Back to Journals » Infection and Drug Resistance » Volume 13
Prevalence of Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae Causing Bloodstream Infections in Cancer Patients from Southwest of Iran
Authors Abbasi Montazeri E, Khosravi AD ![]() , Saki M
, Saki M ![]() , Sirous M
, Sirous M ![]() , Keikhaei B, Seyed-Mohammadi S
, Keikhaei B, Seyed-Mohammadi S ![]()
Received 18 March 2020
Accepted for publication 21 April 2020
Published 6 May 2020 Volume 2020:13 Pages 1319—1326
DOI https://doi.org/10.2147/IDR.S254357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Effat Abbasi Montazeri,1,2,* Azar Dokht Khosravi,1,2,* Morteza Saki,1– 3 Mehrandokht Sirous,2,4 Bijan Keikhaei,5 Sakineh Seyed-Mohammadi1– 3
1Infectious and Tropical Diseases Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 2Department of Microbiology, Faculty of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 3Student Research Committee, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 4Department of Microbiology and Parasitology, Faculty of Medicine, Bushehr University of Medical Sciences, Bushehr, Iran; 5Thalassemia and Hemoglobinopathy Research Center, Health Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
*These authors contributed equally to this work
Correspondence: Morteza Saki; Sakineh Seyed-Mohammadi Tel +98 9364221187
; +98 9352655807
Fax +98 6133332036
Email [email protected]; [email protected]
Introduction: This study aimed to evaluate the frequency rate of extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL-PE) causing bloodstream infections (BSIs) in cancer patients referred to one of the major referral hospitals in Ahvaz city, southwest Iran.
Materials and Methods: In this study, 1700 blood cultures were collected from 610 cancer patients suspected to have BSI from October 2016 to August 2017 referred to the Shafa cancer hospital, Ahvaz, southwest of Iran. The blood culture bottles were incubated aerobically at 35– 37ºC for 24 hours and then sub-cultured on routine microbiology culture media. The bacterial colonies were identified using standard tests. The antibiotic susceptibility testing was achieved by the disc-diffusion method. The phenotypic detection of ESBLs was carried out by the combination disc-diffusion test (CDDT). Finally, the polymerase chain reaction (PCR) was performed to investigate the presence of blaTEM, blaCTX, blaSHV, and blaPER genes.
Results: The prevalence of BSI in cancer patients was 16.4% (100/610). Gram-negative rods with rate of 74% (74/100) were the most prevalent bacteria. The frequency of Enterobacteriaceae family was 21% including Escherichia coli (n: 8), Klebsiella pneumoniae (n: 6), Enterobacter spp. (n: 5), Citrobacter freundii (n: 1), and Serratia marcescens (n: 1). All isolates were multidrug-resistant (resistance to three or more antibiotics). The results of CDDT showed that 42.8% (9/21) of Enterobacteriaceae isolates had a positive ESBL test of which 100% (9/9) indicated positive band for at least one of the ESBL genes by PCR method. The blaCTX-M and blaTEM genes were detected in 38% (8/21) and 23.8% (5/21) of isolates, respectively, while the blaSHV and blaPER were not detected in any isolates.
Conclusion: Based on the results, surveillance, and antibiotic stewardship programs should be implemented for cancer patients to prevent the spread of more ESBL-PE that have limited therapeutically choices.
Keywords: extended-spectrum beta-lactamase, ESBL, cancer patients, Enterobacteriaceae, hematological malignancies, Iran
Introduction
Bloodstream infection (BSI) is a significant complication in cancer patients receiving cytotoxic chemotherapy due to their immunocompromised condition, which accompanies with a high rate of morbidity and mortality.1 The most common outcome of chemotherapeutic agents is neutropenia that could lead to the severity of bacterial infections in patients suffering from cancer.2
The incidence of BSIs among cancer patients has been reported to range from 11.8 to 33.3%, and among these the greater proportion have caused by Gram-negative bacteria.3 In recent years, the spread of BSI caused by extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL-PE) has been reported increasingly in patients with cancer in different regions of the world.4,5 Moreover, emerging of multidrug-resistant Enterobacteriaceae has become a major public health problem.5
The ESBLs are carried on bacterial plasmids that can be transferred to other bacteria.6 Several ESBL classes have been detected in Enterobacteriaceae strains of which the CTX-M, TEM, and SHV beta-lactamases are the most common types.7 ESBL-PE are usually resistant to most beta-lactam antibiotics, however, carbapenems are considered the drugs of choice for treatment of infections caused by these bacteria.7,8
Since there is no adequate epidemiological information of ESBL-PE in cancer patients in Iran, this study aimed to evaluate the frequency of BSI causing ESBL-PE in patients suffering from different cancers in the southwest of Iran to provide a guide for suitable empiric antibiotic therapy.
Materials and Methods
Ethical Consideration
The current study was approved by the ethics committee of Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran (No: IR.AJUMS.REC.1395.323). Written informed consent was obtained from all patients.
Sampling
This cross-sectional study was carried out on blood cultures obtained from cancer patients suspected to BSI during 10 months period from October 2016 to August 2017 referred to the Shafa cancer hospital, Ahvaz, Iran. The Shafa hospital is one of the major referral hospitals for cancer patients in the southwest of Iran which located in Khuzestan province. The demographic data collected from every patient including age, sex, duration of hospitalization, and cancer type. During the febrile period, a volume of 5–10 mL or 1–3 mL of the peripheral blood sample was collected from adults and pediatric patients, respectively. For each patient, 3 separate blood samples from 3 different sites were collected. The blood samples were inoculated in blood culture bottles containing trypticase soy broth (TSB) (Baharafshan Co., Tehran, Iran) and incubated aerobically at 35–37ºC for 24 hours.
Microbial Identification
Bacterial identification carried out by sub-culture of the sample of bottles on blood agar, chocolate agar, MacConkey agar, and mannitol salt agar. All media were prepared from Merck Co., Darmstadt, Germany. The bacterial colonies were identified using standard biochemical tests including coagulase, catalase, triple sugar iron agar, Simmon̍s citrate, urease, indole production, Methyl red/Voges-Proskauer, and oxidase.9 When the same bacterium was isolated from three samples of one patient, only one isolate was considered for further investigation.
