")
Back to Journals » International Journal of Women's Health » Volume 14
Prevalence of Gynecological Related Symptoms and Quality of Life in Women Living with HIV/AIDS: a Secondary Analysis from an Online, Cross-Sectional Survey in China
Received 7 April 2022
Accepted for publication 18 September 2022
Published 28 September 2022 Volume 2022:14 Pages 1425—1433
DOI https://doi.org/10.2147/IJWH.S369781
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Meilian Xie,1,2 Aiping Wang,1 Zhaoxia Lin3
1Department of Public Service, the First Affiliated Hospital of China Medical University, Shenyang, Liaoning Province, People’s Republic of China; 2Department of Nursing, Beijing Ditan Hospital Capital Medical University, Beijing, People’s Republic of China; 3Infection Center, Beijing Ditan Hospital Capital Medical University, Beijing, People’s Republic of China
Correspondence: Aiping Wang, Department of Public Service, the First affiliated Hospital of China Medical University, Shenyang, People’s Republic of China, Email [email protected]
Objective: Our study aims to completely understand the experience of gynecological related symptoms (GRS) and the association between GRS and quality of life (QOL) among HIV-infected women in China.
Design: A cross-sectional, multicenter survey.
Setting: The HIV/AIDS designated medical institutions of seven regions in China.
Participants: One hundred and fifty-three women with HIV infection.
Primary and Secondary Outcome Measures: Primary outcome measures included the score of GRS and QOL from analysis sample.
Results: Among 153 participants, 60.13% were asymptomatic, and 39.87% were symptomatic according to their self-report data. In the symptomatic group, 47.54% reported only one symptom, 18.03% reported 2 symptoms, others reported more than 3 symptoms. The most common symptoms were vaginal discharge (25.49%), followed by irregular period (18.95%), bad cramps (13.07%), vaginal odor (11.11%), and vaginal itching (10.46%). The mean score of QOL was 86.82 ± 15.53. The symptomatic group had higher score than the asymptomatic group on each domain of QOL. GRS were negatively correlated with QOL after adjustment for confounding factors. Correlation matrix of GRS and six domains of QOL demonstrated significant negative correlation with each domain of QOL, especially the most strongly negative correlation with physical function of participants. But the association between GRS and environmental domain was weaker.
Conclusion: These findings present the multidimensionality of common gynecologic related symptoms and highlight the clinically meaningful associations between GRS and quality of life among women with HIV infection in China. There is an urgent need to take measures to increase vaginal care and education in advance, delivered by trusted health professionals.
Keywords: women living with HIV/AIDS, symptoms, gynecologic related symptoms, quality of life
Introduction
HIV continues to be a major global public health issue, having claimed almost 36.3 million (27.2–47.8 million) lives so far.1 Of people living with HIV, women account for nearly 55% (19.96 million) worldwide at the end of 2020.2 Joint United Nations Program on HIV/AIDS3 made a statement in 2021 that about 4500 women aged 15–24 years acquire HIV every week, and young women are twice as likely as men to be living with HIV/AIDS, which remains one of the leading causes of death for women aged 15–49 years globally. In China, the HIV epidemic continues to grow, especially the number of women living with HIV/AIDS (WLWHA), which reached more than 270,000 at the end of 2020, compared with 180,000 in 2010.4 Health issues about WLWHA have been increasing worldwide, but is often overlooked.
The related theories and practices of symptom management5–7 show that symptom occurrence is an important factor affecting the well-being and quality of life (QOL) of patients including people with HIV. Thus, an understanding of symptoms can be essential to improve the health of this population and develop strategies to support adherence to HIV clinical care. Among adolescent and adult women, gynecologic related symptoms (GRS) can be very widespread and range from menstrual irregularities to amenorrhea, also from vaginitis to ovarian polycystosis.8 Several studies have indicated that WLWHA may experience different symptom profiles or menopause at an earlier age than their HIV-negative counterparts,9,10 caused by lower levels of antimullerian hormone (a biological marker of ovarian reserve),11 suggesting ovarian dysfunction earlier. Scientists found that the pathophysiology underlying ovarian dysfunction in WLWHA was likely to be the effects of the virus itself and opportunistic infection on the ovaries and the pituitary gland.12
However, a large number of researches more focused on menopausal symptoms in the last few decades have revealed that menopausal symptoms have consistently impacted negatively upon WLWHA’s quality of life and their social role crossing various sociocultural contexts.10,13 It is known that many young women infected with HIV may have other gynecologic related symptoms. A few studies about GRS are significant because WLWHA who often delay seeking health care are primarily diagnosed with gynecologic related AIDS-defining conditions leading to receiving further medical treatment.14–16 The presence of GRS was significantly predictive of disease progression, and early identification may be lead to health interventions earlier in WLWHA.14 With the advent of a new era of antiretroviral therapy (ART) medication, the disease courses among people with HIV have been changing. Especially GRS in the Chinese women infected with HIV need to be further described clearly. In addition, we also do not know how the burden from GRS affects WLWHA’s quality of life in various dimensions.
