Back to Journals » Infection and Drug Resistance » Volume 12
Prevalence of Staphylococcus aureus carriage and pattern of antibiotic resistance, including methicillin resistance, among contact sport athletes in Italy
Authors Mascaro V, Capano MS, Iona T, Nobile CGA, Ammendolia A, Pavia M ![]()
Received 27 November 2018
Accepted for publication 19 February 2019
Published 7 May 2019 Volume 2019:12 Pages 1161—1170
DOI https://doi.org/10.2147/IDR.S195749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Valentina Mascaro,1 Maria Simona Capano,1 Teresa Iona,2 Carmelo Giuseppe Angelo Nobile,3 Antonio Ammendolia,2 Maria Pavia1
1Department of Health Sciences, University of Catanzaro “Magna Græcia”, Catanzaro, Italy; 2Department of Medical and Surgical Sciences, University of Catanzaro “Magna Græcia”, Catanzaro, Italy; 3Department of Pharmacy, Health and Nutritional Sciences, University of Calabria, Cosenza, Italy
Background and purpose: Athletes participating in contact or collision sports have a great chance of acquiring Staphylococcus aureus infections. The risk factors for colonization and infections include frequent antibiotic use, close contact situations, skin trauma, sharing of sports equipment, and poor hygiene. Therefore, our specific goals were to determine (1) prevalence of S. aureus among different types of contact sport athletes which were barely studied in the European region, (2) antimicrobial resistance of S. aureus isolates, and (3) association of carriage with particular risk factors of spor t practices.
Patients and methods: A cross-sectional study was conducted among contact or collision sport athletes in Italy. A questionnaire was used to gather information about sociodemographic characteristics, specific sport activities, and participants’ health conditions. Swabs were collected from the nares, oropharynx, and fingers and tested for S. aureus isolation and antimicrobial susceptibility.
Results: S. aureus was carried by 42% of 238 enrolled athletes. Colonization was associated with number of weekly training days, sharing of sports equipment, not taking a shower immediately after training, and a previous history of pharyngitis or sinusitis and skin manifestations. Isolates were resistant to clindamycin (24.8%) and erythromycin (15.8%). Of all athletes, 1.3% carried methicillin-resistant S. aureus (MRSA); MRSA were 3% of all S. aureus isolates. No strains were resistant to sulfamethoxazole/trimethoprim.
Conclusion: Our results have shown a high prevalence of S. aureus carriage and a relevant resistance to antimicrobials used for the treatment of S. aureus infections. Prevention efforts aimed at reducing S. aureus colonization, and thus potentially reducing infections, should be improved.
Keywords: S. aureus, MRSA, colonization, athletes, antibiotic resistance, antibiotic susceptible
Introduction
Staphylococcus aureus is an opportunistic human pathogen that causes skin and soft tissue infections (SSTIs), as well as more serious conditions, such as pneumonia or bloodstream infections in both genders and all age groups.
S. aureus has developed resistance to several antibiotics and methicillin-resistant S. aureus (MRSA) infections have become increasingly common not only in hospitalized patients, but also in the community.1 The incidence of community-associated MRSA (CA-MRSA) infections is higher among specific groups, such as athletes, especially those who participate in contact or collision sports,2 even 3-times higher compared to general population.3,4
The association between MRSA colonization and infection is well established.5 Moreover, the risk for MRSA SSTI among MRSA colonized athletes in the 3 months after colonization screening was found to be 7 times greater compared with noncolonized athletes.6
Once contracted by an athlete, MRSA is a threat to the entire team; therefore, it is very important to implement prevention of the spread of the pathogen, including good personal hygiene, cleaning, and dressing of the wounds and avoiding the sharing of objects that come into contact with the skin.7
Although MRSA has attracted major attention, colonization by CA methicillin-sensitive S. aureus (CA-MSSA) resistant to other antimicrobials is also of concern, since increasing antimicrobial resistance has been reported in the community in European countries.8 Moreover, colonization by MSSA has been reported in healthy collegiate athletes,9 and associated to outbreaks in the general population10 and also in athletes11 often sustained by Panton–Valentine leukocidin (PVL) producing strains.
Several studies have been performed in the USA to define S. aureus carriage among athletes,12–17 while only a few studies have been conducted in Europe,18–20 and no studies have been conducted in Italy.
Therefore, our specific goals were to determine (1) prevalence of S. aureus among different types of contact sport athletes which were barely studied in the European region, (2) antimicrobial resistance of S. aureus isolates, (3) association of carriage with particular risk factors of sport practices.
Material and methods
We conducted a cross-sectional study between May 2017 and March 2018 in a region of southern Italy (Calabria). Participants eligible in the study were subjects ≥16 years of age that practiced a contact/collision sport as defined by the American Academy of Pediatrics.21 In particular, “collision” sports are those in which athletes purposely hit or collide with each other or inanimate objects, including the ground, with great force (eg, martial arts, boxing, and wrestling).
Recruitment was performed at the site of practice, mainly public or private gyms. The eligible subjects were all well informed about the purpose and contents of the study and asked to sign a consent form to document their voluntary participation. In the case of minors, a person with parental responsibility had to give informed consent on behalf of the minor.
