Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Prevalence of Milk Teeth Extraction and Enabling Community Factors Among Under Five-Year-Old Children in Alle Special Woreda, SNNPR, Ethiopia, 2022: Community-Based Cross-Sectional Study; Based on Theory of Planned Behavior Model
Authors Otayto K ![]() , Godana W
, Godana W ![]() , Feleke T, Hussen S
, Feleke T, Hussen S ![]() , Alemu M
, Alemu M ![]()
Received 10 March 2022
Accepted for publication 23 June 2022
Published 1 July 2022 Volume 2022:13 Pages 257—269
DOI https://doi.org/10.2147/PHMT.S365768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Kusse Otayto, Wanzahun Godana, Tesfaye Feleke, Sultan Hussen, Mathewos Alemu
School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Kusse Otayto, Email [email protected]; [email protected]
Background: Milk tooth extraction (MTE) is one of the most common harmful traditional practices performed by traditional healers without anesthesia and unsterile materials. The acute and chronic complications of this practice greatly affect the health of children. In order to develop effective preventive measures towards this harmful practice, the extent of the problem and factors contributing to the practice should be verified. The objective of this study was to assess the prevalence and associated factors of MTE among under five-years-old children in Alle special Woreda.
Methods: A community-based cross-sectional survey was undertaken at Alle Special Woreda among 363 women using a multi-stage stratified sampling method. Data was collected using semi-structured questionnaires and data entry was done with Epi-data version 4.4.3.1, while data management and analysis were done with STATA version 14.0. Univariate and multivariate binary logistic regression models were used while model’s fitness was checked by Hosmer and Lemeshow test. Variables having a p-value of less than 0.05 were declared statistically significant in the final model.
Result: Milk teeth extraction was practiced on 58.68% (95% CI:0.5,0.6) of children. Age of the child less than 12 months, AOR:1.27 (95% CI:1.02,1.6), maternal occupation (housewife) AOR:1.3 (95% CI:1.04,65), paternaleducational, level (illiterate) AOR:1.4 (95% CI:1.2,1.9), residence (rural) AOR:3.6 (95% CI:1.08,12.4), positive attitude AOR:1.65 (95% CI:1.01,2.8) and intentions AOR: 1.82 (95% CI:1.1,3.3) towards MTE practice showed statistically significant association with MTE practice.
Conclusions and Recommendations: It was found that milk teeth extraction practice was the most common practice in the study area, with a prevalence of 58.68%. Age of the child, maternal occupation, paternal educational level, residence, having a positive attitude and intentions toward MTE practice all had a statistically significant (P value less than 0.05) association with MTE practice. Society’s barriers, such as knowledge, attitude, and practice (KAP) related, health facility related, and peer and social pressure-related factors, were identified. All stakeholders should put great emphasis on the elimination of this harmful practice.
Keywords: harmful traditions, milk teeth extraction, children under five years old
Background
Traditional practices represent the sum total of all behaviors that are learned, shared by a group of people, and transmitted from generation to generation. MTE practice is a procedure in which early teeth or un-erupted deciduous tooth follicles of a child are pulled out after an incision is made on the gum.1 When the eruption of milk teeth starts, it is painful and makes the child’s gums irritated. As a result, a child chews, bites, and sucks anything that he/she gets more than unusual, or his mother frequently scrubs gum to relieve pain. Due to this, a child acquires microorganisms that cause diarrhea and leads the mother to take her child to traditional healers to extract the child’s teeth.2,3
The deciduous tooth is the tooth that is most likely to be extracted, and it is always lower and bilateral.4 Traditional tooth extraction is popular in African countries, particularly those in East Africa, such as Sudan, Somalia, Kenya, Tanzania, Uganda, and Ethiopia. Different cultures locally call it Ebino, nylon teeth, tooth bud extraction, milk teeth extraction, deciduous canine teeth extraction, and oral mutilation.5,6
Although milk tooth extraction is less common in industrialized countries, it has been detected in dental examinations of children of African emigrants in Israel and Sweden.2,6 Instruments such as razor blades and wire are used by traditional healers, traditional birth attendants, and children’s parents, and the average age of children on whom the technique is conducted is 5–8 months. Canine teeth are thought to be a cause of vomiting, diarrhea, fever, and stunted growth in infants, which is why milk tooth extraction is done.7
Traditional healers who perform MTE practice believe that the cause of chronic diarrhea is a worm that is growing under milk teeth, and it is treated when the worm is removed by incision of the gum.3,8 Unlike in developing countries, where traditional practices are performed by more than 80% of the population. Populations in some countries in the Middle East as well as immigrants to Europe and the USA have abandoned these practices.2,9 Milk tooth extraction practices have a significant impact on children’s health, human rights, and benefits.9
Milk teeth extraction is practiced by children for a variety of reasons; research from numerous countries reviewed suggests that parents choose what is best for their children. It is the most fundamental principle that drives parents to subject their children to conventional customs. Failure to follow social conventions entails shame and social marginalization to children and their families, therefore attempting to follow them proudly perpetuates the habits.10
The problem in Ethiopia is not just that this ritual is still maintained, but that the people who participate in it are unaware of the destructive consequences of their actions. As a result, the Practice is extremely resistant to change.9,10
Milk tooth extraction remains a public health issue for children under the age of five around the world, primarily in East African countries. This is due to the low socioeconomic condition of the residents, deep-seated cultural attitudes, and a lack of a quality healthcare system in these areas.11 In the early 1990s, UN agencies and human rights organizations began to confront harmful traditional practices such as milk tooth extraction, but little progress was made.12
Around the world, about 7.7 million children under the age of five die each year.13,14 The third goal, target (No. 3.2), of the 17 Sustainable Development Goals (SDGs) issued by the United Nations in 2015 stipulates that all countries should strive to eliminate millions of preventable deaths of children under the age of five by 2030. The objectives are to reduce child mortality to no more than 25 deaths per 1000 live births in less than five years. Child mortality rates in the preceding five years ranged from 123 deaths per 1000 live births in the 2005 EDHS to 55 deaths per 1000 live births in the 2019 EMDHS in less than five years. Nearly 7.7 million children under the age of five die each year around the world.13,14
The extent to which the practice is practiced varies by area, cultural setting, religious ideals, and cultural heritage.13,14 It is one of the top five hazardous traditional practices performed on children under the age of five, according to two national studies conducted in Ethiopia.15 According to the baseline survey (BLS) done in 2008, the prevalence of milk teeth extraction was 48.1%, 52.4% in BLS, with a significant decline to 21.2% and 26.6%, respectively, in the follow-up study in the same setting.16
Despite a wide range of initiatives and attempts by a variety of actors aimed at protecting women’s and girls’ rights, this practice continues to jeopardize the well-being and integrity of Ethiopian women and children. Many health consequences, such as hemorrhage, damage to nearby structures, tetanus, heavy scarring, recurrent infections, HIV/AIDS, obstructed labor, fistulae, depression, suicide, and even death, occur in a significant number of women’s and children’s lives as a result of the practice’s high prevalence in Ethiopia.15,17
The factors that influence milk tooth extraction differ from one society to the next. For example, most societies practice milk tooth extractions to address diarrhea and vomiting in youngsters who are experiencing poor body growth. Among Ethiopian children under the age of five, the practice is currently the most common form of HTP.10,18
MTE is widely performed in Alle Woreda, Southern Ethiopia; however its prevalence and associated factors have yet to be investigated. As a result, we used the theory of planned behavior model to examine the prevalence and associated aspects of MTE. The findings of this study will be used to inform evidence-based decision-making in Alle Woreda in the prevention of hazardous traditional behaviors, perhaps lowering child morbidity and death. Furthermore, the findings will aid policymakers in adopting measures into their programs that will minimize the burden of detrimental customs on children.