Our study objectives are: (1) to describe the prevalence, frequency, severity, and distress of GRS among HIV-infected women at designated medical institutions in China, (2) to describe the status of QOL and its six domains in HIV-infected women in the new era of ART, and (3) to examine the extent to which demographic characteristics, HIV clinical status, and GRS influence QOL domains in HIV-infected women.
Methods
Study Design and Setting
This is a secondary analysis from an existing dataset. On the basis of the latest analysis of spatial pattern and spatial-temporal evolution of AIDS, the study was conducted in seven provinces or municipalities with different levels of incidence, covering different parts of eastern, western, northern, and southern regions of China. A cross-sectional, descriptive design was used to gather self-reported data on of HIV-related symptoms and QOL domains among people with HIV infection in the HIV/AIDS designated medical institutions of seven regions in China.
Sample and Recruitment
Participants were purposively sampled using a non-probability technique from November 2021 to January 2022. Participants were invited to take part in the study by investigators of the research team. In view of representativeness, we took into account differences in age and residential conditions during recruitment. We conducted the same proportionate recruitment process in each region based on these factors. Eligibility to participate in the study included being aged 18 years or older, and having a confirmed HIV diagnosis. Excluded participants were those diagnosed with serious comorbidities, patients with cognitive impairment, and those who were unable to complete the survey. Before proceeding to the official survey, the potential participants signed an online informed consent form which disclosed ethics issues in the study.
Data Collection
Data were collected using a serial questionnaire administered by the research team.
Sociodemographic and Clinical Data
The first section gathered information about the sociodemographic and clinical status of respondents including age, education, family income, employment of the participants, HIV duration, ART medication, CD4+ T cell count, disease staging, and so on.
Gynecologic Related Symptoms(GRS)
The second section gathered data on GRS of women according to Vincenzi’s views. Gynecologic related items from the revised Sign and Symptom Check-List for HIV (SSC-HIV rev)17 and the dimensions of the Memorial Symptom Assessment Scale (MSAS)18 were integrated, which was one reliable and valid measurement.19 These participants were asked to characterize their experience concerning that particular symptom across the following four dimensions: yes or no of symptoms, frequency, severity, and distress. The frequency and severity were evaluated with a four-point Likert scale using the following options: 1 = “Rarely/Slight”, 2 = “Occasionally/Moderate”, 3 = “Frequently/Severe”, 4 = “Almost constantly/Very severe”. The distress of symptoms was rated by a five-point Likert scale: 0 = “Not at all”, 1 = “A little bit”, 2 = “Somewhat”, 3 = “Quite a bit”, 4 = “Very much”. If a symptom is absent, each dimension is scored as 0, and the score for that symptom is 0. If a symptom is present, the symptom score is an average of its dimensions. The scoring system yields several subscale scores, including Gynecologic Related Symptoms Frequency (GRSF), Gynecologic Related Symptoms Severity (GRSS), Gynecologic Related Symptoms Distress (GRSD). A higher score indicates a higher level of symptom frequency, severity, and distress.
Quality of Life
The WHOQOL-HIV BREF including 31 items covering six domains (Physical (PH), Psychological (PS), Independence (IN), Social (SO), Environment (EN), and Spirituality (SP)) was used in the survey, which was developed by WHO,20,21 and 31 items were rated on a five-point Likert scale. The domain scores were calculated by multiplying the mean of all items within the domain by 4. All domain scores ranged from 4 to 20. Higher scores in each domain indicated higher QOL for that domain. Cronbach’s α for the Chinese version of overall scale was 0.93, and the test–retest reliability revealed a statistically significant intraclass correlation coefficient of 0.72–0.82 (p<0.001).20
Ethical Consideration
This study was approved by the Institutional Review Board of Beijing Ditan Hospital Capital Medical University, reference number DTZZLX-202106. Informed consent to participate in the study was obtained from all participants, and respondents were provided with anonymity and confidentiality.
