Back to Journals » Clinical Interventions in Aging » Volume 13
Prevalence of functional dependence in Chinese centenarians and its relationship with serum vitamin D status
Authors Yao Y ![]() , Fu S, Shi Q, Zhang H
, Fu S, Shi Q, Zhang H ![]() , Zhu Q, Zhang F, Luan F, Zhao Y, He Y
, Zhu Q, Zhang F, Luan F, Zhao Y, He Y
Received 2 August 2018
Accepted for publication 25 September 2018
Published 17 October 2018 Volume 2018:13 Pages 2045—2053
DOI https://doi.org/10.2147/CIA.S182318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Yao Yao,1,* Shihui Fu,2,* Qiuling Shi,3 Hao Zhang,4 Qiao Zhu,5 Fu Zhang,5 Fuxin Luan,5 Yali Zhao,5 Yao He1
1Institute of Geriatrics, Beijing Key Laboratory of Aging and Geriatrics, National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Department of Geriatric Cardiology, Chinese PLA General Hospital, Beijing, People’s Republic of China; 3Department of Symptom Research, MD Anderson Cancer Center, Houston, TX, USA; 4Department of Health Policy and Management, Texas A&M University, College Station, TX, USA; 5Central Laboratory, Hainan Branch of Chinese PLA General Hospital, Sanya, People’s Republic of China
*These authors contributed equally to this work
Background: Functional dependence (FD) and vitamin D deficiency are common conditions in older adults. However, little is known about the relationship between FD and serum vitamin D status in centenarians. The current study was designed to evaluate the prevalence of FD and examine its relationship with serum vitamin D status among centenarians in China.
Subjects and methods: A cross-sectional study of a large sample of Chinese centenarians including 180 men and 822 women was conducted from June 2014 to December 2016. Home interviews, physical examinations, and blood analyses were performed in 958 centenarians following standard procedures. FD was evaluated using the Barthel index of activities of daily living (ADL). Serum 25-hydroxyvitamin D (25OHD) concentrations were measured as a marker of vitamin D status.
Results: The prevalence of centenarians with FD was 71.2%. Vitamin D deficiency, lack of tea consumption, lack of outdoor activities, visual impairment, and fracture were predictors of FD. Centenarians in the lowest quartile of serum 25OHD concentration had an approximately threefold greater likelihood of FD than those in the highest quartile in multiple logistic regression models (OR =2.88; 95% CI 1.75–4.73; P<0.001). The multivariable OR with a 1 ng/mL decrease in serum 25OHD concentration was 1.06 (95% CI 1.04–1.08; P<0.001) for FD.
Conclusion: Serum 25OHD levels have important associations with FD in Chinese centenarians. Future research could focus on the value of intervening in the case of low serum 25OHD levels through vitamin D supplementation and improving ADL in the older population.
Keywords: centenarians, China, functional dependence, vitamin D
Introduction
Functional dependence (FD), an aspect of disability measured by impairment in the activities of daily living (ADL; eg, feeding, dressing, bathing, and toileting),1 is related to numerous adverse health outcomes such as cognitive decline,2 mental disorder,3 worse resident quality of life,4 and the increased caregiver stress,5 and it plays a major role in transitions from independent living to nursing home care.1,6 In fact, with the rapid increase in life expectancy, the oldest old individuals (85 years of age and older) have been the fastest growing segment of the population. The oldest old individuals are more susceptible to FD with advanced age.7 The maintenance of physical function in late life is an important factor not only for a healthy and independent life in the community but also for preventing negative outcomes such as disability and early mortality.8–10 FD with aging is likely linked to several musculoskeletal and nutritional risk factors; thus, there is a further need to elucidate the impact of these factors in populations with advanced age.11,12
As a musculoskeletal risk factor, hypovitaminosis D is very common among older adults worldwide due to the reduced capacity of the skin to produce vitamin D, reduced sunlight exposure caused by less outdoor activity, and impaired nutrition.13–15 Previous studies have investigated the relationship between FD and vitamin D deficiency in older adults.16–18 However, only a few studies with a limited sample size have examined its relationship among the oldest old individuals, and contentious findings have been reported.19,20 In addition, surveys on the relationship between FD and vitamin D levels in centenarians are scarce, especially in developing countries. Considering the high prevalence of vitamin D deficiency and functional decline as people age, the relationship between vitamin D status and functional performance warrants a more focused examination among the oldest old populations including centenarians.
For these reasons, the aim of the current study was to investigate the prevalence of FD and to evaluate its relationship with serum 25-hydroxyvitamin D (25OHD) status among a group of population-based centenarians in China.
