Back to Journals » Journal of Pain Research » Volume 19
Prevalence, Trajectories, and Predictors of Persistent Postoperative Opioid Use in a Swiss University Hospital: A Prospective Observational Study
Authors Midez R ![]() , Jourdan EF
, Jourdan EF ![]() , Bourezg A, Rehberg B
, Bourezg A, Rehberg B ![]()
Received 10 October 2025
Accepted for publication 23 March 2026
Published 17 April 2026 Volume 2026:19 573377
DOI https://doi.org/10.2147/JPR.S573377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Timothy Atkinson
Remy Midez,1,2,* Eva-Francesca Jourdan,2,* Ali Bourezg,1 Benno Rehberg1
1Department of Anaesthesiology, Pharmacology, Intensive Care and Emergency Medicine, Division of Anesthesiology, Geneva University Hospitals and Faculty of Medicine, Geneva, Switzerland; 2Department of Anaesthesiology, Pharmacology, Intensive Care and Emergency Medicine, Division of Emergency Medicine, Geneva University Hospitals and Faculty of Medicine, Geneva, Switzerland
*These authors contributed equally to this work
Correspondence: Remy Midez, Email [email protected]
Background: Persistent postoperative opioid use (PPOU) is a growing concern, yet European data remain scarce. Switzerland has experienced a rise in opioid prescriptions, yet long-term opioid use after surgery is poorly characterized.
Methods: This single-center prospective observational cohort included adults undergoing elective surgeries at risk for chronic postsurgical pain at the University Hospitals of Geneva. Opioid consumption (morphine milligram equivalents) was assessed preoperatively, 24 h before discharge, and at 6 months. The primary objective was to quantify PPOU prevalence and trajectories at 6 months; secondary objectives were to identify clinical and psychological predictors of PPOU.
Results: Among 338 patients, 19% were preoperative opioid users; 32% of them continued opioids at 6 months. Overall, 8.6% of all patients had persistent opioid consumption, including 3% who were opioid-naïve before surgery. PPOU was most frequent after spine and orthopedic surgery.
Conclusion: Preoperative opioid use and type of surgery are key predictors of PPOU, highlighting spine and orthopedic procedures, and patients with preexisting pain, as priority targets for opioid-sparing and multimodal strategies.
Keywords: persistent postoperative opioid use, preoperative pain, opioid prescription patterns, orthopedic surgery
Introduction
Persistent postoperative opioid use (PPOU) has become a major public health concern, contributing to long-term opioid dependence even after minor surgical procedures.1 However, there is a lack of European data on long-term opioid use after surgery. A survey of European IASP chapters (EFIC) revealed disparities in opioid prescription rates,2 with Switzerland experiencing a significant increase in opioid sales as well as overdose cases over the past decade.3 While some European countries like Sweden have lower rates of opioid prescription compared to the US and Canada,4 data for other European countries are limited.5
Persistent postoperative opioid use varies widely (2 to 41%) across studies in European countries.6 A recent European registry study,7 as well as a large Austrian cohort study,8 found that new persistent opioid use after surgery is less prevalent in Europe compared to the US and Canada, but it may still be problematic in patients with chronic pain unrelated to surgery.
Management of acute pain often justifies use of opioids, but chronic postoperative opioid use has become a significant public health concern. Understanding the prevalence, causes, and factors associated with chronic postoperative opioid use is crucial. Notably, opioid use appears to be more problematic in patients with chronic pain unrelated to surgery.7 However, this study was based on registry data, and prospective studies from Europe are not available. In addition to surgical factors and preoperative opioid use, psychological variables such as anxiety, depression and pain catastrophizing have also been associated with persistent postoperative opioid use.9 We therefore assessed these variables preoperatively to explore their relationship with opioid use at six months.
To address these gaps in knowledge, our study aims to investigate the patterns of prolonged postoperative opioid consumption in a large university hospital of Switzerland. This is the first study of its kind in Switzerland and provides a unique opportunity to contribute to the existing literature. We conducted a single-center observational study, following patients for six months postoperatively, to identify if certain types of surgeries are associated with an increased risk of new persistent opioid use based on our postoperative opioid prescription practices.
Materials and Methods
This prospective observational study was conducted at the University Hospitals of Geneva, designed to identify patients who were at increased risk of developing CPSP and to determine the relationship between opioid consumption and the development of CPSP. Consumption of opioids at 6 months postoperatively was a pre-planned secondary outcome. The primary objective was to describe the prevalence and trajectories of persistent postoperative opioid use (PPOU) at 6 months after elective surgery in a Swiss university hospital. Secondary objectives were to identify predictors of opioid consumption at 6 months, including preoperative opioid use, pain characteristics, and psychological factors (anxiety, depression, and pain catastrophizing). The study was approved by the local ethics committee, Commission cantonale d’éthique de la recherche de Genève (CCER 2016–02111), conducted in accordance with the Declaration of Helsinki and was registered on clinicaltrials.gov (NCT03164954). All participants were provided with information about the study and signed a written consent form. This report follows the STROBE guidelines.10
Patient Cohort
Patient recruitment took place from July 1st, 2017 to November 1st, 2020. Patients aged 18 years or older, able to read and understand the information sheet and consent form, and scheduled for elective surgeries known to carry a risk of chronic postsurgical pain were included. Specifically, patients undergoing the following types of surgery were included: orthopedic surgery (total knee replacements, amputations except for toe amputations), spine surgery, cardiothoracic surgery (Sternotomy, thoracotomy, video-assisted thoracic surgery (VATS)), laparotomy (digestive, gynecological), inguinal hernia surgery, breast surgery (including plastic surgery).
