")
Back to Journals » Clinical Ophthalmology » Volume 17
Prevalence of Glaucoma Following Paediatric Cataract Surgery in an Australian Tertiary Referral Centre
Authors Wood A, Lim B, Matthews J , Karaconji T, Zagora SL, Jamieson RV, Grigg JR , Jones M, Rowe N, Hing S, Donaldson C, Smith JE
Received 26 March 2023
Accepted for publication 19 July 2023
Published 31 July 2023 Volume 2023:17 Pages 2171—2179
DOI https://doi.org/10.2147/OPTH.S400512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alanna Wood,1,2 Benjamin Lim,2 Jim Matthews,3 Tanya Karaconji,1,2 Sophia L Zagora,1,2 Robyn V Jamieson,1,2,4,5 John R Grigg,1,2,4 Michael Jones,2,* Neil Rowe,2,* Stephen Hing,2,* Craig Donaldson,2,* James EH Smith2,*
1Save Sight Institute, Discipline of Clinical Ophthalmology and Eye Health, Faculty of Medicine and Health, Sydney, NSW, Australia; 2Department of Ophthalmology, The Children’s Hospital at Westmead, Sydney, Australia; 3Sydney Informatics Hub, The University of Sydney, Sydney, NSW, Australia; 4Eye Genetics Research, The Children’s Hospital at Westmead, Save Sight Institute, Children’s Medical Research Institute, University of Sydney, Sydney, NSW, Australia; 5Disciplines of Genetic Medicine, and Child and Adolescent, Health, Sydney Medical School, University of Sydney, Sydney, NSW, Australia
*These authors contributed equally to this work
Correspondence: Alanna Wood, Tel +61 404 072 401, Email [email protected]; [email protected]
Purpose: Secondary glaucoma following childhood cataract surgery remains the most common complication in the paediatric population. This study aimed to determine the incidence, time to progression and risk factors associated with the development of secondary glaucoma following childhood cataract surgery in a paediatric population. Outcome measures were the detection of secondary glaucoma, postoperative time frame to development of glaucoma and risk factors in its development.
Patients and Methods: A retrospective case series was conducted between 2003 and 2017 at a tertiary children’s hospital in Sydney. The patient population included those 16 years or less of age who underwent congenital cataract extraction, with or without an intraocular lens implantation and who had been followed up for a minimum of six months following surgery. Patients were excluded if they had cataract aetiology other than congenital idiopathic cataract. Multivariate Cox Regression analysis was used to determine relevant risk factors.
Results: A total of 320 eyes in 216 patients were included in the study. Secondary glaucoma developed in 11.9% of eyes. In those that developed secondary glaucoma, the average time to onset from surgery was 3.2 years (median 2.75 years). The mean age of diagnosis of secondary glaucoma was 4.58 years (median 3.5 years, range 2.5 months to 13.23 years). Microcornea was the only adverse characteristic significantly associated with an increased risk of secondary glaucoma (HR 6.30, p 0.003).
Conclusion: Despite modern surgical techniques, glaucoma remains a significant long-term sequela in children following cataract surgery.
Keywords: secondary glaucoma, paediatric, childhood cataract surgery, glaucoma following cataract surgery
Introduction
Glaucoma following cataract surgery (GFCS, previously termed aphakic and/or pseudophakic glaucoma) remains the most common complication of cataract surgery in the paediatric population.1 The significance of the clinical problem has been recognised by the Childhood Glaucoma Research Network and the World Glaucoma Association who have allocated this form of secondary childhood glaucoma a separate classification category.2,3 A number of studies have investigated the incidence, risk factors and management options associated with secondary glaucoma in the post-cataract paediatric patient. The rate of secondary glaucoma varies widely, with a range reported between 2% and 59%4–18 depending on criteria used to define glaucoma, the age range examined, laterality and surgical technique.