Materials and Methods
Time and Place of Study
This research was carried out at Alle Special Woreda, which is one of the administrative units in the Southern Region, from March 18 to May 18, 2021. Kolango is the peculiar Woreda’s town. Addis Ababa (Ethiopia’s capital) is 650 kilometers away, and Hawassa is 394 kilometers away. Many ethnic groups from all over the world live in Alle Special Woreda. The Woreda’s climate is 59% hot and 29% semi-hot, with the remaining 13% freezing. North of Gamo Zone, south of Konso Zone, east of Derashe Special woreda, and western Konso Zone are all home to the special Woreda. It was made up of 17 rural kebeles and two urban kebeles (the lowest administrative unit in Ethiopia).
Design of the Research
The researchers used a community-based cross-sectional study approach. The source population for this study was all under five-year-old children in the special Alle woreda, while the study population was all under five-year-old children in the selected Kebeles. The current study included all under five-year-old children in the special Alle Woreda whose parents had lived in the study area for at least six months, whereas children whose parents were chronically ill and unable to reply were excluded.
Sample Size Determination
The sample size was calculated using a single population proportion formula: With a 5% margin of error at the 95% confidence level, a design effect of two, and a 10% response rate, the hypothesized prevalence of MTE prevalence estimates is 87.8%10 A total sample size of 363 was obtained as a result of this.
Sampling Procedure
A multi-stage stratified sampling was used with the strata of Kebles in urban and rural areas. A total of 19 kebeles were in the district, of which 17 kebeles were rural and the remaining 2 were urban. As a rule of thumb, 35% (6 kebeles) from rural areas and 1 kebele from urban areas were randomly selected by the lottery method. Once the study kebeles were identified, the total sample size for the study was distributed to the selected kebeles proportionally based on the number of households with fewer than 5 children. The household with 5 children in each kebele was selected by a computer generated random number method from a list of households with less than 5 children registered for deworming and vitamin A supplementation found in the health post. If more than one child exists, one would be selected randomly by the lottery method. Mothers of children under 5 years old were interviewed, and in households without a mother, father, or guardian, they were interviewed (see Figure 1).
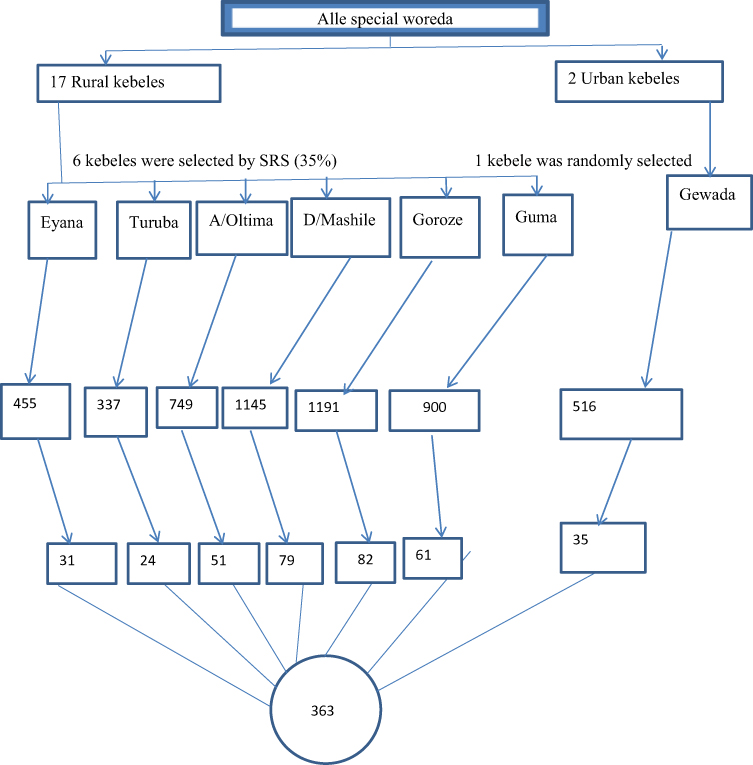 |
Figure 1 Schematic presentation of sampling procedure for population in Alle Special Wereda, 2022. |
Age, sex, education, religion, occupation, marital status, monthly household income, housing condition, presence of media materials, family size, age at first marriage, age at first pregnancy, attitude, subjective norm, perceived behavioral control, and intention towards the milk teeth extraction practice were the independent variables for the study.
Operational Definitions
Milk tooth extraction is the procedure of pulling out the early teeth of children.
Milk teeth extraction practice: A mother who had practiced the MTE procedure on at least one of her children.
Attitude:-A participant who achieved a median score of the attitude question is declared as having a positive attitude towards practicing milk teeth extraction.
A participant who achieved a median score on the subjective norm question is declared to have a positive subjective norm towards practicing the milk teeth extraction.
A participant with a median score above the median in the perceived behavioral control question is declared to have positive perceived behavioral control toward practicing MTE.
Intention: A participant who achieves a median score of more than 50% on the Intention question is declared as having a positive intention towards practicing the milk teeth extraction.
