Back to Journals » Clinical Optometry » Volume 16
Prevalence of Ocular Morbidity and Associated Factors Among Hearing Impaired Children at Embangweni School of the Deaf in Mzimba District, Malawi
Authors Liyo T, Ogbonna GO, Mzumara T ![]() , Ezinne NE
, Ezinne NE ![]()
Received 28 November 2023
Accepted for publication 25 April 2024
Published 3 May 2024 Volume 2024:16 Pages 115—122
DOI https://doi.org/10.2147/OPTO.S444216
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Tambuzai Liyo,1 Grace Obumneke Ogbonna,1 Thokozani Mzumara,1,2 Ngozika Esther Ezinne3
1Department of Optometry, Mzuzu University, Mzuzu, Malawi; 2Department of Ophthalmology, Mzimba North District Hospital, Mzimba, Malawi; 3Optometry Unit, Department of Clinical Surgical Sciences, University of the West Indies, Saint Augustine Campus, Saint Augustine, Trinidad and Tobago
Correspondence: Grace Obumneke Ogbonna, Department of Optometry, Mzuzu University, P/Bag 201, Mzuzu, Malawi, Email [email protected]
Purpose: To assess the prevalence of ocular morbidities and associated factors among hearing-impaired (HI) students at the Embangweni School for the Deaf in Mzimba, Malawi.
Methods: This was an institutional cross-sectional study of HI students at Embangweni School for the Deaf. A series of optometric and audiometric tests was performed, and the results were exported to the Statistical Package for Social Science for statistical analysis (SPSS) version 25. Pearson’s chi-square test was used to assess correlations and associations between variables. A P-value less significance was set at p < 0.05.
Results: A total of 147 children comprising of 76 (51.7%) males and 71 (48.3%) females participated in this study. The prevalence of ocular conditions and visual impairment was 39 (26.5%) and 2 (1.4%), respectively. The Prevalence of eye disease was significantly associated with male sex (p=0.02) and type of HI (p=0.031). Allergic conjunctivitis 36 (24.5%) was the most common ocular condition, followed by refractive error 28 (19%).
Conclusion: The prevalence of ocular conditions among HI students was significant and associated with sex. Regular school vision screening of students with HI is highly advised to reduce the burden of visual impairment.
Plain Language Summary: Hearing impairment places a great burden on the sufferers. Ocular conditions among this population further disadvantages them in terms of education and personal development. The current study evaluated the prevalence of ocular conditions among school children at the Embangweni School of the Deaf. We observed that there is high prevalence of eye conditions among this population which was more prevalent among the males. Conjunctivitis was the most prevalent ocular condition. There is a great need for regular vision screening for this population for early detection and management of ocular conditions among them.
Keywords: child health, hearing impairment, ocular morbidity, special education, vision screening, visual impairment
Introduction
Hearing is an essential aspect of human communication. Hearing impairment (HI) at any stage of life can compromise communication and influence an individual’s quality of life.1 Hearing loss occurs when a person is unable to hear sounds of different intensities.2 Hearing disability can be acquired or congenital, and may be classified as conductive or sensorineural.3 Hearing impairment during childhood can cause delays in the development of speech, language, and cognition, which may later lead to educational and social isolation, and ultimately economic disadvantages.4
The majority of individuals with HI reside in developing regions of South Asia, Asia Pacific, and Sub-Saharan Africa.5 In Africa, Malawi has one of the highest numbers of individuals with HI.6,7 For example, the prevalence of childhood HI is 11.5%.6,7
Visual and hearing senses combined account for 95% information acquisition.8 Hence, Deaf children rely on their sense of vision to interact with the world.9 Individuals with HI use vision to compensate for auditory information,10,11 and hearing impairment can negatively impact their quality of life and social and academic performance; hence, a sense of vision compensates for these effects.12,13 Blindness caused by various ocular diseases poses a major threat to people with HI.14
Ocular disorders, such as refractive errors and cataracts, are common in HI.15,16 Prevalence of ocular morbidity among HI has been reported in various studies.15–17 No study has been done in Malawi. Therefore, this study aimed to determine the prevalence of ocular morbidity and visual impairment in patients with HI response.
