Back to Journals » Nature and Science of Sleep » Volume 18

Prevalence of Insomnia in Healthcare Profession - PIHEP Study: A Large-Scale National Study in Vietnam
Authors Duong-Quy S ![]() , Nguyen-Thi-Thu D, Hoang-Thi-Xuan H, Nguyen-Tung L
, Nguyen-Thi-Thu D, Hoang-Thi-Xuan H, Nguyen-Tung L ![]() , Bui-Ngoc-Phuong H, Duy LTT
, Bui-Ngoc-Phuong H, Duy LTT ![]() , Nguyen-Ngoc-Phuong T, Tang-Thi-Thao T, Nguyen-Duy T
, Nguyen-Ngoc-Phuong T, Tang-Thi-Thao T, Nguyen-Duy T ![]() , Nguyen-Trong B, Nguyen-Thi-Hong L
, Nguyen-Trong B, Nguyen-Thi-Hong L ![]() , Tran-Thi-Doan T, Phan-Thanh T
, Tran-Thi-Doan T, Phan-Thanh T ![]() , Bui-Diem K
, Bui-Diem K ![]() , Tran-Thi-Mong B, Tran-Quang P, Nguyen-Van T, Nguyen-Tuan A, Vu-Doan T, Pham-Van T, Mai-Xuan T, Phan NT, Nguyen-Ba V, Hoang-Thanh T, Tran-Phan-Chung T, Le-Thi-Minh H, Nguyen-Nhu V
, Tran-Thi-Mong B, Tran-Quang P, Nguyen-Van T, Nguyen-Tuan A, Vu-Doan T, Pham-Van T, Mai-Xuan T, Phan NT, Nguyen-Ba V, Hoang-Thanh T, Tran-Phan-Chung T, Le-Thi-Minh H, Nguyen-Nhu V ![]() , Pham-Van L, Le-Khac B, Vu-Van G, Soyez F, Penzel T
, Pham-Van L, Le-Khac B, Vu-Van G, Soyez F, Penzel T ![]() , Kushida C, Martin F
, Kushida C, Martin F
Received 5 March 2026
Accepted for publication 2 June 2026
Published 25 June 2026 Volume 2026:18 597038
DOI https://doi.org/10.2147/NSS.S597038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sarah L Appleton
Sy Duong-Quy,1– 4 Dung Nguyen-Thi-Thu,1,5 Huong Hoang-Thi-Xuan,1,6 Lam Nguyen-Tung,1,7 Hoa Bui-Ngoc-Phuong,1,8 Linh Tran Thanh Duy,1,9 Thu Nguyen-Ngoc-Phuong,1,7 Tram Tang-Thi-Thao,1,2 Thai Nguyen-Duy,1,4 Bang Nguyen-Trong,1 Lien Nguyen-Thi-Hong,1,10 Trang Tran-Thi-Doan,1 Thuy Phan-Thanh,1,11 Khue Bui-Diem,1,9 Bo Tran-Thi-Mong,12 Phap Tran-Quang,12 Toi Nguyen-Van,1,2 Anh Nguyen-Tuan,1,2 Tram Vu-Doan,1,2 Thuc Pham-Van,10 Trung Mai-Xuan,13 Nghia Thanh Phan,14 Viet Nguyen-Ba,14 Tuyen Hoang-Thanh,12 Thuy Tran-Phan-Chung,1,15 Huong Le-Thi-Minh,16 Vinh Nguyen-Nhu,1,9 Linh Pham-Van,1,10 Bao Le-Khac,1,9 Giap Vu-Van,1,11 Franck Soyez,1,17 Thomas Penzel,1,18 Clete Kushida,19 Francis Martin1,17
1Sleep Medicine Research Center, Vietnam Society of Sleep Medicine, Lam Dong, Vietnam; 2Bio-Medical Research Center, Lam Dong Medical College of Medicine, Lam Dong, Vietnam; 3Penn State College of Medicine, Penn State University, Hershey, PA, USA; 4Sleep Medicine Department, University of Medicine and Pharmacy, Hanoi National University, Hanoi, Vietnam; 5Thai Binh Medical College Hospital, Thai Binh Medical College, Hung Yen, Vietnam; 6Nursing Faculty, Phenika University, Hanoi, Vietnam; 7Department of Medicine, Pham Ngoc Thach University, Ho Chi Minh, Vietnam; 8Department of Neurology - Stroke, Vinmec Da Nang International Hospital, Da Nang, Vietnam; 9University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh, Vietnam; 10Hai Phong University of Medicine and Pharmacy, Hai Phong, Vietnam; 11Department of Respiratory Diseases, Bach Mai Hospital, Hanoi, Vietnam; 12Outpatient Department, 199 Hospital, Da Nang, Vietnam; 13Lao Cai Traditional Hospital, Lao Cai, Vietnam; 14Outpatient Department, Quang Ninh General Hospital, Quang Ninh, Vietnam; 15ENT Department, Tam Anh General Hospital, Ho Chi Minh, Vietnam; 16Pediatric Department, Vinmec Times City Hospital, Hanoi, Vietnam; 17French-Vietnamese Association of Pulmonology, Paris, France; 18Interdisciplinary Sleep Medicine Center, Charité Hospital, Berlin, Germany; 19Department of Psychiatry and Behavioral Sciences, Stanford University Center for Human Sleep Research, Redwood City, CA, USA
Correspondence: Sy Duong-Quy, Vietnam Society of Sleep Medicine, Lam Dong Medical College Council, Lam Dong, Vietnam, Email [email protected]
Background: Insomnia is a prevalent sleep disorder worldwide, yet data among healthcare professionals in Southeast Asia remain limited. Occupational stressors, rotating shifts, and high emotional demands may increase vulnerability to sleep disturbance in this population.
Objective: To estimate the prevalence of insomnia among Vietnamese healthcare professionals and to identify associated nocturnal symptoms, daytime impairments, and clinical associated factors.
Methods: We conducted a nationwide multi-region cross-sectional survey of 1655 healthcare professionals across Vietnam. Participants completed a structured questionnaire assessing insomnia symptoms, daytime consequences, comorbidities, and occupational factors. Insomnia was ascertained per ICSD-3 criteria for chronic insomnia, requiring (i) ≥ 1 nocturnal symptom (DIMS: difficulty initiating sleep, difficulty maintaining sleep, or early-morning awakening); (ii) ≥ 1 associated daytime impairment; (iii) symptom frequency ≥ 3 nights/week; and (iv) chronicity ≥ 3 months, despite adequate sleep opportunity. Severity was evaluated using the Insomnia Severity Index (ISI). Logistic regression models estimated odds ratios (ORs) and adjusted odds ratios (aORs) with 95% confidence intervals (CIs), adjusting for age, sex, occupation, marital status, and stimulant use.
Results: The prevalence of insomnia was 24.2% (95% CI, 22.2– 26.3), higher in women than men and increasing with age. The most common nocturnal symptoms were nocturnal awakenings (84.2%) and sleep-onset difficulty (57.2%), while daytime impairments included memory complaints (74.6%), mood disturbances (55.4%), and excessive daytime sleepiness (59.5%). In multivariable analysis, independent associated factors of insomnia included nocturnal awakenings (aOR 6.11), sleep-onset difficulty (aOR 2.89), mood disturbance (aOR 2.20), morning headache (aOR 2.18), and memory impairment (aOR 1.63). Stimulant consumption, particularly tea or coffee (aOR 2.10) and alcohol (aOR 1.98), was also independently associated.