Data Collection Tools and Procedures
The information was gathered through the use of a semi-structured face-to-face interviewer-administered questionnaire that included socio-demographic and other characteristics that measure the prevalence of MTE and associated factors.2,10
Assurance of Data Quality
Following a review of relevant literature, the questionnaire was written in English first, then translated into Amharic and back to English to confirm that the thoughts underlying the questions were consistent. Cronbach’s alpha test was used to ensure internal consistency for the composite variables, and the scores for attitude, subjective norm, perceived behavioral control, and intention items were 0.82, 0.86, 0.76, and 0.9, respectively. A pretest (5%) was conducted in Derashe special wereda prior to the real data collection period, and minor changes to questions, wordings, phrases, and the time required to interview a respondent were made depending on the results. A clear introduction that describes the ethics, purpose, and aims of data gathering should be given during that time.
Data Processing and Statistical Analysis
Study participants’ data were collected, double-checked, and entered into epi-data version 4.4.2.1.STATA version 14.0 was used to export the data. For the most part, descriptive statistics such as frequency, distribution, and percentage calculations have been performed. The variance inflation factor (> 10) was used to assess the multicollinearity among the predictor variables. The factors causing MTE have been identified using univariate and multivariate binary logistic regression. Finally, in order to find statistically significant relationships with milk teeth extraction, 95% confidence intervals and adjusted odds ratios (AORs) were calculated. Candidates for multivariate binary logistic regression were variables with a p-value less than 0.25 in univariate binary logistic regression. The statistical significance level will be set at Pv 0.05.
Ethical Consideration
The Institutional Research Ethical Review Committee of Arba Minch University provided ethical clearance with reference number IRB/1079/21 before the study was conducted. Written approval was received from the special woreda health authorities after receiving ethical clearance. After describing the study’s goal, each study participant gave their informed verbal consent. Individuals were given the option to participate on a voluntary basis, and if they did not volunteer to continue from the beginning or at any point during the interview, they could withdraw from the study without penalty. During the interview, complete confidentiality and privacy were maintained. The information gathered for this study was kept private and retained in files.
Results
Socio-Demographic Characteristics
A total of 363 mothers participated in the study, making it a 100% response rate. The number of female children was 159 (43.8%) and the median age of children was 12 months (range: 1–48 months), while the median age of mothers was 29 years (range: 17–50 years) (See Table 1).
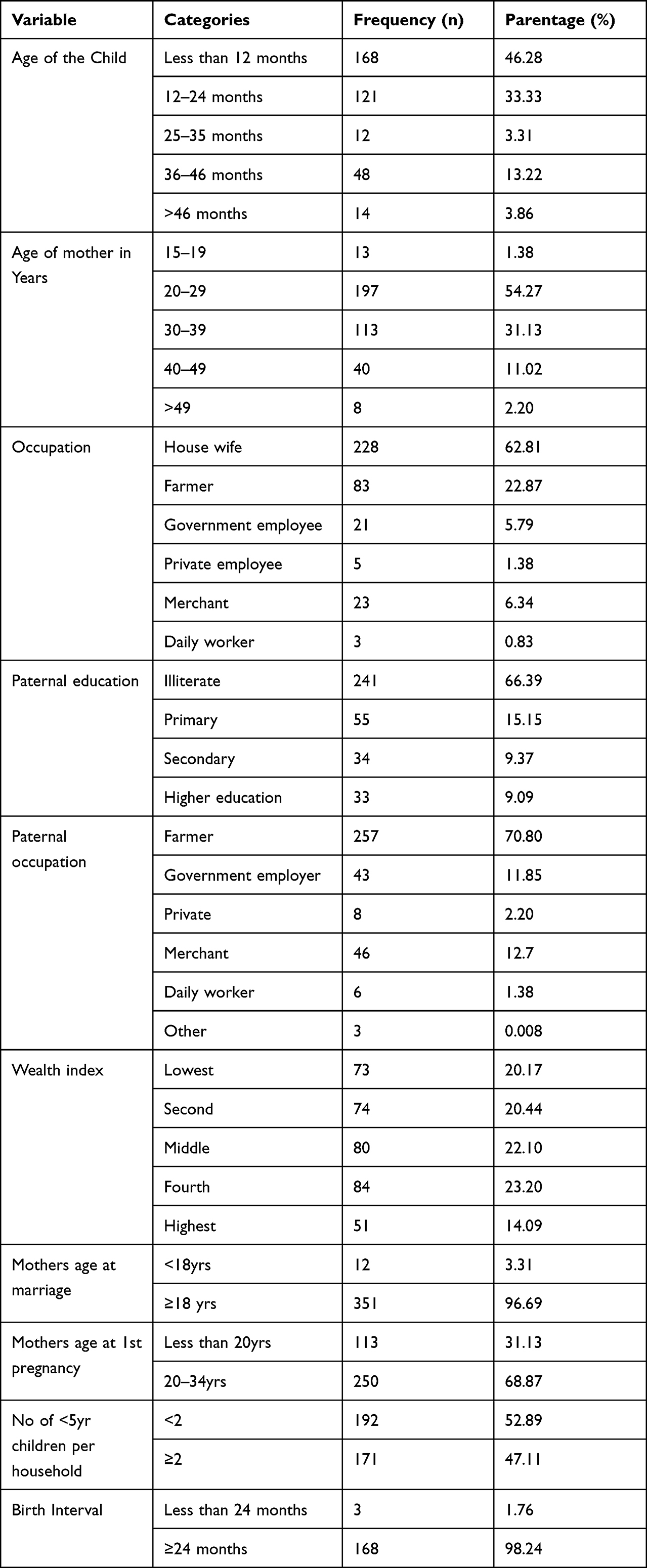 |
Table 1 Shows the Socio-Demographic Characteristics of Respondents’ Attitudes Toward Milk Tooth Extraction Among 5-Year-Old Children in Alle Special Wereda 2021 (n = 363) |
Maternal Information Related Characteristics
Among the study participants, 279 (78.3%) had heard information about milk teeth extraction. The prevalence of MTE among the study participants was 213 (58.58%, 95% CI: 53.6, 63.8).
Psycho-Social and Behavior-Related Factors
Attitude Related Factors
From the study participants, 145 (39.94%) agree that milk tooth extraction practice is good for health and should be promoted forever. Among the study participants, 150 (41.32%) agree that milk teeth extraction practice can manage some childhood illnesses like diarrhea and vomiting, and 124 (34.16%) respondents agree that childhood illnesses are hidden and not managed by health professionals. In addition to this, out of a total of 363 respondents, 166 (42.12%) responded that milk teeth extraction is an effective way for the treatment of childhood illnesses like diarrhea and vomiting (see Table 2).
