")
Back to Journals » Journal of Blood Medicine » Volume 12
Prevalence of Leucopenia and Associated Factors before and after Initiation of ART among HIV-Infected Patients, North East Ethiopia: Cross-Sectional Study
Authors Talargia F , Teshome Y , Aynalem YA , Asefa A
Received 17 February 2021
Accepted for publication 20 April 2021
Published 10 May 2021 Volume 2021:12 Pages 269—276
DOI https://doi.org/10.2147/JBM.S306369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Feredegn Talargia,1 Yonas Teshome,1 Yared Asmare Aynalem,2 Adisu Asefa1
1Department of Biomedical Science, College of Medicine, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Pediatrics Nursing, College of Health Science, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Feredegn Talargia P.O.Box: 445 Tel +251921792491
Email [email protected]
Background: Leucopenia is the commonest hematological abnormaly that occurs in patients with human immune deficiency virus (HIV) infection. The magnitude and related factors of leucopenia during the time of ART are not characterized in Ethiopia. This study aimed to assess the prevalence of leucopenia before and after the initiation of ART among HIV patients attending Debre Berhan Referral Hospital (DBRH), North East Ethiopia.
Methods: A cross-sectional study was conducted from September to December 2020 in DBRH, North-East Ethiopia. A total of 272 patients on ART were selected by simple random sampling techniques. Socio-demographic and clinical characteristics of the study participants were collected by standard questionnaires. Measurements of leucocyte count and CD4 counts were made by Sysmex XT 2000i hematology analyzer and BD FACS count CD4 analyzer, respectively. Statistical analysis of data was done by SPSS version 23. Logistic regression was done and a P-value< 0.05 was taken as statistically significant.
Results: The prevalence of leucopenia, neutropenia, and lymphopenia were 20.9%, 7.0%, and 6.6% before initiation of ART and 15.4%, 1.1, and 4.4% after initiation of ART, respectively. There was a significant difference in total white blood cell count, absolute neutrophil count, and total lymphocyte count between patients on ART and ART naïve patients. HIV patients whose cluster of differentiation (CD4) counts were < 200 cells/μL and patients on a zidovudine (AZT)-based regimen were more likely to have leucopenia than HIV patients whose CD4 counts were ≥ 200 cells/μL and on a tenofovir (TDF)-based regimen.
Conclusion: In this study, the prevalence of leucopenia, neutropenia, and lymphopenia has shown a significant decrement after the initiation of ART. HIV patients with low CD4 count and on an AZT-based regimen are more likely to have leucopenia, neutropenia, and lymphopenia. Based on our findings, we recommend that the health care professional routinely investigate and should treat leucopenia.
Keywords: ART, leucopenia, HIV/AIDS, Ethiopia
Background
Hematologic disorders are the most common complications of HIV AIDS, which include anemia, leucopenia, and thrombocytopenia.1 Among these hematological abnormalities; leucopenia is the common hematological abnormality that occurs in patients with HIV infection. The cause of HIV-related leucopenia is multifactorial, which includes a direct effect of HIV, autoimmune disease, neoplasm and ART drugs (especially zidovudine-based regimen), cotrimoxazole, and opportunistic infection.2–4 The prevalence of leucopenia is higher among treatment naïve people than treated ones in most studies.3–5 The use of antiretroviral therapy (ART) improves total white blood cell count by preventing suppression of bone marrow cells from the HIV virus and it blocks the interference of virus in the hematopoiesis process.6 Leucopenia occurs in HIV-infected patients. Even though low leukocyte count mainly indicates the toxicities of drugs for HIV or associated conditions, studies of untreated patients have also shown a high magnitude of leucopenia.7 The most common form of leucopenia usually encountered is neutropenia, occurring in 10–30% of HIV- infected individuals.8 Neutropenia is caused by decreased production of cells because HIV suppresses the bone marrow by changing the marrow microenvironment and by altering the cytokine expression and it is also common among HIV-infected patients and presents in approximately 10–50% of cases.8,9 In the study conducted in different parts of the United