Back to Archived Journals » Integrated Blood Pressure Control » Volume 13
Prevalence of Hypertensive Emergency and Associated Factors Among Hospitalized Patients with Hypertensive Crisis: A Retrospective Cross-Sectional Study
Authors Desta DM ![]() , Wondafrash DZ
, Wondafrash DZ ![]() , Tsadik AG
, Tsadik AG ![]() , Kasahun GG
, Kasahun GG ![]() , Tassew S
, Tassew S ![]() , Gebrehiwot T
, Gebrehiwot T ![]() , Asgedom SW
, Asgedom SW
Received 29 May 2020
Accepted for publication 3 August 2020
Published 18 August 2020 Volume 2020:13 Pages 95—102
DOI https://doi.org/10.2147/IBPC.S265183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Desilu Mahari Desta,1 Dawit Zewdu Wondafrash,2 Afewerki Gebremeskel Tsadik,1 Gebremicheal Gebreslassie Kasahun,3 Segen Tassew,1 Teklu Gebrehiwot,1 Solomon Weldegebreal Asgedom1
1Clinical Pharmacy Unit, School of Pharmacy, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia; 2Department of Pharmacology and Toxicology, School of Pharmacy, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia; 3Department of Pharmacy, College of Health Sciences, Aksum University, Aksum, Tigray, Ethiopia
Correspondence: Desilu Mahari Desta
Clinical Pharmacy Unit, School of Pharmacy, College of Health Sciences, Mekelle University, P.O. Box: 1871, Mekelle, Tigray, Ethiopia
Tel +251-914681245
Email [email protected]
Background: Hypertensive emergency (HE) is an acute stage of uncontrolled blood pressure which poses a substantial cardiovascular morbidity and mortality in developing countries. In our setting, the prevalence of HE and the characteristics of patients with a hypertensive crisis are not certainly known yet.
Objective: The study assessed the prevalence of hypertensive emergency and associated factors among hospitalized patients with hypertensive crisis.
Methods: A retrospective cross-sectional study was conducted by reviewing records of patients having a diagnosis of hypertensive crisis with systolic/diastolic blood pressure raised to more than 180/120 mmHg admitted to Ayder Comprehensive Specialized Hospital (ACSH) from September 2018 to August 2019. Patients’ medical records with complete information were enrolled consecutively. Socio-demographic, clinical characteristics, and other related variables were collected using a structured data collection tool from patient medical records. Data were entered and analyzed using SPSS version 20. Logistic regression was employed to determine factors associated with HE.
Results: A total of 141 patients’ records with a diagnosis of a hypertensive crisis were enrolled in the study; the majority were females 77 (54.6%) and residing in the urban setting 104 (73.8%). The mean age of the participants was 58.8 years. HE was found in 42 (29.8%) of patients. Intravenous Hydralazine 39 (27.7%) and oral calcium channel blocker 102 (72.3%) were the prescribed drugs for acute blood pressure reduction in the emergency setting. Surprisingly, patients who had no history of hypertension (adjusted odds ratio (AOR)=2.469; 95% confidence interval (CI): 0.176‒0.933) and female sex (AOR=2.494; 95% CI: 1.111‒5.596) were found to be independently associated factors with HE.
Conclusion: The prevalence of HE was found to account a significant proportion of patients. Hence, hypertensive patients should be strictly managed accordingly, and promoting screening programs could reduce the risk of target organ damage.