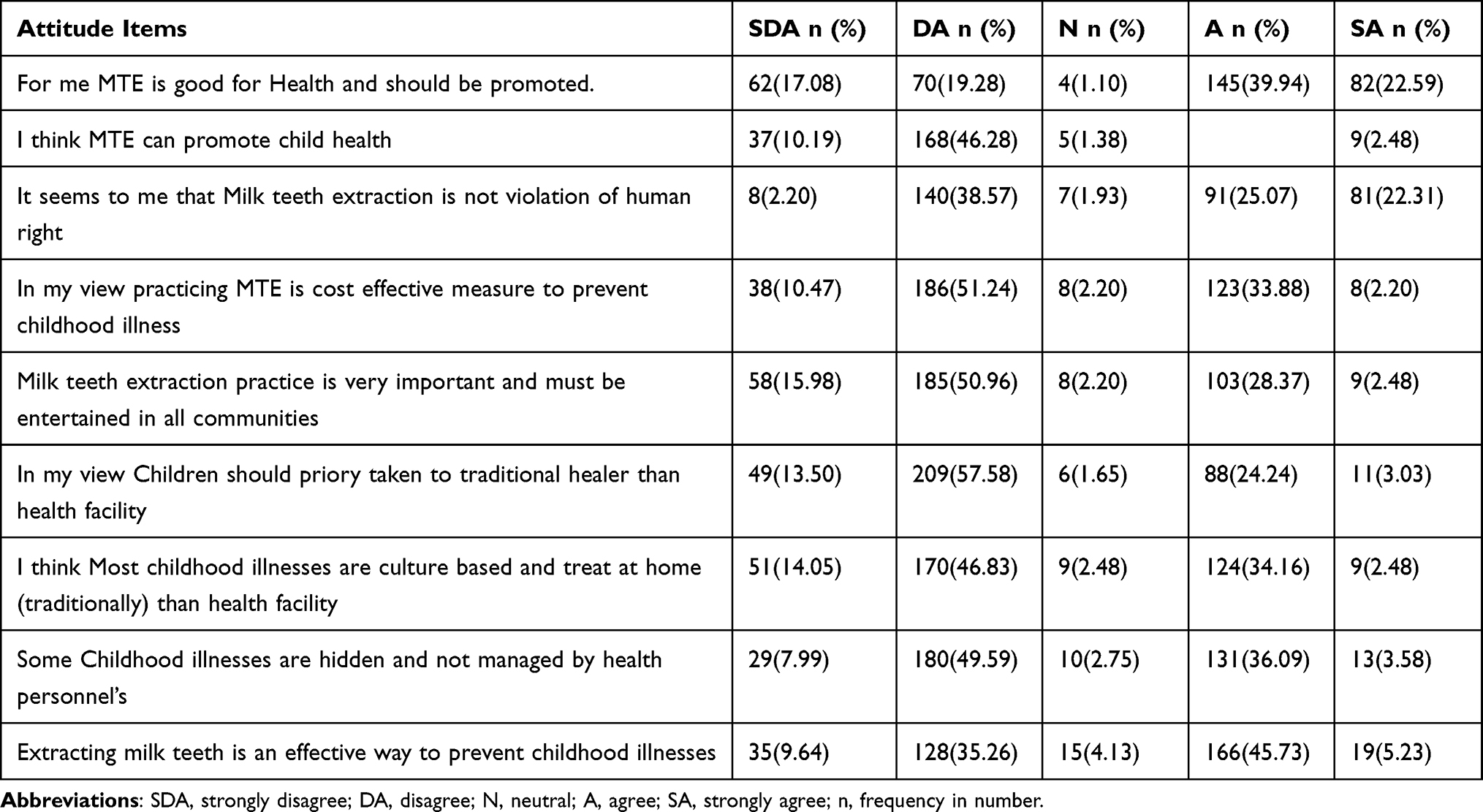 |
Table 2 Descriptive Analysis for Attitude Item Responses of Mothers Who Have Less Than Five Years Children in Alle Special Wereda 2021 (n = 363) |
Subjective Norm-Related Factors
Among the study participants, 166 (45.7%) responded that they practice milk tooth extraction on their children because of the support from those who are most important to them. One hundred and sixty-two (44.63%) respondents believe that they are under social pressure to practice it. Eighty (22%) of the study participants responded that they feel comfortable when they practice milk tooth extraction on their children. Among the study participants, 136 (37.547%) agree that they commit the tradition to their children due to pressure from their husbands (see Table 3).
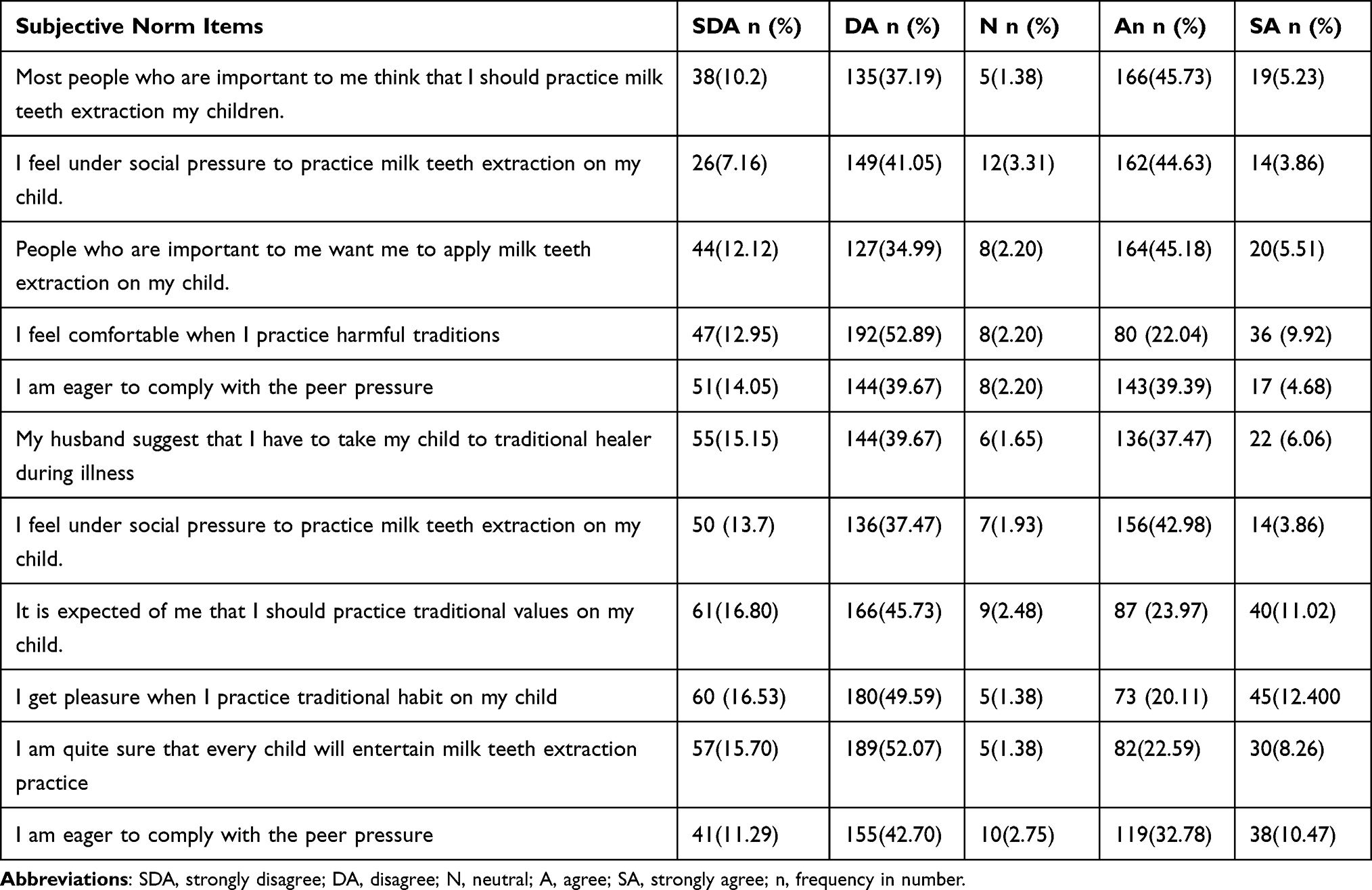 |
Table 3 Descriptive Analysis of Subjective Norm Items Responses from Mothers with Children Under the Age of Five in Alle Special Wereda 2021 (n = 363) |
Perceived Behavioral Control Related Factors