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility test was carried out for Enterobacteriaceae isolates by the disc-diffusion method according to guidelines of the Clinical and Laboratory Standards Institute (CLSI).10 The isolates with turbidity equal to 0.5 McFarland standards were lawn cultured on Mueller-Hinton agar (MHA) plates. Then the antimicrobial discs were placed on the MHA plates. Finally, the plates were incubated at 35ºC for 24h. The antibiotics used were as follows: piperacillin (100 µg), tetracycline (75 µg), piperacillin-tazobactam (100/10 µg), ceftazidime (30 µg), cefotaxime (30 µg), cefepime (30 µg), imipenem (10 µg), meropenem (10 µg), gentamicin (10 µg), ciprofloxacin (5 µg), and aztreonam (5 µg). Escherichia coli ATCC 25922, and Pseudomonas aeruginosa ATCC 27853 were used as quality control strains. Methicillin-resistant S. aureus (MRSA) and methicillin-resistant coagulase-negative staphylococci (MRCONS) isolates were identified using the cefoxitin disc according to guidelines of CLSI.10 The bacterial suspensions equal to 0.5 McFarland standards were inoculated on MHA and a cefoxitin (30 µg) disc placed on the medium. The plates incubated at 33–35ºC for 18–24 h. The isolate was considered methicillin-resistant when the inhibition zone was equal to ≤ 21 mm or ≤ 24 mm for MRSA and MRCoNS, respectively. S. aureus ATCC 29213 and ATCC 33591 were used as methicillin-sensitive and resistant control strains, respectively.
Phenotypic Detection of ESBLs
The Enterobacteriaceae isolates that were resistant to one or more of third-generation cephalosporins were screened for ESBL production by combination disc-diffusion test (CDDT) included ceftazidime and cefotaxime alone and with ceftazidime + clavulanic acid and cefotaxime + clavulanic acid (Mast group, Merseyside, UK). An ESBL positive isolate was identified by the increase of inhibition zone size of ≥ 5 mm in the presence of clavulanic acid.11 Escherichia coli ATCC 25922, and Klebsiella pneumoniae ATCC700603 were used as the ESBL negative and positive controls, respectively.
Polymerase Chain Reaction (PCR) for Detection of ESBL Genes
DNA Extraction
The total DNA was extracted from fresh colonies of Enterobacteriaceae isolates by the boiling method as described previously.12 Briefly, 2 or 3 colonies of an overnight growth of each isolate on nutrient agar (Merck Co., Darmstadt, Germany) were suspended in 500 mL of DNase- and RNase-free water. The suspension was boiled at 100 °C for 10 min in a dry block incubator (Polystat 5; Bioblock Scientific, France), then centrifuged at 14,000 g for 10 min. Finally, 0.5 mL of the supernatant was used as DNA template for PCR. The extracted DNA was stored at −20°C until analysis.
PCR Protocol
The phenotypic ESBL positive isolates in this study were investigated for the presence of blaCTX-M, blaTEM, blaSHV, and blaPER by PCR using specific primer mentioned in Table 1. The PCR was performed in the BIO-RAD C1000 thermal cycler (Applied Biosystems, USA) in a final volume of 25 µL containing 12.5 µL of PCR master mix, 1 µL of each primer (10 pmol), 1 µL of sample DNA, and 9.5 µL of nuclease-free water. The PCR conditions were as follows: initial denaturation at 94°C for 5 minutes, followed by 35 cycles of denaturation at 95°C for 35 seconds, different annealing temperatures (Table 1) for 35 seconds, and extension at 72°C for 30 seconds, with a final extension period of 72°C for 5 minutes. The amplicons were analyzed by agarose gel electrophoresis stained with safe stain (Sinaclon Co., Tehran, Iran) and visualized using an ultraviolet gel documentation device (Protein Simple, San Jose, CA, USA). The control positive genes were prepared from the Pasteur Institute of Iran.
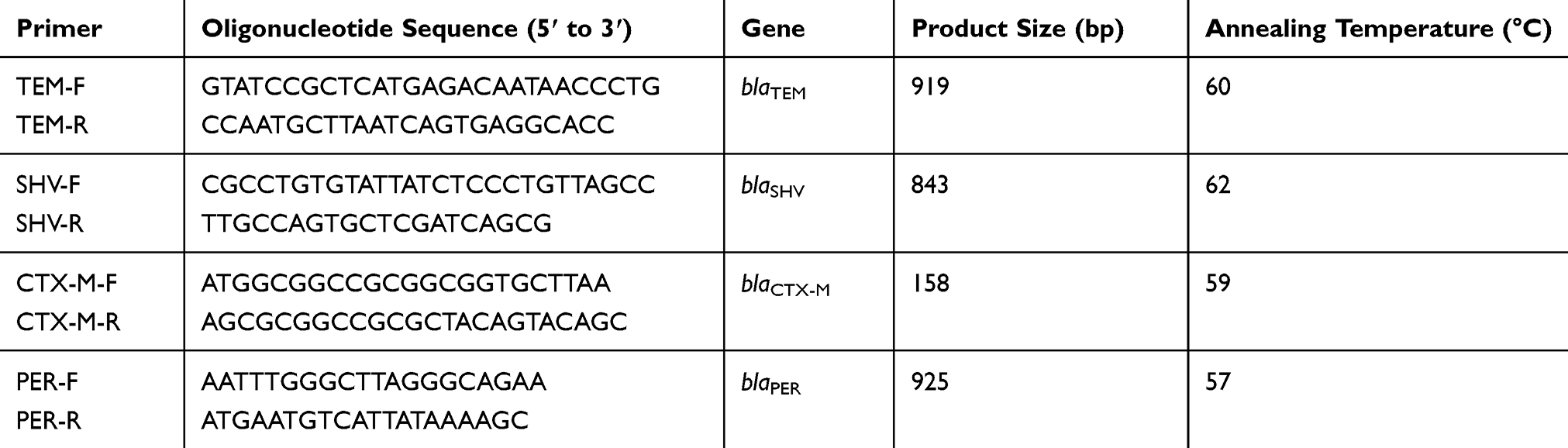 |
Table 1 The Primer Sequences Used for Extended-Spectrum Beta-Lactamase Genes Detection |
Statistical Analysis
The statistical analysis was performed using SSPS version 22.0 (IBM Corporation, Armonk, NY, USA). The comparison of variables was carried out by the chi-square test and Fischer’s exact test where appropriate. A p-value < 0.05 was considered statistically significant.