After informed consent was signed, a questionnaire, assuring confidentiality of responses, was provided and swab samples were collected from the anterior nares, oropharynx, and fingers of participating athletes during the training session.
There were no incentives offered for participation.
The questionnaire was developed by two researchers and based upon extensive review of the relevant literature.13,22 It included several sections, and responses were designed in a variety of formats: closed-ended questions with multiple answers, yes or no questions and open option questions.
The first section examined the socio-demographic characteristics (sex, age, marital status, work activity) of participating athletes. In the second section, the specific sport activities were analyzed [type of practiced activity, number of practicing years and of weekly training days, use and sharing of personal items (eg, towels, soap, clothes, sports equipment), hand washing, and frequency of showers]. The third part investigated the participants’ health conditions, recent hospitalization or surgery, antibiotic use, previous MRSA exposure and/or infection. The last section was related to availability of prevention programs for infections in the gyms.
Before collecting data, a pilot test was conducted on a small sample of athletes to test the comprehensibility of the items in the questionnaire. Answering the questionnaire lasted an average of 10 mins.
Sterile swabs were used to collect samples from the anterior nares, oropharynx, and fingers. Each sample was placed in Amies transport medium, transported to laboratory in refrigerated containers and processed within 24 hrs of collection. The swabs were inoculated on Mannitol Salt Agar (MSA) plates and incubated at 37°C for 24–48 hrs. All typical S. aureus colonies were then subcultured onto Nutrient Agar (NA) plates and incubated at 37°C for 24 hrs. Afterward, Gram stain, catalase, and coagulase tests were performed. All suspect strains were identified to the species level using the API Staph identification system (bioMérieux). All S. aureus isolates were tested for their antibiotic susceptibility by Kirby–Bauer disk diffusion method; the antibiotics for which sensitivity was tested were: ciprofloxacin (5 µg), clindamycin (2 µg), erythromycin (15 µg), gentamycin (10 µg), linezolid (10 µg), mupirocin (200 µg), sulfamethoxazole/trimethoprim (25 µg), rifampicin (5 µg), tetracycline (30 µg), cefoxitin (30 µg), and oxacillin (1 µg). Oxacillin resistance was investigated also through the microdilution method. Interpretation of results of the antibiotic susceptibility testing was performed according to the EUCAST guidelines and clinical breakpoints (version 8.1);23 in particular MIC breakpoint for oxacillin was 2 mg/L, whereas cefoxitin breakpoint was 22 mm. S. aureus strains that showed oxacillin and/or cefoxitin resistance were confirmed by a multiplex PCR amplifying the genes mecA, spa gene, and PVL gene (DTU FOOD, National Food Institute protocol-September 2012). The polymorphic region of spa gene was double-strand sequenced by AB prism 3500 sequencer (Applied Biosystem). The sequences (forward and reverse) were edited by Chromas and Mega v.6.0. The newly sequences were analyzed by spatyper (
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethical Committee (“Mater Domini” Hospital of Catanzaro, Italy) (2017/04/27).
Statistical analysis
Data were summarized using frequencies and percentages for categorical data and mean and standard deviations for continuous data. In the primary analysis, Student's t-test for independent samples (for continuous variables) and Pearson’s chi-square or Fishers exact test (for categorical variables) were used to examine the association between S. aureus carriage and several explanatory variables. Subsequently, a stepwise multivariate logistic regression model was performed to determine the association of several characteristics with S. aureus carriage among athletes (0=non-carrier, 1=carrier). The model was developed according to the Hosmer and Lemeshow strategy, choosing a less than 0.25 p-value at univariate analysis for inclusion of variables in the multivariate model.24 The significance level for variable entering the logistic regression models was set at 0.2 and for removal from the model at 0.4. Adjusted odds ratio and 95% confidence intervals were calculated.
The explanatory variables included in the model were the following: age (ordinal, in years intervals: 0=16–18 years, 1=19–28 years, 2=29–50 years), weekly training days (ordinal, 0=1–2 days/week, 1=3–4 days/week, 2=5–7 days/week), number of years in practice (ordinal, 0=1–3 years, 1=4–7 years, 2=8–10 years), sharing cream/lotions (0=no, 1=yes), sharing soap (0=no, 1=yes), sharing sports equipment (0=no, 1=yes), shower after training (0=no, 1=yes), pharyngitis/sinusitis within the previous 6 months (no=0, yes=1), skin manifestations within the previous 6 months (0=no, 1=yes), presence of educational programs regarding the prevention of infectious diseases in the gym (0=no, 1=yes).
Data were stored and analyzed using Stata Statistical Software, Version 14.1.
Results
A total of 238 athletes were invited to take part in the study, all of them accepted to participate and were enrolled in the survey. Athletes playing 9 different contact sports were included in the study [taekwondo, judo, karate, wushu/kung fu, boxing, kick-boxing, mixed martial arts (MMA), Muaythai, and football]. A total of 19 gyms located in Calabria region were involved.