Seventy-six (20.94%) study participants respond that they are confident enough to practice milk teeth extraction on their children, and 140 (38.57%) perceive committing to milk teeth extraction on children as a good habit. Among the study participants, 147 (40.5%) respond that the decision to practice milk tooth extraction on their children is entirely up to them, while 98 (27%) respond that they get difficulty from their spouse to practice milk tooth extraction on children, and 103 (28.37%) respond that they get difficulty from their relatives (see Table 4).
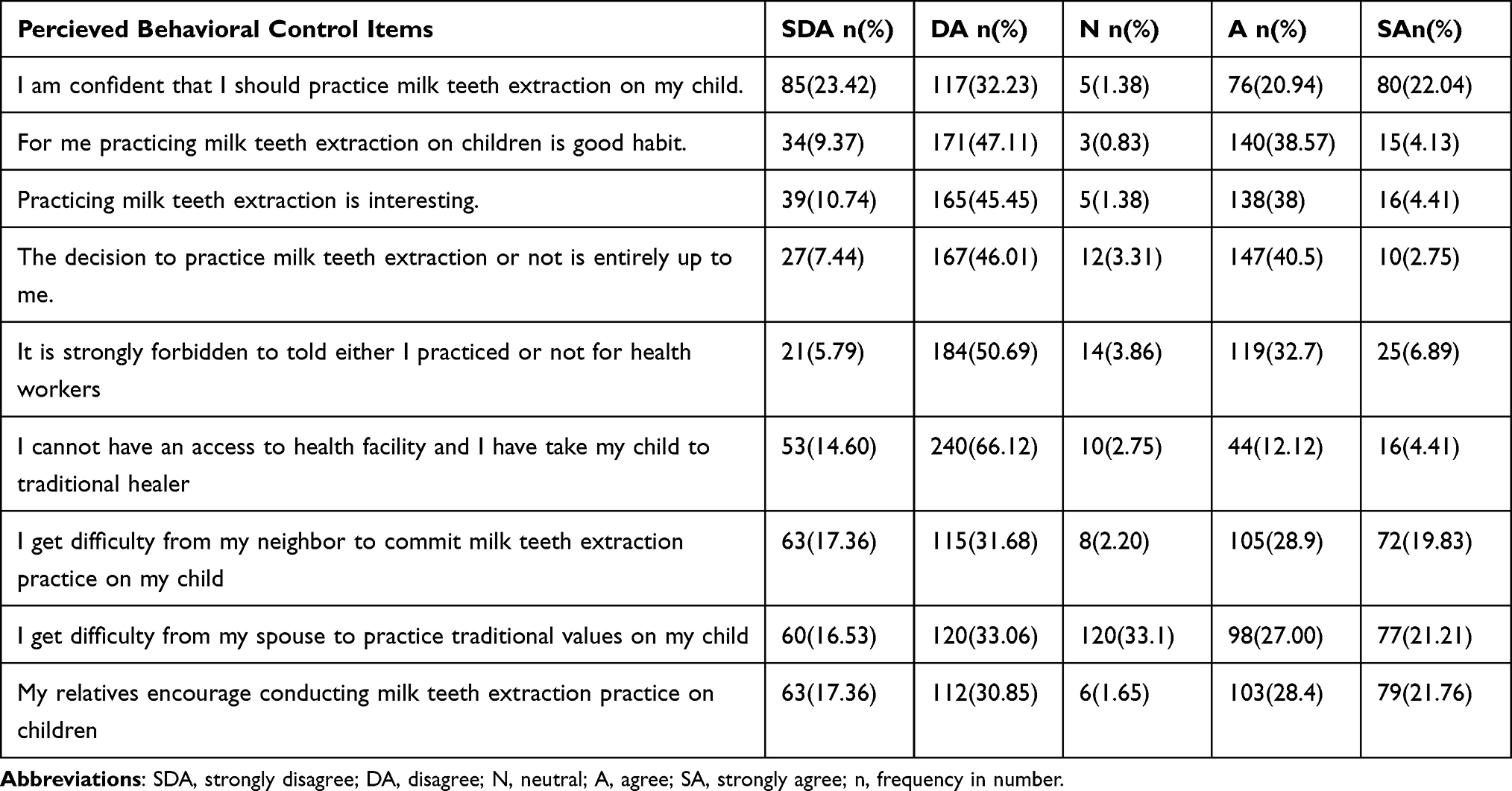 |
Table 4 Descriptive Analysis for Perceived Behavioural Control Item Responses of Mothers Who Have Had Less Than Five Years of Children in Alle Special Wereda 2021 (n = 363) |
Intention Related Factors
One hundred and fifty (42.32%) of study participants agree that they expect to perform milk tooth extraction on their children.One hundred and thirty-one (36%) respondents agree that they want to practice milk tooth extraction on their children. One hundred and twenty-five (34.4%) of the total study participants agreed that they intend to perform milk tooth extraction on their children (see Table 5).
