Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Prevalence of Generalised Anxiety Disorders Among Clinical Training Students at the University of Sharjah
Authors Otim M ![]() , Al Marzouqi AM
, Al Marzouqi AM ![]() , Subu M
, Subu M ![]() , Damaj N, Al-Harbawi S
, Damaj N, Al-Harbawi S
Received 28 April 2021
Accepted for publication 4 June 2021
Published 13 July 2021 Volume 2021:14 Pages 1863—1872
DOI https://doi.org/10.2147/JMDH.S317828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Michael Otim,1,2 Amina M Al Marzouqi,1 Muhammad Subu,1 Naamat Damaj,1 Sara Al-Harbawi1
1College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates; 2Academic Research and Consultancy Directorate, Nexus International University, Kampala, Uganda
Correspondence: Michael Otim
College of Health Sciences, University of Sharjah, PO Box 27272, Sharjah, United Arab Emirates
Email [email protected]
Introduction: This study aimed to determine the prevalence of anxiety among clinical training students. Despite the existence of interventions that address anxieties, lack of data on the size of the problem, especially in the Middle East where mental health stigmatized, means that outcomesmay not be maximized.
Materials and Methods: Our study was cross-sectional survey of the University of Sharjah (UOS), the United Arab Emirates students undergoing clinical training in health sciences. The participants were selected from all the three UOS campuses: medical and science colleges; women’s colleges; and men’s colleges. A sample of 219 clinical training students were randomly sent an electronic link to participate on an online survey. The study received ethical approval from the UOS Research Ethics Committee number is REC-20-03-04-02-S.
Results: The mean score for state anxiety was 47.24± 1.31 and the mean score for trait anxiety was 46.82± 1.21. These scores indicated a high level of anxiety among students undertaking clinical training. Overall, 63% of the sample were classified as having high state anxiety, and 62% had high trait anxiety.
Conclusion: This study shows clinical training students experience high levels of state and trait anxiety. It is necessary to address this issue to improve the conditions and circumstances for students entering clinical training. It may also be necessary to implement strategies to enable students with anxiety to perform well in clinical training.
Keywords: anxiety, clinical students, clinical practice, mental health, STAI
Introduction
Experiencing occasional stress and tension is a normal part of life. However, individuals with anxiety disorders often experience excessive and continual fear and worry about various situations, including daily life situations. Often, anxiety disorders, such as Generalized Anxiety Disorders involve repeated episodes of sudden feelings of excessive anxiety and fear or terror that can cause panic attacks. The National Health Service (NHS) defines Generalized Anxiety Disorder as a long-term condition. It makes you feel anxious about a wide range of conditions. For those with Generalized Anxiety Disorder, anxiety is felt most days and difficulty feeling relaxed. It can cause both mental and physiological signs, such as: feeling restless or worried, trouble concentrating or sleeping, and dizziness.1 The general cause of generalized anxiety disorder is not fully understood. Anxiety disorders develop from a complex set of risk factors, including genetics, brain chemistry, personality, and life events. Treatment can involve psychological therapies, such as cognitive behavioral therapy (CBT) and psychiatric prescribed medications such as antidepressant called selective serotonin reuptake inhibitors (SSRIs). This can interfere in day-to-day activities, and may be difficult to control regardless of general personal characteristics.2
Stress and burnout are common among practicing physicians, nurses, and physiotherapists, as well as among medical students. Perceived stress is associated with elevated rates of depression, relationship problems, anxiety, and suicide.3 Healthcare professionals and medical students who are anxious may not be able to offer as good quality treatment as those who do not experience anxiety. In addition to being a widespread mental health condition, anxiety is also among the most misunderstood.
Globally, about one in three medical students have anxiety—a prevalence rate which is higher than the general population. Quek et al argue that stress or anxiety is an important issue in medical education because it has the potential to impede clinical learning and performance.4 They found the prevalence of anxiety was 33.8% among medical students globally, which is substantially higher than the general population. Francis et al believe that the effort to destigmatize help-seeking behavior for anxiety, and mental health issues in general, should start with the administrators and leaders of medical schools.5 Medical students are vulnerable to anxiety due to the nature of their academic life. In Malaysia,
the prevalence of anxiety symptoms among medical students in a local university were lower than the international studies done, reflecting perhaps increased resilience in this population.6
Stress is a particularly important issue in education because it has the potential to impede learning and performance.7 Some studies also support that nursing students suffer from stress in their clinical practice8,9 The US National Institute of Mental Health indicates anxiety disorder symptoms can be classified by feelings of restlessness, fatigue, and difficulty maintaining focus.4 Anxiety disorders have the highest prevalence compared with other common mental health disorders, with a lifetime prevalence of over 15%.4 For example, anxiety disorders are the most common mental health problem in the US, affecting 40 million adults or 18% of the population each year. However, the prevalence of anxiety disorders in the Middle East remains less known, including in the United Arab Emirates (UAE).
Clinical practice is an essential part of the nursing education program. In Indonesia, nursing students experienced stress and anxiety during their clinical activities9 Another study conducted in Malaysia indicated that among nursing students, clinical assignment was the main stressor and cause of anxiety.10
In Saudi Arabia, a study revealed that half of the pharmacy students suffered from anxiety incidence during their studies at the university11 Anxiety is a leading concern among college students. It affects 41.6% of students, with depression affecting 36.4%.5 Stress and anxiety can interfere with learning, affect academic performance, and impair performance in clinical practice.3 Research suggests that high levels of stress and anxiety in medical education may have negative effects on students’ learning process and clinical success.12 This anxiety and stress among medical students may be related to difficulties in clinical practice and the lack of experience in performing academic tasks.7 Anxiety and stress among medical students have received research attention because of the significant implications.8 Educational practice demands, and stress cause a negative effect on the students’ psychological well-being This condition can precipitate depression and anxiety.13
The US National Institute of Mental Health indicates anxiety disorder symptoms can be classified by feelings of restlessness, fatigue, and difficulty maintaining focus.4 Anxiety disorders have the highest prevalence compared with other common mental health disorders, with a lifetime prevalence of over 15%.4 For example, anxiety disorders are the most common mental health problem in the US, affecting 40 million adults or 18% of the population each year. However, the prevalence of anxiety disorders in the Middle East remains unknown, including in the United Arab Emirates (UAE).