Characteristics of the athletes participating in the study, as well as of S. aureus carriage are reported in Table 1. Age of the participants ranged from 16 to 50 years (mean 23.4 years, median 19 years, SD±8.7, interquartile range: 17–28 years). The male to female ratio was 3:1. Taekwondo was the most practiced sport (26.1%) followed by wushu/kung fu (17.7%) and boxing (15.6%). The average number of years of practice was 2.6 (±1.7) and of weekly training days was 2.2 (±0.8). Sharing of objects was not very common in the sample except for sports equipment (helmet, shin guards, headgear, ankle braces, etc.) that was reported to be shared by 47.1% of the subjects.
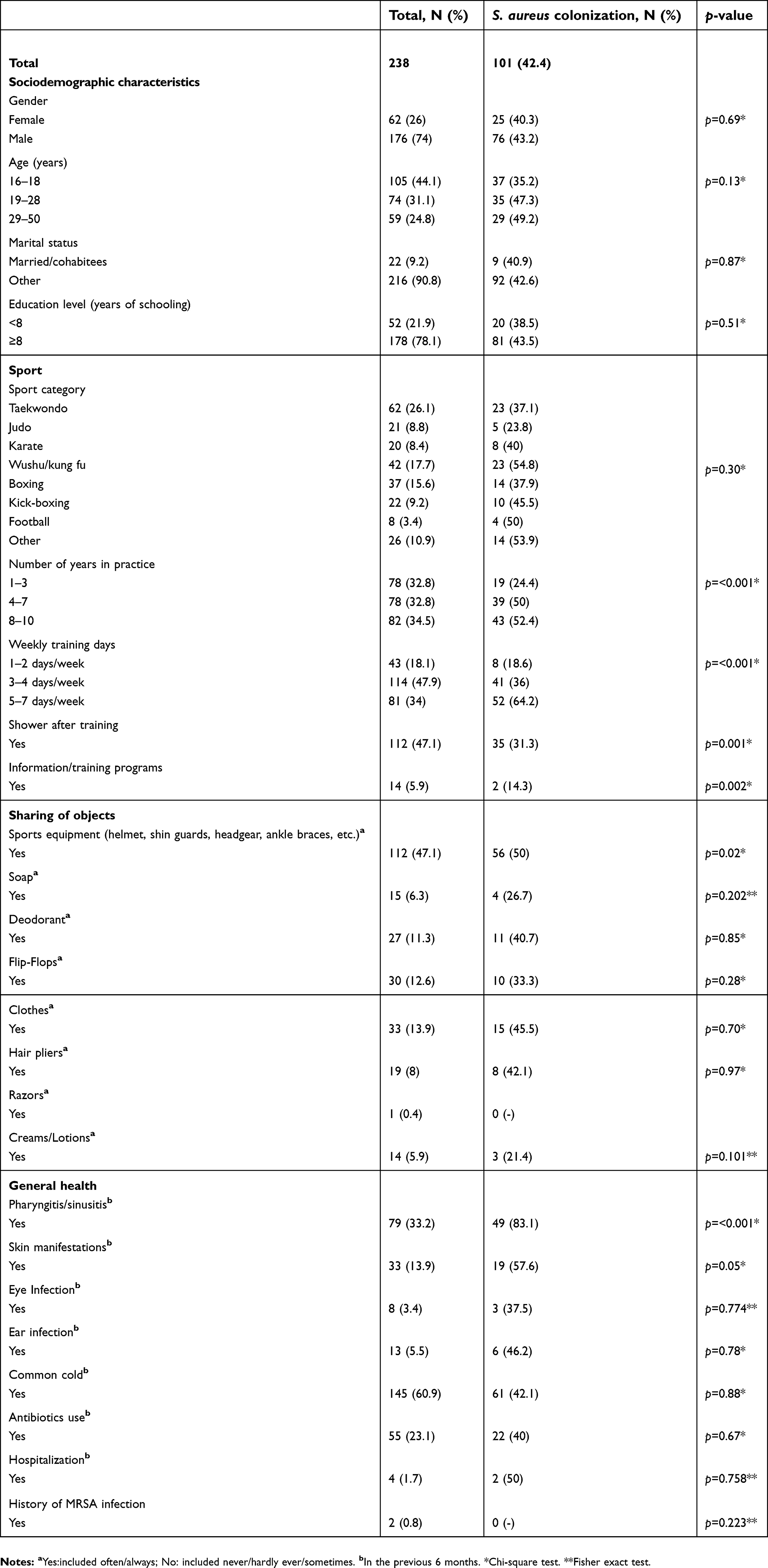 | Table 1 Characteristics of athletes included in the study |
S. aureus was carried by 101 athletes (42.4%), ranging from 23.8% for the judo players to 54.8% for the wushu/kung fu athletes. The most common site of isolation among of the 101 S. aureus carriers was the oropharynx (n=68, 67.3%) followed by the anterior nares (n=46, 45.5%) and the fingers (n=30, 29.7%); in 33 (32.7%) subjects S. aureus harbored more than one site, whereas in 43 (42.6%) only the oropharynx, in 20 (19.8%) only the anterior nares and in 5 (5%) only the fingers were colonized.