Results
In this study, 610 cancer patients aged 1 to 76 years (mean 42 years) referred to Shafa hospital in Ahvaz city, southwest of Iran were evaluated. Hematological malignancies were seen in 400 (65.5%) patients while the remaining had solid organ cancer. During the study period, 1700 peripheral blood cultures were collected from 610 patients. Overall, 450 blood cultures of three hundred patients were positive for bacterial growth, of which 100 non-duplicate isolates were identified. In other words, the prevalence of BSI in cancer patients was 16.4% (100/610) of which 75% was seen in patients with hematological malignancies and 25% in solid tumors cases (Table 2). Of these patients, 53 (53%) were females while 47 (47%) were males. The neutropenia (neutrophil count below <1000/mm3) was seen in 79.4% and 14.3% of hematological cancer and solid tumor patients, respectively.
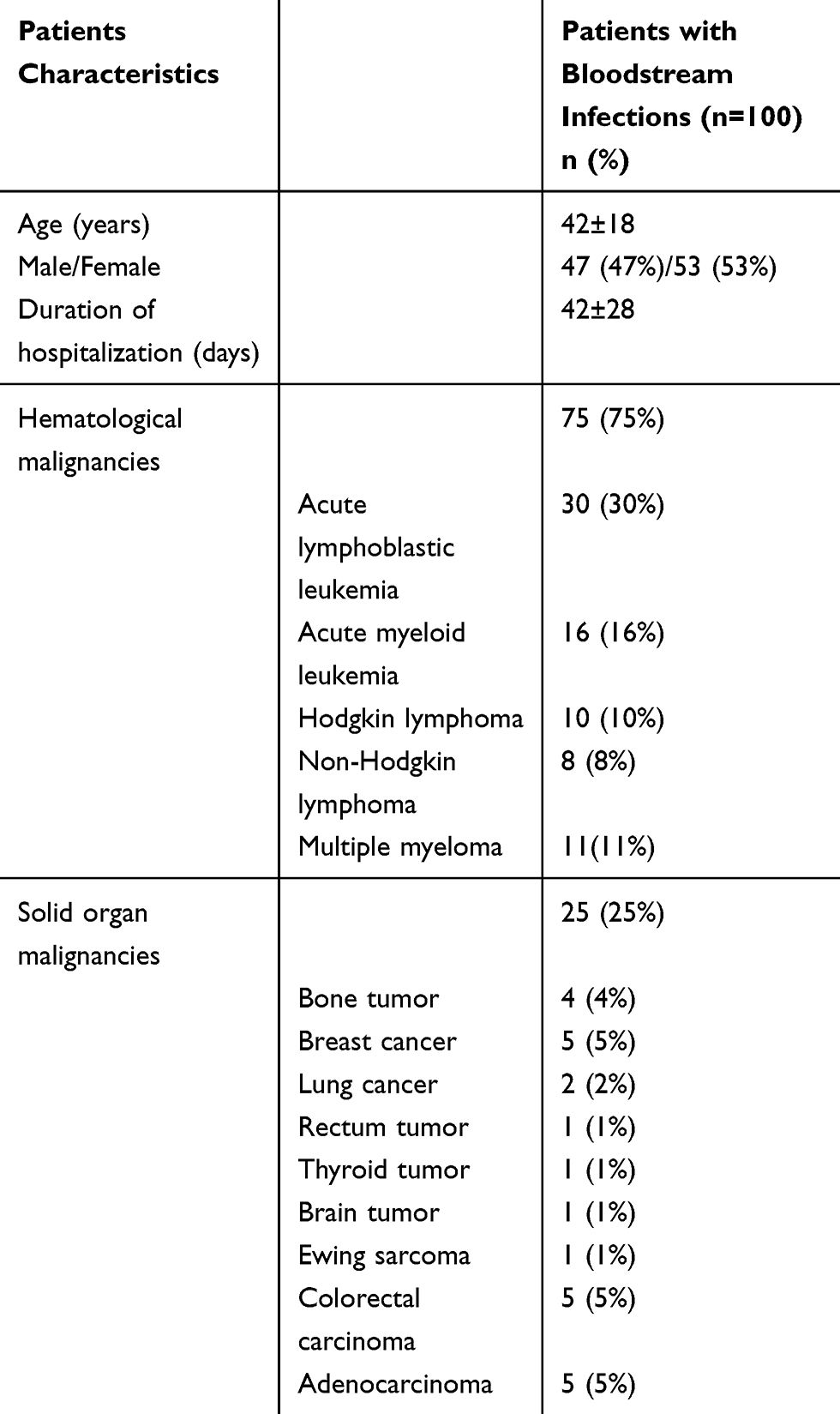 |
Table 2 Demographic Features of Cancer Patients with Bloodstream Infections |
Gram-negative rods with the rate of 74% (74/100) were the most prevalent bacteria. The Pseudomonas aeruginosa was the most frequent isolate (41%), followed by Coagulase-negative staphylococci (16%), and Acinetobacter baumannii (12%). Moreover, 10 (10%) S. aureus strains were isolated of which 5 isolates were methicillin-resistant. Of the 16 coagulase-negative staphylococci, 8 isolates were methicillin-resistant. The frequency of the Enterobacteriaceae family was 21% including Escherichia coli (n: 8), Klebsiella pneumoniae (n: 6), Enterobacter spp. (n: 5), Citrobacter freundii (n: 1), and Serratia marcescens (n: 1) (Table 3). The resistance rate in Enterobacteriaceae isolates was as follows: cefotaxime 76.1%, ceftazidime 85.7%, cefepime 47.6%, imipenem 28.6%, meropenem 90.4%, piperacillin 76.1%, piperacillin-tazobactam 28.6%, tetracycline 38.1%, gentamycin 28.6%, ciprofloxacin 28.6%, and aztreonam 52.3%. The most effective antibiotics against E. coli were imipenem and gentamycin with a 62.5% susceptibility rate, while the less effective antibiotics were ceftazidime and cefotaxime with an 87.5% resistance rate. The detailed results of antibiotic susceptibility test for E. coli, K. pneumonia, and Enterobacter spp. are presented in Table 4. The Citrobacter freundii, and Serratia marcescens isolates were resistant to all tested antibiotics except for piperacillin-tazobactam, gentamycin, and ciprofloxacin. All Enterobacteriaceae isolates were resistant to three or more antibiotics and considered as multidrug-resistant (MDR) strains. The MDR patterns of Enterobacteriaceae isolates are shown in Table 5.