Conclusion: Approximately one in four Vietnamese healthcare professionals experience insomnia, characterized by substantial nocturnal fragmentation and daytime dysfunction. Given its potential implications for clinician well-being and patient safety, systematic screening and integrated occupational sleep-health interventions are warranted.
Keywords: insomnia, sleep deprivation, healthcare professional, occupational health, Vietnam
Introduction
Insomnia is characterized by persistent difficulties initiating and/or maintaining sleep, accompanied by significant daytime impairment despite adequate opportunity for rest. A large meta-analysis encompassing more than eight billion adults estimated that the global prevalence of insomnia is approximately 16.2%, with 7.9% of individuals experiencing severe forms of the disorder.1 Although prevalence varies across populations and sociocultural contexts, healthcare professionals consistently report higher rates, ranging from 25% to 42%.2 These elevated rates likely reflect the unique occupational stressors inherent in clinical environments. Contributing factors include extended working hours, rotating and overnight shift schedules, circadian misalignment, high emotional demands, burnout, female sex, and a prior history of psychiatric disorders.2–4 Additionally, repeated exposure to acute stress, critical decision-making under time pressure, and insufficient recovery periods may further exacerbate vulnerability to chronic sleep disturbance among healthcare workers.
The consequences of insomnia are substantial, particularly within healthcare settings. Insomnia has been significantly associated with increased rates of medical errors, reduced clinical vigilance, and a higher risk of mental health problems, including depression and anxiety.5 Beyond psychological effects, poor sleep quality impairs cognitive domains essential for safe medical practice, such as attention, executive function, reaction time, and decision-making in emergency situations.6 At an organizational level, insomnia contributes to decreased productivity, increased absenteeism, higher staff turnover, and additional financial strain through error-related costs and reduced operational efficiency.7 Consequently, ensuring adequate sleep among healthcare professionals is not merely a matter of individual well-being but a critical determinant of patient safety, quality of care, and healthcare system sustainability.
Cross-country variation in HCW insomnia prevalence is well documented. Meta-analytic data among nurses have reported pooled sleep disturbance prevalence approaching 40% during pandemic periods, and rotating or overnight shift schedules consistently increase the odds of insomnia and shift-work disorder through circadian misalignment and cumulative sleep debt.2,4,8 Country-specific occupational factors, such as patient-to-nurse ratios, statutory rest-period regulations, and case-mix acuity, further contribute to differential outcomes.3 In Vietnam, public hospitals representative of the lower-middle-income Southeast Asian healthcare context operate under persistent workforce shortages, heavy patient loads, and frequent overnight shifts that may heighten this risk.9,10 Although prior Vietnamese studies have reported elevated insomnia rates among HCWs, these were largely single-institution surveys conducted during the COVID-19 pandemic and did not provide post-pandemic, multi-region, or multi-professional estimates using a standardized severity instrument.11,12
Addressing this gap is essential to inform evidence-based occupational health policies. Therefore, this study was conducted to: (1) estimate the first post-pandemic, multi-regional prevalence of chronic insomnia (ICSD-3) among Vietnamese healthcare professionals; (2) characterize associated nocturnal and daytime symptoms; and (3) identify clinical and occupational associated factors of insomnia severity using multivariable analysis. The findings are expected to provide a scientific foundation for targeted interventions aimed at mitigating insomnia, strengthening workforce resilience, and ultimately enhancing patient safety within Vietnam’s healthcare system.
Methods
Study Design and Setting
This nationwide multi-region cross-sectional survey was conducted among healthcare professionals in Vietnam from April to October 2024, in accordance with the STROBE guidelines for reporting observational studies.13
Participants
This multi-region cross-sectional survey was conducted across approximately 14 healthcare and academic institutions in Northern, Central, and Southern Vietnam that voluntarily joined following an open call from the Vietnam Society of Sleep Medicine (VSSM). Recruitment was therefore based on convenience sampling at the institutional level, stratified by profession to ensure occupational diversity.
The structured questionnaire was distributed electronically via Email to institutional mailing lists and the VSSM professional network, with a reminder sent two weeks later. Eligible participants were physicians, nurses, pharmacists, technicians, or other allied health professionals aged ≥ 18 years who were currently engaged in clinical practice and provided informed electronic consent. Participants were excluded if they had incomplete ISI data, current acute psychiatric hospitalization, or pregnancy-related sleep complaints as the sole sleep concern.
Of 2500 invited healthcare workers, 1810 responded (response rate 72.4%), and 1655 provided complete data for analysis (analytic completion rate 91.4%).
Sample Size
The sample size calculation was anchored to the lower bound of international meta-analytic estimates of HCW insomnia prevalence (~25%).2 Assuming an absolute precision of 2.5%, α = 0.05, and a 20% non-response buffer, the minimum required sample size was approximately 1440. The final analytic sample of 1655 exceeds this threshold.
Measures
Data were collected using a structured, self-administered questionnaire approved by the Scientific Committee of the Vietnam Society of Sleep Medicine. All sleep-related symptoms, daytime consequences, anthropometric items, and comorbidities were captured as dichotomous (Yes/No) responses with a one-month recall window (Supplementary Material S1).
The questionnaire included the following domains:
- Sociodemographic and occupational characteristics: age, sex, marital status, profession, years of work experience, workplace setting, and work schedule.
- Comorbidities: hypertension, diabetes, cardiovascular diseases, respiratory diseases, psychiatric disorders, and other chronic conditions.
- Sleep-related symptoms: insomnia, difficulty initiating sleep, nocturnal awakenings, early morning awakening, snoring, witnessed apnea, restless legs, and nightmares.
- Daytime consequences: excessive daytime sleepiness, fatigue, memory impairment, concentration difficulties, and mood disturbances.
- Insomnia definition and severity: The diagnosis of chronic insomnia was based on ICSD-3. The self-report item (Yes/No) asked participants whether they had “difficulty for initiating sleep”, “difficulty for maintaining sleep”, “waking up earlier than desired”; the sleep disturbance occurred despite adequate opportunity and circumstances for sleep. The sleep difficulty was associated with at least one of the following daytime impairments: fatigue, impaired attention/concentration or memory, social/occupational or academic impairment, mood disturbance or irritability, daytime sleepiness, behavioral problems (hyperactivity, impulsivity, aggression), reduced motivation or energy, increased errors or accidents, concerns or dissatisfaction about sleep (Yes/No). The sleep difficulty and associated daytime symptoms occurred at least three times per week and the symptoms presented for at least three months (Supplementary Material S1).
The Insomnia Severity Index (ISI) is a validated self-report questionnaire consisting of seven items designed to assess the severity of insomnia symptoms over the past two weeks (Supplementary Material S1). Each item is rated on a 5-point Likert scale ranging from 0 to 4, where 0 indicates no problem and 4 indicates a very severe problem. Study subjects stick (X) each question as presented in the enclosed PIHEP questionnaires. The total ISI score is calculated by summing the scores of all seven items, resulting in a total score ranging from 0 to 28. Total scores are interpreted as follows: 0–7 indicates no clinically significant insomnia, 8–14 indicates subthreshold insomnia, 15–21 indicates moderate clinical insomnia, and 22–28 indicates severe clinical insomnia.