States, worsening of HIV disease parameters, like lower CD4 counts and higher HIV viral load, was found to be associated with the development of neutropenia.10 ART showed a statistically significant increment in the mean WBC (White blood cells) count in different studies.11–15 On the other hand, some studies reported that patients on ART had low WBC count compared to treatment naïve patients.16,17 Patients on ART showed a significant reduction in the prevalence of leucopenia and neutropenia compared to their ART-naïve groups.6,18 The improvement in these hematological abnormalities after ART initiation was due to increased production of Granulocyte- Macrophage Colony Stimulating Factor (GM-CSF) and Granulocyte Colony Stimulating Factor (G-CSF), which play an important role in the activation of granulocytes.19 Studies indicated that low CD4 count, advanced clinical stage of HIV disease, and zidovudine-based regimen are associated with an increased risk of leucopenia.8,16,20–22 Although hematologic abnormalities have been widely reported in HIV-related infections, there are a few data related with the prevalence of leucopenia and associated factors of leucopenia among HIV-infected patients before and after initiation of ART in Ethiopia. This study provides further information on HIV-associated leucopenia, and it can serve as a baseline for future studies. The aim of this study is to determine the prevalence of leucopenia and associated factors before and after the initiation of ART among HIV patients who attended the ART clinic at DBRH, North-East Ethiopia.
Methods and Materials
Study Period and Area
This study was conducted at the ART clinic of DBRH, North East Ethiopia from September to December 2020.
Study Design
A hospital-based cross-sectional study was conducted.
Source Population
All adult HIV-1 infected people receiving ART at the DBRH.
Study Population
All adult HIV-1 infected people receiving ART for at least 6 months in the ART clinic of DBRH.
Inclusion and Exclusion Criteria
Age greater or equal to 18-years old HIV-positive individuals who received ART for at least 6 months in DBRH were included in this study. Pregnant women, patients referred from other health institutions, patients with hematological disorders, severely sick patients with any other medical conditions, and patients who had taken other medications were excluded from the study.
Sample Size Determination
The sample size was determined by using a statistical for a single population (n=z2 p (1-p)/d2), taking p=19% (prevalence of leucopenia from previous study 85% level of precision (d) with 95% confidence interval plus 15% non-response rate were added.
n= (z2 p (1-p)/d2), substitute the value, n=1.962*0.19*0.81/0.052=236.48, when we added a 15% non-response rate we found approximately 272 sample sizes.
Sampling Procedures and Techniques
The samples of this study were collected by simple random sampling technique until the desired sample size was achieved from the subjects who fulfilled the inclusion criteria during the study period.
Study Variables
Dependent Variables
Prevalence of leucopenia, neutropenia, and lymphopenia
Independent Variables
Age, sex, stage of HIV disease, CD4 count, and type of ART regimen.
Data Collection and Procedures
The standard structured questionnaire was adapted after the review of different literature, and the data was collected by trained ART nurses. Data about socio-demographic, clinical characteristics, and pre-ART information of the study participants were collected by face-to-face interview and a review of medical registration books. After that, a blood sample was collected by laboratory technicians and sent to a hematology analyzer. Based on the standard procedures, WBC count and CD4 cell counts were determined by using the Sysmex XT 2000i hematology analyzer and BD FACS count system, respectively. In order to keep the quality of data, standard procedures were followed in every laboratory aspect of the procedures and the quality of CD4 and hematology analyzer was checked by running quality control samples along with the patient sample. In addition, there was training for data collectors, a pretest of the questioner was made and the data collection process was done two times a day by the principal investigators.
Leucopenia: Defined as WBC counts <4,000 cells/µL.
Neutropenia: Absolute neutrophil count (ANC) less than 1,000 cells/μL.
