Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Prevalence of work-related musculoskeletal disorders and ergonomic practice among dentists in Jeddah, Saudi Arabia
Authors Meisha DE ![]() , Alsharqawi NS
, Alsharqawi NS ![]() , Samarah AA
, Samarah AA ![]() , Al-Ghamdi MY
, Al-Ghamdi MY ![]()
Received 7 February 2019
Accepted for publication 10 June 2019
Published 5 July 2019 Volume 2019:11 Pages 171—179
DOI https://doi.org/10.2147/CCIDE.S204433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Dalia E Meisha,1 Nujud S Alsharqawi,2 Ahmad A Samarah,3 Mohammed Y Al-Ghamdi4
1Department of Dental Public Health, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 2Dental Department, King Salman Armed Forces Hospital, Tabuk, Saudi Arabia; 3Department of Pediatric Dentistry, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Background: Musculoskeletal disorders (MSD) is the second most common cause of disability. MSD due to the occupation are called work-related musculoskeletal disorders (WMSD) and are common among dentists.
Objective: Assess the prevalence of self-reported work-related musculoskeletal disorders (WMSD) and to identify associated ergonomic practice among dentists practicing in Jeddah City, Saudi Arabia.
Methods: Dentists practicing in Jeddah were invited to participate in this cross-sectional study using a self-administered survey. The survey consisted of 20 close-ended questions. The survey included questions regarding demographics, dental practice, general health status, exercising, ergonomic practice, musculoskeletal pain location, the severity of pain using a numeric pain rating scale (0–10), interventions sought, and missed work due to WMSD.
Results: A sample of 234 dentists participated in this study. Prevalence of WMSD was found to be 70%. The most common location for WMSD pain was in the low back (85%) and neck (84.6%). Female dentists and dentists not exercising regularly had an increased risk of WMSD. The prevalence of CTS was 9%, and its risk increased with age and practicing in the private sector. Among the dental specialties, the least to report WMSD or CTS were maxillofacial surgeons and orthodontists. The reported ergonomic practice reached as low as 24%.
Conclusion: Work-related musculoskeletal disorders and inadequate ergonomic practices were common. Ergonomics training intervention programs targeting dentists is suggested as a preventive measure for longer and healthier career lives.
Keywords: musculoskeletal disorders, carpal tunnel syndrome, ergonomic, pain, dentist, Saudi
Introduction
The Center for Disease Control and Prevention in the USA defines musculoskeletal disorders (MSD) as “injuries or disorders of the muscles, nerves, tendons, joints, cartilage, and spinal discs.”1 The Global Burden Disease Study recognized MSD as the second most common cause for disability, with the most prevalent condition being low back pain (42.9% increase in years lived with disability from 1999 to 2010).2 Musculoskeletal disorders due to the occupation are called work-related musculoskeletal disorders (WMSD) and are common among dentists.3 This is attributed to the nature of dental work being in a restricted field, sitting for a prolonged time with an awkward body position, and using heavy forces in repetitive movements compounded by a lack of recovery breaks and exercises. WMSD may also affect dentists’ quality of life negatively and lead to early retirement.4
Carpal tunnel syndrome (CTS) is caused by compression of the median nerve in the carpal tunnel manifested as pain, and numbness in fingers innervated by the median nerve.5 It is more common in the dominant hand. The etiology of CTS is mostly idiopathic, but predisposing factors include repetitive movements, injury or trauma, and pregnancy. Recent research indicates that dentists have a higher risk of developing CTS due to frequent pressure from wrist movements, thus causing inflammation of bending tendons and compression of the median nerve.6
Hayes et al systematic review reported a high prevalence of WMSD among dental professionals, ranging between 64% and 93%. For dentists, the authors found that back pain was the most prevalent region for pain (36.3–60.1%) followed by neck pain (19.8–85%), whereas for dental hygienists, hand and wrist pain were the most prevalent (60–69.5%).4 A higher occurrence of severe WMSD pain was found in women, with a higher prevalence of wrist pain among oral surgeons compared to other dental professionals.7 The prevalence of CTS ranged from 10.3%8 to 86% among dentists.9 It increased with age and working hours per week.6
During the last decade, several studies investigated the prevalence of WMSD or CTS among practicing dentists in Australia,10 Brazil,11 China,12 Czech Republic,13 India,9 Iran,14 Pakistan,8 Spain,7 Taiwan,15 and Turkey.16 Studies investigating MSD in Saudi Arabia focused either on dental students as the population of interest,17,18 or in specific regions of Saudi Arabia as Riyadh,19,20 and Hail.21 A high prevalence of WMSD (90.2%) was reported among dentists practicing in Riyadh. Pain in the low back (68.1%) was the most prevalent location of pain, followed by neck pain (34.3%). General dentists and maxillofacial surgeons reported less WMSD than other specialties. Risk factors that significantly increased the odds of low back and shoulder pain were age, being female, appointment duration, and years of practice.19 Another study in Riyadh reported that dental students or private sector dentists had double the risk of WMSD compared to the governmental sector dentists.20 The few studies exploring the prevalence of MSD among Saudi dentists did not examine associated ergonomic practices. There is a need to understand the Saudi ergonomic practices related to WMSD among Saudi dentists.
The objectives of this study were to assess the prevalence of self-reported WMSD, including CTS among dentists practicing in Jeddah City, Saudi Arabia, and to identify associated ergonomic practice.
Methods
This cross-sectional study design utilized a self-administered survey of a random sample of dentists practicing in Jeddah City, Saudi Arabia. Invited dentists included those practicing in a dental school setting, governmental hospitals, primary healthcare centers and private dental clinics.