Insomnia severity was assessed using the Vietnamese version of the Insomnia Severity Index (ISI), a 7-item validated instrument. Total scores range from 0 to 28, with a cutoff score of ≥8. Severity was categorized as mild (8–14), moderate (15–21), and severe (22–28).
Outcomes
The primary outcome was the prevalence of chronic insomnia as defined by the ICSD-3 criteria above. Secondary outcomes included ISI scores, the distribution of nocturnal and daytime symptoms, and associations between insomnia and sociodemographic characteristics, occupational factors, and comorbidities.
Statistical Analysis
All analyses were performed using Stata version 17.0 (StataCorp LLC, College Station, TX, USA). Descriptive statistics were used to summarize baseline characteristics. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate, while continuous variables were analyzed using the Student’s t-test or the Mann–Whitney U-test, depending on data distribution.
Logistic regression models were applied to estimate odds ratios (ORs) and 95% confidence intervals (CIs). Multivariable models were adjusted for predefined covariates, including age, sex, profession, marital status, and stimulant use. ISI scores were analyzed using linear regression models with robust standard errors to account for potential heteroscedasticity. Variables with p < 0.10 in univariable analyses were included in the multivariable models. A two-sided p-value < 0.05 was considered statistically significant. Sensitivity analyses were conducted with stratification by sex, age group, occupation, and stimulant use to characterize between-group variation in chronic insomnia and to assess the consistency of estimates across major sociodemographic and occupational subgroups.
Results
Characteristics and Prevalence of Insomnia of Study Participants
A total of 1655 participants were included in the study. Females comprised most of the sample (1167; 70.5%), while males accounted for 488 participants (29.5%). Regarding age distribution, the largest proportion of participants was in the 30–40 years group (755; 45.6%), followed by those aged <30 years (451; 27.3%). Participants aged 41–50 years represented 326 individuals (19.7%), and those aged >50 years accounted for 123 individuals (7.4%), constituting the smallest age group. The overall prevalence of insomnia was 24.2% (95% CI, 22.2–26.3); insomnia was also more common in women (25.5%) than in men (21.2%) (Table 1).
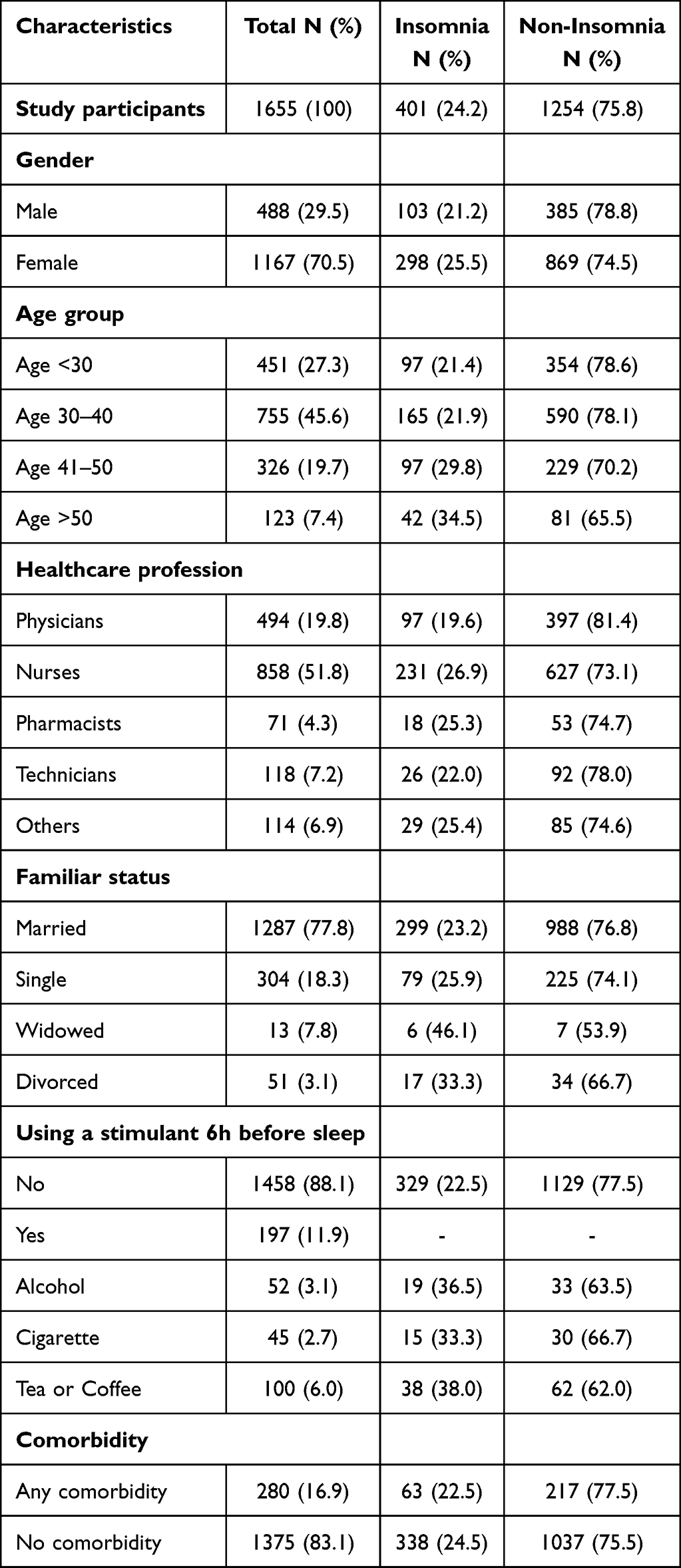 |
Table 1 Baseline Characteristics of the Study Participants |
Regarding healthcare profession, nurses represented the largest proportion of participants (51.8%), followed by physicians (19.8%). Technicians accounted for 7.2%, pharmacists for 4.3%, and other healthcare professionals for 6.9%. In terms of marital status, the majority of participants were married (77.8%), while 18.3% were single. Divorced individuals comprised 3.1%, and widowed participants represented a small proportion of the sample. Concerning stimulant use within six hours before sleep, most participants reported no use (88.1%), whereas 11.9% reported using stimulants. Specifically, 6.0% consumed tea or coffee, 3.1% reported alcohol use, and 2.7% reported cigarette use. Overall, 280 participants (16.9%) reported having at least one comorbidity.
Prevalence of Insomnia of Insomnia Classified by Age Group and Healthcare Profession
The prevalence increased with age, ranging from 21.4% among participants aged <30 years to 34.5% among those aged >50 years (Table 1 and Figure 1A). Regarding insomnia prevalence within each professional category, nurses exhibited the highest number of cases (n = 231), corresponding to 26.9% within their group; similar prevalence rates were observed among pharmacists (25.4%) and other healthcare professionals (25.4%); technicians showed a prevalence of 22.0%, while physicians had the lowest insomnia prevalence at 19.6% (Table 1 and Figure 1B).