Subjects and methods
Study population
The sample of this study was obtained from the baseline survey of the China Hainan Centenarian Cohort Study (CHCCS), which was conducted in Hainan, China, from 2014 to 2016. Details of this study including sampling strategy and interview procedures have been described elsewhere.21,22 In brief, a total of 1,002 centenarians (180 men and 822 women aged 100 years and over) were interviewed, and blood samples were collected in this study. After excluding 44 participants who failed to provide complete information on physical examinations or blood analyses, 958 subjects (176 men and 782 women) were included in the final analysis.
Written informed consent was obtained from all men and women who participated in this study. The ethics committee of the Hainan branch of the Chinese People’s Liberation Army General Hospital (Sanya, Hainan) approved the study protocol (no. of serial: 301hn11201601).
Functional performance
To evaluate the FD of the centenarians, the Barthel index on the ADL was used;23 the validity and reliability of this tool in Chinese older people have been well established.24 The Barthel index consists of ten items that measure a person’s daily activities: grooming, feeding, dressing, bathing, toilet use, transferring from bed to chair, walking, stair climbing, bowel continence, and urinary continence. Each item of the ADL is rated on a scale with a given number of points assigned to each level of activity, and the total score ranges from 0 to 100 points with 5-point increments (Table S1). A higher score indicates higher levels of function. Items of the Barthel index are regarded as dependent if they are performed with any help from other people.25 Participants were deemed to have good functional capacity (independence) when the total score was ≥95 points; participants with a total score of <95 points were regarded as dependent.26
Vitamin D status
Serum circulating 25OHD is commonly measured to reflect vitamin D status.27 Blood samples were obtained from each participant by an experienced nurse and transported in cold storage to the Clinical Laboratory of the Hainan branch of the Chinese PLA General Hospital. Serum 25OHD concentrations were measured by automated radioimmunoassay analyzers (DiaSorin, Stillwater, MN, USA) using a standard procedure. The inter-assay and intra-assay coefficients of variation for serum 25OHD in the current study were 8.3% and 6.7%, respectively. Vitamin D deficiency was defined as 25OHD <20 ng/mL or 50 nmol/L according to the Endocrine Society Clinical Practice Guidelines.28
Covariates
Home interviews were conducted to collect data on the demographic details (age, gender, education, marital status, ethnicity, and living arrangements), season of blood collection, lifestyles (smoking, alcohol use, tea consumption, and outdoor activities), and common conditions (hypertension, diabetes, dyslipidemia, visual and auditory impairments, and fractures) of the participants. The ethnic origin was categorized as “Han” (the predominant ethnicity in China) and “non-Han”; the season of blood sampling was dichotomized into summer (April–September) and winter (October–March). The body mass index (BMI) was calculated as the weight in kilograms divided by the square height in meters. Blood samples from each participant were collected, and the plasma parathyroid hormone (PTH) levels were measured using automated electrochemiluminescence immunoassay (ECLIA) analyzers (Hoffman-La Roche Ltd., Basel, Switzerland). Smoking and alcohol use were categorized as “current,” “past,” and “never.” The habits of daily tea consumption and outdoor activities (more than 10 minutes) were divided into “yes” or “no.” Common conditions, including hypertension, diabetes, dyslipidemia, visual impairment, auditory impairment, and fractures, were recorded as self-reported combined with the medical records of the participants.
Statistical analyses
Categorical variables were reported as numbers with percentages, while continuous variables were reported as the mean with SD, and they were compared by Student’s t-test and chi-squared test, respectively. Multiple logistic regression analyses were performed to investigate the independent factors related to FD.
To examine its relationship with functional dependency, serum 25OHD concentrations were further categorized into quartiles (lowest, <16.3 ng/mL; second, 16.4–21.5 ng/mL; third, 21.6–28.0 ng/mL; and highest, >28.1 ng/mL). Differences of the Barthel index score and the sum of dependent items of ADL among four groups according to the quartiles of serum 25OHD levels were evaluated using one-way ANOVA and linear polynomial contrast analyses.
To elucidate the level of serum 25OHD associated with FD, logistic regression analyses were used to evaluate the odds of FD according to the quartiles of the serum 25OHD concentrations and a 1 ng/mL decrease in serum 25OHD concentrations with multiple adjustments for potential confounders. P for trend was evaluated by entering FD in the model as a ranked variable. A P-value of <0.05 was considered statistically significant. All analyses were carried out using SPSS software (version 19.0 for windows, no. of serial: 5087722; IBM Corporation, Armonk, NY, USA).