Patients were screened and approached for participation in randomized order (sequences generated by random.org) from the operating theatre programs on the day of surgery, and written informed consent obtained the day after surgery. Patients unable to provide informed consent or not meeting these criteria were excluded.
Data Collection
After inclusion, patients completed a series of questionnaires, including the international pain outcomes questionnaire,11 the Hospital Anxiety and Depression Scale (HADS),12 the Pain Catastrophizing Scale (PCS)13 and a custom questionnaire for further potential CPSP risk factors (Appendix 1). This custom questionnaire was originally developed in French and was translated into English for the purposes of this publication (Appendix 1). Data extracted from the electronic anesthesia consultation record were collected, which allowed for the extraction of CPSP risk factors, including preoperative consumption of nonsteroidal anti-inflammatory drugs (NSAIDs), use of opioids, lithium, monoamine oxidase inhibitors (MAOIs), anxiolytics, comorbidities, and chronic pain at the surgical site. Specific antidepressant drug classes or molecules were not systematically collected. Data of preoperative opioid use were retrieved from the electronic anesthesia consultation record. Data from the electronic medical records were extracted to obtain the opioid consumption during the last 24 h before discharge. The electronic medical record does not contain information about opioid prescription at discharge, this information was retrieved manually from scanned documents in the patient chart.
Patients were then contacted again at 6 and 12 months postoperatively (by phone and/or email) to complete questionnaires, including the Brief Pain Inventory (BPI),14 Douleur Neuropathique 4 (DN4),15 analgesic use and opioid consumption. Due to the COVID-19 pandemic, the study team was unable to collect 12-month follow-up data and continue inclusion.
The postoperative management of opioids was left to the discretion of the clinical teams, without any specific study protocol being applied. At our institution, postoperative pain is routinely treated with multimodal, combining non‑opioid systemic analgesics and, when appropriate, regional techniques, but only opioid administration was collected in a standardized way and converted into MMEs for this analysis whereas other analgesic modalities were not protocolized or systematically recorded. The opioids were categorized as strong or weak, and the quantity consumed was noted. To standardize opioid consumption, we converted the consumption of each strong or weak opioid into morphine milligram equivalents (MMEs) using the conversion table of Nielsen et al16 These MME values were then reported for the following time points: preoperative, 24 hours before hospital discharge, and postoperative at 6 months. Preoperative opioid users were defined as patients who reported using opioids during the preoperative anesthesia consultation. Persistent opioid users were those who continued opioid use at 6 months post-discharge. New opioid users were patients who did not use opioids preoperatively but reported opioid use at 6 months postoperatively.
Statistical Methods
Sample Size
This analysis was pre-planned for a secondary outcome. No additional sample size calculation was performed; the trial was powered for the primary CPSP endpoint. Due to the impact of the COVID‑19 pandemic on research resources, recruitment was stopped early after enrolling 338 patients instead of the planned 450. All patients with available 6‑month opioid data were included in the present analysis (n=338).
Data Analysis
Descriptive statistics were performed using Stata version 17.0. To explore predictors of opioid consumption at six months, we applied the Boruta algorithm (version 8.0) in R 4.4.3. Boruta is a feature selection method based on the random forest algorithm, which iteratively assesses the relevance of each variable by comparing it to randomly permuted variables, thereby identifying the most important predictors in a robust manner.17
Results
Between July 1, 2017, and November 1, 2020, a total of 811 patients were screened for eligibility. Out of these, 355 patients were enrolled in the study. Of these, six patients were found to have already participated in the study, four patients withdrew their consent, one patient had his surgery cancelled, and two patients did not meet the inclusion criteria after the surgery was performed. The consolidated cohort consisted of 342 patients, with 4 patients deceased. Ultimately, 338 patients were included in the analysis (Figure 1).