Anxiety is a leading concern among college students. It affects 41.6% of students, with depression affecting 36.4%.5 Stress and anxiety can interfere with learning, affect academic performance, and impair performance in clinical practice.3 Research suggests that high levels of stress and anxiety in medical education may have negative effects on students’ learning process and clinical practice. This anxiety and stress among medical students may be related to difficulties in clinical practice and the lack of experience in performing academic tasks.7 Anxiety and stress among nursing students have received research attention because of the significant implications.8
In nursing education, clinical training is essential to provide students with experience so they can achieve success in the education process. Nursing students have been reported to experience high levels of stress and anxiety during their education.3 A previous study found nursing students considered clinical training as one of the most anxiety-producing aspects of the curriculum, and this anxiety had negative impacts on their learning, performance, and well-being.9 Another study reported the clinical setting was the main cause of stress and anxiety among students, with initial clinical practice considered the most stressful period in a student’s education.9,10 Similarly, physiotherapy students commonly experience psychological distress during clinical training, with specific stressors being patients’ suffering, academic pressure, and tension during interaction with clients.14
A previous study reported feeling unprepared was a common thread among anxious students, meaning students felt anxious while anticipating their clinical practical, and even afterward when they thought about their clinical experience.3 Most research concerning anxiety among students focused on general anxiety in the medical, dental, and nursing fields.4,11 Medical school is perceived more stressful and a cause for general anxiety compared with other graduate programs. However, research and information concerning the prevalence and severity of anxiety among students in other healthcare professions is limited and difficult to find.13,14
A study conducted in Turkey investigated medical students’ anxiety related to clinical training, and compared this anxiety between two medical schools that applied different preclinical curricula.15 The two university samples had similar distributions of sex and age (60.0% male, mean age 21.67±1.06 years; 59.3% male, mean age 21.96±0.98, years), and the difference in mean overall anxiety scores between the two student groups was not statistically significant.15
Anxiety may decrease students’ academic performance, professionalism, and ability to manage their patients’ healthcare. A previous study reported the prevalence of study-related anxiety among female medical students (N=93) was 72.26%.16 That study found anxiety was more common among final-year students (83.10%), followed by first- and second-year students (75%), but less common among fourth-year students (63.23%). In terms of severity, the majority of students had mild (41.07%) or moderate (37.51%) anxiety.16 Another study investigated anxiety and depression among students (288 males, 105 females) at a medical college in Saudi Arabia and reported the prevalence of anxiety and depression was 66.6% for females and 44.4% for males (p=0.01).17 Among first-year students the prevalence was 89.7% in females and 60% in males (p=0.006), although no suicidal ideation was reported by either males or females.17 It is of concern that no such information is available for students in the UAE. Therefore, we surveyed students who entered clinical training regarding anxiety to establish whether this problem existed among students at the University of Sharjah (UOS). Specifically, we aimed to determine if students from the UOS College of Health Sciences experienced anxiety when they attended clinical training and clarify the prevalence of anxiety in this population.
Methodology
Research Design
This study used a descriptive cross-sectional design to investigate anxiety among undergraduate clinical training students at the UOS College of Health Sciences. Simple random sampling was used to enrol participants, which gave an equal chance for all participants to be involved in the study.18
Research Population and Sample
Participants in this study comprised undergraduate students from the seven departments in the College of Health Sciences, University of Sharjah (UOS) undergoing the clinical training programs as part of their degree training. The seven departments include: Medical Diagnostic Imaging, Medical Laboratory Sciences, Physiotherapy, Nursing, Nutrition, Health Services Administration, and Environmental Health. Female students comprise about 96% of students in the College of Health Science. We reflected this female ratio in the sample estimation. We estimated the sample size to be approximately 300 students using Centers for Disease Control and Prevention, Atlanta, Statistical Epi-Info 7 calculator.19 The team distributed the questionnaires to more than 220 students, but 10 of these participations were excluded from the analyses because of invalid answers. We were not able to achieve our target of 300 participants due to the Covid-19 Pandemic and other several University constraints such as students undertaking exams and other activities – constituting the limitation of the study. Only 210 participants participated.
Consent and Ethical Approval
The consent form and information sheet were provided to the respondents in both Arabic and English. Ethical approval for this study was obtained from the UOS Research Ethics Committee. The Committee approval number is REC-20-03-04-02-S. All participants provided informed consent, and this study was conducted in accordance with the Declaration of Helsinki.
Patient and Public Involvement
No patients were involved in this study.
Research Instrument
The State-Trait Anxiety Inventory for Adults (STAI) was used to collect data on anxiety among participants. The STAI is commonly used to measure anxiety among adults, and was developed by Spielberger in 1968.20 The STAI has been validated in various countries with clinical and non-clinical samples.6,21,22 It uses a relatively brief self-report scale to assess both state and trait anxiety and is suitable to be administered in both clinical practice and research. The STAI has been translated into the Greek, Dutch, Japanese, Chinese, and Malaysian languages, with these versions consistently reported to have acceptable reliability.21
In this study, the survey was conducted online, and distributed to students using multiple social media platforms. The questionnaire was available in both the English and Arabic languages. The Arabic version of the STAI had adequate internal consistency reliability similar to that reported in the international literature, suggesting it was appropriate for assessing anxiety in Arabic speaking populations.20,21
Scoring Method
The STAI is a commonly used measure of state and trait anxiety.20 It comprises separate self-report subscales for state anxiety (STAI-S) and trait anxiety (STAI-T). The STAI-T subscale comprises 20 statements that ask people to describe how they generally feel. The STAI-S subscale includes 20 statements that investigate their feelings at a particular moment in time. The STAI-S subscale can be used to determine actual levels of anxiety intensity induced by stressful procedures or events. The validity of the STAI rests on the assumption that the respondent has a clear understanding of the instructions for the “State” and “Trait” subscales.6,23 Each question is rated on a 4-point scale (not at all, somewhat, moderately so, very much so), giving a range of possible scores of 20–80 for each subscale. STAI subscale scores are commonly classified as “no or low anxiety” (20–37), “moderate anxiety” (38–44), and “high anxiety”(45–80).20,21,24,
Statistical and Data Analysis
Data were coded and cleaned using IBM SPSS Version 13.0.25 Statistical analysis was also performed using the SPSS software and emphasis was mainly on descriptive statistics. Data analysis was performed for numerical values. Data for categorical variables were first coded and then analysed using descriptive statistics (eg frequency and percentage). These were reported as frequencies and percentages, means and confidence intervals from quantitative data. Results were also presented using tables. We were not able to test the effect of the different variables on anxiety since this was mainly a descriptive study.
