")
Back to Journals » Clinical Optometry » Volume 13
Prevalence of Prescription Glasses in the First-Grade Thai Students (7–8 Years Old)
Authors Wangtiraumnuay N, Trichaiyaporn S, Lueangaram S, Surukrattanaskul S, Wongkittirux K
Received 9 June 2021
Accepted for publication 21 July 2021
Published 3 August 2021 Volume 2021:13 Pages 235—242
DOI https://doi.org/10.2147/OPTO.S323999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Nutsuchar Wangtiraumnuay, Sumalin Trichaiyaporn, Sirin Lueangaram, Supawan Surukrattanaskul, Kwanjai Wongkittirux
Department of Ophthalmology, Queen Sirikit National Institute of Child Health, Bangkok, Thailand
Correspondence: Nutsuchar Wangtiraumnuay
Department of Ophthalmology, Queen Sirikit National Institute of Child Health, Bangkok, Thailand
Tel +6693-919-6241
Email [email protected]
Purpose: To study the prevalence of the prescription glasses given to first-grade students due to the “Good Sight for Thai Children” (GSTC) policy.
Methods: This was a cross-sectional study that examined all prescription glasses given to first-grade students throughout Thailand, after visual screening due to the GSTC policy between 2016 and 2017. Trained class teachers screened their students’ visual acuity and referred children who had less than 20/40 visual acuity in either eye to a hospital for an eye examination and prescription glasses.
Results: A total of 786,729 students were screened. Of these, 20,401 (2.59%) students were referred to hospital. However, only 9867 (48.37%) students presented to a hospital. Glasses were prescribed for 5324 (53.96%) students following cycloplegic refraction by ophthalmologists or trained refractionists. The mean spherical equivalent was − 1.08 (− 19.00 to +10.00, SD 2.32) diopters. There were 1626 (30.54%) children at amblyopic risk without glasses. A 5.49% had high myopia (< − 6 diopters), 5.22% had high hyperopia (> +5 diopters) and 27.82% had high astigmatism (> 2 diopters). A cylindrical lens analysis showed that 81.53% had with-the-rule astigmatism, 4.07% had against-the-rule astigmatism, and 14.40% had oblique astigmatism.
Conclusion: Although the reliable prevalence of refractive error cannot be estimated, the prevalence of visual impairment may be estimated. There were a number of students who required glasses. The astigmatism was the most common refractive error on prescription glasses for first-grade children. With-the-rule astigmatism was the most prevalent. The visual screening program of school children proved to be valuable and should be continued and developed.
Keywords: refractive errors, primary school, astigmatism, prescription
Introduction
Refractive errors are common pediatric eye conditions.1,2 The prevalence of all types of refractive errors in primary school-based visual screening has been reported in many countries and has ranged from 5.2% in India,3 4% in the Middle East,4 4.3% in Ethiopia,5 34.5% in Malaysia,6 6.3% in Mexico7 and 9.15% in UK.8 The prevalence of refractive errors seems to be higher in older school children (7 to 13 years)9 and varies among ethnic groups.
In Thailand, the prevalence of visual impairment (best-corrected visual acuity of less than 20/70) in children aged 1–14 years in 2006–2007 was 0.11%.10 Refractive amblyopia caused one-third of all children to become blind.10 Previous studies have been conducted on the prevalence of primary school-based children’s refractive errors, with 12.7% in Bangkok, the Capital city of Thailand,11 5.7% in Nakhon Pathom, Central Thailand; urban area,11 7.3–8.7% in Chiang Mai, Northern Thailand,12 6.4% in Songkhla, Southern Thailand13 and 4.14% from 4 other geographic regions in Thailand.1 School visual screening was recommended.14–16 A cost-effectiveness analysis indicated that a vision screening program could be efficacious for primary school-aged children.13
In unpublished data by Wongkittirux to Thailand National Health Security Office (NHSO), the first 10-province school-based visual screening projects (Bangkok, Samutprakan, Saraburi, Ratchaburi, Phetchaburi, Nakornpanom, Nongbualumphu, Lumphun, Suratthani, and Narathiwat) were carried out between 2014 and 2015. During this time, 31,147 students (4948 students from kindergarten and 26,199 students from primary school) were screened by teacher using Lea chart or Snellen chart. Of these students, 244 (4.93%) and 2386 (9.11%) in kindergarten and primary school, respectively, who had a visual acuity of less than 20/40 in at least one eye were referred to hospital. Of which 92.21% and 74.72%, respectively, presented for ophthalmological evaluation. After cycloplegic refraction, glasses were prescribed for 54 (1.09%) kindergarten and 1059 (4.59%) primary school students. The false-positive of school vision screening was found to be 66.22% and 42.01% in kindergarten and primary school students, respectively. The primary school students (7–12 years old) had more cooperative behavior than kindergarten students (4–6 years old).