Univariate analysis showed that S. aureus colonization was associated, although not significantly, with athletes’ age, ranging from 35.2% in the 16–18 years old subjects to 49.2% in those 29–50 (χ2=4.03, p=0.13), with increasing number of years of practice (χ2=15.6, p=≤0.001), as well as with number of weekly training days (χ2=27.6, p=<0.001). Also, the results showed that S. aureus colonization was more common among the athletes who share the sports equipment (χ2=4.95, p=0.02) and in those who do not take showers immediately after training (χ2=10.8, p=≤0.001). Moreover, there was a statistically significant association with a previous history of pharyngitis or sinusitis (χ2=52.9, p=≤0.001), skin manifestations (χ2=3.59, p=0.05) and the lack of appropriate information or training programs regarding the prevention of infectious diseases (χ2=4.82, p=0.002) (Table 2).
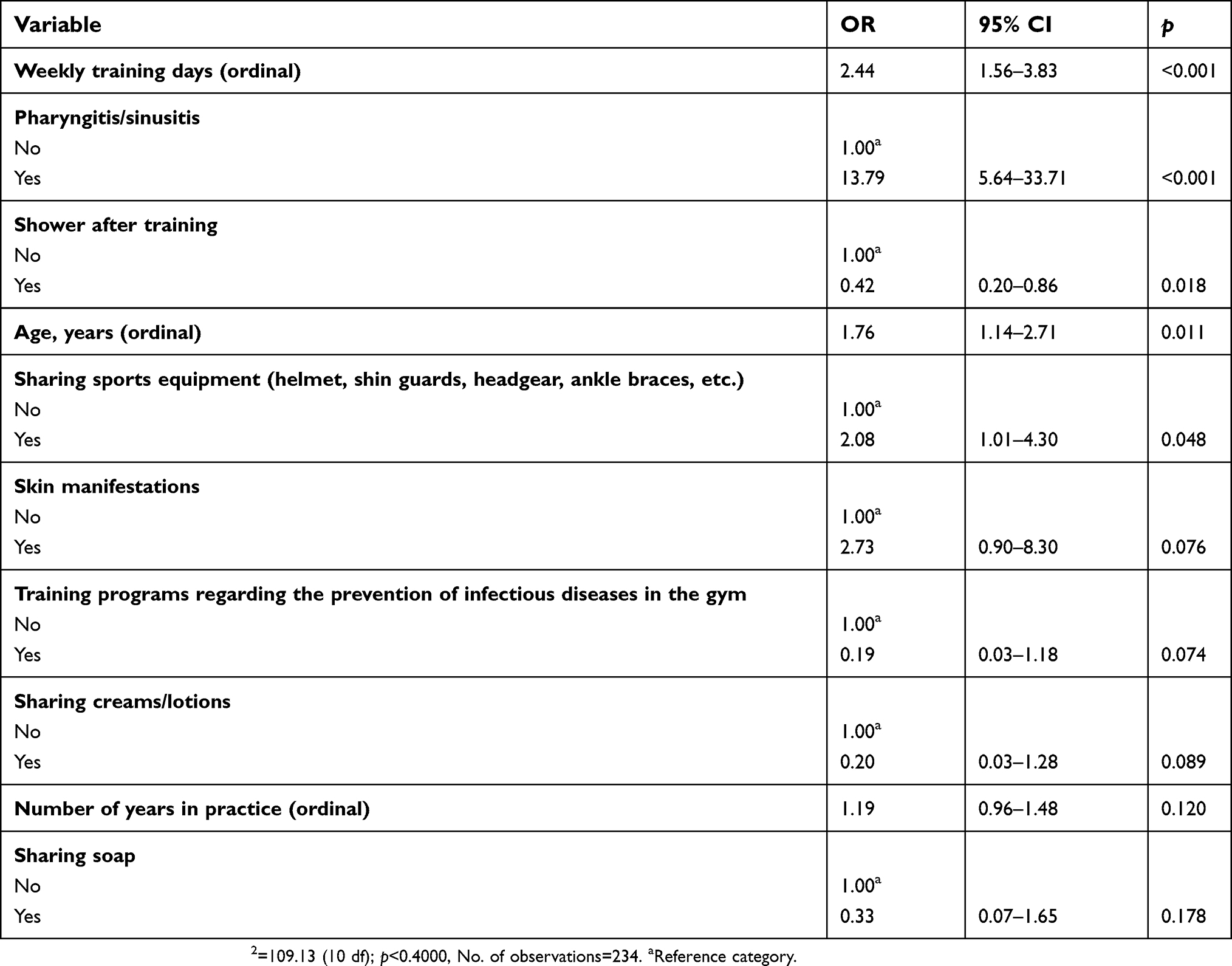 | Table 2 Multiple logistic regression results for estimates of associations of Staphylococcus aureus colonization with potential determinants |
Results of the multivariate analysis confirmed those of the univariate analysis except for number of year of practice and the lack of training and information programs at the gym (Table 2).