Inclusion criteria for this study were dentists currently practicing in Jeddah. Retired dentists or dental students were excluded from this study, as were dentists practicing outside of Jeddah City. Dentists were invited to participate over a period of 5 months. No compensation was provided for participation in this study. Ethical approval for the study protocol was obtained from King Abdulaziz University Faculty of Dentistry research ethics committee conforming to the principles of Helsinki Declaration. Written informed consent was obtained from dentists who agreed to participate in this survey.
The sample size was calculated using the single proportion formula based on the reported prevalence of WMSD (36%).4 Population size was set at 2,567,22 since about 65% of Makkah-region dentists practice in Jeddah out of 3,967 practicing dentists in the Makkah region.23 Thus, a minimum sample size of 225 dentists was therefore required for this study. Assuming a response rate of 60%,24 three hundred sixty surveys were planned for distribution.
The survey consisted of 20 close-ended questions divided into four main sections. The first section asked the dentists about demographics (gender, age), type and duration of the dental practice, general health status, and exercise habits. The second section was adopted from Diaz-Caballero et al’s questionnaire.25 It included questions about ergonomic practices, musculoskeletal pain location adopted from Nordic questionnaires for the analysis of musculoskeletal symptoms,26 and severity of pain using a numeric pain rating scale from 0 (no pain) to 10 (worst pain possible).27 The third section asked about CTS by asking: “Do you have Carpal tunnel syndrome?”. The fourth section asked about interventions sought and missed work due to WMSD.
Statistical analyses were performed using the Statistical Package for Social Sciences (IBM®SPSS® Statistics) Version 24.0.28 Descriptive summary statistics, including frequencies and percentages, were calculated. Bivariate analyses using a Chi-square tests or Fisher Exact test, as appropriate, were performed. Kruskal-Wallis test was used to test for differences in terms of the pain rating scale between different categories. Multiple logistic regression models were used to predict dentists experiencing WMSD and CTS. The outcomes of the study were dichotomous variables—dentists reporting having WMSD or CTS versus those not. All hypotheses were tested at a significance level of 0.05.