After the 10-province school-based visual screening project results were reported, the Good Sight for Thai Children policy (GSTC) was announced by the Thai government in 2016. Before this, the visual screening in Thailand was not extensive. Most children presented at the hospital with ocular symptoms. After this, a visual screening program started in primary schools. The strategy was to integrate eye health care with school health and improve the education levels and health of children simultaneously. This public policy aimed to screen the visual acuity of first-grade students at school by teachers in all regions of Thailand and to prescribe glasses as needed. Here, we report the prevalence of the prescription glasses given to first-grade students due to the “Good Sight for Thai Children” (GSTC) policy and also detail the refractive errors observed.
Materials and Methods
This retrospective cross-sectional study was designed to describe the prevalence of prescription glasses in first-grade students in the policy “Good sight for Thai Children”. The Institutional Review Board (IRB) was obtained from Queen Sirikit National Institute of Child Health and the studies were conducted in accordance with the Declaration of Helsinki in July 2020. The consent was waived from ethics committee according to the screening was national policy and did not involve identifiable private information about the students.
The visual screening policy was part of national regulations approved by NHSO and was conducted in all regions of Thailand from July 2016 to June 2018. Volunteer ophthalmologists came to a meeting to learn about the new guideline due to the GSTC policy. Primary school teachers were trained by local ophthalmologists on the referral guideline and how to screen student’s visual acuity. Visual acuity screening was conducted in primary school by trained teachers, which is the same method used in a number of countries.15 A 6m Snellen chart was used in the screening. The first-grade students, who had a visual acuity of less than 20/40 in at least one eye, were referred to a local ophthalmologist for a comprehensive eye examination. The age of the first-grade students in Thailand is approximately 7–8 years old. Cycloplegic refraction with 1% cyclopentolate was done to the children who had a confirmed visual acuity of less than 20/40 by practitioner experience at the hospital, and glasses were prescribed to those children based on cycloplegic refraction. The glasses were not prescribed to the children with minor refractive error; astigmatism less than 0.5 diopters, hyperopia less than +1.00 diopters and myopia less than −0.50 diopters. The classification of refractive errors is shown in Table 1.17–27
 |
Table 1 Classification of Refractive Errors.16–26 |
We examined the prevalence of refractive errors and the number of children who were at risk of refractive amblyopia if they did not wear glasses. We classified amblyopic risk in two categories: anisometropic amblyopia, and isometropic amblyopia. The amblyopic risk of anisometropia occurs when the refractive errors between two eyes are different by more than 3 diopters in myopia, and 1.5 diopters in hyperopia, and astigmatism.28 The amblyopic risk of isometropia occurs when the refractive errors in each eye are more than 6 diopters in myopia, 5 diopters in hyperopia, and 2 diopters in astigmatism.28
Results
These results are from the first 2-years of the policy, with the first year between July 2016 and June 2017, and the second year between July 2017 and June 2018. Ninety-one hospitals in the first year and 99 hospitals in the second year took part.
A total of 786,729 first-grade students were screened by a trained teacher (441,304 students in the first year and 345,425 students in the second year). Of these, 20,401 students (2.59%) were referred to hospital. However, only 9867 (48.37%) students presented to a hospital. Of those children that presented to a hospital, glasses were prescribed to 5324 (53.96%) students as shown in Figure 1. The false-positive rate of school visual screening was 46.04%. In the first year, the glasses were prescribed to 3226 students (1698 boys and 1528 girls), 879 (27.25%) pairs for children in the northern region, 732 (22.69%) for the northeastern region, 666 (20.64%) for the southern region, 760 (23.56%) for the central region and 189 (5.86%) for Bangkok. In the second year, the glasses were prescribed to 2098 students (1147 boys and 951 girls), 709 (33.79%) pairs for children in the northern region, 322 (15.35%) for the northeastern region, 456 (21.73%) for the southern region, 538 (25.64%) for the central region and 73 (3.48%) in Bangkok. Most of the children stayed in rural area. The information on the preexisting spectacles was not collected.