Results
Demographic Data
Participants’ demographic data are summarized in Table 1 below. Most participants were female (89%, n=187) which was in line with gender distribution within the population of study at the College of Health Sciences. Most of the participants (84%, n=72) were aged 18–22 years, and 72% of them (n=152) lived off-campus. Fifty-nine (28%) students were from the Nursing department, and 21% (n=44) were from the Physiotherapy department.
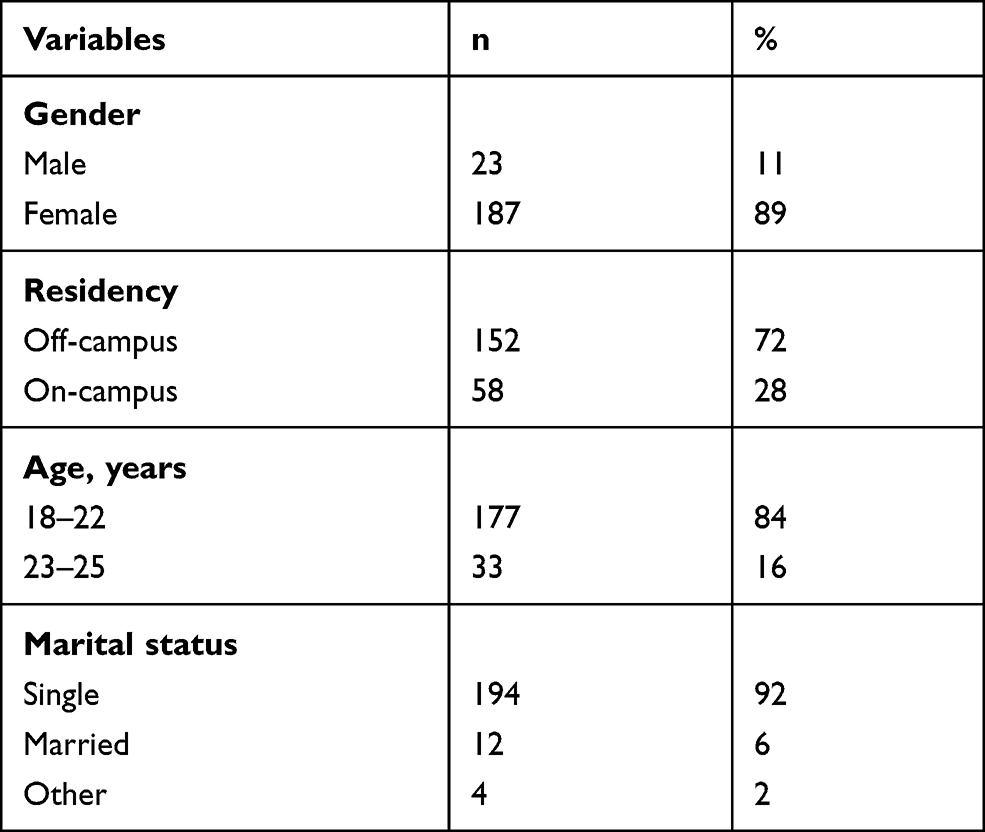 |
Table 1 Participants’ Demographic Data |
Table 2 shows that the majority of participants (64%, n=135) were seniors, reflecting the years of study (senior level) when Departments require their students to undertake clinical training. Some Disciplines require their students to undergo clinical training a later time of their study. Most of the participants were single (92%, n=194), and many of the participants had never smoked (81%, n=170). Over half of the participants had adequate sleep (6–7 hours: 