Back to Journals » Journal of Asthma and Allergy » Volume 16
Prevalence of Poorly Controlled Asthma and Factors Associated with Specialist Referral in Those with Poorly Controlled Asthma in a Paediatric Asthma Population
Authors Kallis C ![]() , Morgan A, Fleming L, Quint JK
, Morgan A, Fleming L, Quint JK ![]()
Received 2 July 2023
Accepted for publication 24 September 2023
Published 3 October 2023 Volume 2023:16 Pages 1065—1075
DOI https://doi.org/10.2147/JAA.S428623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Constantinos Kallis,1,2,* Ann Morgan,1,2,* Louise Fleming,1 Jennifer K Quint1,2
1National Heart and Lung Institute, Imperial College London, London, UK; 2School of Public Health, Imperial College London, London, UK
*These authors contributed equally to this work
Correspondence: Jennifer K Quint, National Heart and Lung Institute and School of Public Health, Imperial College London, Sir Michael Uren Building, White City Campus, Imperial College, London, UK, Tel +44 207 594 8821, Email [email protected]
Background: Significant morbidity and mortality are associated with poor asthma control. The aim of this study was to determine factors associated with poor control and referral to specialist secondary care services.
Methods: We used primary care data from the Clinical Practice Research Datalink Aurum (CPRD) linked with Hospital Episode Statistics (HES) records from 1st January 2007 to 31st December 2019. We selected patients aged 6– 17 years old. Poor control was defined as six or more prescriptions of short-acting beta-agonist (SABA) inhalers, two or more courses of oral corticosteroids (OCS), an Asthma Control test (ACT) or childhood ACT < 20, one hospital admission for asthma, or one visit to Accident & Emergency (A&E) department for asthma-related episodes in the 12 months following asthma diagnosis. Asthma severity was defined following GINA guidelines 2021.
Results: About 17.6% of children aged between 6 and 17 years with active asthma had poor control. Severe asthma, eczema, food allergies, increased BMI and living in deprived areas were identified as risk factors for poor control. Among those with poor control, referral rates to specialist care were extremely low, only 2% overall. Those with severe asthma were three-times more likely to be referred than those with mild-to-moderate asthma [HRcrude = 4.04 (95% CI, 3.35– 4.87); HRadj = 2.72 (95% CI: 2.13– 3.49)]. Other factors associated with referral were food allergy and living in a more deprived area.
Conclusion: Around 1 in 6 children and adolescents with active asthma are not achieving adequate control of their symptoms. Among the subset of 6– 17-year olds with poorly controlled asthma, timely referral for specialist advice in secondary care is rare, especially in those with so-called mild asthma who nevertheless are at significant risk for poor asthma outcomes.
Keywords: asthma, poor control, referral to specialist
Introduction
Asthma is the most common chronic disease in children worldwide. According to global rankings, asthma is in the top 10 causes of disability-adjusted life years (DALYs) lost in children aged 5–14 years.1 In the UK, a child with asthma is admitted to a hospital every 20 minutes, and children with asthma lose up to 2.8 million school days per year.2,3 Asthma management aims to achieve and maintain overall asthma control by reducing the severity of symptoms and minimising the future risk of adverse outcomes (including exacerbations), thus maintaining normal activity levels and good quality of life.4
Despite the availability of effective treatments, the prevalence of suboptimal or poor control among children with asthma remains high. Reported estimates vary, but severe asthma and/or poorly controlled asthma is believed to affect between 5% and 10% of the asthmatic paediatric population.5 Patients with inadequately controlled severe persistent asthma are at a particularly high risk of exacerbations, hospitalization and death, and often have severely impaired quality of life.3,4,6 Uncontrolled asthma in early childhood has also been shown to be associated with impaired lung function in adolescence and early adulthood, especially in females.7 The 2014 National Review of Asthma Deaths (NRAD) recommended referral for specialist review in people with asthma who have received three or more courses of oral steroids (OCS), had two or more visits to accident and emergency (A&E), or have been admitted to hospital due to asthma-related episodes.8 However, there is concern that healthcare professionals still have far higher thresholds for referral than those recommended in national guidelines or by the NRAD.9
The aims of this study were therefore two-fold. Firstly, we sought to identify risk factors for poor control in the UK paediatric asthma population (6–17 years). Secondly, we aimed to better understand specialist referral rates among those with asthma poor control and the factors that may be contributing to delayed referral.