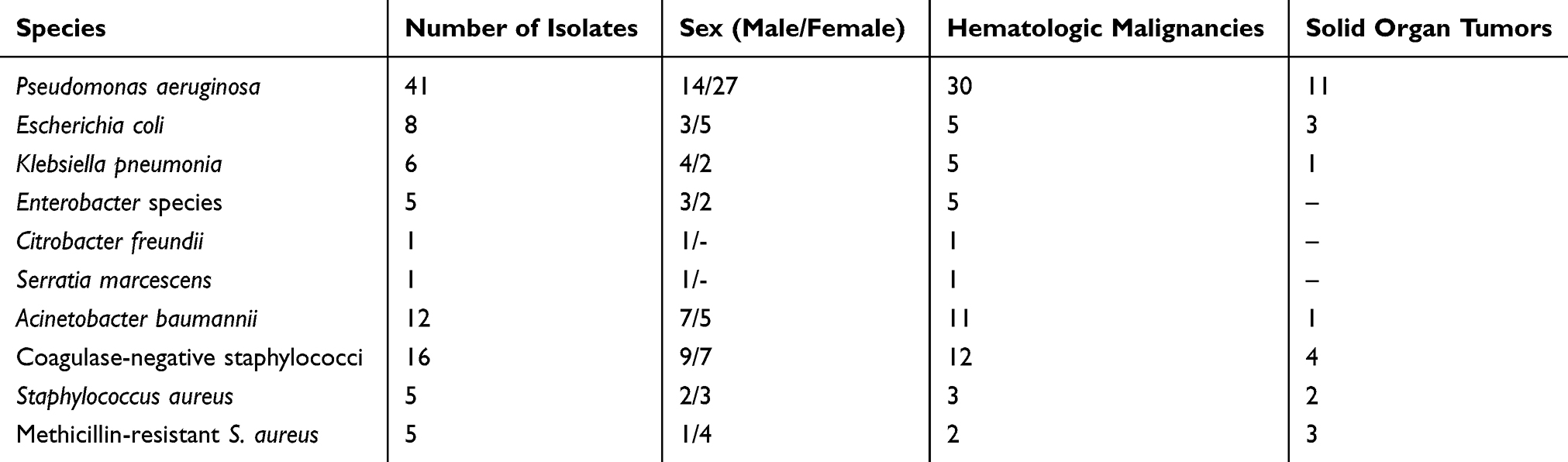 |
Table 3 Bacterial Isolates Causing Bloodstream Infection in Cancer Patients |
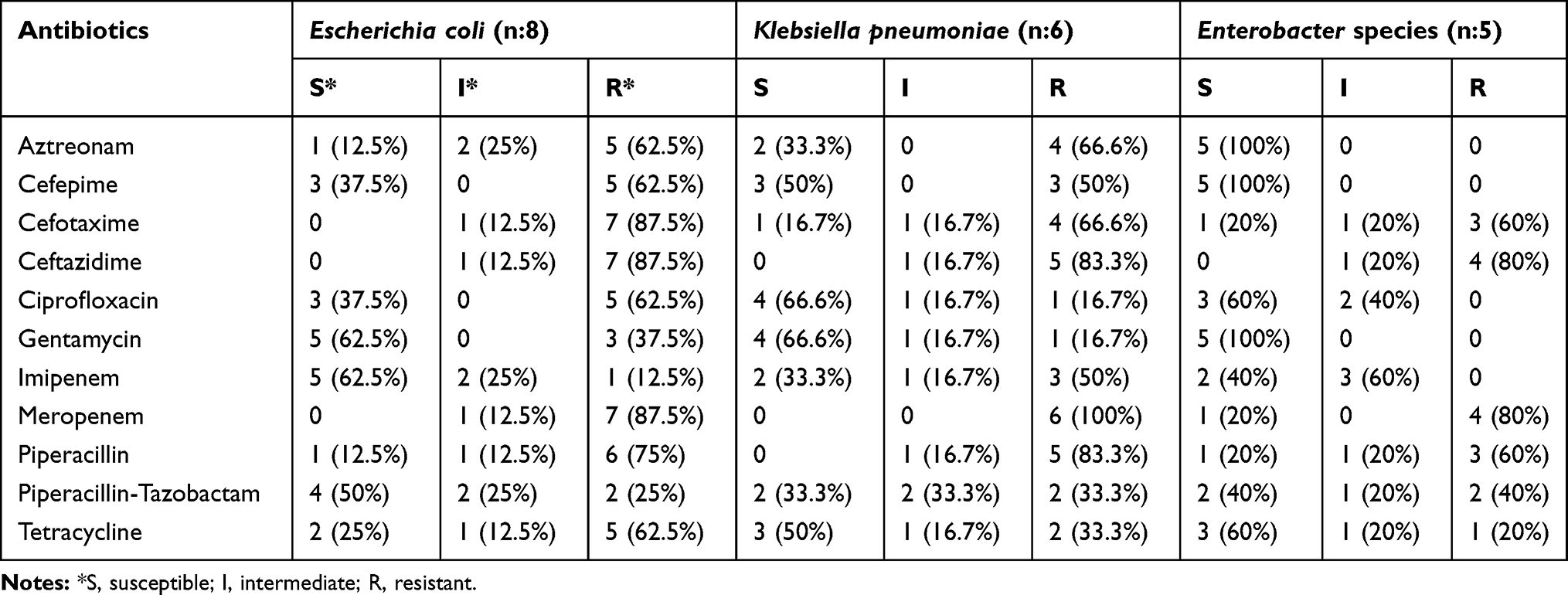 |
Table 4 Antibiotic Resistance Patterns of Enterobacteriaceae Isolates |
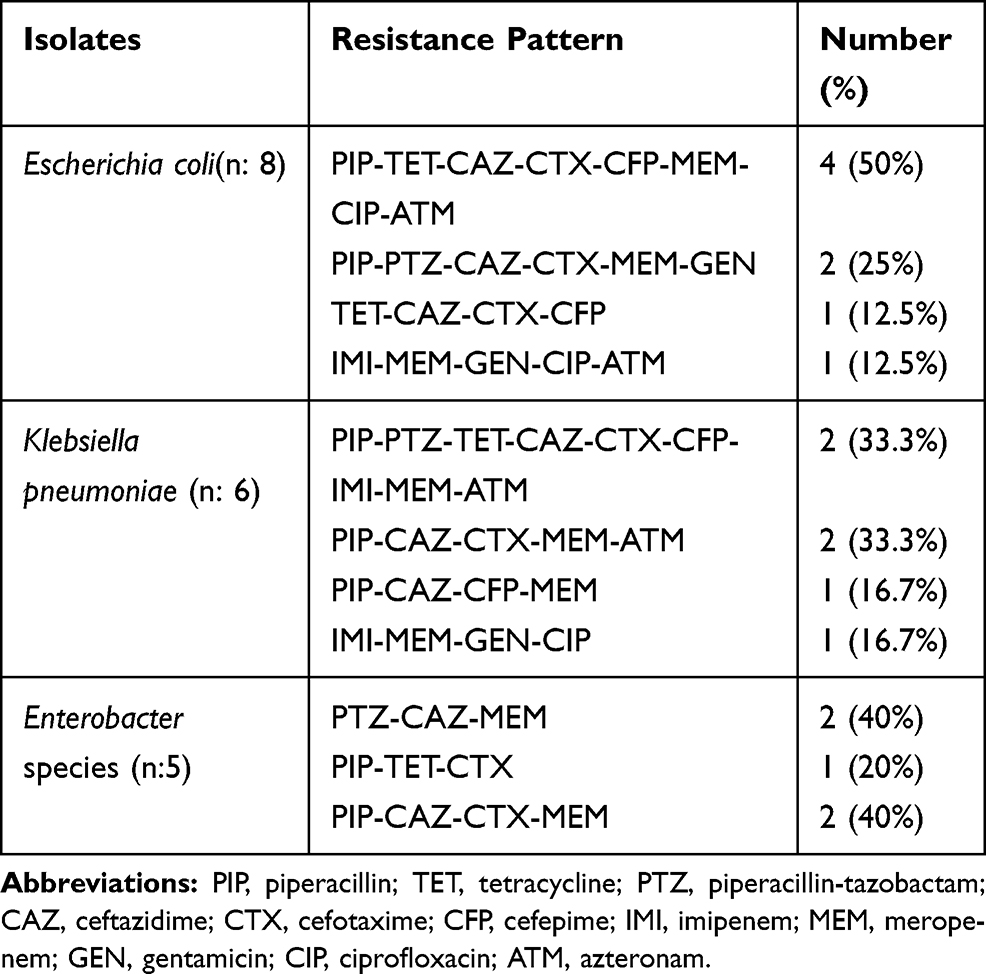 |
Table 5 The Multidrug Resistance Patterns of Enterobacteriaceae Isolates |
The results of CDDT showed that 42.8% (9/21) of Enterobacteriaceae isolates had a positive ESBL test of which 100% (9/9) indicated positive band for at least one of the ESBL genes by PCR method. The blaCTX-M and blaTEM genes were detected in 38% (8/21) and 23.8% (5/21) of isolates, respectively, while the blaSHV and blaPER were not detected in any isolates. Also, 4 (19%) isolates co-harbored blaCTX-M and blaTEM genes. The phenotype and genotype results of ESBL-PE are summarized in Table 6. The statistical analysis revealed that the production of ESBLs in Enterobacteriaceae was not significantly associated with resistance to a particular type of antibiotic (p-value ˃ 0.05) and there was no difference between the two groups of ESBL producers and non-producers. The data were not shown.
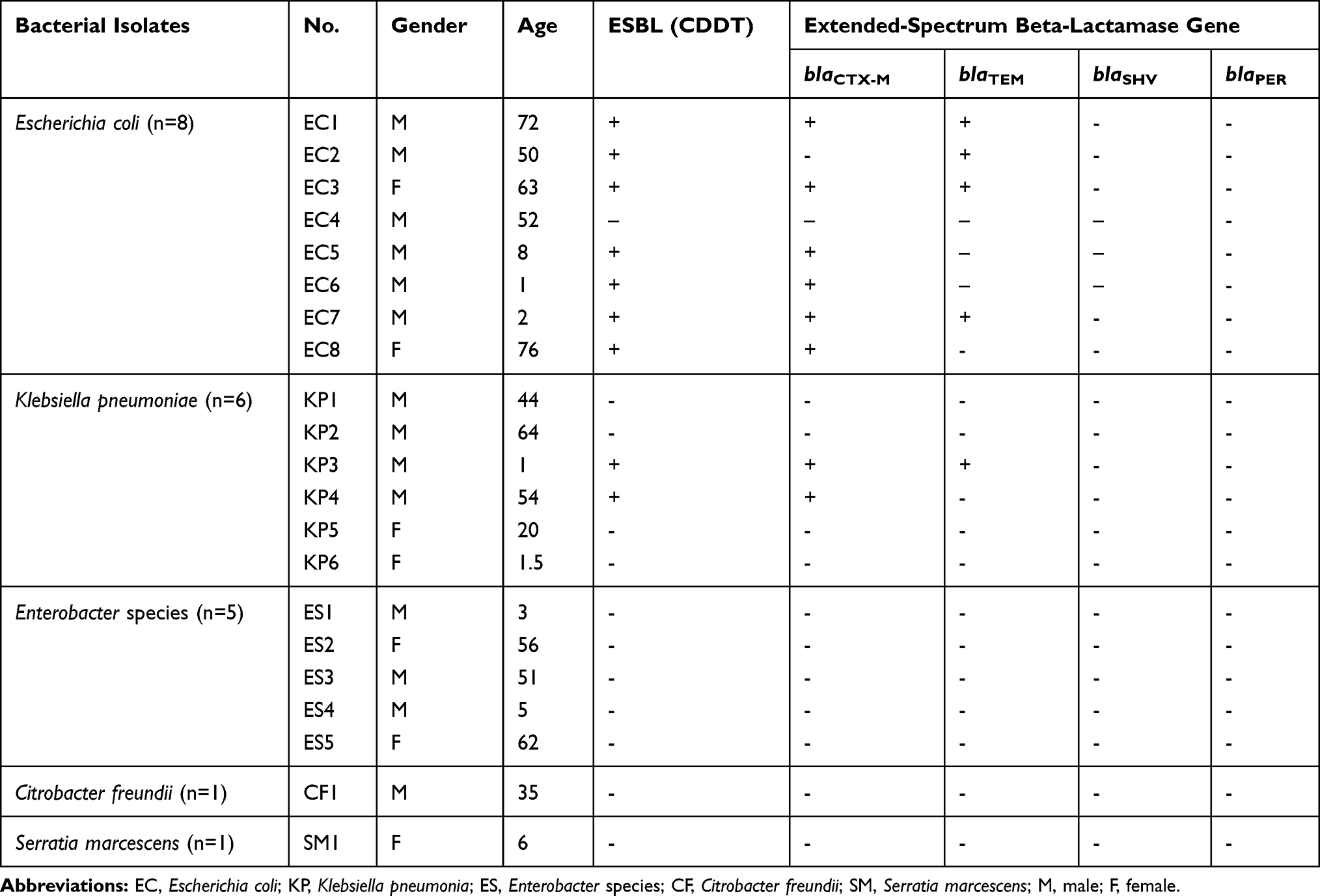 |
Table 6 The Frequency of Extended-Spectrum Beta-Lactamase Genes in Enterobacteriaceae Isolates |
Discussion