Younger surgical age is a well-recognised predictor for development of secondary glaucoma with those operated on prior to the age of 9 months suggested to be up to 7.2 times more likely to develop secondary glaucoma.16,19 Other factors, both favourable and unfavourable, have been proposed. Inter-study variability exists for the protective association of primary intraocular lens (IOL) implantation, as well as the increased risk for baseline characteristics such as microcornea, microphthalmos and persistent fetal vasculature (PFV).6,7,20–22
GFCS remains insidious in onset and continues to present well after initial surgery. It is difficult to manage, often requiring multiple treatment regimens over time.6,8,13,23 For these reasons, surveillance following childhood cataract surgery occurring early and being lifelong, is a consistently drawn conclusion within the literature.
Proposed mechanisms in the pathogenesis of GFCS include trabecular meshwork obstruction by various mechanisms, post-operative steroid use, a reduction in the diameter of Schlemm’s canal and anterior chamber angle narrowing.4,5,8,12,18,24–26 Late-stage open-angle glaucoma now accounts for the vast majority of cases in both aphakic and pseudophakic patients,1,4,6,11,27 with the introduction of modern surgical techniques greatly reducing the rate of angle closure glaucoma.11,28
The aim of this study was to determine the incidence, time to progression and risk factors associated with the development of GFCS in a real-world paediatric clinic setting.
Patients and Methods
A retrospective case series was carried out from the Children’s Hospital at Westmead a tertiary ophthalmology department in Australia. It reviewed outcomes from a multi-surgeon, paediatric cataract cohort undergoing unilateral or bilateral surgery between 2003 and 2017. The study was conducted in accordance with the recommendations of the Declaration of Helsinki and was approved by the Sydney Children’s Hospital Network Human Research Ethics Committee. The approval was for the review of nominated medical records, with patient consent waived due to review of patient notes only, with no contact with patients, parents/guardians or other family members, as part of the approval adhered to.
Medical records of patients aged 16 years or younger who had congenital cataract extraction, with or without an intraocular lens implantation, and who had been followed up for a minimum of six months following surgery, were included. Patients were excluded if they had cataract aetiology other than congenital idiopathic cataract, other ocular pathology associated with glaucoma, retinopathy of prematurity, congenital glaucoma and prior ocular surgery outside of cataract extraction. Follow-up data was obtained from The Children’s Hospital at Westmead and correspondence from associated treating ophthalmologists.
Consecutive patient records with the appropriate inclusion criteria were identified and files reviewed for data including gender, date of birth, eye(s) operated on, date of surgery, last date of follow-up, family history, microcornea, persistent fetal vasculature (PFV), genetic or syndromic anomalies, primary capsulotomy with anterior vitrectomy and secondary membrane management. Cases were also separated into refractive outcome, defined as aphakic, primary intraocular lens (IOL) implantation or secondary IOL implantation. Information regarding the morphological classification of the cataracts was not consistently reported and therefore excluded from the analysis.
The primary outcome measure was incidence of glaucoma following cataract surgery, sub-categorised into glaucoma and glaucoma suspect. Secondary outcome measures were time to develop secondary glaucoma, measured from the surgical procedure to diagnosis; and identifiable risk factors in the development of secondary glaucoma. For secondary outcome measures, secondary glaucoma was considered in isolation of glaucoma suspect, as the date of diagnosis of glaucoma suspect was often difficult to determine from file review.
Definitions
Patients were defined as glaucoma or glaucoma suspect by the Childhood Glaucoma Research Network (CGRN) criteria where possible.29 However, there were several patients included in the study who had been diagnosed prior to these criteria being developed in 2013, and were therefore diagnosed on the basis of the clinician’s decision to treat. Most diagnoses of glaucoma suspect were based on review of the patient file, with the patient meeting CGRN criteria.29 A glaucoma-related adverse event was defined as the occurrence of either glaucoma or glaucoma suspect.
Technical Aspects
Intraocular pressure (IOP) was measured in outpatient clinic using an iCare tonometer (iCare tonometer Helsinki, Finland) or in the operating theatre at anaesthetic induction with a Perkins hand-held tonometer (Clement Clark, Haag-Streit, Essex, UK). Ten surgeons operated on patients over this time period. The type of surgery was categorised as either primary lensectomy, primary IOL implantation or secondary IOL implantation. If a patient did not develop glaucoma between initial lens extraction and secondary IOL implantation and had cataract surgery equal or greater than 6 months after primary lensectomy, the patient was included in the secondary IOL implantation category.