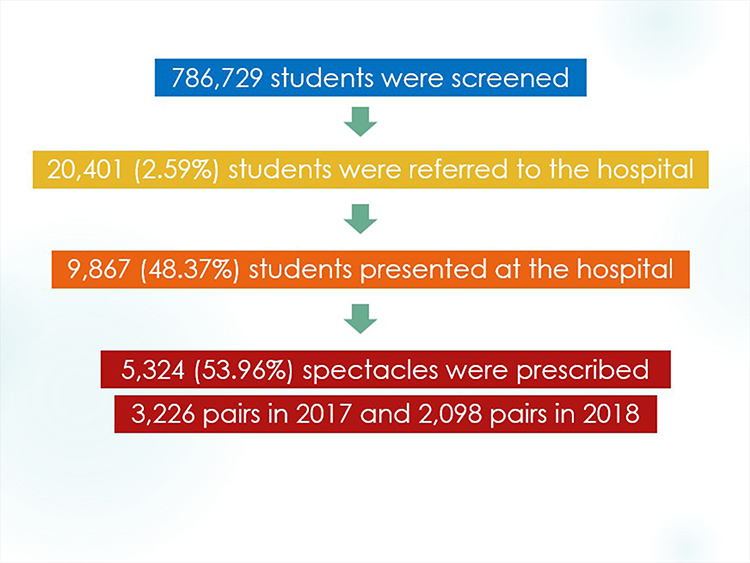 |
Figure 1 Flow chart of the visual screening system and number of students in every stage of the screening. |
The mean spherical equivalent from both years was −1.07 to −1.14 diopters (D) (SD 2.18–2.46), and the median was −0.75 D to −0.88 D, with a range from −19.00 to +10.00 D as shown in Table 2. The prevalence of refractive errors in each category is displayed in Table 3. Simple myopia was defined as a spherical equivalent of equal to or less than −0.50 D without astigmatism. Simple hyperopia was defined as the spherical equivalent of equal to or greater than +1.00 D without astigmatism. Furthermore, astigmatism was defined as multiple focal points on the retina, which can be classified into 5 categories: simple myopic astigmatism, simple hyperopic astigmatism, compound myopic astigmatism, compound hyperopic astigmatism and mixed astigmatism. Of the students, 0.14% (1111.5 students) got simple myopia glasses, 0.05% (402.5 students) got simple hyperopia glasses and 0.46% (3594 students) got astigmatism glasses.
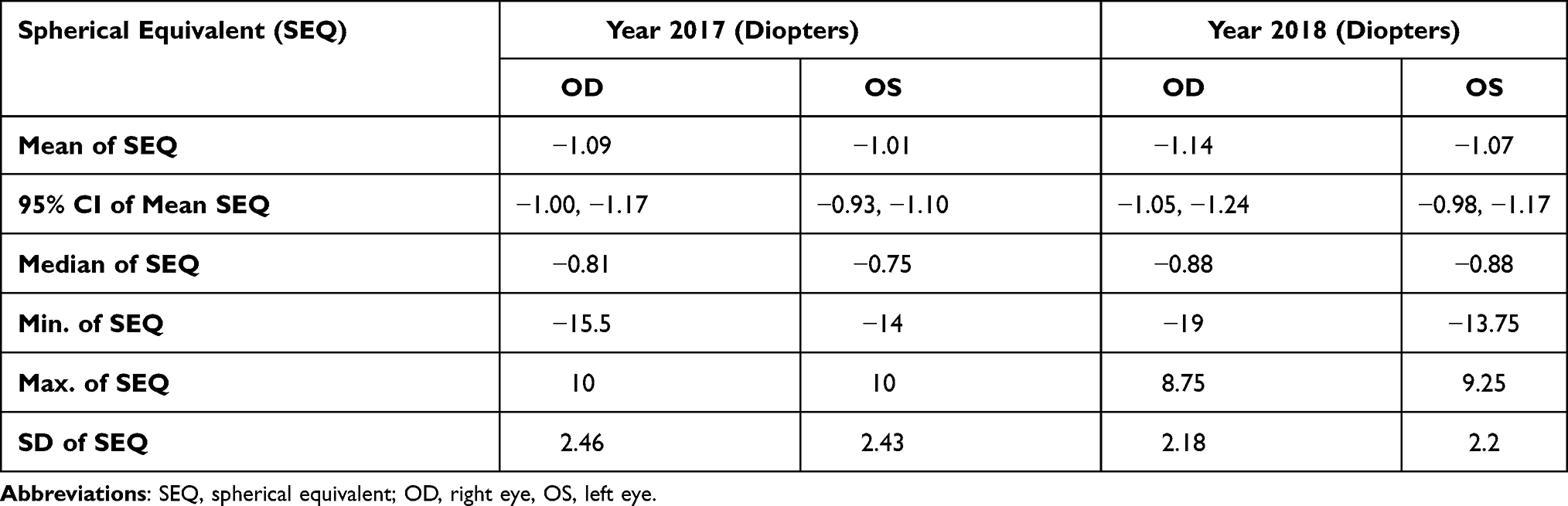 |
Table 2 Spherical Equivalent (SEQ) of Prescription Glasses in the Right Eye and Left Eye in 2017 and 2018 |
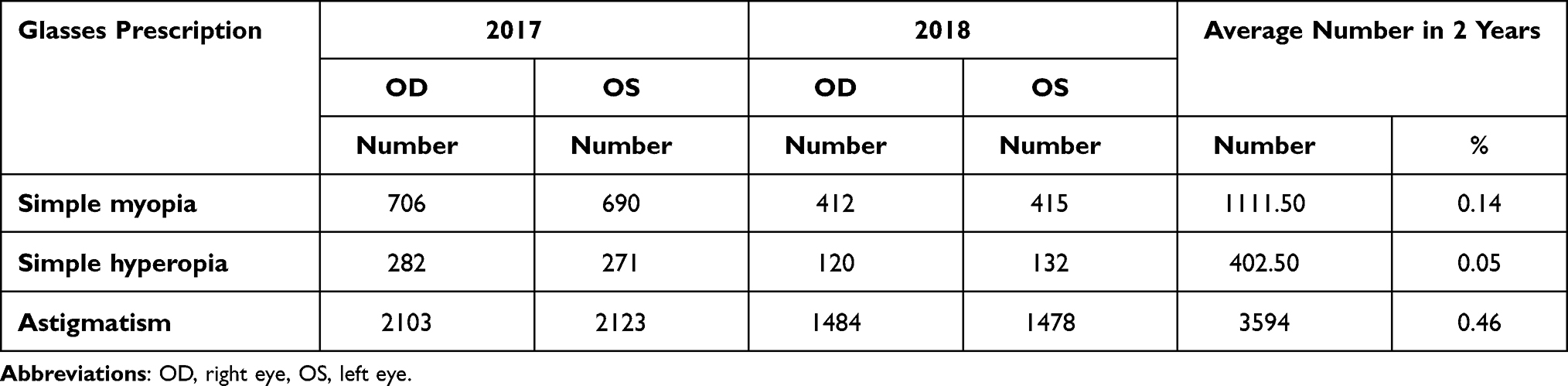 |
Table 3 Prevalence of Myopia, Hyperopia and Astigmatism |
Details of the prescriptions are shown in Table 4, with 68.05% (65.19–70.73%), 20.67% (19.64–21.88%), 7.29% (5.72–8.74%) and 3.99% (3.48–4.40%) of the students having astigmatism, simple myopia, simple hyperopia and plano, respectively. The plano-lens was prescribed to patients with significant refractive errors in the other eye. In total, 5.55% (5.07–5.83%) had high myopia, 4.56% (2.27–6.38%) had high hyperopia and 28.77% (27.29–30.62%) had high astigmatism. The most common refractive error in both years was astigmatism. Regarding the isolated refractive error group, mild myopia, mild hyperopia, and moderate astigmatism were the most common findings. A cylindrical lens analysis showed that 32% of those that were prescribed glasses did not have astigmatism. The rest of those students that were prescribed glasses had astigmatism, the majority of which had with-the-rule astigmatism (55% of those prescribed glasses and 81% of all types of astigmatism), followed by oblique astigmatism (10% of those prescribed glasses and 15% of all types of astigmatism), and against-the-rule astigmatism was the minority in our study (3% of those prescribed glasses and 4% of all types of astigmatism) as shown in Table 5.
