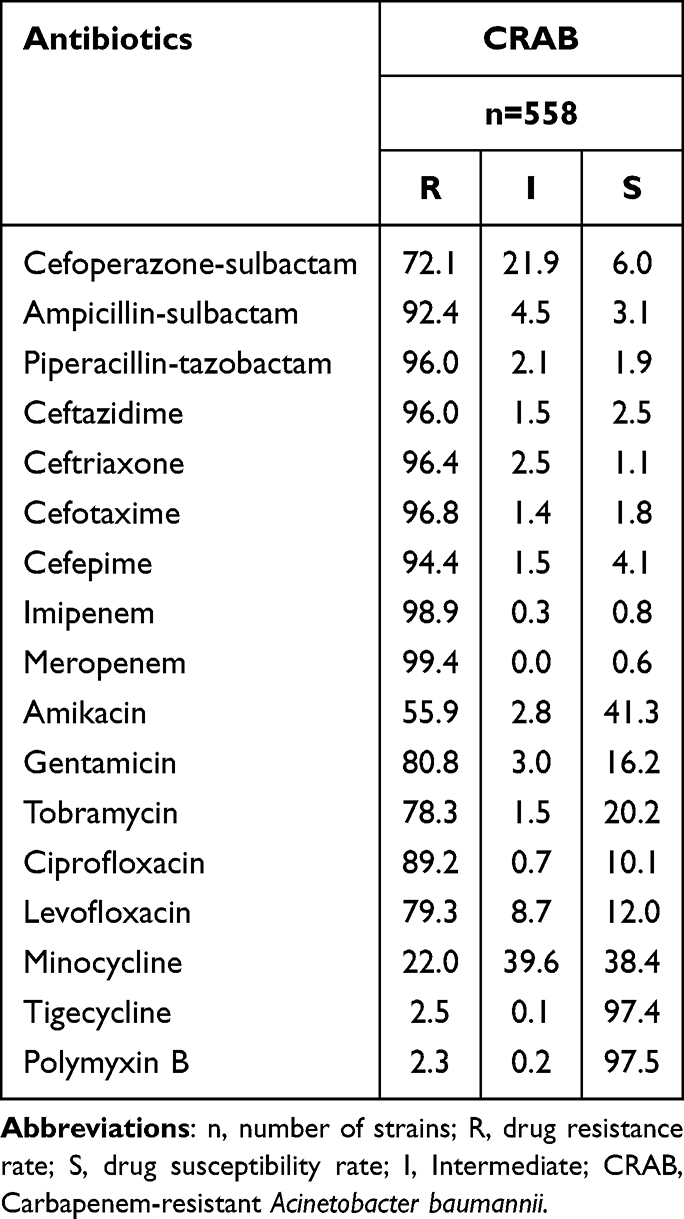 |
Table 4 Antimicrobial Resistance Profiles of CRAB (%) |
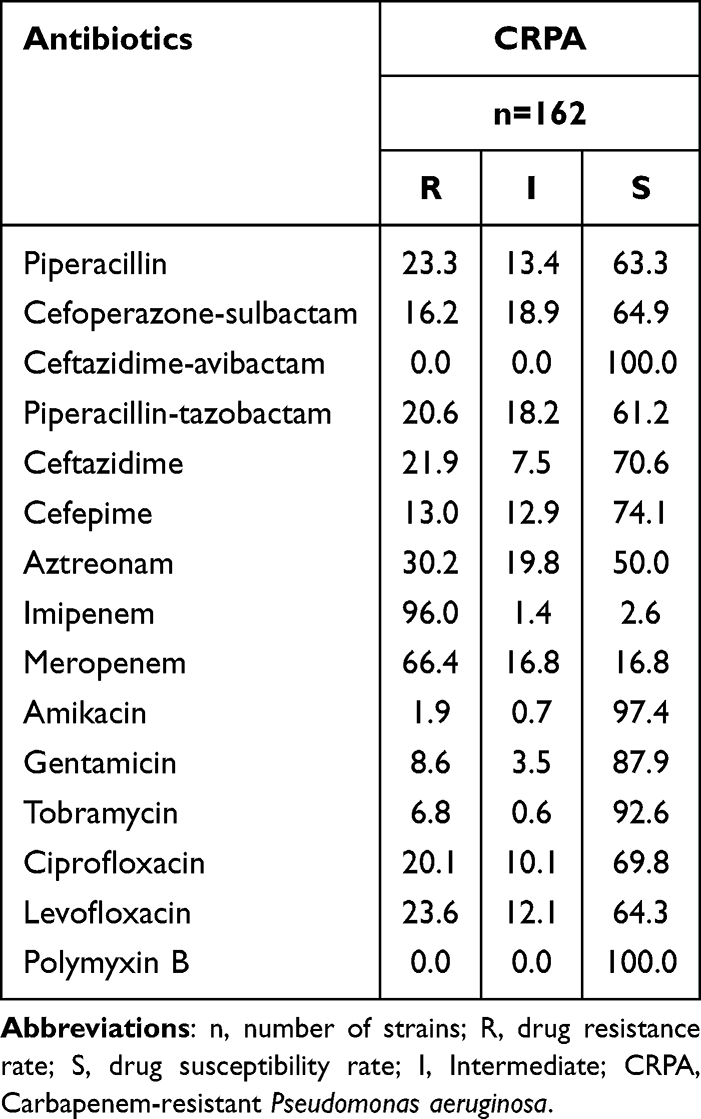 |
Table 5 Antimicrobial Resistance Profiles of CRPA (%) |
Temporal Changes in Major CRGNB Detection Rates
From 2021 to 2025, notable shifts were observed in the detection rates of major CRGNB species. Acinetobacter baumannii (CRAB) consistently accounted for the largest proportion, showing a fluctuating downward trend; the detection rate peaked at 17.8% in 2023 and subsequently declined to 9.8% in 2025. Klebsiella pneumoniae (CRKP) first decreased and then rebounded, declining from 16.3% in 2021 to 4.7% in 2023, followed by a rise to 5.8% in 2025. The detection rate of Enterobacter cloacae (CRECL) fluctuated but showed an overall increase, reaching 6.0%. In contrast, Pseudomonas aeruginosa (CRPA) and Escherichia coli (CRECO) remained at relatively low levels, fluctuating between 1.0–3.3% and 0.7%-1.5%, respectively. Overall, the dominant resistant strains shifted from early predominance of CRAB and CRKP toward a more balanced resistance spectrum (Figure 3).