Statistical Analysis
Statistical analysis was undertaken using Statistical Package for the Social Sciences (SPSS) software. Descriptive statistics were determined for the baseline characteristics of participants with occurrence of both glaucoma and glaucoma suspect (see Table 1). Cox Proportional Hazards Regression modelling was employed to investigate joint effects of variables on the time to development of secondary glaucoma. Univariate and bivariate models were built, with variables considered significant not only by their p-value but by the −2logL value. Inclusion in the multivariate Cox regression model from the bivariate model was based on the Akaike Information Criterion value.30 All models considered glaucoma as a binary outcome, with glaucoma suspect and no glaucoma considered the same. Potential predictors were considered statistically significant in the multivariate model if the p-value was <0.05.
 |
Table 1 Baseline Characteristics and Occurrence of Glaucoma |
Results
A total of 320 eyes in 216 patients were included in the study. Baseline characteristics of the patient cohort along with occurrence of glaucoma-related adverse events are outlined in Table 1.
A glaucoma-related adverse event occurred in 21.3% of eyes, with secondary glaucoma developing in 11.9% (38/320) of eyes and glaucoma suspect in 9.4% (30/320) of eyes. In those that developed secondary glaucoma, the average time to onset from surgery was 3.2 years (median 2.75 years, range 1 month – 13.08 years). The mean age of diagnosis of secondary glaucoma was 4.58 years (median 3.5 years, range 2.5 months to 13.23 years). The mean age of surgery for the cohort was 3.88 years (range 9 days – 16.83 years), with 1.34 years (range 9 days – 6.64 years) for glaucoma and 2.74 years (range 19.8 days – 9.09 years) for glaucoma suspect. The mean follow-up time between surgery and final examination was 5.67 years (range 7 months – 11.42 years) for glaucoma and 4.21 years (range 7 months – 10.66 years) for glaucoma suspect. The average time of follow-up for those patients who did not develop a glaucoma-related adverse event was 3.41 years (range 5 months – 13.91 years).
For bilateral cataract cases, glaucoma-related events occurred in 20.1% of eyes and in unilateral cases 23.8% of eyes. The mean age at cataract surgery was 4.46 years (range 9 days – 16.87 years) for all bilateral cases and 2.59 years (range 16.8 days – 15.12 years) for all unilateral cases. In those patients who developed secondary glaucoma, the average age at cataract surgery was younger for bilateral cases at 1.22 years (range 9 days – 6.64 years), compared to 1.59 years (range 19.8 days – 5.70 years) for unilateral cases.
There were 79 eyes (24.7%) that required secondary membrane management following their surgery and of these, 16.5% developed a glaucoma-related adverse event. The incidence of glaucoma-related adverse events for patients who had other potential risk factors, for example persistent fetal vasculature, is listed in Table 1.
Incidence of glaucoma in patients with lensectomy only was 22.9% compared to 0.7% and 17.4% for primary and secondary intraocular lens insertion, respectively. The mean age at surgery for aphakic patients was 12.76 months (range 9 days to 15.2 years), compared to 5.79 years (range 21.6 days to 16.35 years) for primary IOL implantation and 3.93 years (range 17.7 days to 16.35 years) for secondary IOL implantation (range 19.8 days −16.87 years). The incidence of glaucoma-related events in these patients stratified for age groups of 0–3 months, 3–6 months, 6–12 months, 12–24 months, 24–60 months and over 60 months is outlined in Table 2.