Infection is a significant problem in immunosuppressed patients with cancer due to chemotherapy treatment. Patients suffering from BSI during neutropenia episodes caused by chemotherapy should use an adequate antibiotics as soon as possible. The BSI caused by Gram-negative bacteria has poor prognoses in these patients. Rapid initiation of treatment by adequate antibiotic for neutropenic patients result in reduce the mortality rate.13,14 Thus, the evaluation of the microbial spectrum of BSI in the cancer patients is an important aspect that should be considered in every country for rapid empirical therapy.
In this study, 16.4% of patients suffering from hematological and solid organ malignancies had BSI which was lower than the previous study by Obeng-Nkrumah et al3 from Ghana who reported the BSI in 22% of cancer patients and higher than the report by Lubwama et al15 from Uganda who showed the BSI in 14.1% of cancer patients.
In the current research, The Gram-negative bacteria cause 74% of all BSI cases that was consistent with previous reports.16,17 However, previous studies from Iran and Australia indicated the Gram-positive cocci isolates as a leading cause of BSIs in cancer patients.18–20 These dissimilarities in the bacterial spectrum of different regions and countries indicate that recognizing infection-related pathogens in each area is very important for better control of these microorganisms in the cancer patients. In recent years, various countries have reported that the spectrum of bacteria causing BSIs in the cancer patients has shifted from Gram-positive isolates to Gram-negative strains and Gram-negative bacteria appear to occupy the place of Gram-positive