 |
Table 4 The Number of Prescribing Glasses in 2017 and 2018 |
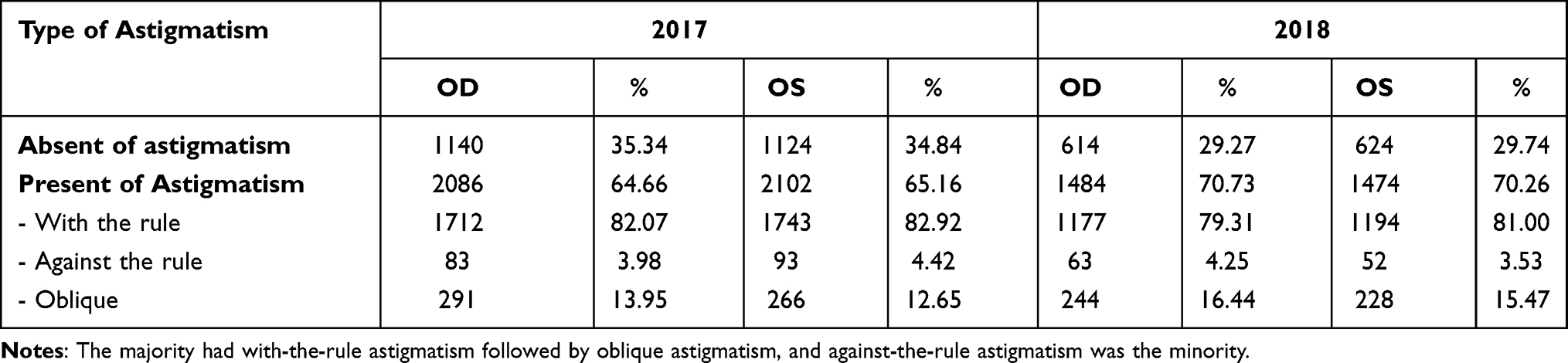 |
Table 5 Type of Astigmatism of the Prescription Glasses in 2017 and 2018 |
We examined the risk of amblyopia. If the students met the criteria for anisometropia or isometropia, we considered that they had amblyopic risk. There were 1626 (30.54%) students who were considered to be at risk of amblyopic in our study. In the second year of the study, we asked the teachers to measure visual acuity on the screening day as well as 3 months after the student started wearing glasses. We received data on 1346 of the 2098 children (64%), which showed that visual acuity improved by about 3 lines on the EDTRS chart (3.25 lines in the right eye and 3.21 lines in the left eye). After wearing glasses for 3 months, 21.84% (294) and 17.98% (242) still had a visual acuity of less than 20/40 in the right and left eye, respectively.
Discussion
This is the largest children’s visual screening program that has been conducted in Thailand. More than 700,000 first-grade children have been screened in 2 years. The prevalence of the children who failed the visual screening was only 2.59% (20,401 out of 786,729 students), which was low compared to other studies conducted in India, Ethiopia, Mexico, China and USA3–5,7,29,30 (Table 6). There are a few possible reasons for this low prevalence. First, some children may already have had glasses, which we did not have information about this. Second, all students were in the first-grade and were aged between 7 and 8 years old. It is known that older age groups are associated with a higher rate of refractive errors.4–9 Lastly, most of the children in this project came from rural areas that might have a lower rate of refractive errors8,31 (Table 6). Only half of the students that failed the visual-screening test presented to a hospital. This might be due to transportation issues, long waiting times at the referral hospital, or lack of parental knowledge and concern about refractive errors in children. The false-positive rate of school visual screening was 46.04%, which was close to the rate found in the 10-province pilot project in relation to primary school-aged students (42.01%). The first-grade students cooperated sufficiently for visual screening. The annual refresh training courses for teachers and repeat visual screening for students might help decrease the false-positive screening rate.