Lymphopenia: Total lymphocyte count (TLC) of less than 800 cells/μL.
Data Processing and Analysis
The data were coded, checked and entered in the EPI data software version 3.1, and exported to SPSS software version 23 for analysis. The results of descriptive statistics were expressed as frequency and percentage. Continuous variables were presented as mean ± standard deviation. Univariate logistic regression was performed to examine the association between dependent and independent variables using crude odds ratio (COR) with a 95% confidence interval (CI). Those independent variables with a P-value<0.2 in univariate analysis were included in multivariate logistic regression models. A P-value<0.05 on multivariate logistic regression was considered a statistically significant association.
Result
General Characteristics
From the total 272 HIV-positive patients, 110 (40.4%) were male and 162 (59.6%) were female. The mean age of the study participants was 40.94±10.88 years, ranging from 18–78 years. Most of the study participants were within the WHO stage one category at the baseline.
The WBC Count, ANC, TLC, and CD4 Counts of the Study Participants
The mean WBC count, ANC, and TLC at baseline were 4.65±1.53 X 103/μL, 2.24±0.9 X 103/μL, 1.48±0.6 X 103/μL, and 5.58±1.82 X 103/μL, 2.92±1.38 X 103/μL, 1.81±0.72 X 103/μL after initiation of ART (P<0.01). Similarly, the mean CD4 counts showed an increment from 264.75±184.5 cells/µL at the baseline to 544.0±261.3 cells/µL after the initiation of ART (P<0.01). The most commonly used ART regimen in the current was 1j (TDF-3TC-DTG) (Table 1).
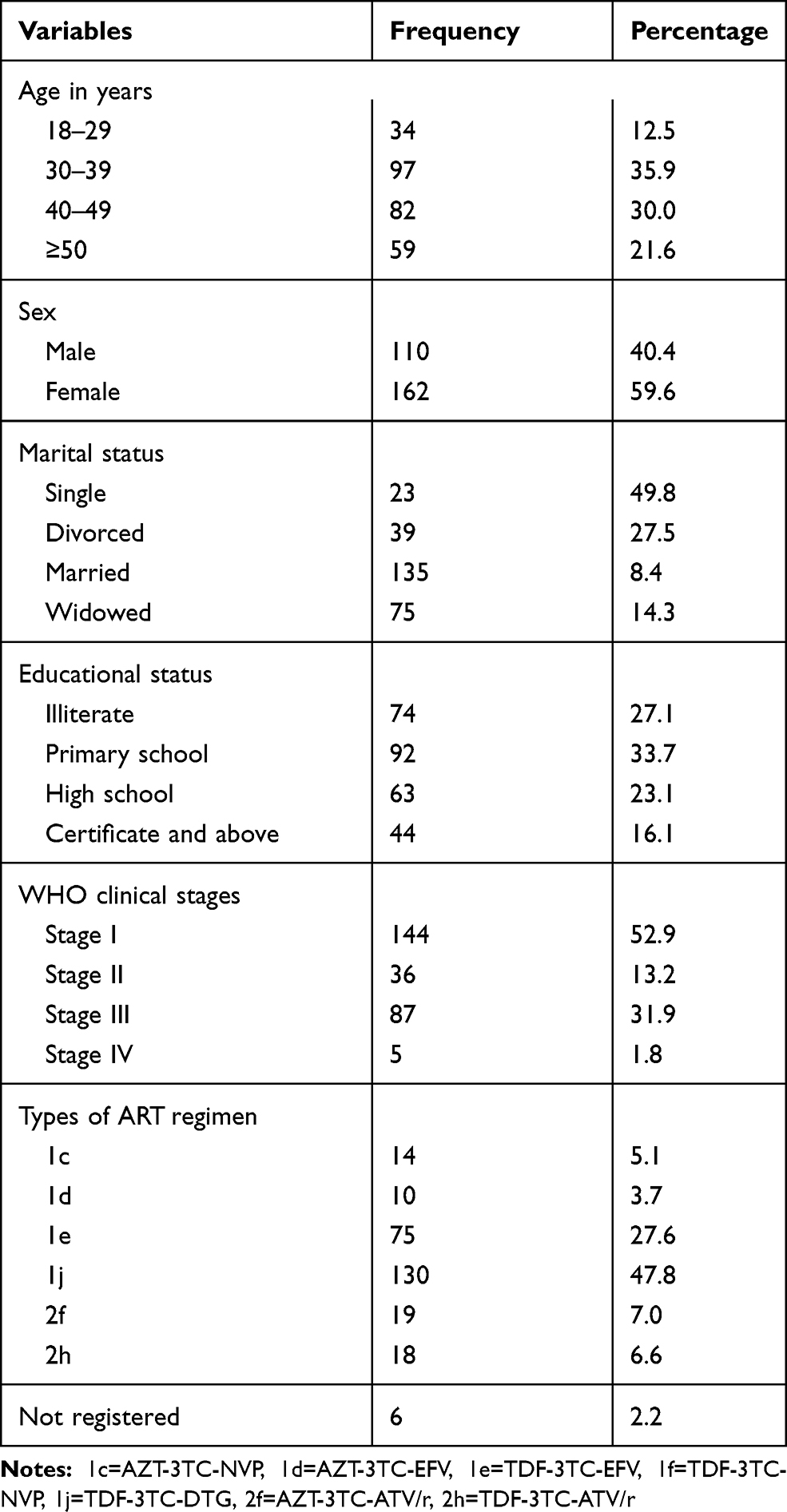 |
Table 1 Socio-Demographic and Clinical Characteristics of HIV Positive Patients Taking ART at DBRH, North East Ethiopia, 2020 |
Prevalence of Leucopenia, Neutropenia, and Lymphopenia and Associated Factors before Initiation of ART