Results
Of the 360 Saudi dentists practicing in Jeddah who received the surveys, Two hundred thirty-four dentists responded and completed the survey (response rate of 65%). Table 1 shows the demographic distribution of responding dentists in this study sample. Dentists participated almost equally by gender. Three out of four respondents were practicing in the governmental sector. In terms of the specialty of responding dentists, approximately half of the dentists were general or restorative dentists. More than half of the dentists (56%) reported playing a type of sport or exercising; however, only 39% reported doing so on a regular basis. Only 5% of dentists reported having muscular pain due to a chronic medical condition.
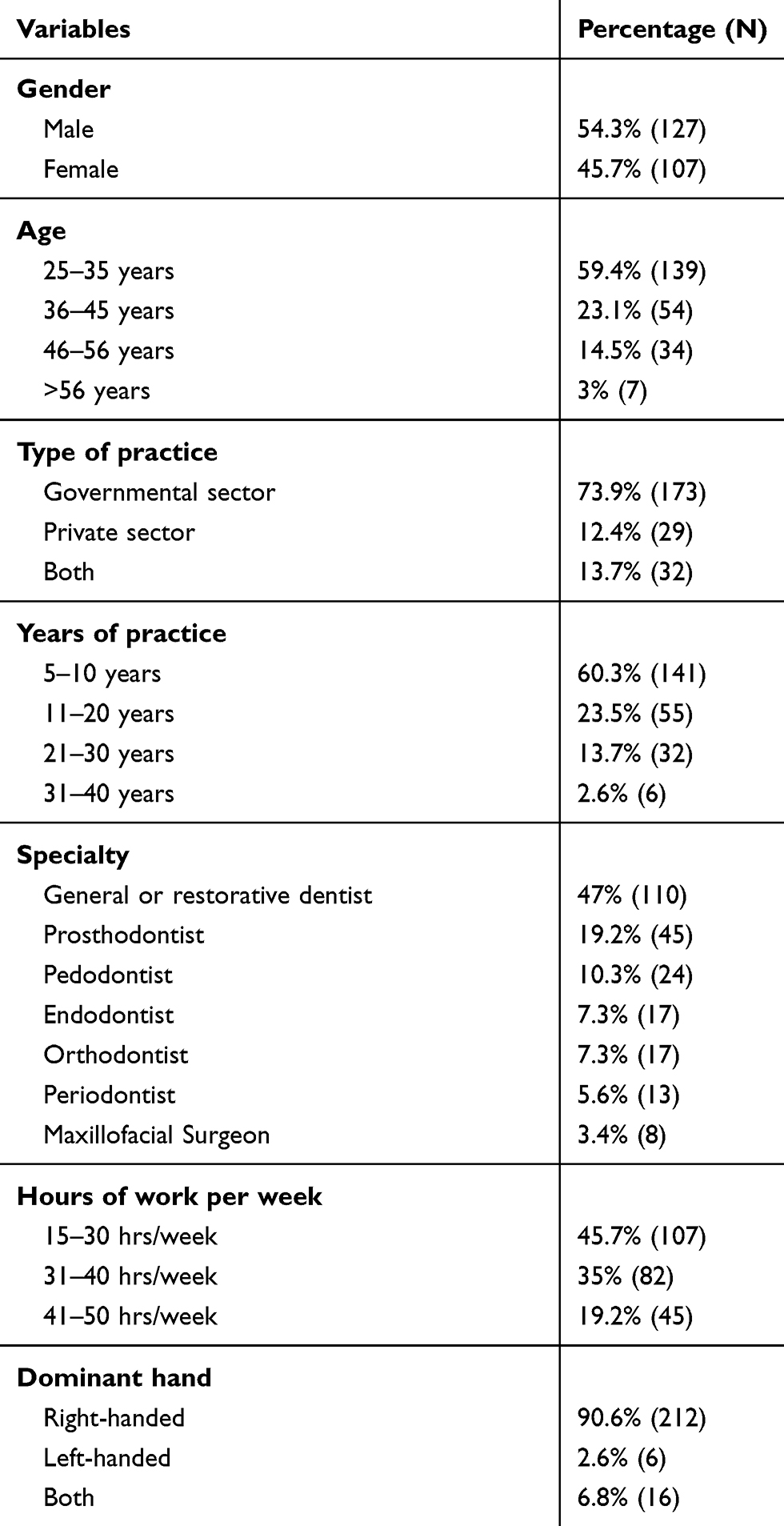 |
Table 1 Demographic and dental practice characteristics of responding dentists in Jeddah. |
Seventy percent of dentists in Jeddah reported having MSD due to dental practice. Carpal tunnel syndrome was reported by only 9% of dentists in this study. The three most common locations for WMSD pain were in the low back (85%), and neck (84.6%), followed by the shoulders (81.2%). Female dentists reported significantly more WMSD (Unadjusted Odds Ratio (OR): 2.8, Confidence Interval (CI): 1.5–5.2) and more CTS (OR: 3.5, CI: 1.3–9.4) compared to male dentists. Figure 1 shows the median pain score (0–10) and frequency of MSD symptoms (%) for male and female dentists in this sample. The median pain score was significantly higher for female dentists for neck, shoulders, upper back, elbows, and wrists/hands compared to male dentists.
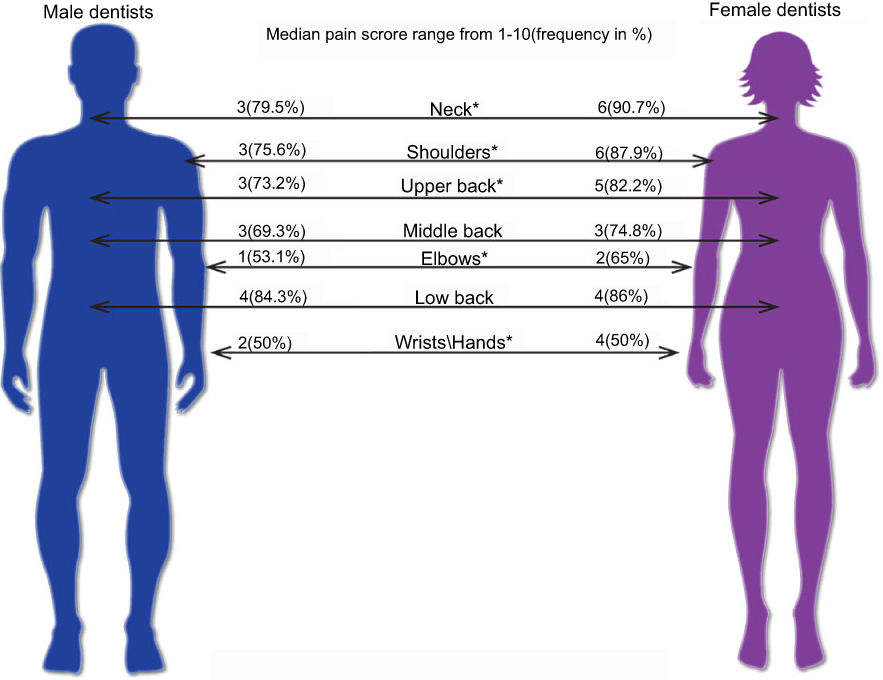 |
Figure 1 Median of pain score (0–10) and frequency of musculoskeletal disorders symptoms (in percentage) among male and female dentists in Jeddah. Note: *Statistically significant differences at alpha of 0.05. |
Dentists practicing in the private sector reported more WMSD (OR: 2.3, CI: 0.8–6.3) and CTS (OR: 3.9, CI: 1.4–10.9) compared to dentists working in the governmental sector. In comparison to general/restorative dentists, the least likely specialty to report WMSD or CTS were maxillofacial surgeons and orthodontists. When comparing the severity of WMSD by pain location among the different dental specialties, the distribution of shoulders pain was significantly different (P: 0.02). Moreover, the severity of shoulders pain was highest among periodontists and lowest among orthodontists (Figure 2).