Methods
Data Sources
This observational cohort study used routinely collected primary care data from GP practices using EMISWeb software, data which are curated by the UK’s Clinical Practice Research Datalink (CPRD) service and made available in pseudo-anonymized form to researchers as the CPRD Aurum database. As of October 2020, CPRD Aurum comprised longitudinal health data, including information on symptoms, clinical diagnoses and prescriptions, for nearly 12 million living patients or around 18% of the UK population. Aurum data have been shown to be nationally representative with respect to age and sex.10 For patients registered at a subset of Aurum practices, CPRD also provides socioeconomic data (Index of Multiple Deprivation (IMD)) and secondary care data covering hospital admissions and A&E attendances (NHS Digital Hospital Episode Statistics (HES)). Linked patient-level was available for approximately 75% of GP practices in England that contribute data to CPRD Aurum.
Study Design and Population
This study used a rolling entry cohort study design. The study population comprised children and adolescents, aged 6–17 years with current asthma who were registered with a HES-Aurum-linked GP practice for at least 6 months during our study period (1st January 2007 to 31st December 2019). Children with a diagnosis of bronchiectasis, cystic fibrosis, primary ciliary dyskinesia, chronic upper airway cough syndrome or bronchopulmonary dysplasia were excluded. Case finding was based on a set of clinical diagnostic codes that have previously been validated for adults using the CPRD GOLD database against a reference standard of physician review of patient notes and was found to have a high positive predictive value (PPV >86%).11 The codelists used in this analysis are available via GitHub (https://github.com/NHLI-Respiratory-Epi/code_lists).
Initially, two patient cohorts were defined (6–11 years and 12–17 years), mirroring the age-based GINA asthma management recommendations. Children became eligible to enter the study on the date of their 6th (or 12th birthday), 1 January 2007 or the start of registration with a participating GP practice, whichever came later. The date of the first asthma record after study entry was defined as the “asthma date” (the assumption being that at this point in time the patient had active asthma). The index date was defined as the asthma date plus 6 months, generating a 6-month assessment period for the determination of baseline characteristics, including asthma severity. Patient follow-up ended at the earliest on 11th (or 17th) birthday, death, end of GP registration, last date of CPRD data collection, last date of HES data collection or 31st December 2019.
Subsequently, we combined the two age-based cohorts into a single cohort, retaining duplicated individuals, provided that they met the inclusion criteria for a second time (ie, they still had active asthma after they had reached the age of 12 years). This study design maximised the use of the available data and disease severity to be determined using the age-appropriate GINA treatment steps (defined separately for children aged 6–11 and 12–17 years).
Exposures, Outcomes and Covariates
Individuals were classified as having poorly controlled asthma if they fulfilled at least one of the following criteria: six or more prescriptions of short acting beta agonist (SABA) inhalers, two or more short courses of OCS, an asthma control test score (ACT) or childhood ACT (cACT) <20 one or more hospital admissions for asthma, or one or more visits to the A&E department for asthma-related episodes in the 12 months following their index date. These criteria were based on a combination of current management guidelines and clinical consensus.
Information on ACT and cACT scores and medication history (SABAs, OCS and other medications used to treat asthma in children) were extracted from primary care records. We restricted OCS prescriptions to those for prednisolone or dexamethasone at doses recommended for the treatment of a mild asthma exacerbation in children and excluded prescriptions given on the same day as an annual review. This was done to exclude prescription of rescue OCS to keep at home. We used the HES admitted patient care (APC) and A&E datasets to determine hospital admissions/attendances due to asthma; events which occurred within 14 days of each other were considered to be the same event.