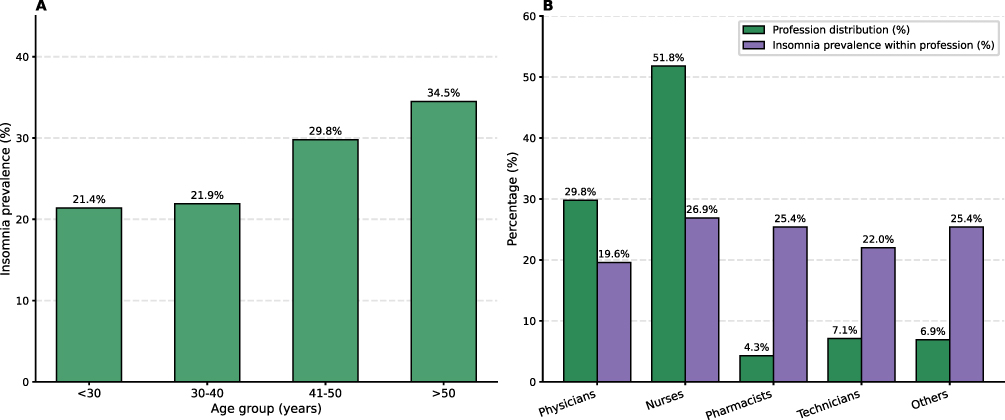 |
Figure 1 Prevalence of insomnia (A) classified by age group; (B) classified by healthcare professionals. |
When compared with the overall insomnia prevalence, physicians demonstrated a significantly lower rate (19.6% vs 24.2%; P=0.011). No statistically significant differences were observed among nurses, pharmacists, technicians, or other healthcare professionals (P>0.05; Table 1 and Figure 1B). Insomnia prevalence was significantly higher among participants consuming tea or coffee within six hours before sleep compared with non-users (38.0% vs 22.5%; P<0.001); alcohol users also demonstrated a higher insomnia rate than non-users (36.5% vs 22.5%: P= 0.019; Table 1). When compared with the overall insomnia prevalence of 24.2%, only the tea/coffee using group remained significantly higher (p = 0.004).
Nocturnal and Daytime Symptoms Related to Insomnia
Among participants with insomnia (N=401; 24.2%), 84.2% reported nocturnal awakenings, 57.2% experienced difficulty initiating sleep, and 40.7% reported morning headaches. Daytime impairments were common, including subjective sleepiness (59.5%), memory difficulties (74.6%), and mood disturbances (55.4%). The prevalence of daytime sleepiness was significantly higher among participants with insomnia compared with those without insomnia (59.5% vs 39.1%; Table 2 and Figure 2).
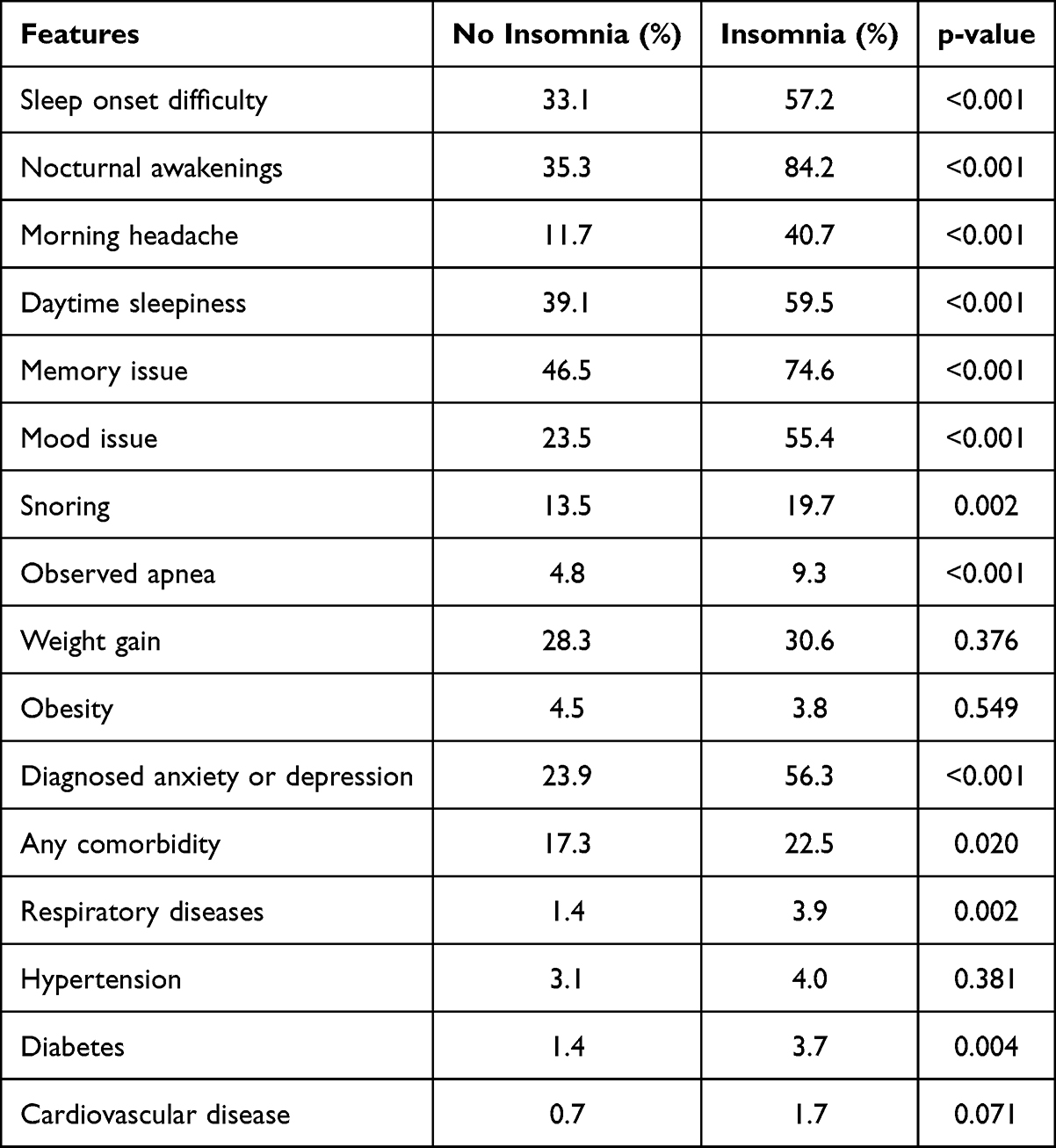 |
Table 2 Comparison of Sleep-Related Symptoms and Clinical Features by Insomnia Status |
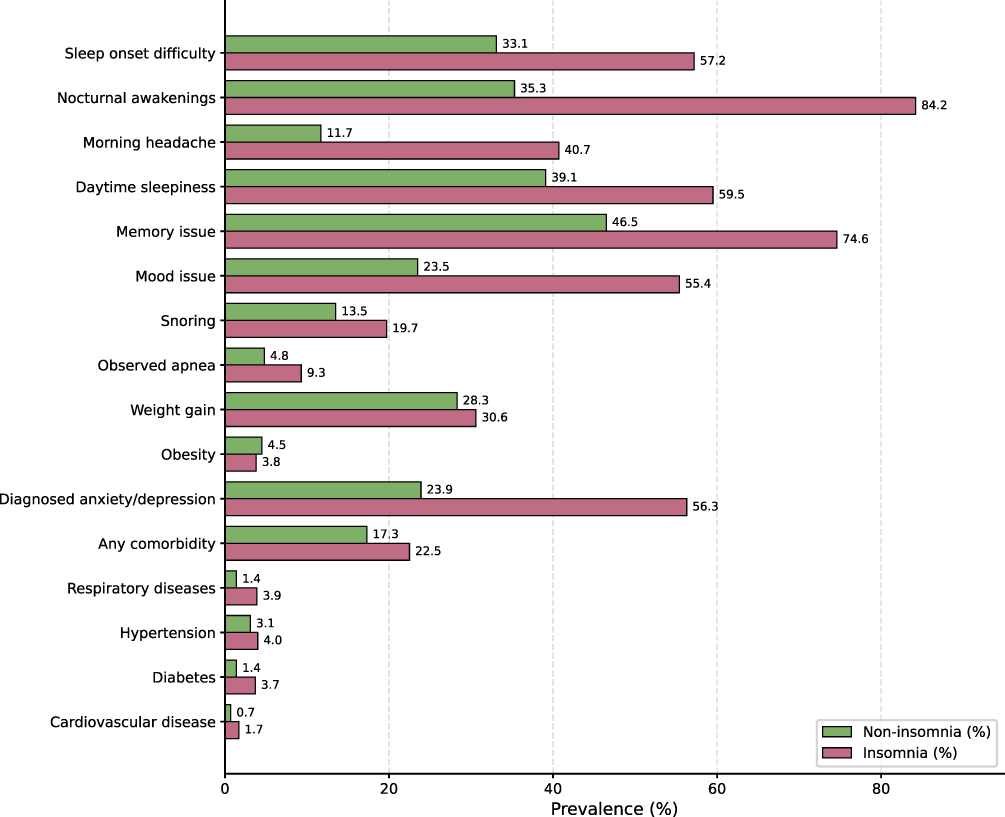 |
Figure 2 Comparison of clinical features between insomnia and non-insomnia. |