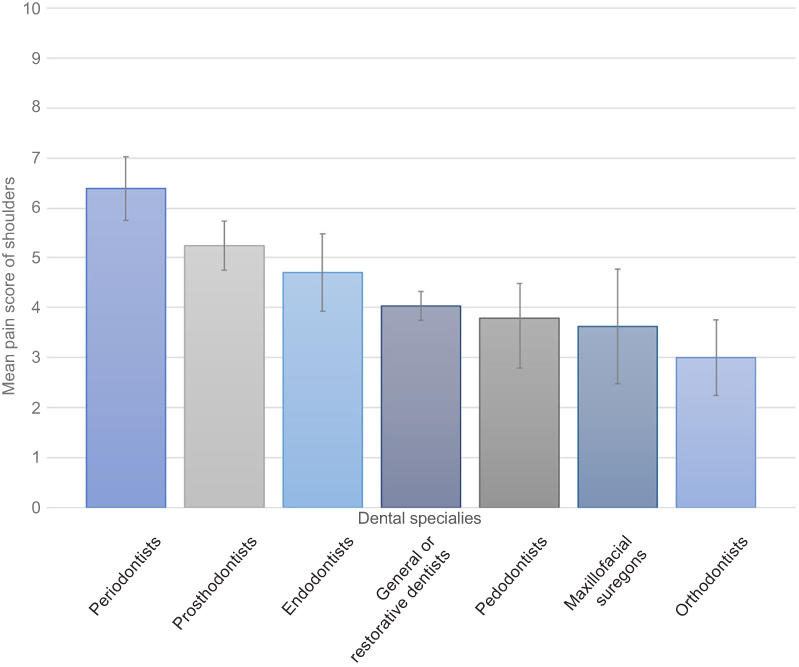 |
Figure 2 Frequency of musculoskeletal disorders among the different dental specialties. |
Table 2 presents the multiple logistic regression model predicting WMSD among Jeddah dentists versus those who did not report WMSD. The logistic regression model was statistically significant, P<0.0001. The model explained 24.9% (Nagelkerke R2) of the variance in WMSD and correctly classified 71.8% of cases.
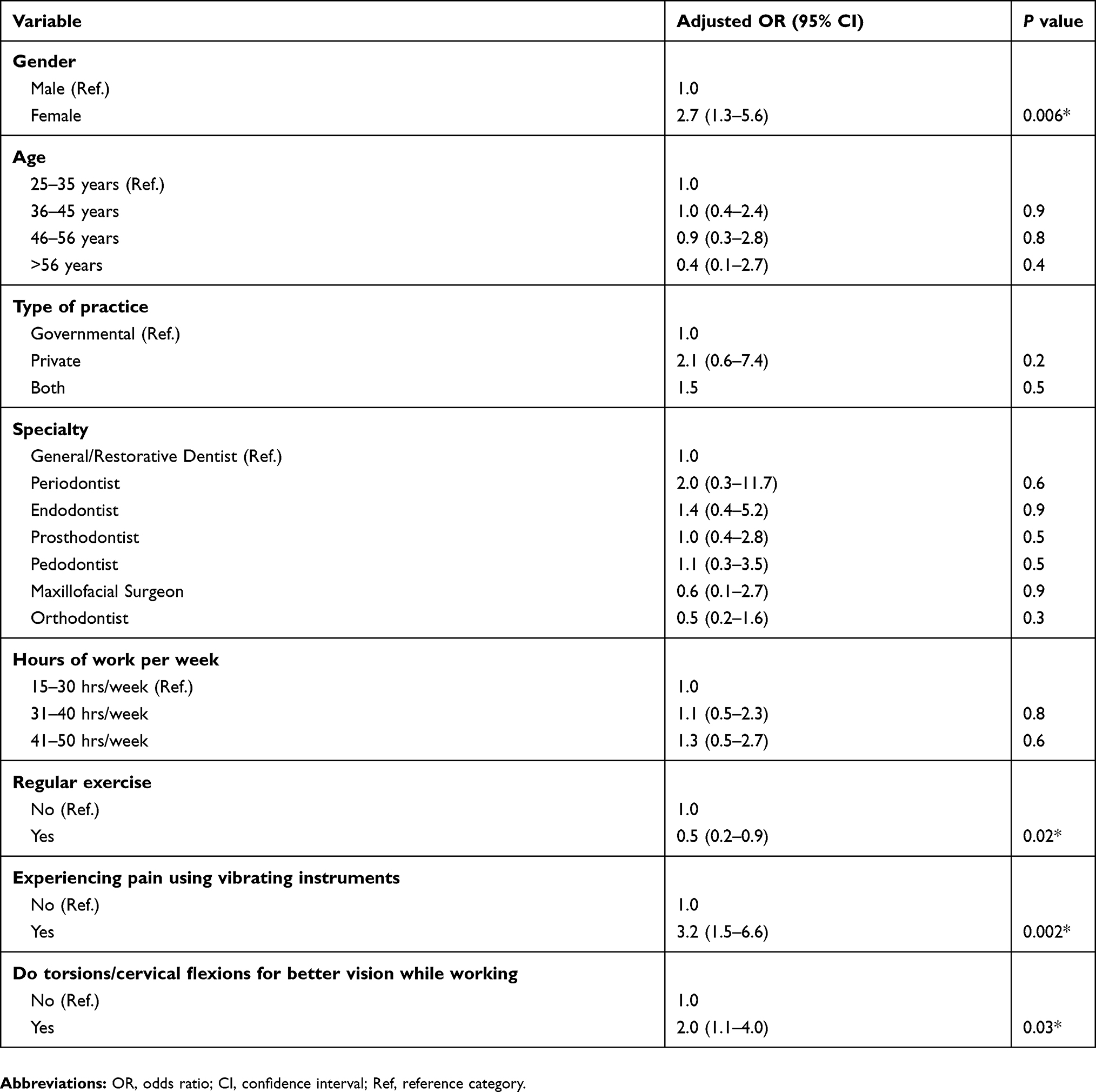 |
Table 2 Multiple logistic regression analysis predicting work-related musculoskeletal disorders. |
Respondents who reported experiencing WMSD were significantly more likely to be a female dentist, more likely to experience pain using vibrating instruments, and more likely to do torsions/cervical flexions for better vision while working. Moreover, as expected, dentists exercising on a regular basis were significantly less likely to report having WMSD. In comparison to general/restorative dentists, periodontists were more likely to report WMSD, followed by endodontists. In contrast, maxillofacial surgeons and orthodontists had lower odds of developing WMSD compared to general dentists. However, none of the differences in dental specialties reached statistical significance in the adjusted model of WMSD.