Data Analysis
Data were analyzed using the statistical software packages R 3.3.2 (http://www.R-project.org, The R Foundation) and Free Statistics software versions 1.5. Categorical variables were expressed as proportions (%). Continuous data were expressed as mean and standard deviation (SD), or median and interquartile range (IQR). Differences between groups were compared using the chi-square tests and t-test, Mann–Whitney U-test, respectively. The Multiple Linear Regression was used to explain the relationship between GRS and QOL among WLWHA. The correlation matrix was used to show how much each domain of QOL correlated with GRS. All the analyses were performed with a two-tailed test, and p < 0.05 was considered statistically significant.
Results
Participant Characteristics
A total of 153 women participants finished all online questions. All participants were aged between 18 and 67 years old (40.843 ± 11.779). Education of WLWHA showed that 114 (74.5%) had attained high school and below, 53.6% were married or cohabiting, and 67.97% were unemployed or freelance or retired. Table 1 displays the descriptive characteristics of this study population. Among 153 WLWHA, 60.13% were asymptomatic, and 39.87% were symptomatic according to their self-report data. There were no significant differences between the two groups on sociodemographic and clinical status (Table 1).
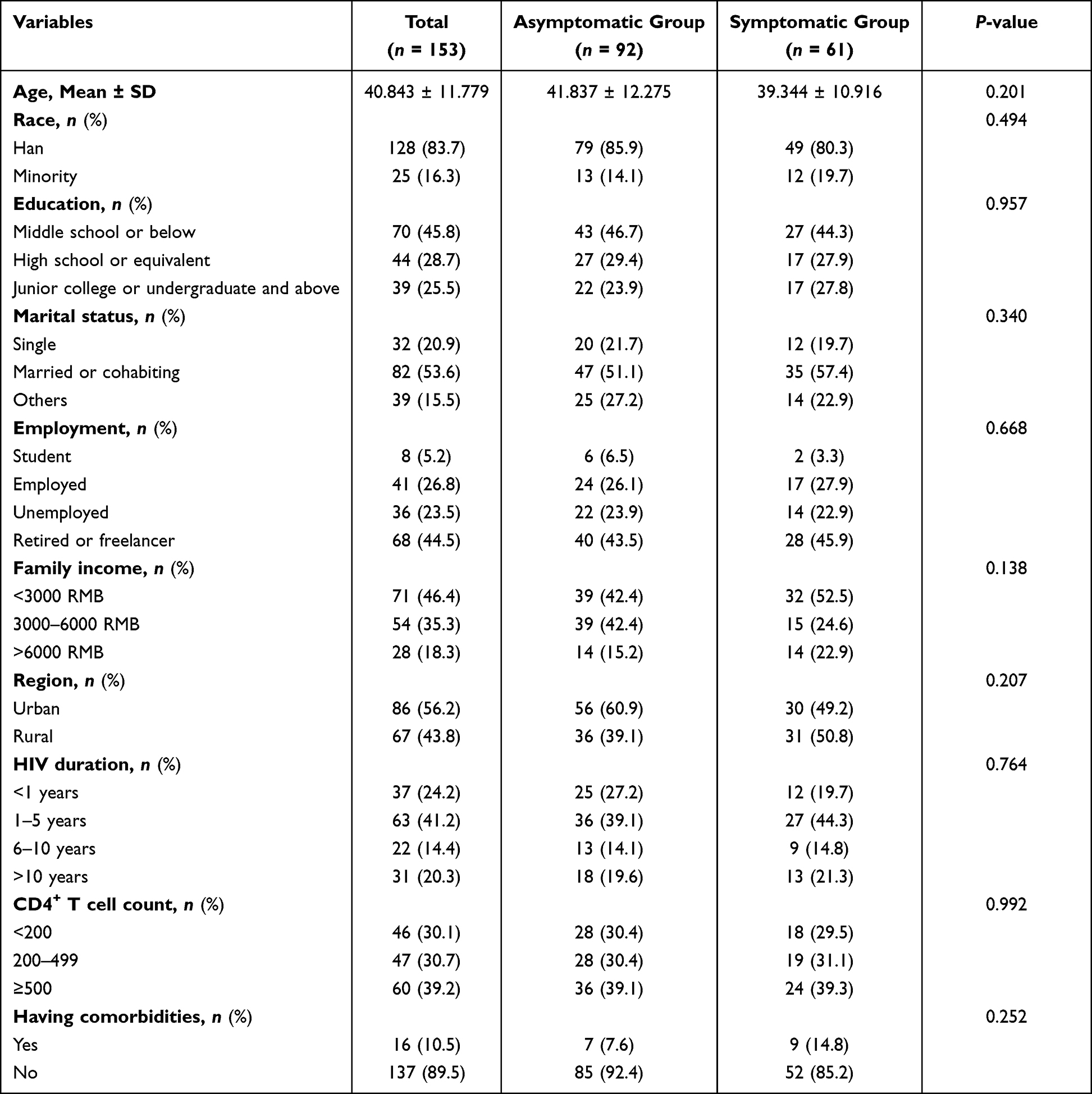 |
Table 1 Baseline Characteristics of Participants (N=153) |
Multidimensionality of Gynecological Related Symptoms
Table 2 shows that the frequency, severity, and distress of symptoms were reported to accord with prevalence. Among 61 WLWHA who reported having symptoms, 47.54% reported only one symptom, 18.03% reported 2 symptoms, others reported more than 3 symptoms. Of all symptoms reported, the most common GRS were vaginal discharge (25.49%), followed by irregular period (18.95%), bad cramps (13.07%), vaginal odor (11.11%), vaginal itching (10.46%), heavy period (5.88%), pelvic pain (5.23%), and bleeding between periods (3.92%) (Table 2). Most of GRS were reported by WLWHA aged nearly 40 years old, except younger WLWHA were subjected to heavy periods and older WLWHA were more likely to have pelvic pain.