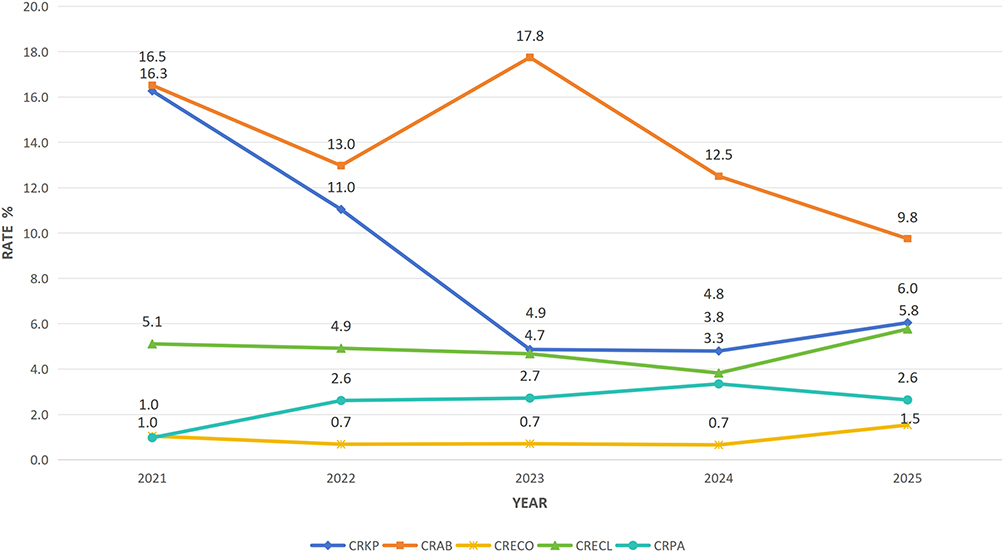 |
Figure 3 Temporal trends in detection rates of major CRGNB species, 2021–2025. |
Discussion
This study retrospectively analyzed 2523 non-duplicate CRGNB isolates recovered from pediatric patients across 134 medical institutions in Sichuan Province from 2021 to 2025. Klebsiella pneumoniae (41.8%) was the predominant species, followed by Acinetobacter baumannii (22.1%) and Escherichia coli (10.0%). Compared with national pediatric antimicrobial resistance surveillance data, the detection rate of CRKP in this region in 2025 was comparable to the overall national level16,17 and lower than those reported in Argentina (9.5%) and the United States (10.7%).18,19 In contrast, the detection rate of CRAB was markedly higher than that reported in Europe and North America.8,10,19 These findings suggest pronounced regional variation in the epidemiology of pediatric CRGNB, potentially associated with differences in antimicrobial usage patterns, infection control practices, and the underlying disease spectrum of pediatric patients in Southwest China.