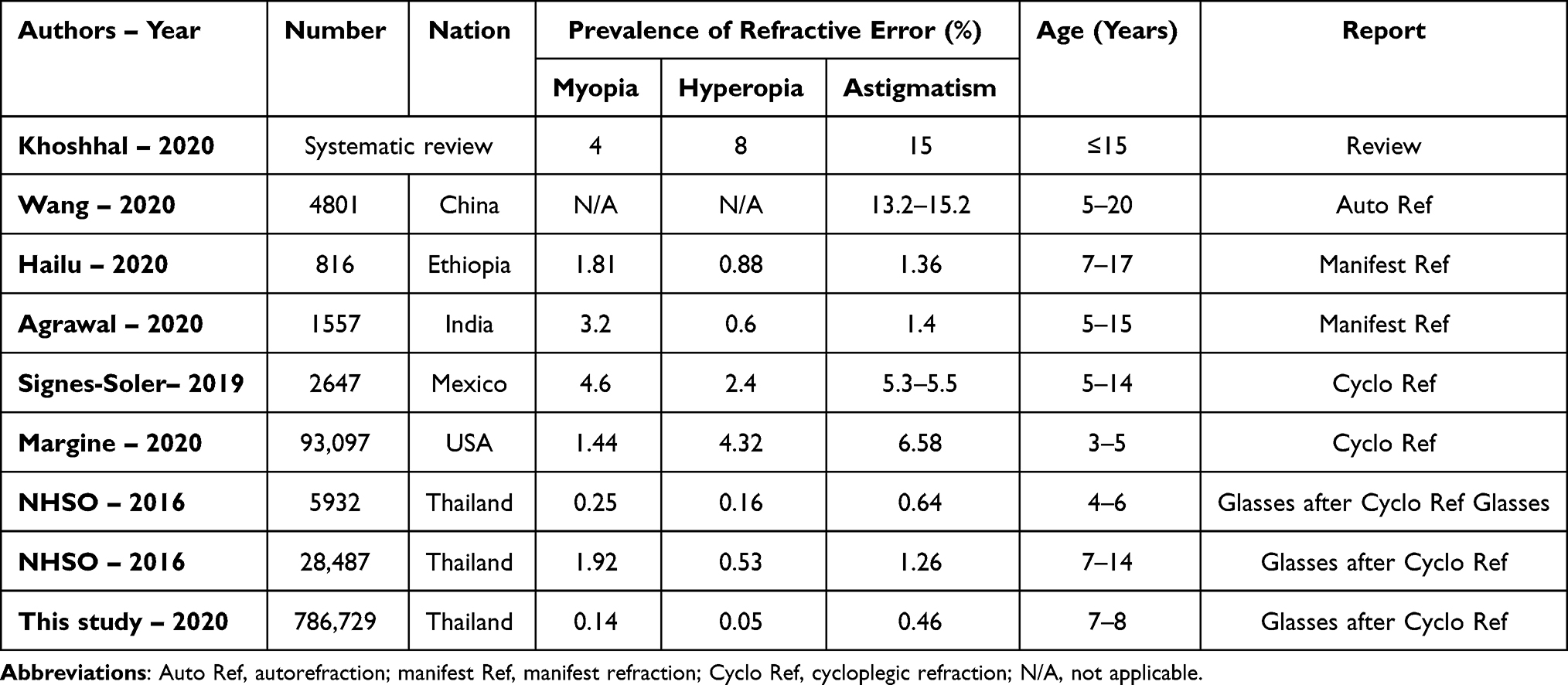 |
Table 6 The Table Compares the Prevalence of Refractive Error in Our Studies to Previous Studies |
There were students with a severe level of myopia, hyperopia, and astigmatism in both years. Astigmatism (seen in 70% of those prescribed glasses) was the most common type of refractive error, which is in agreement with the reports by Khoshhal et al (systematic review), Signes-Soler et al (Mexico), and Margine et al (USA).5,7,30 The majority of studies have found that the prevalence of myopia (0.25–4.6%) is higher than hyperopia (0.16–8%). However, Margine et al30 had conflicting results, which might be due to their younger population and the data being taken after cycloplegic refraction. A similar trend was observed in our study, where the prevalence of myopia was higher than hyperopia. However, our study had a much lower percentage of prevalence because we reported the prevalence of refractive errors seen in those prescribed glasses. The minor refractive errors, which did not affect the vision, were abandoned. The prevalence of prescribed glasses was incomparable with the prevalence of manifest or cycloplegic refractions from all children.
With-the-rule astigmatism was the most prevalent in our study (81%), which was in agreement with Wang et al32 (75%) and Wang et al29 (85%). The meta-analysis showed the prevalence of adult myopia and astigmatism was highest in South-East Asia.33 The in-depth analyses of the parental refractive status and daily life activities are needed to understand the genetics and environmental effects.
Thirty percent of those prescribed glasses were at risk of amblyopia. There were a number of students who required prescription glasses. The vision of children with amblyopia can be improved. On average, visual acuity improved 3 lines on the EDTRS chart over a 3-month period. Twenty percent of the students had a visual acuity of less than 20/40 after wearing glasses for 3 months, which might be patients with amblyopia or refraction errors. The limitations of our study are less than 50% of the referral students presented at a hospital and lack of follow-up data due to large scale of children from all regions in Thailand.