Materials and Methods
Research Design
This was a cross-sectional institution-based study of hearing-impaired children at Embangweni Primary School for the Deaf. The research was conducted from 22nd to 25th of November 2021.
Study Population and Setting
The study was conducted among school children enrolled in Embangweni Primary School for the Deaf (a.k.a. Embangweni School for the Hard of Hearing). Embangweni School for the deaf is one of the three schools of the deaf in the Northern Region of Malawi. It is located 47 km south of Mzimba in Northern Malawi. The Mzimba District is the largest district in the country, covering approximately 10,430 square kilometers, with a total population of 6109. The school has about 201 deaf learners registered, and the age range from 6 years to 24 years. Almost all the pupils’ board at the school as its catchment area is large. It has Classes which include Preschool 1, 2 and 3 and Classes (Standards) 1–9. Malawi schools usually go up to Standard 8, but due to its peculiarity (deaf students) an extra year was added. Because of the school’s proximity to Embangweni hospital which has an audiology department, all of the students have baseline results audiometry results.
Study Sampling Technique and Sample Size
Embagwani School of the deaf was selected for this school because of its proximity to the researchers. All registered students who consented to participate in this study were included. Those who at the time of the exam were absent from the school, sick or on drugs such as lignocaine that can cause fainting or tremors were excluded to avoid disruptions in ocular measurements.
Sample Size
All students who were diagnosed with deafness and are registered students in the school were eligible to participate in the study. Hence, no sample size was used.
Data Collection Procedures
Participant’s information on socio-demographics such as date of birth, sex and position in the family were obtained from the participants with the help of the schoolteachers. Similarly, their medical history such as age of onset of hearing defects, cause of hearing defects, presence of existing systemic disease and audiometry result was also obtained from their records in the school. Ocular history such as any known diseases, ocular trauma, previous eye surgery and/or eye patching were also inquired. Pupil’s health passports were reviewed to ensure that an upto date medical and ocular history of participants were gotten. Subsequently, the tuning forks test was performed (which is a pure tone test that tests for the intensity and tone of sounds) by the audiologist to determine the cause, type, and severity of the participant’s hearing impairment. Further, an audioscope was used to view the ears by the audiologist.
Two optometrists performed the eye examinations including visual acuity, external eye examination, objective refraction using retinoscope (Heinz retinoscope), and intraocular pressure measurement. Visual acuity was measured using a LogMAR chart at 4meters. Subsequently, the external eye examination was done using Haag Streit Slit Lamp biomicroscope. Intraocular measurement was done with I care rebound Tonometer. One ophthalmologist performed the dilated fundus examination using a Volks lens (90D) following the topical dilatation with a combination of 0.5% tropicamide and 2.5% phenylephrine. To ensure adequate communication, teachers who were conversant with the Malawian sign language were trained as support staff for the various stations and examinations. A child psychologist was present to observe the process and each child’s response to ensure that none of the students was in anyway traumatized by the study.
Definition of Terms
Myopia and hyperopia were defined as −0.5 Diopters and ≥+1.00 D respectively. Astigmatism was regarded as −0.50 D cyl. On the other hand, ocular morbidity was defined as both visually impairing and non-visually impairing conditions seen among the study population. Similarly, hearing impairment was defined as any problem or damage to one or more parts of the hearing mechanism.
Ethical Consideration
Ethics was obtained from the Faculty of Health Sciences, Research and Ethics Committee of the Mzuzu University Malawi (FOHS/REC/21/107). Permission to conduct the study in the school was obtained from the Ministry of Education and principal of the school. Written informed consent was obtained from all participants and their parents or care givers. Assent was obtained from children less than 18 years. The study adhered to the declaration of Helsinki.
Data Analysis
The data were entered into the “Statistical Package for Social Science (SPSS) software” version 22 and Microsoft Excel 2016. Descriptive statistics were employed during data analysis to generate frequencies, percentages, and measures of central tendency (mean, and median) as well as standard deviation. The data are illustrated using tables and figures. Independent T-test was used to test for the statistical differences between the mean age of male and female participants. Inferential statistics employing Bivariate Analysis using the chi-square test were used to determine the association between the prevalence of ocular morbidities and sex, age categories, level of HI, and type of HI. In accordance to the study by Hollingsworth et al, the subjects were classified into different groups based on the severity or level of their hearing impairment as (mild [20–40 dB], moderate [41–70 dB], severe [71–95 dB], and profound [> 95 dB]. On the type of hearing loss we classified as sensorineural, conductive and mixed hearing loss. In addition, we employed independent t test to assess differences between groups. Statistical significance was set at P level of less than 0.05.