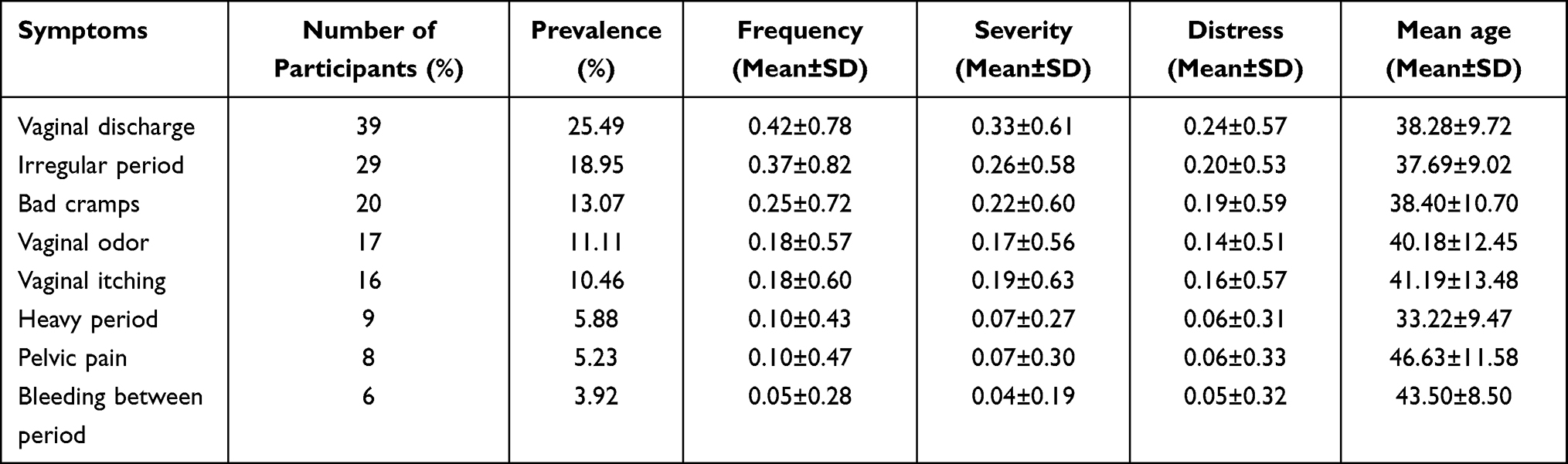 |
Table 2 Prevalence, Frequency, Severity, and Distress of Gynecological Related Symptoms |
QOL Status
The mean score of WLWHA’s QOL for all the domains of the questionnaire was 86.82 ± 15.53. Figure 1 reveals that the symptomatic group had a higher score than the asymptomatic group on each domain of QOL. Table 3 displays the association between GRS and QOL in all participants when confounding variables were considered. In the non-adjusted model, GRS were negatively correlated with QOL. After adjustment for confounding factors, the correlation still was stable. Correlation matrix of GRS and six domains of QOL, shown in Figure 2, demonstrated significant negative correlation with each domain of QOL, especially the most strongly negative correlation with physical function of participants. But the association between GRS and environmental well-being was weaker.