Keywords: hypertensive crisis, hypertensive emergency, hypertensive urgency, target organ damage
Background
Hypertension is a major public health challenge worldwide because of its high prevalence and concomitant increase in the risk of cardiovascular diseases.1 Globally, the proportion of hypertension was estimated to rise to over 29% by 2025 and more than 80% of deaths from hypertension and associated cardiovascular diseases occur in low and middle-income countries.2
Despite the presence of adequate interventions, uncontrolled hypertension is still a substantial cause of cardiovascular diseases.3 Thus, sub-optimal blood pressure (BP) control can result in a hypertensive crisis when systolic blood pressure/diastolic blood pressure (SBP/DBP) is more than 180/120 mmHg.4,5 Hypertensive crisis is classified in the form of hypertensive emergency and urgency; HE is characterized by the presence of target organ damage unlike hypertensive urgency.6
According to the report of different studies, the incidence of HE is increasing. A study conducted in an emergency setting of the United States claimed that HE was increased from 3309 per million in 2006 to 6178 per million cases in 2013.7 The study done from Tanzania revealed that among hypertensive patients admitted to the emergency department about 68% of patients developed HE.8 Similarly, Papadopoulos and his co-authors found that HE accounted 24% of hypertensive crisis cases. Moreover, the study revealed that cerebral infarction (24%), acute pulmonary edema (23%), hypertensive encephalopathy (16%), and cerebral hemorrhage (4.5%) were the involved target organ damages.9 Besides, the Joint National Committee eighth (JNC8) reported that the commonly involved end-organ damages are stroke, cardiac and renal injuries.10
In hypertensive crisis patients, immediate use of anti-hypertensive medications should be started as soon as possible. BP should be monitored carefully to prevent target organ damage and hypotensive effect of the BP-lowering agents in emergency.11 In a hypertensive emergency, BP should reduce by 20% to 25% within minutes to one hour then after to 160/100 mmHg after two to six hours and then gradually to normal in the next one up to two days.12
In Ethiopia, the prevalence of uncontrolled blood pressure is increasing which might predispose patients to HE. A cross-sectional study conducted in Ayder Comprehensive Specialized Hospital (ACSH) among hypertensive patients showed that about 52.5% of the participants had uncontrolled BP status.13
The present study assessed the blood pressure control trend, magnitude of HE and associated factors among hypertensive crisis patients admitted to ACSH. To the best of our knowledge, there have been no published studies in this respect, in the Tigray region of Ethiopia. The study will contribute a lot to improve health-care service; delivering a clue for policymakers, health-care providers, patients, and the community at large on the risk of morbidity and mortality of HE.
Methods
Study Design, Period and Area
A retrospective cross-sectional study was employed by reviewing records of patients with a diagnosis of hypertensive crisis admitted from September 2018‒August 2019 to ACSH, found in Mekelle the capital city of Tigray regional state, 783 km away from Addis Ababa, Ethiopia. The hospital delivers 24 hours full service of emergency care service in its emergency department.
Study Population
Adult patients presented to the emergency setting with a diagnosis of hypertensive crisis who had complete information on their medical records and admitted during the study period were included. Admission and discharge patient registration book from the emergency department was used to find the medical record number of patients having a diagnosis of hypertensive crisis. All patients who fulfilled the inclusion criteria were consecutively included in the study.
Eligibility Criteria
Adult patients with a diagnosis of hypertensive crisis presented to the emergency setting of ACSH from September 2018‒August 2019 who had complete medical record information were deemed eligible. However, patients who had SBP/DBP of ≤180/120, admitted out of the range of the study period and with incomplete medical record information were excluded from the study.
Sample Size and Sampling Technique
About 159 patients’ medical records were found with a diagnosis of hypertensive crisis within the study period, while 11 of them were excluded because of incomplete information, and then 148 patients’ records were found eligible for the study. Furthermore, seven patients’ medical records were used for the pre-test. Lastly, 141 patient medical records were enrolled in the actual study consecutively.
Data Collection Process
The data collection was carried out using a structured data collection tool. The tool was developed by reviewing different relevant literatures8,14–18 and pre-test was done in 5% (seven patients) of them, then after an amendment of the data abstraction tool was undertaken. Four pharmacists who had clinical pharmacy service experience were recruited for data collection. One day training was given to the data collectors by the principal investigator. Supervision was done daily basis by the principal investigator to assure the completeness of the data.
Data Analysis and Interpretation
Data were entered and analyzed using SPSS version 20. Descriptive statistics such as frequency, percentage, mean and SD were determined to summarize the patient’s characteristics and other variables. Bivariate logistic regression was used to determine factors associated with hypertensive emergency at 95% of confidence level and p≤0.25. Furthermore, multivariate logistic regression analysis was carried out for the adjustment of potential confounders and p≤0.05 was considered as statistically significant.