48%, n=100; 8 hours: 12%, n=26). However, most participants reported relatively low physical activity: 1–2 times per week (41%, n=86) and no activity (37%, n=78).
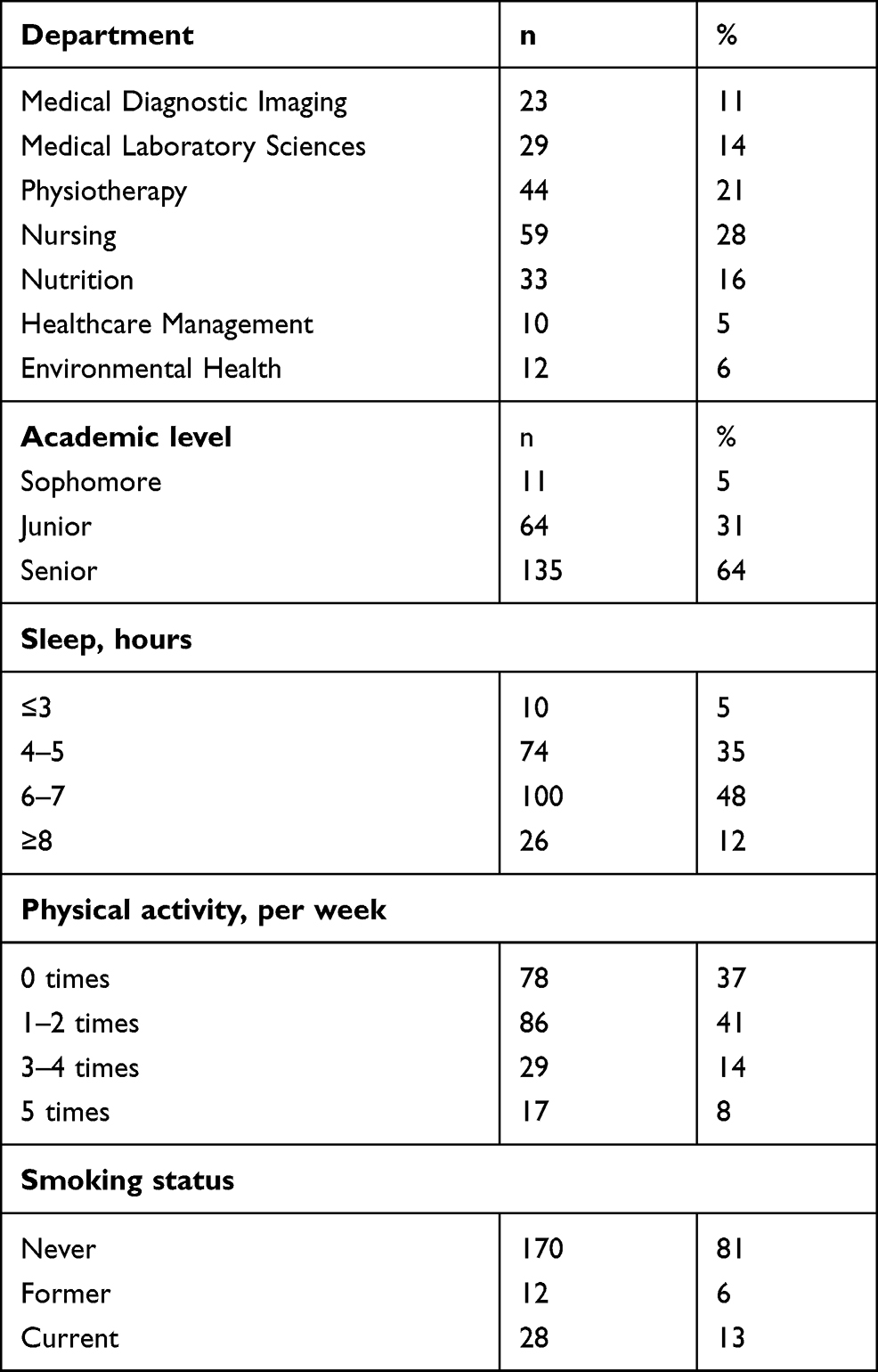 |
Table 2 Percentage Participants in the Study |
Tables 3 and 4 present the mean State and Trait anxiety scores by the demographic variables. The mean State and Trait anxiety levels were a little higher for females than for males, and higher in those aged 18–22 years compared with older students. In addition, higher mean State and Trait anxiety scores were observed among students living off-campus than those living on campus. Among all departments, students from the Health Services Administration department showed the highest State and Trait Anxiety scores. Students that slept for 5 hours or less had higher State and Trait anxiety scores than those that slept for more than 5 hours. Students that reported no physical activity had higher State and Trait anxiety scores than other students, and those