We reported the prevalence of prescription glasses in first-grade students. Although a reliable prevalence of refractive error cannot be estimated from this study, the prevalence of visual impairment may be estimated. There were a number of students who required glasses and had amblyopic risk. Astigmatism is the most common refractive error on prescription glasses for first-grade children. With-the-rule astigmatism was the most prevalent. The visual screening program of school children proved to be valuable and should be continued, developed and expanded to other levels of primary school. More than half of the students who failed the visual screening test did not present to a hospital. Further studies are needed to understand the barriers to their attendance and consider ways to improve attendance.
Acknowledgments
We would like to express the special thanks to “Juthathip Hiriotappa, Pokpong Chantarasomboon, Bung-ornrat Keyurapan, Panee Potima, Suwanee Panklay, Pranee Na-muengruk, Sunisa Tephusdin, Rapeepan Phuyathon, Kankamon Sribua-ngam, Nookade Pukpila, Bung-orn Piyawong, Siripat Wongwik and all participated schools and hospitals” who supported to this project.
Funding
National Health Security Office (NHSO). The funding organization had no role in the design or conduct of this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Teerawattananon K, Myint CY, Wongkittirux K, et al. Assessing the accuracy and feasibility of a refractive error screening program conducted by school teachers in pre-primary and primary schools in Thailand. PLoS One. 2014;9(6):e96684. doi:10.1371/journal.pone.0096684
2. Wadhwani M, Vashist P, Singh SS, Gupta V, Gupta N, Saxena R. Prevalence and causes of childhood blindness in India: a systematic review. Indian J Ophthalmol. 2020;68(2):311–315. doi:10.4103/ijo.IJO_2076_18
3. Agrawal D, Sahu A, Agrawal D. Prevalence of ocular morbidities among school children in Raipur district, India. Indian J Ophthalmol. 2020;68(2):340–344. doi:10.4103/ijo.IJO_1454_19
4. Khoshhal F, Hashemi H, Hooshmand E, et al. The prevalence of refractive errors in the Middle East: a systematic review and meta-analysis. Int Ophthalmol. 2020;40(6):1571–1586. doi:10.1007/s10792-020-01316-5
5. Hailu Y, Hiko D, Shaweno T. Prevalence of visual impairment and associated factors among primary school children in Addis Ababa, Central Ethiopia. Clin Ophthalmol. 2020;14:767–774. doi:10.2147/OPTH.S245675
6. Omar R, Wan Abdul WMH, Knight VF. Status of visual impairment among indigenous (Orang Asli) school children in Malaysia. BMC Public Health. 2019;19(Suppl 4):543. doi:10.1186/s12889-019-6865-3
7. Signes-Soler I, Piñero DP, Murillo MI, Tablada S. Prevalence of visual impairment and refractive errors in an urban area of Mexico. Int J Ophthalmol. 2019;12(10):1612–1617. doi:10.18240/ijo.2019.10.14
8. Toufeeq A, Oram AJ. School-entry vision screening in the United Kingdom: practical aspects and outcomes. Ophthalmic Epidemiol. 2014;21(4):210–216. doi:10.3109/09286586.2014.906627
9. Xie Z, Long Y, Wang J, Li Q, Zhang Q. Prevalence of myopia and associated risk factors among primary students in Chongqing: multilevel modeling. BMC Ophthalmol. 2020;20(1):146. doi:10.1186/s12886-020-01410-3
10. Wongkittirux K. Blindness, low vision and eye diseases in Thai Children. J Health Syst Res. 2012;6(4):501–512.
11. Yingyong P. Refractive errors survey in primary school children (6–12 year old) in 2 provinces: Bangkok and Nakhonpathom (one year result). J Med Assoc Thai. 2010;93(10):1205–1210.
12. Tananuvat N, Manassakorn A, Worapong A, Kupat J, Chuwuttayakorn J, Wattananikorn S. Vision screening in schoolchildren: two years results. J Med Assoc Thai. 2004;87(6):679–684.
13. Tengtrisorn S, Sangsupawanitch P, Chansawang W. Cost effectiveness analysis of a visual screening program for primary school children in Thailand. J Med Assoc Thai. 2009;92(8):1050–1056.