A specialist referral was defined as a referral request for an outpatient hospital appointment at either a thoracic/respiratory medicine clinic (code = 340) or a paediatric respiratory medicine clinic (code = 258) as recorded in the HES Outpatient Activity dataset. We did not include outpatient referrals specific to allergies (317 = Allergy (from 1 April 2004)) or general paediatric referrals, and we restricted the analysis to referrals which occurred in the 12-month period following the ascertainment of patients’ asthma control status. The latter decision was informed by clinical expertise and management guidelines.
Baseline characteristics (and potential risk factors for poor control and specialist referral) included age, sex, socioeconomic status, body mass index (BMI) and selected atopic comorbidities – allergic rhinitis/hay fever, eczema and food allergy. We also categorised subjects according to their asthma severity (mild versus severe) based on their medication history. Socioeconomic status was defined using the Index of Multiple Deprivation (IMD) 2019 classification, which is expressed in terms of quintiles and takes values 1–5, where a value of 1 corresponds to least deprived and 5 to most deprived. All other variables were defined using information in primary care records. We used GP-recorded values of BMI, but where these were not available within our predefined recording window (one year either side of the asthma date), we calculated BMI from recorded values of weight and height. Individuals were assigned to BMI categories (underweight, normal, overweight and obese) using WHO standard thresholds for children which are based on age and gender. Study cohort members were considered to have an atopic comorbidity if they had at least one code indicative of a diagnosis of allergic rhinitis/hay fever, eczema or food allergy at any time prior to their asthma diagnosis.
We used the GINA asthma report for 2020 to stratify patients by disease severity.12 Children and adolescents whose prescription history during the 6-month baseline period suggested they were on GINA treatment steps 1–3 were categorised as having mild-to-moderate asthma (baseline group), while those who were on GINA treatment steps 4 or 5 were considered to have severe asthma. Those patients who were only prescribed a SABA during the baseline period were assigned to an additional category, “step 0” and included in the “mild-to-moderate” asthma group. Those who were not prescribed any asthma medications during the 6-month baseline period were excluded from the analysis at this point.
Statistical Analysis
Descriptive statistics were used to tabulate cohort demographics and clinical characteristics, comparing those whose asthma was poorly controlled and those whose asthma was adequately controlled. We used univariable and multivariable logistic regression models to investigate associations between demographic and clinical characteristics at baseline and poor control. We added a cluster option (patid) to take account of the fact that some patients were included twice. We also used an offset term to allow for a less than full 12 months of follow-up post-index date; this was defined as the natural logarithm of the available number of days of follow-up time.
We used univariable and multivariable Cox proportional hazard models to explore the relationship between the same set of demographic and clinical characteristics and time to specialist referral among children and adolescents with poor asthma control. While the primary aim of this second piece of analyses was to determine whether time to referral was associated with disease severity, our secondary objective was to better understand what other factors might be influencing referral rates. As noted above, follow-up time was censored at 12 months. We tested to ensure models met the PH assumptions. All analyses were carried out using STATA version 17 (Stata Corp., College Station, Texas, USA).
Ethical Approval
The protocol for this research was approved by an external review committee for the Research Data Governance Group (RDG) for the Medicines and Healthcare products Regulatory Agency (MHRA) Database Research (protocol number 21_000521) and the approved protocol was made available to the journal and reviewers during peer review. Generic ethical approval for observational research using CPRD with approval from RDG was granted by a Health Research Authority (HRA) Research Ethics Committee (East Midlands–Derby, REC reference number 05/MRE04/87). Linked pseudonymized data were provided for this study by CPRD. Datasets were linked by National Health Service (NHS) Digital, the statutory trusted third party for linking data, using identifiable data held only by NHS Digital. Select practices consent to this process at a practice level, with individual patients having the right to opt-out.