The prevalence of leucopenia, neutropenia, and lymphopenia before ART was 20.9%, 7.0%, and 6.6%, respectively. The prevalence of leucopenia in males was 24.5% and 17.9% in females, whereas the prevalence of neutropenia and lymphopenia were 8.2%, 7.3% and 5.6%, 5.6% in males and females, respectively. In this study, most of the leucopenia cases (27.12%) were observed in the age groups ≥50 years. However, the majority of neutropenia cases were observed in the age range between 40–49 years and lymphopenia falls between the age group 18–19 years. Patients whose CD4 counts were <200 were strongly associated with a high prevalence of leucopenia and lymphopenia with a P-value<0.05. Lymphopenia was significantly associated with the advanced stage of HIV disease with a P-valve<0.03 (Table 2).
 |
Table 2 Leucopenia, Neutropenia, and Lymphopenia and Associated Factors before ART Initiation in HIV Positive Patients Attended at DBRH, North East Ethiopia, 2020 |
Prevalence of Leucopenia, Neutropenia, and Lymphopenia, and Associated Factors after the Initiation of ART
The prevalence of leucopenia, neutropenia, and lymphopenia after ART was 15.4%, 1.1, and 4.4%, respectively. The prevalence of leucopenia, neutropenia, and lymphopenia after the initiation of ART was decreased by 5.5%, 5.9%, and 2.2%, respectively. The prevalence of leucopenia, neutropenia, and lymphopenia in males was 24.5%, 0.9%, and 6.4% and in females 17.9, 1.2, and 3.1, respectively (Table 3). The prevalence of leucopenia was higher (21.6%) among patients whose age group was ≥50 years. The prevalence of leucopenia, neutropenia, and lymphopenia was high in patients with low CD4 count (<200). However, there was no significant association observed between the low CD4 count (<200) and that of leucopenia, neutropenia, and lymphopenia. HIV patients on an AZT-based regimen are more likely to have leucopenia and lymphopenia than HIV patients on a TDF-based regimen with a significant association at a P-value <0.02 and 0.01, respectively (Table 3).