Results
The study sample included 782 women (81.6%) and 176 men (18.4%) with the mean age of 102.8 years. The prevalence of FD and vitamin D deficiency in the total sample was 71.2% and 39.7%, respectively. It was observed that 74.0% of women and 58.5% of men were functionally dependent (P<0.001), and 80.0% of participants with vitamin D deficiency and 65.4% without vitamin D deficiency had FD (P<0.001).
Table 1 summarizes the characteristics of participants with and without FD. The participants with FD had significantly lower values of serum 25OHD concentrations (21.7±9.5 vs 25.3±8.8 ng/mL; P<0.001) than those without FD. Subjects who were female, were illiterate, lived with family members, were evaluated in winter, were vitamin D deficient, had a higher PTH concentration, participated in less outdoor activities, had visual or auditory impairment, and suffered a fracture were more likely to be functionally dependent (P<0.05). Alcohol use and tea consumption were more common in functionally independent participants (P<0.05). Multiple logistic regression analyses revealed that vitamin D deficiency, tea consumption, outdoor activities, visual impairment, and fracture were significant factors related to FD in this population (Table 2). In addition, the participants with vitamin D deficiency have higher odds of dependence in eight functional items (including grooming, bathing, toilet use, dressing, feeding, stair climbing, transferring from bed to chair, and walking) than those without vitamin D deficiency (Table S2).
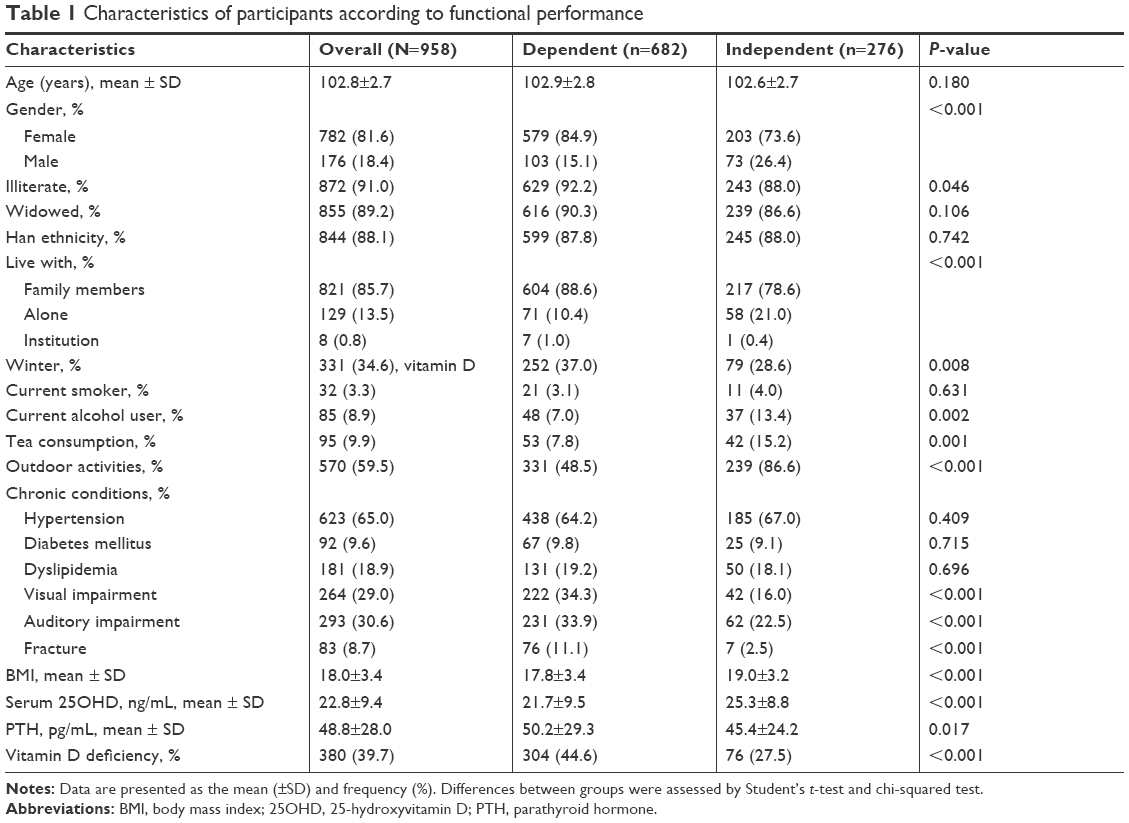 | Table 1 Characteristics of participants according to functional performance |
 | Table 2 Significant correlates of FD |
After participants were categorized into four groups according to the quartiles of serum 25OHD concentrations, an elevated trend of the Barthel index score (ranging from 64.6 in the lowest quartile to 82.5 in the highest quartile, P for trend <0.05) and a decreased trend of the sum of dependent ADL items (ranging from 4.8 in the lowest quartile to 2.6 in the highest quartile, P for trend <0.05) were observed. The trends remained constant after the stratification of participants by gender (Figure 1).