isolates, which may be due to the relatively lower use of indwelling medical devices, as well as lower prescribing of prophylactic antibiotic treatments in cancer patients.3,21,22 Among Gram-positive bacteria the coagulase-negative staphylococci with 16% were the most frequent strains followed by S. aureus with a 10% frequency rate that was comparable to findings of Rosa et al23 from Brazil. Furthermore, half of S. aureus isolates were methicillin-resistant. In the current study, the P. aeruginosa was the most frequent isolate (41%) in BSI that was in line with findings of Marin et al24 from Spain while in contrast with our results a report by Islas-Munoz et al25 from Mexico showed the E. coli as the most predominant isolate causing BSI in cancer patients. Besides, the Enterobacteriaceae isolates that were detected in 21% of BSI cases in this study included E. coli (8%), K. pneumoniae (6%), Enterobacter spp. (5%), C. freundii (1%), and S. marcescens (1%). The frequency of the Enterobacteriaceae family was in agreement with a report from European countries that claimed these bacteria account for approximately 30% (range 8–56%) of the BSIs in hematology centers.26 Also, in this study, the E. coli isolates occupy the first place among the Enterobacteriaceae family in BSIs cases. Likewise, in a prospective study conducted from September 2012 to September 2014 by Babu et al27 from India, the E. coli was the most frequent isolate followed by Acinetobacter baumannii and K. pneumonia.