 |
Table 3 Association Between Gynecological Related Symptoms and Quality of Life in Multiple Regression Model |
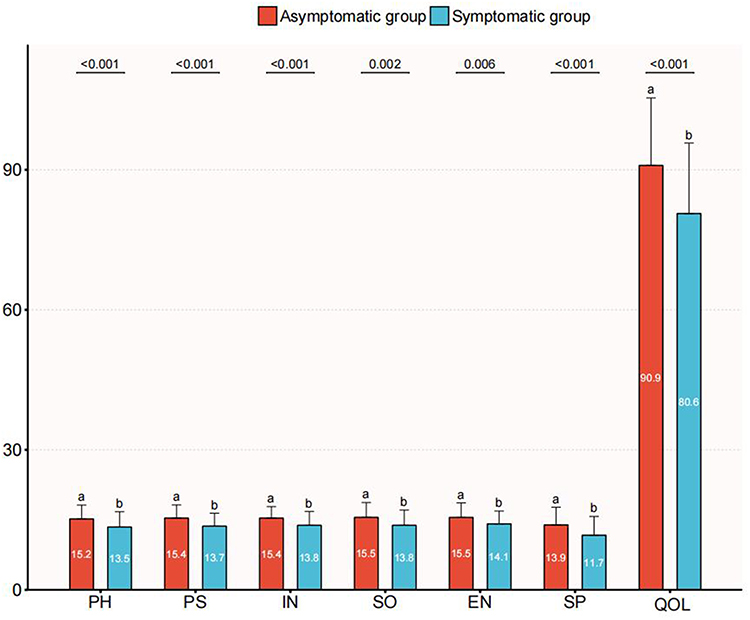 |
Figure 1 Differences in six domains of quality of life between asymptomatic WLWH and symptomatic WLWH. The scores of the two groups are compared with each domain of QOL, and this reveals that the symptomatic group has higher score than the asymptomatic group on each domain. The symbols “a” and “b” in this figure mean that scores of different groups are at different levels and there is some statistical significance between two groups. Abbreviations: PH, physical; PS, psychological; IN, independence; SO, social; EN, environment; SP, spirituality; QOL, quality of life. |
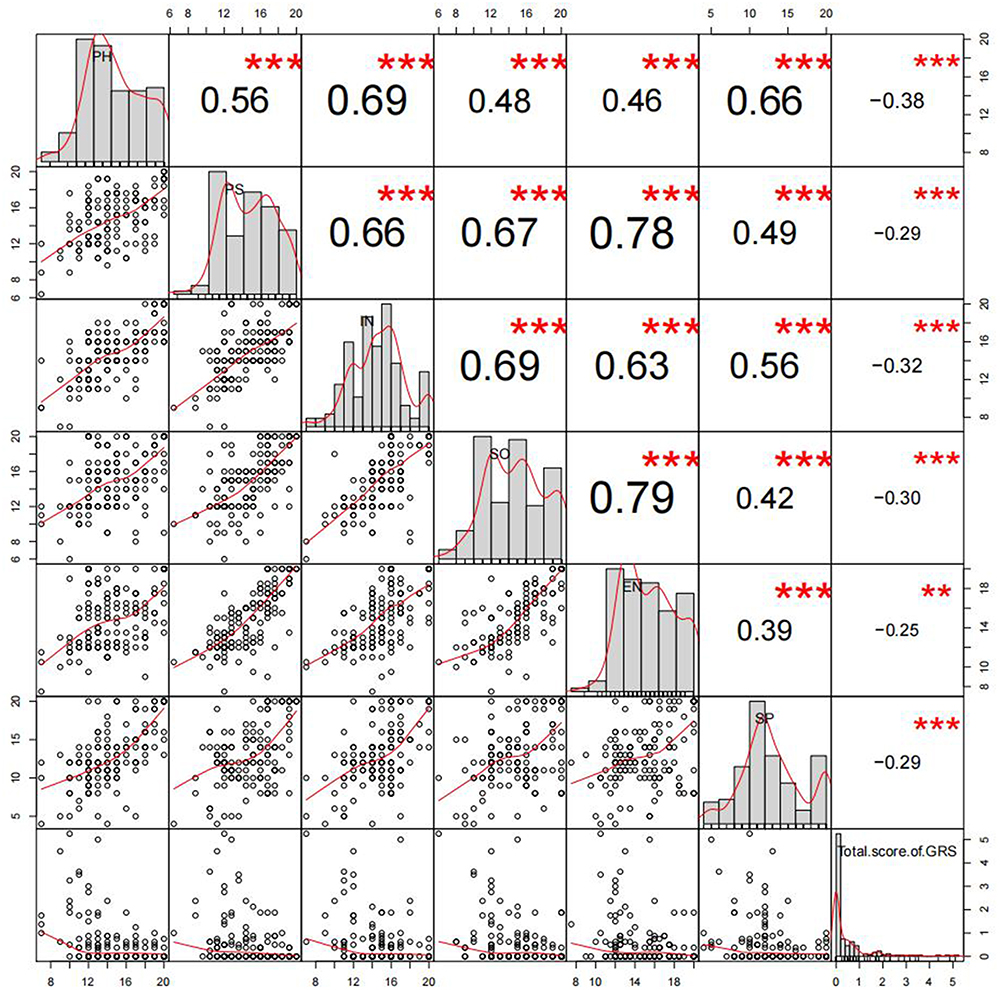 |
Figure 2 Correlation matrix of gynecological related symptoms and domains of QOL. It demonstrates significant negative correlation with each domain of QOL, especially the most strongly negative correlation with physical function of participants. But the association between GRS and environmental well-being is weaker. **p value < 0.01, ***p value < 0.001. Abbreviations: PH, physical; PS psychological; IN, independence; SO, social; EN, environment; SP, spirituality; QOL, quality of life. |
Discussion
This study further explored the multidimensionality of GRS, including prevalence, frequency, severity, and distress, as well as predicted the correlation with QOL domains among WLWHA in China. In addition, this is the first study describing the whole profile of GRS in a sample of WLWHA. What is more, the experience of GRS was transformed into quantifiable data through applying scientific measurements recommended by researchers.