 | Figure 1 Functional performance by vitamin D status and its gender difference. |
Table 3 summarizes that the adjusted OR for the lowest vs highest quartile of serum 25OHD levels was 2.88 (1.75–4.73), and the adjusted odds of FD when comparing the second and third quartiles with the highest quartile were 1.91 (1.23–2.96) and 1.36 (0.90–2.07), respectively (P for trend <0.001). In addition, the multivariable adjusted OR with a 1 ng/mL decrease in serum 25OHD levels was 1.06 (1.04–1.08, P<0.001).
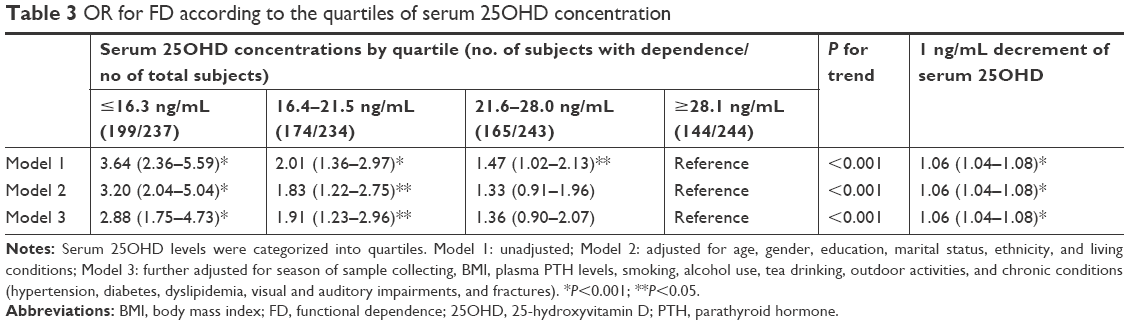 | Table 3 OR for FD according to the quartiles of serum 25OHD concentration |
Discussion
In this study, we observed an association between serum 25OHD levels and FD in a population-based sample of Chinese centenarians in Hainan province. Low serum 25OHD levels were associated with an increased prevalence of FD, and this association remained unchanged after adjusting for demographics and other potential confounders. Based on this Chinese study with a relatively large sample size, we added to the evidence of the association between vitamin D status and FD among extremely longevous people.
Several studies have shown an association between low serum vitamin D levels and FD among older individuals in developed countries such as USA and Japan.16,18 To the best of our knowledge, this is the first study to specifically focus on the relationship between FD and serum 25OHD levels in a representative sample of centenarians from a developing country.
The maintenance of physical function in old age is an important factor not only for a healthy and independent life in the community but also for preventing disability and early mortality.9,29 The current population-based study reported that nearly 3/4 of centenarians were functionally dependent; in other words, these subjects exhibited a decline in physical function and required help in the basic ADL. The finding is consistent with that of previous studies that have reported that the prevalence of FD among centenarians was 81% in Japan,30 76% in the USA,31 67% in Poland,9 and 61% in Australia.32 However, a lower dependence rate of 53% was observed in Denmark.33 Despite the controversy surrounding this concept, it was observed that centenarians who were functionally dependent were more likely to have 1-year mortality at a rate of 11.1% compared to those who were not;9 further effective interventions should be addressed among this population with FD.