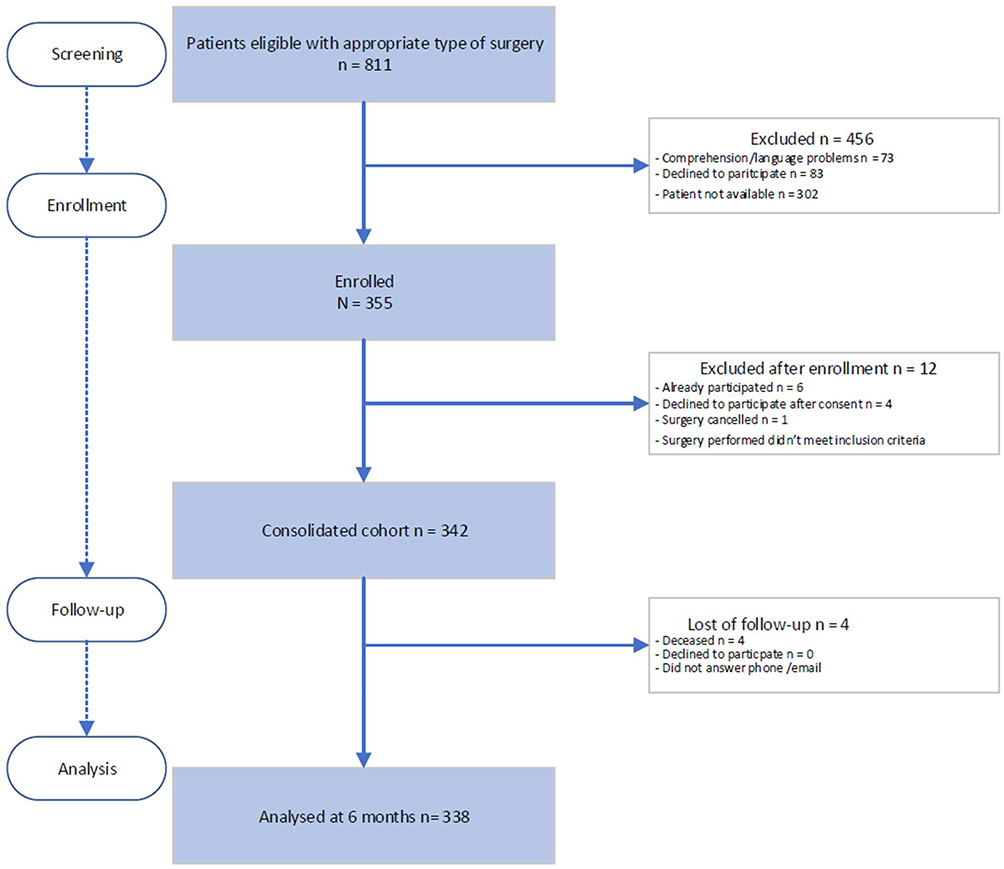 |
Figure 1 Flow chart of patient inclusion and analysis. Flow diagram of patient screening, inclusion, exclusions, loss to follow-up and final number of patients analyzed at 6 months (n = 338). A total of 811 patients were screened for eligibility, 355 were enrolled, 13 were excluded after enrollment, and 4 were not available at 6-month follow-up, leaving 338 patients for analysis. |
Patient characteristics are given in Table 1.
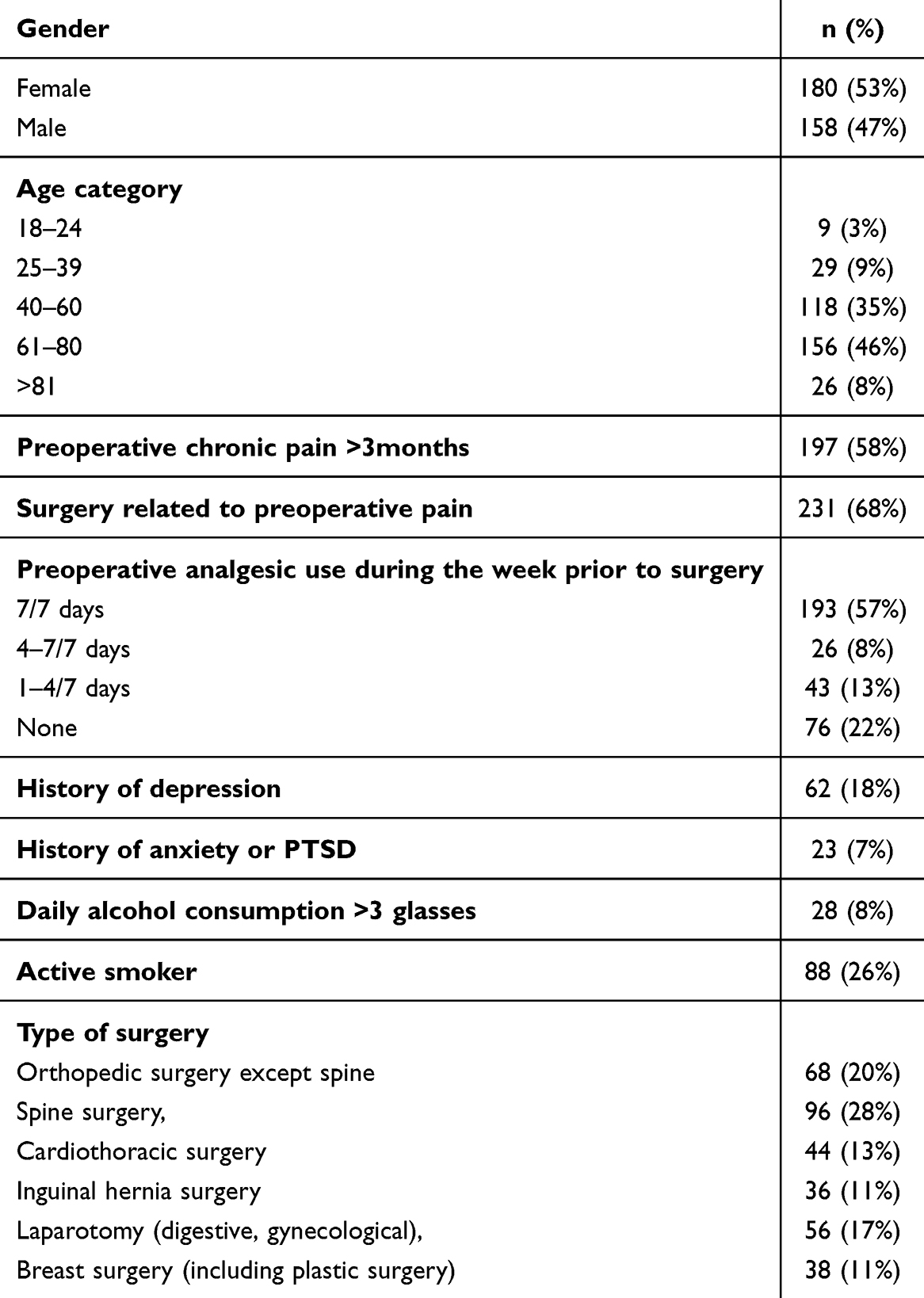 |
Table 1 Preoperative Patient Characteristics of the 338 Patients Included in the Analysis |
Opioid Use Trajectories for the Total Cohort
In this study, preoperative opioid users were defined as patients using opioids before surgery. Persistent opioid users continued opioid use at 6 months after surgery, while new opioid users initiated opioid therapy postoperatively and continued opioid use at 6 months after surgery. Overall, 29 out of 338 patients (8.6%) had persistent opioid consumption at 6 months, including 9 patients (3%) who were new persistent opioid users (ie, they had not used opioids preoperatively but continued using opioids prescribed after surgery). Opioid use trajectories are presented in Figure 2 in the form of a Sankey diagram.