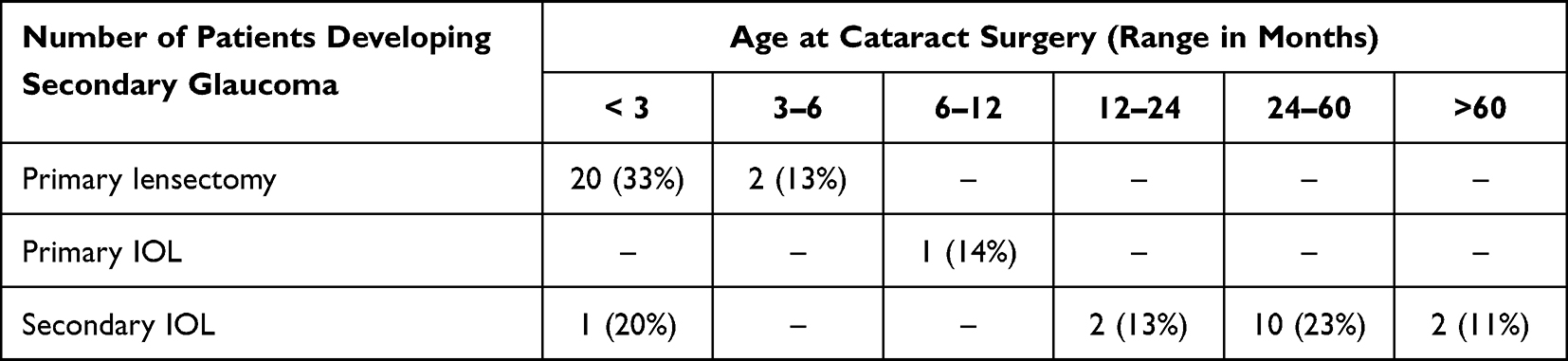 |
Table 2 Optical Status and Secondary Glaucoma Incidence Stratified by Age |
Table 3 outlines the univariate Cox proportional hazards analysis, which assessed potential risk factors and baseline characteristics in the development of secondary glaucoma only. The time to develop for “glaucoma suspect” patients was considered with no glaucoma, as the date of diagnosis for glaucoma suspect was often difficult to determine from patient file review. From the bivariate model, significant risk factors for entry into the multivariate model included age at surgery (continuous), surgery type, microcornea, microphthalmos, PFV and surgical technique. Multivariate analysis (Table 4) demonstrated that primary IOL implantation was a significant predictor in reducing the risk of secondary glaucoma (HR 0.10, p 0.036). Microcornea was the only adverse characteristic significantly associated with an increased risk (HR 6.30, p 0.003). Age at surgery was found to be a significant risk factor in the univariate model, however an association was not demonstrated in the multivariate model (HR 0.97, p 0.131).
 |
Table 3 Univariate Cox Regression Analysis |
 |
Table 4 Multivariate Cox Regression Analysis |
Discussion
Reporting the incidence and time to develop GFCS remains paramount as the management of this complication is challenging and often requires more than one form of treatment.23 Literature suggests that in post-operative aphakic glaucoma, surgery is needed in up to 83% of patients and between 50% and 70% of these will require more than one surgical procedure.6,11,14,23 Patients reported to be at greater risk of developing glaucoma post-operatively include those with microcornea, microphthalmos and PFV.6,8,12,17,21,22,27 The protective value of primary IOL implantation remains uncertain, and whether a particular patient group benefits more from this procedure is still under investigation. Several studies suggest that the original convention of reserving primary IOL implantation for older and less complex patients remains favourable among clinicians.1,7,22,31–33
In this retrospective case series, an incidence of secondary glaucoma of 11.9% was found, after an average follow-up time between surgery and final examination of 5.67 years. Our results are consistent with other studies of a similar surveillance period. After 4.8 years of follow-up in the Infant Aphakia Treatment Study (IATS), the rate of secondary glaucoma was 17%.6 In a large meta-analysis of 470 eyes, an incidence of 17% was also demonstrated, with a median follow-up of 6 years for the total cohort and 4.3 years in those who developed glaucoma7. These studies were performed in unilateral, and both unilateral with bilateral cohorts respectively. A study performed in a group of patients at the same hospital as our study, over a twenty-year period prior, found a glaucoma incidence of 13.4% (Swamy et al).8 In that study, an IOP greater than 26mmHg was used to define glaucoma, consistent with other research at the time. In 2013, the CGRN reached consensus on a new classification system for glaucoma and glaucoma suspect, allowing for greater consistency in diagnosis. Some studies continue to use arbitrary figures for IOP to define glaucoma, such as 25mmHg or 26mmHg.8,11 Our study applied this new criterion where possible; however, clinician’s decision to treat was still applicable to most patients, given our study investigated patient interactions between 2003 and 2017. This notwithstanding, our study has aimed to provide results that can be measured against other studies in which the new standardised criteria have been applied.