14. Olusanya BA, Ugalahi MO, Ogunleye OT, Baiyeroju AM. Refractive errors among children attending a tertiary eye facility in Ibadan, Nigeria: highlight the need for school eye health problems. Ann Ib Postgrad Med. 2019;17(1):49–59.
15. Chen AH, Abu Bakar NF, Arthur P. Comparison of the pediatric vision screening program in 18 countries across five continents. J Curr Ophthalmol. 2019;31(4):357–365. doi:10.1016/j.joco.2019.07.006
16. Gonsalves S, Ganagi S, Vivedkanad U. School screening in Coastal Karnataka. Rom J Ophthalmol. 2019;63(3):245–248. doi:10.22336/rjo.2019.37
17. Xi L, Zhang C, He Y. Single-step transepithelial photorefractive keratectomy in the treatment of mild, moderate, and high myopia: six-month results. BMC Ophthalmol. 2018;18(1):209. doi:10.1186/s12886-018-0888-x
18. Li Q, Yang J, He Y, et al. Investigation of the psychological health of first-year high school students with myopia in Guangzhou. Brain Behav. 2020;10(4). doi:10.1002/brb3.1594
19. Alsaif NK, Al-Sharif EM, Alsaif SK, Mousa A, Al-Muammar AM. Corneal elevation indices and pachymetry values of Saudi myopes using scheimpflug imaging. Saudi Med J. 2020;41(2):168–176. doi:10.15537/smj.2020.2.24876
20. Lim DH, Han J, Chung TY, Kang S, Yim HW; Epidemiologic Survey Committee of the Korean Ophthalmologic Society. The high prevalence of myopia in Korean children with influence of parental refractive errors: the 2008–2012 Korean National Health and Nutrition Examination Survey. [2018 Dec 20; 13(12):e0209876]. PLoS One. 2018;13(11):e0207690
21. Chen AH, Abu Bakar NF, Arthur P. Reply to letter – comparison of the pediatric vision screening program in 18 countries across five continents. J Curr Ophthalmol. 2020;32:120–121. doi:10.4103/JOCO.JOCO_52_20
22. Jenchitr W, Padungkiatsakul P. Ocular pathology of hyperopic patients in University eye clinic. J Curr Sci Technol. 2019;9(2):123–130. ISSN 2630-0656.
23. Hashemi H, Asharlous A, Yekta A, et al. Enantiomorphism and rule similarity in the astigmatism axes of fellow eyes: a population-based study. J Optom. 2019;12(1):44–45. doi:10.1016/j.optom.2017.12.002
24. Eyewiki, American academy of Ophthalmology. Hyperopia; [update January 6, 2015]. Available from: https://eyewiki.aao.org/Hyperopia.
25. Cornea Associates of Texas. Refractive errors and vision correction surgery Dallas Fort Worth. Available from: https://www.corneatexas.com/about/eye-info/refractive-errors.
26. Griffin eye center. Types of vision problems. Available from: https://griffineyecenter.com/vision-problems/.
27. The Laser Center of Coral Gables. Astigmatism. Available from: http://tlccoralgables.com/astigmatism.
28. American Academy of Ophthalmology. Pediatric Ophthalmology and Strabismus, Section 6 of Basic and Clinical Science Course. Chapter 5. San Francisco; 2010:63–64.
29. Wang J, Cheng QE, Fu X, et al. Astigmatism in school students of eastern China: prevalence, type, severity and associated risk factors. BMC Ophthalmol. 2020;20(1):155. doi:10.1186/s12886-020-01425-w
30. Margines JB, Huang C, Young A, et al. Refractive errors and amblyopia among children screened by the UCLA preschool vision program in Los Angeles County. Am J Ophthalmol. 2020;210:78–85. doi:10.1016/j.ajo.2019.10.013
31. Sheeladevi S, Seelam B, Nukella PB, Modi A, Ali R, Keay L. Prevalence of refractive errors in children in India: a systematic review. Clin Exp Optom. 2018;101(4):495–503. doi:10.1111/cxo.12689
32. Wang Z, Huang D, Chen X, et al. Preschool children exhibit evident compensatory role of internal astigmatism in distribution of astigmatism: the Nanjing Eye Study. Invest Ophthalmol Vis Sci. 2019;60(1):73–81. doi:10.1167/iovs.18-24799
33. Hashemi H, Fotouhi A, Yekta A, Pakzad R, Ostadimoghaddam H, Khabazkhoob M. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol. 2017;30(1):3–22. doi:10.1016/j.joco.2017.08.009
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.