that had never smoked had lower scores than former or current smokers. We chose to use confidence intervals to estimate intervals in which the true value of the means would lie.
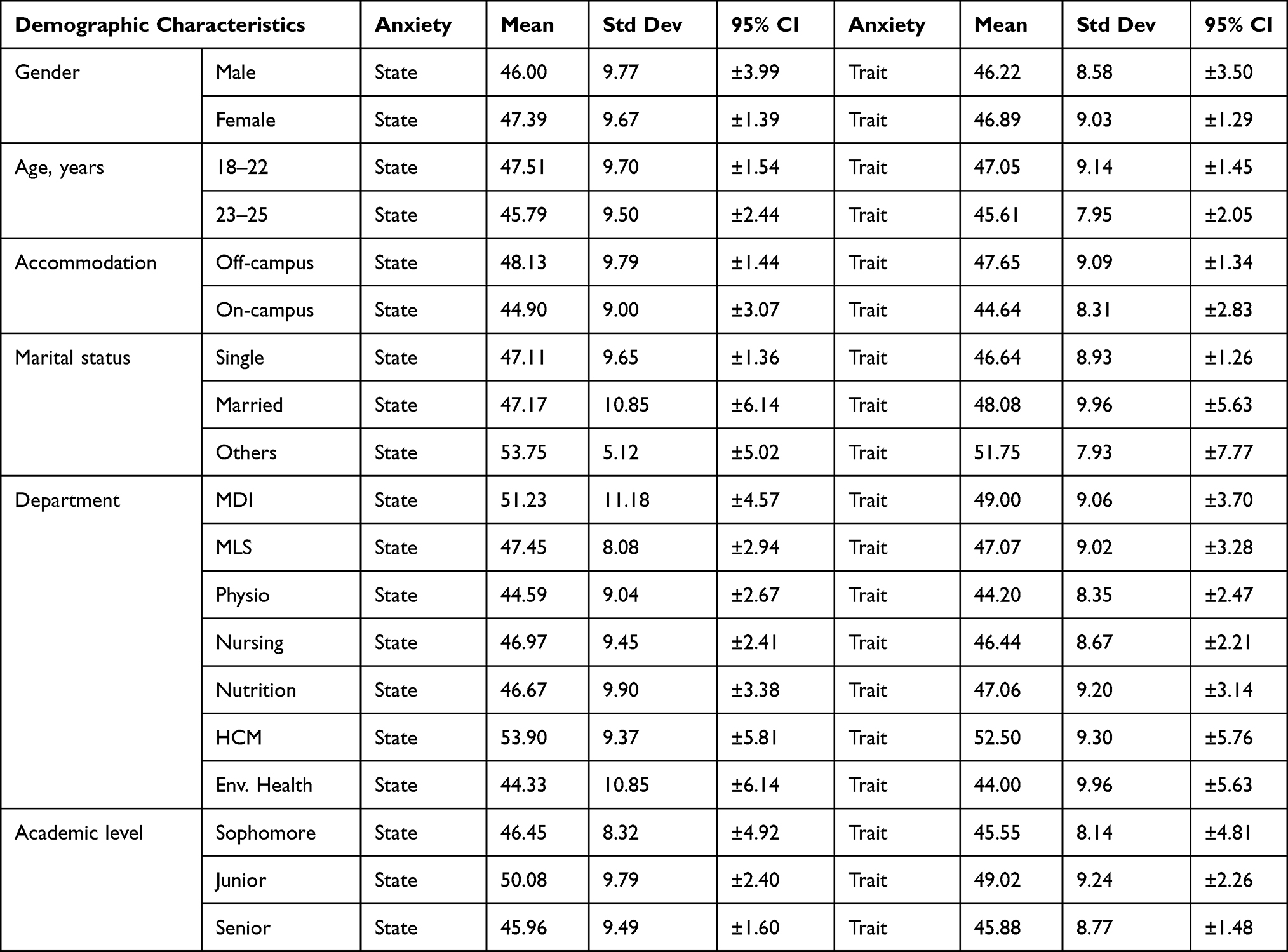 |
Table 3 Mean Anxiety Scores and Confidence Intervals by Demographic Characteristics |
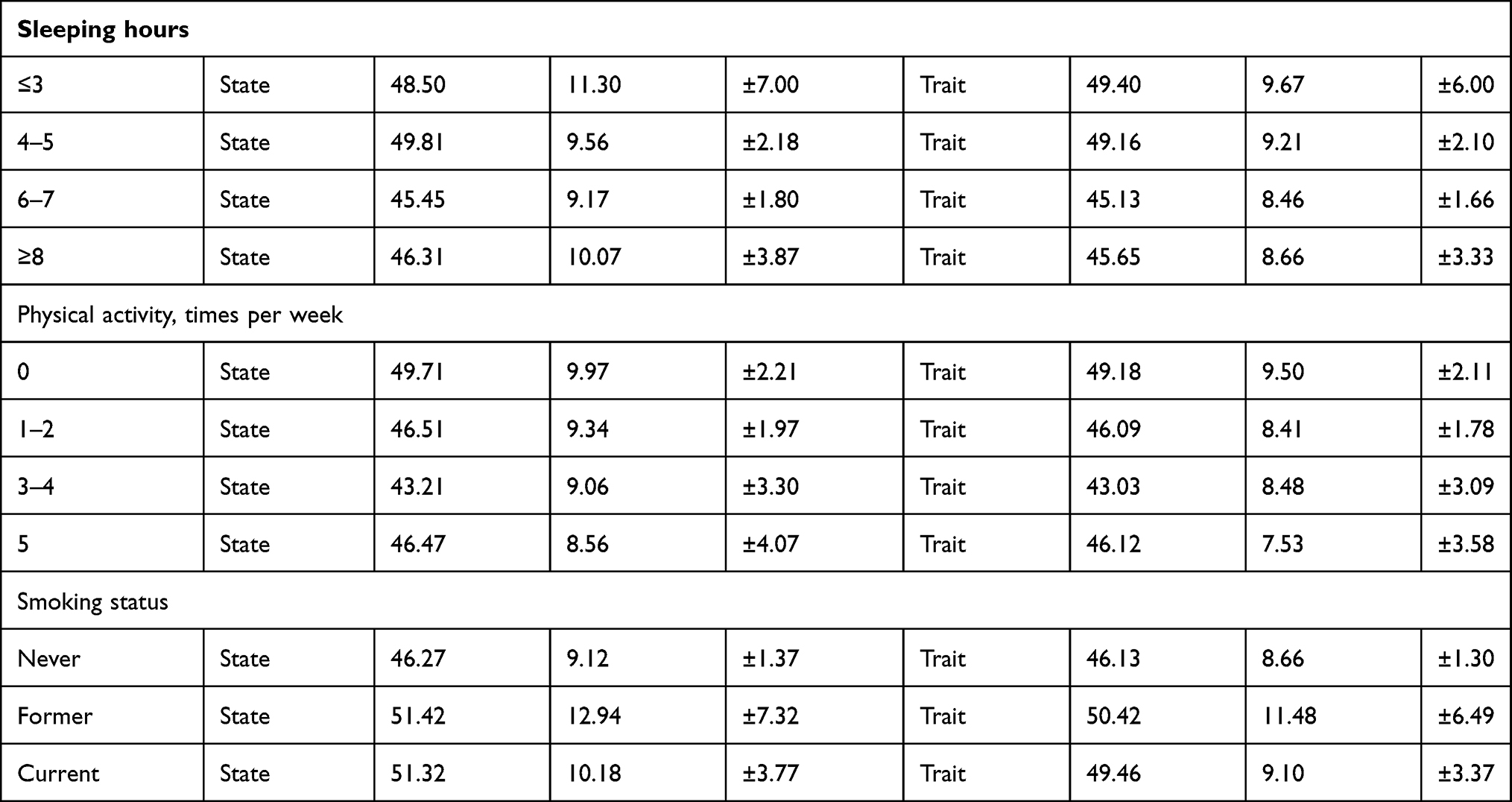 |
Table 4 Mean Anxiety Scores and Confidence Intervals for non-Demographic Variables |
Table 5 presents the prevalence percentages for levels of State and Trait anxiety (no/low, moderate, or high) based on the STAI cut-off points.20 Over half (57%, n=33) of the students living on campus had high State anxiety and 53% (n=31) had high Trait anxiety. The female students had higher Trait Anxiety than males, although the male numbers were small. In absolute numbers, Physiotherapy, Nursing and Nutrition had the largest number of students with high Trait Anxiety. However, in terms of percentages, the lowest Trait Anxiety was exhibited by Nursing students.