Antibiotic susceptibility of S. aureus isolates revealed varying degrees of susceptibility patterns against the antimicrobial agents: 66 (65.4%) S. aureus strains did not exhibit any resistance to the tested antibiotics, 13 (12.9%) were resistant to one antibiotic class, 12 (11.9%) to two antibiotic classes, while multidrug-resistant (MDR) strains were 10 (9.9%).
The most frequent resistance attained was to clindamycin (24.8%), followed by erythromycin (15.8%) whereas 3 (3%) strains were MRSA, for an overall prevalence in the sample of 1.3%. In our sample of 238 athletes, the resistance to clindamycin and erythromycin was 10.5% and 6.7%, respectively, whereas the resistance was low for the other tested antibiotics. All strains were susceptible to sulfamethoxazole/trimethoprim.
Of the 101 individuals harboring S. aureus, 22 (40%) had taken antibiotics in the previous 6 months and amoxicillin was the most frequently used antibiotic, followed by macrolides and fluoroquinolones.
Three S. aureus strains were resistant to both oxacillin and cefoxitin, and one to oxacillin only. Molecular characterization showed that only the 3 strains resistant to both antibiotics were mecA positive, these strains were all PVL negative and their spa type was t022. This spa type has been associated to UK EMRSA-15 clone and to the SCCmec type IV, that is likely to be a CA-MRSA strain.25 The antimicrobial resistance profiles were quite different among these 3 MRSA strains. In particular, two MRSA strains showed resistance also to ciprofloxacin, and one also to clindamycin, erythromycin, and mupirocin. No association was observed between MRSA colonization and previous antibiotic use.
Discussion
To the best of our knowledge, this is the first study investigating overall S. aureus and MRSA colonization in Italian contact sports athletes. Moreover, most studies have focused on single contact sports and predominantly on male athletes, while we evaluated S. aureus colonization in both male and female athletes practicing nine different contact sports.16,26,27
In our population of athletes, overall S. aureus carriage was 42.4%, that is higher than that observed in the general population, approximately estimated to be 20–30%.28,29 In a recent study conducted in nine European countries in the adult population, an overall carriage of 21.6%, ranging from 12.1% in Hungary to 29.4% in Sweden was found.30 Analogously, in a survey conducted in central Italy in the adult population, S. aureus carriage was 25.9%,31 whereas it was 28.3% in the population of Italian biomedical students.32 However, most studies investigating S. aureus carriage in the general population have performed nasal swabs only, whereas in our study oropharynx and fingers were also swabbed. Indeed, we observed a higher S. aureus carriage in the oropharynx (42.6%) than in the anterior nares (19.8%), as recently reported in several populations worldwide,33 as well as in Italy in healthy children.34 Although nasal carriage is a well-documented risk factor for S. aureus infections, recent studies have identified the oropharynx as a potential site of S. aureus colonization, occurring even in the absence of nasal colonization,35,36 and its assessment could sustain a higher detection of S. aureus colonization in healthy individuals.
Our findings showed an MRSA carriage of 1.3% in the total population and of 3% among the colonized athletes. This figure is higher than that reported in the European community population, ranging from 0% in Sweden to 0.4% in several countries, such as Belgium, UK, and France, and from 0 in Sweden to 2.1% in Belgium in the colonized European community population.30 In Italy, a substantially lower colonization by MRSA was found in the community, 0.1% in the total population and 0.4% in the population of S. aureus carriers,31 in children in the community (0.6%),34 whereas no MRSA carriers were found among Italian biomedical students.32
Results from studies on MRSA colonization in athletes performed in different countries display substantial variation in prevalence of carriage, and it turns out to be difficult to compare results reported by different authors because of differences in sampled population, practiced sports, sites of swabs collection, and MRSA circulation in the community. Indeed, in a recently published systematic review and meta-analysis involving 15 studies in asymptomatic athletes, the pooled prevalence of MRSA colonization was 6%, but an extreme variability of prevalence was found, and the higher frequencies were detected in studies conducted in the USA.6 In particular, collegiate athletes had the highest colonization (13%), whereas in professional athletes no MRSA were isolated. Moreover, in this meta-analysis, the three studies conducted in Europe reported a 6% prevalence of MRSA colonization in water sports athletes in Russia,20 whereas no MRSA colonization was revealed in rugby players in the UK37 and in soccer players in the Netherlands,19 although these two latter studies were carried out in response to an outbreak and involved a small number of athletes. Low MRSA prevalence (0.3%) has also been reported in French athletes involved in contact and non-contact sports.18 The 1.3% MRSA prevalence found in this study is within the range reported in the literature in Europe, but should be interpreted in the light of a widely spread methicillin-sensitive S. aureus (MSSA) colonization, since it has been reported that some MRSA strains have probably evolved from MSSA through horizontal transfer of mobile elements,38 with SCCmec IV and ACME being likely acquired from S. epidermidis.39