Factors Associated with Insomnia in Study Participants
In univariate analyses, insomnia was strongly associated with nocturnal awakenings (OR = 9.82, 95% CI: 7.33–13.16), morning headache (OR = 5.16, 95% CI: 3.96–6.71), and diagnosed anxiety or depression (OR = 4.11, 95% CI: 3.24–5.20; Table 3 and Figure 3A). In multivariable logistic regression analysis, tea or coffee consumption remained independently associated with insomnia (adjusted OR [aOR] = 2.10, 95% CI: 1.38–3.21, p < 0.001), as did alcohol use (aOR = 1.98, 95% CI: 1.11–3.52; p = 0.021).
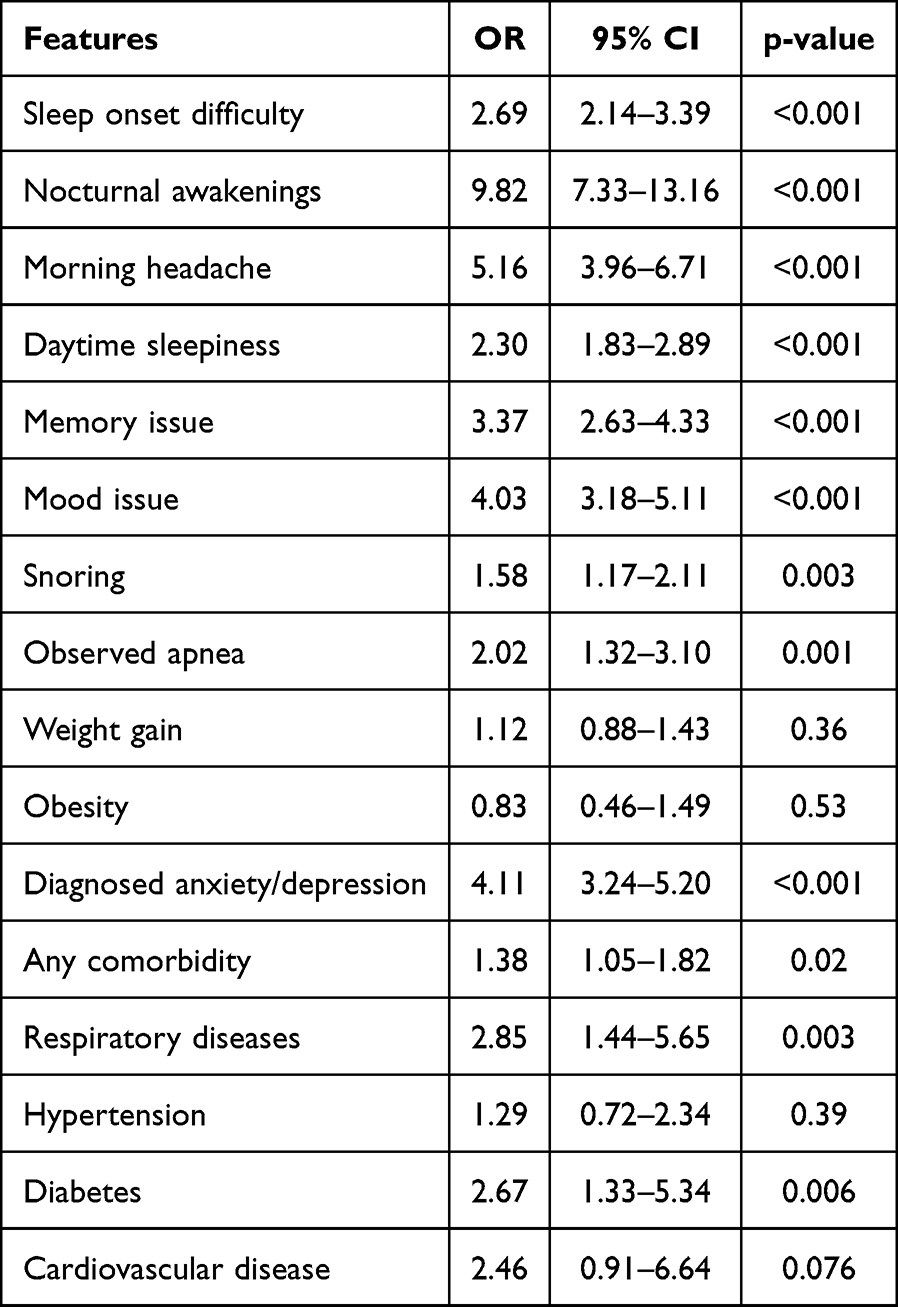 |
Table 3 Association Between Clinical Features and Insomnia Status |
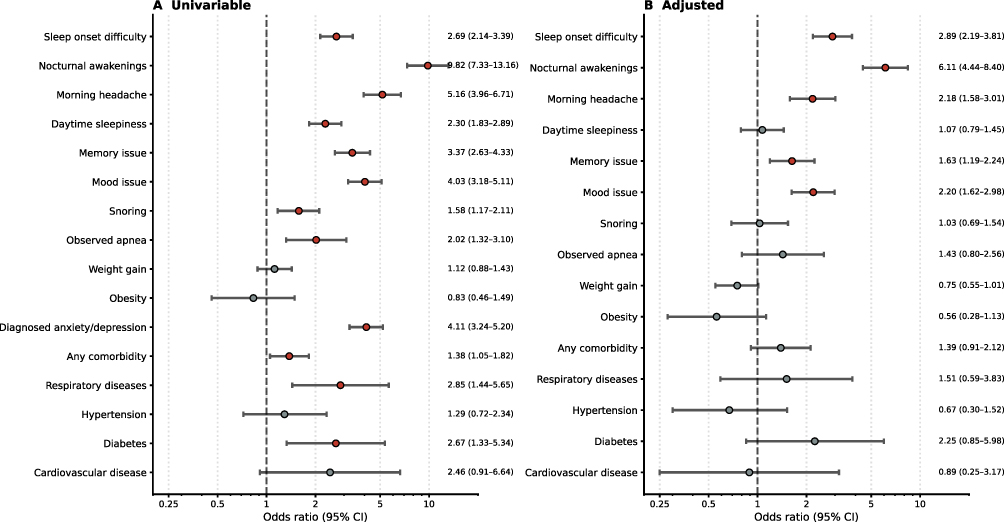 |
Figure 3 (A) Features associated with insomnia in study participants; (B) Adjusted features associated with insomnia. |
In multivariable logistic regression analysis adjusting for age, sex, occupation, marital status, and stimulant use, nocturnal awakenings remained the strongest independent associated factor of insomnia (aOR = 6.11). Sleep onset difficulty was associated with nearly threefold increased odds (aOR= 2.89). Mood issues, morning headache, and memory complaints were also independently associated with insomnia (aOR = 2.20, 2.18, and 1.63, respectively; Table 4 and Figure 3B). Diabetes (aOR 2.25; p = 0.104) and daytime sleepiness (aOR 1.07; p = 0.674) did not reach statistical significance after adjustment and were therefore reported as non-significant trends only. In contrast, obesity, hypertension, weight gain, and cardiovascular disease were not independently associated after adjustment (Table 4 and Figure 3B).