Operational Definitions
Hypertensive crisis case was confirmed when patients had admission SBP record of above 180 mmHg and DBP of over 120 mmHg in the emergency department. Hypertensive crisis is classified into hypertension urgency and emergency, whereby HE is characterized by elevation of SBP/DBP and presence of at least one target organ damage involvement. Hypertensive urgency was deemed SBP/DBP elevation with no evidence of target organ damage. Target organ damage was considered as the presence of evidence of hypertensive encephalopathy, stroke, myocardial infraction, acute pulmonary edema, major bleeding episode, major arrhythmia, and acute renal failure.19,20
Results
Of the total 141 patients medical records reviewed; more than half of them were females 77 (54.6%) and urban residents accounted for 104 (73.8%). The mean age of the patients was 58.8 years (mean ± SD, ± 14.6); patients in the range of 45–64 years attributed to 78 (55.3%). Near to two-thirds of the patients 96 (68.1%) were previously on anti-hypertensive management. Among the medical history/risk factors for admission, the previous history of hypertension was found to be the most abundant 105 (74.5%), followed by diabetes mellitus 23 (16.3%). Stroke was found to be the most common complication which accounted for 27 (19.1%). Almost all of the patients 130 (92.2%) were discharged with improvement, while death was recorded in a few patients 11 (7.8%). Besides, about 102 (72.3%) were taking Nifedipine and 39 (27.7%) patients were prescribed intravenous Hydralazine (Table 1).
 |
Table 1 Sociodemographic and Clinical Characteristics of Patients with Hypertensive Crisis Admitted to Ayder Comprehensive Specialized Hospital, Mekelle, Ethiopia from September 2018‒October 2019 |
As illustrated in Figure 1, HE was recorded in more than one-fourth of patients 42 (29.8%), whereas more than two-thirds of patients 99 (70.2%) had not any evidence of target organ damage. Regarding patients presentation in admission; headache was the most reported symptom (55, 39%), followed by nausea and vomiting (30, 21.3%) and then right/left body weakness (24, 17%) (Figure 2).
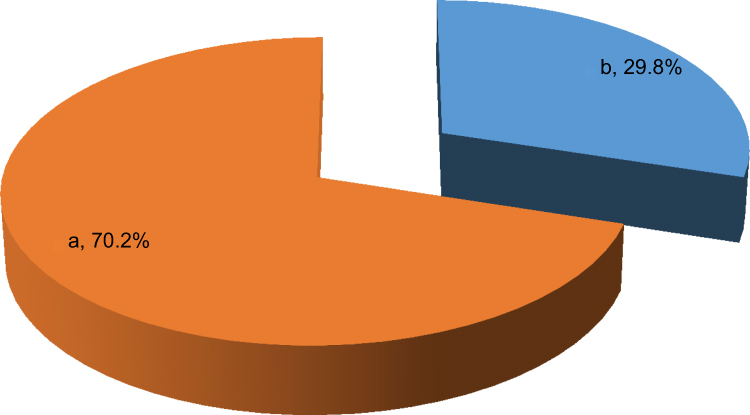 |
Figure 1 Proportion of hypertensive emergency and urgency among patients with hypertensive crisis admitted to Ayder Comprehensive Specialized Hospital, Mekelle, Ethiopia from September 2018‒October 2019. a – hypertensive urgency. b – hypertensive emergency. |
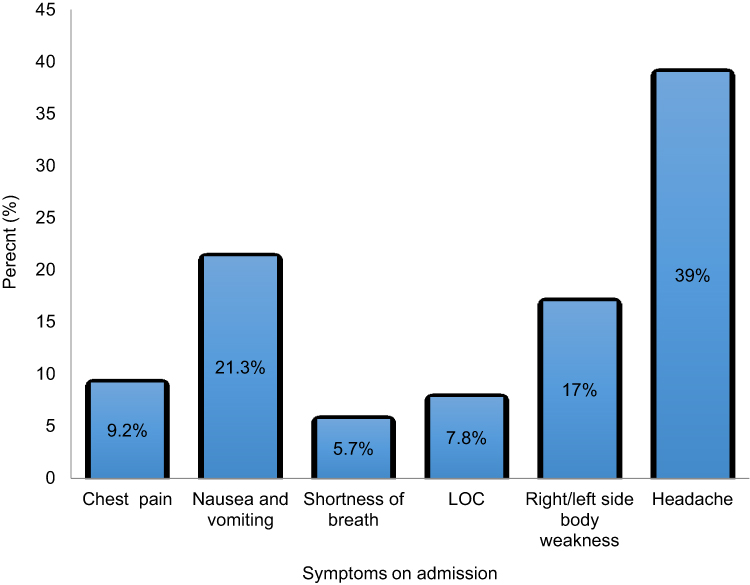 |
Figure 2 Admission symptoms of hypertensive crisis patients admitted to Ayder Comprehensive Specialized Hospital, Mekelle, Ethiopia from September 2018‒October 2019. Abbreviation: LOC, loss of consciousness. |
The mean SBP at admission, after one hour and at discharge was found to be 198.6 mmHg (SD ± 19.4), 184.7 (±15), 132.7 mmHg (± 14.3), respectively. Furthermore, the mean DBP at admission, after one hour and discharge was 111.6 (± 13.5), 106.3 (± 14.3), 81.9 (±12.1) mmHg, respectively, and showed that there was a progressive reduction in blood pressure from admission to discharge, while the mean discharge SBP/DBP was found to be in the normal limit (Figure 3).