Pattern of antimicrobial resistance of isolates deserves an in depth evaluation: first of all, the high percentage of susceptible strains (64.4%) is related to our choice of excluding penicillin from the tested antibiotics, because of the very high reported resistance of S. aureus strains both in Europe (87.1%)30 and in Italy (80.4%)31 in healthy subjects. This choice, that was driven by the fact that penicillin is no more available in Italy as a therapeutic choice since it has been excluded from the drug market, has also probably led to an underestimation of the percentage of MDR strains (9.9%), since resistance to penicillin could not be included in the calculation of the number of classes involved in the antimicrobial resistance. The highest resistance in our findings was associated with clindamycin (24.5%). This figure is higher than that reported in healthy subjects in Italy (7.6%)31 and in Europe (14.6%),30 but is lower than that reported in a meta-analysis of studies conducted in healthy athletes (62.%),6 although in this latter study the antimicrobial susceptibility was evaluated in MRSA strains. Clindamycin is an alternative drug for the treatment of SSTI caused by both MSSA and MRSA, particularly in Europe.40 In addition, this antibiotic is an alternative drug to be used in penicillin-allergic patients.41 Therefore, our findings have revealed that, in the population of athletes, clindamycin represents a limited option for treatment and demand more careful evaluation on the choice of the antibiotic to be used as an empirical treatment.6,14 Resistance to erythromycin (15.8%) appears to be in line with that reported in healthy adults in Europe, and particularly in France (16.5%)30 and in Italy (12.8%)31 and lower than that found in MRSA strains isolated in athletes (40%).6 The resistance to macrolides is common among MRSA isolates, including community strains, creating the question of whether macrolides should still be prescribed empirically for S. aureus infections.30 Indeed, we found a discrepancy between resistance rates for macrolides and lincosamides, although resistance to these antibiotic classes in S. aureus is usually mediated by erm genes.42 However, there is a description in the literature of the detection of lnu genes, conferring lincosamide resistance exclusively, in MRSA and MSSA strains of human origin,43 that could explain the presence of a phenotypic resistance to clindamycin and susceptibility to erythromycin. No resistance was detected to sulfamethoxazole/trimethoprim, an old antibiotic used as a treatment option for S. aureus infections in health care setting and in the community,44 and this finding is in line with the statement of some Italian researchers who, considering the CA-MRSA epidemiology in Europe, strongly suggest sulfamethoxazole/trimethoprim and clindamycin as appropriate first-line therapeutic options for the treatment of SSTI due to CA-MRSA.45
Consistent with other reports, our results implicate the sharing of personal sports equipment, poor hygiene practices, as well as frequency of sports activity, as factors associated to S. aureus colonization.27,46,47 The Centers for Disease Control and Prevention (CDC) recommend measures to control MRSA among sports participants, including hand hygiene both before and after contact, wound care, regular cleaning of the personal athletic equipment, and avoid the sharing of towel and personal items.7,48 Effectiveness of these preventive measures has been indirectly confirmed by our results showing that athletes attending gyms where educational programs regarding the prevention of infectious diseases were organized were less likely to be colonized by S. aureus.
Interpretation of results should take into account some limitations of the study. Sites other than the nares, oropharynx, and fingers were not cultured; thus, underestimation of the true frequency of S. aureus carriage may have occurred, but this decision ensured high participation by athletes. Underestimation of MRSA prevalence might also be related to the use of non-selective medium instead of chromogenic agars where MRSA strains are easily discerned. Moreover, athletes were sampled only once, and no information other than cross-sectional carriage is available. Despite these limitations, the study has added data on S. aureus colonization in European athletes unlike most studies that have been conducted in the USA, addressing overall antimicrobial resistance, not only methicillin resistance, that does not seem to represent a high priority in European athletes.
Conclusion
In conclusion, the results described in this paper have shown, in the context of European contact sports athletes, an emerging scenario of a high prevalence of S. aureus carriage, as well as a relevant resistance to antimicrobials frequently used for the treatment MSSA and MRSA infections. Moreover, colonization has been shown to be related to several preventable practice characteristics. Prevention efforts aimed at reducing S. aureus colonization, and thus potentially reducing infections, should target contact sports athletes also in Europe.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. David MZ, Daum RS. Community-associated methicillin-resistant Staphylococcus aureus: epidemiology and clinical consequences of an emerging epidemic. Clin Microbiol Rev. 2010;23:616–687. doi:10.1128/CMR.00081-09
2. Rice SG. American academy of pediatrics council on sports medicine and fitness. Medical conditions affecting sports participation. Pediatrics. 2008;121:841–848. doi:10.1542/peds.2008-0080
3. Graham PL, Lin SX, Larson EL. A U.S. population-based survey of Staphylococcus aureus colonization. Ann Intern Med. 2006;144:318–325. doi:10.7326/0003-4819-144-5-200603070-00006
4. Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-resistant Staphylococcus aureus: a meta-analysis of prevalence and risk factors. Clin Infect Dis. 2003;36:131–139. doi:10.1086/cid.2003.36.issue-2
5. Davis KA, Stewart JJ, Crouch HK, et al. Methicillin-resistant Staphylococcus aureus (MRSA) nares colonization at hospital admission and its effect on subsequent MRSA infection. Clin Infect Dis. 2004;39:776–782. doi:10.1086/422997
6. Karanika S, Kinamon T, Grigoras C, Mylonakis E. Colonization with methicillin-resistant Staphylococcus aureus and risk for infection among asymptomatic athletes: a systematic review and meta-analysis. Clin Infect Dis. 2016;63:195–204. doi:10.1093/cid/ciw240
7.