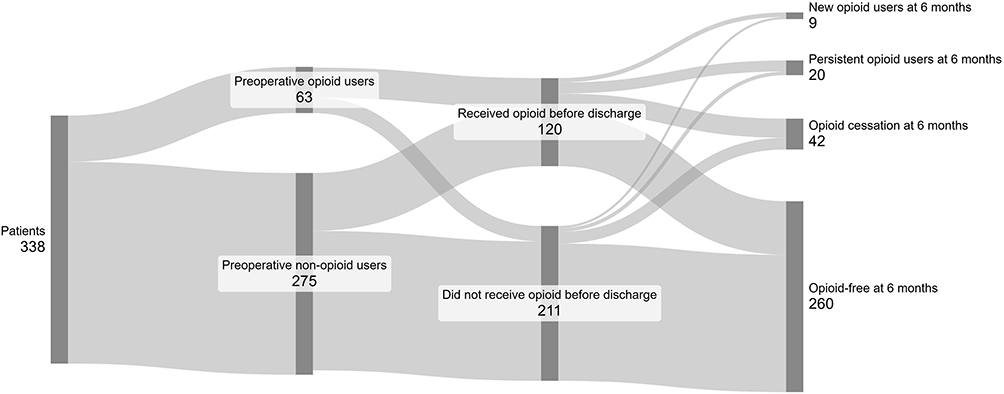 |
Figure 2 Opioid use for all patients analysed. Sankey diagram showing the progression of patients regarding their opioid use from the preoperative phase through 6 months post discharge. Patients: total number of patients analyzed. Preoperative opioid users: patients reporting opioid consumption during the anesthesia consultation prior to surgery. Opioid use 24 h before discharge: any weak or strong opioid received within 24 hours before hospital discharge. Opioid use at 6 months: self reported opioid use status at 6 months post discharge. New opioid users at 6 months: patients who were opioid naïve preoperatively and report opioid use at 6 months. Persistent opioid users at 6 months: patients who used opioids preoperatively and continue opioid use at 6 months. Opioid cessation at 6 months: patients who used opioids preoperatively and/or perioperatively but are no longer using opioids at 6 months. Opioid‑free at 6 months: patients who report no opioid use at 6 months. This group includes patients who never received opioids and those who may have received opioids perioperatively (including up to 24 h before discharge) but did not use opioids preoperatively or at 6 months. |
Opioid Use Trajectories for Patients Using Opioids Preoperatively
Among the 338 patients analysed, 63/338 (19%) were found to use opioids preoperatively. At discharge, 41/63 (65%) of the preoperative users had received opioids within 24 hours before discharge. At 6 months postoperatively, 20/63 (32%) of preoperative opioid users continued opioid use (persistent opioid users), while 43/63 (68%) discontinued use.
Opioid Use Trajectories for Patients Not Using Opioids Preoperatively
Of 275 patients not taking opioids before surgery, 79/275 (29%) received opioids within 24 h before discharge. Six months after surgery, 266/275 (97%) of these initially opioid‑naïve patients reported no opioid use at 6 months.
Opioid Use Trajectories in Relation to the Site of Preoperative Pain
Of the 338 patients analysed, 197 reported pain before surgery, but only 145 answered the question about the localisation of pain before surgery. Of these, 43 patients reported having pain at a different site than the operative site, and 102 reported pain at the surgical site.
Among the 102 patients reporting pain at the surgical site before surgery, 21 used opioids preoperatively, 14 received opioids within 24 hours before discharge, and 9 remained persistent users at day 180. Among the 81 patients with presurgical pain who did not use opioids preoperatively, 32 received opioids within 24 hours before discharge, and 5 became new opioid users at 6 months (Figure 3A).