Results
A total of 155,270 children and adolescents aged between 6 and 17 years with asthma were included in the study, of whom 93,961 (60.6%) had received a diagnosis before the age of 12. Among this younger age group (6–11 years), around a third (n = 29,720) continued to be coded as having ongoing asthma after the age of 12 years and were therefore included twice, resulting in a total of 184,990 observations for analysis purposes. Around 40% of the study cohort (n = 63,309) had no evidence of an asthma diagnosis prior to their 12th birthday and were only included in the older age group cohort. Demographic and clinical characteristics of the study cohort, separated into the two age cohorts, 6–11 and 12–17 years, are summarised in Table 1. As anticipated, boys and children in the most deprived quintile were overrepresented in the study population, and approximately a third of children for whom BMI data were available were overweight or obese. We also observed an increase in the proportion of children with severe asthma with age; 6% of 12–17-year-olds were allocated to GINA steps 4 or 5 compared with only 2% of 6–11-year-olds.
 |
Table 1 Baseline Characteristics of the Study Population, by Age Cohort |
Poor Control
Overall, 17.6% (n = 27,396) of the study cohort had evidence of suboptimal asthma control. The prevalence of poor control was higher in boys than in girls (18.3% vs 16.7%); poor control was also more common in those allocated to GINA steps 4–5 (40.9%) than in those who were allocated to GINA steps 0–3 (16.6%).
We also observed a higher prevalence of poorly controlled asthma among children and adolescents who were either overweight or obese and among those in the highest IMD quintile (most deprived); this pattern was apparent in both age cohorts (Table 1). Analysis of descriptive statistics suggested that the presence of atopic comorbidities (eczema and allergic rhinitis) were also linked to a higher prevalence of poor control in our study population.
The results of our univariable regression analysis (Table 2) confirmed that male gender, living in a more deprived area, underweight or overweight/obese, greater disease severity (on GINA treatment step 4 or 5) and atopic comorbidities were all potential risk factors for poor control. Among the factors considered, severe asthma exhibited the strongest association with poor control; children and adolescents who were on GINA treatment step 4 or 5 were almost four times more likely to have poor controlled asthma compared with those who had mild-to-moderate asthma (ORcrude= 3.94; 95% CI, 3.75–4.14) (Table 2). Adjustment for other risk factors resulted in only a small attenuation of the association between asthma disease severity and risk of poor control (ORadj= 3.79; 95% CI, 3.57–4.03). This apparent association is highly likely to be a result of reverse causality. It is more clinically plausible that patients with poorly controlled asthma are on GINA steps 4 and 5 and not the other way round. Other risk factors, including male gender, high or low BMI, low SES and atopy (in particular food allergy) all remained significant after adjustment (Table 2).
 |
Table 2 Odds Ratios for Selected Risk Factors for Poor Control in a Paediatric Asthma Population (Aged 6–17 Years) |
Referral to Specialist Care
Among the subset of 24,834 unique individuals who were identified as having suboptimal asthma control, only 523 or 2.1% were offered a referral to a pulmonary specialist within a 12-month window. Specialist 12-month referral rates were higher in children and adolescents with severe asthma; 6.2% (n = 158 out of 2534) of 6–17-year-olds with poor control and on GINA treatment steps 4 or 5 were referred to a respiratory specialist compared with only 1.6% (n = 365 out of 22,675) of those with poor control but considered to have mild-to-moderate asthma (GINA steps 0–3). However, in absolute terms, more children with mild-to-moderate asthma were referred than children with severe asthma.
Key characteristics of children and adolescents with poorly controlled asthma, disaggregated by age cohort and referral status, are summarised in Table 3. While boys were overrepresented in the subset of children and adolescents with poor control, among those who are referred the gender balance is more equal suggesting that girls are more likely to be referred for specialist care than boys, especially in the older age cohort. In both age cohorts, greater severity and asthma and atopy were more prevalent among those with a referral than those who were not. In terms of our poor control criteria, around 60% of 6–11-year-olds had been prescribed six or more SABA prescriptions; this proportion rises to around 70% in the older age group. Nearly half of 6–11-year-olds (46%) were hospitalised for asthma exacerbation on at least one occasion in the 12-month period prior to their referral, while 15% had attended A&E prior to being offered a referral. These proportions were similar in the older cohort (Table 3).