The mean time to develop secondary glaucoma in our study was 3.2 years after initial cataract surgery with the last case being diagnosed 13.08 years following surgery. Swamy et al, in a cohort of patients twenty years prior, found an average of 4.9 years to develop glaucoma, while other studies have reported varying average time to progression of glaucoma of 1.34 years to 6.6 years.6–9,11 The variation that exists in the literature is likely due to differences in surveillance protocol, improved diagnostic techniques or differences in the baseline characteristics of the cohort being examined. It highlights the need for both early and ongoing surveillance of patients post-operatively. With standardised criteria being developed in the last decade, there may be potential to identify patients earlier than before, particularly the group that convert from glaucoma suspect to glaucoma.
Our study used age at time of cataract surgery as a continuous variable as it was a more appropriate fit for the model. Some studies have chosen a specific age to dichotomize results. The IATS at ten-year follow-up found younger age at surgery to be the strongest risk factor for secondary glaucoma, and used a cut-off of 48 days of age at surgery.34 Chak et al found that younger age at detection of cataract rather than surgery to be the only factor independently associated with the development of secondary glaucoma.9 In our study, age at the time of surgery was found in the univariate modelling to be associated with the development of secondary glaucoma, however in the multivariate model it was not shown to be a statistically significant predictor (p-value 0.138).
Many studies have investigated whether the placement of a primary IOL is protective, compared to lensectomy only or secondary IOL implantation.1,6–9,18,35 Postulated mechanisms conferring protection include both a mechanical occlusion by the implanted IOL from toxic metabolites entering the anterior chamber, as well as a structural support of the IOL to the trabecular meshwork.22,31,36,37 The IATS found after both 5 and 10 years of follow-up that a primary IOL did not reduce the risk of developing glaucoma-related adverse events in patients with unilateral cataract.6,34 However, this study only looked at unilateral cases and only in children operated on between one and six months of age. Zhang et al did demonstrate a protective effect of IOL placement compared to aphakia and secondary IOL implantation in a meta-analysis of 892 eyes of patients under the age of two, however this reduced risk was only present in bilateral cases.1 In a large meta-analysis, Matafski et al found the placement of a primary IOL reduced the risk of glaucoma in both unilateral and bilateral groups.7 Our multivariate analysis suggests a reduction in occurrence of secondary glaucoma with placement of primary IOL (HR 0.1, p 0.03), in a patient cohort of both unilateral and bilateral cases. The overall incidence of secondary glaucoma for patients across all age groups with primary IOL placement was 0.7%. However, it is important to note that prevalence of surgery type (lensectomy, primary IOL and secondary IOL) differs greatly according to age. We attempted to minimise possible bias through collinearity modelling which demonstrated little correlation between variables, such as age and surgery type. Current literature refers to primary IOL implantation being acceptable and safe in children above the age of two.1,27,31 In our series, most of the children receiving a primary IOL placement were over the age of two, suggesting a tendency to follow previous convention and apply lensectomy in younger patients and insert a primary IOL in older and less complex patients.