The current study found that lower vitamin D levels were associated with higher adjusted odds of FD in the very old. In addition, higher Barthel scores and fewer dependent items of ADL were observed as the serum 25OHD levels increased, suggesting that vitamin D may exert a dose-dependent effect on physical function. This result was comparable with the findings of other studies in old adult populations.16 However, a study of Georgia centenarians has reported that vitamin D status is not associated with physical function but rather with grip strength; this diverse result could be explained by different measurements used by the Georgia Centenarian Study Composite Scale which had very different components from the Barthel index.19
Several pathophysiological mechanisms may explain the link between low serum 25OHD levels and FD. First, vitamin D plays a beneficial role in the musculoskeletal system, and low serum 25OHD levels have been reported to be associated with osteoporosis, sarcopenia, and fractures, which lead to frailty and functional decline.34 The bioactive form of vitamin D, calcitriol, has been reported to regulate the cell biology of skeletal muscle, and the expression of vitamin D receptor (VDR) played a role in skeletal muscle regeneration following injury.35 VDR gene polymorphisms are also associated with variations in muscle strength in human beings, and genetic ablation of VDR leads to muscle fiber atrophy and motor deficits in mice. Second, vitamin D deficiency is associated with arterial stiffness and endothelial function, which have potential adverse influence on physical function.36–38 Calcitriol also modulates expression in vascular smooth muscle cells, thus protecting against vascular calcification and arterial stiffness and further reducing the risk of heart attack, stroke, or other cardiovascular-related disabilities.39 Third, the immunomodulatory effect is also a physiological role of vitamin D, where calcitriol regulates both adaptive and innate immunity and is related to host resistance to infection.40,41 Moreover, vitamin D has been reported to play a critical role in cognitive function and mental health.3,42 Vitamin D plays a neuroprotective role through several physiological mechanisms such as calcium homeostasis, neurogenesis, antioxidant defense, immunomodulation, and amyloid beta clearance.43–45
Serum 25OHD concentrations, not calcitriol, were measured as a marker of vitamin D status in this study. Quantitation of serum 25OHD provides a clinically useful and reliable assessment of one’s vitamin D status for several reasons.46 First, the serum half-life of serum 25OHD is approximately 3 weeks.47 This rather long circulating half-life serves as an accurate marker of vitamin D scores obtained from both ultraviolet B radiation and dietary intake over long periods. Second, liver production of serum 25OHD is not significantly regulated and is primarily dependent on substrate concentration. For these reasons, the measurement of serum 25OHD provides the best estimate of an individual’s vitamin D status.27
Several observational studies have reported associations between functional declines with lower serum 25OHD levels.16,48 In addition, a few randomized control trials have shown evidence that vitamin D supplementation improves functional performance.17,49 Thus, maintaining adequate vitamin D levels or the intake of vitamin D supplements among the very old may potentially help to prevent declines in physical function and preserve good ADL.18,19 Considering the low cost of vitamin D supplements and the lack of habitual intake of vitamin D supplementation among the elderly population in China, it is critical to closely examine the association between vitamin D levels and the preservation or improvement in physical function in this population.