In terms of population distribution, the highest isolation rate was observed in the 29 days to ≤1 year age group (41.8%), indicating that younger age and immature immune function may represent important risk factors for CRGNB colonization or infection in children. Previous studies have reported a higher prevalence of plasmid-mediated resistance genes among isolates from this age group,20 which may facilitate intra-ward dissemination of resistant strains. Consequently, neonatal and infant wards should be considered priority areas for infection prevention and control. In this study, the isolation rate in male patients (56.4%) was higher than that in females, which may be associated with a higher prevalence of underlying diseases and more frequent invasive procedures among male patients; however, the exact mechanism requires further investigation.
Analysis of specimen sources showed that respiratory samples accounted for the largest proportion (59.6%), consistent with reports of high respiratory CRGNB detection rates in pediatric intensive care units (PICUs) in China.21 This finding suggests that the respiratory tract is the most common site of CRGNB isolation in pediatric patients. Clinically, it is essential to distinguish colonization from infection. CRGNB isolated from the respiratory tract may represent true infection or merely mucosal colonization, with colonization being more common in asymptomatic patients without clear infection foci.22 Misinterpreting colonization as infection and initiating broad-spectrum antimicrobial therapy may further promote the selection and spread of resistant strains. Therefore, treatment decisions should be based on a comprehensive assessment of clinical manifestations, infection sites, and disease severity rather than solely on positive culture results.
From 2021 to 2025, the epidemiological trends of major CRGNB species exhibited dynamic fluctuations. The detection rate of CRKP declined from 16.3% to 4.9% before increasing again to 6.0%, whereas CRAB peaked in 2023 (17.8%) and subsequently declined. These patterns suggest that the prevalence of resistant organisms is closely associated with antimicrobial usage and infection control measures. Continuous surveillance of antimicrobial resistance and dynamic optimization of antimicrobial stewardship strategies are therefore essential for controlling the spread of multidrug-resistant organisms in pediatric populations.
In this study, carbapenem-resistant Enterobacterales (CRECO, CRKP, and CRECL) showed resistance rates of 63.9–100.0% to β-lactam antibiotics, while CRAB exhibited resistance rates of 55.9–99.4% to commonly used antimicrobial agents. These findings indicate that carbapenem resistance is frequently accompanied by cross-resistance and co-resistance phenotypes. Such extensive multidrug resistance substantially limits therapeutic options for pediatric CRGNB infections and increases clinical management difficulty. Accordingly, in addition to strengthening infection control for carbapenem-resistant organisms, enhanced surveillance and screening for multidrug-resistant bacteria are necessary, along with refined antimicrobial stewardship to curb their dissemination.