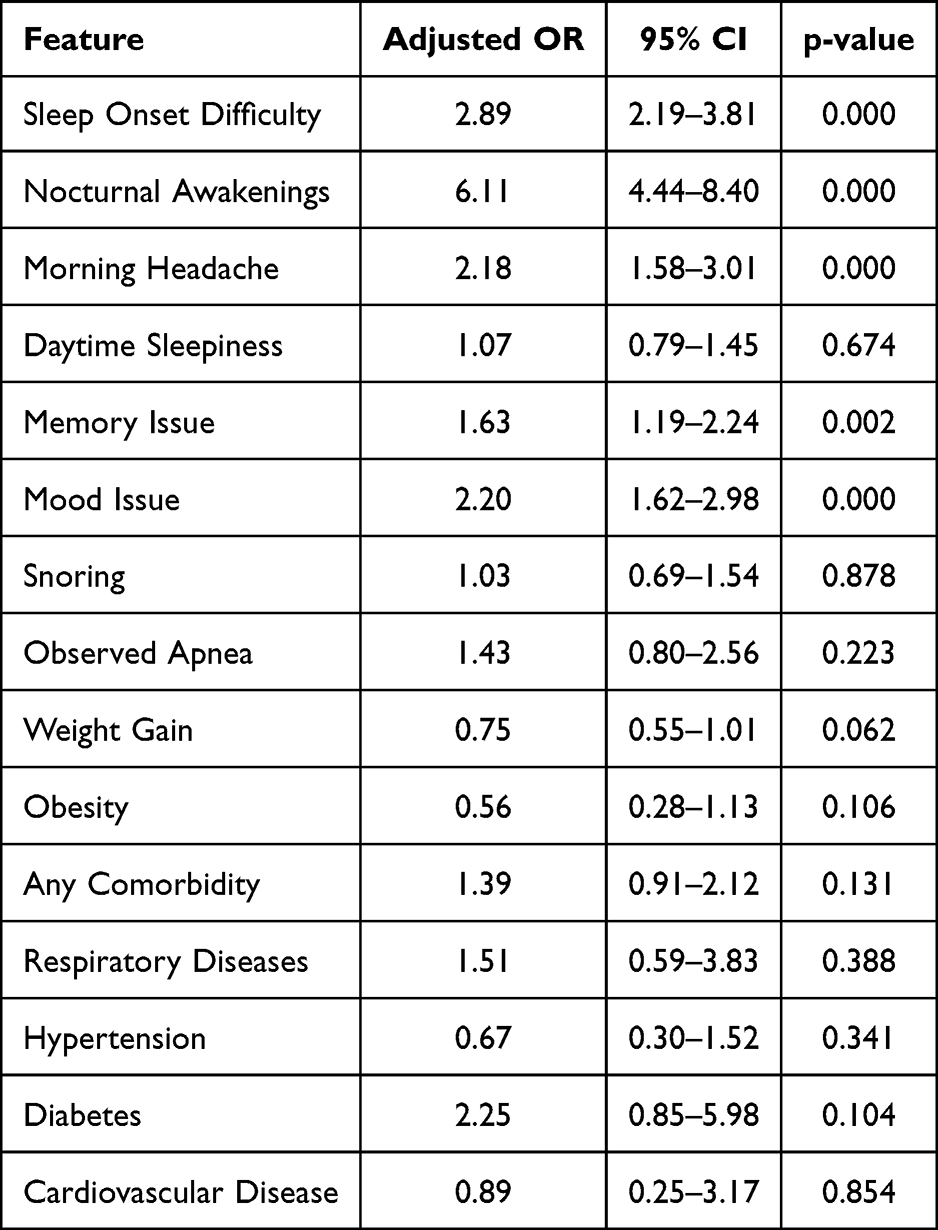 |
Table 4 Clinical Features Associated with Insomnia and Adjusted for Age, Sex, Occupation, Marital Status, and Stimulant Use |
Discussion
This nationwide multi-region study provides one of the first comprehensive evaluations of insomnia among healthcare professionals in Vietnam. We found that 24.2% of participants reported insomnia, a prevalence comparable to lower-bound estimates reported internationally among healthcare workers (25–42%) and substantially higher than that observed in the general population (12–16%).1,14 During the COVID-19 pandemic, prevalence reached 39–50%,8,10,15 and it remains clinically meaningful and highlights persistent occupational sleep vulnerability beyond the acute pandemic period.
Consistent with prior studies,2,8 in the present study, insomnia prevalence was higher among women and increased with age (Table 1 and Figure 1A). These demographic patterns likely reflect combined biological, psychosocial, and occupational mechanisms. Female healthcare workers may experience a higher burden of work–family conflict and emotional labor, while older professionals may accumulate chronic sleep debt and cardiometabolic vulnerability. Within the available occupational data, the only significant profession-level signal was the lower insomnia prevalence among physicians compared with the overall sample (19.6% vs 24.2%; p = 0.011). Differences across the other professional groups did not reach statistical significance. This suggestive workforce-level signal is not definitive evidence of occupational causation.