8. van Bijnen EME, Paget J, de Lange-de Klerk ESM, et al. Antibiotic exposure and other risk factors for antimicrobial resistance in nasal commensal Staphylococcus aureus: an ecological study in 8 European countries. PLoS One. 2015;10:e0135094. doi:10.1371/journal.pone.0135094
9. Jimenez-Truque N, Saye EJ, Soper N, et al. Longitudinal assessment of colonization with Staphylococcus aureus in healthy collegiate athletes. J Pediatric Infect Dis Soc. 2016;5:105–113. doi:10.1093/jpids/piu108
10. Tinelli M, Monaco M, Vimercati M, Ceraminiello A, Pantosti A. Methicillin-susceptible Staphylococcus aureus in skin and soft tissue infections, Northern Italy. Emerg Infect Dis. 2009;15:250–257. doi:10.3201/eid1502.080010
11. Couvé-Deacon E, Tristan A, Pestourie N, et al. Outbreak of panton-valentine leukocidin-associated methicillin-susceptible Staphylococcus aureus infection in a rugby team, France, 2010–2011. Emerg Infect Dis. 2016;22:96–99. doi:10.3201/eid2201.150597
12. Champion AE, Goodwin TA, Brolinson PG, Werre SR, Prater MR, Inzana TJ. Prevalence and characterization of methicillin-resistant Staphylococcus aureus isolates from healthy university student athletes. Ann Clin Microbiol Antimicrob. 2014;13:33. doi:10.1186/s12941-014-0033-5
13. Creech CB, Saye E, McKenna BD, et al. One-year surveillance of methicillin-resistant Staphylococcus aureus nasal colonization and skin and soft tissue infections in collegiate athletes. Arch Pediatr Adolesc Med. 2010;164:615–620. doi:10.1001/archpediatrics.2010.93
14. Oller AR, Province L, Curless B. Staphylococcus aureus recovery from environmental and human locations in 2 collegiate athletic teams. J Athl Train. 2010;45:222–229. doi:10.4085/1062-6050-45.3.222
15. Jiménez-Truque N, Saye EJ, Soper N, et al. Association between contact sports and colonization with Staphylococcus aureus in a prospective cohort of collegiate athletes. Sports Med. 2017;47:1011–1019. doi:10.1007/s40279-016-0618-6
16. Lear A, McCord G, Peiffer J, Watkins RR, Parikh A, Warrington S. Incidence of Staphylococcus aureus nasal colonization and soft tissue infection among high school football players. J Am Board Fam Med. 2011;24:429–435. doi:10.3122/jabfm.2011.04.100286
17. Rackham DM, Ray SM, Franks AS, Bielak KM, Pinn TM. Community-associated methicillin-resistant Staphylococcus aureus nasal carriage in a college student athlete population. Clin J Sport Med. 2010;20:185–188. doi:10.1097/JSM.0b013e3181dba80d
18. Couvé-Deacon E, Postil D, Barraud O, et al. Staphylococcus aureus carriage in French athletes at risk of CA-MRSA infection: a prospective, cross-sectional study. Sports Med Open. 2017;16:3–28.
19. Huijsdens XW, van Lier AM, van Kregten E, et al. Methicillin-resistant Staphylococcus aureus in Dutch soccer team. Emerg Infect Dis. 2006;12:1584–1586. doi:10.3201/eid1210.060387
20. Zaborova VA, Arzumanin VG, Gurevich KG, et al. Species variety of staphylococcal microflora of the skin in athletes engaged in water sports. Bull Exp Biol Med. 2011;151:738–740. doi:10.1007/s10517-011-1429-2
21.
22. Fritz SA, Long M, Gaebelein CJ, Martin MS, Hogan PG, Yetter J. Practices and procedures to prevent the transmission of skin and soft tissue infections in high school athletes. J Sch Nurs. 2012;28:389–396. doi:10.1177/1059840512442899