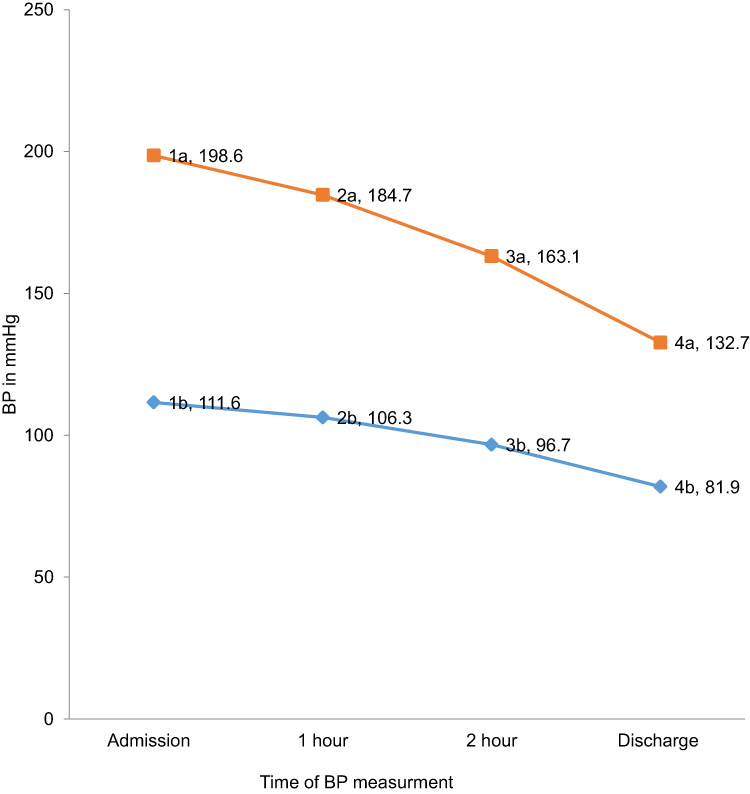 |
Figure 3 Mean of blood pressure control pattern and trend of patients with hypertensive crises admitted to Ayder Comprehensive Specialized Hospital, Mekelle, Ethiopia from September 2018‒October 2019. 1a measured systolic blood pressure at admission. 2a measured systolic blood pressure after one hour. 3a measured systolic blood pressure after two hours. 4a measured systolic blood pressure at discharge. 1b measured diastolic blood pressure at admission. 2b measured diastolic blood pressure after one hour. 3b measured diastolic blood pressure after two hours. 4b measured diastolic blood pressure at discharge.Abbreviations: BP, blood pressure; DBP, diastolic blood pressure; SBP, systolic blood pressure. |
The case of factors associated with HE, on binary logistic regression; gender, age, and patients with no history of hypertension were significantly associated with the incidence of HE. Further analysis by multivariate logistic regression showed that patients who had no history of hypertension (adjusted odds ratio (AOR)=0.405; 95% CI (confidence interval): 0.176‒0.933) and female sex (AOR=2.494; 95% CI: 1.111‒5.596) were found independently associated factors with HE (Table 2).
 |
Table 2 Factors Associated with Hypertensive Emergency Among Patients with Hypertensive Crisis Admitted to Ayder Comprehensive Specialized Hospital, Mekelle, Ethiopia from September 2018‒October 2019 |
Discussion
In this study, an attempt was made to assess characteristics of hypertensive crisis, the magnitude of hypertensive emergency, and factors associated with HE. In addition, the mean of BP control trend of the patients was assessed from admission time up to discharge at different times of measurement.