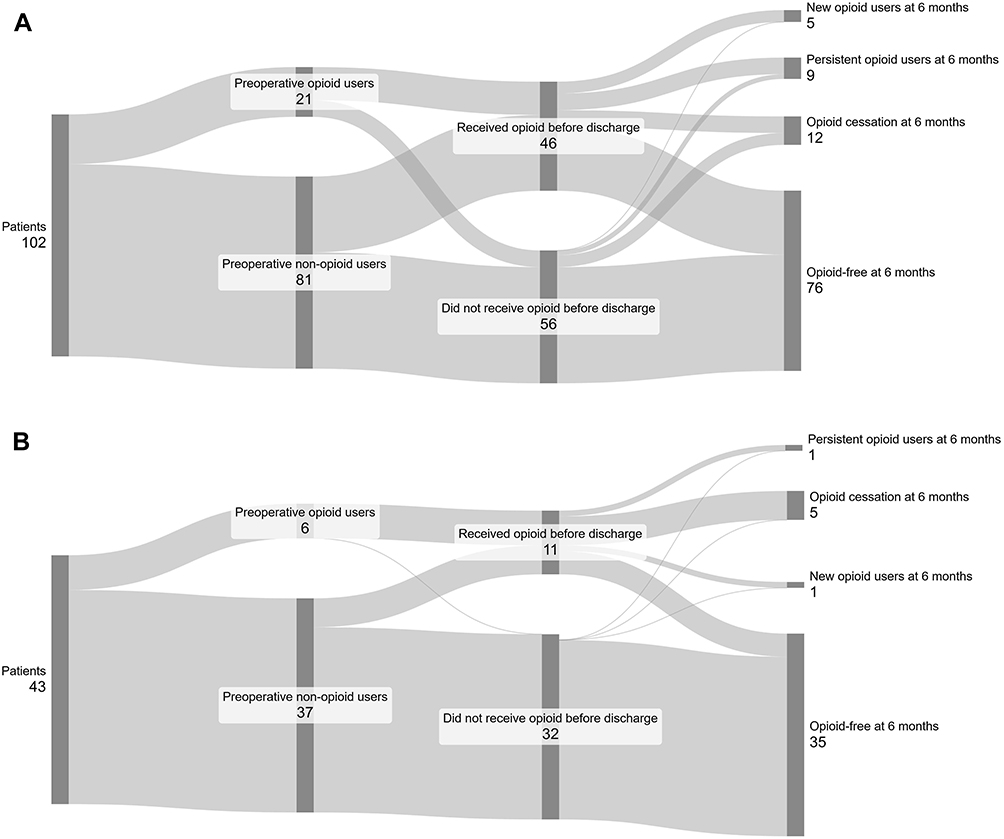 |
Figure 3 Opioid use in relation to site of preoperative pain. (A) patients with preoperative pain related to surgery. (B) patients with pain at a different site than the surgical site. Sankey diagrams showing trajectories of opioid use (preoperative, 24 h before discharge, 6 months). The 6-month categories are: new opioid users at 6 months, persistent opioid users at 6 months, opioid cessation at 6 months, and opioid free at 6 months, defined as in Figure 2. |
Among the 43 patients reporting pain before surgery unrelated to surgery, 6 (14%) used opioids before surgery, 4 received opioids within 24 hours before discharge, and only 1 patient was a persistent opioid user at 6 months. Of the 37 patients reporting pain before surgery unrelated to surgery and not using opioids before surgery, 7 received opioids within 24 hours before discharge, and 1 patient became a new opioid user at 6 months (Figure 3B).
Opioid Use Trajectories in Relation to the Type of Surgery
Most preoperative opioid users (N=63) underwent spine (42/63, 67%) or orthopedic surgery (13/63, 21%). As a corollary, preoperative opioid use rates were highest in spinal (44%) and orthopaedic surgeries (19%), with lower rates in cardio-thoracic (7%), inguinal hernia (3%), laparotomy (5%), breast surgery (3%). Persistent and new opioid users at 6 months were also predominantly from spinal (13 persistent and 3 new users) and orthopedic surgeries (6 persistent and 4 new users). Descriptive statistics by surgery type are presented in Figure 4.
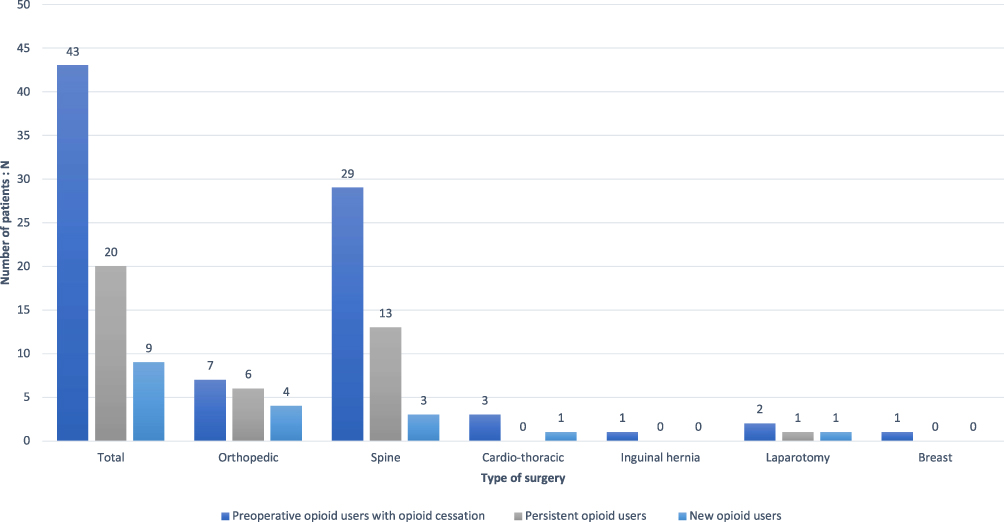 |
Figure 4 Distribution of opioid use status at 6 months across surgical types. Bar chart showing, for each surgical type (orthopedic, spine, cardiothoracic, inguinal hernia, laparotomy, breast), the number of patients in three categories of opioid status at 6 months: Preoperative opioid users with opioid cessation: patients who used opioids before surgery but report no opioid use at 6 months. Persistent opioid users: patients who used opioids preoperatively and continue opioid use at 6 months. New opioid users: patients who were opioid‑naïve preoperatively and report opioid use at 6 months. |
Opioid use was highest in spine (44%) and orthopedic (19%) surgery patients preoperatively, and 16.7% and 14.7% of these groups, respectively, were still using opioids at 6 months. Long-term opioid use was uncommon in other surgery types. For instance, 22/44 (50%) cardiothoracic patients received opioids within 24 h before discharge, but only 1/44 (2.3%) continued opioids at 6 months (Table 2).