A multiple logistic regression model predicting having CTS versus not having CTS is presented in Table 3. This logistic regression model was statistically significant, P<0.003. The model explained 31.7% (Nagelkerke R2) of the variance in WMSD and correctly classified 91.8% of cases. Dentists over the age of 35 are five times more likely to report CTS, and dentists in private practices were also five times more likely to develop CTS compared to dentists in the governmental sector. However, gender, hours of work per week, and dental specialty did not appear to be significantly associated with CTS in this sample.
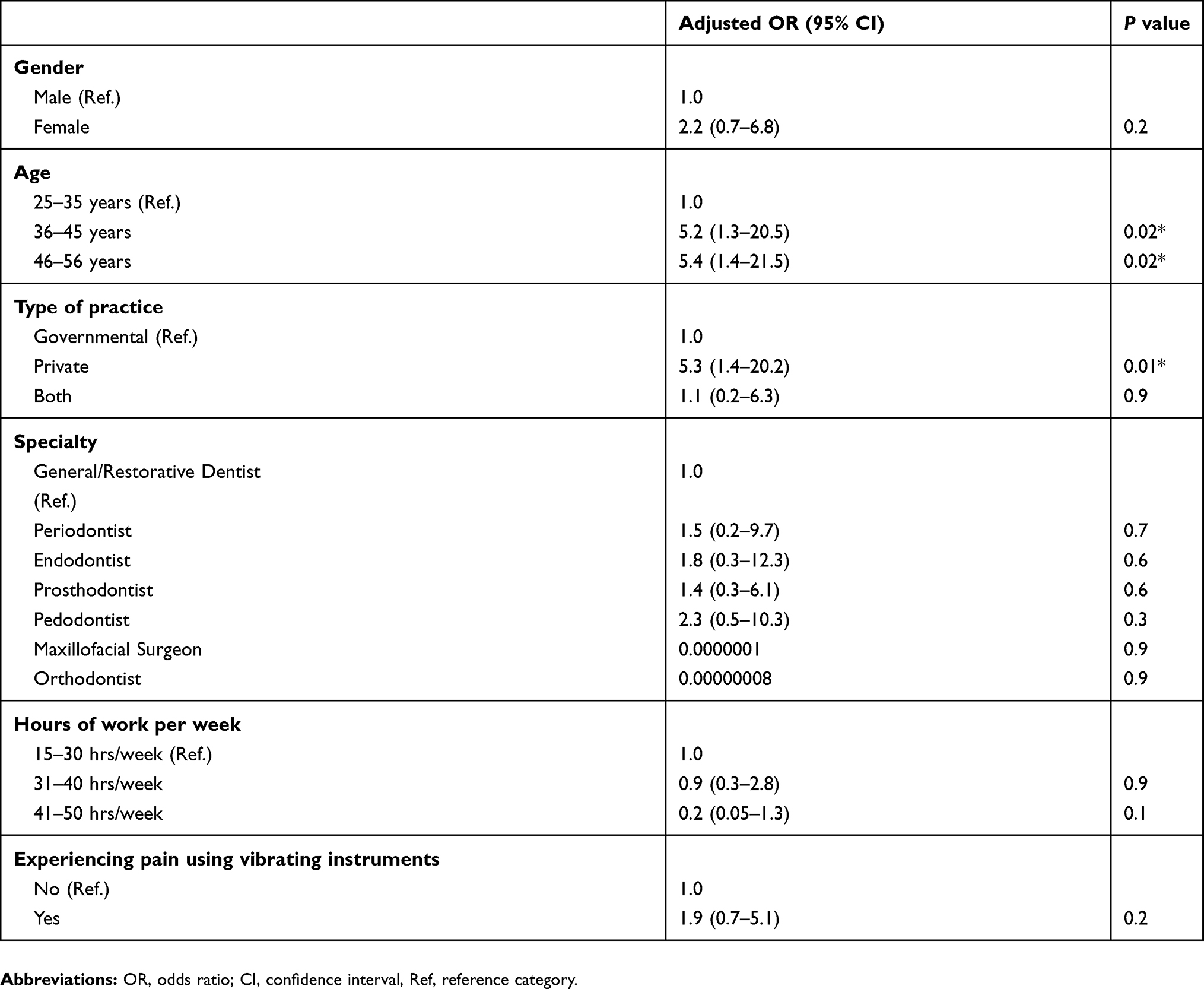 |
Table 3 Multiple logistic regression analysis predicting Carpal tunnel syndrome. |
Table 4 shows ergonomic practice among dentists in Jeddah. Three out of four respondents reported being familiar with good ergonomic practice in the clinic. However, this familiarity did not translate into using ergonomic practice, as less than one-third did stretching exercises after clinical practice, and only one in four wore dental loupes. Dentists doing any sports or exercises had 50% less the odds of reporting MSD. Moreover, being regular in exercising decreased the odds of MSD ever further by 10%. Dentists who do torsions and cervical flexions for better vision while working had double the odds of reporting MSD compared to dentists who don’t. Ergonomic practices that decrease the odds of MSD are wearing dental loupes, positioning the chair to maintain an ergonomic posture, having sufficient light at the workplace, having the instruments within hand’s reach, and performing stretching exercises after clinical practice. In terms of interventions sought, dentists with WMSD were more likely to take medications (OR: 2.6, CI: 1.2–5.8) and to attend physical therapy or massage sessions to relieve muscular pain and discomfort (OR: 2.0, CI: 1.1–3.8). In order to relieve muscular pain and discomfort, dentists with a history of CTS were more likely to take medications (OR: 2.5, CI: 1.1–6.2), and to attend physical or massage therapy sessions (OR: 2.7, CI: 1.1–6.6). Surgical treatment was only attempted by dentists suffering from CTS (OR: 6.9, CI: 1.1–44.2).