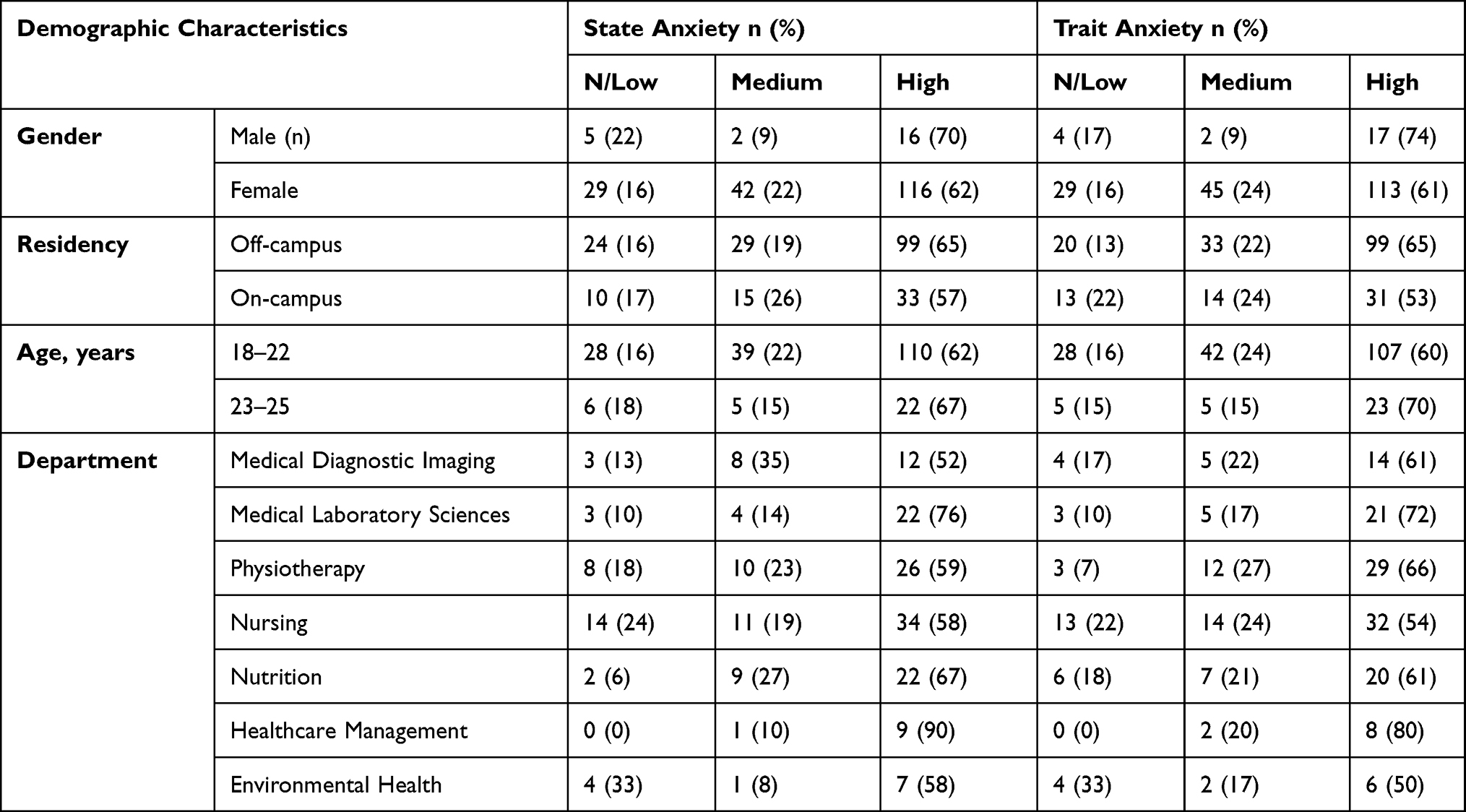 |
Table 5 State and Trait Anxiety prevalence Levels by Demographic Characteristic |
Most of the senior students had high State (64%, n=87) and Trait (63%, n=85) anxiety (Table 6). Only 63% of the junior participants had high anxieties. Those who were single, smokers or not involved in physical activity had high State and Trait Anxiety in general.
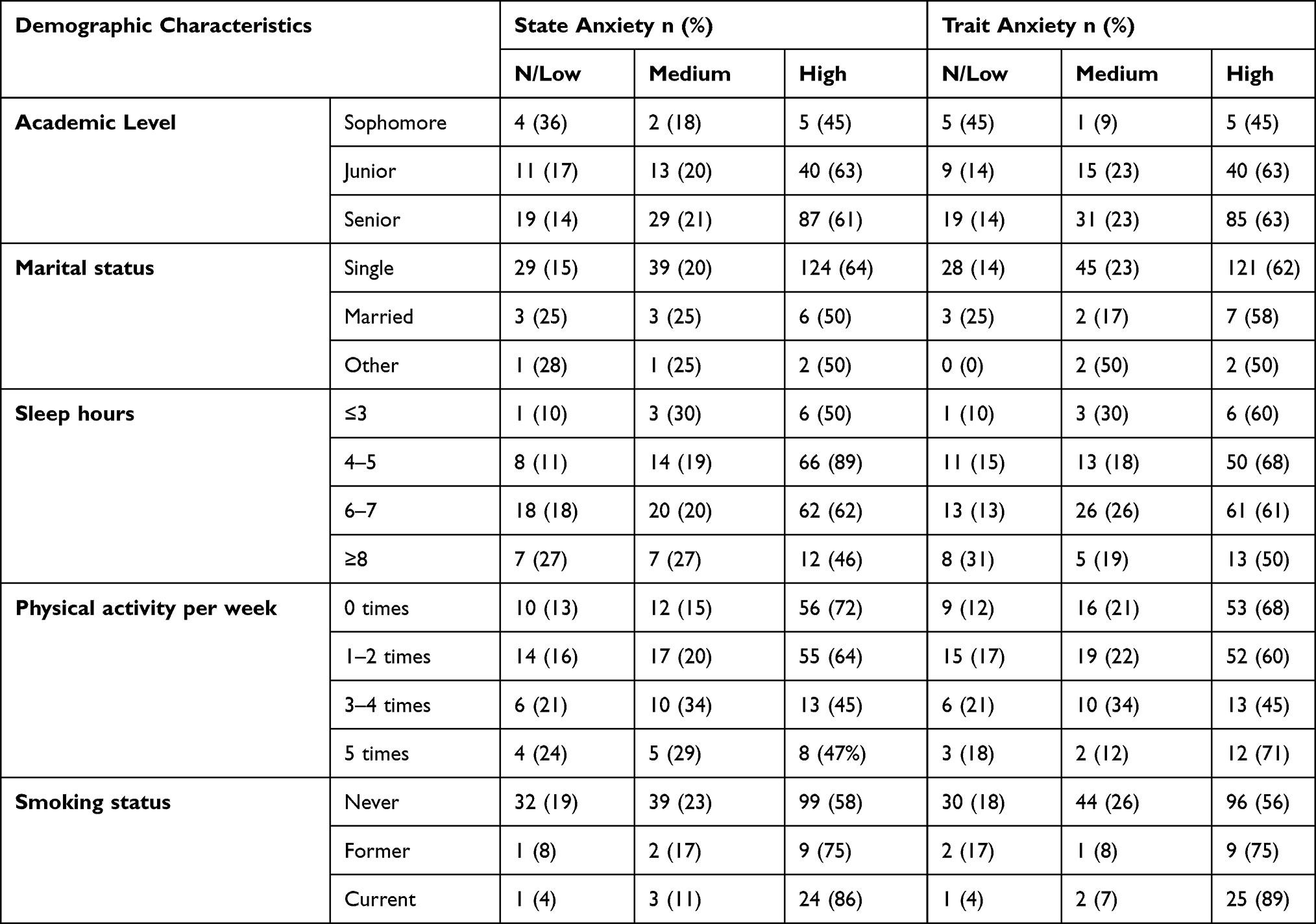 |
Table 6 State and Trait Anxiety Levels by Demographic Characteristic |
Results showed that 63% (n=132) of the sample had high level of State anxiety, and 62% (n=130) had a high level of Trait anxiety. The overall mean score for State anxiety was 47.24±1.31, and that for Trait anxiety was 46.82±1.21 (Table 7). These mean scores suggested there was a high level of anxiety in the sample population. Given the sample size, we can safely generalize to the rest of the UOS population.