 |
Table 3 Leucopenia, Neutropenia and Lymphopenia and Associated Factors after Initiation of ART in HIV Positive Patients Attended at DBRH, North East Ethiopia, 2020 |
Discussion
It’s well documented that hematological abnormalities are common in HIV-infected patients.1 Leucopenia, for instance, occurs in patients with HIV infection. The cause of HIV-associated leucopenia is multifactorial, including a direct consequence of HIV infection, autoimmune disorders, malignancies, and drugs used to treat HIV.3 This study revealed that the prevalence of leucopenia, neutropenia, and lymphopenia were 20.9%, 7.0%, and 6.6% at baseline, and 15.4%, 1.1%, and 4.4% after the initiation of ART. A study conducted in Ghana reported that the prevalence of leucopenia, neutropenia, and lymphopenia were 13%, 72.5%, and 6.5% in pre-ART patients and 6.5%, 85%, and 18% in post-ART patients.4 Another study conducted in Gondar, Ethiopia reported that the prevalence of leucopenia, neutropenia, and lymphopenia were 35.9%, 28.3, and 2.1 on ART patients and 16.9%, 14.5, and 2.1 ART naïve patients.16 The difference in results seen from the present study might be due to the difference in the definition of leucopenia, neutropenia, and lymphopenia, study design and size of the study population. The decrease in the prevalence of leucopenia, neutropenia, and lymphopenia after ART initiation might be due to; disorders of hematopoiesis, opportunistic infections, and immune causes related to HIV leading to low white blood cell count could be reverted after ART initiation.23 In the present study the prevalence of leucopenia was elevated in patients whose age is ≥50 years old, which is in agreement with another study.2 The increase in the prevalence of leucopenia with age might be due to a higher incidence of myelodysplasia in older patients.9 However, leucopenia did not show a statistically significant difference with sex and age. This was in line with previous studies.2,21
According to the present study, the prevalence of leucopenia, neutropenia, and lymphopenia were increased with decreasing in CD4 count both before and after the initiation of ART. Leucopenia, neutropenia, and lymphopenia were more prevalent among HIV-positive patients whose CD4 count was <200 cells/µL. These findings were similar to several studies that reported the leucopenia, neutropenia, and lymphopenia was more prevalent among patients with CD4 count <200 cells/µL.2,3,16 The prevalence of leucopenia and lymphopenia with decreased CD4 count was significantly associated before initiation of ART, but it did not significantly associate after ART initiation, this may be due to ART bringing a statistical increment into the WBC count.11,13 The present study revealed that patients on AZT-based ART regimen had a higher prevalence of leucopenia, neutropenia, and lymphopenia compared to TDF-based ART regimen. Similar to the present study conducted in Ethiopia and Ghana, it revealed an increment in the prevalence of leucopenia, neutropenia, and lymphopenia after initiation of AZT.2,4 However, neutropenia did not show a statistically significant difference with the AZT-based ART regimen. The high prevalence of leucopenia, neutropenia, and lymphopenia may be due to the suppression of bone marrow by Zidovudine-based therapy.16
Conclusion
In this study, the prevalence of leucopenia, neutropenia, and lymphopenia had shown a significant decrement after the initiation of ART. HIV patients with low CD4 count and on AZT-based regimen are more likely to have leucopenia, neutropenia, and lymphopenia. Based on our findings, we recommend that health care professionals routinely investigate and should treat leucopenia.
Abbreviations
AIDS, acquired immunodeficiency syndrome; ANC, absolute neutrophil count; ART, anti-retroviral therapy; AZT, zidovudine; CD4, cluster of differentiation; HIV, human immunodeficiency virus; TLC, total lymphocyte count; TDF, tenofovir.
Data Sharing Statement
The datasets used and analyzed during the present study are available from the corresponding author on reasonable requests.