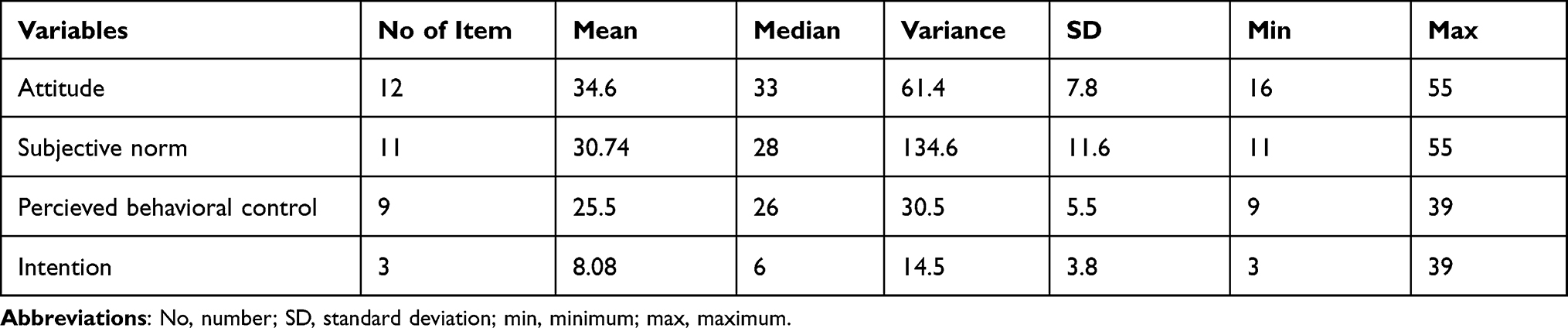 |
Table 5 Descriptive Statistics for Psycho-Social and Behavior-Related Variable Items |
Those participants who scored below the median value had been taken as negative attitude towards milk teeth extraction practice, while the above median score had been declared as positive attitude and the same was for other composite variables (see Figure 2).
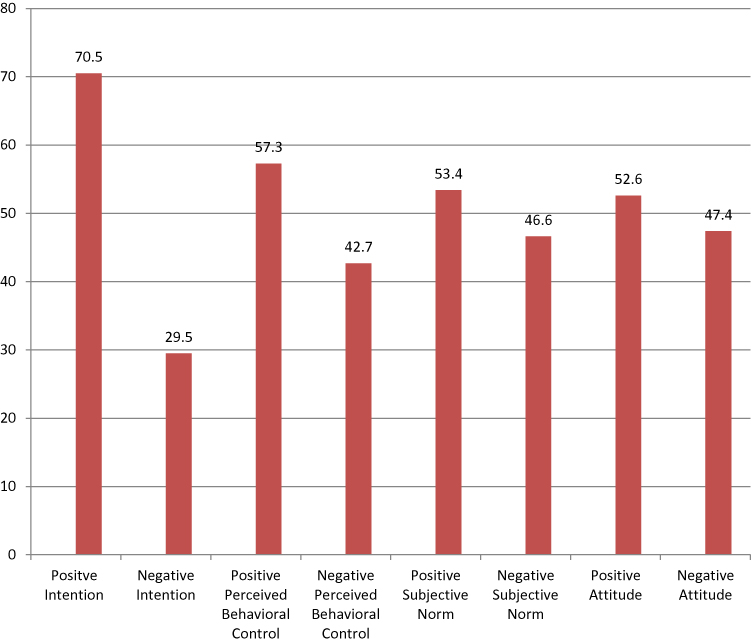 |
Figure 2 Descriptive statistics for summary of attitude, subjective norm, perceived behavioral control and intention of mothers who have less than five years children in Alle Special Wereda, 2022 (n = 363). |
Factors Associated with Milk Teeth Extraction
The variables sex (female), age of the child (less than 12 months, 25–35 months, 36–46 months), maternal occupation (housewife), paternal education (no education), paternal occupation being farmer, rural residence, maternal age at marriage less than 18 years, positive attitude, positive subjective norm, positive perceived behavioral control, and positive attitude, positive subjective norm, positive perceived behavioral control were candidates for multivariate binary logistic regression (P-value less than 0.25). In multivariate binary logistic regression, the variables child age less than 12 months, maternal occupation as a housewife, father’s education, rural residence, and having a positive attitude and intention toward practicing milk teeth extraction all showed statistically significant associations with milk teeth extraction.
Milk teeth extraction is common harmful traditional practice in the study area, in univariate binary logistic regression those variables which were candidate for multivariate binary logistic regression (P-value <0.25) were sex (female), age of the child (less than 12 months,25–35 months,36–46 months), maternal occupation (housewife), paternal education (no education), paternal occupation being farmer, rural residence, maternal age at marriage <18 yrs, positive attitude, positive subjective norm, positive perceived behavioral control and positive intention showed positive association towards practicing milk teeth extraction. The variables that showed statistically significant association with milk teeth extraction in multivariate binary logistic regression were child age less than 12 months, maternal occupation being house wife, father’s education, rural residence, having positive attitude and intention towards practicing the milk teeth extraction practice. The odds of practicing milk teeth extraction was 1.27 times higher among <12 months children than those in older age with (95% CI: 1.02,1.6). This might be due to the fact that during this age the risk of diarrhea increased due to subside of naturally acquired passive immunity of the child.
Those mothers who are house wives are 1.3 (95% CI: 1.04, 1.65) times more likely to practice milk teeth extraction on their children than merchants. This might be due to the fact that merchant mothers were well informed and probably educated as compared to house wives. Fathers with no education are 1.4 (95% CI: 1.2, 1.9) times more likely to exercise milk teeth extraction practice on their children than fathers with above higher education.
Both univariate and multivariate binary logistic regression reveal that as one’s degree of education rises, so does their willingness to extract milk teeth. This declares that education is a tool for addressing the problem. In comparison to mothers in urban regions, moms in rural areas were 3.6 (95% CI: 1.08, 12.4) times more likely to extract their children’s milk teeth. Because rural mothers have less access to information and education, this is the case. Moms with a positive attitude toward traditional child abuse were 1.65 times more likely than mothers with a negative attitude to engage in hazardous traditional child abuse (95% CI: 1.01, 2.8). Mothers who have a favorable attitude about the practice are 1.82 times more likely than those who have a negative attitude (see Table 6).