Our results revealed that more than one-third of respondents reported experiencing one of the eight GRS, which is in accordance with previous research.22 Most of WLWHA only reported one or two symptoms, lower than the mean number of common HIV-related symptoms in the general population in similar studies. For example, a study from Wilson and his team showed a third of patients had seven or more symptoms,23 and another study conducted in China revealed that the median number of symptoms was nine among PLWH.24 However, as there is a lack of evidence or data on GRS from women with HIV worldwide, our study may be of value for further research. Since women have become a key population in fighting against HIV and are more likely to experience reluctance to disclose their disease, stigma, mental disorders, and gender-based violence or inequity,25–28 their self-report may be limited. We found that the most common GRS were vaginal discharge in Chinese WLWHA, similar to the most prevalent GRS of WLWHA in Houston or a sample from New England, who complained of more vaginal itching, vaginal discharge, vaginal pruritus, and bad cramps.16,22 All the above suggests that routine, comprehensive gynecologic evaluation should be given to all HIV-infected women. Additionally, healthcare providers should take scientific intervention strategies on vaginal care earlier. Our findings also demonstrated that there was no statistical significance on sociodemographic and clinical variables between symptomatic and asymptomatic groups. It seemed to present a key clue that the occurrence of GRS might not predict the disease condition, which was different from the previous study.16
Although the women we investigated were at the lower socioeconomic level and had lower educational background, their QOL was at least medium level. A study carried out in China explained that a family caregiver or partner participating in caring for these patients can promote physical QOL and decrease depressive symptomatology among Chinese HIV-infected women.29 Most of our sample were accompanied by partners, which may be a beneficial factor to improve their QOL. In addition, we found that asymptomatic women had higher QOL than the symptomatic group without statistical significances in all sociodemographic and clinical characteristics. Thus we believe that occurrence of gynecological related symptoms can frustrate individual perception of well-being, and healthcare providers should pay attention to these gynecologic symptoms of women with HIV infection. We also found that quality of life in women with HIV infection was affected by GRS after accounting for all potential related confounders, which was in accordance with previous study.14,22 Especially, the physical function and independence of WLWHA was most affected by GRS, while the environmental domain was less affected, suggesting that medical workers should invest more resources in coping with the cause of symptoms in WLWHA and help them explore new methods to stimulate the individual’s ability to perform activities or self-care.30
Conclusion
Gender inequality has been a key driver of the HIV/AIDS epidemic, and women patients should be given enough attention. The prevalence and multidimensionality of gynecological related symptoms suggested that the most common symptoms were vaginal related, and vaginal care or education should be essential to women with HIV infection in advance. The findings of our study also highlighted clinically meaningful associations between gynecological related symptoms and quality of life among women who have HIV. Thus, finding ways to reduce gynecological related symptoms has the potential to enhance the physical function but also to improve the individual’s independence, leading to better self-care or management of their disease. However, identification and deepening understanding of gynecological related symptoms should be dynamic activities, serving as the entry point of nursing care to enhance overall QOL.
Limitations of This Study
There are some limitations in this study. The analysis samples were small, leaving potential for bias. In our study, most of the variables were similar across the entire sample and analysis groups, and 153 WLWHA were selected from seven different regions in China in order to reduce the bias. We are also aware, however, these participants in our study were more reluctant to talk about diseases and their real feeling due to influence by traditional women culture in China, who were more likely to underestimate their GRS. As we know, GRS may be one of clusters among WLWHA, and clusters of symptoms often interact with each other to affect QOL of this population. Our study mainly focused on the GRS, lacking the identification of the impact of other symptom clusters on the quality of life, so further research will be explored. Additionally, the study was cross-sectional and exploratory, thus no causal explanations can be drawn.