Results
Demography
Out of 201 students enrolled at the school, 147 students were readily available at the facility during the study. Out Of 147 that participated in this study, 76 were males (51.7%) and 71 were females (48.3%) (Table 1). The mean age of the participants was 14.3 ±4.6 years ranging from 6 to 24 years old. Males had a mean age of 14.5 ± 4.5, while females had 14.3 ± 4.7. An independent t-test showed that this difference was not statistically significant (P=0.62). The Majority of the participants belonged to the age group of 16–20 years 56 (38.1%). According to type of HI, approximately 98 (66.7%) of the deaf children were congenital, while 49 (33.3%) were acquired. Based on severity, most of the students (93.2%) had profound hearing impairment, with only 5 (3.4%) and 2 (1.4%) having moderate and mild hearing impairments, respectively. Based on gender, 68 (89.5%) males had profound HI than females. Nevertheless, the Pearson chi square test showed no association between gender and level of HI (P=0.42).
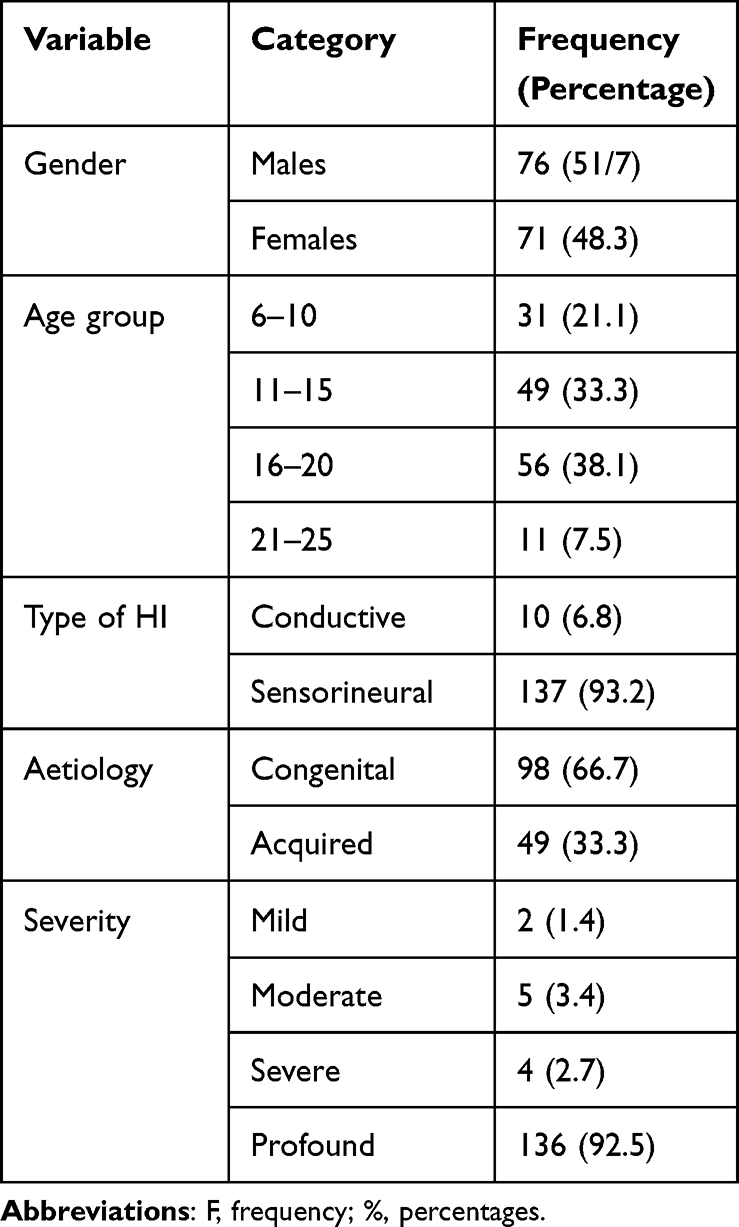 |
Table 1 Characteristics of Study Participants |
Prevalence of Ocular Morbidity
The prevalence of ocular morbidity was 39 (26.5%). The most common ocular morbidity was Glaucoma 18 (46.2%) followed by Vernal Kerato Conjuctivitis (VKC) 7 (17.9%) and bacteria conjuctivitis 3 (7.7%). (Figure 1).