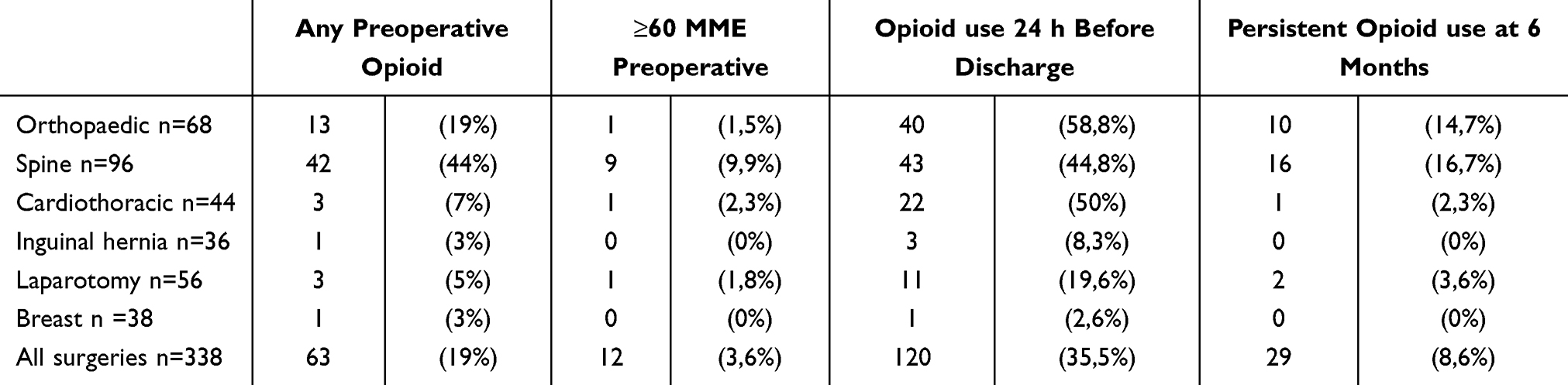 |
Table 2 Preoperative, Perioperative, and Persistent Postoperative Opioid Use by Surgical Type |
Predictors of Opioid Consumption at 6 months
To identify the most relevant predictors of opioid consumption at six months, we applied the Boruta algorithm (version 8.0) in R 4.4.3. Boruta is a wrapper method built around the random forest classification algorithm, designed to perform an exhaustive and unbiased feature selection. Unlike traditional methods that rely on arbitrary statistical thresholds, Boruta iteratively compares each predictor to artificially created “shadow variables” (randomized versions of the original features) and determines their importance based on multiple iterations. A variable is confirmed as important if it consistently outperforms all shadow features across the iterations, while irrelevant variables are discarded.
We chose Boruta for this analysis because of its robustness in handling complex interactions and its ability to account for potential nonlinear relationships in the data. Given the exploratory nature of our study, Boruta provides a comprehensive and reliable selection process, reducing the risk of overfitting while retaining relevant predictors.
Boruta identified four variables as important predictors of opioid consumption at six months: preoperative opioid consumption, anxiety score, depression score, and pain catastrophizing score. Conversely, eleven variables were deemed unimportant, including age, alcohol consumption and gender. One variable, surgical type, remained tentative, meaning its importance could not be conclusively determined within the iterations performed.
Discussion
Our study at the University Hospitals of Geneva revealed that 19% of patients were preoperative opioid users. Our preoperative opioid use rate was higher than that reported for other European hospitals by Hofer et al.7 This discrepancy may be explained by the selection and high proportion (68%) of patients in our cohort undergoing surgeries for chronic preoperative pain conditions, such as spine and orthopedic procedures, which have a well-documented association with prolonged opioid use.1
At six months, 32% of preoperative opioid users continued opioid consumption, defining them as persistent opioid users, and overall 8.6% of all patients remained opioid users, including 3% who developed new persistent opioid use.18 While this overall prevalence of 8.6% is higher than some US population-based reports,19 it likely reflects our high-risk cohort where 68% of patients had surgery-related preoperative pain. However, for specific high-risk procedures such as spine surgery, our rates remain lower than North American benchmarks.
Unlike Kent et al,18 our study defined postoperative opioid use (PPOU) based on patients’ self-reported consumption rather than prescription records or insurance claims. This approach may provide a more accurate representation of actual opioid use, as it accounts for variations in patient adherence and unused prescriptions that remain invisible in administrative data.