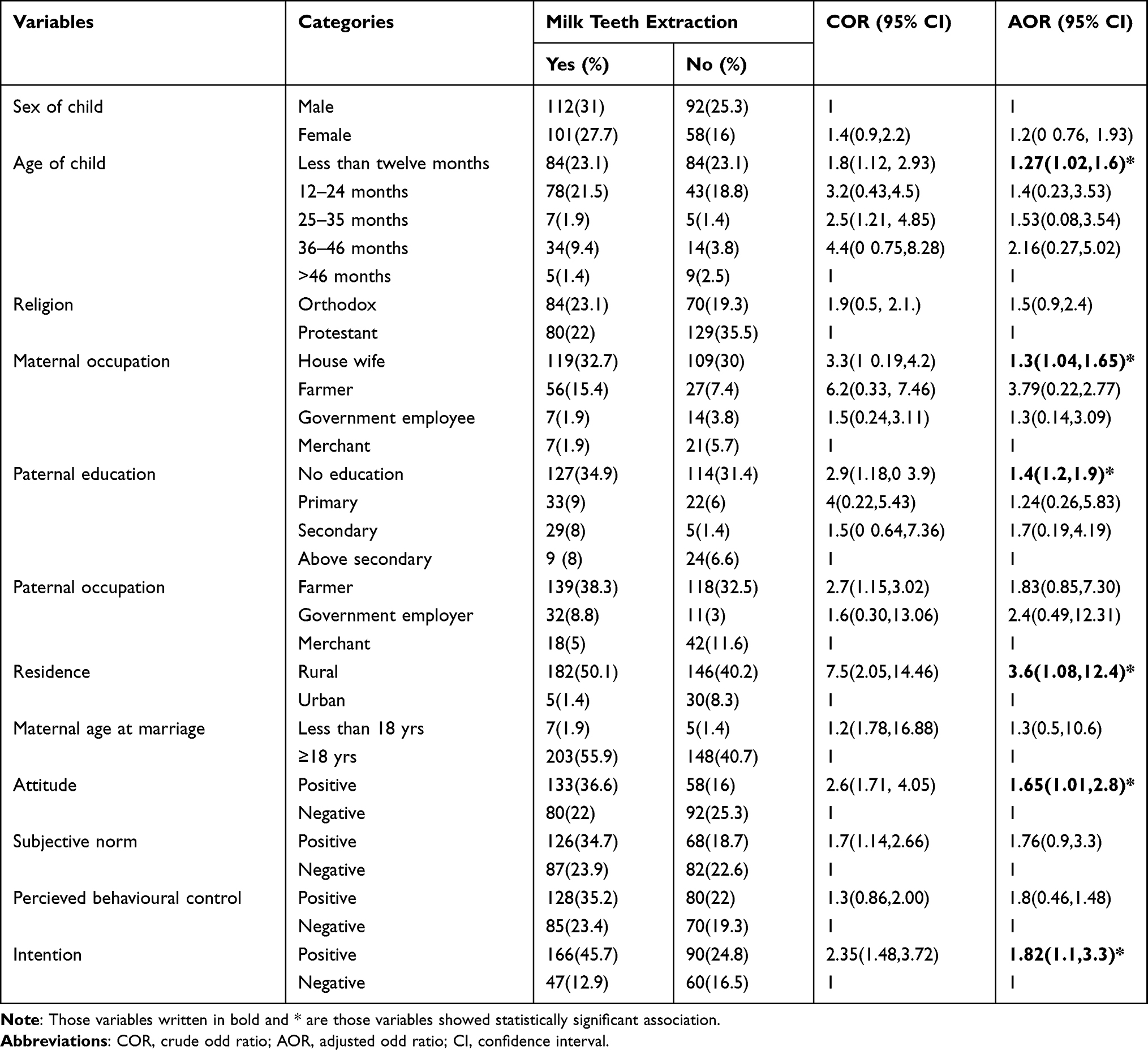 |
Table 6 Univariate and Multivariate Binary Logistic Regression Analysis for Factors Associated with Milk Teeth Extraction Among Less Than Five-Year-Old Children in Alle Special Wereda, Southern Ethiopia in 2021 (n = 363) |
Discussion
The goal of this study was to find out the prevalence, associated causes, and societal barriers of commonly performed harmful practices among children under the age of five in Alle Special Wereda, Ethiopia. According to the findings, 58.68% of children under the age of five had their milk teeth extracted (95% CI: 0.5, 0.6).
The findings of this study are similar to those of a baseline survey done in Ethiopia in 1997.20 The result is lower than a Gondar University baseline survey,19 but much higher than a research conducted in Axum, north Ethiopia, which indicated a prevalence of 12.5%.10 The observed difference could be attributed to differences in custom and time, as well as cultural and community awareness, however it was significantly smaller when compared to a previous study (baseline survey conducted by Gondar university). This significant difference might be due to changes in knowledge, attitude and increased health information.
98.07% of survey participants (95 confidence interval: 0.96, 0.99) have heard about typical hazardous traditional practices. This is in line with the findings of a study conducted in Axum, North Ethiopia (99%). 78.3% of moms have heard about the practice of extracting milk teeth from the total respondents. In North Gondar, this outcome was compared to a baseline study on female genital modulation and harmful traditional practices.16 Despite the huge number of people who heard the information, more than half of mothers (58.68%) extract their children’s milk teeth.
According to the results of our study, 166 (45.73%) moms believed that milk tooth extraction was an efficient treatment for childhood disorders such as diarrhea. This indicates that either there is a lack of knowledge available to influence mothers’ attitudes, or that the mechanism of delivery is insufficient to effect change. Furthermore, the intervention or routine health education may not reach the target demographic and area, which may include moms, spouses, traditional practitioners, the elderly, and those who live in rural and urban areas. The sex of the child had no statistical effect with milk teeth extraction methods in this investigation. This demonstrates that the research area’s male and female youngsters were equally exposed to the danger of malpractice.
Milk tooth extraction was 1.27 times more likely in 12-month-old children than in the later age groups (95% CI: 1.02, 1.6). Housewives are 1.3 (95% CI: 1.04, 1.65) times more likely than moms with other jobs to perform milk teeth extraction on their children. Fathers with no education are 1.4 (95% CI: 1.02, 1.9) times more likely than fathers with a higher education to take milk teeth from their children.
In comparison to mothers in urban regions, moms in rural areas were 3.6 (95% CI: 1.08, 12.4) times more likely to extract their children’s milk teeth. One probable explanation is that moms who live in cities have easy access to health care.