In the present study, the multivariable analysis identified nocturnal awakenings as the strongest independent associated factor (aOR 6.11), followed by sleep-onset difficulty (aOR 2.89) (Table 4 and Figure 3B). However, these two variables are core symptoms used to define insomnia, and their high adjusted odds ratio should therefore be interpreted as reflecting within-syndrome severity. The remaining adjusted associations involve mood disturbances (aOR 2.20) and memory complaints (aOR 1.63), which are best understood as bidirectional accompanying features of insomnia. These findings reinforce the conceptualization of insomnia not merely as difficulty initiating sleep but as a multidimensional disorder involving sleep maintenance disruption and daytime dysfunction. European insomnia guidelines emphasize that nocturnal fragmentation is strongly associated with neurocognitive and emotional consequences.16 The association between insomnia and mood symptoms observed in our cohort aligns with robust evidence demonstrating bidirectional relationships between insomnia, anxiety, and depression.17 By contrast, the external clinical and behavioral correlates included in the model (morning headache, snoring, observed apnea, anthropometric items, comorbidities, and stimulant use) do not overlap with the case definition; among these, stimulant use and morning headache are the most policy-relevant modifiable factors for occupational health interventions.
From a patient safety perspective, these findings are particularly concerning. Sleep disturbance among clinicians has been associated with reduced vigilance, slower reaction time, and increased risk of medical errors.18–20 The Institute of Medicine and subsequent safety analyses have identified fatigue and sleep deprivation as modifiable contributors to adverse events.21 In this context, our findings suggest that addressing insomnia is not solely a personal wellness issue but a systems-level patient safety priority.
The findings of the present study underscore the urgent need for structured interventions to prevent and manage insomnia among healthcare professionals. At the clinical level, evidence-based approaches such as Cognitive Behavioral Therapy for Insomnia (CBT-I), acupressure, and Progressive Muscle Relaxation should be incorporated into occupational health programs, with consideration for scalable digital delivery platforms to enhance accessibility and adherence.22–25 Complementary strategies, including mindfulness-based stress reduction, structured physical activity programs, and targeted sleep hygiene education, may further support sleep restoration and resilience.26
Importantly, fatigue risk management systems should be formally integrated into institutional safety culture, similar to high-reliability industries such as aviation, where systematic monitoring and mitigation of fatigue-related risks are standard practice.27
The study’s strengths include a large and diverse sample, enhancing the representativeness and potential generalizability of the findings. The use of a standardized questionnaire ensured consistency in data collection, while multivariable modeling enabled adjustment for predefined covariates. However, several limitations should be acknowledged. First, the reliance on self-reported sleep measures introduces inherent biases associated with subjective assessment, including recall bias and social desirability bias. Unlike objective evaluations such as actigraphy or polysomnography, which provide physiological and behavioral validation, self-reported data do not directly measure sleep architecture or continuity and may overestimate total sleep duration or underestimate sleep fragmentation. Second, the study did not include systematic screening for obstructive sleep apnea (OSA), particularly among participants with comorbid insomnia symptoms (ie, potential COMISA cases). Given the recognized overlap between insomnia and OSA, the absence of objective OSA assessment may have led to residual confounding and misclassification of sleep-related breathing disorders within the insomnia group. Especially, the prevalence of OSA is also high in healthcare professionals in Vietnam as demonstrated previously.9 Additionally, although the study covered institutions across all three major regions of Vietnam, recruitment was based on convenience sampling at the institutional level via the VSSM network, and the sample is not a probability-based representation of the national healthcare workforce. Lastly, although insomnia was operationalized using the ICSD-3 criteria framework, the assessment relied on a self-reported structured questionnaire rather than a clinician-administered diagnostic interview, and daytime impairments were captured as Yes/No symptom items rather than full validated instruments such as the ESS, PHQ-9, or GAD-7. Future PIHEP follow-up waves should incorporate validated instruments and objective sleep assessments to enable finer-grained characterization of insomnia phenotypes and daytime consequences. These limitations warrant caution when interpreting and generalizing the findings; nevertheless, they do not diminish the overall contribution of the study, given its rigorous methodology and comprehensive analytical approach.
Conclusion
Chronic insomnia is common among healthcare professionals in Vietnam and is associated with nocturnal sleep symptoms, morning headache, mood and memory complaints, and stimulant consumption (tea/coffee, alcohol). Physicians showing a lower prevalence than the overall sample suggest that workforce-level factors warrant further investigation. Findings should be interpreted as associational, given the cross-sectional design and the use of self-reported measures.
These results highlight the importance of systematic screening for insomnia within occupational health programs serving Vietnamese healthcare professionals, with attention to older personnel and individuals with elevated nocturnal symptom burden. The recommendations include reducing modifiable behavioral exposures and considering CBT-I or digitally delivered sleep interventions for affected staff, as supported by international evidence. Confirmatory prospective and interventional studies, ideally incorporating structured shift-schedule measurement and objective sleep assessment, are needed before organizational policy reforms can be recommended with confidence. Future PIHEP waves are planned to address these gaps.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, SDQ, upon reasonable request.
Ethics
The study was approved by the Institutional Review Board of Vietnam Society of Sleep Medicine (HYHGN-VN-NCKH-03-24). Participation was voluntary and anonymous. Informed consent was obtained electronically. All procedures were conducted in accordance with the Declaration of Helsinki.
Author Contributions
Sy Duong-Quy and Dung Nguyen-Thi-Thu share first Authorship.
Duong-Quy: Conceptualization; Methodology; Formal analysis; Writing – original draft; Writing – review & editing; Supervision; Project administration.
Dung Nguyen-Thi-Thu: Methodology; Formal analysis; Data curation; Investigation; Writing – original draft; Writing – review & editing.
Huong Hoang-Thi-Xuan: Data curation; Investigation; Writing – original draft; Writing – review & editing.
Lam Nguyen-Tung: Formal analysis; Writing – original draft; Writing – review & editing.
Hoa Bui-Ngoc-Phuong: Data curation; Investigation; Writing – review & editing.
Linh Tran-Thanh-Duy: Formal analysis; Writing – review & editing.
Thu Nguyen-Ngoc-Phuong: Methodology; Formal analysis; Writing – original draft; Writing – review & editing.
Tram Tang-Thi-Thao: Methodology; Formal analysis; Writing – original draft; Writing – review & editing.
Thai Nguyen-Duy: Data curation; Investigation; Writing – review & editing.
Bang Nguyen-Trong: Methodology; Validation; Writing – review & editing.
Lien Nguyen-Thi-Hong: Data curation; Investigation; Writing – review & editing.
Trang Tran-Thi-Doan: Data curation; Investigation; Writing – review & editing.
Thuy Phan-Thanh: Investigation; Writing – review & editing.
Khue Bui-Diem: Data curation; Investigation; Writing – review & editing.
Bo Tran-Thi-Mong: Investigation; Writing – review & editing.
Phap Tran Quang: Investigation; Writing – review & editing.
Toi Nguyen-Van: Data curation; Investigation; Writing – review & editing.
Anh Nguyen-Tuan: Investigation; Writing – review & editing.
Tram Vu-Doan: Data curation; Investigation; Writing – review & editing.
Thuc Pham-Van: Methodology; Validation; Writing – review & editing.
Trung Mai-Xuan: Investigation; Writing – review & editing.
Nghia Phan-Thanh: Investigation; Writing – review & editing.
Viet Nguyen-Ba: Investigation; Writing – review & editing.
Tuyen Hoang-Thanh: Investigation; Writing – review & editing.
Thuy Tran-Phan-Chung: Data curation; Investigation; Writing – review & editing.
Huong Le-Thi-Minh: Data curation; Investigation; Writing – review & editing.