Ethics Approval and Consent to Participate
This study was conducted after ethical letters obtained from the institute of research ethics and review board (IRB) of college of Medicine, Debre Berhan University, Ethiopia complied with the Declaration of Helsinki. The institute of research and ethics board committee (IRB) had reviewed and looed originality, feasibility, laboratory setting, and ethical aspects of the study. Following thorough discussion the committee approved the research proposal by authors with ethical approval using reference number med/219/2019. Then permission was taken from hospital higher management and data was collected after obtaining informed consent from the study participants. To keep confidentiality, codes were used and unauthorized persons did not have access to the data.
Acknowledgments
We would like to say thanks to the staff of the ART clinic in DBRH for their valuable support and guidance in the provision of medical records and data collection process. We also acknowledge Debre Berhan University for financial support to conduct this project.
Author Contributions
All authors had valuable contributions to the conception and design, data collection, analysis of data and interpretation; involved in drafting of the article or revising it critically for important intellectual content; agreed on journal to which the article will be submitted; gave final approval of the version to be published; agree to be accountable for all aspects of the work.
Funding
This study was funded by Debre Berhan University. The funder has no roles in the study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no competing of interests in this work.
References
1. Shen Y, Wang J, Wang Z, et al. A cross-sectional study of leukopenia and thrombocytopenia among Chinese adults with newly diagnosed HIV/AIDS. Biosci Trends. 2015;9(2):91–96. doi:10.5582/bst.2015.01024
2. Gebreweld A, Fiseha T, Girma N, Haileslasie H, Gebretsadik D. Prevalence of cytopenia and its associated factors among HIV infected adults on highly active antiretroviral therapy at Mehal Meda Hospital, North Shewa Zone, Ethiopia. PLoS One. 2020;15(9):e0239215. doi:10.1371/journal.pone.0239215
3. Fekene TE, Juhar LH, Mengesha CH, Worku DK. Prevalence of cytopenias in both HAART and HAART naïve HIV infected adult patients in Ethiopia: a cross sectional study. BMC Hematol. 2018;18:8.
4. Afari S, Blay E. Prevalence of haematological and serum biochemical abnormalities in hiv infected patients in Ghana, before and after antiretroviral therapy. Int J Virol AIDS. 2018;5(1):039.
5. Tamir Z, Seid A, Haileslassie H. Magnitude and associated factors of cytopenias among antiretroviral therapy naïve Human Immunodeficiency Virus infected adults in Dessie, Northeast Ethiopia. PLoS One. 2019;14(2):e0211708.
6. Choi SY, Kim I, Kim NJ, et al. Hematological manifestations of human immunodeficiency virus infection and the effect of highly active anti-retroviral therapy on cytopenia. Korean J Hematol. 2011;46(4):253–257. doi:10.5045/kjh.2011.46.4.253
7. Akinbami A, Oshinaike O, Adeyemo T, et al. Hematologic abnormalities in treatment-naive HIV patients. Infect Dis Res Treat. 2010;3(IDRT):S6033.
8. Addis Z, Yitayew G, Tachebele B. Prevalence of some hematological abnormalities among HIV positive patients on their first visit to a tertiary health institution in ethiopia; a cross sectional study. Int Blood Res Rev. 2014;2:270–278. doi:10.9734/IBRR/2014/11137
9. Dikshit B, Wanchu A, Sachdeva RK, Sharma A, Das R. Profile of hematological abnormalities of Indian HIV infected individuals. BMC Hematol. 2009;9(1):1–6. doi:10.1186/1471-2326-9-5
10. Levine AM, Karim R, Mack W, et al. Neutropenia in human immunodeficiency virus infection: data from the women’s interagency HIV study. Arch Intern Med. 2006;166(4):405–410. doi:10.1001/archinte.166.4.405
11. Amegor O, Bigila D, Oyesola O, Oyesola T, Buseni S. Hematological changes in HIV patients placed on anti retroviral therapy in Markurdi, Benue State of Nigeria. Asian J Epidemiol. 2009;2(4):97–103. doi:10.3923/aje.2009.97.103
12. Zama II, Amina A, Abdulrahaman Y, Yeldu MH. Some haematological profile of HIV/AIDS patients on Highly Active Antiretroviral Therapy(HAART) in Usamanu Danfodiyo University Teaching Hospital Sokoto, North-Western Nigeria.J Sci Technol. 2014;2(1):27–32.