Those with a positive attitude were 1.65 (95% CI: 1.01, 2.8) times more likely than those with a negative attitude to practice milk tooth extraction. Similarly, women who have a positive attitude regarding milk teeth extraction are 1.82 (95% CI: 1.1, 3.3) times more likely to do so than mothers who have a negative attitude.
Strength
The study employed a mixed community-based cross-sectional study design and the construction of a framework from the theory of planned behavior.
Limitation
Social desirability bias and recall bias were seen during the data collection.
Conclusion
The prevalence of MTE practice in the research area was determined to be 58.68%. In Alle Special Wereda, factors like the child’s age, maternal occupation, paternal educational level, residence, having a positive attitude and intentions toward MTE practice, and having a positive attitude and intentions toward MTE practice showed a statistically significant association (P value less than 0.05) with MTE practice on children under the age of five.
Recommendations
Alle Wereda Special Health Office
- Facilitating the availability of an accessible health facility that provides compassionate care at a reasonable cost in light of the rural community
- They need to work with Alle wereda women’s and children’s affairs to change women’s attitudes and optimize their children’s health status.
- Needs to work with kebele leaders, religious leaders and social institutions to influence perceptions targeting specific aspects of milk tooth extraction as a common harmful traditional practice.
For Alle Special Wereda Road and Transport Office
- Should give great attention to road construction activities for the community to access health facilities.
To Researchers
- Pure qualitative research should be conducted to conduct a detailed exploration of societal experiences regarding common harmful traditions.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; EDHS, Ethiopian Demographic Health survey; EGLDAM, Ethiopian Goji Limadawi Dirgitoch Aswogaji Mahiber; EMDHS, Ethiopian Mini Demographic Health survey; FMOH, Federal Ministry of Health; HIV/AIDS, human immune virus/acquired immune deficiency syndrome; HTTP, harmful traditional practice; IOM, infant oral mutilation; KAP, knowledge, attitude and practice; MTE, milk teeth extraction; NCTPE, National Committee on Traditional Practice in Ethiopia; SD, standard deviation; WHO, World Health Organization.
Data Sharing Statement
All relevant data are available in this paper. The STATA data of individual patients are not permitted to be provided to other bodies as indicated in the ethical clearance. However, researchers who need further clarification can get anonymized data from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
Ethical clearance board of Arba Minch University, College of Medicine and Health Sciences ethically approved all the study methods and protocols and responded with a letter reference number IRB/1079/2021. Informed verbal consent was taken from each study participant after ethical approval.
Acknowledgments
The authors acknowledge the Arba Minch University, College of Medicine and Health Sciences for funding and Alle Special Wereda health office for providing information to access the data. We also would like to acknowledge data collectors, supervisor and study participants for all what they did for accomplishment of the tasks.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was obtained from Arba Minch University, College of Medicine and Health Sciences.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Kipchumba PJ. Deciduous canine tooth bud extraction and nutritional status of children aged 2–5 years in Kajiado District, Kenya; 2013.
2. Dawit A, Getahun M, Berhaneselassie M. Harmful traditional practice in Ethiopia; 2013.
3. Kamimura C. Milk teeth extraction and behavior changes in Rural Amhara, Northwest Ethiopia. Nilo-Ethiop Stud. 2015;2015(20):1–16.
4. Davidovich E, Kooby E, Shapira J, Ram D. The traditional practice of canine bud removal in the offspring of Ethiopian immigrants. BMC Oral Health. 2013;13(1):1–4. doi:10.1186/1472-6831-13-34
5. Shameema GSP, Shenoy RP, Jodalli P, Sonde L. Culture and oral health–A review. Int J Appl Dent Sci. 2016;2:4.
6. Elgamri AI, Ahmed AT, Haj-Siddig OE, Chin JR. Infant oral mutilation (IOM) related to traditional practices among inner city pre-school children in Sudan. Afr Health Sci. 2018;18(2):359–368. doi:10.4314/ahs.v18i2.21
7. Barzangi J. Infant dental enucleation in Sweden: perspectives on a practice among residents of Eastern African Origin. Örebro University; 2017.
8. Sadik E, Gobena T, Mengistu B. Aspects of common traditional medical practices applied for under-five children in Ethiopia, Oromia Region, Eastern-Harargie District, Dadar Woreda, 2011 GC. Commun Med Health Educ. 2013;3(6):8034.
9. Alene GD, Edris M. Knowledge, attitudes and practices involved in harmful health behavior in Dembia district, Northwest Ethiopia. Ethiop J Health Dev. 2002;16(2):199–207. doi:10.4314/ejhd.v16i2.9811
10. Gebrekirstos K, Fantahun A, Buruh G. Magnitude and reasons for harmful traditional practices among children less than 5 years of age in Axum Town, North Ethiopia, 2013. Int J Pediatr. 2014;2014. doi:10.1155/2014/169795
11. Zuberi F. Assessment of Violence Against Children in the Eastern and Southern Africa Region. ESARO: UNICEF; 2005.
12. HaileMeskal F, Kitaw Y, Dejene A. Follow Up National Survey on Harmful Traditional Practices in Ethiopia. Addis Ababa: EGLDAM; 2008.
13. World Health Organization. The promotion and development of traditional medicine: report of a WHO meeting [held in Geneva from 28 November to 2 December 1977]. World Health Organization; 1978.
14. Rajaratnam JK, Marcus JR, Flaxman AD, et al. Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970–2010: a systematic analysis of progress towards Millennium Development Goal 4. Lancet. 2010;375(9730):1988–2008. doi:10.1016/S0140-6736(10)60703-9
15. ATEM C, Service. Baseline survey on the most prevalent HTP and sanitation practices among the community of the Hamer, Dassenech, and NyangatomWoredas of the South Omo Zone in the SNNPR. Addis Ababa, Ethiopia; 2011.
16. Dejene A, Birhanerselase A. Baseline survey on female genital mutilation and other harmful traditional practices. North Gondar Amhara Regional State; 2006.
17. Aaba A. National strategy and action plan on harmful traditional practices (HTPs) against women and children in Ethiopia federal democratic republic of Ethiopia ministry of women (MoWCYA). Children and Youth Affairs; 2013:1–61.
18. WHO U. Every Newborn: An Action Plan to End Preventable Deaths. World Health Organization: Geneva; 2014.
19. Teshome A, Andualem G, Seifu S, Tsegie R. Knowledge, attitude and practice of mothers towards canine tooth bud removal and associated factors among mothers visiting dental clinic of Gondar University Hospital, Ethiopia. J Commun Med Health. 2016;6(396):2161–0711.1000396.
20. Ethiopian G, Limadawi D, Aswegaj M. Initial national level surveys, Addis Ababa; 1997.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.