Our study results suggest that there is a six-fold increase in risk of developing secondary glaucoma if microcornea is present (HR 6.3, p 0.003), with 6 of the 12 patients with microcornea developing this complication. Daniel et al clustered microcornea, microphthalmos and PFV together and found a higher incidence of secondary glaucoma in these patients at 28%, with those operated on at a later age less at risk.38 Matalaia et al found a rate of 10.6% of secondary glaucoma in those with microcornea, with incidence not significantly different between early and late age at surgery.39 The IATS found smaller corneal diameter to be an independent risk factor for all glaucoma-related adverse events,6,34 as did Swamy et al in 2007.8 Praveen et al suggest that both ciliary body architecture and aqueous outflow mechanisms are altered in microcornea and therefore they are more prone to secondary glaucoma.40 The same authors suggest that eyes with microcornea be operated on after three months of age to prevent excessive inflammation that may contribute to the increased prevalence of secondary glaucoma in this group. Contrary to this, Trivedi et al failed to find an association between corneal diameter and age and suggested that those eyes operated on earlier in life have smaller corneal diameters and therefore the risk of glaucoma in this group may be due to age rather than microcornea.35
Other potential predictors reported in the literature as being significant in the development of secondary glaucoma following congenital cataract surgery include secondary membrane surgery, persistent fetal vasculature, microphthalmos and primary capsulotomy with anterior vitrectomy.6,8,12,21,27,31,41–43 These risk factors demonstrated significance in our univariate analysis but failed to show an association in the multivariate analysis.
The retrospective and non-randomised nature of the design of our study could be considered a weakness although it would be difficult to conduct a prospective study in this context. The minimum six-month period for follow-up of our patients could be considered a limitation, given the mean time to diagnosis was over three years; however, this timeframe is consistent with previous studies. Our research adopted the standardised definition of glaucoma where possible, whereas other studies have used IOP alone without consideration of other features of glaucoma such as corneal diameter or axial length. We considered glaucoma and glaucoma suspect separately for part of the analysis, where prior studies have not included the latter. The strengths of the study were the length of follow-up time and the large sample size.
The results of our study highlight that with modern surgical techniques, the occurrence of secondary glaucoma remains a common complication with a rate consistent with both existing literature, as well as incidence within the same hospital over the twenty-year time-frame prior to ours. Risk factors in its development, within our patient cohort, were limited to those with microcornea. Our results reflect a more favourable long-term outcome in patients with primary intraocular lens implantation; however, majority of those receiving a primary IOL were over two years of age.
Acknowledgments
The authors acknowledge the technical assistance provided by the Sydney Informatics Hub, a Core Research Facility of the University of Sydney.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Zhang S, Wang J, Li Y, Liu Y, He L, Xia X. The role of primary intraocular lens implantation in the risk of secondary glaucoma following congenital cataract surgery: a systematic review and meta-analysis. PLoS One. 2019;14(4):1.
2. Grigg JR, Fenerty C. Glaucoma following cataract surgery in aphakic or pseudophakic children. In: Lloyd IC, Lambert SR, editors. Congenital Cataract: A Concise Guide to Diagnosis and Management. Switzerland: Springer; 2017:181–196.
3. Fenerty C. Glaucoma following cataract surgery. In: Weinreb R, Grajewski A, Papadopoulos M, Grigg J, Freedman S, editors. Childhood Glaucoma: The 9th Consensus Report of the World Glaucoma Association. Amsterdam, The Netherlands: Kugler Publications; 2013:233–247.