13. Ako SE, Njunda LA, Akum EA, et al. Immuno-hematological Profile Trends of HIV/AIDs Patients on HAART in the South west region of cameroon: retrospective medical report review for possible stratified follow-up pattern in low income settings. Am J Microbiol Res. 2018;6(2):47–56. doi:10.12691/ajmr-6-2-3
14. Servais J, Nkoghe D, Schmit J-C, et al. HIV-associated hematologic disorders are correlated with plasma viral load and improve under highly active antiretroviral therapy. J Acquired Immune Deficiency Syndromes. 2001;28(3):221–225. doi:10.1097/00042560-200111010-00003
15. Odunukwe N, Idigbe O, Kanki P, et al. Haematological and biochemical response to treatment of HIV-1 infection with a combination of nevirapine+ stavudine+ lamivudine in Lagos Nigeria. Turkish J Haematol. 2005;22(3):125–131.
16. Enawgaw B, Alem M, Addis Z, Melku M. Determination of hematological and immunological parameters among HIV positive patients taking highly active antiretroviral treatment and treatment naïve in the antiretroviral therapy clinic of Gondar University Hospital, Gondar, Northwest Ethiopia: a comparative cross-sectional study. BMC Hematol. 2014;14(1):1–7.
17. Wanjari A, Acharya S, Singh AP, Rathi C. A study of hematological profile in HIV/AIDS. AIDS. 2013;8:9.
18. Idowu C, Oke O, Afolayan D, Olaniran O, Akinloye O, Awodumila O. Effect of HAART on some haematological parameters, correlations between total lymphocyte and CD4 counts of HIV clients attending ssh, ikole-ekiti. Int J Biol Med Res. 2013;4(3):3265–3270.
19. Ijeoma OL, Ifeoma UE, Emmanuel O, Ifeanyi AU, Andrew A. Comparative study of Cd8+ T-Cell count and leukopoietin levels in human immunodeficiency virus infection in Umuahia, Nigeria. IOSR J Dental Med Sci. 2014;13:102–110. doi:10.9790/0853-1392102110
20. Katemba C, Muzoora C, Muwanguzi E, Mwambi B, Atuhairwe C, Taremwa IM. Hematological abnormalities in HIV-antiretroviral therapy naïve clients as seen at an immune suppression syndrome clinic at Mbarara Regional Referral Hospital, southwestern Uganda. J Blood Med. 2018;9:105. doi:10.2147/JBM.S157148
21. Tamir Z, Seid A, Haileslassie H. Magnitude and associated factors of cytopenias among antiretroviral therapy naive Human Immunodeficiency Virus infected adults in Dessie, Northeast Ethiopia. PLoS One. 2019;14(2):e0211708. doi:10.1371/journal.pone.0211708
22. Forna F, Moore D, Mermin J, et al. Hematologic changes associated with Zidovudine following single-drug substitution from stavudine in a home-based AIDS care program in rural Uganda. J Int Assoc Physicians AIDS Care. 2009;8(2):128–138. doi:10.1177/1545109709333081
23. Fekene TE, Juhar LH, Mengesha CH, Worku DK. Prevalence of cytopenias in both HAART and HAART naïve HIV infected adult patients in Ethiopia: a cross sectional study. BMC Hematol. 2018;18(1):1–11. doi:10.1186/s12878-018-0102-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.