Vinh Nguyen-Nhu: Data curation; Validation; Writing – review & editing.
Linh Pham-Van: Methodology; Validation; Writing – review & editing.
Bao Le-Khac: Investigation; Writing – review & editing.
Giap Vu-Van: Investigation; Validation; Writing – review & editing.
Franck Soyez: Conceptualization; Writing – review & editing; Supervision.
Thomas Penzel: Conceptualization; Writing – review & editing; Supervision.
Clete Kushida: Conceptualization; Writing – review & editing; Supervision.
Francis Martin: Conceptualization; Writing – review & editing; Supervision.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this study.
Disclosure
Dr Thomas Penzel reports personal fees from Bayer Healthcare, personal fees from Medical Learning Institute, personal fees from Takeda, personal fees from Idorsia, outside the submitted work; and is the President of the World Sleep Society. All other authors report no furtherconflicts of interest in this work.
References
1. Benjafield AV, Sert Kuniyoshi FH, Malhotra A, et al. Estimation of the global prevalence and burden of insomnia: a systematic literature review-based analysis. Sleep Med Rev. 2025;82:102121. doi:10.1016/j.smrv.2025.102121
2. Al Maqbali M, Al Sinani M, Al-Lenjawi B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: a systematic review and meta-analysis. J Psychosom Res. 2021;141:110343. doi:10.1016/j.jpsychores.2020.110343
3. Shahzad S, Sattar MA, Malik FN, Aqib M, Sattar A. Data-driven insights into predictors of stress and sleep health among Pakistani healthcare workers under rotational shifts. Sci Rep. 2025;15(1):41468. doi:10.1038/s41598-025-28872-z
4. Zhao X, Zhang L, Zhang X, et al. The prevalence and risk factors of shift work disorder among nurses: a systematic review and meta-analysis. Int J Nurs Stud. 2026;174:105273. doi:10.1016/j.ijnurstu.2025.105273
5. Trockel MT, Menon NK, Rowe SG, et al. Assessment of physician sleep and wellness, burnout, and clinically significant medical errors. JAMA Network Open. 2020;3(12):e2028111. doi:10.1001/jamanetworkopen.2020.28111
6. Fox J, McGrail M, Cha YJ, et al. A mixed-methods systematic review of sleep duration and quality in healthcare workers: impacts on patient safety and quality of care. Behav Sleep Med. 2025;23(5):698–13. doi:10.1080/15402002.2025.2522682
7. Weaver MD, Vetter C, Rajaratnam SMW, et al. Sleep disorders, depression and anxiety are associated with adverse safety outcomes in healthcare workers: a prospective cohort study. J Sleep Res. 2018;27(6):e12722. doi:10.1111/jsr.12722
8. Wright KP, Bogan RK, Wyatt JK. Shift work and the assessment and management of shift work disorder (SWD). Sleep Med Rev. 2013;17(1):41–54. doi:10.1016/j.smrv.2012.02.002
9. Duong-Quy S, Nguyen-Duy T, Hoc TV, et al. Self-administered home sleep testing model in screening of OSA in healthcare workers-sohew study: a national multicenter study in Vietnam. Pulm Ther. 2025;11(4):625–643. doi:10.1007/s41030-025-00315-0
10. Duong-Quy S, Tran-Duc S, Hoang-Chau-Bao D, Bui-Diem K, Vu-Tran-Thien Q, Nguyen-Nhu V. Tiredness, depression, and sleep disorders in frontline healthcare workers during COVID-19 pandemic in Vietnam: a field hospital study. Front Psychiatry. 2022;13:984658. doi:10.3389/fpsyt.2022.984658
11. Phan T, Nguyen HPA, Dang CK, et al. Sleep quality and poor sleep-related factors among healthcare workers during the COVID-19 pandemic in Vietnam. J Prev Med Public Health. 2023;56(4):319–326. doi:10.3961/jpmph.22.528
12. Van Nguyen T, Liu HE. A cross-sectional study on sleep disturbances and associated factors among nurses. BMC Psychiatry. 2022;22(1):119. doi:10.1186/s12888-022-03748-y
13. Grech V, Eldawlatly AA. STROBE, CONSORT, PRISMA, MOOSE, STARD, SPIRIT, and other guidelines - Overview and application. Saudi J Anaesth. 2024;18(1):137–141. doi:10.4103/sja.sja_545_23
14. van Straten A, Weinreich KJ, Fábián B, et al. The prevalence of insomnia disorder in the general population: a meta-analysis. J Sleep Res. 2025;34(5):e70089. doi:10.1111/jsr.70089
15. Batra K, Singh TP, Sharma M, Batra R, Schvaneveldt N. Investigating the psychological impact of COVID-19 among healthcare workers: a meta-analysis. Int J Environ Res Public Health. 2020;17(23):9096. doi:10.3390/ijerph17239096
16. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700. doi:10.1111/jsr.12594
17. Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev. 2019;43:96–105. doi:10.1016/j.smrv.2018.10.006
18. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995–1000. doi:10.1097/SLA.0b013e3181bfdab3
19. Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013;17(4):241–254. doi:10.1016/j.smrv.2012.09.005
20. Ganesan S, Magee M, Stone JE, et al. The impact of shift work on sleep, alertness and performance in healthcare workers. Sci Rep. 2019;9(1):4635. doi:10.1038/s41598-019-40914-x
21. Lockley SW, Barger LK, Ayas NT, Rothschild JM, Czeisler CA, Landrigan CP. Effects of health care provider work hours and sleep deprivation on safety and performance. Jt Comm J Qual Patient Saf. 2007;33(11 Suppl):7–18. doi:10.1016/s1553-7250(07)33109-7
22. Alimoradi Z, Jafari E, Broström A, et al. Effects of cognitive behavioral therapy for insomnia (CBT-I) on quality of life: a systematic review and meta-analysis. Sleep Med Rev. 2022;64:101646. doi:10.1016/j.smrv.2022.101646
23. Yeung WF, Chung KF, Poon MM, et al. Acupressure, reflexology, and auricular acupressure for insomnia: a systematic review of randomized controlled trials. Sleep Med. 2012;13(8):971–984. doi:10.1016/j.sleep.2012.06.003
24. Hoang HTX, Molassiotis A, Chan CW, Vu AH, Bui PT. Pilot randomized sham-controlled trial of self-acupressure to manage the symptom cluster of insomnia, depression, and anxiety in cancer patients undergoing chemotherapy. Sleep Breath. 2022;26(1):445–456. doi:10.1007/s11325-021-02370-8
25. Muhammad Khir S, Wan Mohd Yunus WMA, Mahmud N, et al. Efficacy of progressive muscle relaxation in adults for stress, anxiety, and depression: a systematic review. Psychol Res Behav Manag. 2024;17:345–365. doi:10.2147/prbm.S437277
26. Li H, Qin W, Li N, et al. Effect of mindfulness on anxiety and depression in insomnia patients: a systematic review and meta-analysis. Front Psychiatry. 2023;14:1124344. doi:10.3389/fpsyt.2023.1124344
27. Dorrian J, Lamond N, van den Heuvel C, Pincombe J, Rogers AE, Dawson D. A pilot study of the safety implications of Australian nurses’ sleep and work hours. Chronobiol Int. 2006;23(6):1149–1163. doi:10.1080/07420520601059615
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.