4. Abdelmassih Y, Beaujeux P, Dureau P, Edelson C, Caputo G. Incidence and risk factors of glaucoma following pediatric cataract surgery with primary implantation. Am J Ophthalmol. 2021;224:1–6. doi:10.1016/j.ajo.2020.09.025
5. Jamerson EC, Solyman O, Yacoub MS, Abushanab MMI, Elhusseiny AM. Angle surgery in pediatric glaucoma following cataract surgery. Vision. 2021;5(1):9. doi:10.3390/vision5010009
6. Freedman SF, Lynn MJ, Beck AD, et al. Glaucoma-related adverse events in the first 5 years after unilateral cataract removal in the Infant Aphakia Treatment Study. JAMA Ophthalmol. 2015;133(8):
7. Mataftsi A, Haidich AB, Kokkali S, et al. Postoperative glaucoma following infantile cataract surgery: an individual patient data meta-analysis. JAMA Ophthalmol. 2014;132(9):
8. Swamy BN, Billson F, Martin F, et al. Secondary glaucoma after paediatric cataract surgery. Br J Ophthalmol. 2007;91(12):
9. Chak M, Rahi JS; British Congenital Cataract Interest Group. Incidence of and factors associated with glaucoma after surgery for congenital cataract: findings from the British Congenital Cataract Study. Ophthalmology. 2008;115(6):
10. Wood KS, Tadros D, Trivedi RH, Wilson ME. Secondary intraocular lens implantation following infantile cataract surgery: intraoperative indications, postoperative outcomes. Eye. 2016;30(9):
11. Baris M, Biler ED, Yilmaz SG, Ates H, Uretmen O, Kose S. Treatment results in aphakic patients with glaucoma following congenital cataract surgery. Int Ophthalmol. 2019;39(1):
12. Kim JA, Lee SY, Park KH, Yu YS, Jeoung JW. Incidence and risk factors for glaucoma development after bilateral congenital cataract surgery in microphthalmic eyes. Am J Ophthalmol. 2019;208:
13. Shenoy BH, Mittal V, Gupta A, Sachdeva V, Kekunnaya R. Complications and visual outcomes after secondary intraocular lens implantation in children. Am J Ophthalmol. 2015;159(4):
14. Comer RM, Kim P, Cline R, Lyons CJ. Cataract surgery in the first year of life: aphakic glaucoma and visual outcomes. Can J Ophthalmol. 2011;46(2):
15. Tadros D, Trivedi RH, Wilson ME. Primary versus secondary IOL implantation following removal of infantile unilateral congenital cataract: outcomes after at least 5 years. J AAPOS. 2016;20(1):
16. Chan WH, Biswas S, Ashworth JL, Lloyd IC. Congenital and infantile cataract: aetiology and management. Eur J Pediatr. 2012;171(4):
17. Tatham A, Odedra N, Tayebjee S, et al. The incidence of glaucoma following paediatric cataract surgery: a 20-year retrospective study. Eye. 2010;24:1366–1375. doi:10.1038/eye.2010.46
18. Haargaard B, Ritz C, Oudin A, et al. Risk of glaucoma after pediatric cataract surgery. Invest Ophthalmol Vis Sci. 2008;49(5):1791–1796. doi:10.1167/iovs.07-1156
19. Lambert SR. The timing of surgery for congenital cataracts: minimizing the risk of glaucoma following cataract surgery while optimizing the visual outcome. J AAPOS. 2016;20(3):191–192. doi:10.1016/j.jaapos.2016.04.003
20. Serafino M, Trivedi RH, Levin AV, et al. Use of the Delphi process in paediatric cataract management. Br J Ophthalmol. 2016;100(5):611–615. doi:10.1136/bjophthalmol-2015-307287
21. Solebo AL, Russell-Eggitt I, Cumberland PM, Rahi JS; British Isles Congenital Cataract Interest Group. Risks and outcomes associated with primary intraocular lens implantation in children under 2 years of age: the IoLunder2 cohort study. Br J Ophthalmol. 2015;99(11):1471–1476. doi:10.1136/bjophthalmol-2014-306394
22. Spiess K, Peralta Calvo J. Clinical characteristics and treatment of secondary glaucoma after pediatric congenital cataract surgery in a tertiary referral hospital in Spain. J Pediatr Ophthalmol Strabismus. 2020;57(5):292–300. doi:10.3928/01913913-20200707-01
23. Eidbenberger K, Kiss B, Schmidt-Erfurth U, Stifter E. Clinical characteristics and treatment of secondary glaucoma, glaucoma suspects and ocular hypertension after congenital cataract surgery. Eur J Ophthalmol. 2021;31(6):3309–3317.
24. Moritz DC, Dubis AM, Theodorou M, et al. Childhood lensectomy is associated with static and dynamic reduction in schlemm canal size: a biomechanical hypothesis of glaucoma after lensectomy. Ophthalmology. 2019;126:233–241. doi:10.1016/j.ophtha.2018.08.031
25. Gouda J, Tomairek RH, Elhusseiny AM, et al. Changes in intraocular pressure and anterior chamber angle after congenital cataract extraction. J Glaucoma. 2021;30(1):61.