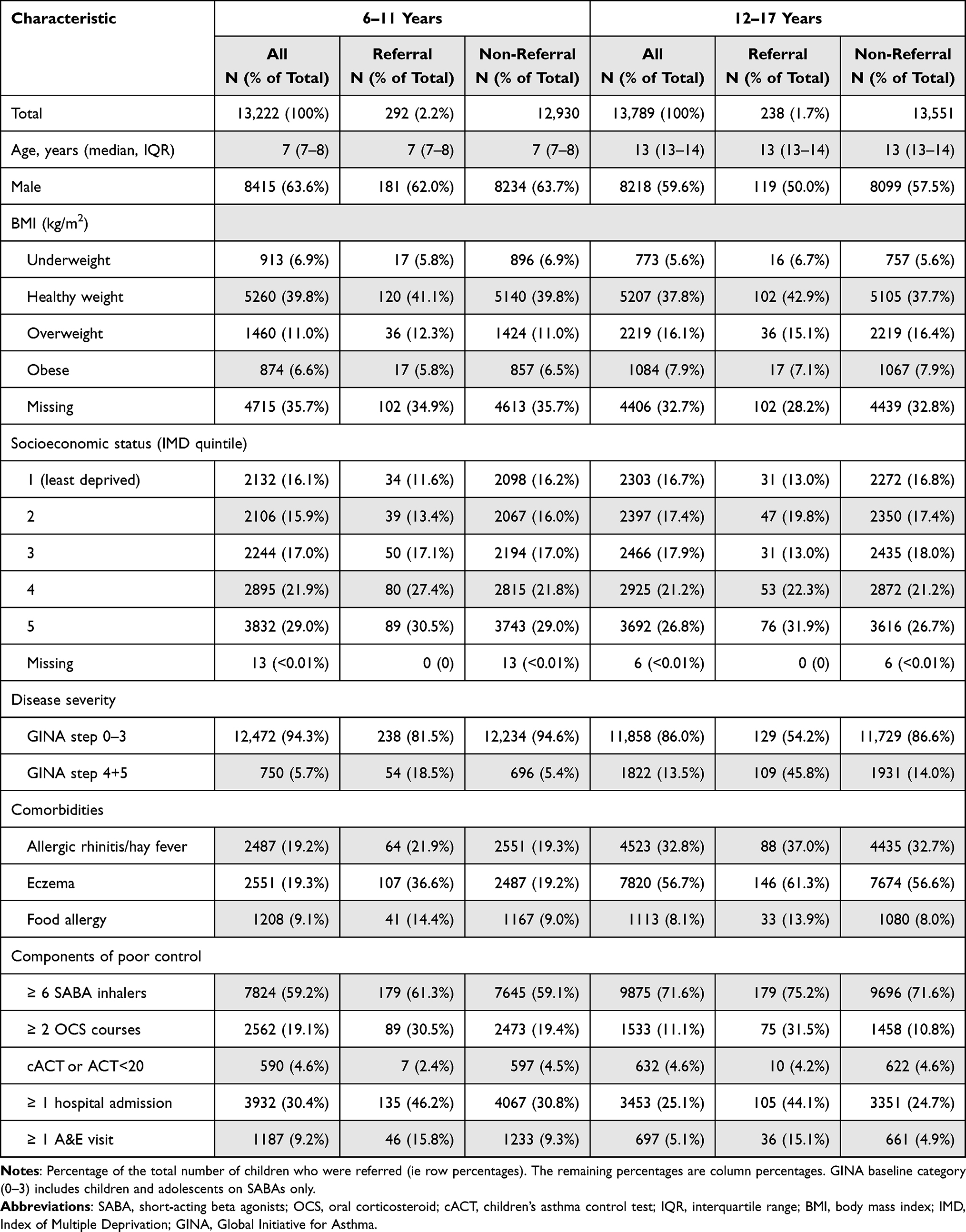 |
Table 3 Characteristics of Children and Adolescents with Poorly Controlled Asthma, by 12-Month Referral Status, by Age Cohort (6–11 and 12–17 Years) |
Among individuals with poor control, 12-month referral was strongly associated with disease severity even after adjustment for potential confounders [HRcrude = 4.04 (95% CI, 3.35–4.87); HRadj = 2.72 (95% CI: 2.13–3.49)] (Table 4). Univariable Cox models identified younger age, female gender, living in a more deprived area and concomitant presence of food allergy as possible factors which increased the likelihood of being offered specialist referral. However, after adjustment, only younger age, high level of deprivation and food allergy were found to be significantly associated with an increased hazard for 12-month referral (Table 4). Among the defining criteria for poor control, hospitalisation for asthma was the strongest predictor of a referral, after adjustment [HRcrude = 2.51 (95% CI, 1.97–3.19)].