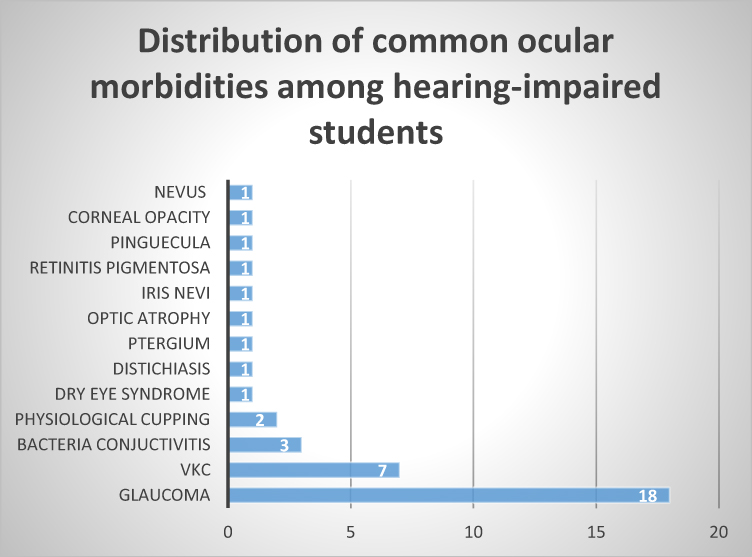 |
Figure 1 Distribution of ocular diseases. |
Associated Factors of Prevalence of Ocular Morbidity
A chi-squared test was performed to determine whether there was a statistically significant association between the prevalence of ocular conditions and the variables in the study. A significant association was observed between sex (p=0.02) such that more males (26 (34.2%) than females 13 (18.3%) had eye condition. The study found no association between prevalence of ocular morbidity and age group (p=0.806), level of HI (p=0.318), and HI etiology (p=0.234). However, the Pearson Chi square test showed that the association between ocular condition and type of HI was statistically significant (p=0.031) (Table 2).
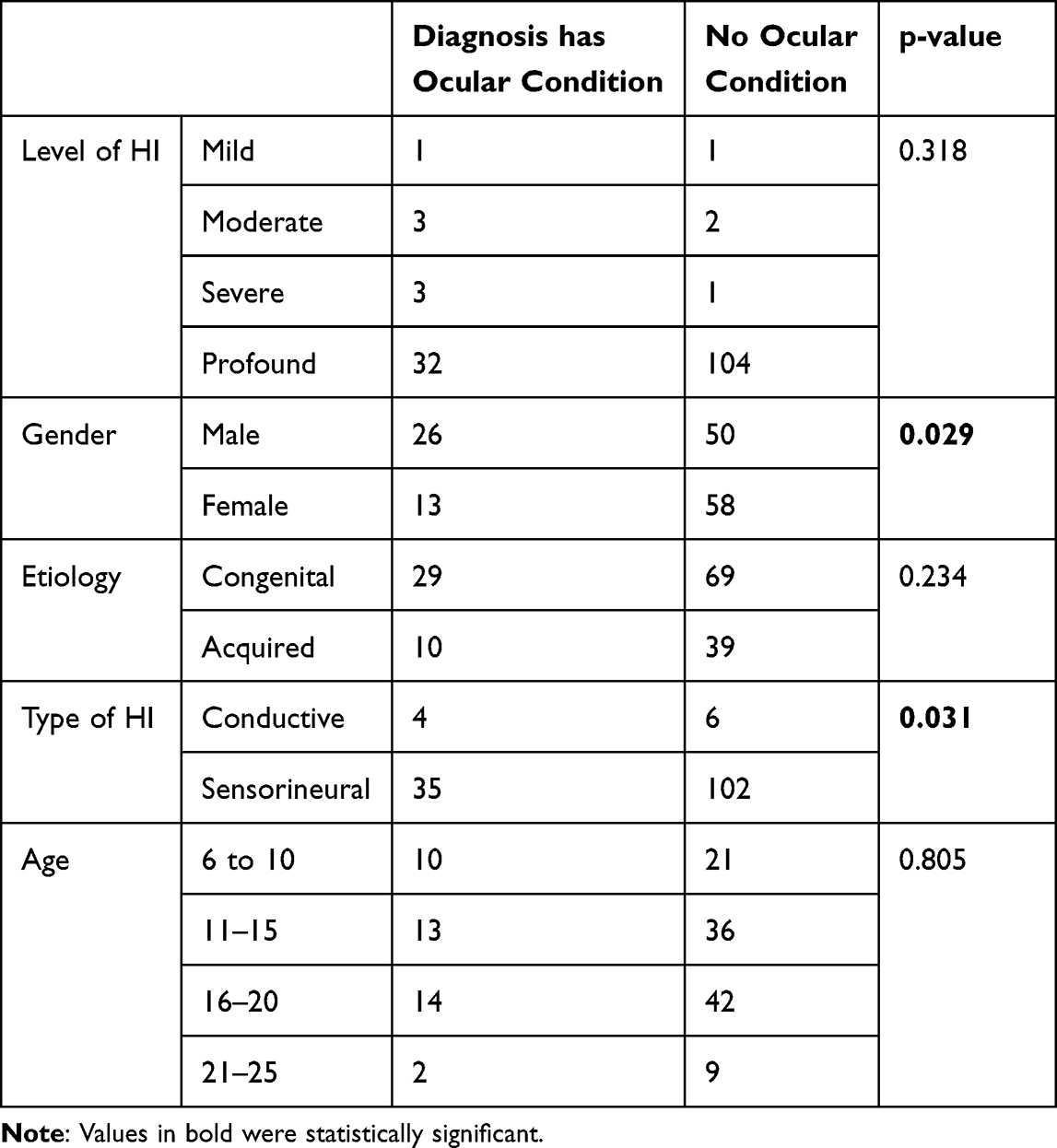 |
Table 2 Factors Associated with the Prevalence of Ocular Conditions |
Discussion
The current study assessed the prevalence of ocular morbidities among hearing-impaired children enrolled at the Embangweni School of the Deaf in the Mzimba District, Malawi. The study observed more male enrollment. Similarly, more male participants had ocular morbidities than their female counterparts did. The male preponderance was found to be statistically significant. In contrast, other factors, such as the type of hearing impairment, severity, and nature of onset, were observed to have no role in the prevalence of ocular morbidities in this population.