Our findings thus reinforce previous research identifying spine and orthopedic surgeries as high-risk for persistent opioid use. In our cohort, 43.75% of spine surgery patients were preoperative opioid users, and 44.8% of them continued opioid use at six months. These rates closely mirror those reported by Uhrbrand et al20 in a European cohort (51%) but remain significantly lower than the 82.4% observed in North America.21 Among opioid-naïve patients, our 4.5% persistence rate at six months was also lower than the 7% reported by Uhrbrand et al and much lower than the 17.5% observed by Gerlach et al.21
Concerning orthopedic surgeries, our findings align with European data. Preoperative opioid use was present in 19.1% of orthopedic patients, similar to 17.1% reported by Melis et al22 At six months, 14.7% of our orthopedic patients remained persistent opioid users, slightly above the 12.5% in Melis et al22 and close to the 13.7% observed in Stark et al.23 These results suggest a relatively stable prevalence of persistent opioid use after orthopedic surgery across European populations. Our findings on spine surgery are also more consistent with European data, while North American cohorts report significantly higher opioid persistence rates. This discrepancy may stem from differences in opioid prescribing regulations, patient expectations regarding pain management, and use of non-opioid analgesia.
Preoperative opioid use has been shown to be a strong predictor of PPOU, as emphasized by Kuck et al.24 Our study supports this notion, highlighting the importance of preoperative opioid use assessment in identifying patients at higher risk for prolonged postoperative opioid consumption. These results are in line with recent findings by Ramo et al9 who describe persistent postoperative opioid use as a distinct entity from chronic postsurgical pain, driven by factors such as preoperative opioid use, anxiety, depression, and pain catastrophizing. Our analysis confirms the relevance of these same predictors, emphasizing the need for targeted strategies in high-risk patients.
Patients with pain at the surgical site before surgery showed a higher likelihood of persistent opioid use at six months post-surgery (8.8%) compared to those with pain at a different site (2.3%). This suggests that preexisting pain at the surgical site may be a risk factor for prolonged postoperative opioid use. These findings are different from those reported by Hofer et al.7 While their study identified chronic pain unrelated to surgery as problematic for persistent postoperative opioid use, our results highlight the location of preoperative pain at the site of surgery as a risk factor for persistent opioid use. A potential explanation for this discrepancy is that Hofer et al7 included mostly general surgery patients, whereas our cohort consisted primarily of orthopedic patients operated for a chronic pain problem.
The low overall opioid consumption observed in our study, particularly as evidenced by prescription analysis, suggests that current postoperative pain management strategies at our institution may be effective in minimizing opioid use. This likely reflects the routine use of multimodal, opioid‑sparing perioperative analgesia, in line with recommendations advocating multimodal strategies to reduce long‑term opioid exposure. However, there is still room for improvement, especially for high-risk patients. Adams et al25 propose several strategies to improve postoperative pain management, including the implementation of multimodal analgesia approaches and enhanced patient education on pain management expectations and opioid risks. For patients with preoperative opioid therapy, Edwards et al26 emphasize the importance of preoperative opioid tapering when possible and close collaboration between pain specialists and surgeons to develop individualized postoperative pain management plans.
Furthermore, our results align with Fiore et al27 who highlight the benefits of non-opioid analgesic therapy after hospital discharge. This approach is particularly relevant given our observation that most patients who did not use opioids preoperatively remained opioid-free at six months post-surgery.
While our study provides valuable insights, it has limitations, including potential selection bias and reliance on self-reported opioid use. We did not systematically record the class of antidepressants, and therefore could not explore potential pharmacological interactions in relation to persistent opioid use. Future research should consider larger, multi-center studies to validate our findings and even get a stratification of detailed preoperative opioid use longer follow-up periods to assess long-term opioid use patterns, and integration of objective measures of opioid consumption.One challenge in our analysis was the imbalance in the outcome variable, with one class being underrepresented (the case of opioid consumption at 6 months). To address this, we tested a weighted version of the model to account for the imbalance. This adjustment did not alter the classification performance of the minority class, suggesting that the model’s ability to predict opioid consumption at six months remained stable regardless of class weighting.
Conclusion
Preoperative opioid use, preoperative pain at the surgical site and psychological factors (anxiety, depression, pain catastrophizing) were associated with prolonged postoperative opioid consumption at 6 months. Spine and orthopedic surgeries showed the highest rates of persistent postoperative opioid use in this cohort. These findings may help identify patients at higher risk who could benefit from targeted, opioid-sparing perioperative strategies.
Data Sharing Statement
Individual deidentified participant data (including data dictionaries) that underlie the results reported in this article will be made available upon reasonable request to the corresponding author Remy Midez for 5 years after publication. Study protocol and statistical analysis code will also be available.
Acknowledgments
We would like to thank the patients and medical staff at the University Hospital of Geneva for their participation and support in this study. We also acknowledge Sankeymatic.com for providing visualization tools that contributed to our data analysis. Finally, we appreciate the contributions of our research team and colleagues for their valuable insights and discussions throughout this project.