Antimicrobial susceptibility testing showed that CRE isolates exhibited susceptibility rates exceeding 96.0% to tigecycline and polymyxin B, higher than those reported in adult populations in the United States (tigecycline susceptibility 62.0%) and in Europe (polymyxin B susceptibility 75.0%).23,24 These findings suggest that both agents may serve as important therapeutic options for pediatric CRE infections in this region. Notably, CRKP demonstrated an 87.5% susceptibility rate to ceftazidime-avibactam, substantially higher than that observed for CRECO (6.9%) and CRECL (5.6%). This difference may be related to the predominance of serine carbapenemases, such as KPC enzymes, among previously reported isolates.25
CRAB exhibited resistance rates of 55.9–99.4% to commonly used antimicrobial agents and retained reliable activity only to tigecycline (2.5% resistance) and polymyxin B (2.3% resistance). Yi Xu et al previously reported that the prevalence of OXA-23 carbapenemase in Acinetobacter baumannii isolates in this region reached 94.7%, with 82.1% of strains simultaneously showing overexpression of the efflux pump gene adeB and loss of the outer membrane porin carO.26 The coexistence of multiple resistance mechanisms may synergistically contribute to the high resistance levels observed in this organism. Given the limited therapeutic options, early combination antimicrobial therapy and strengthened infection control measures should be considered. In contrast, Pseudomonas aeruginosa demonstrated 100.0% susceptibility to ceftazidime-avibactam and polymyxin B, providing a useful reference for empirical therapy of pediatric CRPA infections and showing more favorable results than those reported in global multicenter surveillance data (93.3%).27
Several limitations should be acknowledged. First, clinical outcome data were not collected, preventing evaluation of the therapeutic effectiveness of different antimicrobial regimens. Second, carbapenemase genotyping and investigation of non-enzymatic resistance mechanisms were not performed. Third, the participating institutions were predominantly tertiary hospitals, and the representation of primary healthcare facilities was limited. Future studies should incorporate prospective clinical designs, expand resistance mechanism analyses, and increase surveillance coverage in primary-level hospitals to establish a more comprehensive regional antimicrobial resistance monitoring network.
Conclusion
CRGNB burden remains substantial among pediatric isolates in Sichuan Province, with young infants representing a high-risk population and multidrug resistance being prominent. Clinical management should emphasize precise antimicrobial therapy guided by susceptibility testing, strict differentiation between colonization and infection, and strengthened infection prevention and control measures in neonatal and infant wards. Continuous multicenter surveillance of antimicrobial resistance is essential to provide high-quality evidence supporting regional antimicrobial stewardship, optimization of infection control strategies, and comprehensive prevention and management of resistant infections in pediatric populations.
Abbreviations
CRKP, Carbapenem-resistant Klebsiella pneumoniae; CRPA, Carbapenem-resistant Pseudomonas aeruginosa; CRAB, Carbapenem-resistant Acinetobacter baumannii; CRECO, Carbapenem-resistant Escherichia coli; CRECL, Carbapenem-resistant Enterobacter cloacae; CRE, Carbapenem-resistant Enterobacterales.
Acknowledgment
We thank all participating medical institutions and laboratory staff for their contributions to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Ten threats to global health in 2019. Available from: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
2. Naghavi M, Vollset SE, Ikuta KS, et al. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet. 2024;404(10459):1199–10. doi:10.1016/S0140-6736(24)01867-1
3. World Health Organization. Global leaders set first targets to control antimicrobial resistance crisis. Availble from: https://www.who.int/europe/news/item/27-09-2024-global-leaders-set-first-targets-to-control-antimicrobial-resistance-crisis.
4. Jesudason T. WHO publishes updated list of bacterial priority pathogens. Lancet Microbe. 2024;5(9):100940. doi:10.1016/j.lanmic.2024.07.003
5. CDC. 2019 Antibiotic Resistance Threats Report. Antimicrobial Resistance. April 11, 2025. Available from: https://www.cdc.gov/antimicrobial-resistance/data-research/threats/index.html.
6. Al Dabbagh M, Alghounaim M, Almaghrabi RH, et al. A narrative review of healthcare-associated gram-negative infections among pediatric patients in Middle Eastern Countries. Infect Dis Ther. 2023;12(5):1217–1235. doi:10.1007/s40121-023-00799-w
7. Jiang M, Li H, Liu X, et al. Genomic analysis revealed the international and domestic transmission of carbapenem-resistant Klebsiella pneumoniae in Chinese pediatric patients. Microb Spectr. 2023;11(2):e03213–22. doi:10.1128/spectrum.03213-22
8. Tesfa T, Mitiku H, Edae M, Assefa N. Prevalence and incidence of carbapenem-resistant K. pneumoniae colonization: systematic review and meta-analysis. Syst Rev. 2022;11(1):240. doi:10.1186/s13643-022-02110-3
9. Zhou J, Guoping L, Yan G. Antimicrobial resistance profile of clinical strains isolated from pediatrics intensive care unit in China: A report from the CHIPS program 2023. Chin J Evidence-Based Pediat. 2025;20(3):167–175.