26. Chen D, Gong XH, Xie H, Zhu XN, Li J, Zhao YE. The long-term anterior segment configuration after pediatric cataract surgery and the association with secondary glaucoma. Sci Rep. 2017;7:1–9. doi:10.1038/s41598-016-0028-x
27. Ma F, Wang Q, Wang L. Advances in the management of the surgical complications for congenital cataract. Front Med. 2012;6(4):
28. Solebo AL, Rahi JS; British Congenital Cataract Interest Group. Glaucoma following cataract surgery in the first 2 years of life: frequency, risk factors and outcomes from IoLunder2. Br J Ophthalmol. 2020;104(7):967–973. doi:10.1136/bjophthalmol-2019-314804
29. Beck A, Chang TCP, Freedman S. Definition, classification, differential diagnosis. In: Weinreb R, Grajewski A, Papdopoulos M, Grigg J, Freedman S, editors. Childhood Glaucoma. Amsterdam: Kluger Publications; 2013:3–10.
30. Collett D. Modelling Survival Data in Medical Research.
31. Kim DH, Kim JH, Kim SJ, Yu YS. Long-term results of bilateral congenital cataract treated with early cataract surgery, aphakic glasses and secondary IOL implantation. Acta Ophthalmol. 2012;90(3):
32. Vasavada AR, Vasavada V, Shah SK, et al. Five-year postoperative outcomes of bilateral aphakia and pseudophakia in children up to 2 years of age: a randomized clinical trial. Am J Ophthalmol. 2018;193:33–44. doi:10.1016/j.ajo.2018.06.005
33. Bothun ED, Wilson ME, Yen KG, et al. Outcomes of bilateral cataract surgery in infants 7 to 24 months of age using the Toddler Aphakia and Pseudophakia Treatment Study Registry. Ophthalmology. 2021;128(2):302–308. doi:10.1016/j.ophtha.2020.07.020
34. Freedman SF, Beck AD, Nizam A, et al. Glaucoma-related adverse events at 10 years in the infant aphakia treatment study: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2021;139(2):165–173. doi:10.1001/jamaophthalmol.2020.5664
35. Trivedi RH, Wilson ME Jr, Golub RL. Incidence and risk factors for glaucoma after pediatric cataract surgery with and without intraocular lens implantation. J AAPOS. 2006;10(2):117–123. doi:10.1016/j.jaapos.2006.01.003
36. Magli A, Forte R, Rombetto L. Long-term outcome of primary versus secondary intraocular lens implantation after simultaneous removal of bilateral congenital cataract. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):
37. Sahin A, Caça I, Cingü AK, et al. Secondary glaucoma after pediatric cataract surgery. Int J Ophthalmol. 2013;6(2):216–220. doi:10.3980/j.issn.2222-3959.2013.02.21
38. Daniel MC, Adams GGW, Dahlmann-Noor A. Medical management of children with congenital/infantile cataract associated with microphthalmia, microcornea, or persistent fetal vasculature. J Pediatr Ophthalmol Strabismus. 2019;56(1):
39. Matalia J, Shirke S, Shetty KB, Matalia H. Surgical outcome of congenital cataract in eyes with microcornea. J Pediatr Ophthalmol Strabismus. 2018;55(1):
40. Praveen MR, Vasavada AR, Shah SK, Khamar MB, Trivedi RH. Long-term postoperative outcomes after bilateral congenital cataract surgery in eyes with microphthalmos. J Cataract Refract Surg. 2015;41(9):
41. Rabiah PK. Frequency and predictors of glaucoma after pediatric cataract surgery. Am J Ophthalmol. 2004;137(1):30–37. doi:10.1016/S0002-9394(03)00871-7
42. Walton DS. Pediatric aphakic glaucoma: a study of 65 patients. Trans Am Ophthalmol Soc. 1995;93:403–420.
43. Lloyd IC, Ashworth J, Biswas S, Abadi RV. Advances in the management of congenital and infantile cataract. Eye. 2007;21(10):
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.