Author Contributions
The first two authors contributed equally to this work. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Brummett CM, Waljee JF, Goesling J, et al. New persistent opioid use after minor and major surgical procedures in US adults. JAMA Surg. 2017;152(6):e170504. doi:10.1001/jamasurg.2017.0504
2. Häuser W, Buchser E, Finn DP, et al. Is EUROPE also facing an opioid crisis?—A survey of European pain federation chapters. Eur J Pain. 2021;25(8):1760–11. doi:10.1002/ejp.1786
3. Hooijman MF, Martinez-De La Torre A, Weiler S, Burden AM. Opioid sales and opioid-related poisonings in Switzerland: a descriptive population-based time-series analysis. Lancet Reg Health Eur. 2022;20:100437. doi:10.1016/j.lanepe.2022.100437
4. Ladha KS, Neuman MD, Broms G, et al. Opioid prescribing after surgery in the United States, Canada, and Sweden. JAMA Network Open. 2019;2(9):e1910734. doi:10.1001/jamanetworkopen.2019.10734
5. Bosetti C, Santucci C, Radrezza S, Erthal J, Berterame S, Corli O. Trends in the consumption of opioids for the treatment of severe pain in Europe, 1990–2016. Eur J Pain. 2019;23(4):697–707. doi:10.1002/ejp.1337
6. Sitter T, Forget P. Persistent postoperative opioid use in Europe: a systematic review. Eur J Anaesthesiol. 2021;38(5):505–511. doi:10.1097/EJA.0000000000001346
7. Hofer DM, Harnik M, Lehmann T, et al. Trajectories of pain and opioid use up to one year after surgery: analysis of a European registry. Br J Anaesth. 2024;132(3):588–598. doi:10.1016/j.bja.2023.12.002
8. Bologheanu R, Bilir A, Kapral L, Gruber F, Kimberger O. New Persistent Opioid Use After Surgery. JAMA Network Open. 2025;8(2):e2460794. doi:10.1001/jamanetworkopen.2024.60794
9. Ramo S, Frangakis S, Waljee JF, Bicket MC. Risk factors for persistent postoperative opioid use: an entity distinct from chronic postsurgical pain. Reg Anesth Pain Med. 2025;50(2):121. doi:10.1136/rapm-2024-105599
10. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
11. Rothaug J, Zaslansky R, Schwenkglenks M, et al. Patients’ perception of postoperative pain management: validation of the International Pain Outcomes (IPO) questionnaire. J Pain. 2013;14(11):1361–1370. doi:10.1016/j.jpain.2013.05.016
12. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
13. Sullivan MJL, Bishop SR, Pivik J. The Pain Catastrophizing Scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
14. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singap. 1994;23(2):129–138.
15. Bouhassira D, Attal N, Alchaar H, et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain. 2005;114(1):29–36. doi:10.1016/j.pain.2004.12.010
16. Nielsen S, Degenhardt L, Hoban B, Gisev N. A synthesis of oral morphine equivalents (OME) for opioid utilisation studies. Pharmacoepidemiol Drug Saf. 2016;25(6):733–737. doi:10.1002/pds.3945
17. Kursa MB, Rudnicki WR. Feature Selection with the boruta package. J Stat Soft. 2010;36(11):1–13. doi:10.18637/jss.v036.i11
18. Kent ML, Hurley RW, Oderda GM, et al. American society for enhanced recovery and perioperative quality initiative-4 joint consensus statement on persistent postoperative opioid use: definition, incidence, risk factors, and health care system initiatives. Anesthesia Analg. 2019;129(2):543–552. doi:10.1213/ANE.0000000000003941
19. Schoenfeld AJ, Cooper Z, Banaag A, et al. Long-term prescription opioid use following surgery in the US (2017–2022): a population-based study. Lancet Reg Health Am. 2024;40:100948. doi:10.1016/j.lana.2024.100948
20. Uhrbrand P, Helmig P, Haroutounian S, Vistisen ST, Nikolajsen L. Persistent opioid use after spine surgery: a prospective cohort study. Spine. 2021;46(20):1428. doi:10.1097/BRS.0000000000004039
21. Gerlach EB, Plantz MA, Swiatek PR, et al. The drivers of persistent opioid use and its impact on healthcare utilization after elective spine surgery. Global Spine J. 2024;14(2):370–379. doi:10.1177/21925682221104731
22. Melis EJ, Vriezekolk JE, van der Laan JCC, Smolders JMH, van den Bemt BJF, Fenten MGE. Long-term postoperative opioid use in orthopaedic patients. Eur J Pain. 2024;28(5):797–805. doi:10.1002/ejp.2219
23. Stark N, Kerr S, Stevens J. Prevalence and predictors of persistent post-surgical opioid use: a prospective observational cohort study. Anaesth Intensive Care. 2017;45(6):700–706. doi:10.1177/0310057X1704500609
24. Kuck K, Naik BI, Domino KB, et al. Prolonged opioid use and pain outcome and associated factors after surgery under general anesthesia: a prospective cohort association multicenter study. Anesthesiology. 2023;138(5):462–476. doi:10.1097/ALN.0000000000004510
25. Adams TJ, Aljohani DM, Forget P. Perioperative opioids: a narrative review contextualising new avenues to improve prescribing. Br J Anaesth. 2023;130(6):709–718. doi:10.1016/j.bja.2023.02.037
26. Edwards DA, Hedrick TL, Jayaram J, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on perioperative management of patients on preoperative opioid therapy. Anesth Analg. 2019;129(2):553–566. doi:10.1213/ANE.0000000000004018
27. Fiore JF, El-Kefraoui C, Chay MA, et al. Opioid versus opioid-free analgesia after surgical discharge: a systematic review and meta-analysis of randomised trials. The Lancet. 2022;399(10343):2280–2293. doi: 10.1016/S0140-6736(22)00582-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.