 |
Table 4 Factors Associated with Referral to a Respiratory Specialist Among Children and Adolescents with Poorly Controlled Asthma (6–17 Years) |
Discussion
This analysis found that around 1 in 6 children and adolescents with active asthma are not achieving adequate control of their symptoms. Poor control was strongly associated with disease severity; those with more severe disease (ie, on GINA treatment steps 4 or 5), were nearly four times more likely to have poorly controlled asthma than those with mild-to-moderate asthma. Several studies have demonstrated that inadequate asthma control in the paediatric asthma patient population is associated with a substantially increased risk of poor outcomes. For example, the TENOR study demonstrated that children who have sustained poor control and severe asthma have a six times greater risk of being admitted to hospital for asthma-related episodes, or visiting A&E departments, than children with improved symptom control.13 Multiple studies have found an association between high numbers of SABA prescriptions and increased risk of exacerbations and asthma-related deaths.14,15 Another study identified that 50% of high school children in London have suboptimal asthma control as measured by the ACT score.16 Modifiable factors were found in more than 60% of children and young people (from 196 young people studied) that died due to asthma-related adverse episodes.17,18
Our study also revealed that among children and adolescents meeting our criteria for poor control, referral rates to specialist care were extremely low. Overall, only 2% were offered prompt referral for specialist treatment. While this proportion rose to 6.2% in children and adolescents with severe asthma – a four-fold increase relative to those with mild-to-moderate asthma (1.6%) – this suggests that there is considerable room for improvement in the management of asthma in this high-risk population.
In terms of potential risk factors for poor control, we found that, in addition to more severe disease, male gender, higher BMI, having an atopic condition (allergic rhinitis/hay fever, eczema or food allergies) and living in a more deprived area were associated with inadequate asthma control. In this respect, our findings are in keeping with other published research on this topic.19 Several studies conducted in children and adolescents have identified obesity as risk factor for not just poor symptom control but also an increased risk of developing asthma, worse outcomes and diminished quality of life. It is conceivable that some children who are more deprived also have increased BMI and are likely to engage less in outdoor leisure activities, partly due to associated costs. Findings from a systematic review suggest that weight loss of as little as 10% can improve asthma-related poor outcomes.20
Our finding of low referral rates to specialist care is also not unexpected and speaks to a continued unmet need for timely referral for those patients who are not achieving adequate control of their asthma. The UNTWIST study, which used data from 2007 to 2015, found that among patients eligible for referral to a respiratory specialist, only 4% received a specialist referral; moreover, referrals were often subject to long delays (median referral time, 880 days).21 This study found evidence that several established risk factors for poor control were also associated with referral times, most notably, the presence of atopic comorbidities. Having a food allergy in particular increased the odds of having poorly controlled asthma and increased the likelihood of a referral to a specialist. We also found some evidence to suggest that hospitalisation for asthma was strongly associated with a referral. Conversely, in this study, the absence of an atopic condition, older age and living in a more affluent area were associated with non-referral.