Data Sharing Statement
All raw data and data files are provided by the lead researcher and corresponding author if necessary.
Ethics
The study complies with the Declaration of Helsinki on ethical principles for research involving human subjects. The study was approved by the Institutional Review Board of Beijing Ditan Hospital Capital Medical University, reference number DTZZLX-202106. We obtained informed consents from all participants and reassured them that their personal information would remain confidential.
Acknowledgments
We would like to express our special gratitude to all study participants for their time during data collection. We are grateful to our investigators who gave strong support to the study, especially Junli Cao from the First affiliated Hospital of China Medical University, Shenyang, Liaoning Province; Dandan Ma from Henan Infectious Diseases Hospital; Weixia Bai from Center for Disease Control and Prevention in Shuimogou District, Urumqi, Xinjiang; Liumei Xu from the Third People’s Hospital from Shenzhen, Guangdong Province; Zhihui Guo from Public Health Clinical Center of Chengdu, Sichuan Province; Yongjuan Yang from Chengzhong Center for Disease Control and Prevention, Xining, Qinghai Province; and Zhiyun Zhang, Kerong Wang, and Yanping Yu from Beijing Ditan Hospital.
Author Contributions
All authors made substantial contributions to design, acquisition of data, or analysis and interpretation of data. All authors took part in drafting the article or revising it critically for important content and agreed to submit to the current journal. All authors are responsible for the content and gave final approval of the version to be published.
Funding
This research received no specific grant from any funding agency in the public, commercial or non-profit sectors.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. World Health Organization. Key facts and latest estimates on the global HIV epidemic – 2020; 2020. Available from: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics.
2. Latest HIV estimates and updates on HIV policies uptake, December 2021; 2021. Available from:https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics.
3. UNAIDS.org. GLOBAL AIDS STRATEGY 2021–2026. 2021; DF-1.6 %¡³Å× 1 0 obj ≪/ArtBox[0 0 595.276 841.589]/BleedBox[590 590 595.276 841.589]/Contents 592 590 R /CropBox[590 590 595.276 841.589]/MediaBox[590 590 595.276 841.589]/Parent 932 590 R /PieceInfo<</InDesign<</DocumentID(þÿ. Available from:https://www.unaids.org/en/resources/documents/2021/2021-2026-global-AIDS-strategy.
4. World Health Organization. UNAIDS, UNICEF. Towards Universal Access: Scaling Up Priority HIV/AIDS Interventions in the Health Sector. Geneva: World Health Organization; 2010.
5. The University of California SFSoNSMFG. A model for symptom management. Image J Nurs Sch. 1994;26(4):272–276. doi:10.1111/j.1547-5069.1994.tb00333.x
6. Dodd M, Janson S, Facione N, et al. Advancing the science of symptom management. J Adv Nurs. 2001;33(5):668–676. doi:10.1046/j.1365-2648.2001.01697.x
7. Spirig R, Moody K, Battegay M, De Geest S. Symptom management in HIV/AIDS: advancing the conceptualization. ANS Adv Nurs Sci. 2005;28(4):333–344. doi:10.1097/00012272-200510000-00005
8. Milano W, Ambrosio P, Carizzone F, et al. Menstrual disorders related to eating disorders. Endocr Metab Immune Disord Drug Targets. 2021;4:548.