Importantly, the results of antibiotic susceptibility testing revealed that all Enterobacteriaceae isolates were MDR, of which 42.8% were ESBL producers. In recent decades, the spread of ESBL-PE has become one of the major health concerns because these bacteria have the ability to transfer the antibiotic resistance genes to other bacteria that lead to severe infection with limited therapeutic options. To our knowledge, this is the first research that investigated the prevalence of ESBL-PE in BSIs among cancer patients in Iran. The high frequency of MDR ESBL-producing Gram-negative rods among cancer patients was in line with reports from Uganda,15,28 and India.29 In our study, ESBLs were identified in 9 (42.8%) of 21 Enterobacteriaceae isolates and similar to what has been described in previous reports the E. coli strains were the main ESBL producers.30 Also, there was no significant association between age (p-value: 0.88), sex (p-value: 0.25), and type of cancer (p-value: 0.91) with ESBL-PE in this study. Another noteworthy finding of this study was the higher prevalence rate of ESBL-PE compared to other Eastern Mediterranean countries in which the pooled prevalence of ESBL-PE was reported 7%.31
Carbapenems, such as imipenem, ertapenem, and meropenem are recommended antibiotics for treatment of infection cases caused by ESBL-PE.8 However, the meropenem with a resistance rate of 90.4% did not seem to be an appropriate antibiotic to treat infections caused by Enterobacteriaceae in cancer patients in our region. Another very harmful challenge for the health system of all countries is the increasing trend of carbapenem-resistant Enterobacteriaceae that have also emerged in Iran.32 Meanwhile, another carbapenem, imipenem with 71.4% susceptibility rate showed a more efficiency against MDR Enterobacteriaceae in this study. Likewise, the piperacillin-tazobactam, gentamycin, and ciprofloxacin with 71.4% susceptibility rate showed good effects against Enterobacteriaceae and could be considered for BSIs treatment. Given the good efficacy of ciprofloxacin as a fluoroquinolone, it seems that these antibiotic categories could be prescribed for BSI treatment in cancer patients in our region. This recommendation relies on the high susceptibility rate of the blood culture isolates to fluoroquinolone in clinical trials performed in Western countries as the American Society of Clinical Oncology policy recommends immediate quinolone-based oral empiric antibiotic therapy in cancer patients.33 In the current cross-sectional study the high resistance rate against third-generation cephalosporins which may due to ESBLs production highlights the need of our institution to make an urgent policy to restrict the use of this antibiotic category. In the current study, blaCTX-M with 38% frequency rate was the most prevalent gene followed by blaTEM gene with a prevalence of 23.8% that was in parallel with previous reports that showed the predominance of blaCTX-M in various countries.34–36 Also 19% of ESBL-PE co-harbored blaCTX-M and blaTEM genes. So far, similar to our findings, several studies have reported the co-existence of ESBL genes in Enterobacteriaceae.34,36,37
Conclusion
This study showed the predominance of MDR Gram-negative bacteria caused BSIs in cancer patients that harboring ESBL genes. Thus, surveillance and antibiotic stewardship programs should be implemented for cancer patients to prevent the spread of more ESBL-PE that have limited therapeutically choices. Also, we found that the piperacillin-tazobactam, gentamycin, and ciprofloxacin could be considered in the treatment of BSIs caused by Enterobacteriaceae in our region. Further studies involving healthcare centers of different regions of Iran is needed to warrant the selection of appropriate empirical antibiotics, particularly in cancer patients.
Acknowledgment
This research was financially supported by the Vice Chancellor for Research Affairs and Infectious and Tropical Diseases Research Center, Health Research Institute, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran (grant no: OG-95114).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Garcia-Vidal C, Carratalà J, Gudiol C, et al. Bacteraemia due to multidrug-resistant Gram-negative bacilli in cancer patients: risk factors, antibiotic therapy and outcomes. J Antimicrob Chemother. 2010;66(3):657–663. doi:10.1093/jac/dkq494
2. Strojnik K, Mahkovic-Hergouth K, Novakovic BJ, Seruga B. Outcome of severe infections in afebrile neutropenic cancer patients. Radiol Oncol. 2016;50(4):442–448. doi:10.1515/raon-2016-0011
3. Obeng-Nkrumah N, Labi AK, Acquah ME, Donkor ES. Bloodstream infections in patients with malignancies: implications for antibiotic treatment in a Ghanaian tertiary setting. BMC Res Notes. 2015;8(1):742. doi:10.1186/s13104-015-1701-z
4. Chandramohan L, Revell PA. Prevalence and molecular characterization of extended-spectrum-β-lactamase-producing Enterobacteriaceae in a pediatric patient population. Antimicrob Agents Chemother. 2012;56(9):4765–4770. doi:10.1128/AAC.00666-12
5. Tohamy ST, Aboshanab KM, El-Mahallawy HA, El-Ansary MR, Afifi SS. Prevalence of multidrug-resistant Gram-negative pathogens isolated from febrile neutropenic cancer patients with bloodstream infections in Egypt and new synergistic antibiotic combinations. Infect Drug Resist. 2018;11:791. doi:10.2147/IDR.S163293
6. Bai L, Wang L, Yang X, et al. Prevalence and molecular characteristics of extended-spectrum β-lactamase genes in Escherichia coli isolated from diarrheic patients in China. Front Microbiol. 2017;8:144. doi:10.3389/fmicb.2017.00144
7. Ur Rahman S, Ali T, Ali I, Khan NA, Han B, Gao J. The growing genetic and functional diversity of extended spectrum beta-lactamases. BioMed Res Int. 2018;2018.
8. Rodríguez-Baño J, Gutiérrez-Gutiérrez B, Machuca I, Pascual A. Treatment of infections caused by extended-spectrum-beta-lactamase-, AmpC-, and carbapenemase-producing Enterobacteriaceae. Clin Microbiol Rev. 2018;31(2):e00079–17.
9. Amin M, Sirous M, Javaherizadeh H, et al. Antibiotic resistance pattern and molecular characterization of extended-spectrum β-lactamase producing enteroaggregative Escherichia coli isolates in children from southwest Iran. Infect Drug Resist. 2018;11:1097-1104.
10. CLSI. M100; Performance Standards for Antimicrobial Susceptibility Testing.
11. Kjerulf A, Hansen DS, Sandvang D, Hansen F, Frimodt-Moller N. The prevalence of ESBL-producing E. coli and Klebsiella strains in the Copenhagen area of Denmark. APMIS. 2008;116(2):118–124. doi:10.1111/j.1600-0463.2008.00777.x
12. Sheikh AF, Moosavian M, Abdi M, et al. Prevalence and antimicrobial resistance of Shigella species isolated from diarrheal patients in Ahvaz, southwest Iran. Infect Drug Resist. 2019;12:249–253. doi:10.2147/IDR.S187861
13. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;52(4):e56–e93.