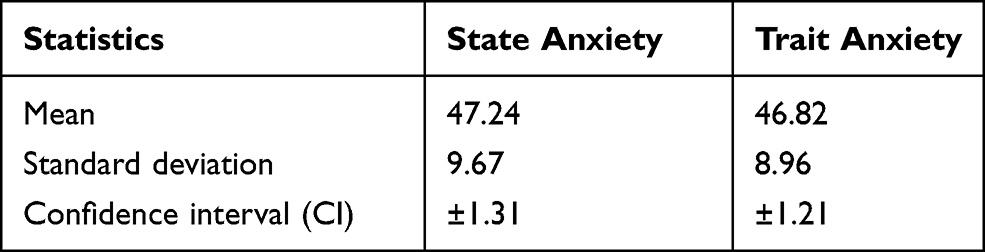 |
Table 7 Summary Statistics for the Total Sample |
Discussion
The present study revealed a high prevalence of both State and Trait anxiety among the sample population. Fewer female students had high levels of State and Trait anxiety (62% and 60%, respectively) compared with male students (70% and 74%, respectively). These findings were inconsistent with a study involving students in healthcare professions that found a higher percentage of females had high anxiety compared with males.26
Our findings of high State (89%) and Trait (68%) anxiety among students that reported sleeping for 4–5 hours or less (60%) was consistent with previous research that suggested sleep deprivation was associated with anxiety disorders.26
Those who were current smokers also reported high State (86%) and Trait (89%) anxiety. A previous study on smoking and anxiety found a strong association between smoking and new-onset mood and anxiety disorders among younger adults.28 Although this finding highlighted the association between smoking and anxiety, the direction of the relationship again remains unclear.
Over half (57%, n=33) of the students living on campus had high State anxiety and 53% had high Trait anxiety. Similarly, the majority (64%, n=87) of senior students had high State anxiety and high Trait anxiety of about 63%. Thus, being a resident off-campus was increased your chances of scoring high State and Trait anxiety. This is consistent with the literature findings.29 In terms of marital status, it did not matter whether one was single or was married, majority of the respondents scored high on the Trait anxiety above 50% and above 50% for the State anxiety.
The overall mean score for State anxiety and Trait anxiety were significantly high, suggesting a high level of anxiety in the university students involved in clinical practice as demonstrated in the literature. This calls for the University to put in place policies and support structures for students engaged in clinical/practicum subjects. The literature indicated that nursing students considered clinical training, an anxiety-producing aspects of their study.30 This also included their learning, performance, and well-being.31 Other causes considered initial clinical practice the most stressful period causing psychological distress. However, STAI scores by those who were involved in physical activity kept decreasing as the number of weekly physical activity increased.13,31 At the very minimum, physical activity, more than twice a week reduced the level of anxiety. This would imply that, students should be given opportunity and chances to be involved in more physical activity to keep their anxieties down.
Conclusions, Implications and Limitations
The primary purpose of this study was to investigate the extent of anxiety among university students undertaking clinical practice. This study indicates that there is a high prevalence of anxiety among clinical training students at the UOS, as 63% of the sample had high State anxiety and 62% had high Trait anxiety. The scores for State and Trait anxiety were high across all demographic variables, with overall mean scores of 47.24 and 46.82 for State and Trait anxiety, respectively. This suggests there is an urgent need to clarify factors associated with anxiety among these students to inform strategies to reduce anxiety and improve the conditions and circumstances for students undergoing clinical training. It is important for educators to recognize students’ anxiety during clinical training, and develop anxiety management strategies or interventions to ensure optimal clinical experiences for these students.
This study suggests that the UOS could enhance the clinical orientation program to reduce anxiety and stress among students. UOS administration could raise awareness on campus for students with anxiety and provide support, which could include offering counseling programs and sessions. We suggest that the UOS and training placements provide students with education and training about anxiety and mental health so that students and medical staff will be aware of the physiological aspects of anxiety reactions. Orientation to the hospital and training program may reduce stress and anxiety among students entering clinical training, especially sophomore and senior students, although the stressors may differ for each group. We recommend further comprehensive research on this topic. We also suggest more awareness on mental health and anxiety is needed in the general community to reduce the stigma associated with mental health problems that may make students reluctant to seek help and support.
The present results have important implications for policy, practice, research, and for students themselves. First, having policies that can protect and provide care and attention for students with anxiety may motivate and encourage students to speak up and seek help when needed. Second, determining the prevalence of anxiety in the UAE population will help the university to better understand the areas or situations that trigger anxiety among students, and work toward reducing or eliminating these factors. Third, this study can serve as a base for further investigation focused on improving the clinical training curriculum and providing the best training environment for students. Finally, the present findings can be used to inform specific measures to support students. This will help to provide a better training environment for students, with improved outcomes and benefits.
This study however had some limitations that should be taken into consideration. Firstly, the calculated sample size (n=219) was not achieved as nine of the original 220 participants were excluded because of unreliable data. However, the change in the sample size (n=210) is unlikely to have affected the results, as almost 96% of desired sample size was reached. Secondly, the sample was supposed to be selected using a simple random probability and got affected by COVID-19 pandemic Furthermore, the survey was supposed to be conducted face-to-face, but an online survey had to be used because of restrictions associated with the COVID-19 pandemic. The results were descriptive and not inferential and this limits the application of the information generated. The survey was disseminated using different social media platforms, and was distributed among students with mutual connections; this might have led to the unreliability of some responses.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The consent form and information sheet were provided to the respondents in both Arabic and English. Ethical approval for this study was obtained from the UOS Research Ethics Committee. The Committee approval number is REC-20-03-04-02-S.
Acknowledgments
The researchers thank all clinical training students from the UOS who took part in this study.
Disclosure
The authors have no competing interests to declare.
References
1. National Health Service, NHS. Overview - Generalised anxiety disorder in adults, NHS; 2018. Available from: https://www.nhs.uk/mental-health/conditions/generalised-anxiety-disorder/overview/#:~:text=GAD%20is%20a%20long%2Dterm,last%20time%20they%20felt%20relaxed.