In this study, the age range was 6–25 years, similar to that in a previous report in Nigeria.18 However, the age range was narrower than what was reported in other studies including a study among HI people in a vocational and technical training center.14 The wide age range of primary school-going children can be attributed to delays in school enrolment due to hearing impairment. This derails academic progress for this group since they lack access to special needs education and there is an obvious prevalence of societal discrimination against them.11,16,19 In Malawi, children with disabilities face systematic barriers to attending, progressing, and learning in schools.20 For instance about 27% of HI children in Malawi are not enrolled in schools for formal education.6 Although the Malawi government has shifted its focus from special education systems to inclusive education systems, the integration process remains muddled, as access to mainstream education is limited for this group owing to the lack of trained special-needs specialists in the primary school education system.21
In addition, the study observed that there were more males than females enrolled in special schools, similar to previous studies.9 This reflects the gender inequality in access to education in the country. This may also imply that more males are affected by hearing impairment than females. This study also noted a male preponderance in the occurrence of ocular morbidities in the study population. This is similar to the reports from other studies which observed that the male gender was more affected by ocular morbidities compared to their female counterparts.22 It is noteworthy that the male population, may be more likely to be involved in outdoor recreational and sporting activities,23,24 thereby exposing themselves to allergens in the environment, which may be a source of certain ocular morbidities such as allergic conjunctivitis.