Limitations
As there is little knowledge on FD and limited data on the relationship between functional decline and vitamin D status among the very old in developing countries, our data provide novel insights into the nature of this relationship among a representative sample of centenarians in China. Nevertheless, the study has some potential limitations. First, our results do not indicate any causal inferences due to the cross-sectional design, and additional cohort studies with follow-up data are essential to strengthen the evidence. Second, other factors such as cognitive impairment and psychological situations were not included in this study, and hence, potential confounders may remain unrecognized. Third, the data on chronic conditions were based on self-reported data; thus, the subjectivity derived from it should also be acknowledged in this study.
Conclusion
This study reports that FD is common in a population-based sample of centenarians in China, and serum 25OHD levels were independently and inversely associated with FD in this extremely longevous population. Future research could focus on the value of intervening in the case of low serum 25OHD levels through vitamin D supplementation and improving ADL in older populations.
Acknowledgments
We appreciate all the staff of the Hainan Centenarian Study for their continued cooperation and contribution to the field work. This study was supported by grants from the National Natural Science Foundation of China (81371561, 81773502) and the Key Research and Development Program of Hainan (ZDYF2016169, ZDYF2017095, and ZDYF2017126). The sponsors had played no role in the design, conduct, interpretation, review, approval, or control of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
Portegijs E, Rantakokko M, Viljanen A, Sipilä S, Rantanen T. Identification of Older People at Risk of ADL Disability Using the Life-Space Assessment: A Longitudinal Cohort Study. J Am Med Dir Assoc. 2016;17(5):410–414. | ||
Black SA, Rush RD. Cognitive and functional decline in adults aged 75 and older. J Am Geriatr Soc. 2002;50(12):1978–1986. | ||
Yao Y, Fu S, Zhang H, et al. The prevalence of depressive symptoms in Chinese longevous persons and its correlation with vitamin D status. BMC Geriatr. 2018;18(1):198. | ||
Lyu W, Wolinsky FD. The Onset of ADL Difficulties and Changes in Health-Related Quality of Life. Health Qual Life Outcomes. 2017;15(1):217. | ||
Bruce DG, Paley GA, Nichols P, Roberts D, Underwood PJ, Schaper F. Physical disability contributes to caregiver stress in dementia caregivers. J Gerontol A Biol Sci Med Sci. 2005;60(3):345–349. | ||
Samus QM, Mayer L, Onyike CU, et al. Correlates of functional dependence among recently admitted assisted living residents with and without dementia. J Am Med Dir Assoc. 2009;10(5):323–329. | ||
Lunney JR, Lynn J, Foley DJ, Lipson S, Guralnik JM. Patterns of functional decline at the end of life. JAMA. 2003;289(18):2387–2392. | ||
Visnjevac O, Lee J, Pourafkari L, Dosluoglu HH, Nader ND, Kritchevsky S. Functional capacity as a significant independent predictor of postoperative mortality for octogenarian ASA-III patients. J Gerontol A Biol Sci Med Sci. 2014;69(10):1229–1235. | ||
Mossakowska M, Broczek K, Wieczorowska-Tobis K, et al. Cognitive performance and functional status are the major factors predicting survival of centenarians in Poland. J Gerontol A Biol Sci Med Sci. 2014;69(10):1269–1275. | ||