14. Marín M, Gudiol C, Ardanuy C, et al. Factors influencing mortality in neutropenic patients with haematologic malignancies or solid tumours with bloodstream infection. Clin Microbiol Infect. 2015;21(6):583–590. doi:10.1016/j.cmi.2015.01.029
15. Lubwama M, Phipps W, Najjuka CF, et al. Bacteremia in febrile cancer patients in Uganda. BMC Res Notes. 2019;12(1):464. doi:10.1186/s13104-019-4520-9
16. Gedik H, Yildirmak T, Simsek F, et al. The outcome of non-carbapenem-based empirical antibacterial therapy and VRE colonisation in patients with hematological malignancies. Afr Health Sci. 2013;13(2):362–368. doi:10.4314/ahs.v13i2.24
17. Gedik H, Şimşek F, Yıldırmak T, et al. Which multidrug-resitant bacteria are emerging in patients with hematological malignancies?: one-Year Report. Indian J Hematol Blood Transfus. 2015;31(1):51–56. doi:10.1007/s12288-014-0402-4
18. Khodashahi R, Hakemi-Vala M, Mardani M, et al. Blood culture and antimicrobial susceptibility pattern of bacteria and fungi isolated from febrile neutropenic patients treated with chemotherapy at Taleghani hospital, Tehran. Iran J Microbiol. 11;2:90–97.
19. Meidani M, Bagheri A, Khorvash F. A population-based study of bacterial spectrum in febrile neutropenic patients. Jundishapur J Microbiol. 2013;6(2):150–156. doi:10.5812/jjm.4941
20. Carvalho AS, Lagana D, Catford J, Shaw D, Bak N. Bloodstream infections in neutropenic patients with haematological malignancies. Infect Dis Health. 2020;25(1):22–29. doi:10.1016/j.idh.2019.08.006
21. Mangaraj O, Barkataki D, Mohan DG. Gram negative bacilli causing blood stream infection in febrile neutropenic patients in a tertiary care centre. Int J Contemp Med Res. 2017;4(7):1599–1603.
22. Arega B, Woldeamanuel Y, Adane K, Sherif AA, Asrat D. Microbial spectrum and drug-resistance profile of isolates causing bloodstream infections in febrile cancer patients at a referral hospital in Addis Ababa, Ethiopia. Infect Drug Resist. 2018;11:1511–1519. doi:10.2147/IDR.S168867
23. Rosa RG, Goldani LZ, Dos Santos RP. Risk factors for multidrug-resistant bacteremia in hospitalized cancer patients with febrile neutropenia: a cohort study. Am J Infect Contr. 2014;42(1):74–76. doi:10.1016/j.ajic.2013.06.025
24. Marin M, Gudiol C, Ardanuy C, et al. Bloodstream infections in neutropenic patients with cancer: differences between patients with haematological malignancies and solid tumours. J Infect. 2014;69(5):417–423. doi:10.1016/j.jinf.2014.05.018
25. Islas-Muñoz B, Volkow-Fernández P, Ibanes-Gutiérrez C, Villamar-Ramírez A, Vilar-Compte D, Cornejo-Juárez P. Bloodstream infections in cancer patients. Risk factors associated with mortality. Int J Infect Dis. 2018;71:59–64. doi:10.1016/j.ijid.2018.03.022
26. Gustinetti G, Mikulska M. Bloodstream infections in neutropenic cancer patients: a practical update. Virulence. 2016;7(3):280–297. doi:10.1080/21505594.2016.1156821
27. Babu KG, Lokanatha D, Lakshmaiah KC, et al. Bloodstream infections in febrile neutropenic patients at a tertiary cancer institute in South India: a timeline of clinical and microbial trends through the years. Indian J Med Paediatr Oncol. 2016;37(3):174–182. doi:10.4103/0971-5851.190352
28. Seni J, Najjuka CF, Kateete DP, et al. Antimicrobial resistance in hospitalized surgical patients: a silently emerging public health concern in Uganda. BMC Res Notes. 2013;6(1):298. doi:10.1186/1756-0500-6-298
29. Ghosh I, Raina V, Kumar L, et al. Profile of infections and outcome in high-risk febrile neutropenia: experience from a tertiary care cancer center in India. Med Oncol. 2012;29(2):1354–1360. doi:10.1007/s12032-011-9858-3
30. Kim Y-J, Jung SM, Kang J, et al. Risk factors for extended-spectrum beta-lactamase-producing Enterobacteriaceae infection causing septic shock in cancer patients with chemotherapy-induced febrile neutropenia. Intern Emerg Med. 2019;14(3):433–440. doi:10.1007/s11739-018-02015-x
31. Alevizakos M, Gaitanidis A, Andreatos N, Arunachalam K, Flokas ME, Mylonakis E. Bloodstream infections due to ESBL-producing Enterobacteriaceae among patients with malignancy: a systematic review and meta-analysis. Int J Antimicrob Agents. 2017;50(5):657–663. doi:10.1016/j.ijantimicag.2017.07.003
32. Zahedi Bialvaei A, Samadi Kafil H, Ebrahimzadeh Leylabadlo H, Asgharzadeh M, Aghazadeh M. Dissemination of carbapenemases producing Gram negative bacteria in the Middle East. Iran J Microbiol. 2015;7(5):226–246.
33. Zhang S, Wang Q, Ling Y, Hu X. Fluoroquinolone resistance in bacteremic and low risk febrile neutropenic patients with cancer. BMC Cancer. 2015;15(1):42. doi:10.1186/s12885-015-1063-x
34. Mirkalantari S, Masjedian F, Irajian G, Siddig EE, Fattahi A. Determination of the frequency of β-lactamase genes (blaSHV, blaTEM, blaCTX-M) and phylogenetic groups among ESBL-producing uropathogenic Escherichia coli isolated from outpatients. J Lab Med. 2020;44(1):27–33. doi:10.1515/labmed-2018-0136
35. Karanika S, Karantanos T, Arvanitis M, Grigoras C, Mylonakis E. Fecal colonization with extended-spectrum beta-lactamase–producing Enterobacteriaceae and risk factors among healthy individuals: a systematic review and metaanalysis. Rev Infect Dis. 2016;63(3):310–318. doi:10.1093/cid/ciw283
36. Zhang Q, Gao HY, Li D, et al. Clinical outcome of Escherichia coli bloodstream infection in cancer patients with/without biofilm formation: a single-center retrospective study. Infect Drug Resist. 2019;12:359–371. doi:10.2147/IDR.S192072
37. Yazdansetad S, Alkhudhairy MK, Najafpour R, et al. Preliminary survey of extended-spectrum β-lactamases (ESBLs) in nosocomial uropathogen Klebsiella pneumoniae in north-central Iran. Heliyon. 2019;5(9):e02349. doi:10.1016/j.heliyon.2019.e02349
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.