In this study, the main (etiology) nature of onset of HI was congenital. This finding is consistent with the results of previous studies.9 It also highlights the need for early eye and ear screening in children as early detection remains the mainstay of clinical management, social integration, and educational interventions. Such screenings could be integrated into primary health centers through the training of nurses on how to identify such cases during vaccination exercises, which are a part of the early care services provided to children.
Furthermore, the current study observed that the majority of participants had sensorineural hearing impairment. This agrees with the findings of Vargas-Díaz and Neira-Torres, who found sensorineural impairment to be the primary cause of HI among children in Colombia,25 and contradicts the study by Ferrite et al, who observed unknown or conductive HI to be more prevalent among their study participants in Cameroon.26 Sensorineural impairment has been shown to be associated with the occurrence of neurological disorders,27 some of which can affect vision.
In this study, the majority of participants had profound HI. However, the current study found no association between the severity of HI and ocular morbidities. These findings contradict those reported by Mulwafu et al, who observed a lower prevalence of profound hearing impairment in children.6 The differences in the study results could be due to the study population, while the current study was conducted in the school for the deaf, the study by Mulwafu et al was a community-based study. The presence of profound HI places a great demand on other senses, especially vision, as they try to compensate for sensory loss. Therefore, the presence of any blinding ocular condition is devastating as it could further hinder their education and personal development. Hence, the lack of association between ocular morbidities and hearing impairment among this population highlights an opportunity at better development and adaption. Nonetheless, it is important to ensure regular eye screenings, as this would guarantee early detection and management of any visually impairing condition.
The prevalence of eye conditions in this study was higher than that reported in India.9 However, in Nepal, it was reported slightly lower (23%).17 The variation in the results can be explained by the differences in study populations between the two studies. The higher prevalence of eye comorbidities observed in this study points to the need for conceited efforts in ensuring increased access and utilization of eye care services among children with HI in Malawi. A study on the utilization of eye care services among children elsewhere found that this group had suboptimal eye care service utilization levels.28 The current study did not assess the utilization of eye care services; however, In Malawi, access to health services among people with disabilities is significantly hindered by financial, practical, and social barriers.29 Accordingly, a recent study found that access to healthcare among people with disabilities in Malawi is heavily influenced by their ability to reach, pay, and engage with services. Although eye care services are provided freely at the point of access as part of the Essential Health Package, Malawians still incur transportation costs.30 Therefore, this study highlights the role of outreach eye screening programs in high-risk population groups.31,32
Elsewhere, the most common ocular problem was refractive error.14,17 (Kwarteng et al, 2022) in contrast, the most common ocular morbidity in our study was glaucoma. Glaucoma is the leading cause of irreversible blindness. It is also known to affect people of black racial descent disproportionately. As such its high prevalence among this population emphasizes the need for regular eye test and integrated school eye health program within the population. The results of our review also showed VKC as common among the study participants. We suspected that the high prevalence of allergic conjunctivitis could in part be due to environmental factors such as the presence of dust and flowering trees at the study centre. As such, there is need for the identification, removal/ and avoidance of possible environmental triggers in the school. Although, refractive errors have been described as one of the leading causes of visual impairment worldwide,33,34 uncorrected refractive error was not found to be prevalent in the study population. This is inconsistent with other studies that found refractive errors to be common in individuals with HI.9
Limitations
The study is not without drawbacks. A significant weakness and limitation of the study was that due to limited resources, the refractions were conducted without adequate cycloplegia which could underestimate hyperopia. Another significant weakness was that the prevalence of refractive error and ocular comorbidities in HI children were not compared to non-HI children from Malawi. Further, the study did not assess the magnitude of visual impairment among the study population.
Conclusion
The prevalence of ocular conditions among HI students in Malawi is high and it is significantly associated with male sex and type of HI, however it was not associated with the severity of HI. Regular school vision screening of students with HI is highly advised to reduce the burden of visual impairment.
Institutional Board Statement
Ethics was obtained from the Faculty of Health Sciences, Research and Ethics Committee of the Mzuzu University Malawi (FOHS/REC/21/107). Permission to conduct the study in the school was obtained from the Ministry of Education and principal of the school. Written informed consent was obtained from all participants and their parents or care givers. Assent was obtained from children less than 18 years. Information about the study and reason to participate in the study was explained to all participants prior to data collection. Participants were informed about their right to discontinue or refuse to participate in the study at any time or stage. The study adhered to the declaration of Helsinki.