Our study has several strengths; the use of routinely collected data that are generalisable and validated case finding definitions. However, asthma diagnosis misclassification may have occurred. We also have not evaluated adherence to treatment in our study. High SABA use was evident in a high proportion of the cohort, and this could reflect poor adherence to therapy in part of the population. One of the criteria for defining poor control used in our cohort was cACT or ACT scores with values lower than 20. Asthma control questionnaires usually focus on the most accurate recall period (gathers symptom information from the previous four weeks). Therefore, we do not overestimate the possible effect that more available information on cACT data records would have had on the results of our study. However, these data were not available in everyone with asthma. Our defining criteria for referral to a respiratory specialist could be another limitation of our study as we did not include codes for general paediatric referral. We did not use other eligibility criteria suggested by GINA guidelines, such as diagnostic uncertainty or the presence of other complications.12 Thus, we might have underestimated the paediatric asthma frequency within primary care records.
Conclusion
We have shown that among the UK paediatric asthma population, a high proportion of children and young people continue to have poor symptom control, especially in the more severe asthma group and that among patients who are at risk for poor asthma outcomes, the referral rates to specialist care are still meagre. We have also shown that among patients with poor control, 12-month referral was associated with disease severity, being female, younger age, high level of deprivation and food allergy. This group of patients with these risk factors represents the at-risk paediatric population for whom specialist assessment can help to identify potentially modifiable factors leading to improved control and characterise those who might be eligible for novel biological therapies.
Data Sharing Statement
This study used existing data from the UK CPRD electronic health record database, this data resource is accessible only to researchers with protocols approved by the CPRD’s independent scientific advisory committee; therefore, no additional unpublished data are available. All data management and analysis computer code are available on request from the corresponding author.
Linked pseudonymised mortality data from the Office for National Statistics (ONS), socioeconomic data from the Index of Multiple Deprivation (IMD), and secondary care data from Hospital Episode Statistics (HES) were provided for this study by CPRD for patients in England. Data is linked by NHS Digital, the statutory trusted third party for linking data, using identifiable data held only by NHS Digital. Select general practices consent to this process at a practice level, with individual patients having the right to opt-out. Use of HES and ONS data is Copyright © (2018), re-used with the permission of The Health & Social Care Information Centre, all rights reserved.
Data are available on request from the CPRD. Their provision requires the purchase of a license, and this license does not permit the authors to make them publicly available to all. This work used data from the version collected in October 2020 and have clearly specified the data selected in the Methods section. To allow identical data to be obtained by others, via the purchase of a license, the code lists have been provided on GitHub. Licenses are available from the CPRD (http://www.cprd.com): The Clinical Practice Research Datalink Group, The Medicines and Healthcare products Regulatory Agency, 10 South Colonnade, Canary Wharf, London E14 4PU.
Acknowledgments
ConstantinDeos Kallis and Ann Morgan are co-first authors for this study. We would like to acknowledge Carmen Amarfei for her input in early manuscript drafts.
Authors and Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
AM and CK have nothing to declare. JKQ reports grants from AUK-BLF, Asthma+Lung UK, MRC, The Health Foundation, Health Data Research UK; grants and personal fees from AZ, BI, GSK, Bayer, grants from Chiesi, outside the submitted work. LF reports grants from AUK, NIHR and personal fees from AZ, Sanofi, Novartis and GSK outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Asher I, Pearce N. Global burden of asthma among children. Int J Tuberc Lung Dis. 2014;18(11):1269–1278. doi:10.5588/ijtld.14.0170
2. Buelo A, McLean S, Julious S, et al.; ARC Group. At-risk children with asthma (ARC): a systematic review. Thorax. 2018;73(9):813–824. doi:10.1136/thoraxjnl-2017-210939
3. De Keyser HH, Szefler S. Asthma attacks in children are always preceded by poor asthma control: myth or maxim? Breathe. 2020;16(3):200169. doi:10.1183/20734735.0169-2020
4. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2022. Available from: https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022-FINAL-22-07-01-WMS.pdf.