Vermeulen J, Neyens JC, van Rossum E, Spreeuwenberg MD, de Witte LP. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: a systematic review. BMC Geriatr. 2011;11:33. | ||
Daly RM, Rosengren BE, Alwis G, Ahlborg HG, Sernbo I, Karlsson MK. Gender specific age-related changes in bone density, muscle strength and functional performance in the elderly: a-10 year prospective population-based study. BMC Geriatr. 2013;13:71. | ||
Singh DK, Manaf ZA, Yusoff NA, Muhammad NA, Phan MF, Shahar S. Correlation between nutritional status and comprehensive physical performance measures among older adults with undernourishment in residential institutions. Clin Interv Aging. 2014;9:1415–1423. | ||
Hilger J, Friedel A, Herr R, et al. A systematic review of vitamin D status in populations worldwide. Br J Nutr. 2014;111(1):23–45. | ||
Holick MF, Chen TC. Vitamin D deficiency: a worldwide problem with health consequences. Am J Clin Nutr. 2008;87(4):1080S–1086S. | ||
Cabral MA, Borges CN, Maia JM, Aires CA, Bandeira F. Prevalence of vitamin D deficiency during the summer and its relationship with sun exposure and skin phototype in elderly men living in the tropics. Clin Interv Aging. 2013;8:1347–1351. | ||
Sohl E, van Schoor NM, de Jongh RT, Visser M, Deeg DJ, Lips P. Vitamin D status is associated with functional limitations and functional decline in older individuals. J Clin Endocrinol Metab. 2013;98(9):E1483–E1490. | ||
Zhu K, Austin N, Devine A, Bruce D, Prince RL. A randomized controlled trial of the effects of vitamin D on muscle strength and mobility in older women with vitamin D insufficiency. J Am Geriatr Soc. 2010;58(11):2063–2068. | ||
Kojima G, Tamai A, Masaki K, et al. Prevalence of vitamin D deficiency and association with functional status in newly admitted male veteran nursing home residents. J Am Geriatr Soc. 2013;61(11):1953–1957. | ||
Haslam A, Johnson MA, Hausman DB, et al. Vitamin D status is associated with grip strength in centenarians. J Nutr Gerontol Geriatr. 2014;33(1):35–46. | ||
Matheï C, van Pottelbergh G, Vaes B, Adriaensen W, Gruson D, Degryse JM. No relation between vitamin D status and physical performance in the oldest old: results from the Belfrail study. Age Ageing. 2013;42(2):186–190. | ||
He Y, Zhao Y, Yao Y, et al. Cohort Profile: The China Hainan Centenarian Cohort Study (CHCCS). Int J Epidemiol. 2018;47(3):694–695. | ||
Yao Y, Chen X, Wu S, et al. Thyroid nodules in centenarians: prevalence and relationship to lifestyle characteristics and dietary habits. Clin Interv Aging. 2018;13:515–522. | ||
Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65. | ||
Leung SO, Chan CC, Shah S. Development of a Chinese version of the Modified Barthel Index – validity and reliability. Clin Rehabil. 2007;21(10):912–922. | ||
Quinn TJ, Langhorne P, Stott DJ. Barthel index for stroke trials: development, properties, and application. Stroke. 2011;42(4):1146–1151. | ||
van Hartingsveld F, Lucas C, Kwakkel G, Lindeboom R. Improved interpretation of stroke trial results using empirical Barthel item weights. Stroke. 2006;37(1):162–166. | ||
Zerwekh JE. Blood biomarkers of vitamin D status. Am J Clin Nutr. 2008;87(4):1087S–1091S. | ||
Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–1930. | ||
Scott WK, Macera CA, Cornman CB, Sharpe PA. Functional health status as a predictor of mortality in men and women over 65. J Clin Epidemiol. 1997;50(3):291–296. | ||
Ozaki A, Uchiyama M, Tagaya H, Ohida T, Ogihara R. The Japanese Centenarian Study: autonomy was associated with health practices as well as physical status. J Am Geriatr Soc. 2007;55(1):95–101. | ||
Jopp DS, Park MK, Lehrfeld J, Paggi ME. Physical, cognitive, social and mental health in near-centenarians and centenarians living in New York City: findings from the Fordham Centenarian Study. BMC Geriatr. 2016;16(1):1. | ||