9. Tariq S, Anderson J, Burns F, Delpech V, Gilson R, Sabin C. The menopause transition in women living with HIV: current evidence and future avenues of research. J Virus Erad. 2016;2(2):114–116. doi:10.1016/S2055-6640(20)30476-3
10. Solomon D, Sabin CA, Burns F, et al. The association between severe menopausal symptoms and engagement with HIV care and treatment in women living with HIV. AIDS Care. 2021;33(1):101–108. doi:10.1080/09540121.2020.1748559
11. Scherzer R, Bacchetti P, Messerlian G, et al. Impact of CD4+ lymphocytes and HIV infection on Anti-Mullerian Hormone levels in a large cohort of HIV-infected and HIV-uninfected women. Am J Reprod Immunol. 2015;73(3):273–284. doi:10.1111/aji.12332
12. Rochira V, Guaraldi G. Hypogonadism in the HIV-infected man. Endocrinol Metab Clin North Am. 2014;43(3):709–730. doi:10.1016/j.ecl.2014.06.005
13. Thapa R, Yang Y, Bekemeier B. Menopausal symptoms and associated factors in women living with HIV in Cambodia. J Women Aging. 2020;32(5):517–536. doi:10.1080/08952841.2019.1593773
14. Hudson AL, Lee KA, Portillo CJ. Symptom experience and functional status among HIV-infected women. AIDS Care. 2003;15(4):483–492. doi:10.1080/0954012031000134728
15. Chirgwin KD, Feldman J, Muneyyirci-Delale O, Landesman S, Minkoff H. Menstrual function in human immunodeficiency virus-infected women without acquired immunodeficiency syndrome. J Acquir Immune Defic Syndr Hum Retrovirol. 1996;12(5):489–494. doi:10.1097/00042560-199608150-00008
16. Frankel RE, Selwyn PA, Mezger J, Andrews S. High prevalence of gynecologic disease among hospitalized women with human immunodeficiency virus infection. Clin Infect Dis. 1997;25(3):706–712. doi:10.1086/513775
17. Holzemer WL, Hudson A, Kirksey KM, Hamilton MJ, Bakken S. The revised Sign and Symptom Check-List for HIV (SSC-HIVrev). J Assoc Nurses AIDS Care. 2001;12(5):60–70. doi:10.1016/S1055-3290(06)60263-X
18. Cheng KK, Wong EM, Ling WM, Chan CW, Thompson DR. Measuring the symptom experience of Chinese cancer patients: a validation of the Chinese version of the memorial symptom assessment scale. J Pain Symptom Manage. 2009;37(1):44–57. doi:10.1016/j.jpainsymman.2007.12.019
19. Vincenzi CB, Moody K, Spirig R. Development and pretesting of a set of symptom assessment tools in HIV: the HIV Symptom Experience Assessment Scale and the HIV Symptom Manageability Scale. Appl Nurs Res. 2009;22(3):204–210. doi:10.1016/j.apnr.2007.10.002
20. Zhu Y, Liu J, Qu B. Psychometric properties of the Chinese version of the WHOQOL-HIV BREF to assess quality of life among people living with HIV/AIDS: a cross-sectional study. BMJ Open. 2017;7(8):e016382. doi:10.1136/bmjopen-2017-016382
21. Hiv Group W; WHOQOL-HIV-GROUP. WHOQOL-HIV for quality of life assessment among people living with HIV and AIDS: results from the field test. AIDS Care. 2004;16(7):882–889. doi:10.1080/09540120412331290194
22. Hudson A, Kirksey K, Holzemer W. The influence of symptoms on quality of life among HIV-infected women. West J Nurs Res. 2004;26(1):9–23. doi:10.1177/0193945903259221
23. Wilson NL, Azuero A, Vance DE, et al. Identifying Symptom Patterns in People Living With HIV Disease. J Assoc Nurses AIDS Care. 2016;27(2):121–132. doi:10.1016/j.jana.2015.11.009
24. Zhu Z, Hu Y, Xing W, et al. Identifying Symptom Clusters Among People Living With HIV on Antiretroviral Therapy in China: a Network Analysis. J Pain Symptom Manage. 2019;57(3):617–626. doi:10.1016/j.jpainsymman.2018.11.011
25. Logie CH, Wang Y, Lacombe-Duncan A, et al. HIV-related stigma, racial discrimination, and gender discrimination: pathways to physical and mental health-related quality of life among a national cohort of women living with HIV. Prev Med. 2018;107:36–44. doi:10.1016/j.ypmed.2017.12.018
26. Scofield D, Moseholm E. HIV-related stigma and health-related quality of life in women living with HIV in developed countries: a systematic review. AIDS Care. 2022;34(1):7–15. doi:10.1080/09540121.2021.1891193
27. Loutfy M, Johnson M, Walmsley S, et al. The Association Between HIV Disclosure Status and Perceived Barriers to Care Faced by Women Living with HIV in Latin America, China, Central/Eastern Europe, and Western Europe/Canada. AIDS Patient Care STDS. 2016;30(9):435–444. doi:10.1089/apc.2016.0049
28. Looby SE, Psaros C, Raggio G, et al. Association between HIV status and psychological symptoms in perimenopausal women. Menopause. 2018;25(6):648–656. doi:10.1097/GME.0000000000001058
29. Chen WT, Shiu C, Yang JP, et al. Quality of life in HIV-infected Chinese women and their family caregivers: an intervention study. AIDS Care. 2018;30(12):1572–1579. doi:10.1080/09540121.2018.1510095
30. WHO. The World Health Organization Quality of Life(WHOQOL); 2002. Available from:https://www.who.int/mental_health/publications/whoqol/en/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.