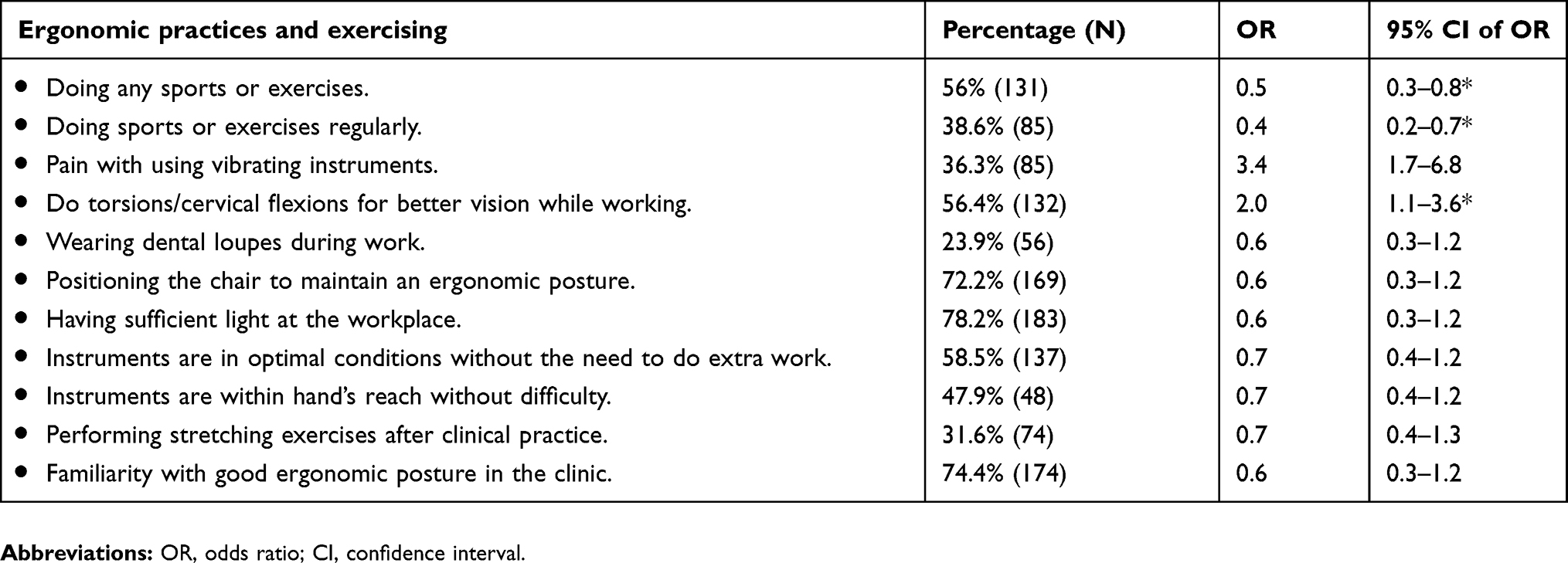 |
Table 4 Ergonomic practices and exercising among dentists in Jeddah |
Dentists suffering from WMSD (OR: 4.4, CI: 1.8–10.9) or CTS (OR: 6.0, CI: 2.4–15.1) also correlated to negative impacts on their career life, as they were more likely to miss work due to musculoskeletal pain.
Discussion
In this study, a self-administered survey was distributed to dentists practicing in Jeddah governmental and private dental sectors to investigate the prevalence of WMSD and CTS. The proportion of respondents practicing in the governmental sector was 74%, and this was comparable to the percentage of dentists practicing in the governmental sector in the Makkah region (73%), according to the Saudi Commission for Health Specialists (SCFHS) data.22 Our study results indicate that 70% of dentists in Jeddah report WMSD, with most of the pain located in the low back, neck, and shoulders. This was comparable to the reported range of MSD prevalence in Hayes et al’s systematic review (64–93%), who also found the most prevalent regions for pain in dentists to be the back and neck regions.4 This prevalence is also comparable to studies conducted in the United Arab Emirates (68%),29 Hail (78%),21 and Riyadh (78.5%).20 On the other hand, Al-Mohrej et al reported a higher WMSD (90.2%) among dentists in Riyadh.19 MSD is considered a major occupation related problem affecting dentists’ future careers and lives.
Female dentists experienced more WMSD in comparison to male dentists. This is in agreement with the literature.19,20,29,30 Some studies attributed this gender difference to low muscle tone and strength, hormonal changes, and a higher incidence of osteoporosis among females.13,31 However, gender difference, according to the location of the musculoskeletal pain, was not found with regard to middle and low back. In our study, periodontists followed by prosthodontists were more likely to report musculoskeletal pain due to the dental practice. The group least likely to report WMSD were orthodontists (53%) and maxillofacial surgeons (50%). Likewise, Kazancıoglu et al reported that oral and maxillofacial surgeons do not have a higher risk of MSD compared to general dentists and other dental specialties.16 Alghadir et al’s study found an increased risk of MSD with pediatric dentists. However, their sample neither included oral and maxillofacial surgeons nor general/restorative dentists.30 Similar to the findings of other studies,19 those who exercise were less likely to report WMSD. Since periodontists were the specialty with the most reported MSD, using lightweight instruments with larger diameters for scaling and root planning is an evidence-based recommendation suggested by Rempel et al in a randomized controlled trial.32
In our study, CTS was reported in only in 9.4% of dentists in Jeddah, and no previous published studies investigating CTS among dentists in Saudi Arabia were identified. Our reported CTS prevalence is in agreement with the Khan et al study, who reported that 10% of dentists had clinical symptoms of CTS.8 Another study found a higher prevalence of CTS (16.7%) among Isfahanian dentists.6 In our study, dentists working in private practice had increased risk of CTS. This finding is similar to the results of a study conducted in Riyadh City that demonstrated an increased risk of musculoskeletal symptoms among private sector dentists.20 In Shaffer et al’s study, 57.1% of United States army dental personnel who had electrodiagnostic evidence of median and ulnar neuropathies also had negative physical examination findings. Moreover, no correlation was observed between nerve conduction studies and history/physical examination.33 This implies that self- reported CTS might be an underestimate of its actual occurrence.