In the current study, 74.5% were a known hypertensive patients previously. This finding is relatively similar to a study from Angola in which 65.9% of patients with the hypertensive crisis were known as hypertensive patients.21 Similarly, another study from India revealed hypertensive emergency was associated with patients being hypertensive previously (P=0.0029).14 Inline with our study, a finding from Cilegon, Banten claimed that a high proportion of patients with HE (93.54%) had the previous history of hypertension than those with hypertensive urgency (86.84%).15 The possible reason might be due to the adherence problem of hypertensive patients to medication and lifestyle adjustment. This was explained by a study conducted in eastern Sudan, whereby poor compliance was associated with an increased risk of hypertensive crisis development (p=0.002).22
Concerning the prevalence of hypertensive emergency, in the present study, hypertensive emergency accounted for 29.8% of the hypertensive crisis cases. Our finding was comparable with the study conducted among African-American patients, in which hypertensive emergencies accounted for 28%,23 Brazil 39.6%,16 and in Gondar, Ethiopia 40.3%.18 However, our finding was relatively lower than studies conducted in; Ghana 47.5%,24 Tanzania 68%,8 eastern Sudan 61.7%,22 Congo 76%,25 Uganda 67.5%14 and Brazil 63.8%.26 The plausible reason for this inconsistency might be due to differences in sample size and variation in the study setting. In this study, stroke was found to be the most abundant complication (19.1%), followed by congestive heart failure (9.2%). Our finding was consistent with a study conducted in Congo, where the common target organ damages were stroke (32%) and heart failure (24.6%).25 Another similar study conducted in Sudan claimed that stroke (30.8%), followed by heart failure (22.2%) were the common target organ damage as a result of hypertensive crisis.22
Regarding the factors associated with the hypertensive emergency, the present study showed that female patients were 2.494 times more likely to develop hypertensive emergencies than males (95% CI: 1.111‒5.596). This might be due to more than half of the patients (54.6%) were females in our study. Similarly, a study conducted by Saguner and his co-authors reported that female sex was significantly associated with hypertensive crisis (P<0.01).27 The plausible reason could be that those female patients might have less awareness of hypertension-related cardiovascular complications.28,29 In contrast to our finding, a study conducted in Brazil revealed that men were at a high risk of developing hypertensive emergencies than women (55.3% vs, 44.7%, respectively).16 This discrepancy might be due to differences in sample size and study setting.
Furthermore, the current study revealed that patients who had no history of hypertension were 2.469 times less likely to develop HE than those who were already hypertensive patients (AOR=0.405; 95% CI: 0.176‒0.933). The plausible reason could be that hypertensive patients might have a good awareness of their BP control, hypertension-related cardiovascular complications, regular monitoring, and follow up.30,31 This was explained by other studies too; on the study conducted by Karmacharya and Paudel, among the hypertensive patients majority of them (73.1%) had awareness of cardiovascular complications of hypertension.32 Another similar study from Iran revealed that about 60% of hypertensive patients had adequate knowledge of hypertension-related complications.33 Furthermore, from the study conducted in Pakistan, about two-thirds of them (69.1%) had regular checkup of their blood pressure status.34
The study has certain limitations such as; retrospective cross-sectional study design, single centered, and small sample size used.
Conclusion
HE accounted considerably significant proportion of patients in the setup. Newly diagnosed hypertensive and female patients were found to be more likely to develop target organ damage. Hence, hypertensive patients should be strictly followed, counseled and screening of hypertension could help to prevent and reduce the risk of target organ damage. Moreover, a multicenter prospective study should be done over the country at large to certainly figure out the prevalence of HE and mortality of patients after they admitted to emergency departments with a hypertensive crisis.
Abbreviations
ACSH, Ayder Comprehensive Specialized Hospital; AOR, adjusted odds ratio; BP, blood pressure; CI, confidence interval; DBP, diastolic blood pressure; HE, hypertensive emergency; JNC8, Joint National Committee eight; SBP, systolic blood pressure; SD, standard deviation.