23. EUCAST breakpoint tables for interpretation of MICs and zone diameters version 8.1 2018.
24. Hosmer DW, Lemeshow S. Applied Logistic Regression. New York, NY: Wiley & Sons; 1989.
25. Deurenberg RH, Vink C, Kalenic S, Friedrich AW, Bruggeman CA, Stobberingh EE. The molecular evolution of methicillin-resistant Staphylococcus aureus. Clin Microbiol Infect. 2007;13:222–235. doi:10.1111/j.1469-0691.2007.01691.x
26. Archibald LK, Shapiro J, Pass A, Rand K, Southwick F. Methicillin-resistant Staphylococcus aureus infection in a college football team: risk factors outside the locker room and playing field. Infect Control Hosp Epidemiol. 2008;29:450–453. doi:10.1086/590662
27. Kazakova SV, Hageman JC, Matava M, et al. A clone of methicillin-resistant Staphylococcus aureus among professional football players. N Engl J Med. 2005;352:468–475. doi:10.1056/NEJMoa040975
28. Kluytmans J, van Belkum A, Verbrugh H. Nasal carriage of Staphylococcus aureus: epidemiology, underlying mechanisms, and associated risks. Clin Microbiol. 1997;10:505–520. doi:10.1128/CMR.10.3.505
29. Wertheim HF, Melles DC, Vos MC, et al. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis. 2005;5:751–762. doi:10.1016/S1473-3099(05)70295-4
30. den Heijer CD, van Bijnen EM, Paget WJ, et al. Prevalence and resistance of commensal Staphylococcus aureus, including meticillin-resistant S. aureus, in nine European countries:a cross-sectional study. Lancet Infect Dis. 2013;13:409–415. doi:10.1016/S1473-3099(13)70036-7
31. Zanelli G, Sansoni A, Zanchi A, et al. Staphylococcus aureus nasal carriage in the community: a survey from central Italy. Epidemiol Infect. 2002;129:417–420. doi:10.1017/S0950268802007434
32. De Giusti M, Marinelli L, Aurigemma C, et al. Prevalence of Staphylococcus aureus colonization and antibiotic susceptibility: A survey among biomedical students. Public Health. 2013;127:392–394. doi:10.1016/j.puhe.2012.09.008
33. Sollid JU, Furberg AS. Hanssen AM, Johannessen M. Staphylococcus aureus: determinants of human carriage. Infect Genet Evol. 2014;21:531–541. doi:10.1016/j.meegid.2013.03.020
34. Esposito S, Terranova L, Zampiero A, et al. Oropharyngeal and nasal Staphylococcus aureus carriage by healthy children. BMC Infect Dis. 2014;14:723. doi:10.1186/s12879-014-0723-9
35. Mertz D, Frei R, Jaussi B, et al. Throat swabs are necessary to reliably detect carriers of Staphylococcus aureus. Clin Infect Dis. 2007;45:475–477. doi:10.1086/520016
36. Nilsson P, Ripa T. Staphylococcus aureus throat colonization is more frequent than colonization in the anterior nares. J Clin Microbiol. 2006;44:3334–3339. doi:10.1128/JCM.00390-06
37. Stacey AR, Endersby KE, Chan PC, Marples RR. An outbreak of methicillin resistant Staphylococcus aureus infection in a rugby football team. Br J Sports Med. 1998;32:153–154. doi:10.1136/bjsm.32.2.153
38. Diep BA, Gill SR, Chang RF, et al. Complete genome sequence of USA300, an epidemic clone of community-acquired meticillin-resistant Staphylococcus aureus. Lancet. 2006;367:731–739. doi:10.1016/S0140-6736(06)68231-7
39. Feng Y, Chen CJ, Su LH, Hu S, Yu J, Chiu CH. Evolution and pathogenesis of Staphylococcus aureus: lessons learned from genotyping and comparative genomics. Microbiol. 2008;32:23–37.
40. Chua K, Laurent F, Coombs G, Grayson ML, Howden BP. Antimicrobial resistance: not community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)! A clinician’s guide to community MRSA—its evolving antimicrobial resistance and implications for therapy. Clin Infect Dis. 2011;52:99–114. doi:10.1093/cid/ciq067
41. Fiebelkorn KR, Crawford SA, McElmeel ML, Jorgensen JH. Practical disk diffusion method for detection of inducible clindamycin resistance in Staphylococcus aureus and coagulase negative staphylococci. J Clin Microbiol. 2003;41:4740–4744. doi:10.1128/JCM.41.10.4740-4744.2003
42. Leclercq R. Mechanisms of resistance to macrolides and lincosamides: nature of the resistance elements and their clinical implications. Clin Infect Dis. 2002;34:482–492. doi:10.1086/324626
43. Lozano C, Aspiroz C, Sáenz Y, et al. Genetic environment and location of the lnu(A) and lnu(B) genes in methicillin-resistant Staphylococcus aureus and other staphylococci of animal and human origin. J Antimicrob Chemother. 2012;67:2804–2808. doi:10.1093/jac/dks320
44. Paul M, Bishara J, Yahav D, et al. Trimethoprim-sulfamethoxazole versus vancomycin for severe infections caused by meticillin resistant Staphylococcus aureus: randomised controlled trial. BMJ. 2015;350:2219. doi:10.1136/bmj.h2219
45. De Angelis G, Cipriani M, Cauda R, Tacconelli E. Treatment of skin and soft tissue infections due to community-associated methicillin-resistant Staphylococcus aureus in Europe: the role of trimethoprim-sulfamethoxazole. Clin Infect Dis. 2011;52:1471–1472. doi:10.1093/cid/cir247
46. Many PS. Preventing community-associated methicillin-resistant Staphylococcus aureus among student athletes. J Sch Nurs. 2008;24:370–378. doi:10.1177/1059840508326448
47. Nguyen DM, Mascola L, Bancroft E. Recurring methicillin-resistant Staphylococcus aureus infections in a football team. Emerg Infect Dis. 2005;11:526–532. doi:10.3201/eid1104.041094
48. Cohen PR. Cutaneous community-acquired methicillin-resistant Staphylococcus aureus infection in participants of athletic activities. South Med J. 2005;98:596–602. doi:10.1097/01.SMJ.0000163302.72469.28
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.