The results of this study suggest that many dentists don’t practice good dental ergonomics. Ohlendrof et al’s kinematic analysis of dentists’ postures documented unfavourable occupational postures during dental treatment.34 Therefore, the role of ergonomics needs to be emphasized, especially among dental students, to avoid the development of later problems and to make it a lifelong habit.
Furthermore, training workshops on ergonomic practice targeting dentists will help raise awareness regarding ergonomic practices and hopefully lessen the negative consequences on dentists’ musculoskeletal health. Other evidence-based health promotion activities include promoting exercise for low back pain.35 A major strength of this study is having a representative sample of practicing dentists evident by comparing the study sample demographics to SCFHS data. Response rate is another strength, since the response rate in our study was above 60%; the recommended threshold for response rate in medical research.36 This reduces the threat of nonresponse bias and supports the validity of the study. A limitation of this study is reliance on self-reported responses, a possible threat of recall bias. The findings of this study could be generalized to comparable populations.
Conclusion
In conclusion, work-related musculoskeletal disorders are common problems among Jeddah dentists. A higher prevalence of WMSD was found among female dentists, those who do not exercise regularly, those who use vibrating instruments, and those who do cervical flexions for better vision during clinical work. Ergonomic practices that could decrease the odds of developing MSD include wearing dental loupes, ergonomic positioning of the chair, having sufficient lightning, having instruments within reach, and performing stretching exercises after clinical practice. The risk of carpal tunnel syndrome increased with age and among private sector dentists. Pain due to MSD and CTS had a negative impact on dentists evident by increased missed days to work due to pain. Interesting trends in musculoskeletal pain and CTS among dentists practicing in Jeddah suggest developing training intervention programs on ergonomics. This could start by training dental students during their clinical practice and be followed up with continuing education workshops for practicing dentists. Further studies incorporating physical examinations and assessments rather than relying on self-reporting are recommended.
Acknowledgments
The authors thank Deema Meisha for her assistance with the graphics.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Division of Population Health. Work-Related Musculoskeletal Disorders & Ergonomics. National Center for Chronic Disease Prevention and Health Promotion, Center for Disease Control and Prevention, Georgia, USA; 2016. Available from: https://www.cdc.gov/workplacehealthpromotion/health-strategies/musculoskeletal-disorders/index.html.
2. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
3. Wang SY, Liu LC, Lu MC, Koo M. Comparisons of musculoskeletal disorders among ten different medical professions in Taiwan: a nationwide, population-based study. PLoS One. 2015;10:4.
4. Hayes M, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009;7(3):159–165. doi:10.1111/j.1601-5037.2009.00395.x
5. Abichandani S, Shaikh S, Nadiger R. Carpal tunnel syndrome - an occupational hazard facing dentistry. Int Dent J. 2013;63:230–236.
6. Haghighat A, Khosrawi S, Kelishadi A, Sajadieh S, Badrian H. Prevalence of clinical findings of carpal tunnel syndrome in Isfahanian dentists. Adv Biomed Res. 2012;1:13.
7. Harutunian K, Gargallo-Albiol J, Figueiredo R, Gay-Escoda C. Ergonomics and musculoskeletal pain among postgraduate students and faculty members of the School of Dentistry of the University of Barcelona (Spain). A cross-sectional study. Med Oral Patol Oral Cir Bucal. 2011;16(3):425–429. doi:10.4317/medoral.16.e425
8. Khan AA, Siddiqui AZ, Ahmed MR, Askari H, Zahid A. Prevalence of carpel tunnel syndrome in the dentists working in Karachi. Pakistan Oral Dent J. 2014;34(4): 588–591.
9. Prasad DA, Appachu D, Kamath V, Prasad DK. Prevalence of low back pain and carpal tunnel syndrome among dental practitioners in Dakshina Kannada and Coorg District. Indian J Dent Res. 2017;28(2):126–132. doi:10.4103/ijdr.IJDR_672_16
10. Sakzewski L, Naser-ud-Din S. Work-related musculoskeletal disorders in Australian dentists and orthodontists: risk assessment and prevention. Work. 2015;52(3):559–579. doi:10.3233/WOR-152122
11. Ísper Garbin A, Barreto Soares G, Moreira Arcieri R, Adas Saliba Garbin C, Siqueira C. Musculoskeletal disorders and perception of working conditions: a survey of Brazilian dentists in São Paulo. Int J Occup Med Environ Health. 2017;30(3):367–377.