Data Sharing Statement
The data sets supporting the conclusions of the study are included in the article. Any additional supplementary material will be available on request.
Ethics Approval
Ethical clearance was obtained from the Ethical Review Board (ERB) committee of College of Health Science, Mekelle University, and letter of support were also issued from the medical director office of ACSH to access patients’ medical records. The patient’s record number was replaced using codes to reassure confidentiality.
Acknowledgments
We thank the management of Ayder Comprehensive Specialized Hospital for invaluable assistance in conducting the study. We also thank data collectors and other staff members for their assistance with this study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. World Health Organization. A global brief on hypertension: silent killer, global public health crisis: world health day 2013. World Health Organization. 2013. Available from: https://apps.who.int/iris/handle/10665/79059.
2. Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217–223. doi:10.1016/S0140-6736(05)17741-1
3. Almas A, Ghouse A, Iftikhar AR, Khursheed M. Hypertensive crisis, burden, management, and outcome at a tertiary care center in karachi. Int J Chronic Dis. 2014;2014. doi:10.1155/2014/413071
4. Rodriguez MA, Kumar SK, De Caro M. Hypertensive crisis. Cardiol Rev. 2010;18(2):102–107. doi:10.1097/CRD.0b013e3181c307b7
5. Gegenhuber A, Lenz K. Hypertensive emergency and urgence. Herz. 2003;28(8):717. doi:10.1007/s00059-003-2506-8
6. Aggarwal M, Khan IA. Hypertensive crisis: hypertensive emergencies and urgencies. Cardiol Clin. 2006;24(1):135–146. doi:10.1016/j.ccl.2005.09.002
7. Janke AT, McNaughton CD, Brody AM, Welch RD, Levy PD. Trends in the incidence of hypertensive emergencies in US emergency departments from 2006 to 2013. J Am Heart Assoc. 2016;5(12):e004511. doi:10.1161/JAHA.116.004511
8. Shao PJ, Sawe HR, Murray BL, Mfinanga JA, Mwafongo V, Runyon MS. Profile of patients with hypertensive urgency and emergency presenting to an urban emergency department of a tertiary referral hospital in Tanzania. BMC Cardiovasc Disord. 2018;18(1):158. doi:10.1186/s12872-018-0895-0
9. Papadopoulos DP, Mourouzis I, Thomopoulos C, Makris T, Papademetriou V. Hypertension crisis. Blood Press. 2010;19(6):328–336. doi:10.3109/08037051.2010.488052
10. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
11. Baurenski L, Trendafilova E. Blood pressure reduction and outcome in patients with hypertensive crisis and acute ischemic stroke. J Hypertens. 2018;36(Supplement 1):e89. doi:10.1097/01.hjh.0000539222.88275.68
12. Papadopoulos D, Sanidas E, Viniou N, et al. Cardiovascular hypertensive emergencies. Curr Hypertens Rep. 2015;17(2):5. doi:10.1007/s11906-014-0515-z
13. Gebremichael GB, Berhe KK, Zemichael TM. Uncontrolled hypertension and associated factors among adult hypertensive patients in Ayder comprehensive specialized hospital, Tigray, Ethiopia, 2018. BMC Cardiovasc Disord. 2019;19(1):121. doi:10.1186/s12872-019-1091-6
14. Manjhvar SK, Thakare S, Gupta H, Indurkar M. Clinical study of hypertensive crisis in medicine ward. Int J Contemp Med Res. 2017;14(11):2258–2261.
15. Onggo SI, Wiharja W, Sutisna B, Sutisna N, Taslim A. 2 clinical profile and epidemiology of hypertensive crisis at emergency unit in Cilegon, Banten. J Hypertens. 2018;36:e1. doi:10.1097/01.hjh.0000544367.43184.52
16. Martin J, Higashiama E, Garcia E, Luizon MR, Cipullo JP. Hypertensive crisis profile. Prevalence and clinical presentation. Arq Bras Cardiol. 2004;83(2):131. doi:10.1590/s0066-782x2004001400004
17. Nakalema I, Kaddumukasa M, Nakibuuka J, Okello E, Sajatovic M, Katabira E. Prevalence, patterns and factors associated with hypertensive crises in Mulago hospital emergency department; a cross-sectional study. Afr Health Sci. 2019;19(1):1757–1767. doi:10.4314/ahs.v19i1.52
18. Abegaz TM, Tefera YG, Befekadu Abebe T. Target organ damage and the long term effect of nonadherence to clinical practice guidelines in patients with hypertension: a retrospective cohort study. Int J Hypertens. 2017;2017. doi:10.1155/2017/2637051