2. Mayo Clinic. Anxiety disorders care at Mayo Clinic. Available from: https://www.mayoclinic.org/diseases-conditions/anxiety/symptoms-causes/syc-20350961.
3. Dyrbye LN, Thomas MR, Shanafelt TD. Medical student distress: causes, consequences, and proposed solutions. Mayo Clin proc. 2005;80(12):1613–1622. doi:10.4065/80.12.1613
4. Quek TT, Tam WW, Tran BX, et al. The global prevalence of anxiety among medical students: a meta-analysis. Int J Environ Res Public Health. 2019;16(15):2735. doi:10.3390/ijerph16152735
5. Francis B, Gill JS, Yit Han N, et al. Religious coping, religiosity, depression and anxiety among medical students in a multi-religious setting. Int J Environ Res Public Health. 2019;16(2):259. doi:10.3390/ijerph16020259
6. Bee Seok C, Abd Hamid HS, Mutang JA, Ismail R. Psychometric properties of the state-trait anxiety inventory (form Y) among Malaysian university students. Sustainability. 2018;10(9):3311. doi:10.3390/su10093311
7. Mahat G. Stress and coping: junior baccalaureate nursing students in clinical settings. Nurs Forum. 1998;33(1):9–11. doi:10.1111/j.1744-6198.1998.tb00976.x
8. Oermann MH, Lukomski AP. Experiences of students in pediatric nursing clinical courses. J Soc Paediatr Nur. 2001;6(2):65–72.
9. Nelwati D, McKenna L, Plummer V. Indonesian student nurses’ perceptions of stress in clinical learning: a phenomenological study. J Nurs Edu Pract. 2013;3(5):56–65. doi:10.5430/jnep.v3n5p56
10. Ab Latif R, Mat Nor MZ. Stressors and coping strategies during clinical practice among diploma nursing students. Malaysian J Med Sci. 2019;26(2):88–98. doi:10.21315/mjms2019.26.2.10
11. Samreen S, Siddiqui NA, Mothana RA. Prevalence of anxiety and associated factors among pharmacy students in Saudi Arabia: a Cross-Sectional Study. Biomed Res Int. 2020;6. doi:10.1155/2020/2436538
12. AIS – The American Institute of Stress. Anxiety in college students: causes, statistics & how universities can help; 2019. Available from: https://www.stress.org/anxiety-in-college-students-causes-statistics-how-universities-can-help. Accessed February 3, 2020.
13. American Psychological Association. College students’ mental health is a growing concern, survey finds. Monitor Psychol. 2013;44(6).
14. Bodenstein K, Nel M, Janse VVEC. Stressors and coping strategies among physiotherapy students: towards an integrated support structure. Health SA Gesondheid. 2018;23(1). doi:10.4102/hsag.v23i0.1091
15. Aktekin M, Karaman T, Senol YY, Erdem S, Erengin H, Akaydin M. Anxiety, depression and stressful life events among medical students: a prospective study in Antalya, Turkey. Med Edu. 2001;35(1):12–17. doi:10.1046/j.1365-2923.2001.00726.x
16. Ishtiaq S, Khan M, Shaheen A, Mansoor S. Prevalence of study related anxiety among female medical students. depression. 2013;5:8–10.
17. Inam SB. Anxiety and Depression among Students of a Medical College in Saudi Arabia. Int J Health Sci. 2007;1(2):295–300.
18. Hayes A. Simple Random Sample, Investopedia; 2019. Available from: https://www.investopedia.com/terms/s/simple-random-sample.asp. Accessed February 17, 2020.
19. Centers for Disease Control (CDC), Statcal, Epi Info™, Division of health informatics & surveillance (dhis), center for surveillance, epidemiology & laboratory services (CSELS). Available from: https://www.cdc.gov/epiinfo/user-guide/statcalc/statcalcandopenepi.html. Accessed June 17, 2021.
20. Spielberger CD. State-trait anxiety inventory for adults. USA: Mind Garden; 1968.
21. Bahammam MA. Validity and reliability of an Arabic version of the state-trait anxiety inventory in a Saudi dental setting. Saudi Med J. 2016;37(6):668. doi:10.15537/smj.2016.6.13935
22. Butcher JN, Taylor J, Fekken, GC. Objective Personality Assessment with Adults. Comprehensive Clinical Psychology. 1998;4:403–429.
23. Moscaritolo V. Interventional strategies to decrease nursing student anxiety in the clinical learning environment. J Nurs Edu. 2009;48(1):17–23. doi:10.3928/01484834-20090101-08
24. Kayikcioglu O, Bilgin S, Seymenoglu G, Deveci A. State and trait anxiety scores of patients receiving intravitreal injections. Biomed Hub. 2017;2(2):1–5. doi:10.1159/000478993
25. IBM _ International Business Machinery, Statistics for Social Scientists (SPSS) Software. Available from: https://www.ibm.com/ae-en/analytics/spss-statistics-software. Accessed 7 August, 2020.
26. Macauley Y, Plummer K, Bemis L, Brock C, Larson G, Spangler J. Prevalence and predictors of anxiety in healthcare professions students. Health Prof Edu. 2018;4(3):176–185. doi:10.1016/j.hpe.2018.01.001
27. ADAA – Anxiety and Depression Association of America. Sleep Disorders; 2018. Available from: https://adaa.org/understanding-anxiety/related-illnesses/sleep-disorders. Accessed June 14, 2020.
28. Mojtabai R, Crum RM. Cigarette smoking and onset of mood and anxiety disorders. Am J Public Health. 2013;103(9):1656–1665. doi:10.2105/AJPH.2012.300911
29. Liselotte N, Dyrbye MD, Matthew R, Thomas MD, Tait D, Shanafelt MD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian Medical Students. Acad Med. 2006;81(4).
30. Wang AH, Lee CT, Espin S. Undergraduate nursing students’ experiences of anxiety-producing situations in clinical practicums: a descriptive survey study. Nurse Educ Today. 2019;76:103–108. doi:10.1016/j.nedt.2019.01.016
31. Mosley TH Jr, Perrin SG, Neral SM, Dubbert PM, Grothues CA, Pinto BM. Stress, coping, and well-being among third-year medical students. Acad Med. 1994;69(9):765–767. doi:10.1097/00001888-199409000-00024
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.