12. Feng B, Liang Q, Wang Y, Andersen LL, Szeto G. Prevalence of work-related musculoskeletal symptoms of the neck and upper extremity among dentists in China. BMJ Open. 2014;4(12):e006451. doi:10.1136/bmjopen-2014-006451
13. Hodacova L, Sustova Z, Cermakova E, Kapitan M, Smejkalova J. Self-reported risk factors related to the most frequent musculoskeletal complaints among Czech dentists. Ind Health. 2015;53(1):48–55. doi:10.2486/indhealth.2013-0141
14. Borhan Haghighi A, Khosropanah H, Vahidnia F, Esmailzadeh S, Emami Z. Association of dental practice as a risk factor in the development of carpal tunnel syndrome. J Dent (Shiraz, Iran). 2013;14(1):37–40.
15. Lin TH, Liu YC, Hsieh TY, Hsiao FY, Lai YC, Chang CS. Prevalence of and risk factors for musculoskeletal complaints among Taiwanese dentists. J Dent Sci. 2012;7(1):65–71. doi:10.1016/j.jds.2012.01.009
16. Kazancioglu HO, Bereket MC, Ezirganli S, Ozsevik S, Sener I. Musculoskeletal complaints among oral and maxillofacial surgeons and dentists: a questionnaire study. Acta Odontol Scand. 2013;71(3/4):469–474. doi:10.3109/00016357.2012.696688
17. Kanaparthy A, Kanaparthy R, Boreak N. Postural awareness among dental students in Jizan, Saudi Arabia. J Int Soc Prev Community Dent. 2015;5(Suppl 2):S107–S111. doi:10.4103/2231-0762.172950
18. Rayyan MR, Hetou SC, Al Salem RF, et al. Work-related musculoskeletal disorders among dental students of different academic levels. J Int Oral Health. 2016;8(4):471–475.
19. Al-Mohrej OA, AlShaalan NS, Al-Bani WM, Masuadi EM, Almodaimegh HS. Prevalence of musculoskeletal pain of the neck, upper extremities and lower back among dental practitioners working in Riyadh, Saudi Arabia: a cross-sectional study. BMJ Open. 2016;6(6):e011100. doi:10.1136/bmjopen-2016-011100
20. Al-Shehri Z, Al Zoughool M. Prevalence and risk factors of musculoskeletal symptoms among dental students and dental practitioners in Riyadh City, Saudi Arabia. Arch Environ Occup Health. 2017;73(1):56–63.
21. Aljanakh M, Shaikh S, Siddiqui AA, Al-Mansour M, Hassan SS. Prevalence of musculoskeletal disorders among dentists in the Hail Region of Saudi Arabia. Ann Saudi Med. 2015;35(6):456–461. doi:10.5144/0256-4947.2015.456
22. AlBaker AA, Al-Ruthia YS, AlShehri MB, Alshuwairikh S. The characteristics and distribution of dentist workforce in Saudi Arabia: a descriptive cross-sectional study. Saudi Pharm J. 2017;25(8):1208–1216. doi:10.1016/j.jsps.2016.09.002
23. Ministry of Health. 1436 Statistical Yearbook. Ministry of Health, Riyadh, Kingdom of Saudi Arabia; 2015.
24. Wiebe ER, Kaczorowski J, MacKay J. Why are response rates in clinician surveys declining? Can Fam Physician. 2012;58(4):e225–8.
25. Diaz-Caballero AJ, Gómez-Palencia IP, Díaz-Cárdenas S. Ergonomic factors that cause the presence of pain muscle in students of dentistry. Med Oral Patol Oral Cir Bucal. 2010;15(6):906–911.
26. Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen FA, Jørgensen K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–237. doi:10.1016/0003-6870(87)90010-X
27. McCaffery M, Pasero C. Pain: Clinical Manual.
28. IBM Corp. IBM® SPSS® Statistics 24. Armonk (NY): IBM Corp; 2016.
29. Al-Ali K, Hashim R. Occupational health problems of dentists in the United Arab Emirates. Int Dent J. 2012;62(1):52–56. doi:10.1111/j.1875-595X.2011.00091.x
30. Alghadir A, Zafar H, Iqbal ZA. Work-related musculoskeletal disorders among dental professionals in Saudi Arabia. J Phys Ther Sci. 2015;27(4):1107–1112.
31. Bedi HS, Moon NJ, Bhatia V, Sidhu GK, Khan N. Evaluation of musculoskeletal disorders in dentists and application of DMAIC technique to improve the ergonomics at dental clinics and meta-analysis of literature. J Clin Diagnostic Res. 2015;9(6):ZC01–3.
32. Rempel D, Lee DL, Dawson K, Loomer P. The effects of periodontal curette handle weight and diameter on arm pain: a four-month randomized controlled trial. J Am Dent Assoc. 2012;143(10):1105–1113.
33. Shaffer SW, Alexander K, Huffman D, et al. Median and ulnar neuropathies in US Army dental personnel at Fort Sam Houston, Texas. US Army Med Dep J. 2014;34: 65–73.
34. Ohlendorf D, Erbe C, Hauck I, et al. Kinematic analysis of work-related musculoskeletal loading of trunk among dentists in Germany. BMC Musculoskelet Disord. 2016;17(1):427. doi:10.1186/s12891-016-1134-4
35. Choi BK, Verbeek JH, Tam WW-S, Jiang JY. Exercises for prevention of recurrences of low-back pain. In: Choi BK, editor. Cochrane Database of Systematic Reviews. Chichester (UK): John Wiley & Sons, Ltd; 2010:CD006555.
36. Burns K, Duffett M, Kho M, et al. A guide for the design and conduct of self-administered surveys of clinicians. CMAJ. 2008;179(3):245–252. doi:10.1503/cmaj.080372
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.