Richmond RL, Law J, Kay-Lambkin F. Physical, mental, and cognitive function in a convenience sample of centenarians in Australia. J Am Geriatr Soc. 2011;59(6):1080–1086. | ||
Andersen-Ranberg K, Schroll M, Jeune B. Healthy centenarians do not exist, but autonomous centenarians do: a population-based study of morbidity among Danish centenarians. J Am Geriatr Soc. 2001;49(7):900–908. | ||
Hirani V, Cumming RG, Naganathan V, et al. Longitudinal Associations Between Vitamin D Metabolites and Sarcopenia in Older Australian men: The Concord Health and Aging in Men Project. J Gerontol A Biol Sci Med Sci. 2017;12;73(1):131–138 | ||
Srikuea R, Zhang X, Park-Sarge OK, Esser KA. VDR and CYP27B1 are expressed in C2C12 cells and regenerating skeletal muscle: potential role in suppression of myoblast proliferation. Am J Physiol Cell Physiol. 2012;303(4):C396–C405. | ||
Mozos I, Stoian D, Luca CT. Crosstalk between Vitamins A, B12, D, K, C, and E Status and Arterial Stiffness. Dis Markers. 2017;2017(2):8784971. | ||
Wang TJ, Pencina MJ, Booth SL, et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation. 2008;117(4):503–511. | ||
Caraba A, Crişan V, Romoşan I, Mozoş I, Murariu M. Vitamin D Status, Disease Activity, and Endothelial Dysfunction in Early Rheumatoid Arthritis Patients. Dis Markers. 2017;2017(8). | ||
Mary A, Hénaut L, Boudot C, et al. Calcitriol prevents in vitro vascular smooth muscle cell mineralization by regulating calcium-sensing receptor expression. Endocrinology. 2015;156(6):1965–1974. | ||
Cantorna MT, Zhu Y, Froicu M, Wittke A. Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system. Am J Clin Nutr. 2004;80(6 Suppl):S1717–S1720. | ||
Christakos S, Dhawan P, Verstuyf A, Verlinden L, Carmeliet G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol Rev. 2016;96(1):365–408. | ||
Matchar DB, Chei CL, Yin ZX, et al. Vitamin D Levels and the Risk of Cognitive Decline in Chinese Elderly People: the Chinese Longitudinal Healthy Longevity Survey. J Gerontol A Biol Sci Med Sci. 2016;71(10):1363–1368. | ||
Dickens AP, Lang IA, Langa KM, Kos K, Llewellyn DJ. Vitamin D, cognitive dysfunction and dementia in older adults. CNS Drugs. 2011;25(8):629–639. | ||
Kalueff AV, Eremin KO, Tuohimaa P. Mechanisms of neuroprotective action of vitamin D(3). Biochemistry. 2004;69(7):738–741. | ||
Kesby JP, Eyles DW, Burne TH, McGrath JJ. The effects of vitamin D on brain development and adult brain function. Mol Cell Endocrinol. 2011;347(1–2):121–127. | ||
Holick MF. Vitamin D: importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am J Clin Nutr. 2004;79(3):362–371. | ||
Clemens TL, Zhou XY, Myles M, Endres D, Lindsay R. Serum vitamin D2 and vitamin D3 metabolite concentrations and absorption of vitamin D2 in elderly subjects. J Clin Endocrinol Metab. 1986;63(3):656–660. | ||
Houston DK, Neiberg RH, Tooze JA, et al. Low 25-hydroxyvitamin D predicts the onset of mobility limitation and disability in community-dwelling older adults: the Health ABC Study. J Gerontol A Biol Sci Med Sci. 2013;68(2):181–187. | ||
Janssen HC, Samson MM, Verhaar HJ. Muscle strength and mobility in vitamin D-insufficient female geriatric patients: a randomized controlled trial on vitamin D and calcium supplementation. Aging Clin Exp Res. 2010;22(1):78–84. |
Supplementary materials
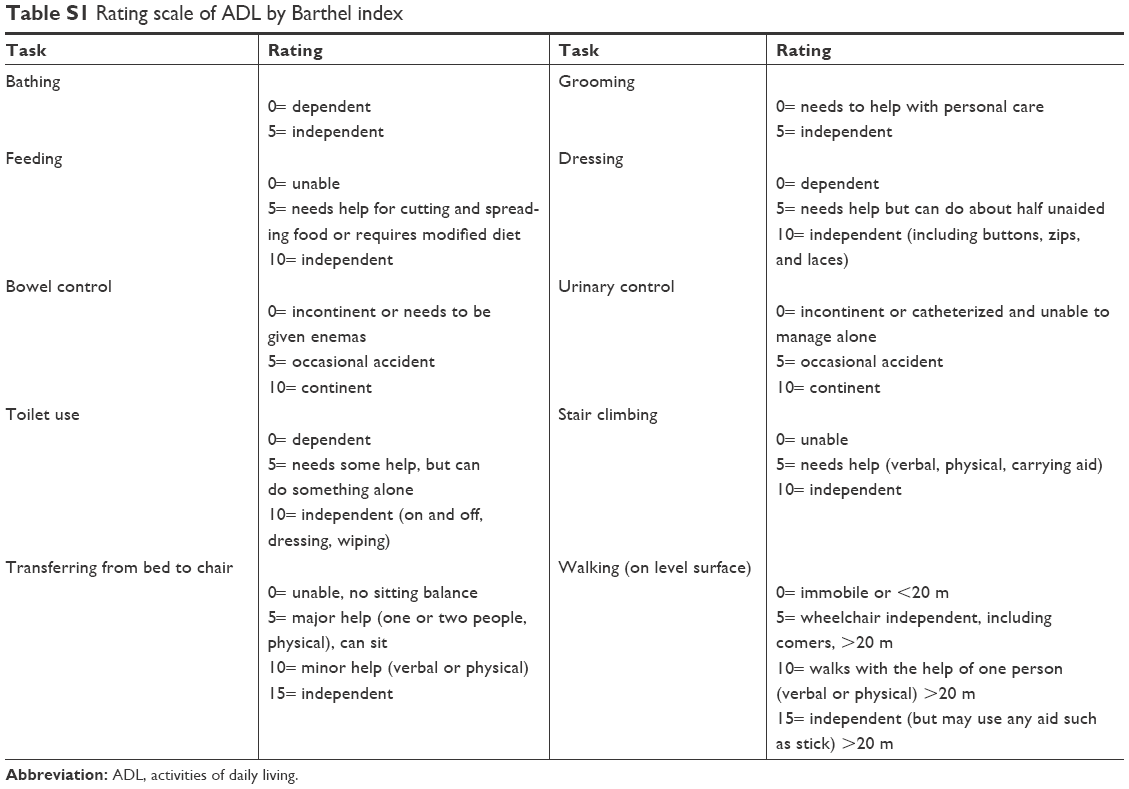 | Table S1 Rating scale of ADL by Barthel index |
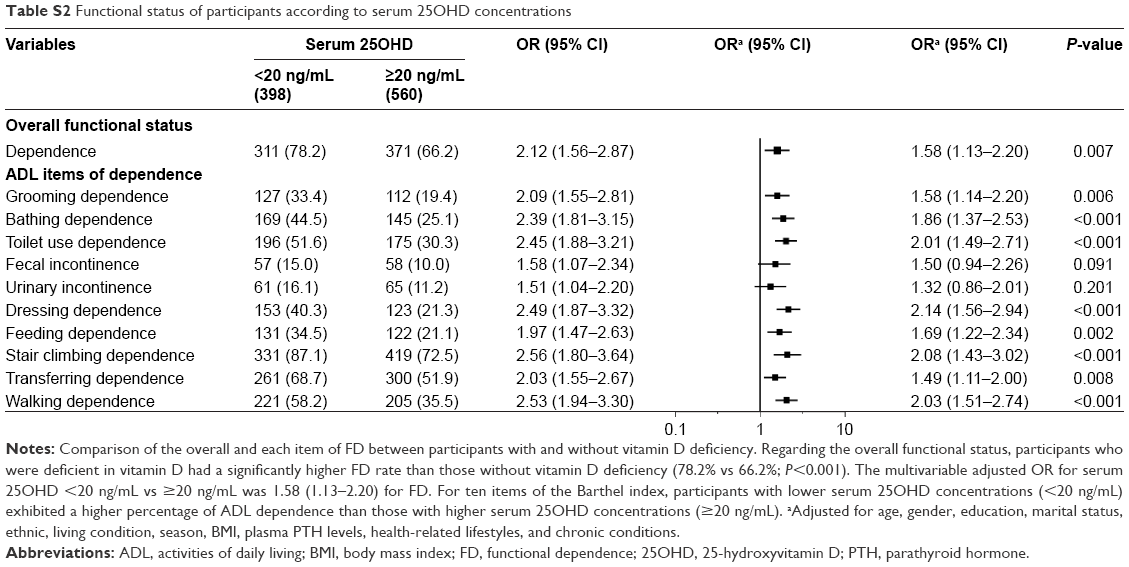 | Table S2 Functional status of participants according to serum 25OHD concentrations |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.