10. Singh S, Sahoo RK, Sahu MC. Understanding recent developments in colistin resistance: mechanisms, clinical implications, and future perspectives. Antibiotics. 2025;14(10):958. doi:10.3390/antibiotics14100958
11. Zakhour R, Khafaja S, Korman R, et al. Rates of multidrug-resistant gram-negative bacterial infections in hospitalized non-immunocompromised pediatric patients: a 9-year retrospective study at a lebanese tertiary medical center. IDR. 2025;18:363–376. doi:10.2147/IDR.S488436
12. Sisay A, Asmare Z, Kumie G, et al. Prevalence of carbapenem-resistant gram-negative bacteria among neonates suspected for sepsis in Africa: a systematic review and meta-analysis. BMC Infect Dis. 2024;24(1):838. doi:10.1186/s12879-024-09747-6
13. Hawken SE, Snitkin ES. Genomic epidemiology of multidrug‐resistant Gram‐negative organisms. Annals New York Acad Sci. 2019;1435(1):39–56. doi:10.1111/nyas.13672
14. James S, Amy JM, April MB, Alexandra LB, Shelley C, Sharon KC. CLSI M100 Performance Standards for Antimicrobial Susceptibility Testing.
15. U.S. Food and Drug Administration. Tigecycline – injection products | FDA. Available from: https://www.fda.gov/drugs/development-resources/tigecycline-injection-products.
16. Yun L, Zheng B, Cui L. China antimicrobial resistance surveillance study (CARST) 2023–2024 gram-negative bacteria surveillance report. Chin J Clin Pharmacol. 2567–2587.
17. Liu J, Yan H, Yan G. Antimicrobial resistance surveillance of clinically isolated bacteria in paediatric intensive care units in China, 2020–2022. Chin J Infection Chemother. 2025;25(No.03):303–311.
18. Pellegrini JL, Aguirre C, Soto SM, et al. Resistencia a colistina en aislados de Klebsiella pneumoniae resistente a carbapenémicos en un hospital pediátrico de Corrientes. Rev Chil Infectol. 2022;39(2):109–116. doi:10.4067/S0716-10182022000200109
19. Grome HN, Grass JE, Duffy N, et al. Carbapenem-resistant and extended-spectrum β-lactamase–producing enterobacterales in children, United States, 2016–2020. Emerg Infect Dis. 2024;30(6). doi:10.3201/eid3006.231734
20. Jiang J, Zhang H, Lun H. Molecular epidemiological characteristics of Klebsiella pneumoniae infections in children. J Shanghai Jiao Tong Univ. 2025;2025(No.08):1027–1034.
21. Lin L, Liu Z, Qiao L. Pharmacological analysis of colistin B therapy for severe carbapenem-resistant gram-negative bacilli infections in paediatric patients. J Clin Paediat. 2025;2025:1
22. CDC. Antimicrobial Resistance. Antimicrobial Resistance 2025. Available from: https://www.cdc.gov/antimicrobial-resistance/index.html.
23. Goedken CC, Guihan M, Brown CR, et al. Evaluation of carbapenem-resistant Enterobacteriaceae (CRE) guideline implementation in the veterans affairs medical centers using the consolidated framework for implementation research. Implement Sci Commun. 2021;2(1):69. doi:10.1186/s43058-021-00170-5
24. Kon H, Abramov S, Amar Ben Dalak M, et al. Performance of Rapid PolymyxinTM NP and Rapid PolymyxinTM Acinetobacter for the detection of polymyxin resistance in carbapenem-resistant Acinetobacter baumannii and Enterobacterales. J Antimicrob Chemother. 2020;75(6):1484–1490. doi:10.1093/jac/dkaa050
25. Wang W, Wang L. GeneXpert testing system analyses carbapenem-resistant Enterobacteriaceae resistance genes in paediatric patients. Clin Lab Sci Clin Med. 2021;2021(No.10):1369–1372.
26. Xu X, Xu C, Salisu RB, Xu W. Beta-lactamase gene expression level of hospital-acquired CRAB isolated from children in Picu. IDR. 2021;14:3195–3205. doi:10.2147/IDR.S322604
27. Zalas-Więcek P, Prażyńska M, Pojnar Ł, et al. Ceftazidime/Avibactam and other commonly used antibiotics activity against enterobacterales and Pseudomonas aeruginosa isolated in Poland in 2015–2019. IDR. 2022;15:1289–1304. doi:10.2147/IDR.S344165
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.