19. Brook RD, Rajagopalan S. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Soc Hypertens. 2018;12(3):238.
20. Varounis C, Katsi V, Nihoyannopoulos P, Lekakis J, Tousoulis D. Cardiovascular hypertensive crisis: recent evidence and review of the literature. Front Cardiovasc Med. 2017;3:51. doi:10.3389/fcvm.2016.00051
21. García GM, Miúdo V, Lopes C, Gomes JV. Characterization of patients aged 45 or under admitted with hypertensive emergencies in the Hospital do Prenda. Rev Port Cardiol. 2014;33(1):19–25. doi:10.1016/j.repce.2013.04.013
22. Abdallah TM, Ibrahem AA, Ali EA, Ahmed EG, Ali AA. Clinico-epidemiological characteristics and survival outcome of patients with hypertensive crisis at Kassala Hospital, Eastern Sudan. J Crit Care Med. 2018;3:029–034. doi:10.29328/journal.jcicm.1001017
23. Waldron FA, Benenson I, Jones-Dillon SA, et al. Prevalence and risk factors for hypertensive crisis in a predominantly African American inner-city community. Blood Press. 2019;28(2):114–123. doi:10.1080/08037051.2019.1568183
24. Addo J, Smeeth L, Leon DA, von Elm E. Hypertensive target organ damage in Ghanaian civil servants with hypertension. PLoS One. 2009;4(8):e6672. doi:10.1371/journal.pone.0006672
25. Kadima JN, Bavhure B, Sepa JD, Murhura D. Hypertensive urgencies or emergencies and co-morbidities in Bukavu Referral Hospitals: clinical profile, management regimens, outcomes and drug related problems. J Basic Clin Pharmacol. 2018;9(1).
26. Vilela-Martin JF, Vaz-de-Melo RO, Kuniyoshi CH, Abdo ANR, Yugar-Toledo JC. Hypertensive crisis: clinical–epidemiological profile. Hypertens Res. 2011;34(3):367–371. doi:10.1038/hr.2010.245
27. Saguner AM, Dür S, Perrig M, et al. Risk factors promoting hypertensive crises: evidence from a longitudinal study. Am J Hypertens. 2010;23(7):775–780. doi:10.1038/ajh.2010.71
28. Gudmundsdottir H, Høieggen A, Stenehjem A, Waldum B, Os I. Hypertension in women: latest findings and clinical implications. Ther Adv Chronic Dis. 2012;3(3):137–146. doi:10.1177/2040622312438935
29. Everett B, Zajacova A. Gender differences in hypertension and hypertension awareness among young adults. Biodemography Soc Biol. 2015;61(1):1–17. doi:10.1080/19485565.2014.929488
30. Kumar A, Dwivedi A, Chaturvdi AK, Kumar R. Hypertension – the silent killer, awareness of risk factors and complications in Rohilkhand region. Int J Contemp Med Res. 2018;5(3):C35–C37.
31. Hien HA, Tam NM, Tam V, Derese A, Devroey D. Prevalence, awareness, treatment, and control of hypertension and its risk factors in (central) vietnam. Int J Hypertens. 2018;2018. doi:10.1155/2018/6326984
32. Karmacharya R, Paudel K. Research article awareness on hypertension and its self-management practices among hypertensive patients in Pokhara, western Nepal. J Interdiscip Stud. 2017;6:110–120. doi:10.3126/jjis.v6i0.19313
33. Rashidi Y, Manaflouyan H, Azar FP, Nikniaz Z, Nikniaz L, Ghaffari S. Knowledge, attitude and practice of Iranian hypertensive patients regarding hypertension. J Cardiovasc Thorac Res. 2018;10(1):14. doi:10.15171/jcvtr.2018.02
34. Bilal M, Haseeb A, Lashkerwala SS, et al. Knowledge, awareness and self-care practices of hypertension among cardiac hypertensive patients. Glob J Health Sci. 2016;8(2):9. doi:10.5539/gjhs.v8n2p9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.