5. Dharmage SC, Perret JL, Custovic A. Epidemiology of asthma in children and adults. Front Pediatr. 2019;7:246. doi:10.3389/fped.2019.00246
6. Haselkorn T, Zeiger RS, Chipps BE, et al. Recent asthma exacerbations predict future exacerbations in children with severe or difficult-to-treat asthma. J Allergy Clin Immunol. 2009;124(5):921–927. doi:10.1016/j.jaci.2009.09.006
7. Mogensen I, Hallberg J, Ekström S, Bergström A, Melén E, Kull I. Uncontrolled asthma from childhood to young adulthood associates with airflow obstruction. ERJ Open Res. 2021;7(4):00179–2021. doi:10.1183/23120541.00179-2021
8. Royal College of Physicians. Why asthma still kills: the National Review of Asthma Deaths (NRAD) confidential enquiry report; London; 2014. Available from: https://www.rcplondon.ac.uk/file/868/download.
9. Price D, Bjermer L, Bergin DA, Martinez R. Asthma referrals: a key component of asthma management that needs to be addressed. J Asthma Allergy. 2017;10:209–223. doi:10.2147/JAA.S134300
10. Wolf A, Dedman D, Campbell J, et al. Data resource profile: Clinical Practice Research Datalink (CPRD) aurum. Int J Epidemiol. 2019;48(6):1740–1740g. doi:10.1093/ije/dyz034
11. Nissen F, Morales DR, Mullerova H, Smeeth L, Douglas IJ, Quint JK. Validation of asthma recording in the Clinical Practice Research Datalink (CPRD). BMJ Open. 2017;7(8):e017474. doi:10.1136/bmjopen-2017-017474
12. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2020. Available from: https://ginasthma.org/wp-content/uploads/2020/06/GINA-2020-report_20_06_04-1-wms.pdf.
13. Haselkorn T, Fish JE, Zeiger RS, et al.; TENOR Study Group. Consistently very poorly controlled asthma, as defined by the impairment domain of the expert panel report 3 guidelines, increases risk for future severe asthma exacerbations in The epidemiology and natural history of asthma: outcomes and Treatment Regimens (TENOR) study. J Allergy Clin Immunol. 2009;124(5):895–902.e1–4. doi:10.1016/j.jaci.2009.07.035
14. Nwaru BI, Ekström M, Hasvold P, Wiklund F, Telg G, Janson C. Overuse of short-acting β2-agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programme. Eur Respir J. 2020;55(4):1901872. doi:10.1183/13993003.01872-2019
15. Bloom CI, Nissen F, Douglas IJ, Smeeth L, Cullinan P, Quint JK. Exacerbation risk and characterisation of the UK’s asthma population from infants to old age. Thorax. 2018;73(4):313–320. doi:10.1136/thoraxjnl-2017-210650
16. Harris K, Mosler G, Williams SA, Whitehouse A, Raine R, Grigg J. Asthma control in London secondary school children. J Asthma. 2017;54(10):1033–1040. doi:10.1080/02770903.2017.1299757
17. Carroll W, Clayton S, Frost S, et al. If it’s ‘only’ asthma, why are children still dying? Arch Dis Child. 2020;105(5):494–498. doi:10.1136/archdischild-2019-318215
18. Levy ML. The national review of asthma deaths: what did we learn and what needs to change? Breathe. 2015;11(1):14–24. doi:10.1183/20734735.008914
19. Robinson DS, Campbell DA, Durham SR, Pfeffer J, Barnes PJ, Chung KF; Asthma and Allergy Research Group of the National Heart and Lung Institute. Systematic assessment of difficult-to-treat asthma. Eur Respir J. 2003;22(3):478–483. doi:10.1183/09031936.03.00017003
20. Okoniewski W, Lu KD, Forno E. Weight loss for children and adults with obesity and asthma. A systematic review of randomized controlled trials. Ann Am Thorac Soc. 2019;16(5):613–625. doi:10.1513/AnnalsATS.201810-651SR
21. Blakey JD, Gayle A, Slater MG, Jones GH, Baldwin M. Observational cohort study to investigate the unmet need and time waiting for referral for specialist opinion in adult asthma in England (UNTWIST asthma). BMJ Open. 2019;9(11):e031740. doi:10.1136/bmjopen-2019-031740
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.