Data Sharing Statement
The dataset is available upon request from the corresponding authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The data collection for this study was funded by outreach funds from Canadian Vision Care (CVC).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ramma L, Sebothoma B. The prevalence of hearing impairment within the cape town metropolitan area. South African J Commun Disord. 2016;63(1):1–10. doi:10.4102/sajcd.v63i1.105
2. Busenbarrick H, Davenport KL. Music to our ears: are dancers at risk for high sound level exposure. Med Probl Perform Art. 2020;35(4):227–232. doi:10.21091/mppa.2020.4033
3. Zahnert T. Differenzialdiagnose der schwerhörigkeit. Dtsch Arztebl. 2011;108(25):433–444.
4. Lang-Roth R Hearing impairment and language delay in infants: diagnostics and genetics. GMS Curr Top Otorhinolaryngol Head Neck Surg; 2014. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25587365%0Ahttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC4273166.
5. World Health Organization. Addressing The Rising Prevalence of Hearing Loss. Geneva, Switzerland: World Health Organization; 2018:655–658. Available from: https://apps.who.int/iris/handle/10665/260336.
6. Mulwafu W, Tataryn M, Polack S, Viste A, Goplen K, Kuper H. Children with hearing impairment in Malawi, a cohort study. Bull World Heal Organ. 2019;97:5.
7. Hunt L, Mulwafu W, Knott V, et al. Prevalence of paediatric chronic suppurative otitis media and hearing impairment in rural Malawi: a cross-sectional survey. PLoS One. 2017;12(12):1–12. doi:10.1371/journal.pone.0188950
8. Abikoye TM, Aribaba OT, Musa KO, Idowu OO. Prevalence and causes of visual impairment among hearing impaired students in Lagos, Nigeria. Int J Pediatr Otorhinolaryngol. 2020;139:110487. doi:10.1016/j.ijporl.2020.110487
9. Pehere NK, Khanna RC, Marlapati R, Sannapaneni K. Original Article Prevalence of ophthalmic disorders among hearing ‑ impaired school children in Guntur district of Andhra Pradesh. Indian J Ophthalmol. 2019;5:530–535.
10. Bist J, Adhikari P, Sharma AK. Ocular morbidity in hearing impaired schoolchildren. Child Care Health Dev. 2011;37(3):394–397. doi:10.1111/j.1365-2214.2010.01137.x
11. Marschark M, Morrison C, Lukomski J, Borgna G, Convertino C. Are deaf students visual learners? Learn Individ Differ. 2013;25:156–162. doi:10.1016/j.lindif.2013.02.006
12. Rahmah DN, Widodo APA, Sihadi M. The learning of musical art for students with visual impairement. In: 2nd INDOEDUC4ALL-Indonesian Education for All (INDOEDUC 2018), Atlantis Press. 2018;272:216–218.
13. Thangavelu K, Martakis K, Feldmann S, Roth B, Lang-Roth R. Referral rate and false-positive rates in a hearing screening program among high-risk newborns. Eur Arch Oto-Rhino Laryngol. 2023;280(10):4455–4465. doi:10.1007/s00405-023-07978-y
14. Kwarteng MA, Mashige KP, Kyei S, Sunkwa D, Dogbe Q, Govender-poonsamy P. Prevalence and causes of visual impairment amongst hearing impaired school-going children in sub-Saharan Africa: a scoping review. African Health Sci. 2022;22(4):199–204. doi:10.4314/ahs.v22i4.24
15. Zaheer H, Parameswarappa D, Zaheer M, Chhablani J, Patil-Chhablani P. Ocular manifestations in patients with sensorineural hearing loss. J Ophthalmic Vis Res. 2022. doi:10.18502/jovr.v17i4.12321
16. Majekodunmi O, Olusanya B, Oluleye T. Pattern of ocular abnormalities among students attending schools for the hearing impaired in Ibadan, South-West Nigeria. Niger J Ophthalmol. 2018;26(1):24. doi:10.4103/njo.njo_38_17
17. Dhungana AP. Ocular morbidity in hearing impaired school children in Eastern Nepal. J Kathmandu Med Coll. 2014;3(1):4–7. doi:10.3126/jkmc.v3i1.10916
18. Onakpoya OH, Omotoye OJ. Screening for ophthalmic disorders and visual impairment in a Nigerian school for the deaf. Eur J Ophthalmol. 2010;20(3):596–600. doi:10.1177/112067211002000310
19. Wezzie Khomera S, Fayiah M, Gwayi S. Challenges faced by learners with hearing impairments in a special school environment: a case study of embangweni primary school for the deaf, Mzimba District, Malawi. World J Vocat Educ Train. 2020;2(1):21–36. doi:10.18488/journal.119.2020.21.21.36
20. Banks LM, Hunt X, Kalua K, Nindi P, Zuurmond M, Shakespeare T. ‘I might be lucky and go back to school’: factors affecting inclusion in education for children with disabilities in rural Malawi. African J Disabil. 2022;11:1–12. doi:10.4102/ajod.v11i0.981
21. Kawaguchi J, Kuroda K. Diffusion of inclusive education in Malawi. Sustain Dev Goals Diffus Contestation Asia Eur. 2022;9781003205:86–97.
22. Getahun A, Abayo G, Gessesse GW, Asaminew T. Prevalence and pattern of ocular morbidity among school children in Southern Ethiopia. Ethiopian J Health Sci. 2021:31:2–7.
23. Kling KG, Kling KG, Margaryan L, Fuchs M. (In) equality in the outdoors: gender perspective on recreation and tourism media in the Swedish mountains (In) equality in the outdoors: gender perspective on recreation and tourism media in the Swedish mountains. Curr Issues Tour. 2018;1–15. doi:10.1080/13683500.2018.1495698
24. Rahman MWA, Amirul M, Shaari A, et al. Comparison of Participation Motives in Outdoor Recreation Activities Between Genders of Kelab Rekreasi UiTM Malaysia (KRESMA) Members Comparison of Participation Motives in Outdoor Recreation Activities Between Genders of Kelab Rekreasi UiTM Malaysia. World Leisure J. 2022;1(10):1069–1076.
25. Vargas-Díaz EJ, Neira-Torres LI. The prevalence of hearing loss in children in Colombia. Rev Fac Med. 2014;62(4):529–538. doi:10.15446/revfacmed.v62n4.43955
26. Ferrite S, Mactaggart I, Kuper H, Oye J, Polack S. Prevalence and causes of hearing impairment in Fundong Health District, North-West Cameroon. Trop Med Int Heal. 2017;22(4):485–492. doi:10.1111/tmi.12840
27. Li S, Cheng C, Lu L, et al. Hearing Loss in Neurological Disorders. Front Cell Dev Biol. 2021;9:1.
28. Majekodunmi OI, Olusanya BA, Oluleye TS. Utilization of eye care services among students attending schools for the hearing impaired in Oyo State, South-West Nigeria. Ann Ibadan Postgrad Med. 2019;17(2):181–186.
29. Harrison JAK, Thomson R, Banda HT, et al. Access to health care for people with disabilities in rural Malawi: what are the barriers? BMC Public Health. 2020;20(1):1–17. doi:10.1186/s12889-020-08691-9
30. Banda O, Mzumara T, Ogbonna G. The burden of ocular morbidities among elderly patients visiting a district healthcare facility in Malawi: a retrospective study. Heal Sci Rep. 2023;6:6.
31. Trotignon G, Engels T, Ali SS, et al. Measuring equity of access to eye health outreach camps in rural Malawi. PLoS One. 2022;17(5):1–16. doi:10.1371/journal.pone.0268116
32. Munthali AC, Tsoka M, Mvula P, Milner J. A situation analysis of children with disabilities in Malawi. Univ Malawi Cent Soc Res. 2013;2:1–45.
33. Dandona R, Dandona L. Refractive error blindness. Bull World Health Organ. 2001;79(3):237–243.
34. World Health Organization. Key Facts: blindness and vision impairment. World Health Organization. 2021;11:5–9.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.